Back to Journals » Journal of Inflammation Research » Volume 19
Comparative Evaluation of Prolonged Dual Antiplatelet Therapy versus Conventional Regimens on Prognosis in Patients with High Residual Inflammatory Risk: Results from a Prospective Observational Study
Authors Wang Z, Song Y, Zheng Z, Du Y, He J, Song C, Fu R, Dong Q, Song W, Yin D, Dou K
Received 29 March 2026
Accepted for publication 15 June 2026
Published 25 June 2026 Volume 2026:19 607214
DOI https://doi.org/10.2147/JIR.S607214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Qing Lin
Ziyi Wang,1– 3,* Yanjun Song,1– 3,* Zhihao Zheng,1– 4,* Yuan Du,1– 3,* Jining He,1– 3 Chenxi Song,1– 3 Rui Fu,1– 3 Qiuting Dong,1– 3 Weihua Song,1– 3 Dong Yin,1– 3 Kefei Dou1– 3
1Cardiometabolic Medicine Center, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2State Key Laboratory of Cardiovascular Disease, Beijing, People’s Republic of China; 3National Clinical Research Center for Cardiovascular Diseases, Beijing, People’s Republic of China; 4Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kefei Dou, Cardiometabolic Medicine Center, Fuwai Hospital, National Center for Cardiovascular Diseases, State Key Laboratory of Cardiovascular Disease, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 167, Beilishi Road, Xicheng District, Beijing, 100037, People’s Republic of China, Email [email protected] Dong Yin, Cardiometabolic Medicine Center, Fuwai Hospital, National Center for Cardiovascular Diseases, State Key Laboratory of Cardiovascular Disease, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 167, Beilishi Road, Xicheng District, Beijing, 100037, People’s Republic of China, Email [email protected]
Introduction: High residual inflammatory risk (hs-CRP≥ 2mg/L) predicts worse prognosis and increased ischemic risk following percutaneous coronary intervention (PCI). The optimal duration of dual antiplatelet therapy (DAPT) and its risk-benefit profile in post-PCI patients with high residual inflammatory risk remain unclear.
Methods: Patients undergoing PCI with high residual inflammatory risk at Fuwai Hospital were consecutively enrolled. Patients were stratified into two groups based on DAPT duration: prolonged (> 12 months) and conventional (≤ 12 months) groups. The primary outcome was a composite endpoint of all-cause death, myocardial infarction, definite or probable stent thrombosis, or stroke at 3 years. The key safety outcome was the 3-year rate of Bleeding Academic Research Consortium 2, 3, or 5 bleeding.
Results: Among post-PCI patients with high residual inflammatory risk, 2440 individuals (69.5%) continued DAPT beyond 12 months. After three years of follow-up, prolonged DAPT was associated with a significantly lower risk of the primary outcome (1.5% vs. 4.2%; adjusted hazard ratio [HR]: 0.347, 95% CI: 0.224– 0.539). Similar benefits were observed for net adverse clinical events (1.4% vs. 4.1%; adjusted HR: 0.338, 95% CI: 0.216– 0.53) and for the composite endpoint of all-cause death or myocardial infarction (0.6% vs. 3.1%; adjusted HR: 0.182, 95% CI: 0.097– 0.341). Notably, the key safety endpoint did not differ significantly between the two DAPT durations during follow-up (1.0% vs. 1.2%; adjusted HR: 0.793, 95% CI: 0.401– 1.57).
Conclusion: In patients who underwent PCI with high residual inflammatory risk, prolonged DAPT improved clinical outcomes by mitigating ischemic risk without increasing clinically significant bleeding. An infographic titled “Comparative Evaluation of Prolonged Dual Antiplatelet Therapy versus Conventional Regimens on Prognosis in Patients with High Residual Inflammatory Risk” presents a study from Fuwai Hospital, Beijing, China, conducted in 2013. It involved patients undergoing PCI with high residual inflammatory risk (hs-CRP ≥ 2 mg/L). The treatment compared was Aspirin + P2Y12 inhibitor for durations of ≤ 1 year and > 1 year. Findings included two plots: MACCE and bleeding. The MACCE plot showed a significant reduction in events with prolonged DAPT (> 1 year) with end values of 6.2% and 2.4% (Log Rank P< 0.001). The bleeding plot showed no significant difference, with end values of 1.4% and 1.1% (Log Rank P=0.482). The conclusion was that prolonged DAPT (> 1 year) reduced 3-year MACCE rates without increasing bleeding risk in patients with high residual inflammatory risk.Infographic comparing prolonged DAPT vs conventional regimens after PCI in patients with high residual inflammatory risk.
Keywords: blood platelets, inflammation, percutaneous coronary intervention, high-sensitivity C-reactive protein
Introduction
Despite the widespread use of more effective lipid-lowering therapies, inflammation remains a prominent driver of residual cardiovascular risk.1,2 Inflammation, as assessed by high-sensitivity C-reactive protein (hs-CRP), has been recognized as a more potent predictor of future cardiovascular events and mortality than low-density lipoprotein cholesterol (LDL-C).3 Patients who underwent percutaneous coronary intervention (PCI) with residual inflammatory risk (hs-CRP ≥ 2 mg/L) experienced significantly higher rates of all-cause mortality, major adverse cardiovascular events, and myocardial infarction (MI),2,4,5 indicating a possible need for more intensive secondary prevention strategies for those patients.
Dual antiplatelet therapy, consisting of aspirin and a P2Y12 inhibitor, is the standard of care for preventing atherothrombotic events in patients undergoing PCI with either acute or chronic coronary syndrome.6,7 However, the optimal duration of DAPT following PCI remains a topic of ongoing debate.8,9 Several DAPT modulation strategies have been developed to improve outcomes in a precision medicine approach.10,11 Therefore, determining the optimal duration of DAPT remains a clinical challenge, which requires a delicate balance between ischemic and bleeding risks informed by individual patient characteristics and clinical circumstances.12
The current guideline-recommended DAPT duration is based mainly on the balance between ischemic and bleeding risks in the general post‑PCI population,6,7,13,14 and DAPT of 12 months is generally recommended for acute coronary syndrome (ACS) and chronic coronary syndrome (CCS) with high ischemic risk.6,7 High residual inflammatory risk (≥2 mg/L) was present in 40~50% of patients undergoing PCI,4,15 and these patients had a significantly higher ischemic risk than those with lower hs-CRP levels.16,17 In addition, inflammation is involved in the platelet and coagulation cascade activation, suggesting the potential benefit of intensive antiplatelet therapy in patients with high residual inflammatory risk.18 So far, however, no specific recommendations have been issued by existing guidelines for this subgroup of patients. Evidence evaluating the benefit-risk trade‑off of different DAPT durations in these patients is scarce, leaving a critical knowledge gap. Therefore, we aimed to investigate the effectiveness and risks of DAPT beyond 12 months versus the conventional regimen (≤12 months) in post-PCI patients with high residual inflammatory risk, and to explore whether the effect of DAPT duration is influenced by the degree of inflammatory elevation, using data from a large, prospective PCI registry.
Materials and Methods
Study Design and Population
This was an analysis using data from the Fuwai Percutaneous Coronary Intervention Registry, which consecutively enrolled patients with coronary artery disease undergoing PCI with drug-eluting stent (DES) implantation from January 2013 to December 2013 at Fuwai Hospital, National Center for Cardiovascular Diseases (Beijing, China). The details of the study design were previously reported.19,20 Clinical indications for PCI included: significant stenosis (non‑left main >70% and/or left main >50%) with typical myocardial ischemia symptoms, and severe stenosis (non‑left main ≥90%) with atypical symptoms of myocardial ischemia. This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the ethics committee of Fuwai Hospital (Approval Number 2016–847). All eligible patients provided written informed consent before enrollment. This study adhered to the RECORD (REporting of studies Conducted using Observational Routinely-collected health Data) guidelines.
Patients with high residual inflammatory risk, defined as a preoperative high-sensitivity C-reactive protein (hs-CRP) level of 2 mg/L or higher,4,21 were enrolled in this study. This threshold is recommended by the 2025 ACC Scientific Statement for identifying residual inflammatory risk,22 and it predicts recurrent ischemic events and worse clinical outcomes in the secondary prevention setting.3,23 In East Asian populations, patients undergoing PCI with hs-CRP ≥2 mg/L had a higher risk of ischemic events and cardiovascular death.16,17,24 Hence, the ≥2 mg/L cutoff is a well-validated and clinically relevant threshold for post-PCI secondary prevention risk stratification.
Participants were excluded if their data on antiplatelet therapy were missing or if they experienced adverse events (death, myocardial infarction, stroke, repeated revascularization, stent thrombosis, or Bleeding Academic Research Consortium [BARC] type 2, 3, or 5 bleeding) within 12 months after initial PCI. The detailed flow chart is presented in Figure 1.
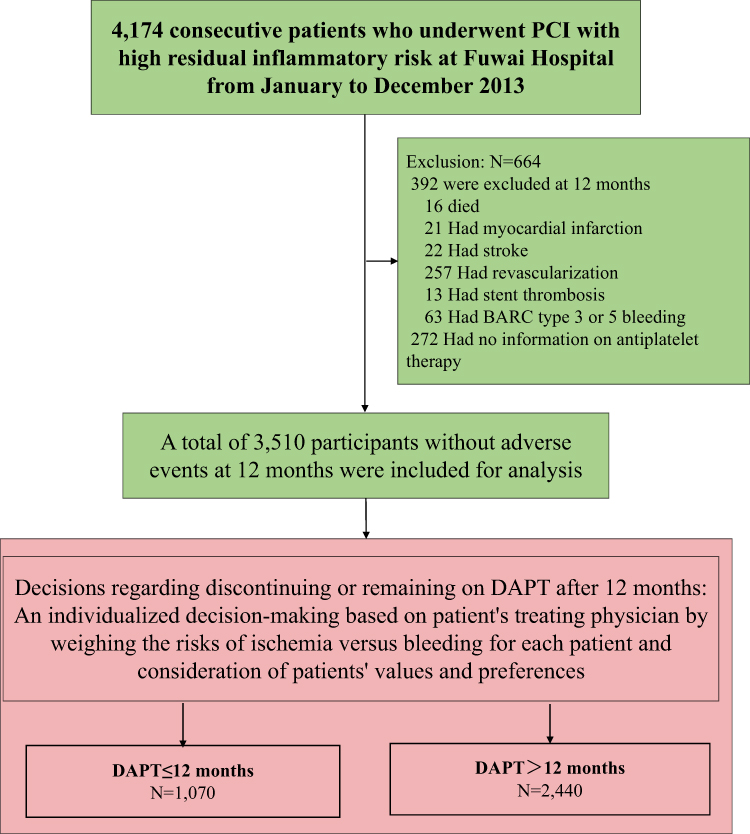 |
Figure 1 Flowchart of the study population. Abbreviations: DAPT, dual antiplatelet therapy; High residual inflammatory risk was defined as having a preoperative high-sensitivity C-reactive protein (hs-CRP) level of 2 or higher. |
Procedures and Biochemical Analysis
All PCI procedures and medical therapy during hospitalization were conducted according to the guidelines and at the discretion of cardiologists, as previously described.25
Unfractionated heparin or bivalirudin was used for anticoagulation during the procedure. Coronary angiographic and procedural data were interpreted and documented by two independent interventional cardiologists from catheter laboratory records.
Prior to the coronary intervention, blood samples were collected following at least 12-hour fasting for biochemical analysis. All tests were conducted in the clinical chemistry department of Fuwai Hospital. The level of hs-CRP was examined with standard biochemical techniques at the core laboratory of Fuwai Hospital. Concentrations of low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides, total cholesterol, fasting plasma glucose (FPG), and creatinine were examined using the same methods as reported before.26
DAPT and Data Collection
Before PCI, all patients received loading doses of aspirin (300 mg) and a P2Y12 inhibitor (clopidogrel 300 or 600 mg), unless they had already been prescribed these antiplatelet medications. After coronary intervention, aspirin 100 mg/day was prescribed indefinitely, and clopidogrel 75 mg/day was typically administered for 12 months unless there were undisputed reasons to stop DAPT. Whether to discontinue or continue the DAPT after 1 year was determined mainly by the patients’ treating physicians based on individual ischemic and bleeding risks, and the patients’ preferences.
Demographic and clinical data of all participants were collected by independent research personnel. Demographic data were comprised of age, gender, body mass index (BMI), concomitant diseases, smoking status, previous myocardial infarction, and revascularization history (PCI or coronary artery bypass grafting [CABG]). Clinical information included the initial diagnosis at admission, results from physical examinations, medical imaging, laboratory tests, and medications prescribed at discharge.
Follow-Up and Study Endpoints
After the index PCI, patients were followed up at 1, 6, and 12 months and then annually. Follow-up data were collected via medical records, clinical visits, or telephone interviews by well-trained investigators who were blinded to the study design and patients’ clinical information, through the end of the follow‑up period or until death. At each follow‑up visit, information on patients’ clinical status, angiographic and procedural characteristics, and adverse events (including but not limited to death, MI, stroke, definite or probable stent thrombosis, bleeding, repeat revascularization procedures, repeat hospitalization for any reason, and results of such, if applicable) was documented. Specifically, adherence to antiplatelet medication was routinely assessed by recording the exact start date (first dose taken) and exact stop date (last dose taken), including identifying the decision maker (ie, who decided the start or stop) and the reason each antiplatelet medication was stopped. Patients were advised to return for coronary angiography if any indications of ischemic events emerged. To obtain follow-up information for more than 2 years per patient, the follow-up period was extended to January 31, 2016. The status of antiplatelet therapy was acquired by dedicated questionnaires and the electronic prescribing system at Fuwai Hospital.
The primary endpoint was major adverse cardiac and cerebrovascular events (MACCE), which was defined as a composite of all-cause mortality, MI, stroke (hemorrhagic or ischemic), or definite or probable stent thrombosis at 3 years after the index PCI. The key safety outcome was BARC type 2, 3, or 5 bleeding. The major secondary endpoint was net adverse clinical events (NACE), a composite of cardiac death, target-vessel MI, clinically driven target-lesion revascularization, stent thrombosis, or major bleeding (BARC type 3 or 5). Other secondary endpoints included death from any cause or MI, death from cardiovascular causes, death from any cause, MI, target vessel revascularization, definite or probable stent thrombosis, and stroke.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR) and were compared using 2-sample Student’s t-tests or the Mann–Whitney U-test as appropriate. Categorical variables were presented as counts and percentages and were compared using the chi-square test or Fisher’s exact test as appropriate. The cumulative incidence of clinical events was estimated using Kaplan-Meier curves, and the differences were compared using the Log rank test. Univariable and multivariable Cox regression models were used to calculate the hazard ratios (HRs) and 95% confidence intervals (CIs). Variables significantly associated with the outcomes in the univariate Cox regression analysis (P < 0.05, Supplementary Table 1), or considered clinically relevant, were included in the multivariable Cox regression models. The following covariates were included in the final multivariable model: age, sex, BMI, diabetes, dyslipidemia, hypertension, chronic kidney disease (CKD), previous MI, and left ventricular ejection fraction (LVEF). Subgroup analyses were conducted to investigate the relationships between differences in the DAPT duration and MACCEs in patients stratified by age (< 75 vs. ≥ 75 years), sex (male vs. female), diabetes status (yes vs. no), hypertension (yes vs. no), dyslipidemia (yes vs. no), CKD (yes vs. no), history of MI (yes vs. no), current smoker (yes vs. no), or clinical presentation (ACS vs. CCS). In the subgroup analyses, all covariates used in the primary multivariable Cox regression were retained, excluding the variable used to define the subgroups. To evaluate effect modification, we performed a likelihood ratio test comparing the original regression model with the model that included an interaction term between the subgroup indicator and DAPT duration; the resulting P value was reported as the P for interaction. The interaction between hs-CRP tertiles and DAPT duration was also explored. A two-sided P < 0.05 was considered to indicate statistical significance unless otherwise specified. All statistical analyses were performed using R software version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline Characteristics
Among 10724 patients undergoing PCI (January to December 2013, Fuwai PCI registry), 4174 patients presented with high residual inflammatory risk (preoperative hs-CRP ≥2 mg/L). A total of 3510 patients were included after excluding 272 without antiplatelet information and 392 with adverse events within 12 months after PCI (Figure 1). The mean age of enrolled patients was 58.36 ± 10.36 years, and 76.5% (2684/3510) were male (Table 1). The median hs-CRP in the overall population was 4.24 (2.75, 9.04) mg/L.
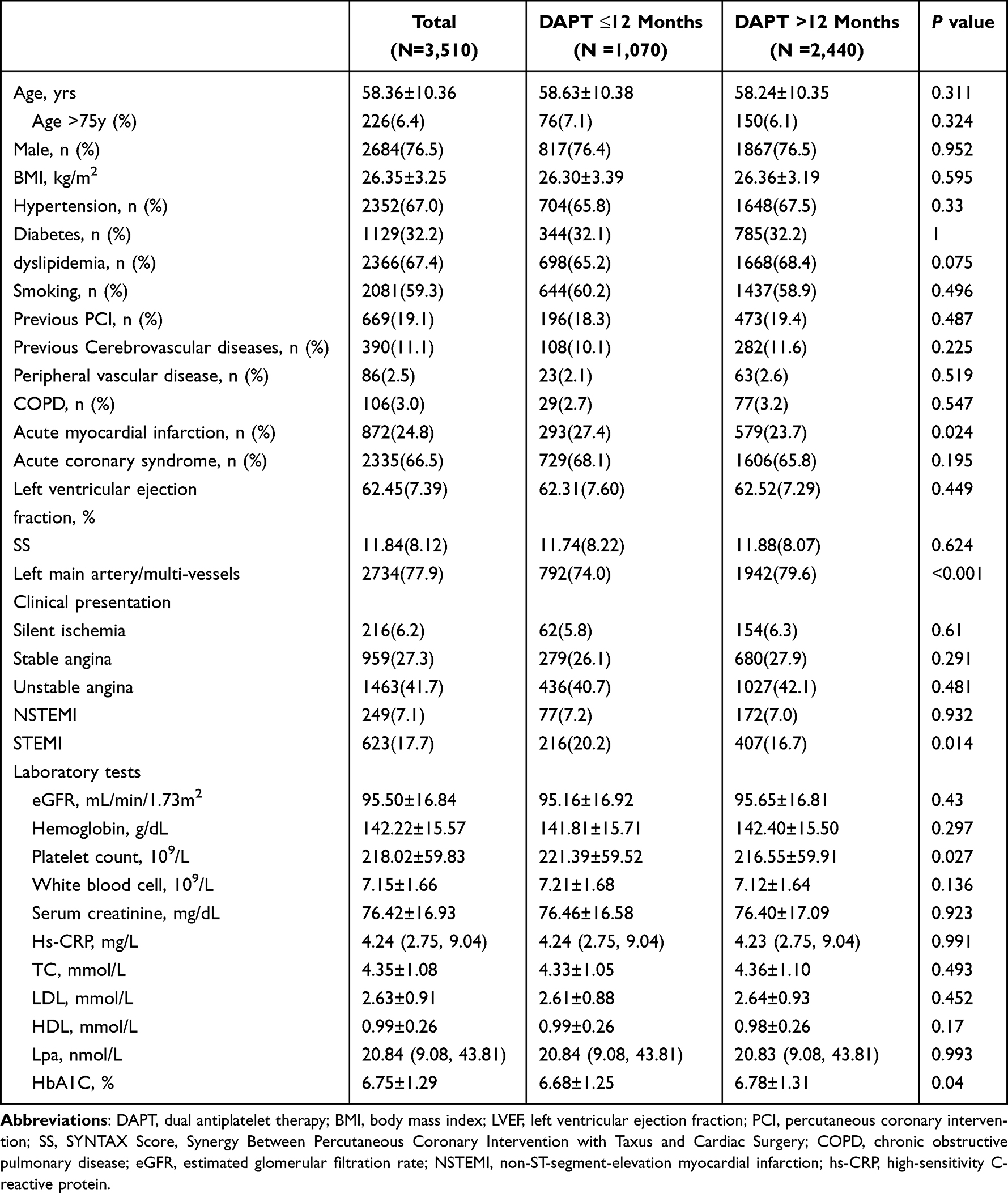 |
Table 1 Baseline Characteristics of Patients with High Residual Inflammatory Risk Undergoing PCI: a Comparison of DAPT Duration >12 Months vs ≤12 Months |
The enrolled population comprised 1070 patients receiving DAPT for ≤1 year and 2440 patients receiving DAPT for >1 year. Patients taking DAPT for ≤1 year had a higher proportion of acute MI (27.4% vs 23.7%, P=0.024), and were less likely to have left main or multivessel coronary artery disease (74.0% vs 79.6%, P<0.001). There was no significant difference in the median hs-CRP levels between the two groups. The mean duration of DAPT for the whole group was 571.35 ± 203.94 days, with a mean duration of 351.10 ± 50.09 days for the conventional DAPT group and 667.93 ± 167.70 days for the prolonged DAPT group (Table 2).
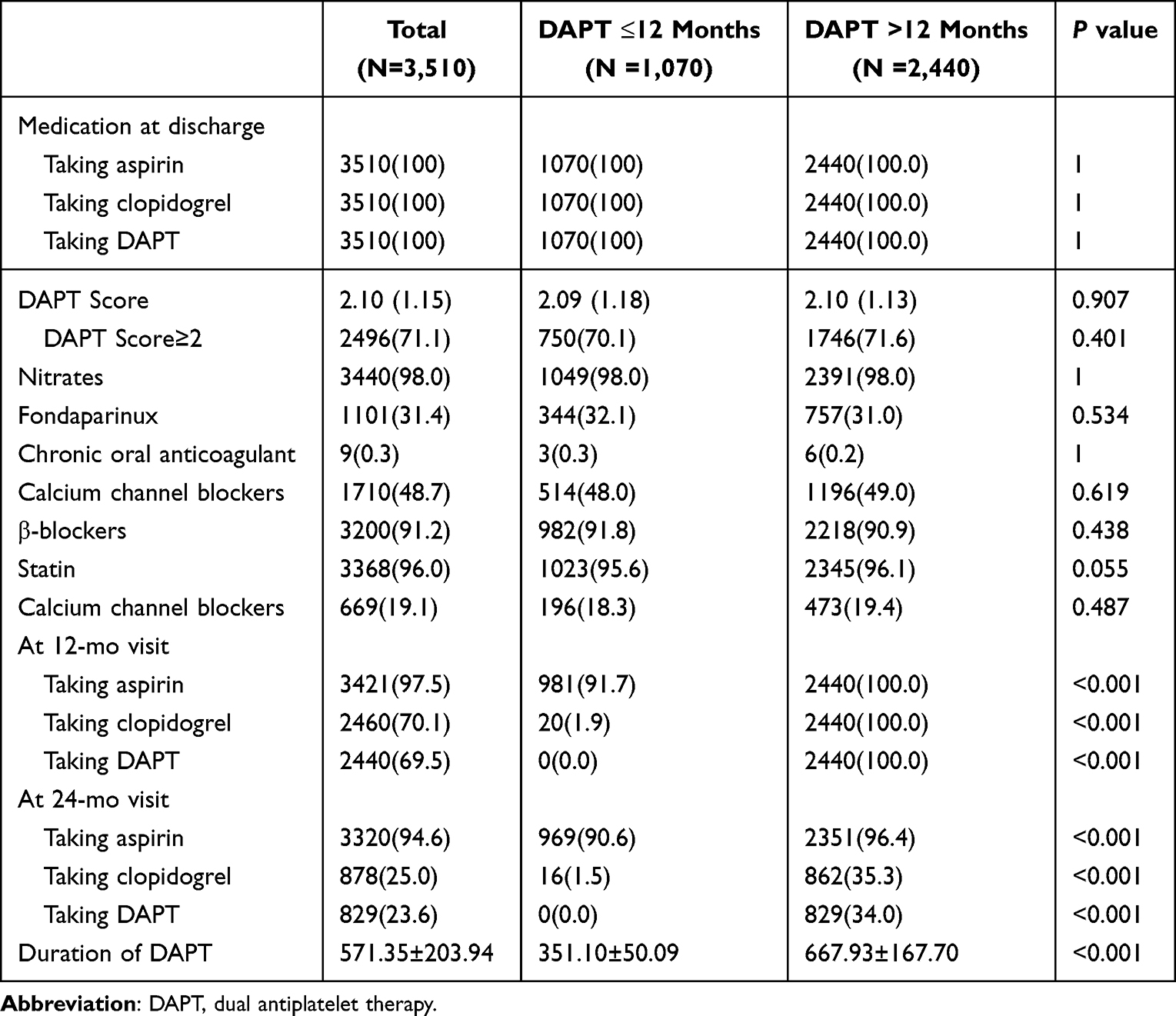 |
Table 2 Medication Information of Patients with High Residual Inflammatory Risk Undergoing PCI: a Comparison of DAPT Duration >12 Months Vs ≤12 Months |
Clinical Outcomes
After the 3-year follow-up, a total of 82 MACCEs and 37 BARC 2, 3, or 5 bleeding events were recorded. The clinical outcomes stratified by DAPT duration are presented in Figure 2 and Table 3. In the multivariable Cox regression analysis, prolonged DAPT was associated with a significantly lower prevalence of 3-year MACCEs (adjusted HR=0.347, 95% CI: 0.224–0.539, Table 4) compared with DAPT ≤1 year. The adjusted HR for the key safety outcome was 0.793 (95% CI: 0.401–1.57) for patients taking DAPT>1 year versus DAPT≤1 year.
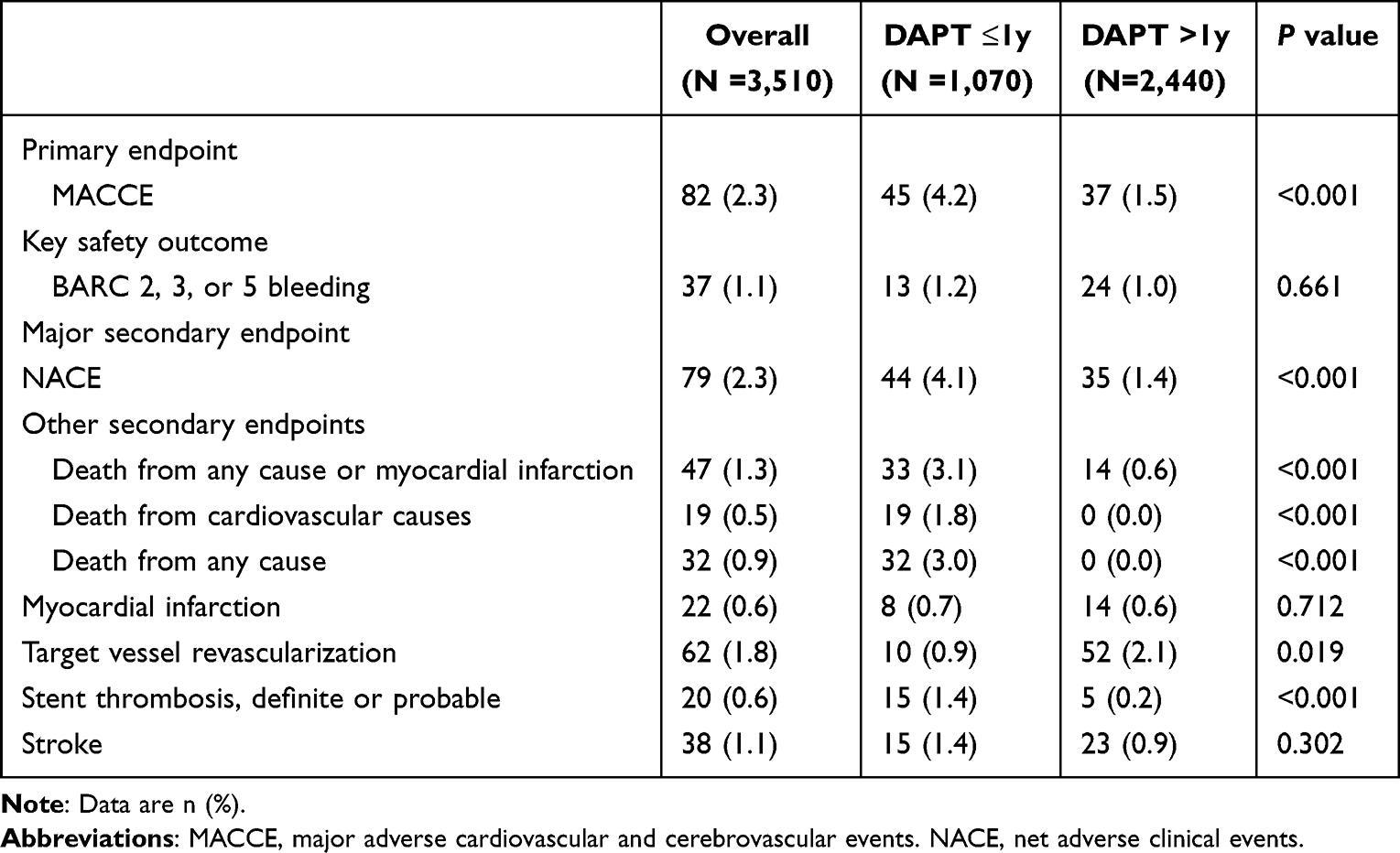 |
Table 3 Three-year Event Rates of DAPT >12 Months versus DAPT ≤12 Months Between 12 and 36 Months in Patients with High Residual Inflammatory Risk Free of Events at 12 Months After PCI |
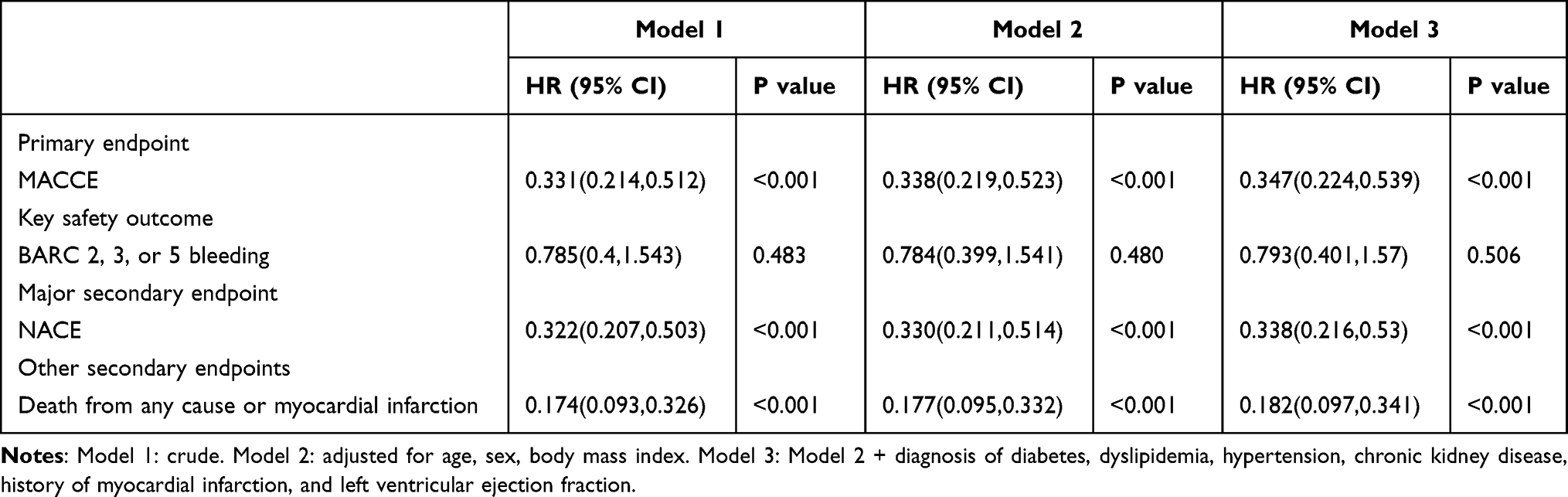 |
Table 4 Three-year Clinical Events of DAPT >12 Months Versus DAPT ≤12 Months Between 12 and 36 Months in Patients with High Residual Inflammatory Risk Free of Events at 12 Months After PCI |
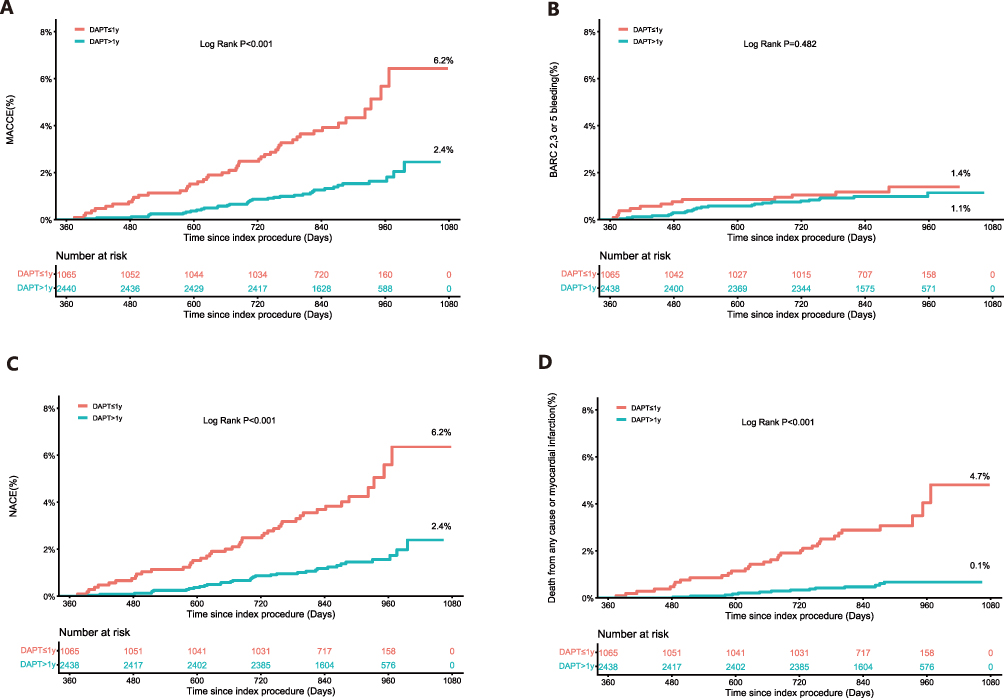 |
Figure 2 Kaplan-Meier curves for clinical outcomes according to DAPT duration (>1 year vs ≤1 year) in patients with elevated inflammatory status and drug-eluting stent implantation. (A) MACCE, (B) BARC Type 2, 3, or 5 Bleeding, (C) NACE, (D) Death from any cause or myocardial infarction. Abbreviations: DAPT, dual antiplatelet therapy; MACCE, major adverse cardiovascular and cerebrovascular event; NACE, net adverse clinical events. |
The 3-year NACE risk was significantly lower in the prolonged DAPT group (adjusted HR=0.338, 95% CI: 0.216–0.53, Table 3). A similar trend was observed for the composite endpoint of death from any cause or MI among patients taking DAPT for >1 year (adjusted HR=0.182, 95% CI: 0.097–0.341). Additionally, patients with prolonged DAPT also had lower rates of death from cardiovascular causes (0 vs. 1.8%), death from any cause (0 vs. 3.0%), and definite or probable stent thrombosis (0.2% vs. 1.4%) at 3-year follow-up (all P values <0.001). Intriguingly, the 3-year cumulative incidence of target vessel revascularization was higher in the prolonged DAPT group (2.1% vs. 0.9%, p=0.019).
Subgroup Analysis According to DAPT Duration
The reduced MACCEs associated with prolonged DAPT remained consistent across subgroups defined by age (<75 vs. ≥ 75 years), sex, hypertension, dyslipidemia, CKD, history of MI, current smoker, and clinical presentation (ACS vs. CCS) (all P for interaction values >0.05, Table 5). Diabetes was identified as an effect modifier of the relationship between DAPT duration and 3-year MACCE risk (P for interaction=0.025). Importantly, however, prolonged DAPT (>1 year) was associated with a lower cumulative incidence of MACCEs at 3 years than a shorter regimen (≤1 year) in both patients with and without diabetes.
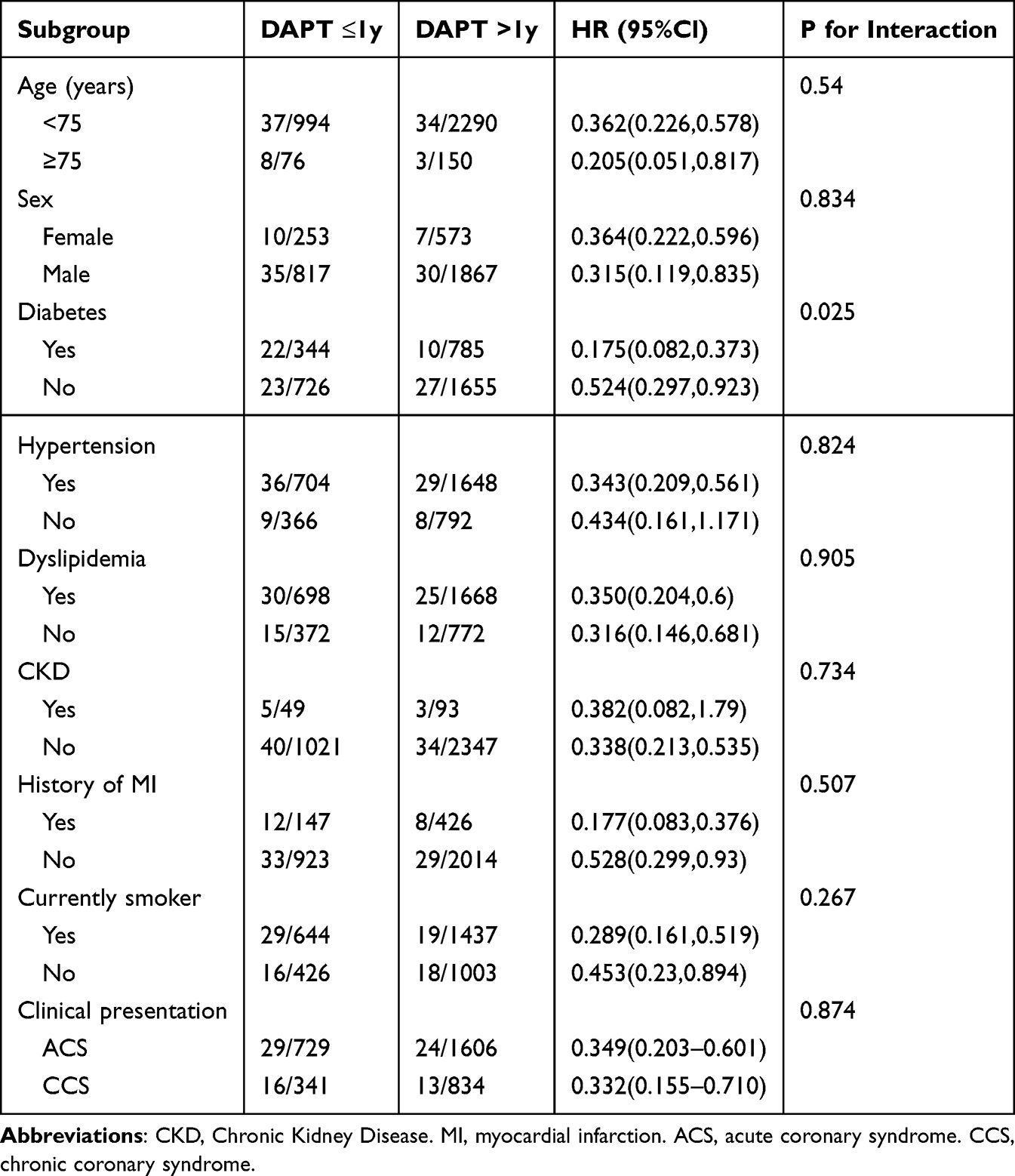 |
Table 5 Subgroup Analysis of the Primary Endpoint According to DAPT Duration |
Interaction Effect Between Hs-CRP and DAPT Duration
To assess whether the benefit of prolonged DAPT in patients with high residual inflammatory risk varies by hs-CRP levels, the interaction between hs-CRP tertiles and DAPT duration was evaluated. No significant interaction was observed for MACCE risk (P for interaction = 0.912) or for other secondary outcomes (Supplementary Table 2). This suggests that the cardiovascular benefit of prolonged DAPT was consistent across hs-CRP tertiles among patients with high residual inflammatory risk.
Discussion
This study, using a large-scale, prospective, real-world registry, investigated the efficacy and safety of extended DAPT duration in 3510 patients with high residual inflammatory risk. The major findings are as follows: (1) Prolonged DAPT (>1 year) was associated with lower risks of MACCEs, NACEs, and the composite endpoint of all-cause death and MI, without increasing the risk of BARC 2, 3, or 5 bleeding within 3 years after PCI in patients with high residual inflammatory risk. (2) Compared with those taking DAPT ≤ 1 year, patients with high residual inflammatory risk taking prolonged DAPT had lower cumulative incidence of all-cause death, death from cardiovascular causes, and definite or probable stent thrombosis over three years. (3) The effect of prolonged DAPT on 3-year MACCEs was consistent with the overall population across most major clinical subgroups. Taken together, these results provide supportive evidence for prolonged DAPT in patients undergoing PCI with high residual inflammatory risk, and inflammatory status may serve as an additional factor for clinicians to consider when deciding the optimal duration of DAPT.
The optimal duration of DAPT for patients after PCI has been a controversial and much-debated topic. An adequate duration of DAPT prevents thrombotic complications of the stented segments, reduces ischemic events, and improves clinical outcomes after coronary stent implantation.27–29 Evidence suggests that some patients at high ischemic risk will benefit from prolonged DAPT treatment beyond 12 months after PCI, including those with left main coronary artery stenting, chronic total occlusion, or elevated lipoprotein(a) concentrations.30–32 Results from the DAPT (Dual Antiplatelet Therapy) trial showed that prolonged DAPT was superior to 12-month DAPT for preventing ischemic events after drug-eluting stent (DES) implantation, with lower rates of stent thrombosis and MACCEs in groups receiving continued treatment with thienopyridine and aspirin.33 Another multi-center randomized trial suggested that patients with acute coronary syndrome receiving 12-month or longer DAPT after current-generation DES implantation had significantly lower MI rates, without a significant difference in major bleeding or BARC 2 to 5 bleeding rates.34 A previous meta-analysis demonstrated that long-term DAPT (≥12 months) led to significant reductions in MACEs in the complex PCI group, compared with short-term DAPT.35 Therefore, identifying patients at high ischemic risk is critical to determining who may benefit from the prolonged DAPT strategy.
The primary finding of our study was that, in patients undergoing PCI with high residual inflammatory risk, prolonged DAPT (>12 months) was associated with lower risks of 3-year MACCEs, NACEs, and the composite endpoint of all-cause death and MI, without significantly increasing the risk of BARC 2, 3, or 5 bleeding. This suggests that patients with high residual inflammatory risk may benefit from DAPT for more than 12 months. Similarly, a post hoc analysis of the Clopidogrel for the Reduction of Events During Observation (CREDO) study found that adding clopidogrel to aspirin reduced the 1-year composite endpoint (death, MI, or stroke) in patients in the highest two tertiles of hs-CRP after nonurgent PCI with bare metal stents, but not in the lowest tertile.36 Our study adds to previous evidence from the CREDO substudy that patients after PCI with high residual inflammatory risk are more likely to benefit from prolonged DAPT. The higher 3-year target vessel revascularization rate in the prolonged DAPT group could be partly explained by the higher proportion of patients with left main or multi-vessel coronary artery disease,37,38 and by the fact that physicians tend to extend DAPT for those with more residual lesions or complex procedures.
The mechanisms underlying the benefits of prolonged DAPT in patients with high residual inflammatory risk remain unclear. Prior studies have indicated that patients undergoing PCI with residual inflammatory risk have worse clinical outcomes, and elevated hs-CRP levels serve as an independent predictor of major adverse cardiovascular events and MACCEs.15,39,40 Additionally, a series of studies have investigated the relationship between hs-CRP levels and ischemic and bleeding risks in patients after PCI. High hs-CRP levels have been associated with increased ischemic risk, as confirmed by previous studies,16,41,42 suggesting the need for intensified ischemic risk management after PCI in patients with high residual inflammatory risk. Cook et al also observed that very late thrombosis (>1 year) after DES implantation was associated with histopathological and serological signs of inflammation,43 which may explain why patients with high residual inflammatory risk benefit from DAPT for more than 1 year. Furthermore, inflammatory conditions influence platelet function and the antiplatelet effect, both of which are closely related to ischemic risk. Jiang et al found that aspirin and clopidogrel exhibited less effective platelet aggregation inhibition and an unstable antiplatelet effect in patients with high hs-CRP levels44 Inflammatory status, as depicted by CRP or hs-CRP, has been associated with high platelet reactivity in patients receiving DAPT,45–47 which has been linked to an increased risk of ischemic events after PCI.48 Moreover, protein related to platelet aggregation was found to be reduced with colchicine therapy, further validating the modulatory impact of inflammation on platelet function.49 Accumulating evidence suggests that inflammation and thrombosis share common signaling pathways, and that inflammatory responses can promote activation of the coagulation cascade and stimulate platelet activation.18 Therefore, continuation of DAPT beyond 1 year may provide benefits from these factors for patients who underwent PCI with high residual inflammatory risk.
Bleeding risk is another crucial factor to consider when determining the duration of DAPT. Although reduced ischemic events are often at the cost of increased bleeding risk from prolonged DAPT, our findings indicated that DAPT for more than 1 year did not significantly increase BARC 2, 3, or 5 bleeding among patients with high residual inflammatory risk. Current studies on bleeding risk in patients with high residual inflammatory risk have yielded conflicting results.16,41,50 Several studies found there was no association between hs-CRP levels and bleeding risk,16,41 while other studies observed a higher bleeding risk in those with persistent residual inflammatory risk.24 Such discrepancy may be explained by different thresholds of hs-CRP level, definitions of bleeding and ethnic factors. It’s noteworthy that all participants in our study were prescribed aspirin and clopidogrel because other more potent P2Y12 inhibitors were unavailable in China during the study period. And clopidogrel was associated with lower bleeding risk as compared with ticagrelor or prasugrel,51 so it should take caution before extrapolating our findings to all DAPT regimens. Because the evidence evaluating bleeding risk in patients with high inflammatory risk is relatively limited, a robust conclusion on the safety of prolonged DAPT should be cautiously drawn from further studies.
Subgroup analysis of our study revealed that diabetes appeared to modulate the effect of DAPT on the 3-year MACCE rate in patients with high residual inflammatory risk. Patients with diabetes were more likely to benefit from prolonged DAPT therapy, corroborating previous studies showing that the benefits of extended clopidogrel therapy were more pronounced in diabetic patients receiving DES compared with nondiabetic patients.52,53 Diabetic patients often have an increased proinflammatory and prothrombotic state, and are more likely to be poor responders to antiplatelet therapy due to higher platelet turnover and pharmacokinetic changes.54,55 Taken together, these factors may help explain the favorable results of prolonged DAPT therapy in patients with diabetes.
However, the findings of our study should be interpreted cautiously due to several limitations. First, due to the observational, non-randomized nature of this single-center study, it precludes causal inferences and is limited by selection bias and unbalanced baseline characteristics. The duration of DAPT was not predefined but was determined at the discretion of cardiologists. For example, the short-DAPT group had a higher proportion of patients with MI at baseline, reflecting clinicians’ preference to prescribe prolonged DAPT to higher-risk patients. Residual confounding from unmeasured factors could not be fully identified despite robust multivariable Cox regression adjustments. The results of our study should be considered hypothesis-generating and further validated by prospective randomized trials. Second, all participants were prescribed clopidogrel and aspirin because ticagrelor and prasugrel were unavailable during the recruitment of our study, which limits the extrapolation of our conclusions to more potent P2Y12 inhibitors. Third, our analysis was based on the baseline hs-CRP levels of participants, and the hs-CRP levels during follow-up were unknown, which could have influenced the clinical outcomes. Fourth, given the lower‑than‑expected event rate, the statistical power of the present analysis may be constrained, increasing the risk of a type II error. Therefore, our findings cannot draw definitive conclusions, and large studies with adequate power are warranted to validate these findings. Fifth, the study population was defined by the PCI procedure rather than by the underlying clinical diagnosis. Patients undergoing primary PCI (for STEMI) and those undergoing elective PCI, inherently with different baseline ischemic risk, were analyzed in the same cohort. While we have reported the distribution of index diagnoses in Table 1, the study was not adequately powered to perform formal subgroup analyses by each diagnostic category or by PCI indication (primary vs. elective). Future prospective studies with larger sample sizes and predefined diagnostic subgroups are needed to validate our findings.
Conclusion
In patients undergoing PCI with high residual inflammatory risk, prolonged DAPT (>1 year) was associated with reduced 3-year MACCE rates, without a significant increase in bleeding risk. Our study suggested that inflammation could be an important factor to consider when deciding the optimal duration of DAPT. Further larger randomized trials with predefined diagnostic subgroups evaluating the efficacy and safety of DAPT for more than 1 year in patients with high residual inflammatory risk are warranted in the future.
Abbreviations
DAPT, dual antiplatelet therapy; PCI, percutaneous coronary intervention; hs-CRP, high-sensitivity C-reactive protein; MI, myocardial infarction; DES, drug-eluting stent; BARC, Bleeding Academic Research Consortium; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; FPG, fasting plasma glucose; CABG, coronary artery bypass grafting; MACCE, major adverse cardiac and cerebrovascular event; NACE, net adverse clinical events; SD, standard deviation; IQR, interquartile range; HR, hazard ratio; CI, confidence interval; CKD, chronic kidney disease; LVEF, left ventricular ejection fraction; ACS, acute coronary syndrome; CCS, chronic coronary syndrome.
Data Sharing Statement
The data that supports the findings of this study are available from the corresponding author, upon reasonable request.
Acknowledgments
The abstract of this paper was presented at the 37th Transcatheter Cardiovascular Therapeutics Conference as a poster presentation with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ in Journal of the American College of Cardiology (DOI: 10.1016/j.jacc.2025.09.1188).
Author Contributions
Ziyi Wang: Data curation, Formal analysis, Methodology, Software, Visualization, Writing – original draft;
Yanjun Song: Conceptualization, Data curation, Formal analysis, Methodology, Software, Visualization, Writing – original draft;
Zhihao Zheng: Conceptualization, Data curation, Formal analysis, Methodology, Software, Visualization, Writing – original draft;
Yuan Du: Data curation, Formal analysis, Methodology, Software, Visualization, Writing – original draft;
Jining He: Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Writing – original draft;
Chenxi Song: Data curation, Investigation, Methodology, Validation, Writing – original draft;
Rui Fu: Investigation, Methodology, Supervision, Validation, Visualization, Writing – review and editing;
Qiuting Dong: Data curation, Investigation, Methodology, Supervision, Validation, Writing – review and editing;
Weihua Song: Investigation, Methodology, Project administration, Resources, Supervision, Writing – review and editing;
Dong Yin: Investigation, Methodology, Project administration, Resources, Supervision, Writing – review and editing;
Kefei Dou: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review and editing. Kefei Dou and Dong Yin contributed equally as senior authors.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Noncommunicable Chronic Diseases–National Science and Technology Major Project (2025ZD0548200, 2024ZD0539300), the Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (CIFMS) (2025-I2M-XHCL-022, 2023-I2M-C&T-B-055), Beijing Clinical Key Specialized Projects (PM202401220002), Beijing Natural Science Foundation (24L60308), CAMS Fund for Clinical and Translational Medicine Research Project (2024-I2M-C&T-B-042), Beijing Health Promotion Association (T2021-ZX004), and the National High Level Hospital Clinical Research Funding (2022-GSP-QN-06, 2023-GSP-GG-02, 2023-GSP-QN-17, 2023-GSP-QN-34, 2023-GSP-RC-05).
Disclosure
The authors declare that they have no competing interests for this study.
References
1. Lawler PR, Bhatt DL, Godoy LC, et al. Targeting cardiovascular inflammation: next steps in clinical translation. Eur Heart J. 2021;42(1):113–15. doi:10.1093/eurheartj/ehaa099
2. Riaz H, Khan SU, Lateef N, Talluri S, Khan MS, Desai MY. Residual inflammatory risk after contemporary lipid lowering therapy. Eur Heart J Qual Care Clinl Outcomes. 2020;6(2):105–111. doi:10.1093/ehjqcco/qcz055
3. Ridker PM, Bhatt DL, Pradhan AD, Glynn RJ, MacFadyen JG, Nissen SE. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lance). 2023;401(10384):1293–1301. doi:10.1016/S0140-6736(23)00215-5
4. Kalkman DN, Aquino M, Claessen BE, et al. Residual inflammatory risk and the impact on clinical outcomes in patients after percutaneous coronary interventions. Eur Heart J. 2018;39(46):4101–4108. doi:10.1093/eurheartj/ehy633
5. Ma X, Chu H, Sun Y, et al. The effect of hsCRP on TyG index-associated cardiovascular risk in patients with acute coronary syndrome undergoing PCI. Scientific Reports. 2024;14(1):18083. doi:10.1038/s41598-024-69158-0
6. Byrne RA, Rossello X, Coughlan JJ, et al. ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720–3826. doi:10.1093/eurheartj/ehad191
7. Vrints C, Andreotti F, Koskinas KC, et al. ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45(36):3415–3537. doi:10.1093/eurheartj/ehae177
8. Valgimigli M, Landi A, Angiolillo DJ, et al. Demystifying the contemporary role of 12-month dual antiplatelet therapy after acute coronary syndrome. Circulation. 2024;150(4):317–335. doi:10.1161/CIRCULATIONAHA.124.069012
9. Byrne RA, Valgimigli M, Bhatt DL, et al. Great debate: default duration of dual antiplatelet treatment after percutaneous coronary intervention in acute coronary syndrome should be 12 months. Eur Heart J. 2025;46:1965–1978. doi:10.1093/eurheartj/ehaf070
10. Capodanno D, Mehran R, Krucoff MW, et al. Defining Strategies of Modulation of Antiplatelet Therapy in Patients With Coronary Artery Disease: a Consensus Document from the Academic Research Consortium. Circulation. 2023;147(25):1933–1944. doi:10.1161/CIRCULATIONAHA.123.064473
11. Öz A, Toprak K, Aydin E, et al. Fixed-dose antiplatelet dual combination in patients with coronary artery disease in turkish population: DAPT-TR. Arquivos brasileiros de cardiologia. 2024;121(11):e20240202. doi:10.36660/abc.20240202
12. Capodanno D, Alfonso F, Levine GN, Valgimigli M, Angiolillo DJ. ACC/AHA Versus ESC guidelines on dual antiplatelet therapy. J. Am. Coll. Cardiol. 2018;72(23):2915–2931. doi:10.1016/j.jacc.2018.09.057
13. Lawton JS, Tamis-Holland JE, Bangalore S, et al. ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation. 2022;145(3).
14. Rao SV, O’Donoghue ML, Ruel M, et al. ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: a Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025;151. doi:10.1161/CIR.0000000000001328
15. Guedeney P, Claessen BE, Kalkman DN, et al. Residual inflammatory risk in patients with low ldl cholesterol levels undergoing percutaneous coronary intervention. J Am Coll Cardiol. 2019;73(19):2401–2409. doi:10.1016/j.jacc.2019.01.077
16. Duan Y, Qiu M, Na K, et al. Inflammatory and bleeding risks on clinical outcomes in acute coronary syndrome patients undergoing percutaneous coronary intervention. Thromb Haemost. 2025;125(12):1256–1265. doi:10.1055/a-2531-3268
17. Li J, Zhu P, Tang X, et al. Combined effect of D-dimer, hs-CRP, and Lp(a) on 5-year clinical outcomes after percutaneous coronary intervention: a large real-world study in China. iScience. 2023;26(7).
18. Croce K, Libby P. Intertwining of thrombosis and inflammation in atherosclerosis. Current Opinion in Hematology. 2007;14(1):55–61. doi:10.1097/00062752-200701000-00011
19. Zhang D, Yan R, Gao G, et al. Validating the performance of 5 risk scores for major adverse cardiac events in patients who achieved complete revascularization after percutaneous coronary intervention. Can J Cardiol. 2019;35(8):1058–1068. doi:10.1016/j.cjca.2019.02.017
20. Wang H-Y, Dou K-F, Wang Y, Yin D, Xu B, Gao R-L. Benefit-Risk profile of dapt continuation beyond 1 year after pci in patients with high thrombotic risk features as endorsed by 2018 esc/eacts myocardial revascularization guideline. Cardiovascular Drugs and Therapy. 2020;34(5):663–675. doi:10.1007/s10557-020-07030-9
21. Bay B, Tanner R, Gao M, et al. Residual cholesterol and inflammatory risk in statin-treated patients undergoing percutaneous coronary intervention. Eur Heart J. 2025;46(32):3167–3177. doi:10.1093/eurheartj/ehaf196
22. Mensah GA, Arnold N, Prabhu SD, Ridker PM, Welty FK. Inflammation and Cardiovascular Disease: 2025 ACC Scientific Statement. Jacc. 2026;87(11):1381–1404. doi:10.1016/j.jacc.2025.08.047
23. Mazhar F, Faucon AL, Fu EL, et al. Systemic inflammation and health outcomes in patients receiving treatment for atherosclerotic cardiovascular disease. Eur Heart J. 2024;45(44):4719–4730. doi:10.1093/eurheartj/ehae557
24. Ahn JH, Tantry US, Kang MG, et al. Residual inflammatory risk and its association with events in east asian patients after coronary intervention. JACC Asia. 2022;2(3):323–337. doi:10.1016/j.jacasi.2021.11.014
25. Bian X, He J, Zhang R, Yuan S, Dou K. The combined effect of systemic immune-inflammation index and type 2 diabetes mellitus on the prognosis of patients undergoing percutaneous coronary intervention: a large-scale cohort study. Journal of Inflammation Research. 2023;16:6415–6429. doi:10.2147/JIR.S445479
26. Cui K, Wang H-Y, Yin D, et al. Benefit and risk of prolonged dual antiplatelet therapy after percutaneous coronary intervention with drug-eluting stents in patients with elevated lipoprotein(a) concentrations. Frontiers in Cardiovascular Medicine. 2021;8:807925
27. Mehta SR, Yusuf S, Peters RJ, et al. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 2001;358(9281):527–533. doi:10.1016/S0140-6736(01)05701-4
28. Steinhubl SR, Berger PB, Mann JT, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288(19):2411–2420. doi:10.1001/jama.288.19.2411
29. Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005;293(17):2126–2130. doi:10.1001/jama.293.17.2126
30. Choi J, Kim IS, Cho S, et al. Optimal duration for dual antiplatelet therapy after left main coronary artery stenting. Circ j. 2020;85(1):59–68. doi:10.1253/circj.CJ-20-0362
31. Sachdeva A, Hung YY, Solomon MD, McNulty EJ. Duration of dual antiplatelet therapy after percutaneous coronary intervention for chronic total occlusion. Am J Cardiol. 2020;132:44–51. doi:10.1016/j.amjcard.2020.06.066
32. Cui K, Yin D, Zhu C, et al. How do lipoprotein(a) concentrations affect clinical outcomes for patients with stable coronary artery disease who underwent different dual antiplatelet therapy after percutaneous coronary intervention? J Am. Heart Assoc. 2022;11(9). doi:10.1161/JAHA.121.023578.
33. Mauri L, Kereiakes DJ, Yeh RW, et al. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents. The New England Journal of Medicine. 2014;371(23):2155–2166. doi:10.1056/NEJMoa1409312
34. Hahn JY, Song YB, Oh JH, et al. 6-month versus 12-month or longer dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndrome (SMART-DATE): a randomised, open-label, non-inferiority trial. Lancet. 2018;391(10127):1274–1284. doi:10.1016/S0140-6736(18)30493-8
35. Giustino G, Chieffo A, Palmerini T, et al. Efficacy and safety of dual antiplatelet therapy after complex PCI. J Am Coll Cardiol. 2016;68(17):1851–1864. doi:10.1016/j.jacc.2016.07.760
36. Dosh K, Berger PB, Marso S, et al. Relationship between baseline inflammatory markers, antiplatelet therapy, and adverse cardiac events after percutaneous coronary intervention. Circ. Cardiovasc. Interv. 2009;2(6):503–512. doi:10.1161/CIRCINTERVENTIONS.109.879312
37. Lee PH, Ahn JM, Chang M, et al. Left main coronary artery disease: secular trends in patient characteristics,treatments, and outcomes. J Am Coll Cardiol. 2016;68(11):1233–1246. doi:10.1016/j.jacc.2016.05.089
38. Gragnano F, Mehran R, Branca M, et al. P2Y(12) inhibitor monotherapy or dual antiplatelet therapy after complex percutaneous coronary interventions. J Am Coll Cardiol. 2023;81(6):537–552. doi:10.1016/j.jacc.2022.11.041
39. Beyhoff N, Cao D, Mehran R, et al. Prognostic impact of high-sensitivity c-reactive protein in patients undergoing percutaneous coronary intervention according to BMI. JACC Cardiovasc Interv. 2020;13(24):2882–2892. doi:10.1016/j.jcin.2020.09.024
40. Lee M, Lee K, Kim DW, et al. Relationship of serial high-sensitivity c-reactive protein changes to long-term clinical outcomes in stabilised patients after myocardial infarction. Can J Cardiol. 2022;38(1):92–101. doi:10.1016/j.cjca.2021.10.007
41. Vinayak M, Cao D, Tanner R, et al. Impact of bleeding risk and inflammation on cardiovascular outcomes after percutaneous coronary intervention. JACC Cardiovasc Interv. 2024;17(3):345–355. doi:10.1016/j.jcin.2023.12.004
42. Liao J, Qiu M, Su X, et al. The residual risk of inflammation and remnant cholesterol in acute coronary syndrome patients on statin treatment undergoing percutaneous coronary intervention. Lipids in Health and Disease. 2024;23(1):172. doi:10.1186/s12944-024-02156-3
43. Cook S, Ladich E, Nakazawa G, et al. Correlation of intravascular ultrasound findings with histopathological analysis of thrombus aspirates in patients with very late drug-eluting stent thrombosis. Circulation. 2009;120(5):391–399. doi:10.1161/CIRCULATIONAHA.109.854398
44. Jiang H, Wang H, Liang B, Sun L, Bai L. Prognostic implication of systemic inflammatory state on antiplatelet effect in patients after percutaneous coronary intervention for ST-elevation myocardial infarction. Medicine. 2021;100(37):e27214. doi:10.1097/MD.0000000000027214
45. Marcucci R, Gori AM, Paniccia R, et al. Residual platelet reactivity is associated with clinical and laboratory characteristics in patients with ischemic heart disease undergoing PCI on dual antiplatelet therapy. Atherosclerosis. 2007;195(1):e217–223. doi:10.1016/j.atherosclerosis.2007.04.048
46. Park DW, Lee SW, Yun SC, et al. A point-of-care platelet function assay and C-reactive protein for prediction of major cardiovascular events after drug-eluting stent implantation. J Am Coll Cardiol. 2011;58(25):2630–2639. doi:10.1016/j.jacc.2011.08.057
47. Elsenberg EH, van Werkum JW, van de Wal RM, et al. The influence of clinical characteristics, laboratory and inflammatory markers on ‘high on-treatment platelet reactivity’ as measured with different platelet function tests. Thromb Haemost. 2009;102(4):719–727. doi:10.1160/TH09-05-0285
48. Bernlochner I, Steinhubl S, Braun S, et al. Association between inflammatory biomarkers and platelet aggregation in patients under chronic clopidogrel treatment. Thromb Haemost. 2010;104(6):1193–1200. doi:10.1160/TH10-05-0266
49. Yu M, Zhu ZF, Yang F, et al. Different anti-inflammatory drugs on high-sensitivity c-reactive protein in patients after percutaneous coronary intervention: a pilot randomized clinical trial. J. Cardiovasc. Pharmacol. 2024;83(3):234–242. doi:10.1097/FJC.0000000000001509
50. W-f H, L-h Z, Z-j L, et al. Association between high-sensitivity C-reactive protein and bleeding in dual antiplatelet therapy age: a retrospective observational study. BMJ Open. 2025;15(2). doi:10.1136/bmjopen-2023-082900.
51. Navarese EP, Khan SU, Kołodziejczak M, et al. Comparative Efficacy and Safety of Oral P2Y(12) Inhibitors in Acute Coronary Syndrome: network Meta-Analysis of 52 816 Patients From 12 Randomized Trials. Circulation. 2020;142(2):150–160. doi:10.1161/CIRCULATIONAHA.120.046786
52. Cho SW, Park K, Ahn JH, et al. Extended clopidogrel therapy beyond 12 months and long-term outcomes in patients with diabetes mellitus receiving coronary arterial second-generation drug-eluting stents. Am J Cardiol. 2018;122(5):705–711.
53. Thukkani AK, Agrawal K, Prince L, et al. Long-term outcomes in patients with diabetes mellitus related to prolonging clopidogrel more than 12 months after coronary stenting. J Am Coll Cardiol. 2015;66(10):1091–1101. doi:10.1016/j.jacc.2015.06.1339
54. Babes EE, Bustea C, Behl T, et al. Acute coronary syndromes in diabetic patients, outcome, revascularization, and antithrombotic therapy. Biomedicine & Pharmacotherapy = Biomedecine & Pharmacotherapie. 2022;148:112772.
55. M DB-R, Robert-Halabi M, Bloom S, et al. Aspirin for primary cardiovascular prevention in patients with diabetes: uncertainties and opportunities. Thromb Haemost. 2022;122(9):1443–1453.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.