Back to Journals » Journal of Pain Research » Volume 19
Comparative Efficacy of Canggui Tanxue Acupuncture Combined with Scapular Stabilization Training versus Scapular Stabilization Training Alone for Rotator Cuff Injury: A Retrospective Cohort Study
Authors Geng Y, Song M, Huang B, Lin R, Wu S, Lin A, Wang X
Received 12 January 2026
Accepted for publication 25 March 2026
Published 15 April 2026 Volume 2026:19 591459
DOI https://doi.org/10.2147/JPR.S591459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yining Geng,1,* Manping Song,1,* Bing Huang,1,* Ru Lin,1 Shiwen Wu,2 An Lin,2 Xiaolin Wang3
1Department of Acupuncture, Hainan General Hospital, Haikou, Hainan, People’s Republic of China; 2Department of Traditional Chinese Medicine and Western Medicine, Hainan General Hospital Branch-Tunchang Hospital, Tunchang, Hainan, People’s Republic of China; 3Rehabilitation Medicine Department, Pingliang Traditional Chinese Medicine Hospital, Pingliang, Gansu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaolin Wang, Email [email protected]
Aim: To evaluate the clinical efficacy of combining Canggui Tanxue acupunc-ture combined with scapular stabilization training (SST) versus SST alone for mild-to-moderate rotator cuff injuries (RCI) in a real-world clinical setting.
Methods: This retrospective cohort study analyzed 160 patients with mild-to-moderate RCI treated at Department of Acupuncture, Hainan General Hospital between January 2024 and June 2025. Patients were categorized into two groups based on treatment received: SST alone (Control group, n = 80) and SST plus Canggui Tanxue acupuncture (Combination group, n = 80). Primary outcomes included shoulder function (American Shoulder and Elbow Surgeons [ASES] score), pain intensity (Visual Analog Scale [VAS]), active range of motion (ROM), quality of life (Short Form-36 [SF-36]), and clinical efficacy rates. Data were extracted from electronic medical records.
Results: The Combination group demonstrated significantly superior outcomes compared to the Control group: higher ASES scores (93.31 ± 9.09 vs. 81.42 ± 8.45, P < 0.001), lower VAS scores (2.09 ± 0.48 vs. 3.52 ± 0.93, P < 0.001), greater ROM improvements (e.g. external rotation: 80.40 ± 8.22 vs. 65.59 ± 7.86, P < 0.001), and higher SF-36 scores (80.51 ± 8.48 vs. 65.44 ± 8.29, P < 0.001). Clinical efficacy rates were superior in the Combina-tion group (excellent: 76.25% vs. 47.50%; total efficacy: 93.75% vs. 77.50%, P < 0.001). Effect sizes were large for ASES (Cohen’s d=1.42) and VAS (d=− 1.89). The number needed to treat (NNT) for achieving excellent efficacy was 3.48.
Conclusions and Implications: The study demonstrates that integrating Canggui Tanxue acupuncture with SST yields clinically meaningful improvements in shoulder function, pain relief, and quality of life for mild-to-moderate RCI patients, surpassing SST alone. These findings support the adoption of this combined approach in routine clinical practice, particularly given its high efficacy (NNT = 3.48) and large effect sizes.
Keywords: rotator cuff injury, acupuncture, Canggui Tanxue, scapular stabilization, real-world evidence, retrospective cohort study
A Letter to the Editor has been published for this article.
Introduction
Rotator cuff injury (RCI), characterized by structural damage to the supraspinatus, infraspinatus, teres minor, and subscapularis tendons, is among the most prevalent musculoskeletal disorders worldwide and a major contributor to chronic shoulder pain cases. Its primary etiology involves mechanical stressors (eg. repetitive overhead activity, trauma, or age-related degeneration), resulting in tendon inflammation, microtears, and functional impairment.1 Clinically, RCI manifests as debilitating pain, restricted range of motion (ROM), and compromised activities of daily living (ADLs), significantly reducing quality of life and imposing substantial socioeconomic burdens.2 Without timely intervention, RCI may progress to irreversible complications, including muscle atrophy, fatty infiltration, and glenohumeral joint instability, often necessitating surgical management.
Current therapeutic strategies encompass conservative and surgical approaches. While arthroscopic repair demonstrates efficacy for severe tears, its inherent risks include surgical complications, prolonged rehabilitation, and variable functional outcomes.3,4 Consequently, non-surgical modalities remain first-line for mild-to-moderate RCI, focusing on pain control, functional restoration, and prevention of disease progression. Among these, scapular stabilization training (SST) has emerged as a cornerstone intervention by targeting scapulothoracic dyskinesia—a key biomechanical factor in RCI pathogenesis. SST enhances neuromuscular control, optimizes shoulder kinematics, and promotes tendon healing through structured exercises that facilitate scapular repositioning and muscle coordination.5 Nevertheless, SST monotherapy exhibits limitations, including slow symptomatic relief, suboptimal pain modulation, and plateaued efficacy in subsets of patients, underscoring the need for adjunctive therapies.
Complementary to biomechanical approaches, Canggui Tanxue acupuncture—a specialized technique involving multi-directional, layered needle stimulation—offers a neurophysiological pathway to pain management and tissue repair.6 By targeting acupoints such as Jianyu (LI15) and Ashi points, this method is proposed to modulate nociceptive signaling, resolve local qi-blood stasis, and improve microcirculation, synergistically addressing inflammatory and functional aspects of RCI. From a Traditional Chinese Medicine perspective, the Canggui Tanxue acupuncture deeply penetrates fascial layers to resolve local Qi and blood stasis. Neurophysiologically, this multi-directional and layered mechanical stimulation disrupts fibrotic adhesions and modulates peripheral nociceptors, thereby reducing central sensitization and optimizing local microcirculation.7 Although acupuncture is empirically integrated into some rehabilitation protocols, robust evidence evaluating its combination with evidence-based SST for RCI remains limited.
Given the multifactorial nature of RCI—encompassing biomechanical dysfunction, peripheral sensitization, and chronic pain pathways—a combinatorial strategy targeting both structural and neurophysiological dimensions holds theoretical promise. However, the clinical synergy between SST and Canggui Tanxue acupuncture remains underexplored, with limited high-quality trials quantifying their integrated efficacy. This knowledge gap impedes the optimization of non-surgical RCI management algorithms. While randomized trials are ideal, real-world evidence from clinical practice is critical for validating treatment effectiveness. This retrospective cohort study leverages existing clinical data to compare outcomes between SST monotherapy and SST combined with Canggui Tanxue acupuncture, providing pragmatic insights into potential synergistic effects. We hypothesize that the combined protocol will yield superior improvements in pain relief, functional recovery, and quality of life by concurrently modulating scapulothoracic biomechanics and pain modulation pathways. The findings aim to inform evidence-based clinical decision-making, offering a safer, more effective conservative strategy for RCI patients.
Materials and Methods
Study Design and Participants
Retrospective cohort study using electronic health records from the Depart-ment of Acupuncture, Hainan General Hospital, Hainan Medical University (January 2024–June 2025). A total of 160 eligible patients meeting inclusion cri-teria were enrolled and assigned based on actual treatment received into two groups: Control group (SST alone, n = 80) or Combination group (SST plus Canggui Tanxue acupuncture, n = 80). As a retrospective cohort study, patients were not randomized. Treatment allocation was based on shared clinical decision-making, patient preference regarding the acceptance of acupuncture, and the availability of acupuncturists at the time of consultation. Ethical approval was granted by the Insti-tutional Review Board of Hainan General Hospital, Hainan Medical University (Approval No. YL-2025-03). All procedures adhered to the Declaration of Hel-sinki.
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Diagnosis of RCI per standard Western medical crite-ria; (2) Grade I or II RCI; (3) Age 25–60 years; (4) Symptom duration > 7 days; (5) Complete clinical data; (6) Voluntary participation with informed consent.
Exclusion Criteria
(1) Concurrent shoulder pathologies (eg., dislocation, fracture); (2) Massive rotator cuff tear; (3) Hepatic or renal dysfunction; (4) Psychiatric disorders or cognitive impairment; (5) Prior surgical intervention for RCI; (6) Concurrent malignancy or participation in other trials; (7) Inability to cooperate with treatment.
Treatment Methods
Control Group
Patients received SST twice daily for 6 weeks. To ensure both professional guidance and adequate treatment frequency, this regimen consisted of one supervised session conducted in the hospital rehabilitation center and one prescribed home-based exercise session. The supervised SST protocol included the following: (1) Scapular Facilitation Training (10 min/session): The therapist, positioned beside the seated patient, elevated the scapular girdle while adducting the scapula and externally mobilizing the pectoralis major. Then reversed the motion (abduction/upward ro-tation of scapula with adduction/depression of pectoralis major). (2) Scapular Control Training (10 min/session): Patients maintained a seated position, using the Bobath handshake grip under therapist guidance to ensure correct gleno-humeral alignment. (3) Trunk Anti-gravity Extension Training (10 min/session): Patients maintained a seated position and is instructed by the therapist to perform scapular adduction while the head is extended against gravity.
Combination Group
Patients received SST (identical to the Control Group) plus Canggui Tanxue acupuncture. The acupuncture sessions were administered on the same day, immediately prior to the supervised hospital SST session. This specific sequence was designed to maximize initial pain relief and fascial release, thereby facilitating better gleno-humeral alignment and biomechanical execution during the subsequent stabilization exercises. The acupuncture protocol was as follows: (1) Positioning: Lateral decubitus (healthy side down) or seated based on tear location. (2) Acupoints: Jianyu (LI15), Jianqian (Extra), Jianhou (SI10), Ashi points. (3) Needling: 0.30 mm × 40 mm filiform needles inserted perpendicularly to the Di (Earth) region depth; withdrawn to Tian (Heaven) region upon Deqi. (4) Technique: Oblique needling (45°) per-formed in multiple directions (superior, inferior, left, right) and depths (Tian, Ren, Di regions), seeking Deqi each time. (5) Retention: Needles retained for 30 minutes per session. (6) Frequency: Twice per session, five times weekly for 6 weeks.
Outcome Measures
- Shoulder function: American Shoulder and Elbow Surgeons (ASES) score (0–100, lower = worse function).8
- Pain intensity: Visual Analog Scale (VAS) (0–10 cm, lower = less pain).9
- Active myofascial trigger points (MTrPs): Counted via systematic palpation by trained clinicians.10
- Active range of motion (ROM): Assessed using a universal goniometer for external rotation, internal rotation, anterior flexion, and posterior extension (mean of 3 measurements).11
- Quality of life: 36-Item Short-Form Health Survey (SF-36) (0–100, lower=worse quality of life).12
- Clinical Efficacy Rate: Classified by VAS improvement: Cured (≥ 90%), Markedly Effective (60–89%), Effective (30–59%), Ineffective (< 30%). Excellent Rate = (Cured + Markedly Effective)/Total × 100%. Total Efficacy Rate = (Cured + Markedly Effective + Effective)/Total × 100%.6
All outcome assessments were conducted immediately following the 6-week intervention period. Due to the retrospective nature of the database, standardized long-term follow-up data beyond 6 weeks were not available. Outcome assessments (including ASES, VAS, ROM, MTrPs, and SF-36) were performed by independent blinded assessors who were not involved in treatment delivery and were unaware of group allocation. To maintain blinding, all patient identifiers and treatment codes were concealed during data collection and analysis.
Statistical Analysis
Baseline-adjusted analyses used ANCOVA with baseline scores as covariates. False discovery rate (FDR) correction was applied for multiple comparisons (q<0.05 considered significant). All statistical analyses were performed using R software (version 4.2.2) and SAS statistical software (version 9.4; SAS Institute Inc., Cary, NC, USA). Categorical variables were presented as frequencies (per-centages), and group comparisons were conducted using the chi-square test. Normally distributed continuous variables were expressed as mean ± standard deviation (SD), and group comparisons were performed using analysis of vari-ance (ANOVA). Non-normally distributed continuous variables were reported as median (interquartile range [IQR]), and group comparisons were analyzed using the Wilcoxon rank-sum test. Pearson correlation analysis (for normally distribut-ed data) or Spearman correlation analysis (for non-normally distributed data) was employed to explore the associations between demographic characteristics and study outcomes.
Advanced analyses: (1) Stratified analysis to evaluate efficacy across sub-groups; (2) Multiple linear regression and binary logistic regression models to assess the effects of interventions and clinical indicators on clinical outcomes and improvement effects; (3) Receiver operating characteristic (ROC) curve, decision curve analysis (DCA), and Kolmogorov–Smirnov (KS) curve to evaluate the pre-dictive performance of various indicators for treatment excellent rate and overall response rate; (4) Least absolute shrinkage and selection operator (LASSO) re-gression to screen key predictive variables and construct a nomogram prediction model.All hypothesis tests were two-sided, and a P-value < 0.05 was considered statistically significant.
Furthermore, to validate the methodological strength of this retrospective cohort, a post-hoc power analysis was conducted using the pwr package in R. For the primary continuous outcomes, utilizing an observed large effect size (Cohen’s d > 1.4), a sample size of 80 patients per group, and a two-tailed significance level of 0.05, the statistical power was calculated to exceed 0.99. This confirms that the current sample size was highly sufficient to detect the observed intervention effects.
Results
Patient Characteristics
A total of 160 RCI patients were divided into the Control group (SST alone, n = 80) and Combination group (SST + Canggui Tanxue acupuncture, n = 80). Baseline characteristics were comparable between groups (all P > 0.05). The Control group comprised 48 males (60.00%) and 32 females (40.00%), with a mean age of 48.55 ± 7.21 years; the Combination group included 51 males (63.75%) and 29 females (36.25%), mean age 48.41 ± 7.30 years. Disease dura-tion was comparable (Control: 4.90 ± 0.75 months; Combination: 4.84 ± 0.71 months). Regarding injury distribution, the Control group presented with 37 left-sided injuries, 36 right-sided injuries, and 7 bilateral injuries, whereas the Combination group had 36 left-sided, 39 right-sided, and 5 bilateral injuries. Sta-tistical analysis confirmed no significant differences in any baseline characteris-tics between groups (P > 0.05), as detailed in Table 1.
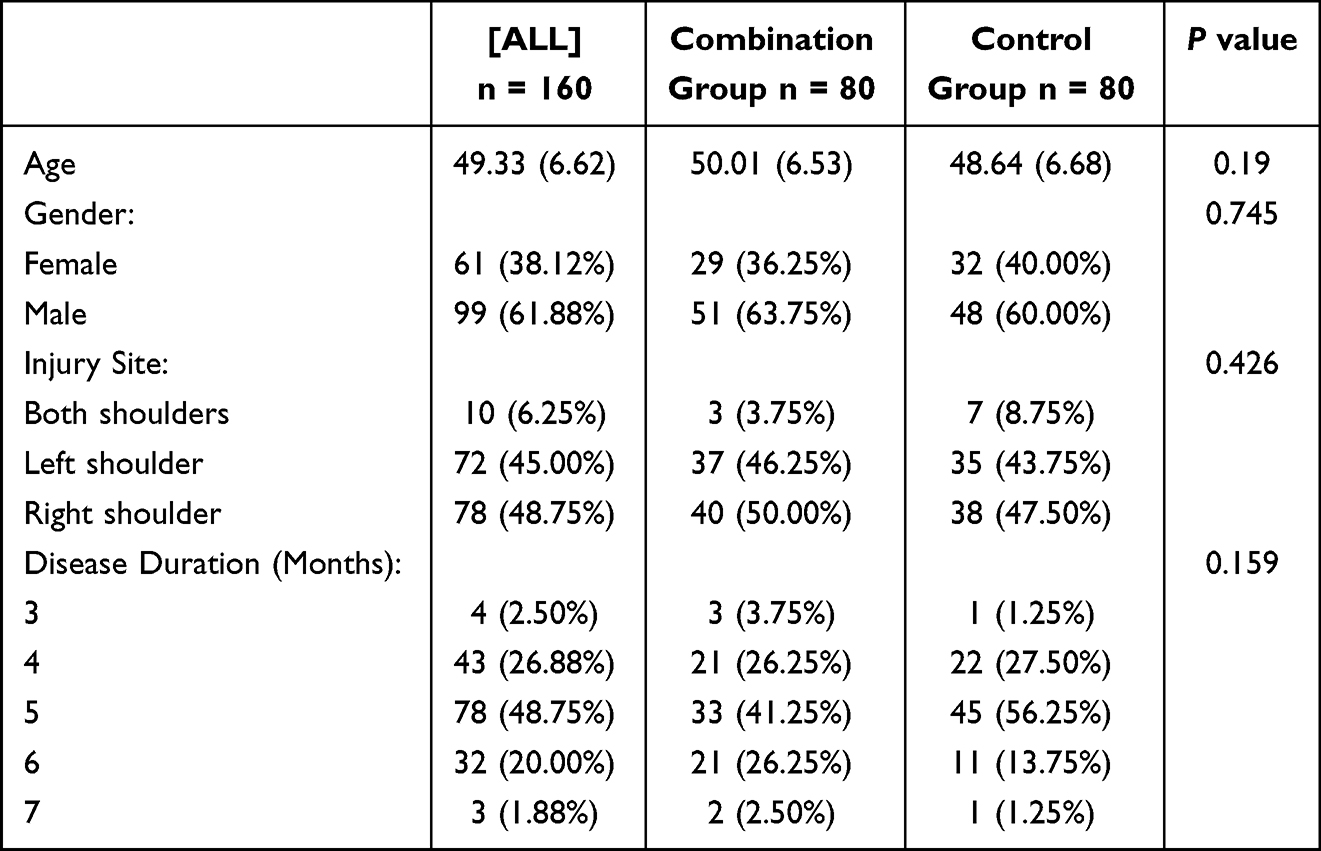 |
Table 1 Patient Characteristics |
Primary Outcomes
After baseline adjustment, the Combination group showed superior outcomes across all primary endpoints. Shoulder function assessed by ASES scores improved markedly in the Combination group (93.56 ± 8.69) compared to Controls (82.14 ± 9.11, P < 0.001), paralleled by greater pain reduction in VAS scores (2.09 ± 0.48 vs. 3.52 ± 0.93, P < 0.001) and fewer active myofascial trigger points (MTrPs: 2.95 ± 0.57 vs. 4.00 ± 0.80, P < 0.001). ROM measurements revealed substantial gains in the Combination group: external rotation increased to 80.40 ± 8.22 vs. 65.59 ± 7.86 in Controls (P < 0.001), internal rotation to 59.26 ± 6.82 vs. 48.33 ± 5.56 (P < 0.001), anterior flexion to 176.41 ± 19.25 vs. 150.65 ± 18.98 (P < 0.001), and extension to 58.52 ± 6.18 versus 48.78 ± 5.39 (P < 0.001). SF-36 scores also improved more significantly in the Combination group (80.51 ± 8.48 vs. 65.44 ± 8.29, P < 0.001). Critically, clinical efficacy rates favored the Combination group, with a 76.25% excellent rate (vs. 47.50% in Controls) and 93.75% total efficacy rate (vs. 77.50%, P < 0.001) (Table 2 and Figure 1).
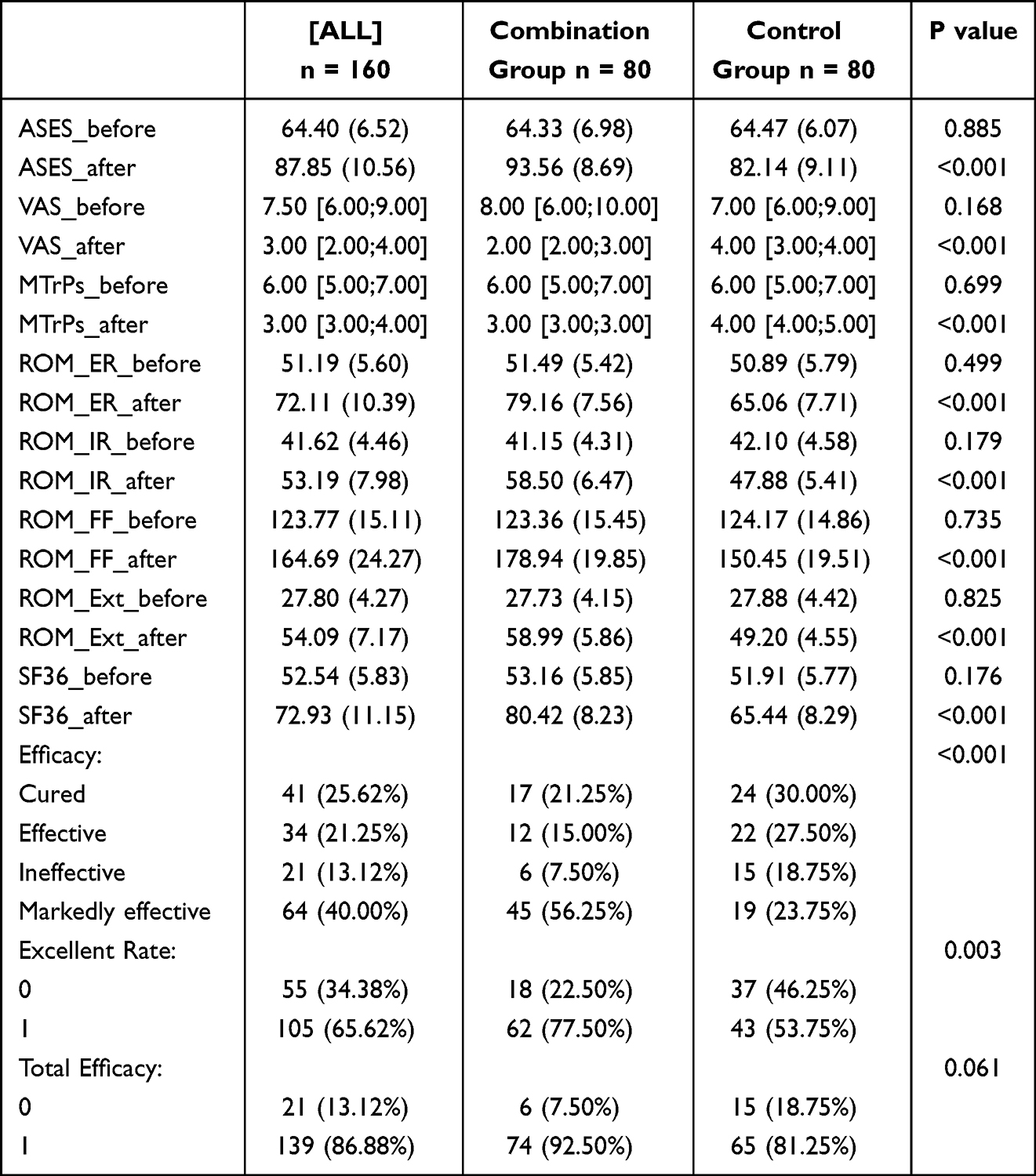 |
Table 2 Primary Outcomes |
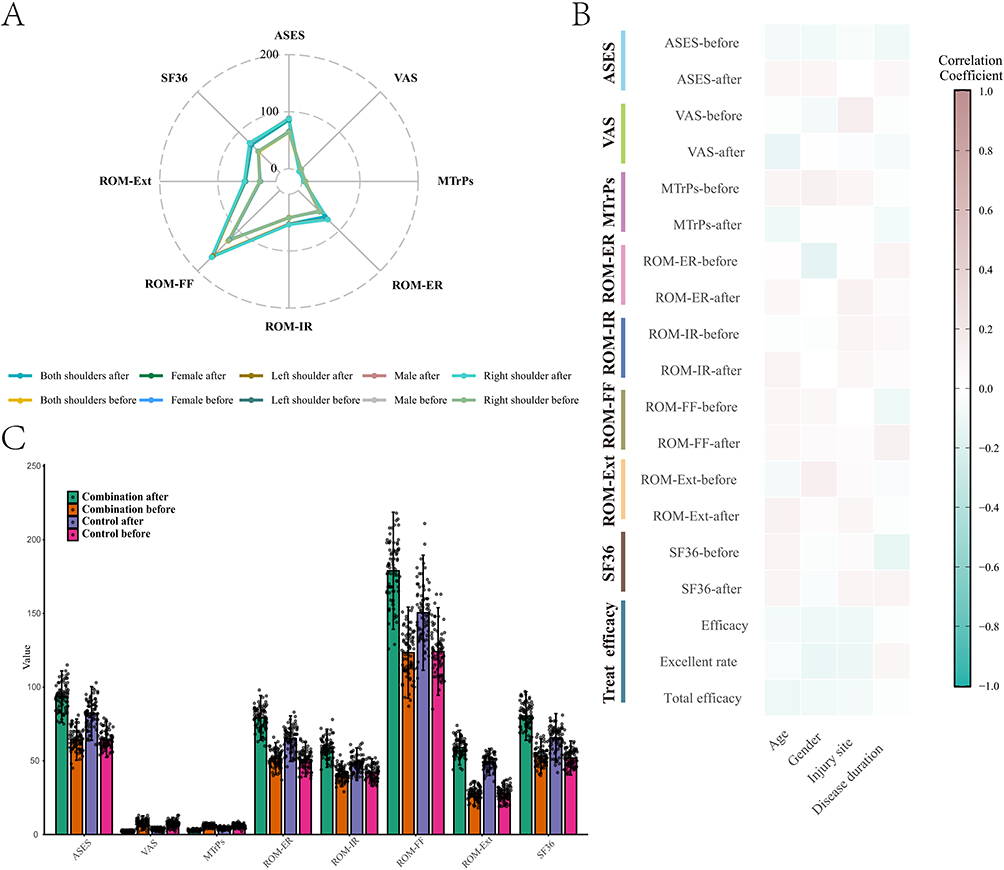 |
Figure 1 Multidimensional assessment of treatment outcomes. (A) Radar chart displaying changes in ASES, VAS, SF-36, MTrPs, and ROM parameters across injury site/gender subgroups; (B) Heatmap showing correlations between demographic factors and clinical indicators; (C) Intergroup comparison of assessment metrics pre- and post-intervention. Abbreviations: ASES, American Shoulder and Elbow Surgeons score; VAS, Visual Analog Scale; MTrPs, Myofascial Trigger Points; ROM, Range of Motion; SF-36, 36-Item Short-Form Health Survey. |
Correlation and Regression Analyses
Robust correlations were observed between functional recovery and pain modulation. Post-intervention ROM parameters strongly correlated with ASES/SF-36 scores (r > 0.7) and inversely correlated with VAS/MTrPs (r < −0.6; all P < 0.001). Excellent efficacy rates showed negative associations with residual MTrPs (r = −0.53) and VAS (r = −0.61) (Figure 2). Linear regression quantified the treatment effect: the combined protocol independently improved ASES (β = 11.334, 95% CI: 8.508–14.160) and reduced VAS (β = −1.443, 95% CI: −1.686 to −1.200; both P < 0.001), with ROM-Extension (β = 9.767) and ROM-Internal Rotation (β = 10.593) identified as key functional drivers (Figure 3). Predictive modeling reinforced these findings: ROM-Extension (AUC = 0.722) and MTrP reduction (AUC = 0.697) emerged as top predictors for excellent efficacy, while the comprehensive model (ALL) achieved optimal clinical utility (AUC = 0.740; net benefit: 0.4–0.8 across risk thresholds; Figures 4–6). LASSO-based nomograms further validated ROM-Extension (OR = 1.091) and ROM-Internal Rotation (OR = 1.062) as primary determinants of excellent outcomes (both P ≤ 0.001; Figures 7–9).
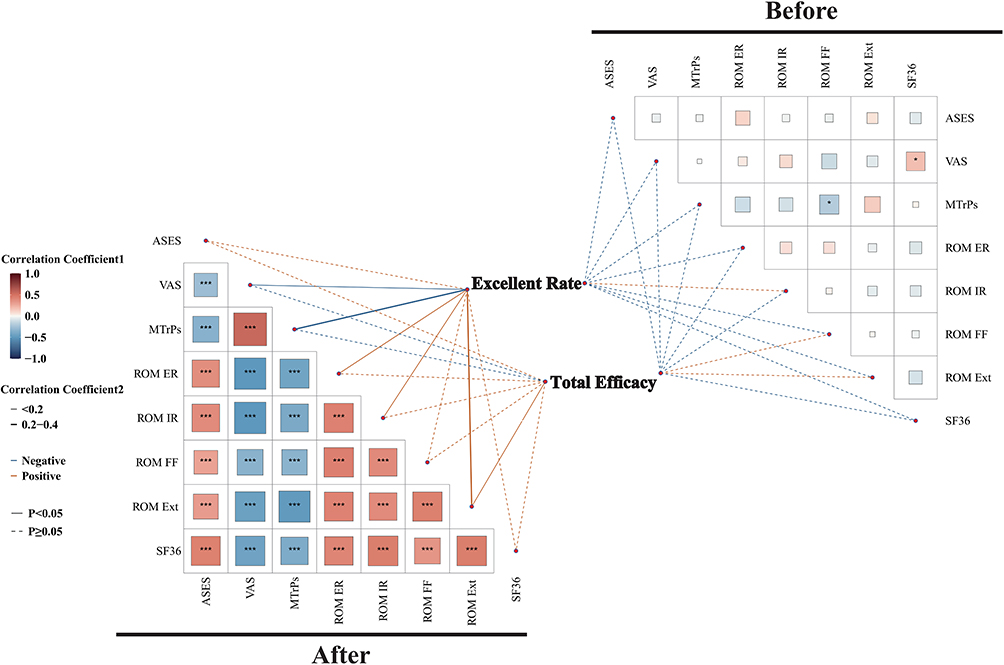 |
Figure 2 Correlation matrix of clinical indicators. The lower triangle presents the post-intervention associations between functional and pain metrics, while the upper triangle displays the pre-intervention baseline associations. Color intensity reflects the strength of the correlation (red = positive, blue = negative). Statistical significance is denoted as: *P<0.05; ***P<0.001. |
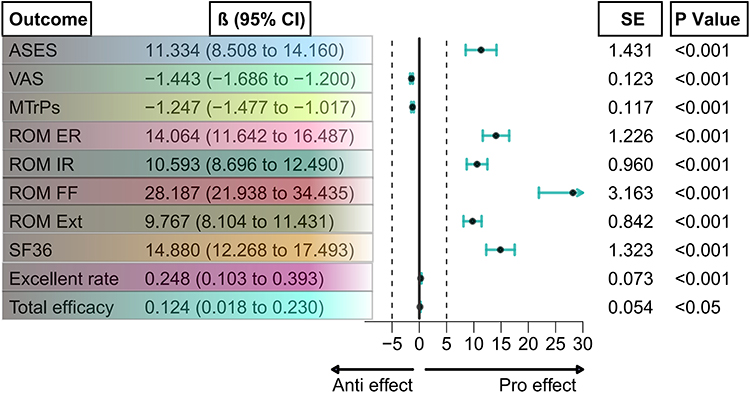 |
Figure 3 Forest plot of linear regression coefficients (β) with 95% confidence intervals (CIs). The plot demonstrates the independent treatment effects of the combined protocol on functional outcomes (ASES, SF-36), pain metrics (VAS, MTrPs), ROM parameters, and overall clinical efficacy, adjusting for baseline covariates. The dashed vertical line indicates a null effect (β = 0). |
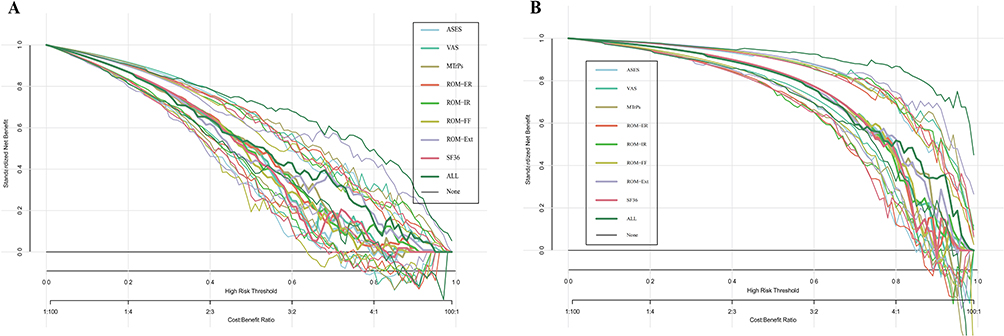 |
Figure 4 Receiver operating characteristic (ROC) curves evaluating the predictive performance of clinical indicators for (A) excellent efficacy rate and (B) total efficacy rate. Area under the curve (AUC) values with 95% CIs are presented for individual post-intervention parameters. The comprehensive prediction model (ALL) specifically includes ASES_after + VAS_after + ROM_Ext_after, demonstrating the highest diagnostic accuracy. |
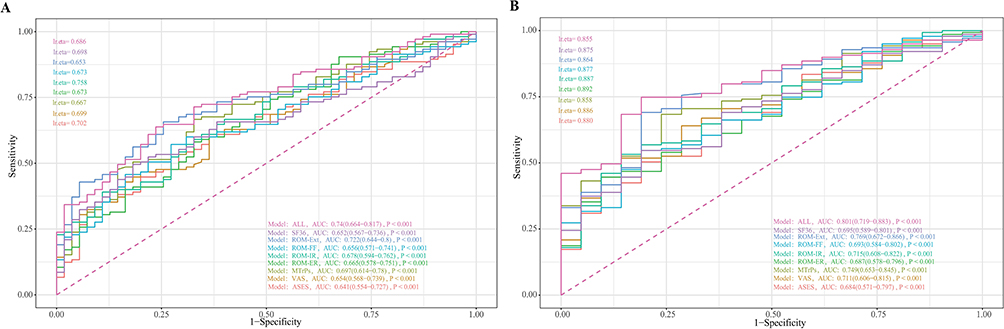 |
Figure 5 Decision curve analysis (DCA) evaluating the clinical utility of the predictive models across various risk thresholds for (A) excellent efficacy rate and (B) total efficacy rate. The standardized net benefit (Y-axis, range 0–1.0) is plotted against the threshold probability (X-axis, high-risk threshold from 0–1.0). Higher net benefit values indicate superior clinical utility across different clinical decision-making scenarios. The comprehensive model (ALL: ASES_after + VAS_after + ROM_Ext_after) consistently demonstrates the highest net benefit. |
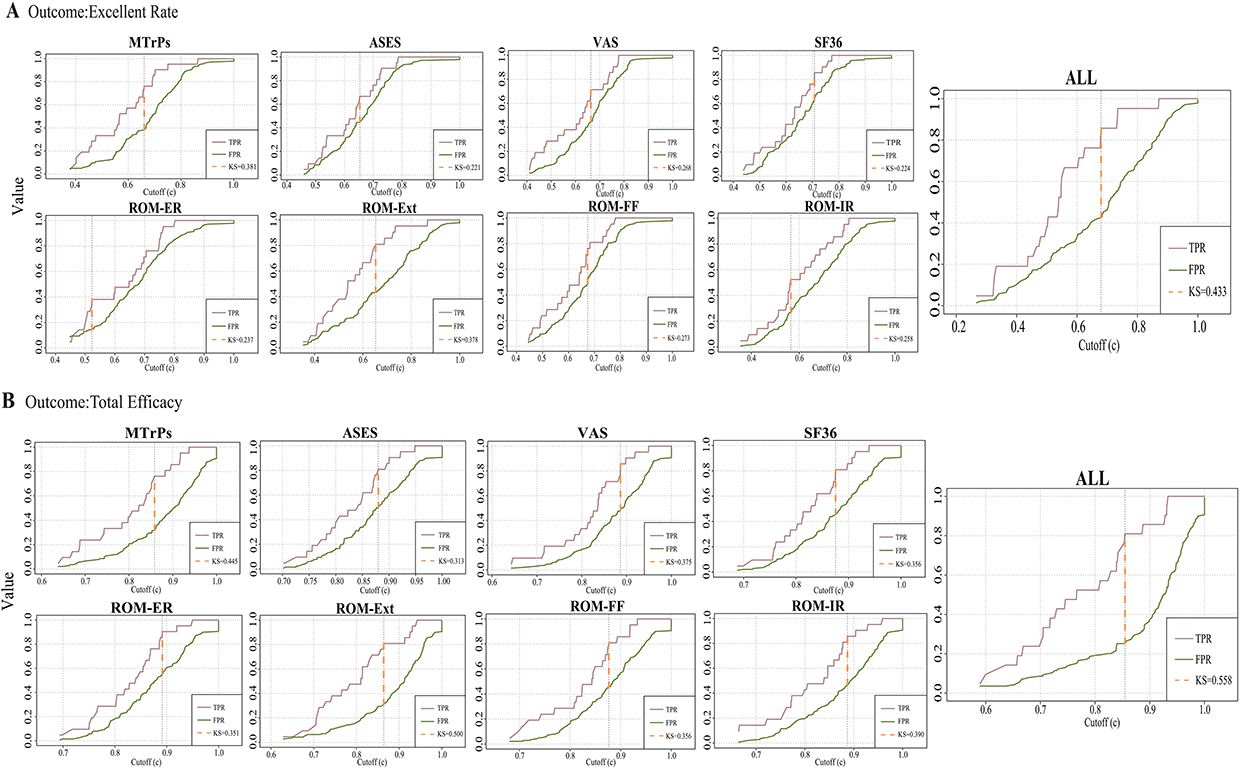 |
Figure 6 Kolmogorov–Smirnov (KS) curves displaying the distributions of the true positive rate (TPR) and false positive rate (FPR) for (A) excellent efficacy rate and (B) total efficacy rate predictions based on the comprehensive model (ALL: ASES_after + VAS_after + ROM_Ext_after). The TPR curve illustrates the rapid ascent with increasing predicted probability, indicating effective capture of high-probability positive cases. The FPR curve demonstrates a gradual increase, suggesting minimal misclassification of low-probability positive cases. The maximum vertical distance between the TPR and FPR curves relative to the diagonal represents the KS statistic value. |
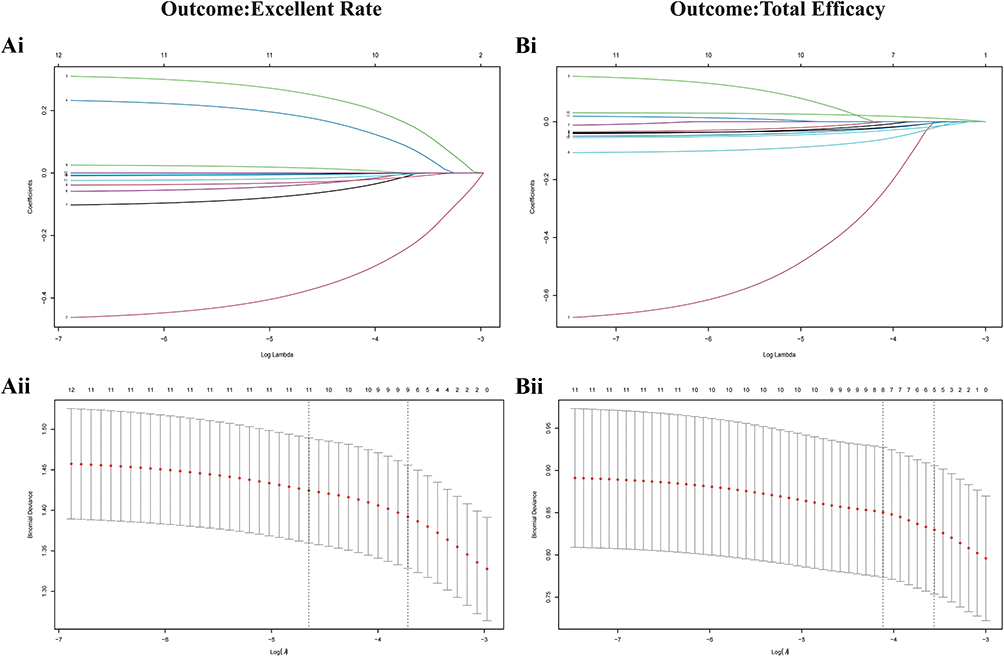 |
Figure 7 Least absolute shrinkage and selection operator (LASSO) regression analysis for variable selection. (Ai) Coefficient profile plot for predicting the excellent efficacy rate. The trajectory of each predictor’s coefficient is shown as log(λ) changes. (Bi) Coefficient profile plot for predicting the total efficacy rate. (Aii and Bii) 10-fold cross-validation curve plots used to select the optimal lambda (λ) for the excellent rate (Aii) and total efficacy (Bii) prediction models. The vertical axis represents the model error (binomial deviance), and the horizontal axis represents log(λ). The two dotted vertical lines indicate the optimal values: the left dotted line represents the λ value that yields the minimum criteria (λmin), and the right dotted line represents the λ value that yields the 1 standard error of the minimum criteria (λ1se). Key predictive variables were selected based on the optimal λmin values to construct the nomogram models. |
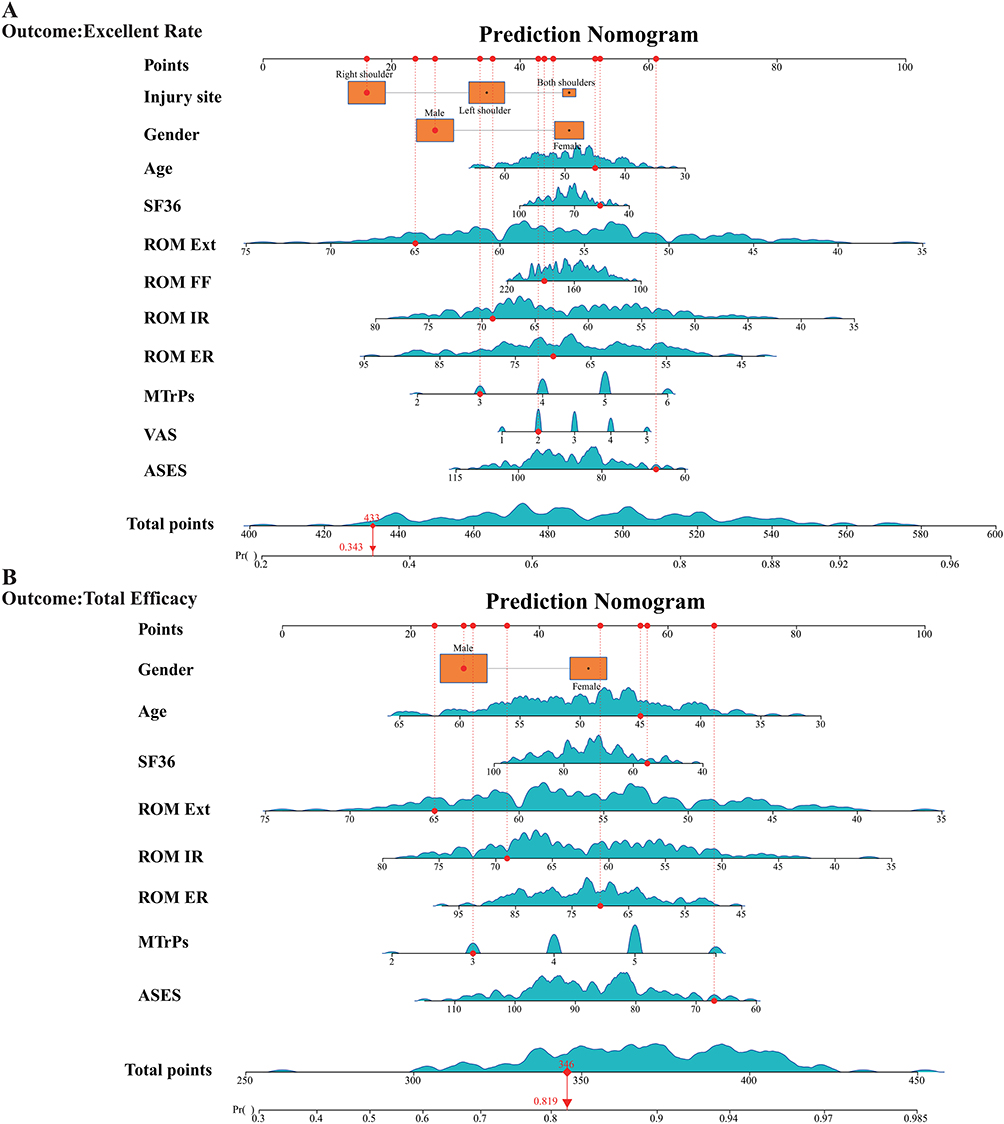 |
Figure 8 Nomogram prediction models for estimating clinical outcomes. (A) Nomogram predicting the probability of achieving an excellent efficacy rate; (B) Nomogram predicting the probability of achieving total efficacy. Segment lengths on the respective scales indicate the relative contribution weights of each selected predictor. The red visual elements illustrate how to use the nomogram for a hypothetical patient example. The red dots on each variable axis represent the patient’s specific clinical values. The red vertical dotted lines map these individual values upwards to the “Points” axis (top scale) to assign a specific score for each variable. The red diamond on the “Total points” axis represents the sum of all individual scores for this patient (e.g., 433 in (A), and 346 in (B)). The solid red downward arrow projects this total score onto the bottom “Pr()” axis to reveal the final predicted probability of the clinical outcome (e.g., 0.343 in (A), and 0.819 in (B). |
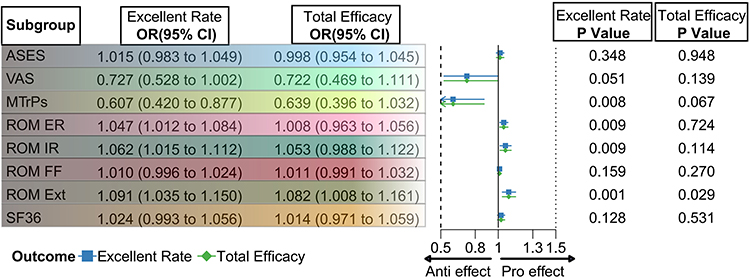 |
Figure 9 Forest plots displaying the odds ratios (ORs) with 95% CIs for the impact of individual clinical indicators on achieving an excellent efficacy rate and total efficacy. The vertical dashed line indicates a null effect (OR = 1). |
Subgroup Analyses Reinforced These Findings
Subgroup analyses reinforced these findings, consistently favoring the combined therapy. Gender-stratified data confirmed significant improvements in both males and females for all functional and pain metrics (P < 0.05; Figure 10). Critically, the integrated protocol amplified the impact of clinical indicators: it enhanced the pain-modulating effects of MTrPs/VAS on excellent efficacy and augmented functional benefits from ASES/SF-36/ROM metrics, while uniquely strengthening the influence of anterior flexion (ROM-FF) on total efficacy—a phenomenon absents in the control group (Figure 11). No adverse events were reported, and treatment adherence exceeded 95% in both cohorts, underscoring the safety and feasibility of the combined intervention.
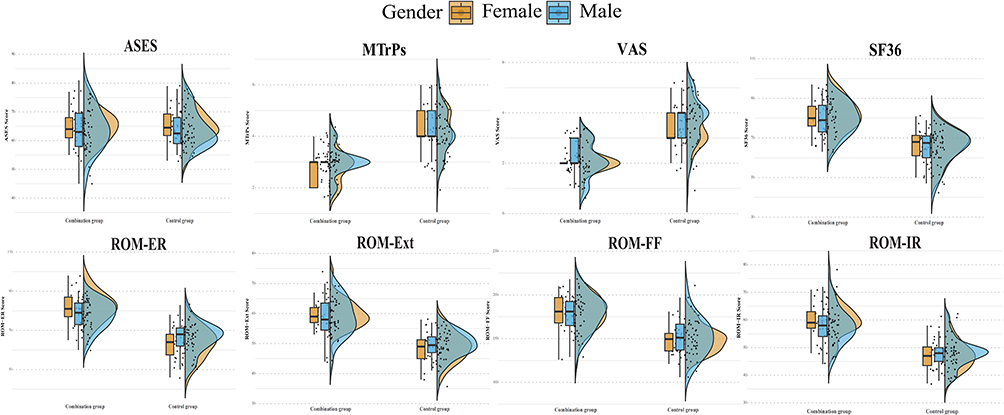 |
Figure 10 Distribution of primary outcomes stratified by gender. Left panel shows box plots (median, IQR, range). Right panel displays violin plots with probability density. |
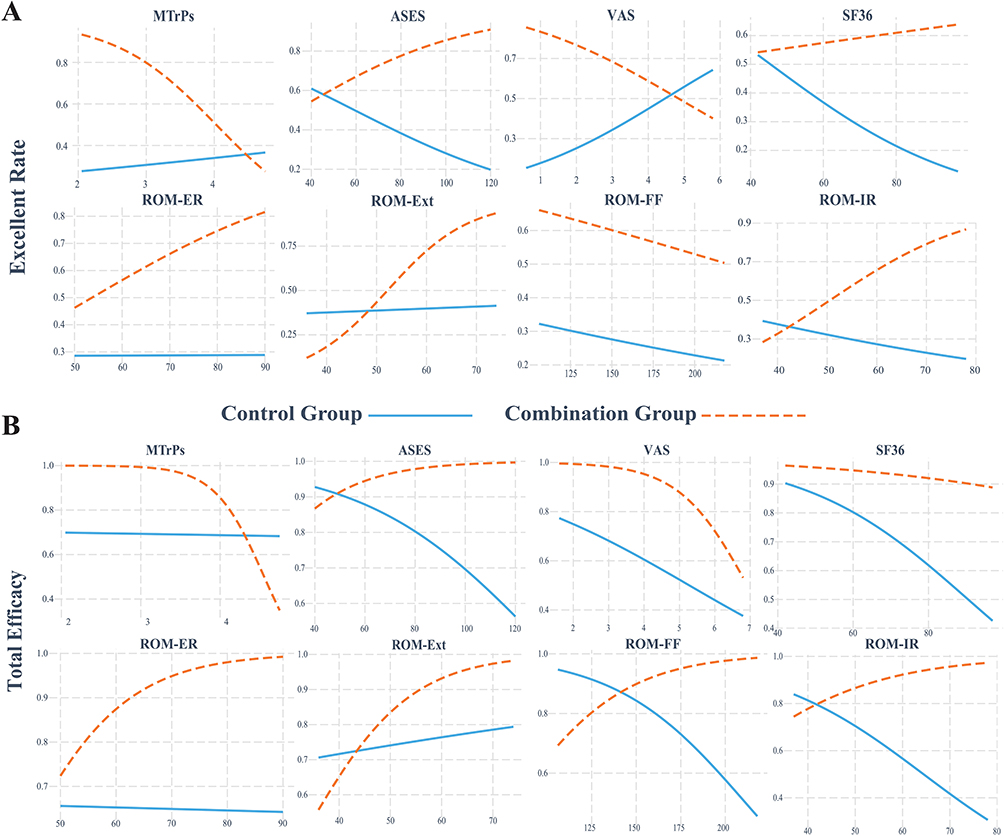 |
Figure 11 Subgroup analysis demonstrating the differential influence of specific clinical indicators on (A) the excellent efficacy rate and (B) total efficiency between the combination therapy group and the control group. |
Discussion
RCI manifests primarily manifests as shoulder pain and restricted range of motion, with early symptoms often developing insidiously as nocturnal or post-exertional pain. Without timely intervention, progression led to complications including muscular atrophy and glenohumeral instability, significantly impairing daily function. Current management focuses on three primary objectives: pain relief, adhesion release, and functional restoration. Although surgery rapidly improves mobility, its operative risks and prolonged rehabilitation,13 establish conservative approaches as valuable for mild-to-moderate cases. Rehabilitation training, particularly scapular stabilization exercises, enhances motor control, neuromuscular coordination, and strength,14 thereby improving function and promoting tissue repair. Systematic scapular training demonstrably increases active ROM and optimizes outcomes,15,16 yet its limitations include extended treatment duration and efficacy plateaus.16 Consequently, developing safer and more efficient integrated strategies is crucial for improving patients’ quality of life. This study suggests that integrating Canggui Tanxue acupuncture with SST yields higher overall efficacy compared to exercise monotherapy (P < 0.05), indicating enhanced tissue repair and superior therapeutic outcomes. Superior ASES scores (P < 0.001) confirmed significant functional improvement, likely attributable to synergistic mechanisms: SST corrects shoulder joint rhythm imbalances and enhances scapulothoracic stability, while acupuncture precisely targets pathological lesions through its unique acupuncture technique. This technique expands stimulation intensity while minimizing tissue damage. Collectively, these actions reduce inflammation and optimize function.15,17,18 Critically, the combination group achieved significantly lower VAS scores and fewer active MTrPs; P < 0.001), reflecting enhanced pain modulation. This analgesic effect may stem from acupuncture interrupting nociceptive signaling and suppressing central sensitization,19 potentially via its action at key shoulder acupoints that resolve qi-blood stasis and restore meridian flow.20,21 Significantly greater improvements in all ROM parameters (internal/external rotation, anterior flexion, extension; P < 0.001) further demonstrated superior mobility restoration through dual pathways:1) SST normalizes aberrant muscle tension and coordinating contraction, and 2) acupuncture releases myofascial/sarcomere spasms. Furthermore, as noted by recent literature, restoring ROM is critical not only for arm movement but also for overall body kinematics and postural stability.22 Finally, significantly elevated SF-36 scores (P < 0.001) confirmed substantive quality-of-life enhancement and improved long-term prognosis. Notably, unlike conventional electroacupuncture studies primarily focused on pain relief, this protocol adopts a “Heaven, Human, Earth” layered penetrating needling technique. By systematically penetrating the superficial fascia (Heaven), muscular layer (Human), and periosteal region (Earth), it effectively breaks down multi-layered fascial adhesions. This multi-depth release reduces tissue stiffness, which directly optimizes scapulothoracic kinematics and restores normal gleno-humeral rhythm. This approach may be the key mechanism behind the significant improvement in joint range of motion. Importantly, our real-world retrospective findings align closely with the results of recent high-quality randomized controlled trials (RCTs) investigating multimodal acupuncture therapies. For instance, a recent RCT23 evaluating Qihuang acupuncture combined with conventional rehabilitation for post-arthroscopic rotator cuff repair similarly targeted key acupoints such as Jianyu (LI15) and Jianqian (Extra). Consistent with our data, they demonstrated that the integrative approach yielded significantly greater reductions in VAS scores, superior improvements in ROM (particularly forward flexion and abduction), and a higher total effective rate (95.2% vs. 75.6%) compared to conventional therapy alone. While their trial focused on post-surgical rehabilitation and our cohort consisted of patients undergoing conservative management for mild-to-moderate RCI, the striking consistency in functional and analgesic outcomes provides compelling cross-validation. This comparison highlights that integrating specialized, multi-directional acupuncture techniques with structured physical rehabilitation represents a robust and broadly applicable strategy across the continuum of rotator cuff pathology. Additionally, future research should further validate the differential contributions of various needling techniques (eg., electroacupuncture frequency, penetration angle) to functional recovery.
Key strengths of this study include its novel integrated approach, strategically designed to address limitations of conventional therapies by providing an optimized alternative for RCI pain and dysfunction. The multi-dimensional assessment framework systematically validated treatment effectiveness across pain relief, functional recovery, and overall efficacy domains.
Limitations include inherent experimental design constraints. First, the lack of patient and practitioner blinding may introduce bias, particularly in patient-reported outcome measures (PROMs) such as VAS and ASES. Second, treatment standardization may be affected by individual practitioner variance during acupuncture and SST. Third, due to the retrospective nature, unmeasured confounding factors (eg., patient belief in acupuncture, adherence to home exercises, and lifestyle factors) could not be fully controlled. Fourth, the study may have limited power from a sample size of 160, affecting generalizability, and a short-term follow-up (6 weeks), precluding evaluation of long-term outcomes. Future research should prioritize long-term follow-up studies, conduct comparative trials with different acupuncture protocols (eg., electroacupuncture), and focus on patient phenotyping to identify subgroups that optimize treatment outcomes.
Conclusions
This real-world cohort study demonstrates that the integration of Canggui Tanxue acupuncture with SST provides statistically and clinically superior outcomes compared to SST monotherapy, evidenced by: 1) Functional restoration (28.75% absolute increase in excellent efficacy rates, ASES Δ=11.89 points exceeding MCID); 2) Pain modulation (VAS reduction Δ1.43 points, NNT=3.48 for excellent pain relief); 3) Biomechanical improvement (ROM-extension increased by 9.74°—critical for overhead activities). The observed synergy likely stems from concurrent targeting of scapulothoracic dyskinesis (via SST) and peripheral nociceptive sensitization (via Canggui Tanxue’s multi-directional needling). These findings suggest that the combined protocol may be particularly beneficial for patients with: 1) Baseline ROM-extension ≤50° (OR=3.21 from nomogram); 2) High pain catastrophizing scores (indirect evidence from SF-36 subanalysis). The implementation of this multimodal approach offers a safe and highly effective conservative strategy for enhancing functional recovery in RCI management.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author(s).
Ethics Statement
The study was conducted in accordance with the Decla-ration of Helsinki and was approved by the Institutional Review Board of Hainan General Hospital, Hainan Medical University (Approval No. YL-2025-03).
Informed Consent Statement
The need for written informed consent was waived by the IRB be-cause: 1) Data were anonymized prior to analysis; 2) All treatments represented standard clinical practice; 3) No additional biospecimen/procedure was required.
Publication Consent Statement
We confirm that all images and materials in this manuscript are approved for publication, and all authors have read and approved the final version of the manuscript to be published.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Zhao W, Yang J, Kang Y, et al. Animal models of rotator cuff injury and repair: a systematic review. Tissue Eng Part B Rev. 2022;28(6):1258–15. doi:10.1089/ten.teb.2022.0034
2. Xu P. Effects of ultrasound-guided platelet-rich plasma combined with sodium hyaluronate on shoulder function recovery, pain degree and mental health of patients with rotator cuff injury. Biotechnol Genet Eng Rev. 2024;40(1):217–236.
3. Feuerriegel GC, Fritz B, Marth AA, Sommer S, Wieser K, Sutter R. Assessment of the rotator cuff muscles: state-of-the-art MRI and clinical implications. Radiology. 2025;315(2):e242131. doi:10.1148/radiol.242131
4. Silveira A, Luk J, Tan M, et al. move it or lose it? The effect of early active movement on clinical outcomes following rotator cuff repair: a systematic review with meta-analysis. J Orthopaed Sports Phys Ther. 2021;51(7):331–344. doi:10.2519/jospt.2021.9634
5. Powell JK, Lewis JS. Rotator cuff-related shoulder pain: is it time to reframe the advice, “you need to strengthen your shoulder”? J Orthopaed Sports Phys Ther. 2021;51(4):156–158. doi:10.2519/jospt.2021.10199
6. Li C, Qi X, Wang F, Wang J. Clinical efficacy of acupuncture with Canggui Tanxue technique on huantiao point for treating sciatica caused by lumbar disc herniation. Alternative Therap Health Med. 2023;29(7):376–381.
7. Xu CC, Li XH, Li JL. Comparative study on curative effect and recurrence rate of chronic scapulohumeral periarthritis treated with different acupuncture techniques. Zhen Ci Yan Jiu. 2024;49(2):164–170. doi:10.13702/j.1000-0607.20221004
8. Hill BW, Joyce CD, Singh A, Guttman MJ, Williams GR, Namdari S. Patients with mild osteoarthritis are less likely to achieve a clinically important improvement in pain or function after anatomic total shoulder arthroplasty. Clin Orthopaedics Related Res. 2023;481(8):1464–1470. doi:10.1097/CORR.0000000000002609
9. Goudman L, Pilitsis JG, Billet B, et al. The level of agreement between the numerical rating scale and visual analogue scale for assessing pain intensity in adults with chronic pain. Anaesthesia. 2024;79(2):128–138. doi:10.1111/anae.16151
10. Kobylarz MD, Klich S, Sánchez-Jorge S, Buffet-García J, Ortega-Santiago R, Valera-Calero JA. Shear-Wave elastography supports that muscle stiffness should NOT be considered a criterion to determine the presence of myofascial trigger points in the infraspinatus muscle. Am J Phys Med Rehabil. 2025;104:890–895. doi:10.1097/PHM.0000000000002721
11. Hanks J, Myers B. Validity, reliability, and efficiency of a standard goniometer, medical inclinometer, and builder’s inclinometer. Int J Sports Phys Ther. 2023;18(4):989–996. doi:10.26603/001c.83944
12. Moosmayer S, Lund G, Seljom US, et al. Fifteen-year results of a comparative analysis of tendon repair versus physiotherapy for small-to-medium-sized rotator cuff tears: a concise follow-up of previous reports. J Bone Hoint Surg Am. 2024;106(19):1785–1796.
13. Bedi A, Bishop J, Keener J, et al. Rotator cuff tears. Nat Rev Dis Primers. 2024;10(1):8. doi:10.1038/s41572-024-00492-3
14. Liaghat B, Skou ST, Søndergaard J, Boyle E, Søgaard K, Juul-Kristensen B. Short-term effectiveness of high-load compared with low-load strengthening exercise on self-reported function in patients with hypermobile shoulders: a randomised controlled trial. Br J Sports Med. 2022;56(22):1269–1276. doi:10.1136/bjsports-2021-105223
15. Sun JN, Zheng QY, Wang RS, Ma YR, Chen P. An additional rehabilitation program to improve postoperative outcomes in patients with rotator cuff tear and scapular dyskinesis: a propensity score-matched study. BMC Musculoskelet Disorders. 2025;26(1):338. doi:10.1186/s12891-025-08596-x
16. Yuksel E, Yesilyaprak SS. Scapular stabilization exercise training improves treatment effectiveness on shoulder pain, scapular dyskinesis, muscle strength, and function in patients with subacromial pain syndrome: a randomized controlled trial. J Bodywork Movement Therap. 2024;37:101–108. doi:10.1016/j.jbmt.2023.11.005
17. Manceron A, Jawa A, Mantovani M, Werthel JD. Involvement of the scapulothoracic articulation after well-functioning reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2025;34:2258–2268. doi:10.1016/j.jse.2024.12.018
18. Xie J, Li J, Sun Q, Jiang J. Multidimensional evaluation of the clinical efficacy and potential mechanisms of acupuncture combined with rehabilitation training in the treatment of stroke: a study based on multiple evaluation indicators. Front Neurol. 2025;16:1573073. doi:10.3389/fneur.2025.1573073
19. Liu Y, Jin F, Zhou L, et al. Platelet-derived growth factor receptor-α induces contraction knots and inflammatory pain-like behavior in a rat model of myofascial trigger points. Anesthesiology. 2024;141(5):929–945. doi:10.1097/ALN.0000000000005167
20. Xiong J, Zhou X, Luo X, et al. Acupuncture therapy on myofascial pain syndrome: a systematic review and meta-analysis. Front Neurol. 2024;15:1374542. doi:10.3389/fneur.2024.1374542
21. Liu S. Chronic supraspinatus tendonitis pain: an integrative approach for treatment with cross-fiber massage, electroacupuncture, far-infrared heat, and photobiomodulation. Med Acupuncture. 2022;34(4):251–255. doi:10.1089/acu.2022.0041
22. Ata AM, Tuncer B, Kara O, Başkan B. The relationship between kinesiophobia, balance, and upper extremity functions in patients with painful shoulder pathology. Pm r. 2024;16(10):1088–1094. doi:10.1002/pmrj.13145
23. Sun Q, Xu Z, Yu J, et al. [Qihuang acupuncture therapy for mid-term postoperative pain after arthroscopic rotator cuff repair: a randomized controlled trial]. Zhongguo Zhen Jiu. 2026;46(3):341–346. doi:10.13703/j.0255-2930.20250217-0006 Dutch
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.