Back to Journals » Journal of Pain Research » Volume 19
Comparative Efficacy of Scalene versus Scapular Approach for Ultrasound-Guided Corticosteroid Hydrodissection in Dorsal Scapular Nerve Entrapment: A Randomized Controlled Trial
Authors Elawamy AM, Lam KHS ![]() , Allam AES
, Allam AES ![]() , Abo Elfadl GM
, Abo Elfadl GM ![]() , Moshrif A
, Moshrif A ![]() , Ahmad AA, Mohamed EF
, Ahmad AA, Mohamed EF ![]() , AbdelRady MM
, AbdelRady MM ![]() , Shabaan N, Ghoraba Y, Yoon Y
, Shabaan N, Ghoraba Y, Yoon Y ![]() , Hassanien M
, Hassanien M
Received 23 October 2025
Accepted for publication 19 February 2026
Published 26 February 2026 Volume 2026:19 576439
DOI https://doi.org/10.2147/JPR.S576439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Abdelraheem Mahmoud Elawamy,1 King Hei Stanley Lam,2– 6 Abdallah El-Sayed Allam,7,8 Ghada Mohammad Abo Elfadl,1 Abdelhfeez Moshrif,9 Ashraf Abdelsalam Ahmad,9 Eman F Mohamed,10 Marwa Mahmoud AbdelRady,1 Nehal Shabaan,11 Yasser Ghoraba,11 Yonghyun Yoon,4,6,12,13 Manal Hassanien14
1Anesthesia, Intensive Care and Pain Department, Faculty of Medicine, Assiut University, Assiut, Egypt; 2Department of Family Medicine, Faculty of Medicine, the Chinese University of Hong Kong, Shatin, Hong Kong; 3Department of Family Medicine, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong; 4Department of Clinical Research, The International Association of Musculoskeletal Medicine, Kowloon Bay, Kowloon, Hong Kong; 5Department of Clinical Research, The Hong Kong Institute of Musculoskeletal Medicine, Kowloon Bay, Kowloon, Hong Kong; 6Department of Clinical Research, The International Academy of Regenerative Medicine, Incheon, Republic of Korea; 7Department of Physical Medicine, Rheumatology and Rehabilitation, Faculty of Medicine, Tanta University, Tanta, Egypt; 8Morphological Madrid Research Center (MoMaRC), Madrid, Spain; 9Rheumatology Department, Faculty of Medicine, Al-Azhar University, Assiut, Egypt; 10Internal Medicine and Rheumatology, Faculty of Medicine for Girls, Al-Azhar University, Assiut, Egypt; 11Neurosurgery Department, Faculty of Medicine, Tanta University, Tanta, Egypt; 12Department of Orthopedic Surgery, Hallym University Gangnam Sacred Heart Hospital, Seoul, Republic of Korea; 13IncheonTerminal Orthopedics, Incheon, Republic of Korea; 14Rheumatology and Rehabilitation Department, Faculty of Medicine, Assiut University, Assiut, Egypt
Correspondence: King Hei Stanley Lam, Department of Family Medicine, Li Ka Shing Faculty of Medicine, the University of Hong Kong, Pokfulam, Hong Kong, Tel +85223720888, Fax +85223720848, Email [email protected]
Background: Dorsal scapular nerve (DSN) entrapment is a common cause of chronic interscapular pain. Ultrasound-guided corticosteroid hydrodissection is an effective intervention, but no randomized controlled trial has directly compared the efficacy of the proximal (scalene) and distal (scapular) injection approaches.
Methods: In this multicentre, prospective, randomized controlled study conducted across seven centers in Egypt, patients and outcome assessors were blinded; proceduralists could not be blinded due to inherent technical differences. Sixty patients with electrodiagnostically-confirmed DSN entrapment were randomly assigned to receive a single ultrasound-guided hydrodissection injection of triamcinolone acetonide (40 mg) and lidocaine in 10 mL saline. Group I (n=30) received the injection at the DSN within the middle scalene muscle, while Group II (n=30) received it below the levator scapulae muscle. The primary outcome was the Visual Analog Scale (VAS) for pain at rest. Secondary outcomes included VAS during movement, Fatigue Assessment Scale (FAS), patient satisfaction, and motor distal latency, assessed at baseline, 1, and 3 months.
Results: The groups were well-matched at baseline. The scalene group demonstrated a significantly greater reduction in pain at rest at both 1 month (Z = 6.68, p < 0.001) and 3 months (Z = 6.68, p < 0.001). Similar significant differences favoring the scalene group were observed for pain during movement and fatigue scores at all follow-ups (p < 0.001). Patient satisfaction was significantly higher in the scalene group at all follow-ups (p < 0.001). No significant between-group difference was found in motor distal latency, and no major complications occurred.
Conclusion: Ultrasound-guided corticosteroid hydrodissection administered at the middle scalene muscle resulted in significantly greater short-term improvement in pain, fatigue, and patient satisfaction over three months compared to the distal scapular approach. The scalene approach may be considered more effective for short-term management, though longer-term studies are needed to confirm durability.
Keywords: dorsal scapular neuropathy, ultrasonography, interventional, nerve block, hydrodissection, middle scalene muscle, randomized controlled trial, pain management
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Gakhar has been published for this article.
Introduction
The dorsal scapular nerve (DSN) is a significant motor nerve that arises primarily from the C5 nerve root, with occasional contributions from C4, within the posterior cervical triangle.1,2 It courses through the pre-vertebral fascia and traverses the middle scalene muscle, where it provides motor innervation to the levator scapulae and rhomboid muscles. Distally, as it continues along the medial border of the scapula, it passes beneath the levator scapulae muscle and becomes more superficial between the rhomboid major and minor muscles.1,2
DSN entrapment neuropathy represents a frequent cause of unilateral pain in the neck root and interscapular region.3 The clinical presentation of this entrapment includes sharp, stabbing, and burning pain, as well as dysesthetic sensations in the neck, shoulder, arm, and interscapular region.3,4 Other symptoms may include motor weakness during shoulder abduction and scapular winging.4,5 The frequently nonspecific nature of these symptoms can lead to misdiagnosis and ineffective treatment.4 DSN neuropathy can contribute to scapular winging and is associated with the SICK scapula syndrome, a condition characterized by scapular malpositioning, inferior medial border prominence, coracoid pain and malposition, and dyskinesis of scapular movement.5 Furthermore, DSN neuropathy has also been linked to referred pain patterns in the posterolateral arm, forearm, neck, axilla, and lateral thoracic wall.6,7
Despite its clinical significance, DSN neuropathy is often underdiagnosed as a potential cause of mid-scapular and upper-to-mid-back pain.3 Patients may experience pain, stiffness, dysesthesia, and dysfunction in the upper-to-mid-thoracic and costovertebral regions, particularly after traumatic events such as motor vehicle accidents.8–10 Standard medical care, including chiropractic manipulation, physiotherapy, massage therapy, and pharmacological management, often fails to provide more than temporary partial relief for these symptoms.1
The evolution of ultrasound-guided techniques has revolutionized the diagnosis and management of peripheral nerve entrapment syndromes, enabling precise real-time visualization and targeted intervention.11,12 As these advanced techniques become increasingly integral to pain management practice, determining the most effective application for specific neuropathies remains crucial for optimizing patient outcomes.
Fatigue is a common and debilitating complaint among individuals with chronic pain and can exert a significant impact on daily functioning.13,14 Prolonged pain-related fatigue can result in work absenteeism and disability. Emotional exhaustion, a defining feature of burnout, is often associated with this type of fatigue.15
Ultrasound-guided (US) interventions and selective nerve blocks have emerged as valuable tools for diagnosing and treating DSN entrapment neuropathy.2,16 Two primary approaches are utilized depending on the needle access path: the anterior approach (also known as the scalene approach) and the posterior approach (or scapular approach). The anterior approach targets the nerve within the posterior triangle of the neck (Figure 1, Video S1), while the posterior approach involves injecting below the levator scapulae or rhomboid muscles in the back, medial to the scapula (Figure 2, Video S2).11,17,18 The safety of ultrasound-guided hydrodissection of the DSN via the posterior approach below the levator scapulae and rhomboid muscles has been described by Lam et al18
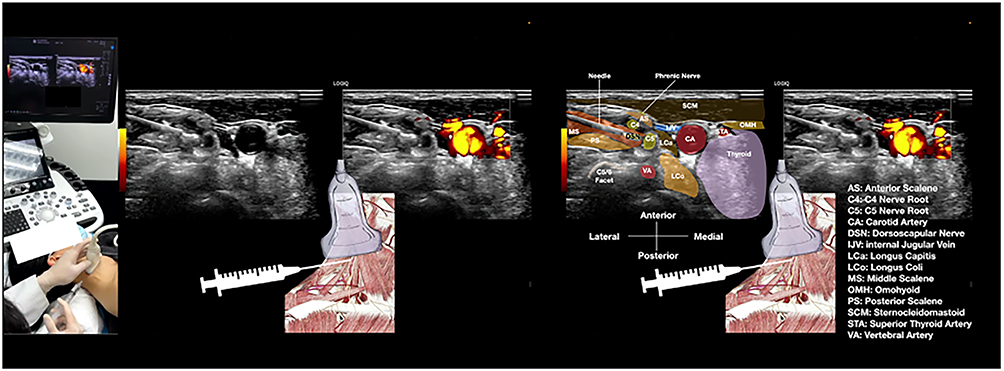 |
Figure 1 Setup for Ultrasound-Guided Dorsal Scapular Nerve Block via the Scalene Approach. This schematic illustrates the patient positioning and technical setup for performing a dorsal scapular nerve (DSN) block within the middle scalene muscle using hydrodissection. Key elements include: patient in supine position with neck slightly hyperextended; high-frequency linear ultrasound probe positioned in the transverse plane; 25-gauge, 2-inch needle inserted in-plane from lateral to medial; target DSN visualized as a hypoechoic structure within the middle scalene muscle; and hydrodissection performed with triamcinolone acetonide 40 mg + 2 mL lidocaine (2%) diluted to 10 mL with saline (see Video S1). This dynamic ultrasound video demonstrates the in-plane hydrodissection technique for the dorsal scapular nerve (DSN) within the middle scalene muscle. The video shows: (1) initial identification of the DSN as a hypoechoic oval structure within the middle scalene muscle; (2) needle advancement in-plane from lateral to medial under continuous ultrasound guidance; (3) real-time hydrodissection as the injectate (triamcinolone acetonide 40 mg + 2 mL lidocaine 2% in 10 mL saline) creates circumferential separation of the nerve from surrounding tissues; and (4) confirmation of adequate spread around the nerve. The procedure was performed with the patient in supine position using a high-frequency linear transducer. |
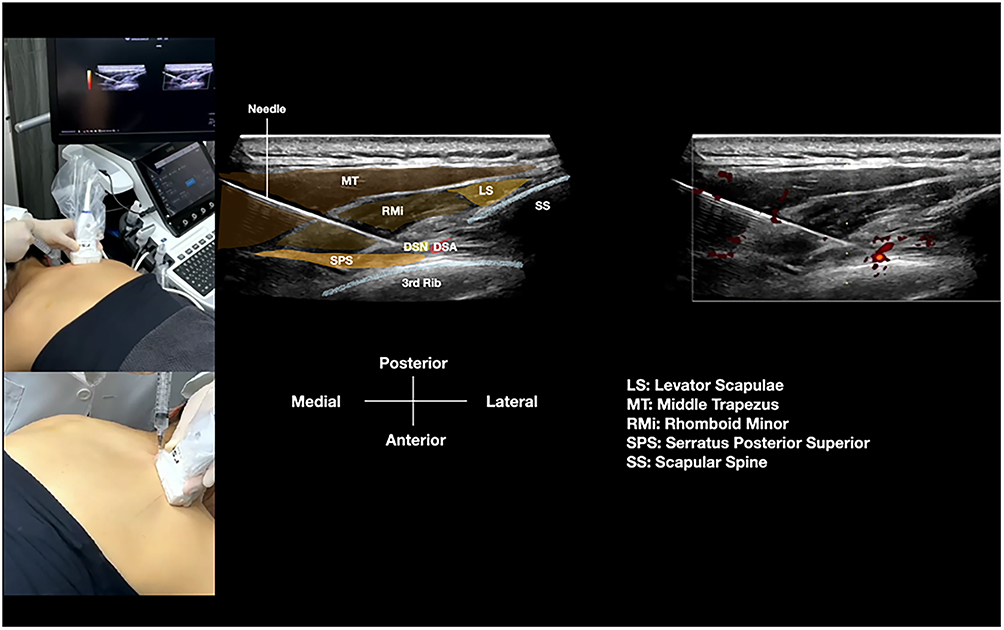 |
Figure 2 Setup for Ultrasound-Guided Dorsal Scapular Nerve Block via the Scapular Approach. This schematic illustrates the patient positioning and technical setup for performing a dorsal scapular nerve (DSN) block in the interscapular region using hydrodissection. Key elements include: patient in prone position with arms and scapulae protracted to open interscapular spaces; high-frequency linear ultrasound probe positioned medial to the scapular border; 25-gauge, 2-inch or 22-gauge, 2 3/4-inch needle inserted in-plane from medial to lateral; target DSN visualized as a hypoechoic oval structure deep to the levator scapulae and rhomboid minor muscles, superficial to the serratus posterior superior muscle, and medial to the dorsal scapular artery; and hydrodissection performed with triamcinolone acetonide 40 mg + 2 mL lidocaine (2%) diluted to 10 mL with saline (see Video S2). This dynamic ultrasound video demonstrates the in-plane hydrodissection technique for the dorsal scapular nerve (DSN) in the interscapular region. The video shows: (1) identification of key anatomical landmarks including the levator scapulae, rhomboid minor, and serratus posterior superior muscles, and the dorsal scapular artery; (2) visualization of the DSN as a hypoechoic structure medial to the artery; (3) needle advancement in-plane from medial to lateral under continuous ultrasound guidance; (4) real-time hydrodissection as the injectate (triamcinolone acetonide 40 mg + 2 mL lidocaine 2% in 10 mL saline) separates the nerve from surrounding fascial planes; and (5) confirmation of adequate fluid spread around the nerve. The procedure was performed with the patient in prone position using appropriate transducer selection based on body habitus. |
This anatomical and technical background, however, presents a clear clinical dilemma for the practitioner. While the DSN can be entrapped at multiple sites along its course, the most proximal entrapment at the middle scalene muscle is considered the most common.3,19,20 In contrast, the distal scapular approach is often perceived as safer and anatomically simpler due to its location away from critical neurovascular structures in the neck.11,18 This creates an unresolved question in clinical practice: should the intervention target the suspected primary site of pathology (proximal) or the technically more accessible and perceived safer site (distal)? However, current evidence is limited to technical reports and case series. To the best of our knowledge, no randomized controlled trial has yet directly compared the clinical efficacy of these two common anatomical approaches, leaving this choice to operator preference rather than evidence.
Therefore, the primary aim of this study was to compare the short-term efficacy of the scalene versus scapular approach for DSN corticosteroid hydrodissection, with the primary outcome being pain reduction at rest. Secondary aims were to compare effects on movement-related pain, fatigue, patient satisfaction, electrodiagnostic parameters, and safety.
Materials and Methods
This was a multicentric, prospective, randomized controlled study conducted across seven different centers in Egypt: three in Cairo (one Al-Azhar, Cairo branch and two private hospitals) that mainly receive patients from an urban setting, two Delta university hospitals (Al-Azhar Domiatta branch and Tanta University Hospital), and two university hospitals in upper Egypt (Al-Azhar, Assuit branch and Assuit University Hospital) that receive patients from urban, semirural, and rural settings. Patients and outcome assessors were blinded to group assignment; the proceduralists could not be blinded due to the inherent technical differences between the two approaches. This study was approved by the Medical Research Ethics Committee of Assiut University’s Faculty of Medicine in Assiut, Egypt (approval no: 17300649). It was registered at ClinicalTrials.gov (NCT04693312) and adhered to the tenets of the Helsinki Declaration. The study was conducted from January 2020 to July 2020.
Patients
A total of 60 patients aged 20–60 years with scapular pain clinically and electrodiagnostically confirmed as DSN entrapment (via nerve conduction study and electromyography) were included. All enrolled patients had chronic pain for at least three months, a pain intensity of >50 on a 100-point Visual Analog Scale (VAS) (where 0 indicated no pain and 100 indicated the worst pain possible), and had not responded to previous medical treatment. All adult patients scheduled for elective interventional procedures for scapular pain management for DSN entrapment syndrome under local anesthesia provided written informed consent.
Exclusion criteria included patients with overlapping syndromes (especially those of lower cervical radiculopathy and double-crush syndromes), history of trauma, surgery, or structural pathology in the target location, coagulopathy, neuromuscular disorders, cervical radiculopathy, allergy to local anesthetics, ankylosing spondylitis, morbid obesity (body mass index >40), spinal metastatic tumor, opioid addiction, preexisting mental illness, psychological problems, administration of sedatives, infection at the injection site, or refusal to participate. Cases demonstrating significant needle-entry sensitivity were also excluded.
Randomization and Blinding
Randomization was performed using serially numbered, opaque, sealed envelopes. Upon enrollment, each patient was assigned a sequential number from a computer-generated randomization table and allocated to the corresponding group. Participants received appropriate counselling prior to recruitment.
In Group I (the scalene group, n=30), the anterolateral approach was used, traversing through the posterior triangle of the neck to access the middle scalene muscle, using the hydrodissection technique.21,22 The DSN block was performed by hydrodissecting the nerve inside the middle scalene muscle, using an in-plane technique from lateral to medial with an injectate composed of triamcinolone acetonide 40 mg + 2 mL lidocaine (2%) diluted to 10 mL with saline (Figure 1, Video S1).
In Group II (the scapular group, n=30), the posterior approach through the interscapular region was used. The DSN block was performed using the hydrodissecting technique, from medial to lateral, with the needle tip positioned below the levator scapulae and rhomboid minor, and superficial to the serratus posterior superior muscle, at the level of the second or third rib,18 using the same injectate composition and volume as Group I (Figure 2, Video S2).
The patients, the electrodiagnostic physician, and the outcome-assessing physicians were blinded to the group assignment. To maintain patient blinding despite different positions (supine vs prone), all patients were informed that the study compared two standard, validated ultrasound-guided injection techniques for their condition, and that the patient position was a technical requirement of the specific approach being used. They were not informed which position corresponded to which anatomical target (scalene vs scapular). The procedural screen was positioned so patients could not view the injection site or ultrasound monitor. The physicians performing the injections could not be blinded due to the different patient positions (supine for Group I vs prone for Group II) and distinct sonographic approaches required for each technique.
Intervention Protocol
An intravenous cannula was placed before the procedure, and patients were monitored using continuous pulse oximetry, non-invasive blood pressure measurement, and electrocardiography. Patients were placed in the supine position for the scalene group and the prone position for the scapular group. Local anesthesia was administered at the injection site immediately before the procedure.
A standardized injectate volume of 10 mL was used for hydrodissection in both groups. This volume was selected a priori based on previous technical reports for peripheral nerve hydrodissection, which indicate that a volume of this magnitude is typically required to achieve adequate circumferential spread around the nerve and ensure complete separation from constricting fascial structures.21,22
It is important to note that as both groups received identical steroid-containing injectates, this study compares the efficacy of administering the combined mechanical and pharmacologic intervention at two different anatomical sites, rather than isolating the effect of hydrodissection alone.
Standardization Protocol
All ultrasound-guided procedures were performed by experienced pain physicians or musculoskeletal specialists at the participating centers. To ensure procedural consistency and minimize inter-operator variability, all operators followed a detailed, standardized protocol as described in this manuscript and demonstrated in Videos S1, S2, S3, and S4. This included standardized patient positioning, transducer placement, sonographic landmarks for nerve identification, needle approach, and injection endpoint.
Technique in Group I – Middle Scalene Group
An anterolateral approach was employed, traversing through the posterior triangle of the neck to target the Dorsal Scapular Nerve (DSN) within the middle scalene muscle using the hydrodissection technique. The long axis of a linear high-frequency ultrasound transducer was positioned in the transverse plane of the neck. The brachial plexus was identified between the anterior and middle scalene muscles at the interscalene level. A cranial short-axis slide of the transducer was used to locate the DSN within the middle scalene muscle. The DSN was recognized as a monofascicular anechoic fascicle with a hyperechoic boundary, which originates immediately as the C5 nerve root emerged between the less prominent but equally-sized anterior and posterior tubercles (refer to Figure 3, Video S3). Further confirmation of the C5 nerve root was achieved through axial movement of the US transducer. The C6 nerve root, located caudal to C5, emerged between the most prominent anterior and posterior tubercles of the cervical spine. In contrast, the C7 nerve root typically exhibited only a prominent posterior tubercle with a rudimentary anterior tubercle. After confirming the nerve, the injection was administered using an in-plane hydrodissecting technique (Figure 1, Video S1).
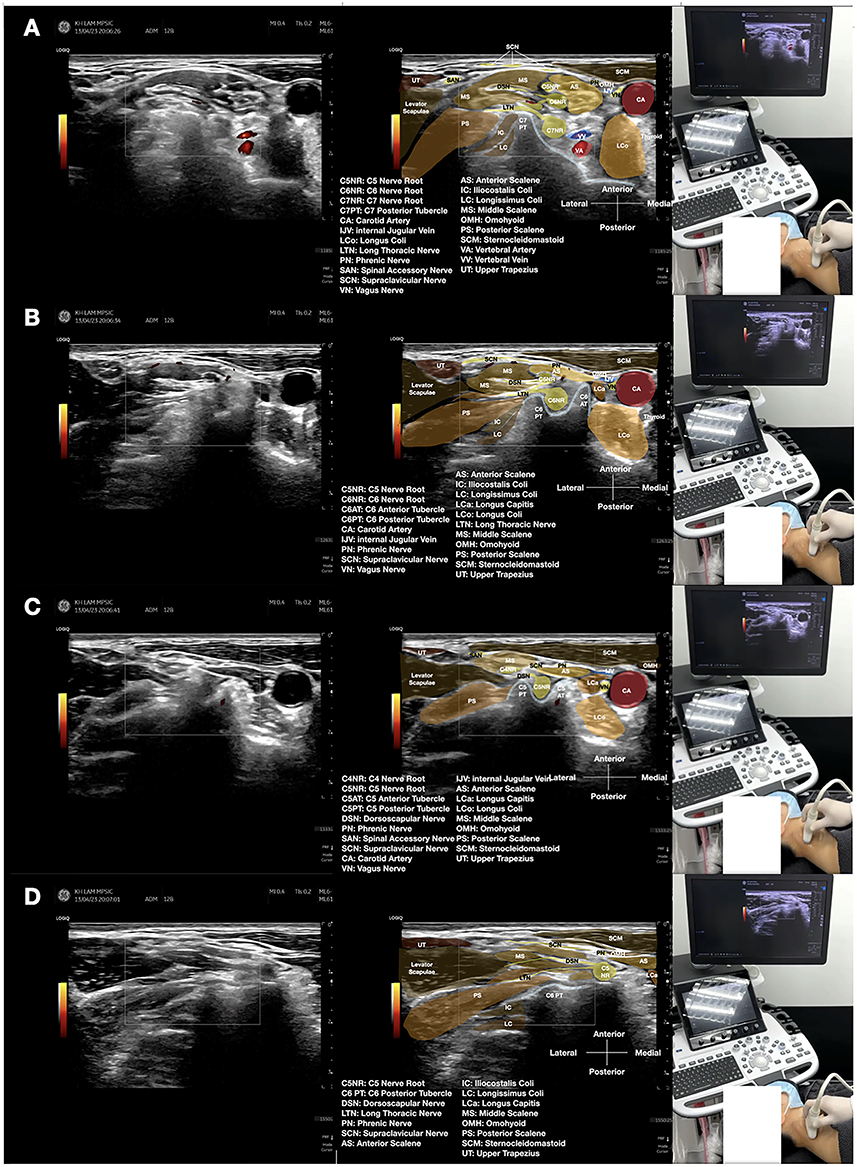 |
Figure 3 Sonoanatomy of the Dorsal Scapular Nerve in the Middle Scalene Muscle. Ultrasound images demonstrating the anatomical relationships for dorsal scapular nerve (DSN) identification at the scalene level. (A) C7 nerve root level showing characteristic anatomy with prominent posterior tubercle. (B) C6 nerve root level emerging between prominent anterior and posterior tubercles. (C) C5 nerve root level, the origin of the DSN. (D) The DSN visualized within the middle scalene muscle as a hypoechoic oval structure (short axis) or fascicular structure (long axis). Key anatomical features include: middle scalene muscle appearing as a hypoechoic, striated structure; cervical nerve roots as hypoechoic round structures emerging from intervertebral foramina; and the DSN coursing through the middle scalene muscle (see Video S3). This dynamic ultrasound video demonstrates the systematic approach to identifying the dorsal scapular nerve (DSN) within the middle scalene muscle. The video shows: (1) cranial-to-caudal scanning technique to identify cervical nerve roots C7, C6, and C5; (2) recognition of characteristic bony landmarks (cervical tubercles) at each level; (3) identification of the C5 nerve root as the origin of the DSN; (4) tracking the DSN within the middle scalene muscle; and (5) differentiation of the DSN from surrounding structures in both short-axis and long-axis views. The scanning was performed with a high-frequency linear transducer in the transverse plane. |
Technique in Group II – Scapular Group
For patients in Group II, the posterior approach through the interscapular region was utilized. In the transverse plane of the trunk, the transducer was positioned medial to the superomedial border of the scapula. Typically, a high-frequency linear transducer was used, although a curvilinear transducer was employed for patients with obesity. The levator scapulae muscle was observed attached to the most superior and medial scapular border. More distally, at a similar fascial plane, the rhomboid minor was identified attached to the medial border of the scapula at the level of the scapular spine, while the rhomboid major was attached to the medial border below the scapular spine. Under power Doppler mode, the dorsal scapular artery (DSA) was visualized deep to the levator scapulae and rhomboid muscles, but superficial and lateral to the serratus posterior superior (SPS) muscle. The dorsal scapular nerve (DSN) was identified as a hypoechoic oval structure medial to the DSA (Figure 4, Video S4). When the transducer was repositioned in the sagittal plane, the long axis of the DSN was visualized as a linear hypoechoic structure running above the ribs and intercostal muscles, usually just lateral to the insertions of the SPS muscle but medial to the DSA. Once the nerve was confirmed, the injection was administered using an in-plane technique and a medial-to-lateral approach, targeting the separation of the DSN from the fascia of the SPS and the fascia at the bottom of the levator scapulae or rhomboid minor (Figure 2, Video S2).18
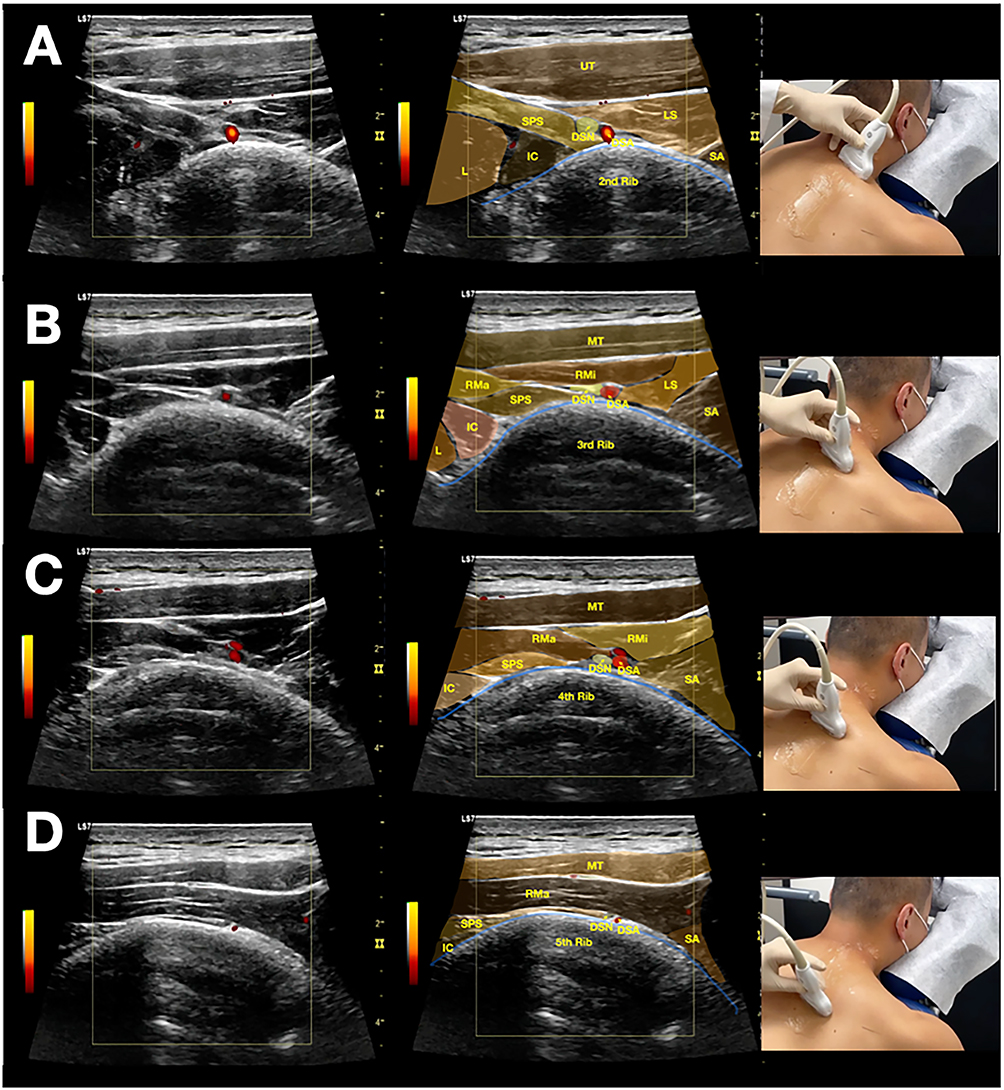 |
Figure 4 Sonoanatomy of the Dorsal Scapular Nerve in the Scapular Region. Ultrasound images demonstrating the anatomical relationships for dorsal scapular nerve (DSN) identification in the interscapular region from the 2nd to 5th rib levels. (A) DSN at the level of the 2nd rib. (B) DSN at the level of the 3rd rib. (C) DSN at the level of the 4th rib. (D) DSN at the level of the 5th rib. Key anatomical features include: the DSN visualized as a hypoechoic oval structure located deep to the levator scapulae and rhomboid minor muscles, superficial to the serratus posterior superior muscle, and medial to the dorsal scapular artery; superficial muscles appearing as hypoechoic triangular structures; serratus posterior superior as a fan-shaped deep muscle; and ribs as hyperechoic linear structures with acoustic shadowing (see Video S4). This dynamic ultrasound video demonstrates the systematic approach to identifying the dorsal scapular nerve (DSN) along its course in the interscapular region. The video shows: (1) medial-to-lateral scanning technique from the 2nd to 5th rib levels; (2) identification of superficial muscles (levator scapulae and rhomboid minor) and deep muscles (serratus posterior superior); (3) use of the dorsal scapular artery as a key vascular landmark; (4) recognition of the DSN as a hypoechoic structure medial to the artery within the intermuscular plane; and (5) dynamic tracking of the nerve across multiple rib levels. The scanning was performed with a high-frequency linear transducer in the transverse plane. Abbreviations: DSA, dorsal scapular artery; DSN, dorsal scapular nerve; IC, iliocostalis thoracis; L, longissimus thoracis; LS, levator scapulae; MT, middle trapezius; RMa, rhomboid major; RMi, rhomboid minor; SA, serratus anterior; SPS, serratus posterior superior; UT, upper trapezius. |
Post-Procedure Monitoring
Patients in both groups were observed for 1 hour after the intervention and discharged after fulfilling the standard discharge criteria.
Assessment Parameters
Demographic and Anthropometric Data
Baseline data, including patient age and sex, were collected.
Pain Assessment
Pain intensity was assessed using the Visual Analog Scale (VAS).23–25 Patients were instructed to rate their worst localized interscapular pain on a scale from 0 to 100, where 0 indicated no pain and 100 indicated the most severe disabling pain imaginable. Assessments were performed for two conditions: pain at rest and pain during active shoulder movement. VAS scores were recorded pre-injection and at one and three months post-injection.
Fatigue Assessments
Fatigue was assessed using the Fatigue Assessment Scale (FAS), a unidimensional 10-item scale.26 The 5-point rating system ranges from 1 (never) to 5 (always), with higher scores indicating greater fatigue. The total score ranges from 10 to 50. Fatigue was assessed pre-injection and at one and three months post-injection.
Electrodiagnosis
To quantify a key objective physiological parameter, motor distal latency of the dorsal scapular nerve was selected as an outcome measure. This standard electrodiagnostic parameter was included to provide an objective correlate to the subjective clinical improvements, despite its recognized limited sensitivity to clinical change in entrapment neuropathies. All nerve conduction studies were performed by an experienced electrophysiologist using a calibrated electromyograph. Studies were conducted at a controlled room temperature (22–24 °C), with skin temperature maintained above 32°C to ensure accuracy. Motor distal latency was recorded before the injection and three months after the intervention.
Patient Satisfaction Score
Patient satisfaction was recorded during the first week, first month, and third month using a 5-point Likert scale:27 1, strongly unsatisfied; 2, moderately unsatisfied; 3, neutral; 4, moderately satisfied; 5, strongly satisfied.
Complications
Complications, such as local infection, allergic reaction, muscular spasm, increased pain, or skin discoloration, were monitored and reported. The use of sedatives and any related complications were also to be recorded.
Before the trial began, a successful outcome was defined as a 50% reduction in the VAS score.
Outcome
The primary outcome measure was pain severity assessed using the VAS for localized interscapular pain at rest. Key secondary outcome measures were the VAS for pain during shoulder movement, the Fatigue Assessment Scale (FAS) score, motor distal latency, patient satisfaction scores, and the incidence of complications.
A successful outcome was defined a priori as a 50% reduction in the VAS score from baseline.
Sample Size
The sample size was calculated using the G-Power calculator (version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany).28 An a priori analysis for a t-test (difference between two independent means) indicated that a total sample size of 52 patients (26 in each group) would be sufficient, assuming a one-tailed type I error of 0.05, a power of 0.8, and an effect size of 0.7. This effect size (large) was chosen based on preliminary, non-published observations from our clinical practice and previous non-comparative studies suggesting substantial pain relief from DSN interventions.29,30 To account for potential dropouts, four additional participants were enrolled in each group, resulting in a final sample of 60 patients (30 per group).
Statistical Analysis
The statistical analysis followed a pre-specified plan that accounted for data distribution characteristics. The normality of all continuous variables was formally assessed using the Shapiro–Wilk test. Based on these results, which indicated non-normal distributions for VAS, FAS, and satisfaction scores, the Mann–Whitney U-test was selected for between-group comparisons of these outcomes; data are presented as median [interquartile range]. For significant Mann–Whitney U-test results, the location difference—a non-parametric measure of effect size—is reported. For normally distributed motor latency data, independent samples t-tests were employed, with results expressed as mean ± standard deviation. This analytical approach aligns with contemporary methodological recommendations for analyzing patient-reported outcomes, which often demonstrate non-parametric distributions.31 Categorical variables were analyzed using chi-square or Fisher’s exact tests, as appropriate. All analyses were conducted using R software (version 4.2.0; R Foundation for Statistical Computing, Vienna, Austria), with a two-sided alpha level of 0.05 defining statistical significance.
Results
Patient Recruitment and Demographics
Seventy-one patients were assessed for eligibility. Four did not meet inclusion criteria and two declined participation. Sixty-five patients were enrolled, with five lost to follow-up, resulting in 60 patients (30 per group) included in the final analysis (Figure 5).The groups were well-matched at baseline with no significant differences in demographic or clinical characteristics (all p > 0.05), indicating successful randomization (Table 1).
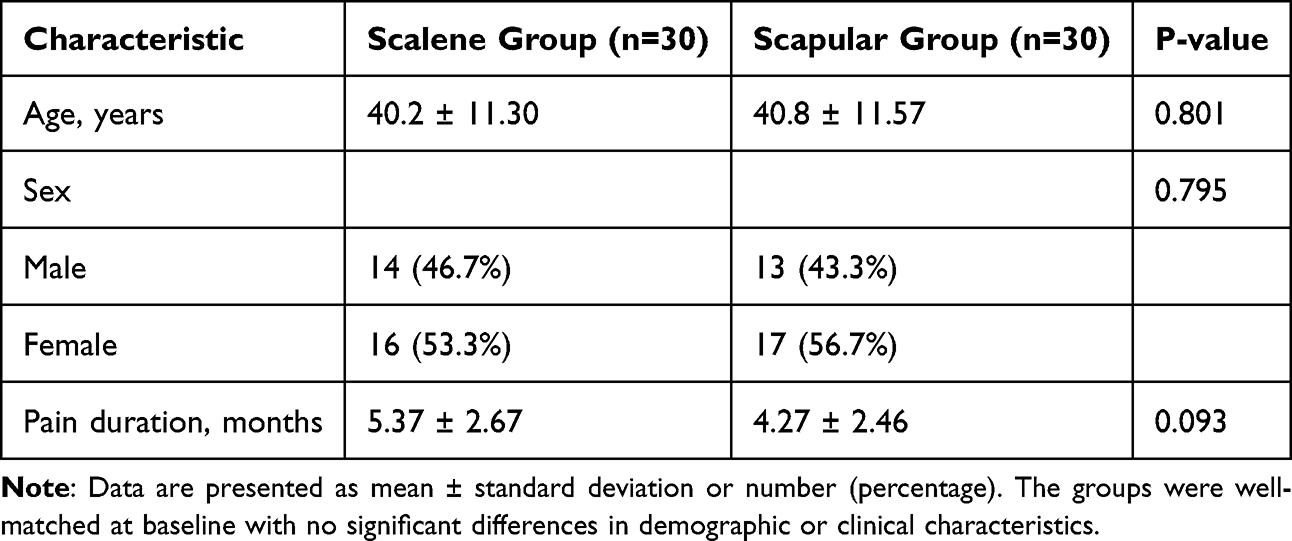 |
Table 1 Demographic and Clinical Characteristics at Baseline |
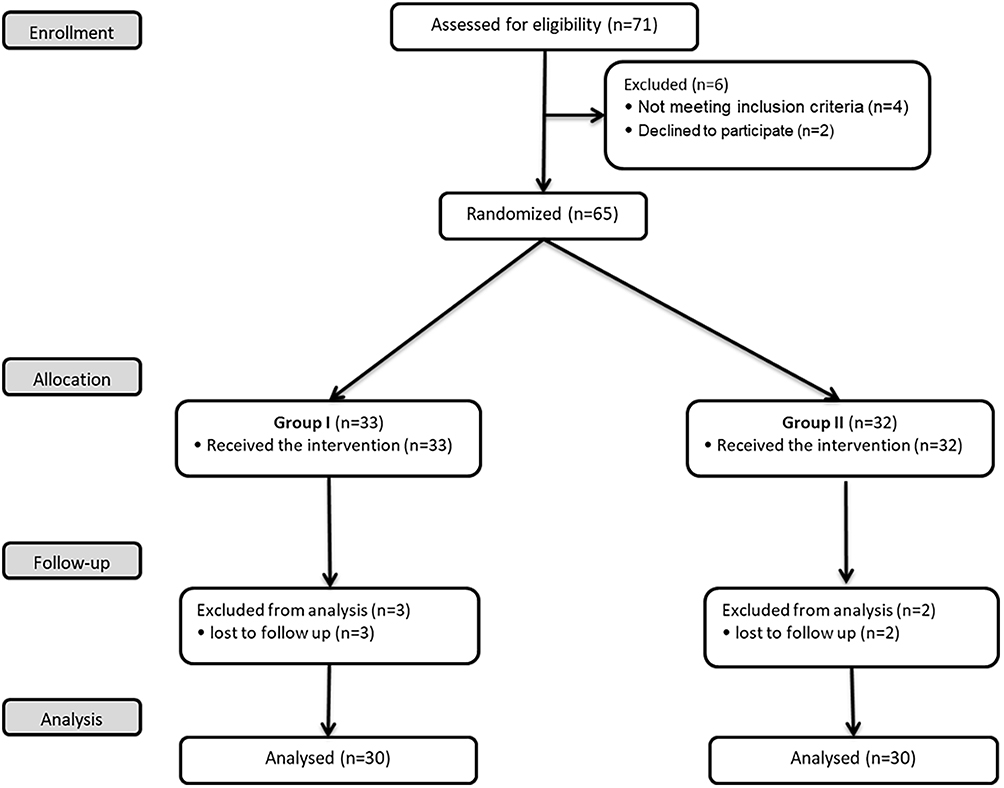 |
Figure 5 Participant Flow Diagram. This flowchart illustrates the progression of participants through all stages of the randomized controlled trial, according to the CONSORT guidelines. It details the number of patients assessed for eligibility, randomly assigned to each intervention group (Scalene Group and Scapular Group), received the intended treatment, lost to follow-up, and included in the primary analysis. |
Primary Outcome: Pain at Rest
No significant between-group difference existed at baseline (Z = −0.48, p = 0.633). Post-intervention, the scalene group showed greater improvement compared to the scapular group. At 1-month post-injection, the difference was highly significant (Z = 6.68, p < 0.001, location difference = 45). This greater improvement was maintained at 3-month follow-up (Z = 6.68, p < 0.001, location difference = 57) (Figure 6).
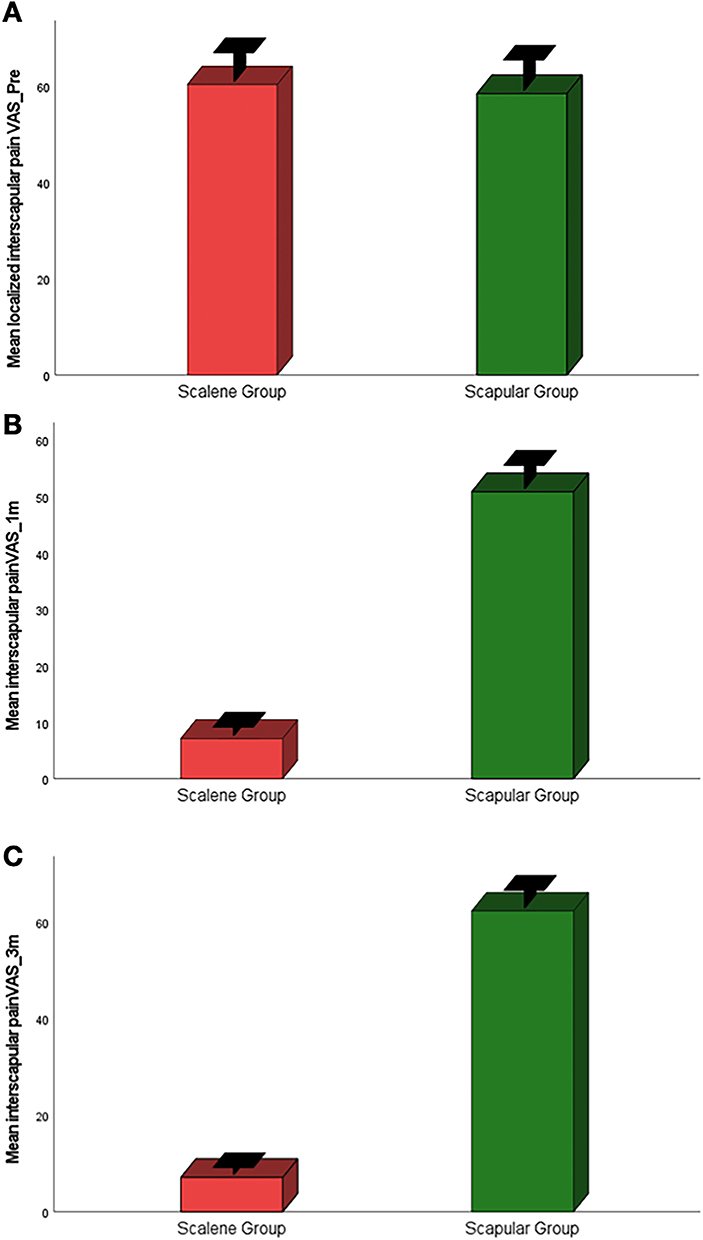 |
Figure 6 Visual Analog Scale (VAS) Scores for Pain at Rest Over Time. Bar graphs display the mean Visual Analog Scale (VAS) scores for localized interscapular pain at rest for the Scalene Group (n=30) and the Scapular Group (n=30) at three time points: (A) pre-injection (baseline), (B) 1 month post-injection, and (C) 3 months post-injection. The Scalene Group demonstrates a profound and consistent reduction in pain scores compared to the Scapular Group at both follow-up intervals. Statistical significance between groups was determined by the Wilcoxon-Mann–Whitney test (p < 0.001). |
Pain with Shoulder Movement (VAS)
Significant differences favoring the scalene group emerged at 1-month (Z = 6.68, p < 0.001) and persisted at 3-months (Z = 6.69, p < 0.001) (Figure 7).
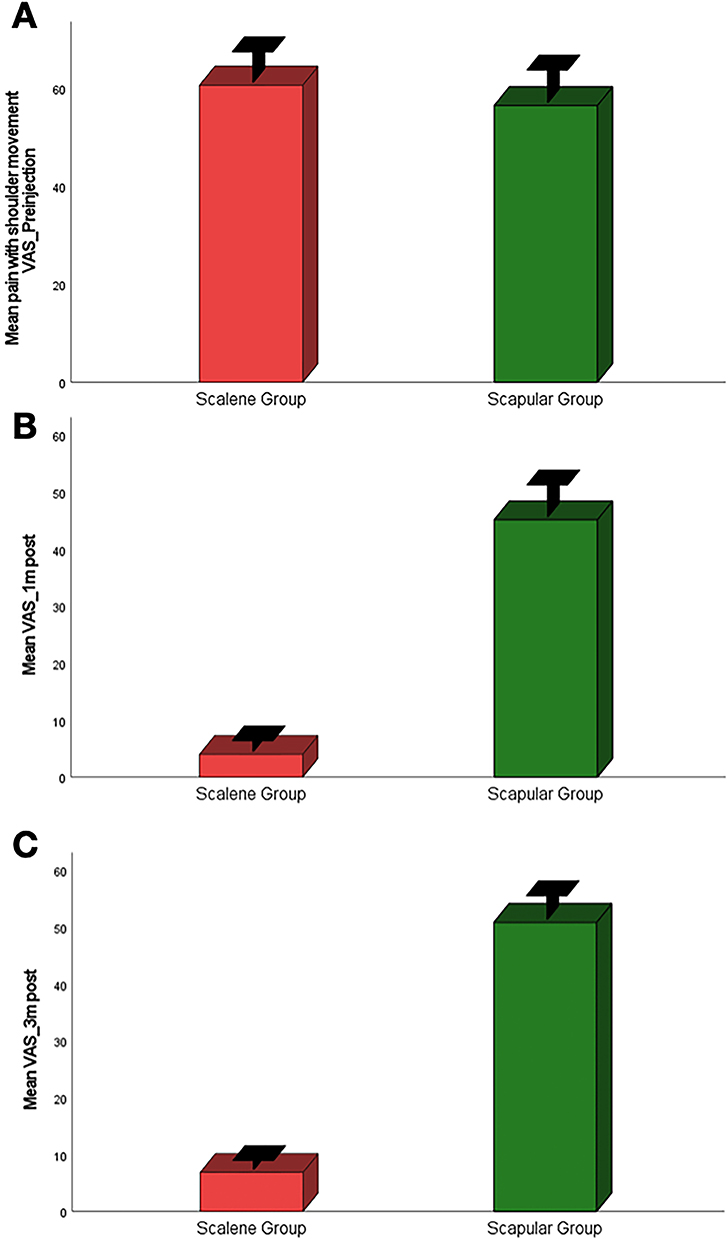 |
Figure 7 Visual Analog Scale (VAS) Scores for Pain During Shoulder Movement Over Time. Bar graphs display the mean Visual Analog Scale (VAS) scores for pain during active shoulder movement for the Scalene Group (n=30) and the Scapular Group (n=30) at three time points: (A) pre-injection (baseline), (B) 1 month post-injection, and (C) 3 months post-injection. The Scalene Group demonstrates a pronounced and sustained reduction in movement-related pain compared to the Scapular Group. Statistical significance between groups at each time point was determined by the Wilcoxon-Mann–Whitney test (p < 0.001). |
Secondary Outcomes
Fatigue Assessment Scale (FAS)
The two groups had comparable fatigue levels at baseline (Z = −1.09, p = 0.280). A statistically significant difference favoring the scalene group emerged at one-month post-injection (Z = 3.76, p < 0.001, location difference = 10), which further increased and became more pronounced at three months (Z = 5.93, p < 0.001, location difference = 20), indicating greater reduction in fatigue in the scalene group (Figure 8).
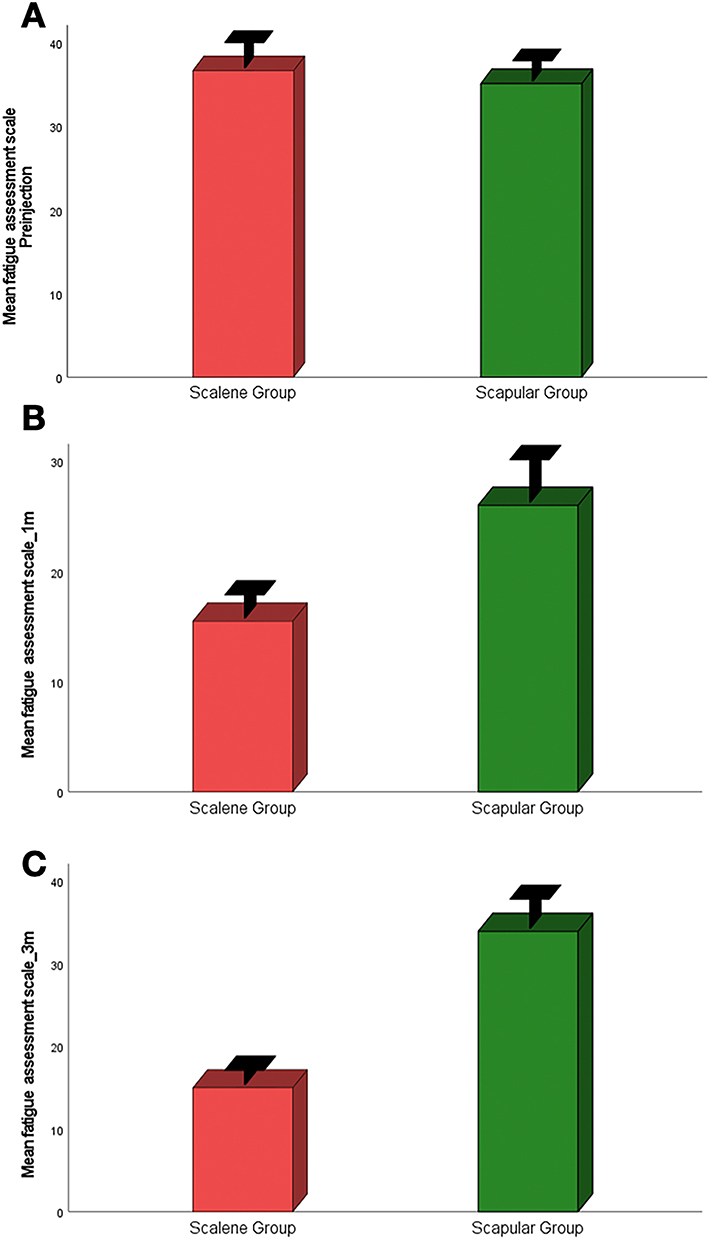 |
Figure 8 Fatigue Assessment Scale (FAS) Scores Over Time. Bar graphs display the mean Fatigue Assessment Scale (FAS) scores for the Scalene Group (n=30) and the Scapular Group (n=30) at three time points: (A) pre-injection (baseline), (B) 1 month post-injection, and (C) 3 months post-injection. The Scalene Group demonstrates substantially greater improvement in fatigue scores compared to the Scapular Group throughout the study period. Statistical significance between groups at each time point was determined by the Wilcoxon-Mann–Whitney test (p < 0.001). |
Motor Distal Latency
No significant between-group differences were found in motor distal latency at baseline (t = −0.075, p = 0.941) or at three months post-injection (Z = 1.47, p = 0.145). Furthermore, there were no significant within-group changes from baseline to three months in either group (Figure 9).
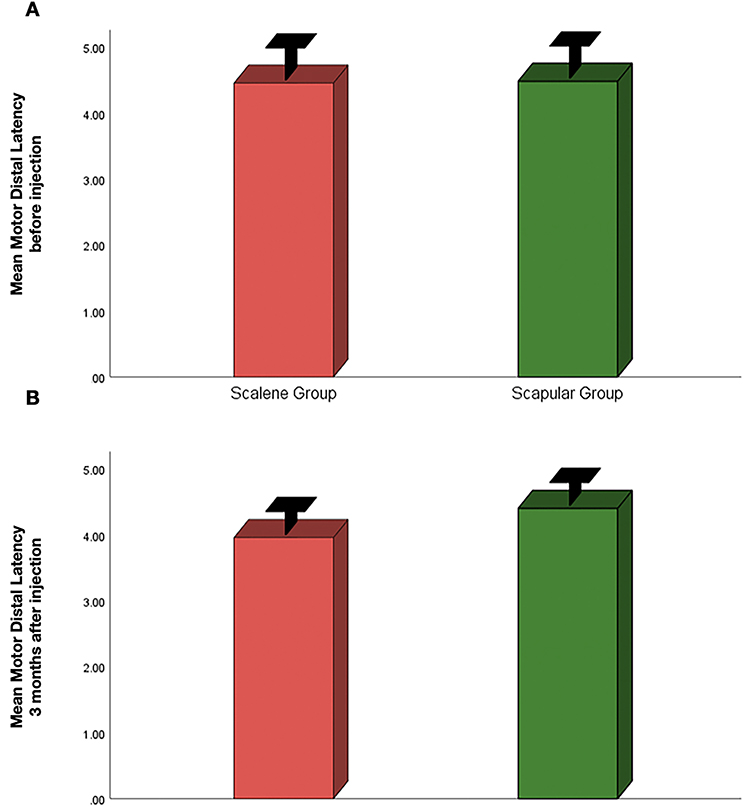 |
Figure 9 Motor Distal Latency Measurements Over Time. Bar graphs display the mean motor distal latency (ms) for the Scalene Group (n=30) and the Scapular Group (n=30) at two time points: (A) pre-injection (baseline) and (B) 3 months post-injection. No significant between-group differences were observed at either time point (baseline: p=0.941; 3 months: p=0.145). Statistical significance was determined by independent samples t-test at baseline and Mann–Whitney U-test at 3 months. |
Patient Satisfaction
Satisfaction scores were significantly higher in the scalene group at all assessed time points. The difference was most notable at one week (Z = −6.28, p < 0.001) and remained highly significant at one month (Z = −3.64, p < 0.001) and three months (Z = −5.96, p < 0.001) (Table 2).
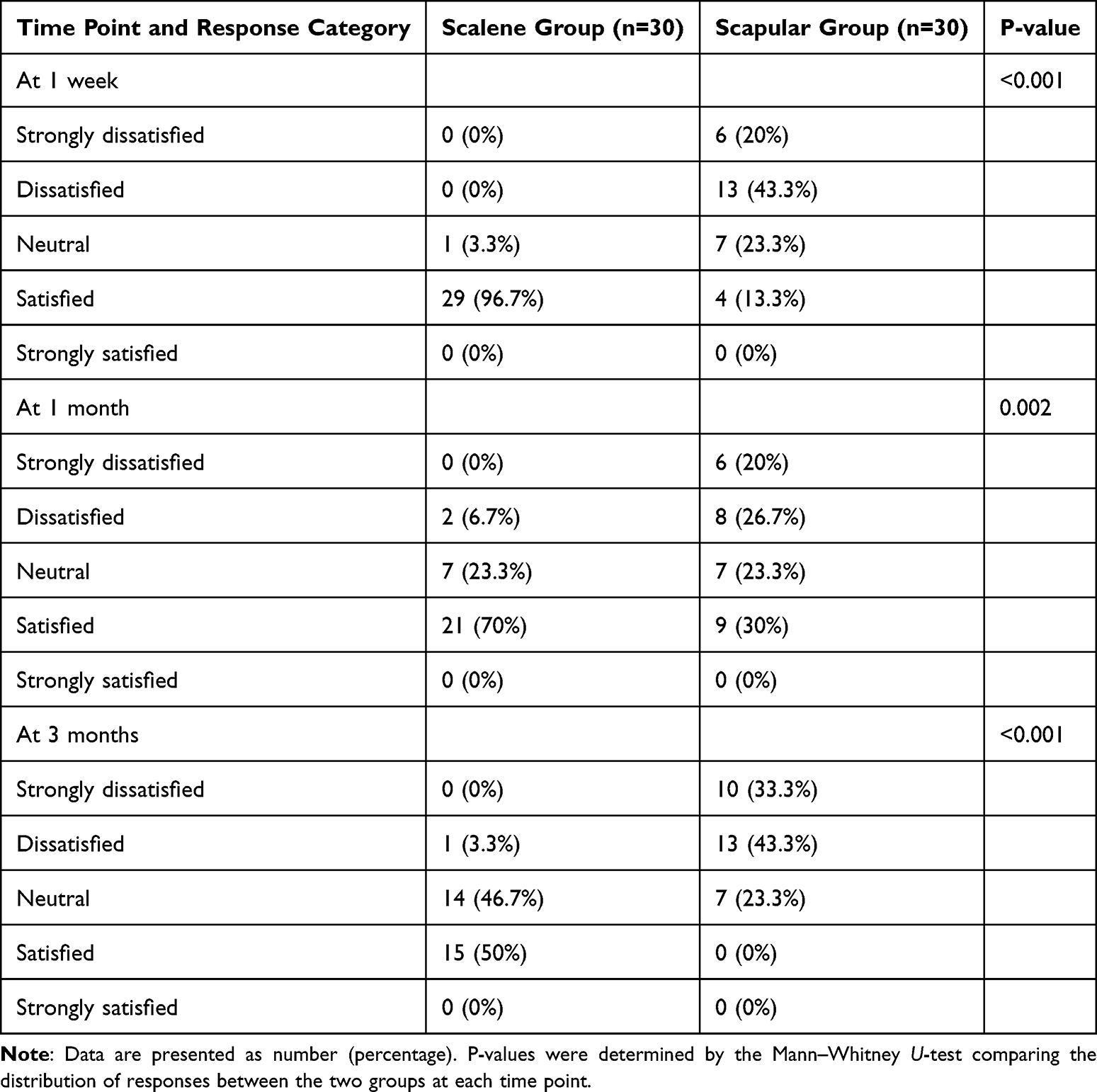 |
Table 2 Patient Satisfaction Scores at Different Time Points |
The consistency of these results across multiple domains—pain at rest, pain with movement, fatigue, and patient satisfaction—demonstrates a consistent pattern of greater improvement with the scalene approach. The large effect sizes (location differences of 45–57 points for pain, 20 points for fatigue) and extremely low p-values (p < 2.2e-16) provide evidence that the scalene approach resulted in better outcomes than the scapular approach over the three-month study period.
The scalene group demonstrated significantly greater improvement than the scapular group across all patient-reported outcomes at the 1- and 3-month follow-ups (all p < 0.001), with no significant difference in motor distal latency (p = 0.145). The complete results for all outcomes are presented in Table 3.
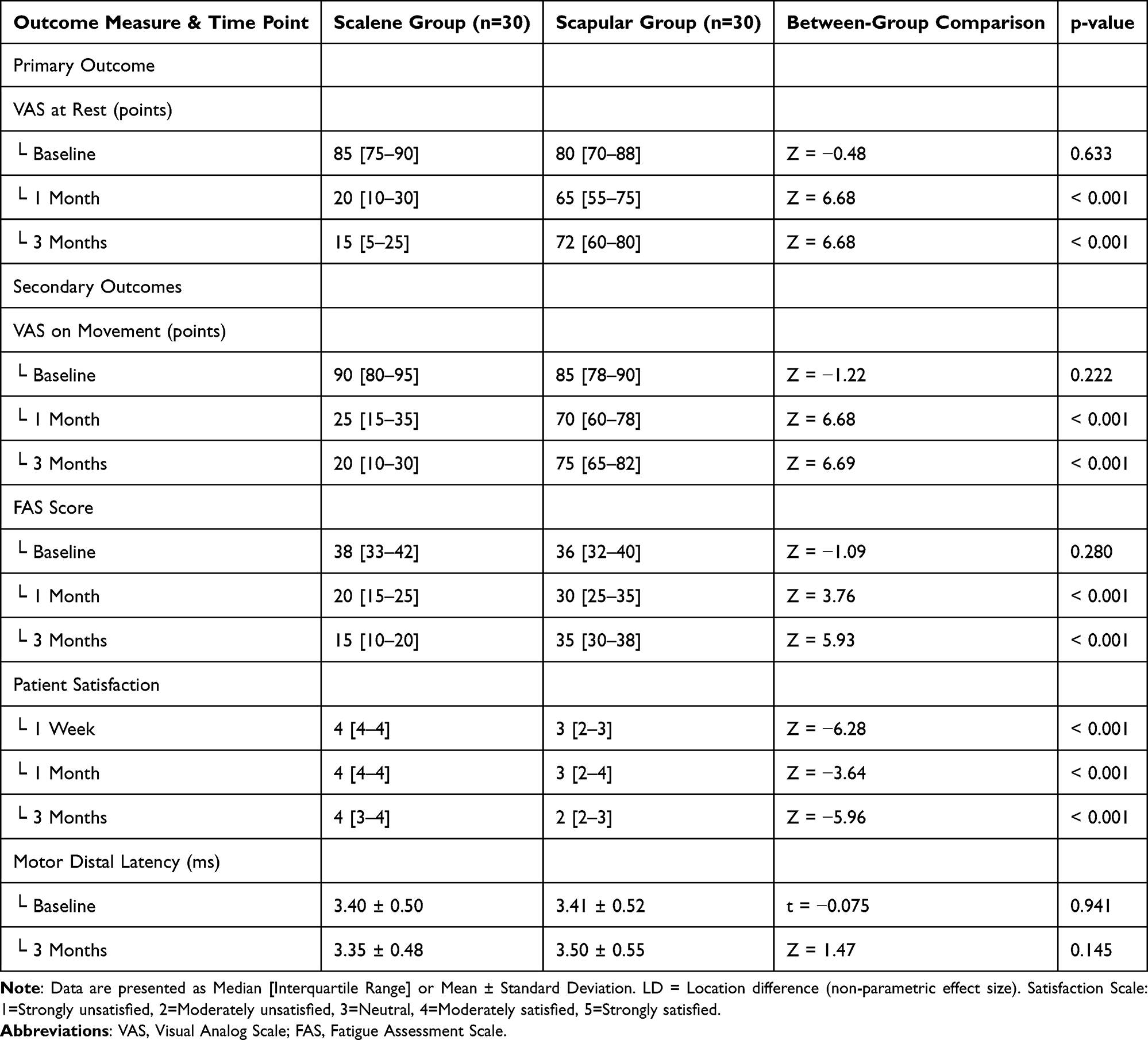 |
Table 3 Summary of Primary and Secondary Outcomes |
Side Effects
No major complications, such as infection, significant hemorrhage, or allergic reactions, were reported in either group during the follow-up period. Specifically, in the scalene group, there were no clinical signs or patient reports suggestive of transient brachial plexus blockade (eg, limb weakness or sensory changes) or phrenic nerve involvement (eg, shortness of breath).
Discussion
The current study employed a comprehensive outcome assessment to evaluate the efficacy of corticosteroid hydrodissection injections at two distinct anatomical levels in patients with DSN entrapment syndrome. Our findings offer comparative evidence to address the clinical dilemma of injection site selection, suggesting that the proximal scalene approach resulted in better outcomes than the distal scapular approach over the three-month study period. Specifically, the combined corticosteroid hydrodissection intervention at the level of the middle scalene muscle was associated with greater pain alleviation and functional improvement. Furthermore, for up to three months following the intervention, Group I (scalene approach) demonstrated greater improvements in fatigue and satisfaction scale scores relative to Group II (scapular approach), with no major complications reported in either group.
The assessment of motor distal latency, when compared to clinical parameters, appears to be less sensitive for evaluating symptomatic improvement following entrapment neuropathy, particularly for the DSN, after local injection at three months. This dissociation between objective electrodiagnostic measures and subjective clinical improvement could be explained by the fact that symptomatic improvement in entrapment neuropathies often precedes electrophysiological recovery. The therapeutic effect in both groups likely resulted from a combination of corticosteroid-mediated anti-inflammatory action and mechanical hydrodissection.21,22 It is important to note that Group II participants demonstrated considerable improvement; however, they consistently exhibited higher VAS scores than Group I participants throughout the study period.
The observed differences between approaches can be considered in the context of anatomical and pathophysiological reasoning. The most common site of DSN entrapment is at the middle scalene muscle, where the nerve pierces the fascia.3,19,20 It should be noted that our study design does not allow separation of the mechanical hydrodissection effect from the pharmacological effect of the corticosteroid, as both groups received an identical injectate. Therefore, the observed effects are attributable to the combined corticosteroid and hydrodissection intervention delivered at two different anatomical sites. The rationale for comparing the two sites stems from the hypothesis that delivering the combined intervention at the suspected primary site of pathology may be more likely to address the fundamental cause of the neuropathy than administration further downstream. The substantial treatment effects observed (location differences of 45–57 points for pain) are consistent with this anatomical hypothesis and suggest that targeting the scalene region may be advantageous. Therefore, the sustained benefit at three months should be interpreted as the result of the combined intervention delivered at a more effective anatomical site, not attributed solely to one component.
The use of the pre-specified 10 mL volume for hydrodissection was aimed at ensuring adequate circumferential nerve separation, consistent with technical principles for this procedure.21,22
A particularly noteworthy finding was the significant and progressively increasing improvement in fatigue scores in the scalene group. The location difference in FAS scores increased from 10 at one month to 20 at three months, indicating a sustained therapeutic effect over time. Chronic pain is well-established to contribute to a cycle of pain-related fatigue, sleep disturbance, and functional decline.15 We hypothesize that by providing more effective and durable relief from the primary nociceptive input, the scalene approach may help to disrupt this debilitating cycle. The resultant improvement in sleep quality and reduction in the constant energy expenditure associated with coping with chronic pain could explain the marked reduction in FAS scores. This finding is clinically significant as it demonstrates that the intervention, when delivered at the scalene site, provides benefits that extend beyond simple pain reduction to meaningfully impact overall quality of life and functional capacity.
Existing literature on DSN interventions is limited and highlights specific challenges, including the difficulty of consistent ultrasound identification of the nerve.32 Previous studies, while demonstrating feasibility, have been preliminary in nature. For instance, Restrepo-Garces et al32 described a rhomboid muscle stimulation-guided technique at the middle scalene using 2 mL of 0.5% bupivacaine, which, while effective, provided only transient analgesia with a 70% pain reduction lasting 24 hours. Similarly, in a larger but non-comparative study, Liu et al33 treated 128 patients with “pain-point” injections, finding that over 90% of patients requiring 4–6 injections had chronic symptoms exceeding six months. These findings collectively suggest that repeated, non-targeted procedures were often necessary for sustained relief, highlighting a significant limitation in existing treatment paradigms.
Building upon this foundation and extending beyond previous technical reports from our group and others,18,21,22 our study was designed to address these key methodological gaps. Specifically, we provide Level I evidence from a randomized controlled trial that directly compares two standardized ultrasound-guided approaches. Furthermore, our results demonstrate that a single, precisely targeted corticosteroid hydrodissection at the suspected primary entrapment site provides symptom relief for up to three months, thereby potentially obviating the need for the multiple injection sessions reported in earlier studies.
The primary strengths of this study—its randomized design and blinding of patients and outcome assessors—help ensure the validity of the findings. To the best of our knowledge, it is the first to directly compare the therapeutic efficacy of the middle scalene and scapular approaches for DSN intervention. Finally, the consistency of our findings across multiple outcome domains—pain at rest, pain with movement, fatigue, and patient satisfaction— supports the clinical relevance of the observed differences.
Several limitations of this study should be considered. First, the sample size was relatively small, though it was adequately powered to detect the large effect sizes we observed. Second, the follow-up period of three months, while demonstrating symptom improvement, represents a relatively short-term outcome. Long-term follow-up studies are warranted to determine the durability of these benefits beyond three months and to establish the optimal frequency of repeat interventions. Third, due to the inherent nature of the interventions requiring different patient positions (supine vs prone) and distinct sonographic windows, the physicians performing the procedures could not be blinded to the group assignment. However, every effort was made to minimize potential bias by blinding the patients, the outcome assessors, and the electrodiagnostic physician. It is also important to note that while ultrasound-guided procedures are operator-dependent, their reliability and reproducibility can be significantly enhanced with standardized protocols and adequate training, as implemented in this multicenter study.34 Fourth, the absence of a sham-control group limits our ability to account for placebo effects, although the large between-group differences strongly suggest a specific anatomical-site effect. Fifth, as noted above, the study design does not separate the effects of mechanical hydrodissection from those of corticosteroid injection. Furthermore, while we observed no adverse effects, the use of a 10 mL volume in the confined scalene region warrants continued vigilance for potential effects on adjacent structures in larger clinical practice. Future studies could incorporate a sham-controlled design and mechanistic comparisons to further validate these findings. Therefore, while our results provide comparative evidence favoring the scalene approach for short-term outcomes, larger, randomized, controlled, multi-center trials with long-term follow-up, sham controls, and comprehensive outcome assessments are needed to confirm these findings and establish their clinical implications.
Conclusion
This randomized controlled trial provides comparative evidence addressing a key clinical question in the management of dorsal scapular nerve entrapment. Our findings demonstrate that ultrasound-guided corticosteroid hydrodissection at the suspected primary site of entrapment—the middle scalene muscle—resulted in better outcomes than a distal scapular approach over a three-month period. The scalene approach was associated with greater improvement across a spectrum of patient-centered outcomes, including pain at rest and during movement, fatigue, and satisfaction.
The consistency and magnitude of these results —with large effect sizes and high statistical significance— suggest that the combined intervention may be most effective when delivered at the primary anatomical site of suspected nerve compression. The significant improvement in fatigue, a debilitating comorbidity of chronic pain, underscores that this approach provides benefits that extend beyond analgesia to potentially enhance overall quality of life.
Therefore, for clinicians managing patients with DSN entrapment syndrome, the middle scalene approach may be considered a preferred option for ultrasound-guided corticosteroid hydrodissection, based on the short-term comparative evidence of greater efficacy and demonstrated safety profile. However, these conclusions are tempered by the study’s three-month follow-up duration and the inability to separate the effects of mechanical hydrodissection from corticosteroid pharmacology. Future research with longer-term follow-up is warranted to confirm the durability of these benefits. Additionally, mechanistic studies are needed to establish the individual contributions of the corticosteroid and hydrodissection components of the intervention.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
The authors want to appreciate Editage for providing professional English editing. The authors would like to declare that both Abdelraheem Mahmoud Elawamy and King Hei Stanley Lam are the co-first authors for their equal contribution to this manuscript.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Tubbs RS, Tyler-Kabara EC, Aikens AC, et al. Surgical anatomy of the dorsal scapular nerve. J Neurosurg. 2005;102(5):910–19. doi:10.3171/jns.2005.102.5.0910
2. Cho H, Kang S, Won H-S, et al. New insights into pathways of the dorsal scapular nerve and artery for selective dorsal scapular nerve blockade. Korean J Pain. 2019;32(4):307–312. doi:10.3344/kjp.2019.32.4.307
3. Sultan HE, Younis El-Tantawi GA. Role of dorsal scapular nerve entrapment in unilateral interscapular pain. Arch Phys Med Rehabil. 2013;94(6):1118–1125. doi:10.1016/j.apmr.2012.11.040
4. Srikumaran U, Wells JH, Freehill MT, et al. Scapular winging: a great masquerader of shoulder disorders: AAOS exhibit selection. J Bone Joint Surg Am. 2014;96(14):e122. doi:10.2106/JBJS.M.01031
5. Akgun K, Aktas I, Terzi Y. Winged scapula caused by a dorsal scapular nerve lesion: a case report. Arch Phys Med Rehabil. 2008;89(10):2017–2020. doi:10.1016/j.apmr.2008.03.015
6. Myrtos CD. Functional soft-tissue examination and treatment by manual methods. J Can Chiropr Assoc. 2011;55(1):64.
7. Chen D, Gu Y, Lao J, et al. Dorsal scapular nerve compression. Atypical thoracic outlet syndrome. Chin Med J. 1995;108(8):582–585.
8. Aronsson G, Gustafsson K, Dallner M. Sick but yet at work. An empirical study of sickness presenteeism. J Epidemiol Community Health. 2000;54(7):502–509. doi:10.1136/jech.54.7.502
9. Briggs AM, Smith AJ, Straker LM, et al. Thoracic spine pain in the general population: prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskelet Disord. 2009;10:77. doi:10.1186/1471-2474-10-77
10. Hincapie CA, Cassidy JD, Côté P, et al. Whiplash injury is more than neck pain: a population-based study of pain localization after traffic injury. J Occup Environ Med. 2010;52(4):434–440. doi:10.1097/JOM.0b013e3181bb806d
11. Chang KV, Lin C-P, Lin C-S, et al. Sonographic tracking of trunk nerves: essential for ultrasound-guided pain management and research. J Pain Res. 2017;10:79–88. doi:10.2147/JPR.S123828
12. Lam KHS, Wu YT, Reeves KD, Galluccio F, El-Sayed Allam A, Peng PWH. Ultrasound-guided interventions for carpal tunnel syndrome: a systematic review and meta-analyses. Diagnostics. 2023;13(6).doi:10.3390/diagnostics13061138
13. Adamowicz JL, Vélez-Bermúdez M, Thomas EBK. Fatigue severity and avoidance among individuals with chronic disease: a meta-analysis. J Psychosom Res. 2022;159:110951. doi:10.1016/j.jpsychores.2022.110951
14. Sturgeon JA, Darnall BD, Kao M-CJ, et al. Physical and psychological correlates of fatigue and physical function: a Collaborative Health Outcomes Information Registry (CHOIR) study. J Pain. 2015;16(3):291–8.e1. doi:10.1016/j.jpain.2014.12.004
15. Schaufeli W, van Dierendonck D. Burnout, een begrip gemeten. De Nederlandse versie van de Maslach Burnout Inventory (MBI-NL) [Burnout, the measurement of a concept. The Dutch version of the Maslach Burnout Inventory (MBI-NL)]. Gedrag Gezondheid. 1994;22(4):153–172.
16. Lin TY, Chang KV, Wu WT, Mazian K, Ricci V, Özçakar L. Ultrasound-Guided Interventions for Neuropathic Pain: a Narrative Pictorial Review. Life. 2025;15(9).doi:10.3390/life15091404
17. Haim K, Urban BJ. Dorsal scapular nerve block: description of technique and report of a case. Anesthesiology. 1993;78(2):361–363. doi:10.1097/00000542-199302000-00021
18. Lam KHS, Hung CY, Su D. Comments on “Dorsal scapular nerve entrapment neuropathy managed by ultrasound-guided hydrodissection - a case report”. J Ultrason. 2021;21(86):e267–e269. doi:10.15557/JoU.2021.0044
19. Martin RM, Fish DE. Scapular winging: anatomical review, diagnosis, and treatments. Curr Rev Musculoskelet Med. 2008;1(1):1–11. doi:10.1007/s12178-007-9000-5
20. Hanson NA, Auyong DB. Systematic ultrasound identification of the dorsal scapular and long thoracic nerves during interscalene block. Reg Anesth Pain Med. 2013;38(1):54–57. doi:10.1097/AAP.0b013e31826f0a63
21. Lam KHS, Hung C-Y, Chiang Y-P, et al. Ultrasound-guided nerve hydrodissection for pain management: rationale, methods, current literature, and theoretical mechanisms. J Pain Res. 2020;13:1957–1968. doi:10.2147/JPR.S247208
22. Lam SKH, Reeves KD, Cheng AL. Transition from deep regional blocks toward deep nerve hydrodissection in the upper body and torso: method description and results from a retrospective chart review of the analgesic effect of 5% dextrose water as the primary hydrodissection injectate to enhance safety. Biomed Res Int. 2017;2017:7920438. doi:10.1155/2017/7920438
23. Karcioglu O, Topacoglu H, Dikme O, et al. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36(4):707–714. doi:10.1016/j.ajem.2018.01.008
24. Boonstra AM, Schiphorst Preuper HR, Reneman MF, et al. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int J Rehabil Res. 2008;31(2):165–169. doi:10.1097/MRR.0b013e3282fc0f93
25. Delgado DA, Lambert BS, Boutris N, et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J Am Acad Orthop Surg Glob Res Rev. 2018;2(3):e088. doi:10.5435/JAAOSGlobal-D-17-00088
26. Chalder T, Berelowitz G, Pawlikowska T, et al. Development of a fatigue scale. J Psychosom Res. 1993;37(2):147–153. doi:10.1016/0022-3999(93)90081-P
27. Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932;140:5–55.
28. Faul F, Erdfelder E, Lang A-G, et al. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
29. Lam KHS, Allam AE-S, Lai WWM, et al. Ultrasound-guided hydrodissection for dorsal scapular nerve entrapment: a technical report on the scalene and scapular approaches. Cureus. 2025;17(12):e98571. doi:10.7759/cureus.98571
30. Modi DJ, Tuttle JM, Kang S, et al. Utilizing an ultrasound guided 5-in-1 trigger point and hydrodissection technique for interscapular mid-thoracic myofascial pain: a retrospective review. Intervent Pain Med. 2023;2(4):100285. doi:10.1016/j.inpm.2023.100285
31. Fagerland MW. t-tests, non-parametric tests, and large studies--a paradox of statistical practice? BMC Med Res Methodol. 2012;12:78. doi:10.1186/1471-2288-12-78
32. Restrepo-Garces C. Dorsal scapular nerve block under ultrasound guidance. In:
33. Liu Q-J, Xia ZX-P, Zhu J, Li J. Clinical analysis of 128 patients with dorsal scapular nerve compression treated with pain-point injections. Pain Clin J. 2010;1:10–12.
34. Chiaramonte R, Bonfiglio M, Castorina EG, et al. The primacy of ultrasound in the assessment of muscle architecture: precision, accuracy, reliability of ultrasonography. Physiatrist, radiologist, general internist, and family practitioner’s experiences. Rev Assoc Med Bras. 2019;65(2):165–170. doi:10.1590/1806-9282.65.2.165
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.