Back to Journals » Nature and Science of Sleep » Volume 17

Comparative Effects of Two Acupuncture Protocols in the Management of Chronic Insomnia: A Randomized Controlled Trial
Authors Li L, Xia M ![]() , Chen X, Wang F, Li J
, Chen X, Wang F, Li J ![]() , Zhao N, Liu Z, Chen Y
, Zhao N, Liu Z, Chen Y
Received 3 April 2025
Accepted for publication 23 June 2025
Published 7 August 2025 Volume 2025:17 Pages 1789—1803
DOI https://doi.org/10.2147/NSS.S521578
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Marco Veneruso
Lianbo Li,1,* Mingyue Xia,1,* Xinyu Chen,2,* Fengxiao Wang,1 Jie Li,1 Na Zhao,1 Zhen Liu,1 Yunfei Chen1
1Department of Acupuncture and Moxibustion, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Macau University of Science and Technology, Macau, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunfei Chen, Department of Acupuncture and Moxibustion, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China, Tel/Fax +86-21-65162628, Email [email protected] Zhen Liu, Department of Acupuncture and Moxibustion, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China, Tel/Fax +86-21-65162628, Email [email protected]
Background: Chronic Insomnia Disorder (CID) significantly impairs both sleep quality and daytime functioning. However, current treatments have limited efficacy in improving daytime function and are often associated with side effects. This highlights the urgent need for effective and safe therapeutic approaches that can target both nocturnal and daytime symptoms.
Objective: To evaluate the clinical efficacy and safety of acupuncture in improving sleep quality and daytime functioning in patients with chronic insomnia, and to optimize its treatment protocol.
Methods: This study was a single-blind, randomised, controlled trial. The treatment group received acupuncture at HT7, BL15, LR3 and BL18, while the control group was treated at GV20, EX-HN22, BL62 and KI6. Each group underwent 10 sessions administered three times per week. The Insomnia Severity Index (ISI) served as the primary evaluation index for sleep efficacy, while the Pittsburgh Sleep Quality Index (PSQI) and polysomnography (PSG) were secondary indexes for sleep quality. The Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), Fatigue Severity Scale (FSS), and Epworth Sleepiness Scale (ESS) were used to evaluate daytime functional impairment.
Results: Totally 76 patients were included in this study and randomly assigned to the treatment group (n=38) and the control group (n=38). Both groups showed significant improvements in sleep quality and daytime functioning. The treatment group exhibited a mean ISI reduction of 7.58 points versus 5.71 points in the control group; however, this difference was not statistically significant. PSG data revealed similar improvements in total sleep time, sleep efficiency, and REM sleep percentage across groups. Notably, the treatment group demonstrated significantly greater reductions in BAI and BDI scores (p< 0.05), while improvements in FSS and ESS scores were comparable.
Conclusion: Acupuncture is an effective and safe treatment to improve sleep as well as daytime functioning for chronic insomnia. The protocol using HT7, BL15, LR3 and BL18 may offer added benefits for reducing anxiety and depressive symptoms.
Clinical Trial Registration: This study was registered with the China Clinical Trial Registry (CCTR), registration ID: ChiCTR2200066102.
Plain Language Summary: Chronic Insomnia Disorder (CID) significantly impairs sleep quality and daytime functioning, leading to fatigue and mood disturbances, and poses a major public health challenge. Current treatments face limitations in accessibility and may cause side effects. This highlights the need for safe, effective, and accessible therapies that address both nocturnal and daytime symptoms.
This study introduces an optimized acupuncture protocol targeting the heart and liver through the Heart-Liver Shu-Yuan acupoint combination. Unlike previous studies that focused primarily on sleep quality, this research evaluates both nocturnal sleep and daytime functioning, addressing emotional and cognitive disturbances often overlooked in CID management.
The findings of this RCT have important clinical implications, offering evidence for a personalized, efficient acupuncture approach that improves both sleep and daytime symptoms. This could inform more comprehensive treatment guidelines for CID and promote the integration of acupuncture into standard care practices.
Keywords: acupuncture, chronic insomnia, daytime function, randomised controlled trial
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zhou has been published for this article.
Introduction
Chronic insomnia disorder (CID) is characterized by difficulty falling or staying asleep for over three months despite adequate opportunity to sleep, leading to daytime dysfunction.1 CID is the most common sleep disorder,2 affecting approximately 10% of the global population and nearly 19.6% of adults in China.1,3 Beyond disrupted sleep, patients with CID often suffer from impaired daytime functioning—such as fatigue, mood disturbances,4,5 which significantly reduce quality of life and are the main reason patients seek treatment.6,7 Improving daytime functioning is therefore a key therapeutic goal.2 Furthermore, CID is associated with serious comorbidities, including cardiovascular disease,8 cognitive and mood disorders,9 metabolic disturbances and even life-threatening conditions,10 making it a major public health concern.
Clinical treatments for CID primarily include pharmacological and non-pharmacological approaches. Cognitive behavioral therapy for insomnia (CBTi) is an effective first-line treatment for CID.11,12 However, its application is often hindered by resource constraints.13 In addition, pharmacological interventions may provide short-term relief,11 but these medications are linked to side effects like hangover effect,14 cognitive impairment,15 tolerance, dependence,16 leading to their restricted use. As many patients do not fully benefit from existing therapies, there is a pressing need to explore safe and effective complementary and alternative treatments.
Acupuncture, a distinctive therapy in traditional Chinese medicine, has been incorporated in recent Chinese Insomnia Diagnosis and Treatment Guidelines.17 Meta-analysis suggest that acupuncture can decrease Pittsburgh Sleep Quality Index(PSQI) scores, increases total sleep time (TST) and sleep efficiency (SE),which is recognized for its natural, low-risk, and holistic approach.18,19 Our previous studies have confirmed its safety and efficacy for chronic insomnia.20,21 However, the role of acupuncture in improving daytime function in CID remains insufficiently studied. A precise acupoint strategy targeting both sleep and daytime symptoms may offer better clinical outcomes.
Traditional Chinese medicine (TCM) theory posits that the heart governs the mind and that the liver regulates emotions, both closely linked to insomnia.22,23 Liver-Fire Disturbing the Heart Syndrome (LHS), one of the common TCM patterns in insomnia,24 is often associated with mood disorders.25 Acupuncture points are thought to regulate internal organs by linking them with meridians.26 This study used the Heart-Liver Shu-Yuan acupoint combination (BL15, BL18, HT7, LR3) to regulate heart-liver imbalance, while the control group received commonly used CID-related points (GV20, BL62, KI6, EX-HN22),27 in order to enhance the therapeutic efficacy of TCM.
We hypothesize that acupuncture can improve both sleep quality and daytime function in patients with CID. This RCT evaluates its efficacy in CID with LHS, aiming to clarify the rationale for specific acupoint combinations and to develop more effective and generalizable treatment protocols.
Methods
Study Design
This study was a randomised, single-blind, single-centre controlled trial, all patients were randomly allocated in a 1:1 ratio into two parallel groups: the treatment group and the control group. The study was conducted in accordance with the CONSORT guidelines28 and the Guidelines for Reporting Standards for Interventions in Acupuncture Clinical Trials.29 Ethical approval was granted by the Ethics Committee of Yueyang Hospital of Integrative Medicine, Shanghai University of Traditional Chinese Medicine (Ethics Review Approval No. 2022–084). The trial was registered with the Chinese Clinical Trial Registry (ChiCTR) under registration number ChiCTR2200066102. The study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to their inclusion in the study.
Participants
The participants in this study were primarily individuals diagnosed with CID who attended the outpatient clinic of the Department of Acupuncture and Moxibustion at Yueyang Hospital of Integrative Medicine, Shanghai University of Traditional Chinese Medicine from November 2022 to May 2023. In addition, the subjects were also recruited through WeChat campaigns, scientific lectures, charity clinics, and recruitment advertisements. Participation was voluntary, and prior to enrollment, all subjects underwent an initial clinical interview, either by telephone or in person, to assess eligibility and obtain informed consent.
The diagnostic criteria for chronic insomnia were based on the Chronic Insomnia Disorder criteria outlined in the ICSD-3, developed by the American Academy of Sleep Medicine(AASM) in 2014.30 Based on prior research,20,31 inclusion criteria were as follows: (1) age between 18 and 65 years, with no gender restrictions; (2) meeting the diagnostic criteria for CID according to ICSD-3; (3) diagnosis of insomnia according to TCM criteria, specifically with the TCM syndrome pattern of liver-fire disturbing the heart; (4) stable use of sedative sleep aids for at least 3 months, or no medication use prior to study enrollment; (5) Insomnia Severity Index (ISI) >7;32 (6) patients volunteered to participate in the study and signed an informed consent form.
To confirm that participants met the inclusion criteria, an experienced clinician conducted a semi-structured interview with each subject expressing interest in participation prior to enrollment. The interview questionnaire assessed factors such as the reasons for insomnia, primary symptoms, frequency, daytime functioning, current treatments, sleep-related habits, and the history of physical or mental health conditions. Additionally, all potential participants were required to complete a 7-day sleep diary before the clinical interview to provide insights into their sleep patterns.
Exclusion criteria included (1) patients with infectious diseases; (2) patients with severe cardiac, hepatic, renal, hematological, respiratory, or psychiatric disorders; (3) patients with severe digestive disorders or malnutrition; (4) individuals with untreated sleep disorders other than chronic insomnia disorder, such as obstructive sleep apnea, narcolepsy, restless legs syndrome, periodic limb movement disorder, delayed sleep phase syndrome, or central apnea syndrome; (5) pregnant or breastfeeding women; (6) patients with severe trauma, conditions unsuitable for acupuncture, or severe skin diseases/allergies; (7) scores of ≥25 on the Beck Depression Inventory (21-item version) in the past 3 months; (8) individuals who have participated in other clinical trials within the last 3 months.
To ensure the inclusion of clinically significant insomnia patients and broader generalizability, the inclusion criteria were modified based on clinical trial registration, changing the requirement from PSQI > 5 to ISI > 7.33 The exclusion criterion pertaining to PSG was eliminated since PSG was not conducted for every participant. As a substitute, clinical interviews were employed to identify other sleep disorders, guaranteeing a more feasible and clinically pertinent method. This modification still falls within the originally registered eligibility scope and does not deviate from the intended study cohort.
Intervention
All acupuncture operators were qualified TCM practitioners with intermediate-level (attending physician) or higher certification in acupuncture and at least 3 years of clinical experience. Before the study began, they underwent 3 days of specialized training on point selection and standard acupuncture procedures.
Treatment Group
Subjects in the treatment group were positioned prone and received acupuncture at Xinshu (BL15), Ganshu (BL18), Shenmen (HT7), and Taichong (LR3), as illustrated in Figure 1. These acupoints were selected to regulate the imbalance between the heart and liver, in accordance with classical Chinese medicine theory. The precise locations of the points were determined based on the national standard Nomenclature and Location of Meridian Points (GB/T 12346–2021) issued by the People’s Republic of China in 2021.33
 |
Figure 1 Acupoints for the acupuncture in Treatment group. (A) HT7; (B) LR3; (C) BL15 (above) and BL18 (below). |
Routine disinfection was performed with 75% alcohol cotton balls, and single-use sterile acupuncture needles (0.25 mm × 40 mm; Andy, Guizhou, China; 20182270011) were used. Needling depth and angle were adjusted based on adipose tissue thickness and anatomical structures at each acupoint. For HT7, needles were inserted perpendicularly to 7.5mm–12.5 mm, avoiding the ulnar artery and vein. For BL15 and BL18, needles were inserted obliquely toward the spine to 12.5mm–25 mm, and for LR3, perpendicularly to 12.5mm–25 mm. Needle manipulation was performed to elicit deqi sensations (soreness, numbness, heaviness, distension, or sinking), after which needles were retained for 20 minutes.
Control Group
The subjects were placed in the supine position, and acupuncture was administered using a routine acupoint combination, including Baihui (GV20), bilateral Shenmai (BL62), bilateral Zhaohai (KI6), and bilateral Anmian (EX-HN22), as illustrated in Figure 2. The prescription was based on the primary acupuncture points for insomnia outlined in the textbook, Acupuncture and Tuina Therapy,34 as well as commonly used high-frequency clinical points.35 Acupoint localization followed the national standard “ Nomenclature and location of meridian points” (GB/T12346-2021).33
 |
Figure 2 Acupoints for the acupuncture in Control group. (A) GV20; (B) EX-HN22; (C) KI6; (D) BL62. |
Routine disinfection was performed with 75% alcohol cotton balls, followed by the insertion of single-use sterile acupuncture needles (0.25 mm × 40 mm; Andy, Guizhou, China; 20182270011). For GV20, needles were inserted obliquely to a depth of 7.5mm–12.5 mm; for EX-HN22, perpendicularly to 12.5mm–25 mm; and for BL62 and KI6, perpendicularly to 2.5mm–7.5 mm. Needling depth and angle were adjusted according to adipose tissue thickness and the anatomical structures of each acupoint. After insertion, manipulation techniques, including twisting, lifting, and thrusting, were applied to elicit deqi sensations (soreness, numbness, heaviness, distension, or sinking). Needles were retained for 20 minutes after deqi was achieved.
Subjects in both groups were treated once in the afternoon on Tuesdays, Thursdays, and Saturdays for 20 minutes each for 10 consecutive sessions. All subjects were treated equally to prevent sensory differences in patients; patients were placed in different rooms or at different times of day to avoid communication between patients.
Measures
Primary Outcome Measures
The primary efficacy indicator in this study was the Insomnia Severity Index (ISI) score. The ISI is a self-assessment scale consisting of seven items that evaluate the severity of insomnia, sleep onset and maintenance difficulties, early morning awakening, daytime functioning, and mood disturbances over the past two weeks.32 It is commonly used for screening and assessing the clinical efficacy of insomnia treatments. The total score ranges from 0 to 28, with a score of 14 or higher indicating clinically significant insomnia. A reduction of 6 or more points on the ISI indicates significant clinical improvement.36
Secondary Outcome Measures
The Pittsburgh Sleep Quality Index (PSQI): PSQI was used as supplemental information to assess nighttime sleep quality and daytime functioning.37 The PSQI evaluates sleep over the past month, with a total score ranging from 0 to 21. A PSQI score greater than 5 indicates poor sleep quality and is considered clinically significant.38
Polysomnographic monitoring (PSG): PSG was utilized to assess objective improvements in insomnia before and after acupuncture treatment. The primary efficacy index in this study was EEG data from PSG (NIHON KOHDEN, Nippon Kohden, Japan Photonics Corporation), including total sleep time (TST), sleep efficiency (SE), sleep onset latency (SOL), wake after sleep onset (WASO), arousal index (ArI), and the percentages of N1, N2, and N3 sleep (N1%, N2%, N3%) as well as REM sleep (REM%). Subjects underwent PSG monitoring once before and once after treatment, from their usual bedtime to the following morning, with a total recording duration of 8 hours. Measurements were conducted in accordance with the guidelines in the Manual for the Scoring of Sleep and Associated Events: Rules, Terminology, and Technical Specifications (version 3.0) by the American Academy of Sleep Medicine.39
Beck Anxiety Inventory (BAI): The BAI scale was used to assess the anxiety levels of subjects. In clinical practice, a total score of 45 or higher is typically used as the threshold for identifying clinically significant anxiety.40
Beck Depression Inventory (BDI): The BDI scale was used to assess the depressive state of subjects. Developed by Beck, it is based on the diagnostic criteria for depression outlined in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).41 The scoring is as follows: 0–13 indicates no depression, 14–19 indicates mild depression, 20–28 indicates moderate depression, and 29–63 indicates severe depression.
Fatigue Severity Scale (FSS): FSS is used to assess daytime fatigue in patients before and after treatment.42 Studies have shown that a score above 5.5 on the FSS indicates a high prevalence of daytime fatigue in insomnia patients.43
Epworth Sleepiness Scale (ESS): is used to assess the severity of daytime sleepiness in patients before and after treatment. It is internationally recognized as a concise tool for measuring sleepiness.44 The ESS has a total score of 24, with higher scores indicating greater daytime sleepiness.
The above scales are all validated in Chinese, demonstrating good reliability and validity for research applications.45–50 During the screening period, subjects were assessed using these scales at baseline, after completing 10 acupuncture treatments (post-treatment), and during follow-up at 2 weeks and 4 weeks after treatment completion.
All PSG scores and questionnaires will be assessed by an experienced PSG technician who is blinded to group assignment. Pre-study training will be provided to data collection assessors to enhance subject compliance, ensure high-quality and complete data collection, and facilitate follow-up. Data entry will be carried out by a dedicated staff member who will receive specialized training in data entry, coding, and secure data storage.
Safety Assessments
In this study, the occurrence of adverse events such as pneumothorax, needle fainting, needle stagnation, bleeding, and subcutaneous hematoma was monitored and recorded during each needling intervention. All adverse events were reported to the chief study manager, who assessed whether they were related to the intervention. A Serious Adverse Event (SAE) recording form was used to document any major adverse events that occurred during the clinical study.
Sample Size
The required sample size was estimated based on the primary outcome ISI. Based on our team’s previous study,21 the control group had an ISI of 21.73 ± 4.14. It was hypothesized that acupuncture treatment targeting the treatment group would reduce the ISI by an additional 4.60 points compared to the conventional treatment group. The cut-off value for the test of superiority was set at 1.4, with α = 0.025 for a one-sided test and 1 - β = 0.85. Using the formula for calculating the sample size for a superiority test, the required sample size was determined as follows:
Using the values above, the sample size was calculated to be 30 cases per group. Accounting for a 20% dropout rate, the required sample size per group was 38, resulting in a total of 76 subjects across both groups.
Randomization and Blinding
The statistical commissioner used SPSS 26.0 to generate a random number table with 76 numbers. These numbers were then rearranged in ascending order, with numbers 1–38 assigned to the treatment group and numbers 39–76 assigned to the control group. The random number table was reproducible (random seed: 20220620). Independent research assistants randomly allocated subjects to either the treatment or control group in a 1:1 ratio.
All patients were blinded to their group assignment. Both the treatment and control groups received real acupuncture that elicited the typical “de qi” sensation. The main difference between the two groups lay in the specific acupoints used; however, participants were unaware of which acupoint combination corresponded to the treatment or control group, thereby achieving participant blinding.
Each patient’s corresponding random number and treatment protocol were printed on a card, placed in an opaque envelope by an independent research assistant, and then given to the acupuncturist. The acupuncturist administered the treatment according to the protocol on the card, ensuring the treatment process was identical in both groups. Throughout the study, the generation of the randomization list, subject recruitment, acupuncture treatment, outcome assessment, follow-up, data entry, and statistical analysis were all conducted independently by different investigators, none of whom were aware of the group assignments.
Statistical Analysis
Statistical analyses were conducted using SPSS 26.0 software with two-sided tests, where p < 0.05 was considered statistically significant. To ensure accuracy, all data were independently entered twice by two researchers.
Measurement Data: Data that conformed to a normal distribution were expressed as mean ± standard deviation ( ) to describe the central tendency and variability. Comparisons between two groups were made using independent samples t-tests, while comparisons at multiple time points were performed using repeated measures analysis combined with multivariate analysis of variance (ANOVA). For data that did not conform to a normal distribution, results were presented as median (M) and interquartile range (IQR, Q1-Q3). Comparisons between two groups were conducted using the Mann–Whitney U-test or Wilcoxon signed-rank test, and comparisons among multiple groups were made using the Friedman test.
) to describe the central tendency and variability. Comparisons between two groups were made using independent samples t-tests, while comparisons at multiple time points were performed using repeated measures analysis combined with multivariate analysis of variance (ANOVA). For data that did not conform to a normal distribution, results were presented as median (M) and interquartile range (IQR, Q1-Q3). Comparisons between two groups were conducted using the Mann–Whitney U-test or Wilcoxon signed-rank test, and comparisons among multiple groups were made using the Friedman test.
Count Data: Frequency and proportion (constitutive rate) were used to describe categorical data. The chi-square (χ²) test was used for comparisons between groups when the analyzed variables were dichotomous or multicategorical unordered data. The Mann–Whitney U-test was applied for comparisons between groups when the analyzed variables were rank-ordered count data.
Results
Participants Characteristics
A total of 157 subjects were recruited for this study, of whom 81 were excluded during screening. The remaining 76 participants were randomly assigned to either the treatment group (n = 38) or the control group (n = 38) to complete the full treatment and follow-up (Figure 3).
 |
Figure 3 Trial flow diagram. |
Table 1 presents the demographic characteristics of the participants. Except for educational level, no statistically significant differences were found between the baseline characteristics of the two groups (P > 0.05), indicating that the baseline clinical characteristics were balanced and comparable.
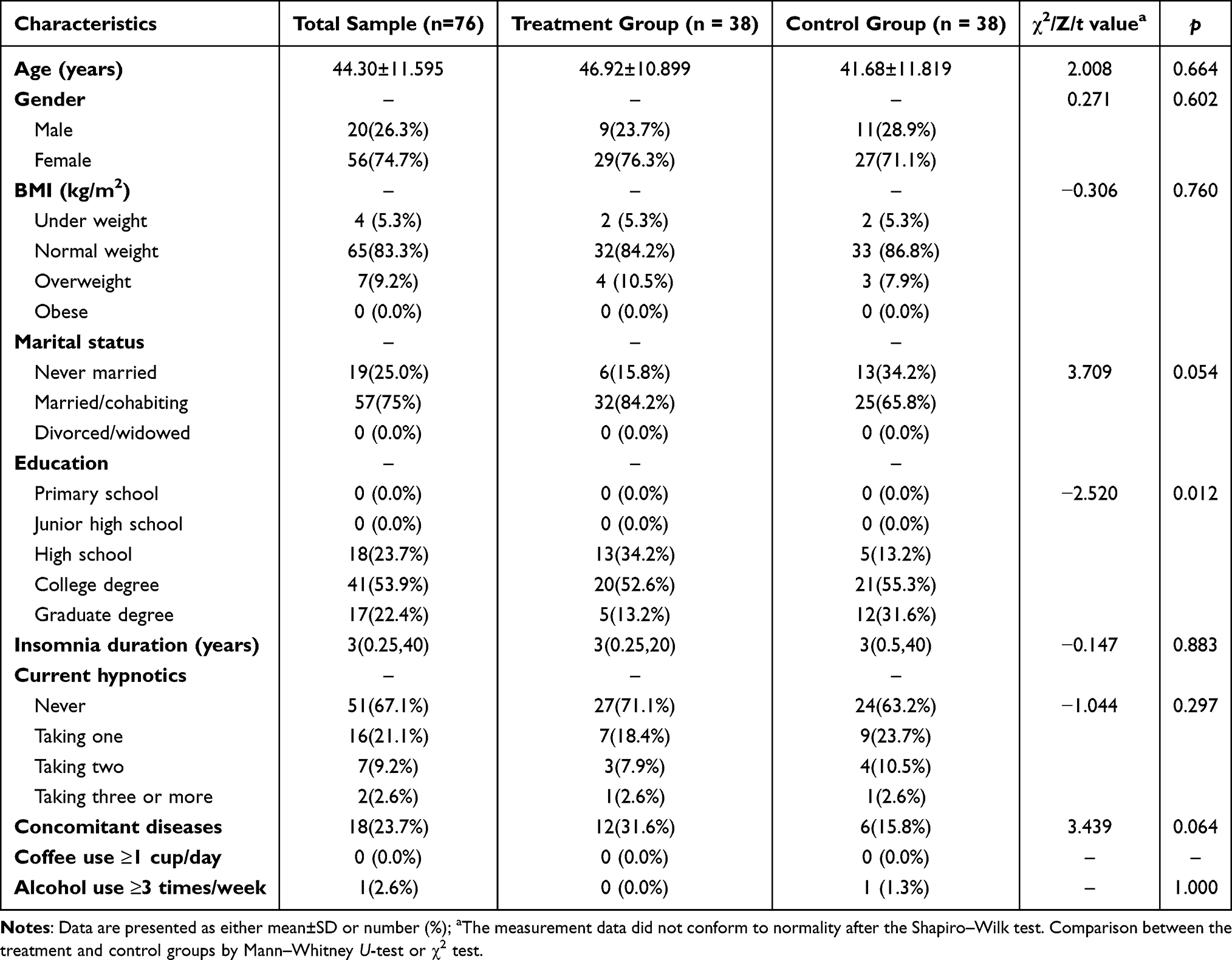 |
Table 1 Baseline Characteristics of Participants |
Participant-Reported Sleep Assessments
The changes in ISI and PSQI scores are demonstrated in Table 2 and Figure 4. Compared with the pre-treatment period, the ISI score in the treatment group decreased from 18.29 to 10.71, and the PSQI score decreased from 12.66 to 7.42, both showing statistically significant differences (P < 0.05). In the control group, the ISI score decreased from 17.74 to 12.03, and the PSQI score decreased from 12.29 to 8.45, also with statistically significant differences (P < 0.05). After treatment and during follow-up, the ISI and PSQI scores in the treatment group remained lower than those in the control group, although the difference between the two groups was not statistically significant.
 |
Table 2 Participant-Reported Sleep Assessments from Baseline to 4-week Follow-Up |
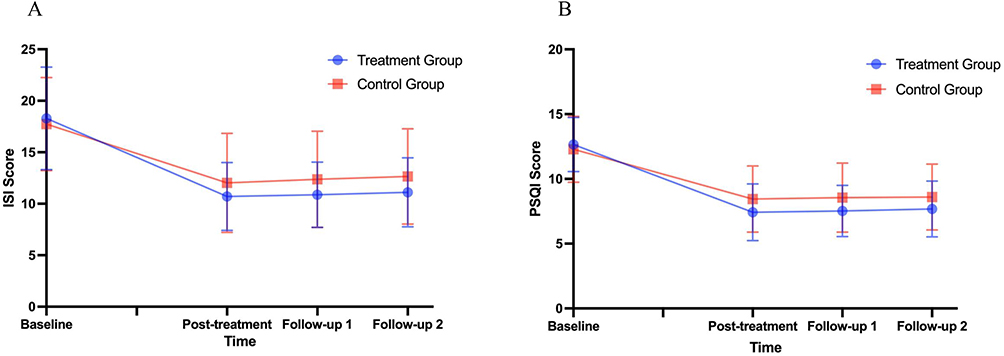 |
Figure 4 Mean ISI and PSQI scores of two groups from baseline to 4-week Follow-Up. (A) Changes in ISI scores from baseline to 4-week follow-up; (B) Changes in PSQI scores from baseline to 4-week follow-up. Abbreviations: PSQI, Pittsburgh sleep quality index; ISI, insomnia severity index. Notes: Data were analyzed using a mixed-effect model for repeated measures (MMRM). |
Secondary Outcome
PSG Assessments
The results of PSG measurements are presented in Table 3. In the treatment group, TST, SE, REM-SL, and REM% showed statistically significant improvements compared to pre-treatment (P < 0.05). Similarly, in the control group, TST, SE, and REM% demonstrated statistically significant improvements (P < 0.05). However, the intergroup comparisons of pre-treatment and post-treatment data revealed no statistically significant differences between the two groups (P > 0.05).
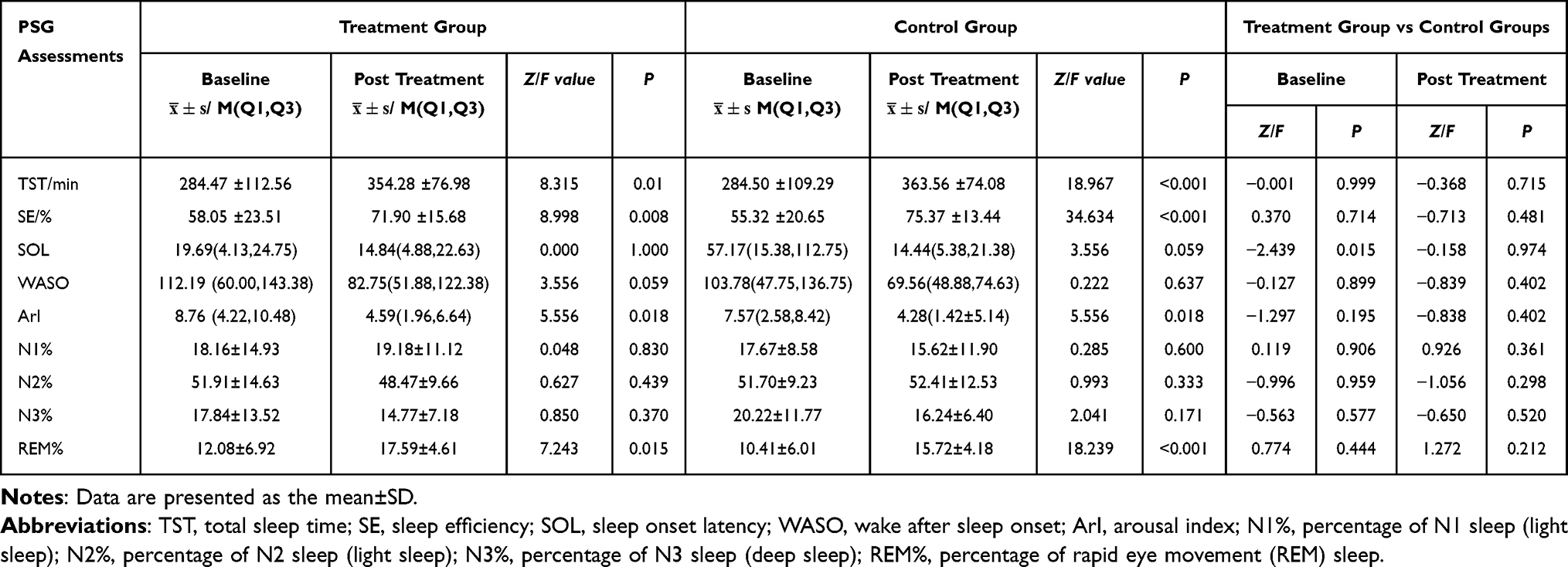 |
Table 3 PSG Sleep Assessments |
Daytime Function Assessments
The results of the daytime functional assessment are shown in Table 4 and Figure 5. Compared with the pre-treatment period, the BAI, BDI, FSS, and ESS scores in the treatment group decreased significantly, with statistically significant differences (P < 0.001). Similarly, in the control group, the BAI, BDI, FSS, and ESS scores also decreased significantly (P < 0.001). After treatment, there was a statistically significant difference between the two groups for the BDI and BAI scores (P < 0.05). However, at the 2-week and 4-week follow-ups, no statistically significant differences were observed between the two groups.
 |
Table 4 Daytime Function Measurements from Baseline to 4-week Follow-Up |
 |
Figure 5 Mean Daytime Function scores of two groups from baseline to 4-week Follow-Up. (A) Changes in BAI scores from baseline to 4-week follow-up; (B) Changes in BDI scores from baseline to 4-week follow-up; (C) Changes in ESS scores from baseline to 4-week follow-up; (D) Changes in FSS scores from baseline to 4-week follow-up. Abbreviations: BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; ESS, Epworth Sleepiness Scale; FSS, Fatigue Severity Scale. Notes: Data were analyzed using a mixed-effect model for repeated measures (MMRM); *P<0.05 vs control treatment group. |
Safety Assessment
During the study, three subjects experienced localized spot bleeding from the needles after acupuncture, which lasted no longer than one minute and caused no other discomfort. No acupuncture-related adverse events were reported during the study period.
Discussion
Although the previous RCTs have shown that acupuncture improves nocturnal sleep in insomnia, they have not adequately addressed the impact on daytime functioning in individuals.51 Acupoint selection plays a crucial role in treatment outcomes, yet previous acupoint combinations have shown limited efficacy in improving daytime functions and often lack alignment with TCM syndrome differentiation principles. This discrepancy is not consistent with clinical practice. Therefore, this study aims to explore the efficacy of two acupuncture point selection schemes—Heart-Liver Shu-Yuan acupoint combination and classical point combinations—on sleep quality and daytime functioning in patients with chronic insomnia, with the goal of harnessing the synergistic and specific effects of acupoints.
After treatment, the ISI scores decreased by 7.58 points in the treatment group and 5.71 points in the control group. Although no statistically significant differences were observed between groups at any time point, the reduction in ISI in the treatment group exceeded the 6-point threshold considered clinically meaningful improvement in insomnia severity,36 and this improvement was maintained at the 1-month follow-up. PSQI scores decreased by 5.24 points in the treatment group and by 3.84 points in the control group after treatment, both groups achieved changes exceeding the 3-point threshold considered clinically meaningful improvement in sleep quality.52 The magnitude of PSQI improvement was greater in the treatment group than in the control group; however, between-group differences did not reach statistical significance. This indicates that both acupuncture methods can effectively reduce the severity of insomnia and improve subjective sleep quality.
The acupoints for the treatment group were selected based on the heart-liver pattern. According to the literature, liver-fire disturbing the heart is a common type of insomnia.53 The heart governs mental activities and is a primary site of insomnia, while the liver plays a crucial role in emotional regulation. The dorsal points, located along the first lateral line of the Bladder Meridian, are near their corresponding internal organs, offering a localized therapeutic effect. Yuan-source points are traditionally used to address disorders of the five major organs (heart, liver, spleen, lungs, and kidneys). The combination of these four acupoints targeting the heart and liver works synergistically to regulate organ function, restore harmony, and enhance therapeutic outcomes, ultimately improving sleep quality.54 The results of the current study provide evidence supporting the clinical efficacy of the Shu-Yuan pairing points in improving subjective sleep quality.
The control group received a commonly used acupoint combination for insomnia, including GV20 (Baihui), BL62 (Shenmai), KI6 (Zhaohai), and EX-HN22 (Anmian). GV20, on the Governor Vessel, calms shen and alleviates mental restlessness via its connection to the brain. KI6 and BL62, master points of the Yin and Yang Heel Vessels, help rebalance the sleep–wake cycle by harmonizing yin and yang. EX-HN22, an empirical point for insomnia, further stabilizes shen and supports sleep onset. The control group’s acupuncture points were similar to those of the other teams. For example, Yin et al achieved a 3.7-point decrease in ISI scores after 12 treatments and a 6.2-point decrease in PSQI scores after 24 treatments.52,55 Jiang et al achieved a 5-point decrease in PSQI scores after using similar acupoint combinations.56 The present study reconfirmed the effectiveness of these acupoints in improving sleep quality. Although the treatment group showed a greater reduction in insomnia symptoms than the control group, the between-group differences were not statistically significant, possibly due to the use of active acupuncture in both groups, which was performed consistently except for the different selection of acupoints.
In terms of daytime functioning, the results of the current study indicated that after treatment, both groups showed improvement, but significant differences were observed in the BAI and BDI scores between the two groups. This suggests that the personalized acupuncture protocol had a greater effect on reducing anxiety and depression in patients with liver-fire disturbing the heart. This is consistent with the TCM theory of dispelling liver-fire, calming the heart, and regulating mood. A meta-analysis of 11 non-pharmacological interventions indicated that acupuncture was more effective in improving both sleep quality and alleviating depression compared to other therapies.57
This study used PSG as an objective efficacy index, which is internationally recognized as a method used to objectively assess sleep structure.58 The results showed a significant increase in TST for both groups, which was beneficial for improving daytime mood.59 Additionally, REM% increased and sleep duration was prolonged after treatment. REM sleep processes significantly influence mood in insomnia patients, and higher REM sleep and lower REM% are closely linked to worsening anxiety and depression.60,61 These results suggest that acupuncture improves sleep structure, which in turn improves daytime mood. Both acupuncture protocols resulted in increased TST, improved sleep efficiency, and prolonged REM%, aligning with findings from previous studies.20,21,55,62 However, the difference between the groups was not statistically significant, likely because both groups received true acupuncture, which explains the improvement in subjective sleep quality observed in both groups.
Acupoint selection is a key determinant of acupuncture’s therapeutic efficacy. However, the acupoints used in these studies varied.63 The lack of standardized acupoint selection leads to challenges for acupuncturists and hinders the reproducibility and comparison of experimental results.64 This situation poses a significant obstacle to the advancement of both clinical and scientific research in acupuncture. Moreover, a survey revealed that 36.1% of respondents felt that standardizing acupuncture treatments might limit the personalized approach that is integral to TCM.64 This highlights the challenge of balancing standardization with the individualized nature of acupuncture. Achieving a harmonious integration of standardized and personalized acupuncture treatment remains a key challenge for the future development of acupuncture. Although research has shown that acupoints possess specific therapeutic effects,65 there is insufficient data to quantify how acupoints selected based on TCM evidence contribute to treatment outcomes. The findings of this study suggested that “Heart-Liver Shu-Yuan acupoint combination” offer greater benefits in alleviating anxiety and depression symptoms compared to the treatment group. This provides preliminary support for exploring the differential effects of acupoint combinations on emotional symptoms and daytime functioning in patients with insomnia.
During the treatment period, no subjects experienced adverse reactions such as pneumothorax, needle fainting, or subcutaneous hematomas, demonstrating the high safety, rapid onset, and long-lasting effects of acupuncture in treating insomnia. The Heart–Liver Shu–Yuan acupoint combination was associated with improvements in both subjective and objective outcomes, with its concise point selection potentially enhancing patient compliance.
Overall, the findings support these results underscore the safety and efficacy of acupuncture as a complementary treatment for chronic insomnia, with HT7, BL15, LR3 and BL18 shows positive treatment effects in this study. In addition, this study provides preliminary insights into balancing standardized and individualized acupoint selection, which inform the future refinement of acupuncture treatment strategies.
Limitation
This trial has several limitations. First, due to constraints such as research funding and the COVID-19 pandemic, this study was unable to implement a multi-center, large-sample, subgroup analysis, and long-term follow-up randomized controlled trial. Additionally, the wide age range was not stratified in the analysis. Furthermore, PSG monitoring was conducted only for one night before and after treatment, monitoring sleep for just one night may not suffice for a comprehensive diagnosis. We did not formally assess blinding effectiveness, however, both groups received real acupuncture, which likely helped reduce bias and expectation effects. Future research should aim to address these limitations by conducting multi-center studies with larger sample sizes, extended follow-up periods to improve generalizability.
Conclusion
This study provides preliminary evidence supporting the efficacy and safety of acupuncture in improving both nocturnal sleep quality and daytime function in CID patients. The Heart–Liver Shu–Yuan acupoint combination showed a trend toward greater benefit in daytime mood symptoms. However, further large sample sizes and extended follow-up are needed to confirm these findings.
Data Sharing Statement
The data that support the findings of this randomized controlled trial on acupuncture for chronic insomnia are available from the corresponding author upon reasonable request. Due to ethical considerations and patient confidentiality agreements, individual participant data cannot be made publicly available. However, de-identified data sets and related materials can be provided to qualified researchers for academic purposes, subject to approval by the corresponding author and in compliance with institutional and ethical guidelines.
Acknowledgments
The PSQI used in this study is in the public domain. Usage permissions for the ESS and ISI have been obtained (ISI: SPECIAL TERMS No. 116783; ESS: SPECIAL TERMS No. 116648). Verbal permission to use the Chinese versions of the BAI and BDI was obtained from Pearson’s headquarters.
Author Contributions
LL–Conceptualization, Methodology, Data Curation, Investigation, Writing – Review & Editing; YC–Conceptualization, Funding Acquisition, Supervision, Writing–Review & Editing; ZL –Formal Analysis, Methodology, Funding Acquisition, Writing–Review & Editing; XC–Investigation, Writing – Review & Editing; JL–Investigation, Writing–Review & Editing; FW–Formal Analysis, Resources, Software, Writing–Review & Editing; NZ–Validation, Writing–Review & Editing; MX– Visualization, Writing–Original Draft.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Shanghai Municipal Health Commission Youth Health Talents Training Program(2022YQ034), National Natural Science Foundation of China (81904300), Clinical Research Project of Shanghai Municipal Health Commission(20224Y0071), Shanghai “Hospital Rising Star” Young Medical Talents Training Program, Training Program for High-caliber Talents of Clinical Research at Affiliated Hospitals of SHUTCM(22023LCRC15).
Disclosure
The authors declare no financial relationships with any organizations that might have an interest in the submitted work.The authors declare no non-financial competing interests related to this study.
References
1. Darien I. International Classification of Sleep Disorders.
2. Wilson S, Anderson K, Baldwin D, et al. British association for psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: an update. J Psychopharmacol. 2019;33(8):923–947. doi:10.1177/0269881119855343
3. Chung KF, Yeung WF, Yu YM, Ho FY. A population-based 2-year longitudinal study of insomnia disorder in a Chinese population in Hong Kong. Psychol Health Med. 2018;23(5):505–510. doi:10.1080/13548506.2017.1363397
4. Shekleton JA, Flynn-Evans EE, Miller B, et al. Neurobehavioral performance impairment in insomnia: relationships with self-reported sleep and daytime functioning. Sleep. 2014;37(1):107–116. doi:10.5665/sleep.3318
5. Fortier-Brochu E, Beaulieu-Bonneau S, Ivers H, Morin CM. Insomnia and daytime cognitive performance: a meta-analysis. Sleep Med Rev. 2012;16(1):83–94. doi:10.1016/j.smrv.2011.03.008
6. Roth T, Jaeger S, Jin R, Kalsekar A, Stang PE, Kessler RC. Sleep problems, comorbid mental disorders, and role functioning in the national comorbidity survey replication. Biol Psychiatry. 2006;60(12):1364–1371. doi:10.1016/j.biopsych.2006.05.039
7. Morin CM, LeBlanc M, Daley M, Gregoire JP, Mérette C. Epidemiology of insomnia: prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006;7(2):123–130. doi:10.1016/j.sleep.2005.08.008
8. McAlpine CS, Kiss MG, Rattik S, et al. Sleep modulates haematopoiesis and protects against atherosclerosis. Nature. 2019;566(7744):383–387. doi:10.1038/s41586-019-0948-2
9. Meyer N, Faulkner SM, McCutcheon RA, Pillinger T, Dijk DJ, MacCabe JH. Sleep and circadian rhythm disturbance in remitted schizophrenia and bipolar disorder: a systematic review and meta-analysis. Schizophr Bull. 2020;46(5):1126–1143. doi:10.1093/schbul/sbaa024
10. Yuan X, Zhu C, Wang M, Mo F, Du W, Ma X. Night shift work increases the risks of multiple primary cancers in women: a systematic review and meta-analysis of 61 articles. Cancer Epidemiol Biomarkers Prev. 2018;27(1):25–40. doi:10.1158/1055-9965.Epi-17-0221
11. Riemann D, Espie CA, Altena E, et al. The European insomnia guideline: an update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035. doi:10.1111/jsr.14035
12. Kjørstad K, Sivertsen B, Vedaa Ø, et al. The effects of digital CBT-I on work productivity and activity levels and the mediational role of insomnia symptoms: data from a randomized controlled trial with 6-month follow-up. Behav Res Ther. 2022;153:104083. doi:10.1016/j.brat.2022.104083
13. Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2021;17(2):255–262. doi:10.5664/jcsm.8986
14. Rapoport MJ, Lanctôt KL, Streiner DL, et al. Benzodiazepine use and driving: a meta-analysis. J Clin Psychiatry. 2009;70(5):663–673. doi:10.4088/JCP.08m04325
15. Stranks EK, Crowe SF. The acute cognitive effects of zopiclone, zolpidem, zaleplon, and eszopiclone: a systematic review and meta-analysis. J Clin Exp Neuropsychol. 2014;36(7):691–700. doi:10.1080/13803395.2014.928268
16. Scharner V, Hasieber L, Sönnichsen A, Mann E. Efficacy and safety of Z-substances in the management of insomnia in older adults: a systematic review for the development of recommendations to reduce potentially inappropriate prescribing. BMC Geriatr. 2022;22(1):87. doi:10.1186/s12877-022-02757-6
17. Chinese Society of Neurology SDG. Guidelines for the diagnosis and treatment of adult insomnia in China(2023 edition). Chin J Neurol. 2024;57(06):560–584.
18. Zhao FY, Spencer SJ, Kennedy GA, et al. Acupuncture for primary insomnia: effectiveness, safety, mechanisms and recommendations for clinical practice. Sleep Med Rev. 2024;74:101892. doi:10.1016/j.smrv.2023.101892
19. Zhao FY, Fu QQ, Kennedy GA, et al. Can acupuncture improve objective sleep indices in patients with primary insomnia? A systematic review and meta-analysis. Sleep Med. 2021;80:244–259. doi:10.1016/j.sleep.2021.01.053
20. Wang C, Xu WL, Li GW, et al. Impact of acupuncture on sleep and comorbid symptoms for chronic insomnia: a randomized clinical trial. Nat Sci Sleep. 2021;13:1807–1822. doi:10.2147/nss.S326762
21. Fu C, Zhao N, Liu Z, et al. Acupuncture improves peri-menopausal insomnia: a randomized controlled trial. Sleep. 2017;40(11). doi:10.1093/sleep/zsx153
22. Li S, Xue Q, Zhong Y, et al. Research trends in complementary and alternative treatments for insomnia over the past decade: a bibliometrics analysis. Medicine. 2023;102(29):e34346. doi:10.1097/md.0000000000034346
23. Cui Y, Zheng W, Xu L, Meng Y, Wang Y, Chang X. Distribution of elements extracted from symptom patterns and characteristics of polysomnograph of common symptom patterns of insomnia with traditional Chinese medicine. J Tradit Chin Med. 2016;36(5):649–653. doi:10.1016/s0254-6272(16)30085-1
24. Poon MM, Chung KF, Yeung WF, Yau VH, Zhang SP. Classification of insomnia using the traditional Chinese medicine system: a systematic review. Evid Based Complement Alternat Med. 2012;2012:735078. doi:10.1155/2012/735078
25. Yeung WF, Chung KF, Zhang NL, et al. Identification of Chinese medicine syndromes in persistent insomnia associated with major depressive disorder: a latent tree analysis. Chin Med. 2016;11(1):4. doi:10.1186/s13020-016-0076-y
26. Rong P, Zhu B, Li Y, et al. Mechanism of acupuncture regulating visceral sensation and mobility. Front Med. 2011;5(2):151–156. doi:10.1007/s11684-011-0129-7
27. Yunpeng D, Xuguang Y, Tengteng W, et al. Study on acupoint selection law of acupuncture treatment for intractable insomnia based on data mining. Chin J Inf Trad Chin Med. 2023;30(5):32–37.
28. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2012;10(1):28–55. doi:10.1016/j.ijsu.2011.10.001
29. MacPherson H, Altman DG, Hammerschlag R, et al. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. J Altern Complement Med. 2010;16(10):St1–14. doi:10.1089/acm.2010.1610
30. Sateia MJ. International classification of sleep disorders-third edition. Chest. 2014;146(5):1387–1394. doi:10.1378/chest.14-0970
31. You Y, Chen Y, Zhang Y, Zhang Q, Yu Y, Cao Q. Mitigation role of physical exercise participation in the relationship between blood cadmium and sleep disturbance: a cross-sectional study. BMC Public Health. 2023;23(1):1465. doi:10.1186/s12889-023-16358-4
32. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/s1389-9457(00)00065-4
33. Huang Longxiang ZJ, Wu X, Zhong H, Ding L. Nomenclature and location of Meridian points. 2021.
34. Liang fanrong LP. Acupuncture and Tuina Therapy, 3rd Edition of the New Century. China Traditional Medicine Press; 2023.
35. Guo Liang BY, Changchun J, Zhangyin S, Sirui X. Analysis on the laws of main acupoints of acupuncture for the treatment of primary insomnia. J Liaoning Univ Traditional Chin Med. 2022;2024(007):024.
36. Yang M, Morin CM, Schaefer K, Wallenstein GV. Interpreting score differences in the insomnia severity index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25(10):2487–2494. doi:10.1185/03007990903167415
37. Pilz LK, Keller LK, Lenssen D, Roenneberg T. Time to rethink sleep quality: PSQI scores reflect sleep quality on workdays. Sleep. 2018;41(5). doi:10.1093/sleep/zsy029
38. Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F. Test-retest reliability and validity of the Pittsburgh sleep quality index in primary insomnia. J Psychosom Res. 2002;53(3):737–740. doi:10.1016/s0022-3999(02)00330-6
39. Berry RB, Brooks R, Gamaldo C, et al. AASM scoring manual updates for 2017 (Version 2.4). J Clin Sleep Med. 2017;13(5):665–666. doi:10.5664/jcsm.6576
40. Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. doi:10.1037//0022-006x.56.6.893
41. Beck AT, Steer RA, Ball R, Ranieri W. Comparison of beck depression inventories -IA and -II in psychiatric outpatients. J Pers Assess. 1996;67(3):588–597. doi:10.1207/s15327752jpa6703_13
42. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol. 1989;46(10):1121–1123. doi:10.1001/archneur.1989.00520460115022
43. Scullin MK, Bliwise DL. Sleep, cognition, and normal aging: integrating a half century of multidisciplinary research. Perspect Psychol Sci. 2015;10(1):97–137. doi:10.1177/1745691614556680
44. Chervin RD. Epworth sleepiness scale? Sleep Med. 2003;4(3):175–176. doi:10.1016/s1389-9457(03)00030-3
45. Yu DS. Insomnia Severity Index: psychometric properties with Chinese community-dwelling older people. J Adv Nurs. 2010;66(10):2350–2359. doi:10.1111/j.1365-2648.2010.05394.x
46. Zheng B, Li M, Wang KL, Lv J. Analysis of the reliability and validity of the Chinese version of Pittsburgh sleep quality index among medical college students. Beijing Da Xue Xue Bao Yi Xue Ban. 2016;48(3):424–428.
47. Liang Y, Wang L, Zhu J. Factor structure and psychometric properties of Chinese version of Beck Anxiety Inventory in Chinese doctors. J Health Psychol. 2018;23(5):657–666. doi:10.1177/1359105316658971
48. Wu PC, Huang TW. Gender-related invariance of the beck depression inventory II for Taiwanese adolescent samples. Assessment. 2014;21(2):218–226. doi:10.1177/1073191112441243
49. Wang MY, Liu IC, Chiu CH, Tsai PS. Cultural adaptation and validation of the Chinese version of the Fatigue severity scale in patients with major depressive disorder and nondepressive people. Qual Life Res. 2016;25(1):89–99. doi:10.1007/s11136-015-1056-x
50. Peng LL, Li JR, Sun JJ, et al. Reliability and validity of the simplified Chinese version of Epworth sleepiness scale. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2011;46(1):44–49.
51. Kim SA, Lee SH, Kim JH, et al. Efficacy of acupuncture for insomnia: a systematic review and meta-analysis. Am J Chin Med. 2021;49(5):1135–1150. doi:10.1142/s0192415x21500543
52. Yin X, Li W, Liang T, et al. Effect of electroacupuncture on insomnia in patients with depression: a randomized clinical trial. JAMA Network Open. 2022;5(7):e2220563. doi:10.1001/jamanetworkopen.2022.20563
53. Zhang Ya HJ, Wu S, Zhang Y. Analysis of clinical features of traditional Chinese medicine symptoms and syndromes of 1 379 patients with primary insomnia. China J Trad Chin Med Pharm. 2017;34(1):43–5.
54. Wang Qianna GL, Liu C, Jin X, et al. Combination of yuan-source point, luo-connecting point and back-shu point for 66 cases of refractory insomnia. Chinese Acupuncture Moxibustion. 2022;42(4):2.
55. Yin X, Gou M, Xu J, et al. Efficacy and safety of acupuncture treatment on primary insomnia: a randomized controlled trial. Sleep Med. 2017;37:193–200. doi:10.1016/j.sleep.2017.02.012
56. Jiang TF, Chen ZY, Liu J, et al. Acupuncture modulates emotional network resting-state functional connectivity in patients with insomnia disorder: a randomized controlled trial and fMRI study. BMC Complement Med Ther. 2024;24(1):311. doi:10.1186/s12906-024-04612-0
57. Sun A, Wu X. Efficacy of non-pharmacological interventions on improving sleep quality in depressed patients: a systematic review and network meta-analysis. J Psychosom Res. 2023;172:111435. doi:10.1016/j.jpsychores.2023.111435
58. Pinto Jr LR Jr, Alves RC, Caixeta E, et al. New guidelines for diagnosis and treatment of insomnia. Arq Neuropsiquiatr. 2010;68(4):666–675. doi:10.1590/s0004-282x2010000400038
59. Tsui HTC, Chan WS. Daily associations between sleep parameters and depressive symptoms in individuals with insomnia: investigating emotional reactivity and regulation as mediators. Behav Sleep Med. 2024;23(1):1–16. doi:10.1080/15402002.2024.2399620
60. Ma HY, Xu YF, Qiao D, et al. Abnormal sleep features in adolescent MDD and its potential in diagnosis and prediction of early efficacy. Sleep Med. 2023;106:116–122. doi:10.1016/j.sleep.2023.01.021
61. Riemann D, Dressle RJ, Benz F, et al. Chronic insomnia, REM sleep instability and emotional dysregulation: a pathway to anxiety and depression? J Sleep Res. 2025;34(2):e14252. doi:10.1111/jsr.14252
62. Cheuk DK, Yeung WF, Chung KF, Wong V. Acupuncture for insomnia. Cochrane Database Syst Rev. 2012;2012(9):Cd005472. doi:10.1002/14651858.CD005472.pub3
63. Zhao K. Acupuncture for the treatment of insomnia. Int Rev Neurobiol. 2013;111:217–234. doi:10.1016/b978-0-12-411545-3.00011-0
64. Liang Z. Research on Present Situation and Counterplan of International Standardization of Acupuncture and Moxibustion. [dissertation]. China:Shandong University of traditional Chinese Medicine;2012.
65. Xing JJ, Zeng BY, Li J, Zhuang Y, Liang FR. Acupuncture point specificity. Int Rev Neurobiol. 2013;111:49–65. doi:10.1016/b978-0-12-411545-3.00003-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.