Back to Journals » Infection and Drug Resistance » Volume 16
Comparative Efficacy of Super Bioavailable Itraconazole Capsules 50 mg vs 65 mg Twice Daily in the Management of Glabrous Tinea
Authors Shah B, Mistry D, Jairam D ![]() , Kansara K, Pandya R
, Kansara K, Pandya R ![]() , Vasani P, Dhoot D
, Vasani P, Dhoot D ![]() , Mahadkar N, Bhushan S, Barkate H
, Mahadkar N, Bhushan S, Barkate H
Received 22 February 2023
Accepted for publication 15 April 2023
Published 24 April 2023 Volume 2023:16 Pages 2409—2416
DOI https://doi.org/10.2147/IDR.S407946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Bela Shah,1 Deval Mistry,2 Dharmender Jairam,1 Kajal Kansara,1 Rutvi Pandya,1 Presha Vasani,1 Dhiraj Dhoot,3 Namrata Mahadkar,3 Sumit Bhushan,3 Hanmant Barkate3
1Department of Dermatology, B J Medical College, Civil Hospital, Ahmedabad, Gujarat, India; 2Mistry Skin Clinic, Ahmedabad, Gujarat, India; 3Department of Global Medical Affairs, Glenmark Pharmaceuticals Ltd, Mumbai, Maharashtra, India
Correspondence: Dhiraj Dhoot, Glenmark Pharmaceuticals Ltd., B D Sawant Marg, Near Bisleri Plant, Chakala, Andheri (E), Mumbai, 400099, India, Tel +919619811219, Email [email protected]
Introduction: Owing to pharmacokinetic challenges of itraconazole, super-bioavailable itraconazole (SB) was developed and recently approved in strengths of 50mg and 65mg. But comparative study was lacking between these two strengths in glabrous tinea (dermatophytosis) management. Hence, this study was planned to compare the efficacy of both these strengths in dermatophytosis.
Methods: One hundred eligible patients were enrolled in this prospective, randomized, clinical study during May-2022 to September-2022 at tertiary hospital in Ahmedabad in adults. Efficacy and safety assessments were done at week-3 and 6 with follow up at week-10 for relapse. Primary objective was to assess the proportion of patients achieving complete cure at week-6 following treatment in both the groups. Secondary outcomes compared safety, clinical and mycological cure rates.
Results: Of the 100 patients enrolled, 98 patients (50 in SB-50mg and 48 in SB-65mg group) included in the final analysis. At week 6, 20 patients (40%) and 30 patients (62.5%) achieved complete cure (p < 0.05) in SB-50mg and SB-65mg groups, respectively. In completely cured patients, relapse was reported in 3 (15%) and 5 (17%) patients of SB-50mg and SB-65mg groups, respectively (p = 1). A significant difference was noted in clearance of symptoms and lesions in SB-65mg group (p < 0.05). Moreover, similar results were also obtained in sub-group analysis of recalcitrant dermatophytosis. Both the treatments were found to be safe and well tolerated with no discontinuation.
Conclusion: Study result concluded the superiority of SB-65mg over SB-50mg in terms of cure rate and resolution of symptoms in dermatophytosis management.
Keywords: comparison, dermatophytosis, efficacy, super-bioavailable itraconazole, 50mg, 65mg
Introduction
Itraconazole is considered as one of the most reliable therapeutic options in the management of glabrous tinea1 or dermatophytosis in India.2 Though, its efficacy is unquestionable, intra-patient and inter-patient differences in bioavailability, requirement of acid and food for optimal absorption, and the poor gastrointestinal tolerability had shown fluctuations in results.3 Super-bioavailable itraconazole (SBITZ), a better itraconazole formulation, has been developed in order to address these issues4 and has been given the approval by both; the European Medicines Agency (EMA) and the United States Food and Drug Administration (USFDA) in dosages of 50 mg and 65 mg, respectively.5,6 Recently, in India as well, both these strengths were approved by Drugs Controller General of India (DCGI).7,8
SBITZ is an improved formulation of conventional itraconazole (CITZ), and hence indications approved for CITZ were applicable for SBITZ as well. Since conventional itraconazole is approved for systemic mycosis, SBITZ also received approval for the same indications. Nonetheless, itraconazole is rather frequently used in India for the treatment of dermatophytosis and so the SBITZ.
Since both the strengths have received approval on the basis of bioequivalence against CITZ 100, these can be prescribed in place of CITZ 100. However, the availability of both the strengths has caused some confusion among doctors as to where to prescribe either of these. A recently published retrospective study had concluded SB-65 as better therapeutic option over SB-50 mg.9 However, there is no prospective clinical trial to compare these strengths. Hence, this study was planned to compare the efficacy of both these strengths in the treatment of glabrous tinea.
Materials and Methods
Study Participants
This open label, prospective, double arm clinical study was carried out with prior approval of the ethics committee (Om Institutional Ethics Committee, ECR/1168/Inst/GJ/2018, Ahmedabad) and registration with Clinical trial registry of India (CTRI/2022/05/042655). After obtaining informed consent, we enrolled 100 adult patients with glabrous tinea (aged between 18 and 60 years) requiring systemic antifungal medication and had no prior history of using an oral antifungal in the previous four weeks or a topical antifungal/steroid in the prior two weeks. Individuals with serious medical disorders that would have affected clinical outcomes, such as metabolic diseases or immunocompromised conditions, were not included in the study. The study was carried out in Ahmedabad, India, in the dermatology outpatient department of a tertiary hospital during May 2022 and September 2022, in accordance with good clinical practices and the Declaration of Helsinki 1996.
Study Design and Treatment
The patients were randomized by computer generated randomization method into two groups to receive either super-bioavailable itraconazole 50 mg twice a day (SB 50) or super-bioavailable itraconazole 65 mg twice a day (SB 65), after food, for a duration of 6 weeks. According to the protocol, patients were not permitted to use any other antifungal drugs throughout the trial time, but prescribed a topical emollient combining white soft paraffin and light liquid paraffin.
Clinical examination was used to make the diagnosis, and at the initial visit, the demographics, baseline clinical traits, such as the duration of the current disease, the degree of the lesion, and the clinical sign and symptom score of the diagnosed patients were noted. All patients’ diagnoses were confirmed on direct microscopy under 10% potassium hydroxide examination (KOH mount), which was repeated at the end of the treatment period of 6 weeks. KOH mounts were made from all active clinical lesions and all fields within each smear were examined using 40X magnification. No special stains were added for microscopic examination of skin scrapings. Additionally, liver function tests (LFTs) were performed at baseline and end of treatment. Upon confirmation by KOH mount, on visit 2 (day 1), all of the patients were either prescribed SB 50 mg or SB 65 mg twice daily, after food. Scoring of Dermatology Life Quality Index (DLQI) was also recorded at the same visit.
The study lasted for ten weeks, with a six-week treatment period and a four-week observation period. Patients were monitored as per standard protocol during the course of the treatment, and clinical assessment information was gathered on visits 2 (day 1), 3 (day 22±2), and 4 (day 43±2). Those who had fully recovered were not prescribed any antifungal medication after this time of treatment, while the remaining patients were permitted to take antifungal medication at the treating physician’s discretion. By day 71±2, all patients who had fully recovered were telephoned to inquire about any disease recurrence. Figure 1 depicts the full research design in its entirety.
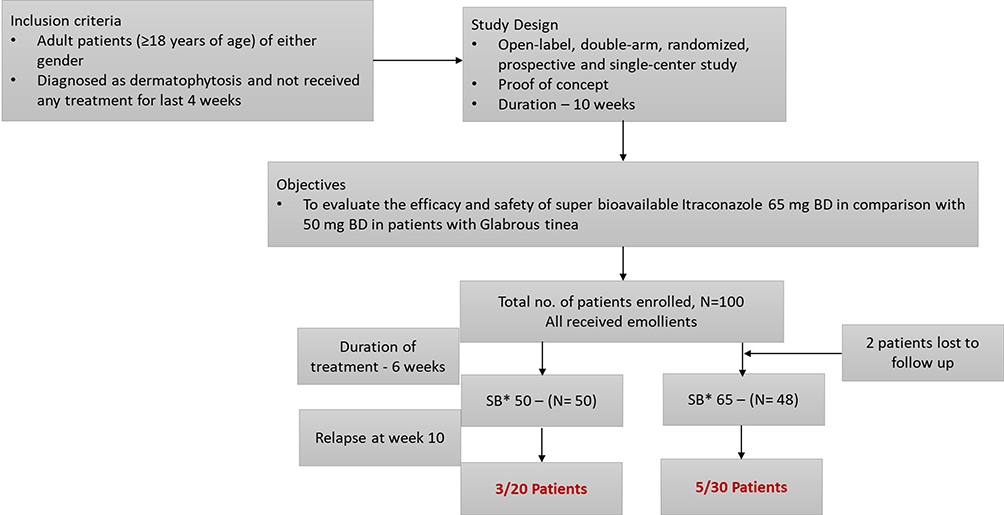 |
Figure 1 Study design. Abbreviation: *SB, Super-bioavailable itraconazole. |
Outcome Assessment
The study’s main goal was to assess the proportions of patients in each group who had fully recovered from their condition, ie, complete cure comprising clinical and mycological cure, at the end of the treatment period. Clinical cure was defined as the absence of all indications and symptoms. Scaling, erythema, pruritus, and margin continuity or elevation of the typical lesion were the four symptoms that made up the Lesion Severity Score (LSS). Each symptom was graded on a 4-point Likert scale, with 0 signifying the absence of the symptom and 3 signifying the symptom’s highest level of intensity. The individual indications and symptom score at each time point were added up to create the LSS (range 0–12). Body Surface Area (BSA) was used to calculate the Area severity score (ASS), which ranged from 0 to 3. A score of 0 indicates no lesions, a score of 1 indicates BSA involvement of less than 3%, a score of 2 indicates BSA involvement of between 3% and 10%, and a score of 3 indicates BSA involvement of more than 10%.10 Additionally, Quality of Life was assessed by DLQI pre and post treatment.
Analysis Set
For analysis of efficacy and safety, patients who had received at least one dosage of the medicine and had attended at least one post-baseline follow-up visit were referred to as the full analysis set (FAS).
Analytical Statistics
Initial clinical and demographic data were provided as means with standard deviations, percentages, and numbers. The chi-square test was used to examine the difference in the percentage of patients with total signs and symptom scores (based on improvement criteria). The significance threshold was set at 0.05. The Fisher’s exact test was used to compare the two groups. SPSS version 16.0 (SPSS, Chicago, IL, USA) was used to conduct all statistical analyses.
Results
Study Participants
Ninety-eight of the 100 patients who participated in the study were part of the FAS. The SB 50 mg group had 50 patients, while the SB 65 mg group included 48 patients. Table 1 lists all of the standard characteristics. In both groups, the patient distribution was uniform. Most patients in both groups had at least five lesions. In the SB 50 and SB 65 groups, 72% and 75% of patients, respectively, experienced illnesses that lasted longer than six months.
 |
Table 1 Demographic Information of All Patients in Both the Groups |
Treatment Response
Complete Cure
At week 6, 20 patients (40%) and 30 patients (62%) achieved complete cure in the SB 50 group and SB 65 groups, respectively, which was statistically significant (p < 0.05). Of these completely cured patients, three patients in SB 50 (15%) and 5 patients in SB 65 (17%) group reported to have relapse at week 10.
On subgroup analysis, similar results were obtained for recalcitrant dermatophytosis (≥6 months of duration); in the SB 50 group, 13 out of 36 patients (36%) and in the SB 65 group 23 out of 36 patients (64%) achieved complete cure (p<0.05) of which 2 patients (15%) and 4 patients (17%) relapsed at week 10 in SB 50 and SB 65 group, respectively, as shown in Table 2.
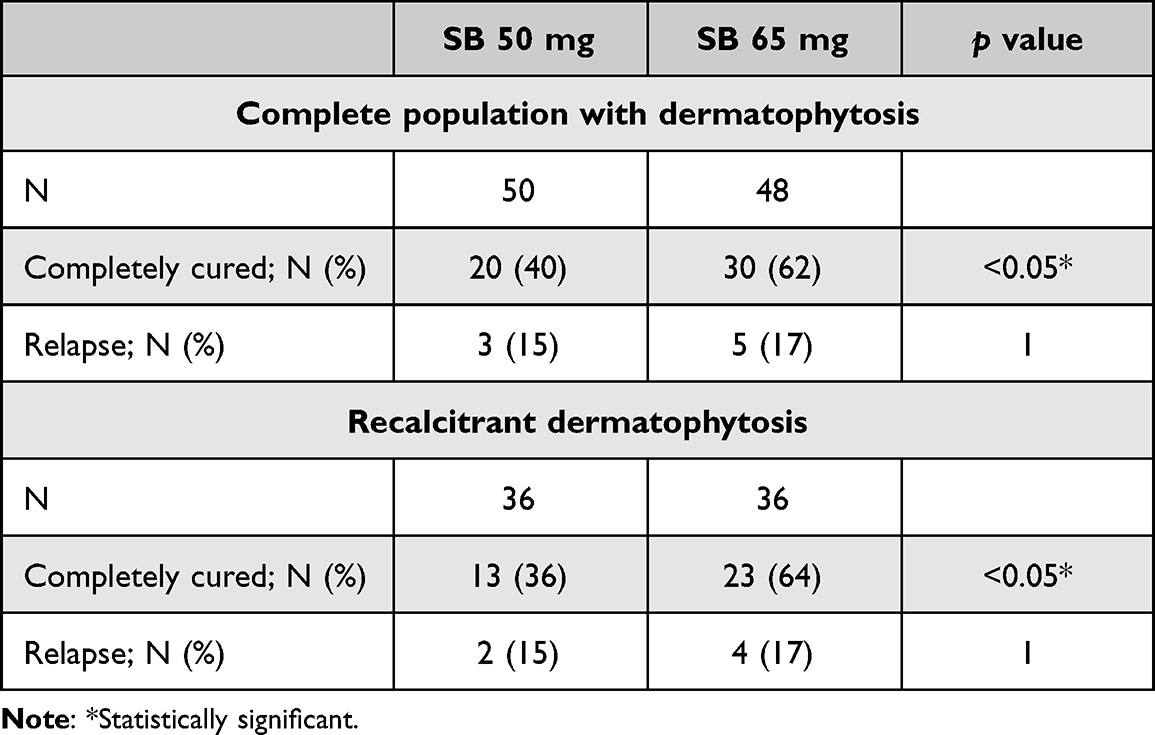 |
Table 2 Complete Cure Rates in Different Dermatophytosis Groups |
Improvement in Mean Scores
In the SB 50 group, the mean LSS decreased from 7.21±2.04 to 4.27±1.52 (41% reduction) after week 3, whereas in the SB 65 group, it decreased from 7.50±1.90 to 4.04±1.50 (46% reduction). By week 6, the mean LSS in the SB 50 and SB 65 groups had further decreased to 1.57±1.22 (78% reduction) and 0.78±0.82 (90% reduction), respectively. On intergroup comparison, a statistically significant difference was detected at week 6 (p < 0.05) in the SB 65 group, as indicated in Table 3. Both treatments were statistically significant in lowering LSS at both visits (p < 0.05) from baseline.
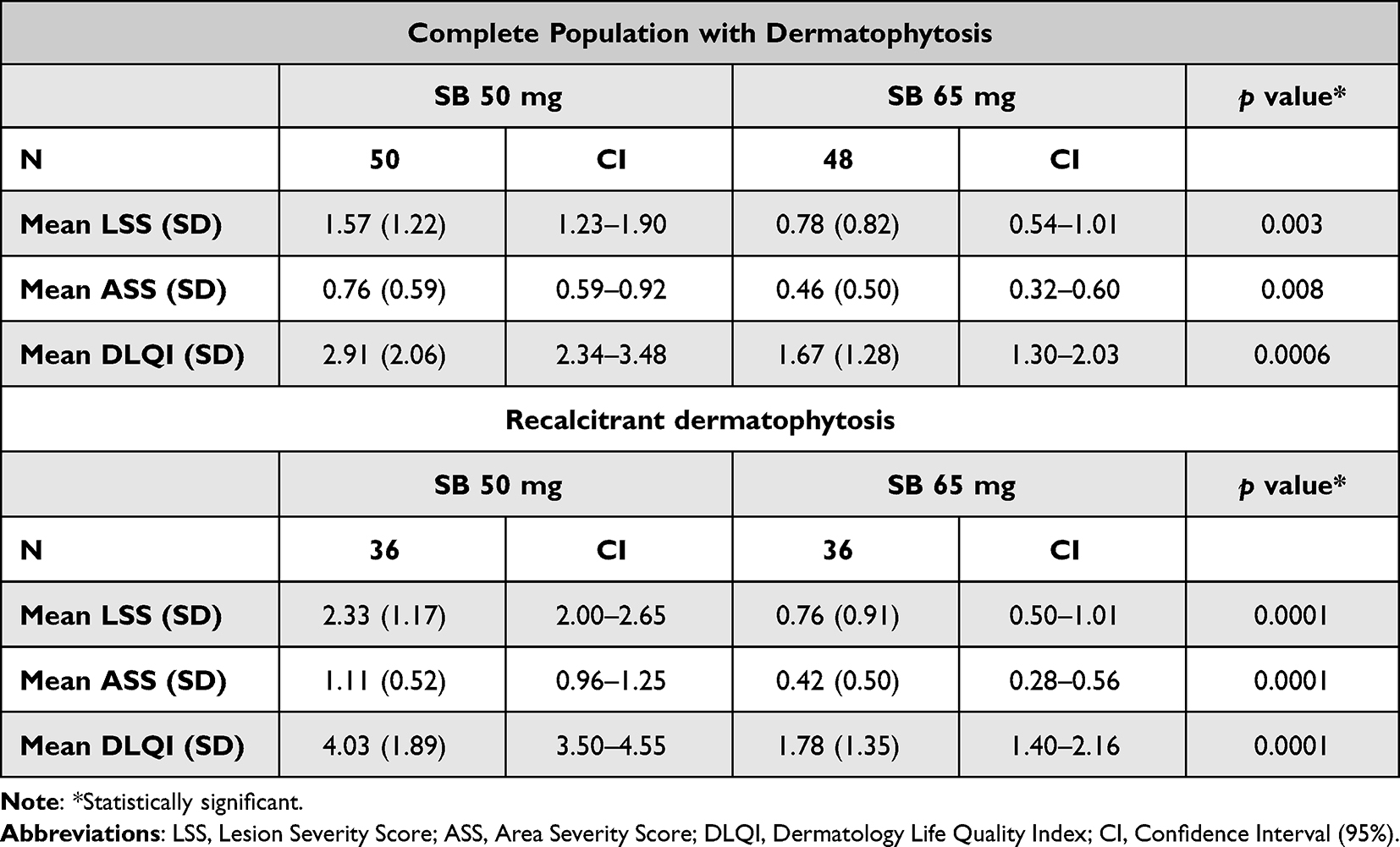 |
Table 3 Efficacy Scores in Terms of Mean LSS, ASS and DLQI at Week 6 |
Significant lesion clearance was also observed in both groups at both visits. At week 3, the mean ASS of 2.81±0.42 reduced to 1.63±0.49 (42% reduction) in the SB 50 group, whereas it reduced from 2.92 ±0.34 to 1.54±0.50 (47% reduction) in the SB 65 group. At week 6, the mean ASS in the SB 50 group decreased even more, to 0.76±0.59 (73% reduction), as opposed to 0.46±0.50 (84% reduction), in the SB 65 group. At both visits, it was determined that both groups had statistically significant reductions in the size of the lesions; however, as indicated in Table 3, SB 65 was more statistically significant than SB 50 at week 6.
Mean DLQI score of 13.43±2.54 reduced to 2.91±2.06 (78%) in SB 50 group while in SB 65 group, it reduced to 1.67±1.28 from 13.64±2.12 (88%) which was statistically significant for SB 65 over SB 50. Similar results were also seen in recalcitrant dermatophytosis (Table 3).
Safety Outcome
Treatment in both the group was found to be well tolerated by patients with no adverse events in any of the groups. Additionally, no derangements in liver enzymes were noted at the end of treatment in both the groups. There were no serious adverse events or discontinuation of treatment in any of the groups.
Discussion
Recently, in India, there has been a radical change in presentation of dermatophytosis with change in the disease pattern and its occurrence, recurrence and chronicity which have added to the morbidity and reduced quality of life. This may be partly attributed to the changing lifestyles, misuse of topical corticosteroids and injudicious use of oral antifungals.11,12 Despite these, the most helpful medication is an older but still effective antifungal called itraconazole. However, itraconazole’s utility is constrained by its inherent pharmacokinetic issues, which cause uneven therapeutic concentrations.13 SBITZ, a more recent formulation, has demonstrated more consistently achieving therapeutic concentration when compared to CITZ.14,15 SBITZ 50 mg and 65 mg were recently approved by DCGI in India.7,8 Both strengths can be prescribed in place of CITZ 100 mg because they have both been approved based on their bioequivalence to CITZ 100 mg. Yet, the availability of these strengths presented some positioning issues for either strength to physicians. In order to compare the clinical efficacy of both strengths in the treatment of glabrous tinea infection, we therefore undertook this prospective study.
The results of this study exhibited higher cure rates in SB 65 group than SB 50 group. In SB 65 group, 62% of patients achieved a complete cure, whereas the same was achieved by 40% of the patients in the SB 50 group. In a recently published retrospective study, 75% of the patients reported complete cure while 63% reported the same in SB 65 and SB 50 groups, respectively, in 8 weeks.9 But in this study, topical antifungals were also prescribed in addition to SBITZ. Similarly, Shenoy et al had also demonstrated 65% complete cure rate with SBITZ 50 only at week 4.16 The results of both the studies are not in accordance with the current study for SB 50 results. A slightly lower cure rate in both groups has been seen when compared to current studies on CITZ cure rates.12,17 Yet, in our study, the length of the treatment was likewise on the shorter side.
Both groups experienced recurrence, and there was no statistically significant difference between them. Similar results were seen for recalcitrant dermatophytosis on subgroup analysis, where SB 65 group showed statistically significant results above SB 50 group.
Additionally, significant percentage reductions in all mean LSS and ASS were observed across the board as well as in patient subgroups, demonstrating that SB 65 cleared lesions and severity more effectively than SB 50. While 78% of individuals in our study experienced a reduction in LSS, 93% of patients in the SB 50 group did so in a previously published study.18 In our investigation, greater LSS clearance was seen with SB 65 group. Similar results were also found for ASS clearance demonstrating superiority of SB 65 over SB 50 group. Notably, a significant portion of individuals who did not recover experienced ongoing itching. According to a recent article, it might be caused by dermatophytes altering barrier function.19
These better results with SB 65 could be attributed to better serum concentration achieved by SB 65 mg. Previously published articles had documented relative bioavailability of 180% and absolute bioavailability of 90% with SB 65.20 Abuhelwa showed relative bioavailability of 173% with SB 50 mg.4 Moreover, as per the published reports, real itraconazole concentration in SB 50 mg is about 46 mg and about 58 mg with SB 65 mg.5,6,9,20 As a result, only 69% of the patients achieved therapeutic concentration with SB 50 whereas in SB 65, it was achieved by 81% of the patients.14,21 But these values were related to systemic mycosis and Khurana et al had mentioned the minimal serum concentration requirement for efficacy of itraconazole as 200 ng/mL in the management of dermatophytosis.22
However, one of the most significant factors affecting systemic antifungals’ efficiency in the management of dermatophytosis is their concentration in the skin. Itraconazole’s stratum corneum concentration and sebum excretion in patients with dermatophytosis in particular are crucial due to the drug’s lipophilicity.22–24 Cauwenbergh et al had reported sebum concentration of itraconazole about 2–5 times higher than corresponding serum concentration.25 Thus, a higher serum concentration of drug can lead to high skin concentration resulting in extensive eradication of fungi from the lesions. This was supported by recently published study on serum and sebum analysis of SB 50 mg and SB 65 mg in which authors reported statistically significant serum and sebum concentration with SB 65 mg than SB 50 mg.26 The improvement in the SB 65 group in our study may therefore be attributable to the potential for increased sebum content.
There were no adverse effects reported in either group, and all patients in both groups tolerated the therapy quite well.
According to our knowledge, this is the first clinical comparison research of SBITZ in dermatophytosis that compares two different strengths. Although the medication in this trial lasted for six weeks, other studies on itraconazole have shown that longer-term therapy may be necessary to avoid relapse.12,17 Smaller sample size stands out as a major limitation of this study, therefore long-term clinical trials with a bigger sample size are necessary to confirm its findings.
Conclusion
Patients treated with SB 65mg demonstrated significant results over SB 50mg in terms of achieving complete cure rates in dermatophytosis. Additionally, significant improvement in the clearance of lesions and cure rate in subgroup of patients like recalcitrant dermatophytosis was also noticed for SB 65 mg capsules. All these findings may lead SB 65mg to be placed in the armamentarium of dermatophytosis management.
IRB Approval Status
This study was approved by an independent ethics committee.
Data Sharing Statement
The datasets are available only on request due to privacy/ethical restrictions, and can be requested from [email protected].
Funding
The drugs used in this study were supplied by Glenmark Pharmaceuticals Ltd. The company had no role in study design and conduct of the study, nor the collection, management, analysis, and interpretation of the data.
Disclosure
Dhiraj Dhoot, Namrata Mahadkar, Sumit Bhushan, Hanmant Barkate are employees of Glenmark Pharmaceutical Ltd. The rest of the authors have no other conflicts of interest to declare in this work.
References
1. Rengasamy M, Shenoy MM, Dogra S, et al. Indian Association of Dermatologists, Venereologists and Leprologists (IADVL) Task Force against Recalcitrant Tinea (ITART) Consensus on the Management of Glabrous Tinea (INTACT). Indian Dermatol Online J. 2020;11(4):502–519. doi:10.4103/idoj.IDOJ_233_20
2. Das S, De A, Saha R, et al. The current Indian epidemic of dermatophytosis: a study on causative agents and sensitivity patterns. Indian J Dermatol. 2020;65:118–122. doi:10.4103/ijd.IJD_203_19
3. Lindsay J, Mudge S, Thompson GR
4. Abuhelwa AY, Foster DJ, Mudge S, Hayes D, Upton RN. Population pharmacokinetic modeling of itraconazole and hydroxyitraconazole for oral SUBA-itraconazole and Sporanox capsule formulations in healthy volunteers in fed and fasted states. Antimicrob Agents Chemother. 2015;59:5681–5696. doi:10.1128/AAC.00973-15
5. European Medicines Agency. List of nationally authorised medicinal products. Available from: https://www.ema.europa.eu/en/documents/psusa/itraconazole-list-nationally-authorised-medicinal-products-psusa/00001798/201703_en.pdf.
6. Mayne Pharma. TOLSURA prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208901s000lbl.pdf.
7. Central Drugs Standard Control Organization. List of drugs approved from SND Division from 01.01.2020 to 30.06.2020. Available from: https://cdsco.gov.in/opencms/resources/UploadCDSCOWeb/2018/UploadApprovalMarketingFDC/List%20of%20drugs%20approved%20from%20SND%20Division%20till%2030%20June%202020.pdf.
8. Central Drugs Standard Control Organization. Recommendations of the SEC (Antimicrobial & Antiviral) made in its 103nd meeting held on 25.08.2021 at CDSCO HQ, New Delhi. Available from: https://cdsco.gov.in/opencms/resources/UploadCDSCOWeb/2018/UploadCommitteeFiles/RecommendationSE%20Antimicrobial%20&%20Antiviral%2025.08.2021n.pdf.
9. Mahadkar N, Dhoot DS, Barkate H. Comparative real-world effectiveness and safety of super-bioavailable itraconazole 50 mg bd and 65 mg bd in the management of dermatophytosis. Int J Res Dermatol. 2022;8:433–436. doi:10.18203/issn.2455-4529.IntJResDermatol20221567
10. Rajagopalan M, Inamadar A, Mittal A, et al. Expert consensus on the management of dermatophytosis in India (ECTODERM India). BMC Dermatol. 2018;18(1):6. doi:10.1186/s12895-018-0073-1
11. Sarkar S. A treatise on topical corticosteroid in dermatology. Indian J Dermatol. 2018;63:530–531.
12. Singh SK, Subba N, Tilak R. Efficacy of terbinafine and itraconazole in different doses and in combination in the treatment of tinea infection: a randomized controlled parallel group open labeled trial with clinico-mycological correlation. Indian J Dermatol. 2020;65:284–289. doi:10.4103/ijd.IJD_548_19
13. Prentice AG, Glasmacher A. Making sense of itraconazole pharmacokinetics. J Antimicrob Chemother. 2005;56(Suppl 1):i17–i22 . doi:10.1093/jac/dki220
14. Lindsay J, Sandaradura I, Wong K, et al. Serum levels, safety and tolerability of new formulation SUBA-itraconazole prophylaxis in patients with haematological malignancy or undergoing allogeneic stem cell transplantation. J Antimicrob Chemother. 2017;72:3414–3419. doi:10.1093/jac/dkx295
15. Nield B, Larsen SR, van Hal SJ. Clinical experience with new formulation SUBA®-itraconazole for prophylaxis in patients undergoing stem cell transplantation or treatment for haematological malignancies. J Antimicrob Chemother. 2019;74:3049–3055. doi:10.1093/jac/dkz303
16. Shenoy M, Dhoot D, Mahajan H, Barkate H. An open-label, randomized, double-arm clinical trial to compare the effectiveness and safety of super bioavailable itraconazole capsules and itraconazole capsules in the management of dermatophytosis in India. Clin Cosmet Investig Dermatol. 2021;14:1367–1376. doi:10.2147/CCID.S326642
17. Khurana A, Agarwal A, Agrawal D, et al. Effect of different itraconazole dosing regimens on cure rates, treatment duration, safety, and relapse rates in adult patients with tinea corporis/cruris: a randomized clinical trial. JAMA Dermatol. 2022;158:1269–1278. doi:10.1001/jamadermatol.2022.3745
18. Ghate S, Dhoot D, Mahajan H, Barkate H. Clinical assessment of super bioavailable Itraconazole 50 mg in dermatophytosis (clear 50). IP Indian J Clin Exp Dermatol. 2021;7:125–129. doi:10.18231/j.ijced.2021.024
19. Sardana K, Gupta A, Mathachan SR. Immunopathogenesis of dermatophytoses and factors leading to recalcitrant infections. Indian Dermatol Online J. 2021;12:389–399. doi:10.4103/idoj.IDOJ_503_20
20. Rauseo AM, Mazi P, Lewis P, Burnett B, Mudge S, Spec A. Bioavailability of single-dose SUBA-itraconazole compared to conventional itraconazole under fasted and fed conditions. Antimicrob Agents Chemother. 2021;65:e0013421. doi:10.1128/AAC.00134-21
21. Thompson GR, Lewis P, Mudge S, Patterson TF, Burnett BP. Open-label crossover oral bioequivalence pharmacokinetics comparison for a 3-day loading dose regimen and 15-day steady-state administration of SUBA-itraconazole and conventional itraconazole capsules in healthy adults. Antimicrob Agents Chemother. 2020;64:e00400–20. doi:10.1128/AAC.00400-20
22. Khurana A, Agarwal A, Singh A, et al. Predicting a therapeutic cut-off serum level of itraconazole in recalcitrant tinea corporis and cruris - a prospective trial. Mycoses. 2021;64:1480–1488. doi:10.1111/myc.13367
23. De Doncker P, Pande S, Richarz U, Garodia N. Itraconazole: what clinicians should know? Indian J Drugs Dermatol. 2017;3:4–10. doi:10.4103/ijdd.ijdd_20_17
24. Sardana K, Arora P, Mahajan K. Intracutaneous pharmacokinetics of oral antifungals and their relevance in recalcitrant cutaneous dermatophytosis: time to revisit basics. Indian J Dermatol Venereol Leprol. 2017;83:730–732. doi:10.4103/ijdvl.IJDVL_1012_16
25. Cauwenbergh G, Degreef H, Heykants J, Woestenborghs R, Van Rooy P, Haeverans K. Pharmacokinetic profile of orally administered itraconazole in human skin. J Am Acad Dermatol. 1988;18:263–268. doi:10.1016/S0190-9622(88)70037-7
26. Dhoot DS, Mahadkar N, Jain G, Kesharwani P. Comparative analysis of serum and sebum concentration of super-bioavailable itraconazole 50 versus 65 mg in healthy adult volunteers. Int J Res Dermatol. 2023;9:59–60. doi:10.18203/issn.2455-4529.IntJResDermatol20223279
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.