Back to Journals » Advances in Medical Education and Practice » Volume 17
Comparative Effectiveness of Ultrasound-Guided Posterior Approach versus Landmark-Based Middle Approach for Internal Jugular Vein Puncture in Resident Training
Authors Yu L, Feng Z, Han Y, Wu X, Zheng S
Received 12 March 2026
Accepted for publication 16 June 2026
Published 30 June 2026 Volume 2026:17 608680
DOI https://doi.org/10.2147/AMEP.S608680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Ling’an Yu, Ziqi Feng, Yingmin Han, Xinhong Wu, Shouhao Zheng
Department of Nephrology, Taizhou First People’s Hospital, Taizhou, People’s Republic of China
Correspondence: Ziqi Feng, Email [email protected]
Objective: To evaluate the teaching effectiveness of bedside ultrasound-guided posterior internal jugular vein puncture in the training of resident physicians.
Methods: From March 2019 to June 2024, 24 resident physicians at Taizhou First People’s Hospital were randomly assigned to a study group (n=12) and a control group (n=12). The study group received simulation-based training using a Mindray ultrasound skill training system, including repeated practice on a phantom model, followed by supervised patient procedures. The control group received training in anatomical landmark-based middle internal jugular vein puncture with equal practice time. Both groups received 2 hours of didactic teaching and self-study materials. Each physician performed the procedure on three patients, resulting in 36 cases per group. Procedural success was defined as successful guidewire insertion and catheter placement, confirmed by blood aspiration and subsequent chest X-ray. After completing the procedures, resident satisfaction was assessed using a standardized questionnaire.
Results: The study group had a 100% success rate, compared to 66.67% in the control group (χ 2=14.40, P< 0.001). First-attempt success rates were 83.33% in the study group versus 41.76% in the control group (χ 2=13.33, P< 0.001). The study group required fewer attempts (1.22± 0.54 versus 1.92± 0.91, t=− 3.95, P< 0.001), had no arterial punctures (0% versus 19.44%, χ 2=5.70, P=0.02), and shorter procedure times (4.53± 3.09 versus 7.08± 4.99 minutes, t=− 2.61, P=0.01). Resident satisfaction was higher in the study group (100% versus 58.33%, χ 2=4.04, P=0.01), No pneumothorax, hemothorax, or clinically significant hematoma occurred in either group. Post-procedural chest X-ray confirmed correct catheter tip position in all 72 patients (100%).
Conclusion: Short-term training in bedside ultrasound-guided posterior internal jugular vein puncture enables resident physicians to master this technique effectively, demonstrating good clinical application outcomes.
Keywords: ultrasound, internal jugular vein, visualization, hemodialysis
Introduction
Hemodialysis (HD) is one of the primary treatment methods for uremia and plays a significant role in improving patient survival rates. A reliable vascular access is the “lifeline” for patients undergoing maintenance hemodialysis. Autogenous arteriovenous fistula (AVF) offers numerous advantages, including long service life, low infection rates, and reduced mortality, making it the optimal vascular access for hemodialysis patients. However, when uremic patients undergo their first hemodialysis, an AVF has not yet been established. Therefore, establishing vascular access by inserting a hemodialysis catheter via right internal jugular vein puncture is the first choice.1
Although ultrasound guidance is recommended as the standard of care for central venous catheterization by multiple guidelines, many training programs in resource-limited settings still rely on anatomical landmark techniques due to equipment availability, time constraints, or curricular requirements. This study was designed under ethical approval with clinical equipoise, as all participating residents had no prior independent experience with internal jugular vein puncture, and patients in the control group received immediate rescue by supervising physicians if the landmark technique failed. For novice operators with no prior independent experience, it remains uncertain whether ultrasound guidance confers superiority over the landmark method in terms of first-attempt success rate or safety, as inexperienced residents may struggle with probe manipulation, potentially prolonging procedure time and increasing risk.
Internal jugular vein puncture is a clinical skill that resident physicians are required to master. Traditional internal jugular vein puncture employs the anatomical blind technique, relying mainly on the practitioner’s tactile experience. This method results in poor puncture accuracy, low success rates, and a high incidence of postoperative complications, posing significant challenges in clinical procedural training, The posterior approach via the oblique-axis in-plane view was selected because it combines the advantages of both short-axis and long-axis ultrasound-guided techniques. This approach offers clearer needle visualization, better real-time tracking of needle tip position, and a lower risk of carotid artery injury compared to the traditional middle approach.2
With the application of bedside ultrasound visualization technology in clinical practice, new tools and methods have become available for clinical procedures. Under the guidance of teaching physicians, resident physicians can perform safe and effective operations on patients under visualized conditions.3 Previous studies have evaluated the effectiveness of simulation-based ultrasound training for resident physicians in central venous catheterization. Koh et al4 demonstrated that after a formal training program consisting of a simulation-based workshop and five supervised ultrasound-guided internal jugular vein catheterizations on patients, novice residents achieved optimal clinical outcomes after performing seven procedures, with overall success rates improving from 82% to 99% and mechanical complications decreasing from 11% to 0%. La Fuente et al5 reported that in a randomized controlled trial involving anesthesia and emergency medicine residents, both groups showed improved performance in ultrasound-guided central venous catheter placement after simulation-based training, compared with their pretraining performance. These findings support the integration of simulation-based ultrasound training into resident education to improve procedural outcomes.
This study introduces bedside ultrasound visualization technology into the clinical procedural teaching of posterior internal jugular vein puncture. The aim is to achieve favorable outcomes and provide new training methods for standardized procedural training of resident physicians. The report is as follows.
Materials and Methods
General Information
Twenty-four resident physicians undergoing standardized training from March 2019 to June 2024 were selected as study subjects. They were randomly divided into a study group and a control group, each consisting of 12 resident physicians. Each physician was assessed by performing the procedure on three patients, totaling 72 patients. Based on a pilot study, assuming α=0.05 and power=0.80, we calculated that 12 residents per group (each performing 3 punctures) would be sufficient to detect a clinically meaningful difference in first-attempt success rates between the two groups. None of the participating residents had previously performed an internal jugular vein puncture independently; all had observed fewer than 5 procedures and received standardized training before study participation. Although the study spanned 5 years, no changes were made to the training curriculum, supervision protocol, or ultrasound equipment during this period. All residents received identical teaching materials and practice time.
Inclusion Criteria for Patients
- Patients aged 18 years or older, diagnosed with stage 5 chronic kidney disease, requiring hemodialysis treatment.
- Patients with stable vital signs who are able to cooperate with the surgical procedure.
Exclusion Criteria
- A history of mental disorders or psychological conditions.
- Severe coagulation dysfunction.
All patients meeting the inclusion criteria and their families were informed of the purpose of the procedure and possible complications before inclusion in the study, and they signed informed consent forms.
The study group received operational teaching on posterior internal jugular vein puncture using the ultrasound-guided method, while the control group received teaching on middle internal jugular vein puncture using the anatomical landmark localization method. The teaching duration was two academic hours for both groups. After the teaching sessions, each group was provided with self-study materials in the form of operational teaching videos produced by the department.
Our department purchased a Mindray ultrasound machine equipped with an ultrasound simulation skill training system. Resident physicians in the study group repeatedly practiced on the simulation system. The system’s built-in teaching guidance function ensured that resident physicians became familiar with operating the ultrasound equipment in a short time. By adjusting relevant settings and parameters, they achieved high-quality ultrasound images. The control group practiced the landmark technique on a conventional neck model for the same amount of time as the study group practiced on the ultrasound simulation system.
Once the resident physicians had basically mastered the internal jugular vein puncture technique, they proceeded to perform the puncture on patients in their respective groups.
A comparison of general information between the two groups of resident physicians showed no significant differences in age, gender, or educational background (P>0.05), indicating that the groups were comparable. See Table 1.
 |
Table 1 Comparison of General Information of Resident Physicians in the Two Groups |
Training Methods
Ultrasound-Guided Posterior Approach Right Internal Jugular Vein Puncture
All patients were placed in a supine position without a pillow, adopting the Trendelenburg position (head-down, feet-up) to maintain venous filling and reduce the risk of air embolism. The head was turned approximately 45° to the left. The puncture site was located at the intersection of the middle and lower thirds of the posterior border of the sternocleidomastoid muscle, serving as the insertion point. The ultrasound probe was directed from the insertion point toward the sternoclavicular joint. The puncture needle was generally kept horizontal (see Figure 1). Under ultrasound guidance, the positional relationship between the needle tip and shaft and the internal jugular vein was clearly visible (see Figure 2). The syringe was advanced with negative pressure maintained; when dark red blood was observed, needle advancement was stopped. A guide wire was inserted, followed by the placement of a dialysis catheter. The posterior approach was chosen because it allows an oblique-axis in-plane view, reducing the risk of carotid artery injury and shortening puncture time.6,7
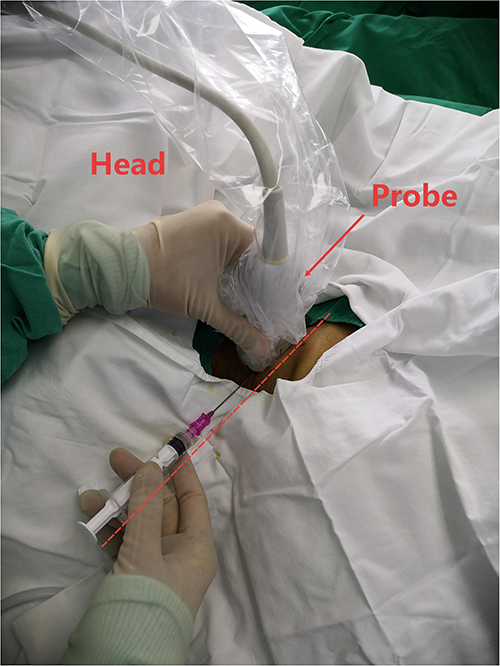 |
Figure 1 The linear probe is positioned at the intersection of the lower third of the posterior border of the sternocleidomastoid muscle, directed towards the sternoclavicular joint. The needle insertion direction is aligned with the probe’s orientation. |
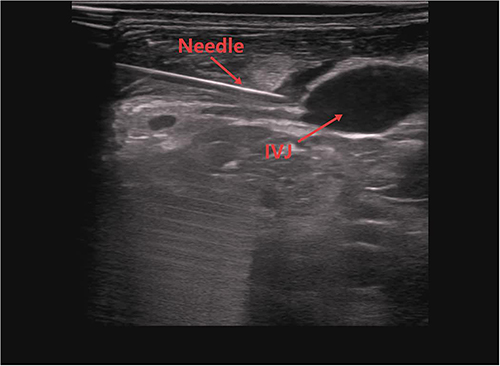 |
Figure 2 The ultrasound image clearly shows the positional relationship between the needle body, needle tip, and the internal jugular vein. |
Anatomical Landmark Localization Middle Approach Right Internal Jugular Vein Puncture
The same patient position was used as above. The puncture point was at the apex of the triangle formed by the clavicle and the clavicular and sternal heads of the sternocleidomastoid muscle. The internal jugular vein is centrally located within this triangle, approximately 3 cm above the superior border of the clavicle. The puncture needle was inserted at a 45° angle to the skin, directed toward the right nipple. The syringe was advanced with negative pressure maintained; when dark red blood was observed, needle advancement was stopped. After successful puncture, a guide wire was promptly inserted, and the dialysis catheter was placed.
All procedures were performed under direct supervision of an experienced attending physician who could intervene at any time. Patients were informed that residents would perform the puncture with supervision, and written informed consent was obtained from all participants.
Observation Indicators
A single puncture was defined as one insertion and withdrawal of the needle at the same puncture site. To protect patients and resident physicians, operations were terminated if puncture was unsuccessful after three attempts or if the internal carotid artery was injured; the internal jugular vein puncture was then declared a failure, and subsequent procedures were performed by the supervising physician. The total success rate, first-attempt success rate, total number of attempts, incidence of accidental arterial injury, and puncture time were recorded for both groups. After the operational assessments, a subjective questionnaire survey was conducted among the resident physicians of both groups to evaluate their satisfaction with the two teaching methods for internal jugular vein puncture.
Statistical Methods
Measurement data were expressed as mean ± standard deviation ( ). Intergroup comparisons were performed using the t-test. Comparisons of rates in count data were conducted using the chi-square (χ2) test. Statistical analysis was performed using SPSS 20.0 software, with P < 0.05 considered statistically significant.
). Intergroup comparisons were performed using the t-test. Comparisons of rates in count data were conducted using the chi-square (χ2) test. Statistical analysis was performed using SPSS 20.0 software, with P < 0.05 considered statistically significant.
Results
Evaluation of the Teaching Effectiveness of the Two Internal Jugular Vein Puncture Techniques
In the study group, all 36 patients achieved successful puncture, resulting in a total success rate of 100%. In the control group, 24 out of 36 patients had successful punctures, with a total success rate of 66.67%. The total success rate in the study group was significantly higher than that in the control group (P<0.05). The first-attempt success rate was 83.33% in the study group compared to 41.76% in the control group; this difference was statistically significant (P<0.05). The average number of attempts was 1.22 ± 0.54 in the study group and 1.92 ± 0.91 in the control group; the study group required significantly fewer attempts (P<0.05). The incidence of accidental arterial injury was 0.00% in the study group and 19.44% in the control group (χ2=5.70, P=0.02); the study group had a significantly lower incidence of arterial injury (P<0.05). The average puncture time was 4.53 ± 3.09 minutes in the study group and 7.08 ± 4.99 minutes in the control group; the puncture time was significantly shorter in the study group (P<0.05). See Table 2. No case of pneumothorax, hemothorax, or clinically significant hematoma occurred in either group. Post-procedural chest X-ray confirmed correct catheter tip position in all 72 patients (100%). No catheter malposition was observed.
 |
Table 2 Comparison of Teaching Effectiveness Between the Two Internal Jugular Vein Puncture Techniques |
Evaluation of Resident Physicians’ Satisfaction with the Operational Teaching of Internal Jugular Vein Puncture
All 12 resident physicians in the study group expressed satisfaction with the operational teaching of internal jugular vein puncture. Specifically, the ultrasound-guided posterior approach to the right internal jugular vein puncture provided operators with clear imaging, allowing them to understand their own procedural process and receive comprehensive guidance from supervising instructors as the puncture needle entered the venous vessel. In contrast, a higher number of resident physicians in the control group were dissatisfied after training. The anatomical landmark-based middle approach to the right internal jugular vein puncture required longer procedure times, often necessitated multiple punctures for success, and had a higher risk of accidental arterial injury. Additionally, resident physicians could not obtain precise guidance from their instructors, leading to doubts and apprehensions about the technique among many in the control group. There was a significant difference in satisfaction rates between the two groups regarding the operational teaching of internal jugular vein puncture (P<0.05). See Table 3.
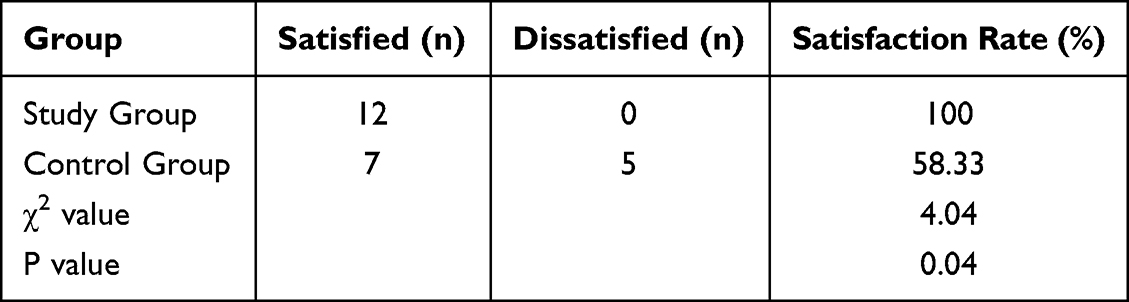 |
Table 3 Satisfaction with Operational Teaching of Internal Jugular Vein Puncture Among Resident Physicians in Both Groups |
Discussion
Ultrasound-Guided Posterior Internal Jugular Vein Puncture Enhances Patient Safety
As an invasive procedure, internal jugular vein puncture carries inherent risks. Complications arising from the procedure itself, prolonged operation time, or procedural failure can harm patients and even lead to serious consequences. Traditional teaching methods for internal jugular vein puncture rely on anatomical landmark localization, with instructors imparting their experiential knowledge. This approach is challenging for beginners to grasp and is prone to complications such as accidental arterial puncture, local hematoma, pneumothorax, and air embolism. The “Chinese Expert Consensus on Vascular Access for Hemodialysis” recommends ultrasound guidance for internal jugular vein puncture, especially in patients with neck masses or a history of neck surgery, where altered local anatomy can lead to inaccurate venous localization and increased risk of injury to blood vessels, nerves, and the pleural apex. Therefore, experiential internal jugular vein puncture without ultrasound guidance is not advisable.8
Many enrolled hemodialysis patients had a history of prior catheterizations, which may cause venous stenosis or scarring. Ultrasound guidance allowed real-time assessment of vessel patency and facilitated selection of an alternative puncture site when the primary target vein was compromised.
Current guidelines, including those from the European Federation of Societies for Ultrasound in Medicine and Biology, the American Society of Echocardiography, and the Society of Hospital Medicine, strongly recommend real-time ultrasound guidance for central venous catheterization to improve patient safety and reduce complications.9,10
Studies report a success rate of 85% to 99% for central venous catheterization, with complication rates ranging from 10% to 20%.11 Ultrasound-guided central venous puncture significantly reduces the number of venous puncture attempts, offers a higher first-attempt success rate, shortens operation time, and decreases complications, thereby effectively enhancing patient safety.12 The ultrasound-guided long-axis in-plane method for internal jugular vein puncture can display the needle path and the process of needle entry into the vessel lumen but cannot show the anatomical structures surrounding the internal jugular vein. Conversely, the ultrasound-guided short-axis out-of-plane method clearly displays the structures around the internal jugular vein, especially the positional relationship between the common carotid artery and the internal jugular vein, but does not clearly show the needle trajectory and insertion depth. Therefore, both the short-axis and long-axis approaches have advantages and limitations.13
In this study, we employed ultrasound-guided posterior internal jugular vein puncture for operational teaching. This technique utilizes the ultrasound oblique-axis in-plane method, combining the advantages of both the short-axis and long-axis ultrasound-guided puncture techniques.7 It reduces the number of adjustments in puncture direction, shortens puncture time, lowers the incidence of accidental arterial injury, and serves as a safer ultrasound-guided pathway for internal jugular vein puncture.14
Ultrasound-Guided Posterior Internal Jugular Vein Puncture Improves Resident Physicians’ Confidence and Learning Efficiency
The ultrasound-guided posterior internal jugular vein puncture, using the ultrasound oblique-axis in-plane technique, allows the procedural process to be displayed in real-time to resident physicians. This approach tightly integrates the tactile sensation of the puncture with ultrasound imaging, providing authentic feedback on the positional relationship between the puncture needle (both shaft and tip) and the internal jugular vein. This facilitates instructors in explaining the puncture localization and safe, effective operational force, giving resident physicians an intuitive and vivid understanding of the puncture maneuver, thereby enhancing their confidence and significantly improving learning efficiency.15
Our study demonstrates that, compared with traditional anatomical landmark-based middle approach internal jugular vein puncture training, ultrasound-guided posterior internal jugular vein puncture training increases resident physicians’ overall success rate and first-attempt success rate, reduces the total number of puncture attempts and the incidence of accidental arterial injury, and shortens puncture time. Numerous factors affect the success of internal jugular vein puncture, with vascular anatomical variations being a primary reason. Maecken et al16 reported that in ultrasound examinations of 600 patients, over 20% had the internal jugular vein located anteromedial to the common carotid artery, making successful puncture difficult using traditional anatomical landmark methods. In obese patients with short necks, unclear surface landmarks and inexperienced operators can also lead to puncture failure. Under ultrasound guidance, the vascular pathway is clearly visible, allowing for accurate vessel localization even in cases of anatomical variation, thus improving success rates and reducing severe complications.17
In this study, fluoroscopy was not routinely used. However, for patients with difficult anatomy or prior catheterization history, combined ultrasound and fluoroscopic guidance might further improve safety and accuracy of catheter placement. Fluoroscopy can confirm guidewire and catheter tip position in real time, reduce the risk of malposition, and facilitate management of central venous stenosis or obstruction.
Operational Teaching of Ultrasound-Guided Posterior Internal Jugular Vein Puncture Enhances Resident Physicians’ Satisfaction
The internal jugular vein, carotid artery, and vagus nerve are enclosed within the carotid sheath. The relatively safe area for internal jugular vein puncture is bounded superiorly by the level of the cricoid cartilage, inferiorly by a horizontal line midway between the cricoid cartilage and the sternal head of the sternocleidomastoid muscle, laterally by the belly of the clavicular head of the sternocleidomastoid muscle, and medially by the belly of the sternal head of the sternocleidomastoid muscle.18 A puncture point that is too high may damage critical structures such as the carotid sinus, carotid body, and the main trunk of the vagus nerve. A puncture point that is too low may injure the lung apex, causing hemopneumothorax.
Traditional internal jugular vein puncture uses the anatomical blind technique, generally selecting the apex of the triangle formed by the sternal head and clavicular head of the sternocleidomastoid muscle and the clavicle as the puncture site—known as the middle approach—which lies within the safe area for internal jugular vein puncture. However, this teaching method relies entirely on the instructor’s theoretical knowledge and clinical experience, without real-time visualization of the resident physician’s needle position within the patient’s body. This leads to a slow improvement in the resident’s operational skills and a higher likelihood of complications, resulting in frustration and fear regarding their abilities.
In contrast, ultrasound-guided posterior internal jugular vein puncture training allows instructors to clearly see the position, direction, and depth of the needle relative to the internal jugular vein, providing real-time guidance for adjustments. This method offers strong controllability, higher success rates, fewer complications, strengthened operational confidence among resident physicians, and higher satisfaction with the training. The anatomical relationship between the internal jugular vein and the common carotid artery exists in four configurations: lateral (16%), anterolateral (37%), anterior (44%), and medial (3%), which contradicts the traditional anatomical textbooks that describe the internal jugular vein as solely lateral to the common carotid artery.19 Therefore, the traditional anatomical landmark-based middle approach has a low success rate.
With continuous innovation and development in visualization technology and equipment, ultrasound-guided posterior internal jugular vein puncture is destined to become the developmental trend in internal jugular vein puncture techniques. In clinical operational training, enabling resident physicians to master advanced clinical techniques reflects a commitment to keeping pace with the times and continuous innovation in clinical teaching.
Conclusion
In summary, within the context of this single-center randomized teaching study, short-term training in ultrasound-guided posterior internal jugular vein puncture combined with simulation-based practice enabled resident physicians to achieve higher success rates, fewer complications, and shorter procedure times compared with traditional anatomical landmark-based training. These findings support the integration of ultrasound-guided techniques into resident training curricula, although further multi-center studies with larger sample sizes are needed to confirm generalizability. Limitations of this study include the relatively small sample size, single-center design, and the inherent challenges associated with the retrospective nature of data collection. Additionally, while both groups received standardized didactic instruction, the study did not objectively assess baseline technical proficiency of the residents prior to training. Nevertheless, traditional anatomical landmark techniques remain an essential component of clinical training curricula, as training resident physicians in ultrasound probe manipulation presents practical challenges in some settings. The relatively complex and time-consuming preparation of ultrasound equipment may also increase the difficulty of maintaining aseptic conditions, which should be addressed in future curriculum development.
Data Sharing Statement
All data generated and analyzed during this study are included in this article.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Taizhou First People’s Hospital (approval number: 2023-KY023-01), Patients were consented by an informed consent process that was reviewed by the Ethics Committee of Taizhou First People’s Hospital and certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Science and Technology Plan Project of Taizhou (grant number: 23ywa25).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Schmidli J, Widmer MK, Basile C, et al. Editor’s choice - vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55(6):757–9. doi:10.1016/j.ejvs.2018.02.001
2. Schmidt GA, Blaivas M, Conrad SA, et al. Ultrasound-guided vascular access in critical illness. Intensive Care Med. 2019;45(4):434–446. doi:10.1007/s00134-019-05564-7
3. Sun W, Jiang X, Dong X, Yu G, Feng Z, Shuai L. The evolution of simulation-based medical education research: from traditional to virtual simulations. Heliyon. 2024;10(15):e35627. doi:10.1016/j.heliyon.2024.e35627
4. Koh J, Xu Y, Yeo L, et al. Achieving optimal clinical outcomes in ultrasound-guided central venous catheterizations of the internal jugular vein after a simulation-based training program for novice learners. Simul Healthc. 2014;9(3):161–166. doi:10.1097/SIH.0000000000000010
5. de la Fuente R, Galvez-Yanjari V, Delfino A, et al. Process-oriented feedback for ultrasound-guided central venous access training: a randomized controlled trial. BMC Anesthesiol. 2025;25(1). doi:10.1186/s12871-025-03341-2
6. Chennakeshavallu GN, Gadhinglajkar S, Sreedhar R, Babu S, Sankar S, Dash PK. Comparison of three ultrasound views for internal jugular venous cannulation in patients undergoing cardiac surgery. J Med Ultrasound. 2021;29(3):176–180. doi:10.4103/JMU.JMU_135_20
7. DiLisio R, Mittnacht AJC. The “Medial-Oblique” approach to ultrasound-guided central venous cannulation—maximize the view, minimize the risk. J Cardiothorac Vasc Anesth. 2012;26(6):982–984. doi:10.1053/j.jvca.2012.04.013
8. Zhang H, Lu H, Li W, Jiang G, Zou H. Expert consensus on the establishment and maintenance of native arteriovenous fistula. Chronic Dis Transl Med. 2021;7(4):235–253. doi:10.1016/j.cdtm.2021.05.002
9. Vegas A, Wells B, Braum P, et al. Guidelines for performing ultrasound-guided vascular cannulation: recommendations of the American society of echocardiography. J Am Soc Echocardiography. 2025;38(2):57–91. doi:10.1016/j.echo.2024.12.004
10. Jenssen C, Brkljacic B, Hocke M, et al. EFSUMB guidelines on interventional ultrasound (INVUS), Part VI – ultrasound-guided vascular interventions. Ultraschall in der Medizin. 2015;37(05):473–476. doi:10.1055/s-0035-1553450
11. Lorchirachoonkul T, Ti LK, Manohara S, et al. Anatomical variations of the internal jugular vein: implications for successful cannulation and risk of carotid artery puncture. Singapore Med J. 2012;53(5):325–328.
12. Kunhahamed MO, Abraham SV, Palatty BU, Krishnan SV, Rajeev PC, Gopinathan V. A comparison of internal jugular vein cannulation by ultrasound-guided and anatomical landmark technique in resource-limited emergency department setting. J Med Ultrasound. 2019;27(4):187–191. doi:10.4103/JMU.JMU_2_19
13. Maitra S, Bhattacharjee S, Baidya DK. Comparison of long-, short-, and oblique-axis approaches for ultrasound-guided internal jugular vein cannulation: a network meta-analysis. J Vasc Access. 2020;21(2):204–209. doi:10.1177/1129729819868927
14. Tammam TF, El-Shafey EM, Tammam HF. Ultrasound-guided internal jugular vein access: comparison between short axis and long axis techniques. Saudi J Kidney Dis Transpl. 2013;24(4):707–713. doi:10.4103/1319-2442.113861
15. Ho AM, Ricci CJ, Ng CS, et al. The medial-transverse approach for internal jugular vein cannulation: an example of lateral thinking. J Emerg Med. 2012;42(2):174–177. doi:10.1016/j.jemermed.2011.05.033
16. Maecken T, Marcon C, Bomas S, Zenz M, Grau T. Relationship of the internal jugular vein to the common carotid artery: implications for ultrasound-guided vascular access. Eur J Anaesthesiol. 2011;28(5):351–355. doi:10.1097/EJA.0b013e328341a492
17. Abbadie F, Kosmadakis G, Aguilera D, Piraud A. Duplex ultrasound-guided angioplasty of hemodialysis vascular access. J Vasc Surg. 2023;78(5):1292–301.e3. doi:10.1016/j.jvs.2023.07.007
18. Pérez Reyes JM, Bethencourt Muñoz S, Cabrejas Ibarz MT, Tejero García M, Valdivia Martín J, González Miranda F. Ultrasound-guided puncture of the jugular vein using a posterior approach. Rev Esp Anestesiol Reanim. 2008;55(10):616–620. doi:10.1016/S0034-9356(08)70673-X
19. Bai C, Wang Z, Guan J, et al. Probable factors affecting clinical outcomes of internal jugular vein stenosis. Ann Transl Med. 2019;7(22):621. doi:10.21037/atm.2019.11.05
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.