Back to Journals » Drug Design, Development and Therapy » Volume 20
Comparative Effectiveness of Single-Dose Epidural Esketamine versus Hydromorphone in Thoracic and Upper Abdominal Surgery: A Randomized Trial
Authors Song Y, Wang C, Huang N, He H ![]() , Hong W, Wu J, Yao M, Miao C, Liang C
, Hong W, Wu J, Yao M, Miao C, Liang C
Received 10 November 2025
Accepted for publication 29 January 2026
Published 3 February 2026 Volume 2026:20 580521
DOI https://doi.org/10.2147/DDDT.S580521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Yuejiao Song,1,* Chengyu Wang,2,* Ning Huang,2,* Huangwei He,1 Weifeng Hong,1 Junmei Wu,1 Minmin Yao,2 Changhong Miao,2 Chao Liang1,2
1Department of Anesthesiology, Zhongshan Hospital (Xiamen), Fudan University, Xiamen, Fujian, People’s Republic of China; 2Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Liang, Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China, Tel/Fax +86-021-64041990, Email [email protected] Changhong Miao, Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China, Tel/Fax +86-021-64041990, Email [email protected]
Purpose: This study aimed to evaluate the effectiveness of a single epidural dose of esketamine versus hydromorphone in patients undergoing abdominal and thoracic surgeries.
Patients and Methods: Patients undergoing elective abdominal and thoracic surgery were randomly assigned to receive either a single epidural injection of 15 mg esketamine (Group E) or 0.5 mg hydromorphone (Group H) at the end of surgery. All patients received intravenous patient-controlled analgesia postoperatively. The primary outcome was hydromorphone consumption within 48 hours after surgery. Secondary outcomes included time to first rescue analgesia, hydromorphone consumption within 0– 24, 24– 48, and 48– 72 hours, numerical rating scale (NRS) pain scores, postoperative recovery scores, and complications.
Results: In total, 205 patients were enrolled, with 186 randomly assigned to either group E (n = 93) or group H (n = 93). Hydromorphone consumption within 48 hours postoperatively was significantly higher in group E than in group H. The time to first rescue analgesia was significantly longer in group H compared to group E. Within the first 24 hours postoperatively, patients in group E required more hydromorphone than those in group H. No significant difference in hydromorphone consumption between the two groups at 24– 48 and 48– 72 hours postoperatively. The NRS scores during movement were significantly higher in group E than in group H at 3 and 6 hours postoperatively.
Conclusion: Single-dose epidural esketamine for postoperative analgesia resulted in higher hydromorphone consumption and a shorter time to first rescue analgesia compared to hydromorphone.
Keywords: esketamine, epidural anesthesia, postoperative analgesia, hydromorphone
Introduction
Multimodal analgesia is a cornerstone of Enhanced Recovery After Surgery (ERAS), playing a critical role in optimizing recovery. Within this approach, regional nerve blocks are a fundamental component.1,2 Among these techniques, epidural analgesia remains the gold standard for thoracic and upper abdominal surgeries due to its well-documented efficacy in attenuating perioperative stress responses,3,4 and its integral role in multimodal analgesic regimens.2,5,6
Although epidural local anesthetics provide effective analgesia, their use is limited by adverse effects such as hypotension, extensive sensory blockade, and urinary retention. The addition of opioids may reduce these complications.3,7 Nevertheless, traditional opioid-based analgesia, albeit widely used perioperatively, is associated with significant side effects ranging from common issues like postoperative nausea and vomiting (PONV) and pruritus to more serious risks of postoperative delirium and respiratory complications.8 These concerns have led to the development of opioid-sparing and opioid-free analgesic strategies, with recent studies demonstrating that opioid-free anesthesia is non-inferior to traditional opioid-containing regimens.9
Esketamine has gained prominence as an effective opioid-sparing agent, attracting growing clinical and research attention. Compared with racemic ketamine, esketamine exhibits enhanced pharmacodynamic properties, including more rapid sedation and analgesia due to its greater receptor affinity, alongside a favorable safety profile.10 Notably, current pharmaceutical formulations of esketamine are preservative-free, with several studies validating both the safety and efficacy of its epidural administration.10,11 When administered via the epidural route, esketamine potently inhibits nociceptive signaling pathways, achieving two clinically significant effects: (1) enhanced analgesic quality and (2) prolonged morphine efficacy without a concomitant increase in adverse effects.12 Epidural esketamine administration has been shown to significantly reduce postoperative opioid consumption, attenuate hyperalgesia, and mitigate postsurgical pain.8 However, the effectiveness and duration of analgesia from a single-dose epidural esketamine remain uncertain, and it is unclear whether its effects and duration are comparable to those of conventional epidural opioids, such as hydromorphone.
Therefore, this study aimed to evaluate the analgesic efficacy and duration of single-dose epidural esketamine through a direct comparison with hydromorphone. We hypothesized that single-dose epidural esketamine would provide postoperative analgesia that is non-inferior to that of hydromorphone.
Materials and Methods
Study Design and Participants
This prospective, single-center, randomized, triple-blind clinical trial was conducted at Zhongshan Hospital, Fudan University (Xiamen Branch), from August 2024 to April 2025. The study was approved by the Ethics Committee of Zhongshan Hospital Xiamen Branch (Approval No.: B2024-041R), and written informed consent was obtained from all participants. The trial was registered before patient enrollment in the Chinese Clinical Trial Registry (ChiCTR2400087004, https://www.chictr.org.cn/showproj. html? Proj =237457; principal investigator: Liang Chao; Registration date: July 17, 2024).
Eligible participants included those aged 18–80 years with an American Society of Anesthesiology (ASA) status of I–III, and were scheduled for laparoscopic surgery involving the chest and upper abdomen. The exclusion criteria included refusal to sign the consent form, contraindications to epidural anesthesia, inability to cooperate during epidural manipulation, chronic use of analgesics, pre-existing chronic pain, known allergy to any study medication, and inability to understand the trial procedures or accurately report pain scores.
Randomization and Blinding
Patients were randomly allocated in equal proportions to receive either esketamine (E) or hydromorphone (H) upon arrival in the preoperative holding area. Group allocation was determined using a random number table generated in Microsoft Excel, where even numbers corresponded to group E and odd numbers to group H.
This study utilized a triple-blind approach. A single assigned researcher handled the randomization process, including the generation of allocation sequences and drug preparation for surgical use. A separate investigator, assisted by a research assistant, prepared the trial medications intraoperatively. Both the anesthesia providers and outcome assessors were unaware of group assignments. Independent evaluators performed postoperative assessments, data collection, and statistical analysis. Patients were also kept blinded for the entire duration of the trial.
Anesthetic Treatment
After entering the operating room, patients received an epidural puncture at either the T7–T8 or T8–T9 intervertebral space, followed by catheter insertion (6–8 cm depth). Standard monitoring was implemented for all patients, including electrocardiography (ECG), invasive blood pressure measurement, pulse oximetry (SpO2), and bispectral index (BIS; Covidien), the latter providing a quantitative measure of sedation level (range: 0–100).
General anesthesia was initiated with a target-controlled infusion of propofol (Corden Pharma S.P.A), maintaining a plasma concentration target of 4.0 μg/mL according to Schnider’s three-compartment pharmacokinetic model.13 Additionally, remifentanil (0.2 μg/kg/min; Jiangsu Nhwa Pharmaceutical Co., Ltd) and rocuronium bromide (0.6 mg/kg; Merck Sharp & Dohme Corp) were administered. To sustain adequate anesthesia depth (BIS 40–60), desflurane was administered at 0.8–1.0 MAC throughout the procedure. Intermittent bolus doses of rocuronium were administered to maintain adequate neuromuscular blockade throughout the surgical procedure. Intraoperative analgesic administration was titrated according to continuous hemodynamic monitoring (blood pressure, heart rate, and mean arterial pressure), supplemented by nociceptive evaluation using the Surgical Pleth Index (SPI) to optimize analgesia. When necessary, supplemental doses of sufentanil (5μg per dose; Yichang Renfu Pharmaceutical Co. Ltd) were administered. The epidural analgesia protocol comprised an initial bolus of 10 mL 0.2% ropivacaine for thoracic procedures or 10 mL 0.3% ropivacaine for upper abdominal surgeries. This was supplemented by continuous epidural infusion at 5 mL/h using the corresponding concentration (0.2% for thoracic, 0.3% for upper abdominal procedures). Before the end of the surgery, a single epidural dose of esketamine (15 mg) was administered to patients in group E, and hydromorphone (0.5 mg) to those in group H. The epidural catheter was subsequently removed in both groups. Precisely 2g of propacetamol, 50 mg of dexketoprofen trometamol, and 0.6 mg of ramosetron were administered toward the end of the operation. Sugammadex was administered at a dose of 2 mg/kg to reverse the residual neuromuscular block.
After surgery, awakened patients were transferred to the post-anesthesia care unit (PACU). A bolus dose of intravenous patient-controlled analgesia (PCA) was administered when the NRS score was ≥4. The patients were transferred to the ward after at least 1 hour of observation if their NRS score remained <4 and their Steward score ≥4. All patients received intravenous PCA containing hydromorphone (14 mg) and granisetron (6 mg) diluted in 250 mL of normal saline, delivered with a basal rate of 0 mL/h, a 4 mL bolus dose, a lock-out time of 10 minutes, and a maximum hourly volume limit of 24 mL.
An additional 40 mg of parecoxib was administered every 12 hours until the surgical drain was removed. Another research assistant monitored the NRS score and anesthesia-associated complications postoperatively. Patients were instructed that PCA pump rescue is required whenever the NRS score exceeded 3. Postoperative NRS scores at each time point refer to the highest recorded scores following PCA administration.
Outcome Parameters
The primary outcome of this study was cumulative hydromorphone consumption within 48 hours postoperatively. Secondary outcomes included: resting and dynamic NRS pain scores (ranging from 0 = pain-free to 10 = worst imaginable pain) with the highest scores recorded at baseline immediately after surgery and at 1, 3, 6, 24, 48, and 72 hours postoperatively; the incidence and rescue treatment of breakthrough pain; daily opioid consumption up to postoperative day 3; number of effective PCA demands; postoperative recovery quality (assessed using Quality of Recovery-15 (QoR-15) scale), cognitive function (evaluated by Mini-Mental State Examination (MMSE)), and delirium screening (using Confusion Assessment Method) on postoperative day 1; mental status evaluations including dizziness, headache, drowsiness, hallucinations, nightmares, and nystagmus; as well as the incidence of anesthesia-related adverse events and length of hospital stay.
Statistical Analysis
The analysis included measures such as mean (standard deviation) for normally distributed variables, median (interquartile range) for non-normally distributed continuous variables, and frequencies and percentages for categorical variables. Normality tests and QQ plots were used to assess the distribution of the data, and appropriate descriptive statistical methods were applied to both normally and non-normally distributed variables. Group comparisons for normally distributed continuous variables were performed using Welch’s t-test or analysis of variance (ANOVA), while non-normally distributed variables were analyzed using the Wilcoxon rank–sum test or Kruskal–Wallis test. For comparisons between groups of categorical data, Fisher’s exact test was used for expected frequencies <5; otherwise, the chi-squared test was applied.
All statistical analyses were performed using the R software (version 4.2.2) and MSTATA software (https://www.mstata.com).
Sample Size Calculation
The primary endpoint of this study was intravenous morphine-equivalent consumption within 48 hours postoperatively. Preliminary findings indicated that the hydromorphone group had a mean 48-hour morphine-equivalent consumption of 22 mg, with a standard deviation of 5.7 mg. We hypothesized that the non-inferiority margin for esketamine compared to hydromorphone in terms of 48-hour morphine-equivalent consumption would be 3 mg. With α = 0.05 and 1-β = 0.9, the required sample size was calculated to be 154 patients. After accounting for a 20% dropout rate during follow-up, the final estimated sample size was 186 patients, with 93 patients assigned to each group.
Results
Study Population
During the study period (from August 26, 2024, to April 27, 2025), a total of 205 patients were screened for eligibility. Exactly 19 patients were excluded before randomization: 7 patients declined to participate, 8 patients had unsuccessful epidural catheterization, 1 patient had a history of chronic pain, and 3 patients had a history of abdominal surgery. 186 patients were enrolled and randomized, 93patients each into groups E and H. All 186 participants were included in the final analysis. A CONSORT flow diagram is presented in Figure 1. Baseline characteristics and surgical details of the patients are summarized in Table 1. Patient demographics, underlying conditions, and surgical procedures were consistent across all study participants.
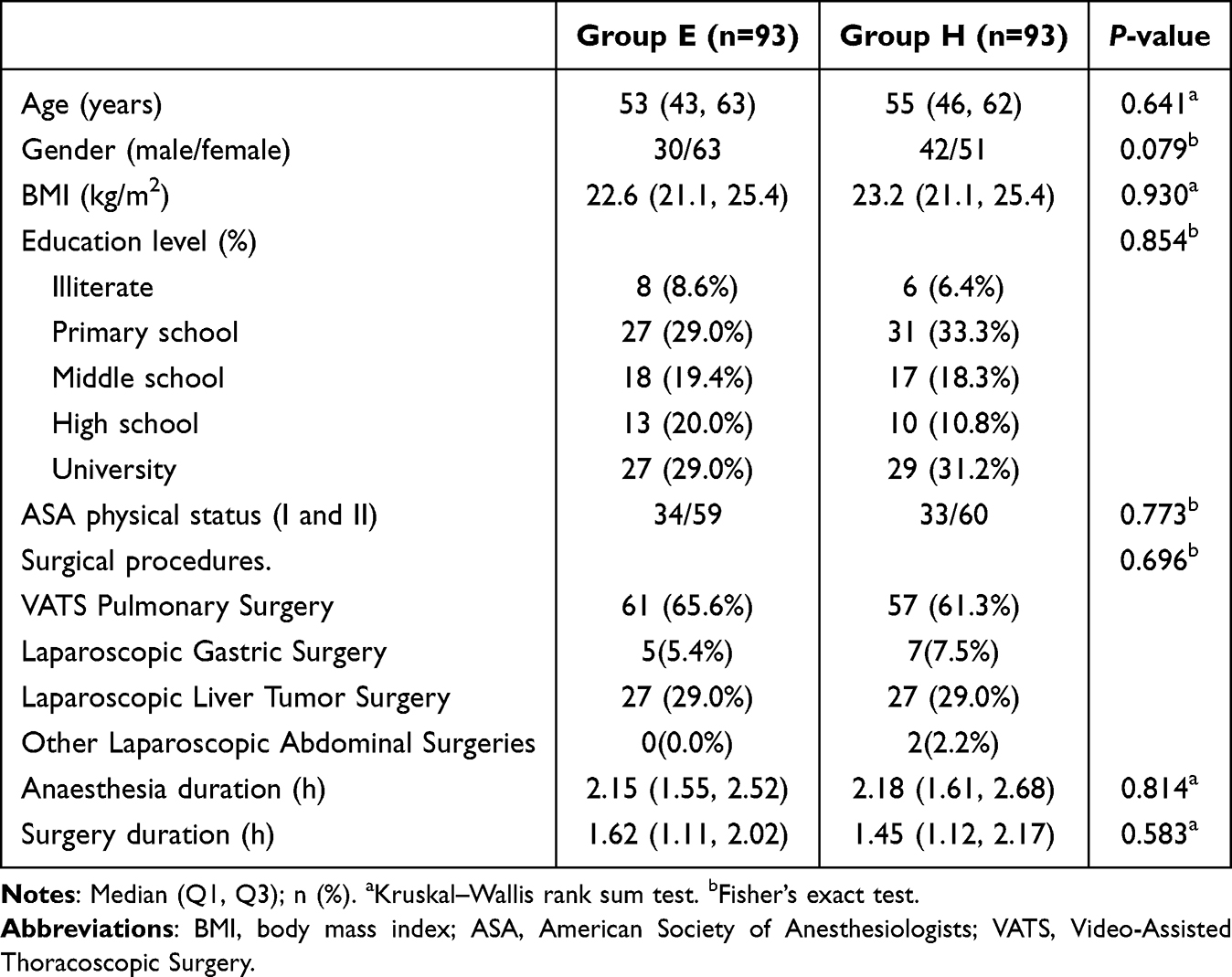 |
Table 1 Patient Demographics and Baseline Characteristics |
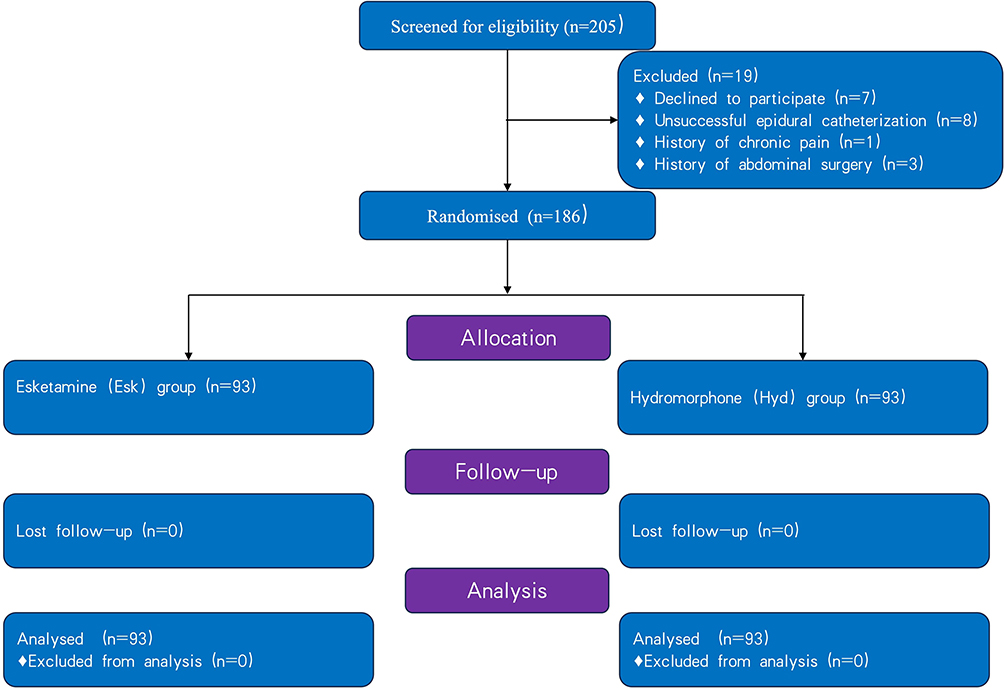 |
Figure 1 Flow diagram of the patients in this study. |
Primary Outcome
All patients completed postoperative follow-up (Table 2). Within the first 48 hours, patients in the epidural esketamine group (Group E) required significantly higher hydromorphone consumption than those in the epidural hydromorphone (Group H) (1.8 mg vs 1.0 mg; P < 0.001). Additionally, the time to first rescue analgesia was significantly longer in Group H compared to Group E (35.5 hours vs 12.6 hours; P < 0.001).
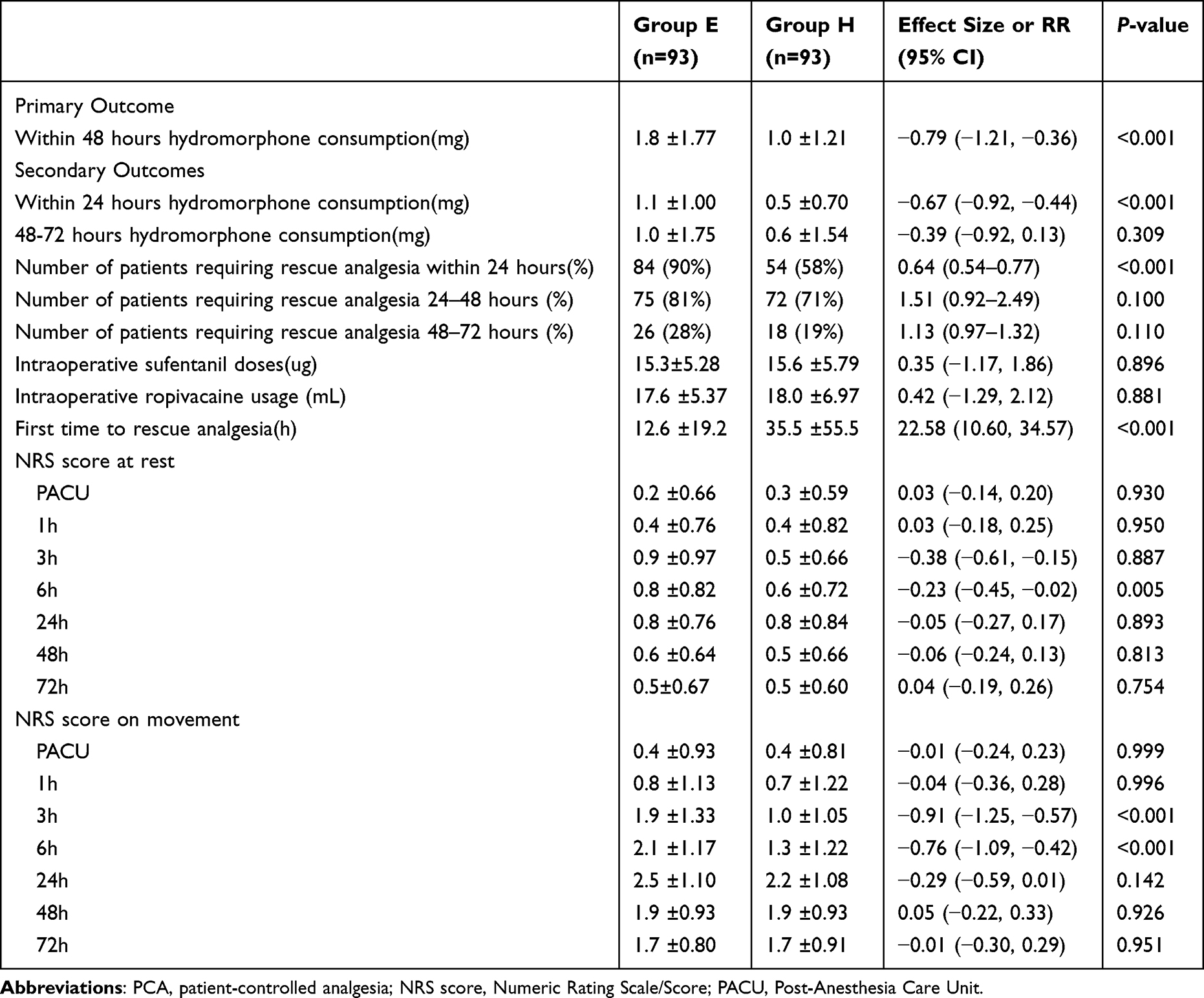 |
Table 2 Primary and Secondary Outcomes |
Secondary Outcomes
Hydromorphone consumption within the first 24 hours was significantly higher in Group E than in Group H (1.1 mg vs 0.5 mg; P < 0.001). However, hydromorphone consumption at 48–72 hours postoperatively did not differ significantly between groups (1.0 mg vs 0.6 mg; P = 0.309).These data are showed in Figure 2.
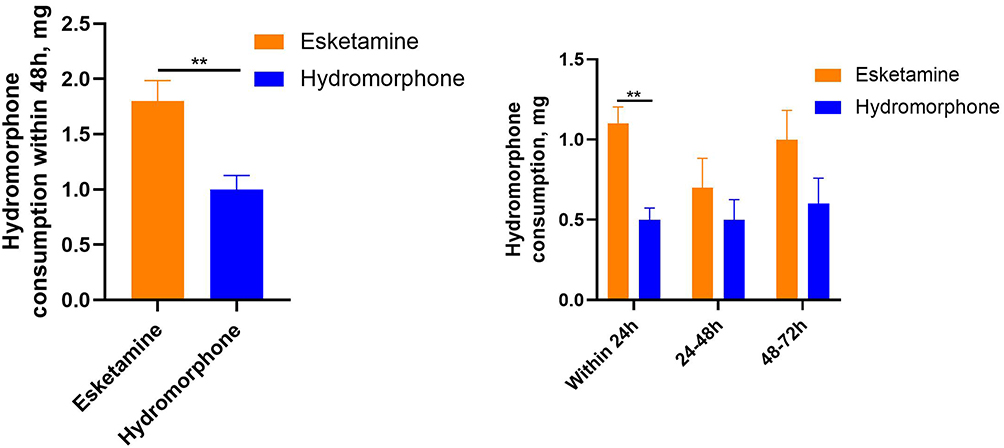 |
Figure 2 Hydromorphone consumption after surgery. **P <0.001 indicates statistical significance for between-group comparisons. |
A significantly higher proportion of patients in Group E required rescue analgesia within 24 hours compared to group H (90% vs 58%; P < 0.001). No statistically significant differences were observed between groups at 24–48 hours (81% vs 71%; P = 0.10); 48–72 hours (28% vs 19%; P = 0.11). The two groups showed comparable use of intravenous sufentanil and epidural ropivacaine intraoperatively (P > 0.05). Regarding pain scores at rest, a significant difference was found only at 6 hours postoperatively (0.8 vs 0.6; P = 0.005). For pain during movement, Group E reported significantly higher NRS scores at 3 hours (1.9 vs 1.0; P<0.001) and 6 hours (2.1 vs 1.3; P<0.001). These data are summarized in Table 2.
Postoperative adverse events and patient satisfaction scores in both groups are presented in Table 3. No statistically significant differences were observed between groups in terms of PONV, dizziness, QoR-15 scores, MMSE results, or length of hospital stay (all P > 0.05).
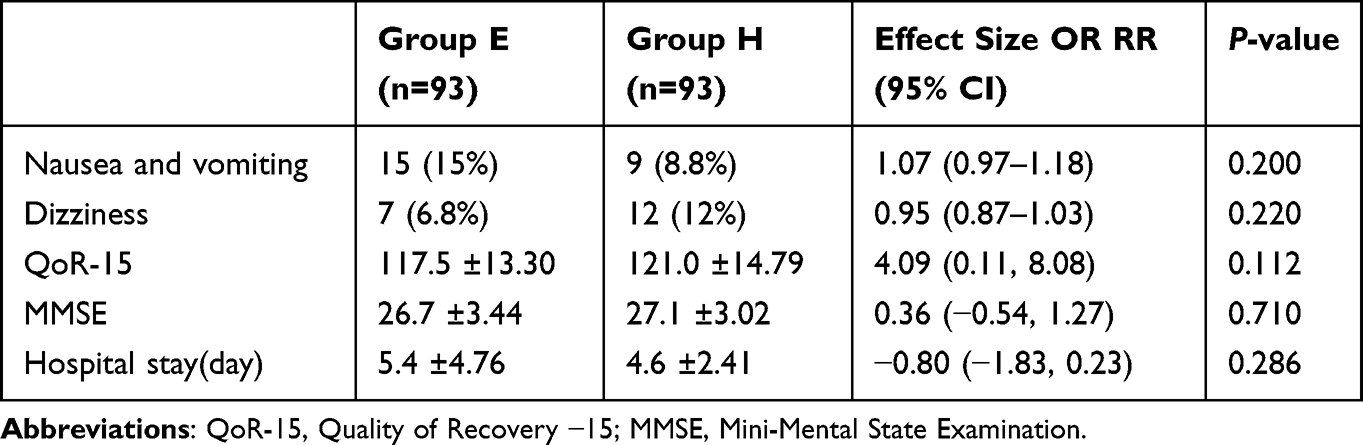 |
Table 3 Postoperative Adverse Events and Satisfaction |
Discussion
Opioid-sparing regimens are an important part of the ERAS protocol, prompting the increasing use of non-opioid alternatives. Despite growing interest, the effectiveness of single-dose epidural esketamine has not been systematically evaluated. In this triple-blind randomised trial, a single epidural bolus of esketamine (15 mg) provided inferior postoperative analgesia compared with epidural hydromorphone (0.5 mg), as reflected by higher cumulative hydromorphone consumption within 48 h and a shorter time to first rescue analgesia. Differences were most evident within the first 24 h, whereas analgesic requirements and pain scores converged thereafter.
Huan Yan et al demonstrated the feasibility of utilizing continuous low-dose epidural esketamine as a sole analgesic agent in patients undergoing endoscopic thoracic surgery. Their findings indicated that this regimen effectively reduces the incidence of chronic postoperative pain, though it is accompanied by a relatively higher incidence of acute pain. No neurotoxic effects such as dizziness or hallucinations were observed with esketamine in that study.14 The selected dose of 15 mg esketamine in this study fell within the established safety range, and its efficacy was further substantiated by the study outcomes. In the study by Lifeng Ni et al, epidural analgesia with esketamine combined with local anesthetics was associated with a higher consumption of rescue analgesics compared to the regimen combining fentanyl with local anesthetics.15 These findings align with the results of the present study. Previous studies have demonstrated that adjuvant esketamine with epidural morphine (0.05 mg/mL morphine in 0.1% ropivacaine solution) significantly decreases the required dose of postoperative epidural analgesia.16 Compared with morphine alone, epidural ketamine combined with morphine provided a longer time to first rescue analgesia, while the total postoperative epidural morphine consumption remained comparable.17 Huanyu Luo et al reported that the adjunctive use of esketamine in epidural analgesia was associated with reduced postoperative pain scores and a decreased requirement for rescue analgesics.18 It should be noted, however, that their study did not assess the duration of analgesia after a single dose, which is a key determinant of clinical utility for a bolus analgesic.
A recent meta-analysis assessing the efficacy and safety of neuraxial hydromorphone indicated the limited research evidence available on the safety and efficacy of epidural hydromorphone.19 Previous studies have reported that the potency ratio between epidural and intravenous anesthetic analgesics ranges from 5:1 to 10:1. While the estimated conversion of morphine remains relatively conservative, that of hydromorphone tends to be more aggressive.20 This study demonstrated that the epidural administration of hydromorphone (0.5 mg) provides effective analgesia. In their study of epidural analgesia in orthopedic surgery, Spencer et al demonstrated that hydromorphone is an effective agent for achieving analgesia.21 A previous study reported that in patients undergoing open thoracic, abdominal, or perineal surgery, the duration of analgesia with a single dose of epidural hydromorphone (1 mg) alone is 9.8 ± 5.5 hours,7 which is significantly shorter than the 35.5-hour duration observed in the present study. This discrepancy may be due to differences in patient selection (laparoscopic surgery in this study) and study design. In a study examining epidural analgesia in thoracoabdominal surgery, Melissa et al reported that hydromorphone and fentanyl demonstrated comparable analgesic efficacy, with hydromorphone showing a slight increase in the incidence of certain associated events.22
In our preliminary study involving 20 patients, postoperative follow-up data revealed that epidural administration of 0.2% ropivacaine alone provided an analgesic duration of approximately 2.8 ± 0.5 hours (time to first rescue analgesia). Our findings demonstrate that although the duration of single-dose epidural esketamine was shorter than that of hydromorphone, it yielded a prolonged analgesic duration relative to local anesthetic monotherapy.
Esketamine, when used at subanesthetic doses, exerts potent analgesic effects; however, it still has hallucinogenic properties.23 Notably, in our study, delirium or psychiatric symptoms were not observed in either patient group. Ketamine, provides analgesia through stereospecific binding to opioid receptors, direct action on the dorsal horn and within descending inhibitory systems and interaction with cholinergic, adrenergic, and 5-hydroxytryptamine antagonists. It also has this potential owing to its local anesthetic property.17 Esketamine hydrochloride is both water soluble and lipophilic, while its free base form is lipophilic. The water solubility of the hydrochloride salt allows for injectable use, while its lipophilicity ensures rapid blood-brain barrier crossing for CNS activity.24 Nonetheless, its precise mechanism of action remains unclear. Previous studies have demonstrated that hydromorphone, a moderately hydrophilic opioid, achieves analgesia via dual pathways involving local spinal effects and systemic supraspinal mechanisms.25,26 The shorter duration of action observed with esketamine, compared to hydromorphone, may be due to its higher lipophilicity.
Previous studies have indicated that an opioid-sparing regimen based on continuous epidural esketamine administration reduces the incidence of PONV within 48 hours postoperatively compared to epidural morphine.14 Similarly, in patients undergoing sleeve gastrectomy, an opioid-sparing multimodal analgesic approach combining ketamine and dexmedetomidine has been associated with a reduced incidence of PONV.27 However, in this study, although postoperative hydromorphone consumption was higher in group E than in group H, no significant difference in PONV incidence was observed. This may be due to the limited sample size and the predominance of low-risk patients, as defined by the established PONV risk stratification criteria.
This study indicates that, although opioid-sparing strategies are central to enhanced recovery protocols, a single-dose epidural esketamine regimen may not achieve early analgesic efficacy equivalent to that of low-dose epidural hydromorphone in the acute postoperative period. Future studies should focus on optimizing dosing regimens or developing combination strategies to more effectively integrate epidural esketamine into multimodal analgesia frameworks.
Our study has certain limitations. First, it focused on a single epidural dose of esketamine and its impact on the duration of effect, without assessing the relevant effects of continuous use. Second, the epidural esketamine dosage used was derived from prior studies and pilot tests; this study employed a single-dose regimen of esketamine and did not validate multiple dosage levels; whether dose escalation extended analgesia duration warrants further study. Third, the limited sample size within each surgical procedure may have necessitated large-scale studies to validate our findings.Finally, that opioid consumption is influenced by institutional and clinician factors, which may confound its association with true pain intensity.
Conclusion
Compared to hydromorphone, a single dose of epidural esketamine for postoperative analgesia was associated with higher hydromorphone consumption and a shorter time to first rescue analgesia. These findings indicate that single-dose epidural esketamine provides inferior analgesic efficacy compared to hydromorphone.
MMSE Statement
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (https://www.parinc.com).
Data Sharing Statement
Dataset are available upon reasonable request to the corresponding author: Chao Liang, [email protected].
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was approved by the Ethics Committee of the Zhongshan Hospital (Xiamen), Fudan University (ZSXMEC) (study number: B2024-041R),and informed consent was obtained from all participants or their relatives.
Acknowledgments
We would like to express our sincere gratitude to Xiaoqing Qian and Suqin Zhang for their dedicated efforts and invaluable contributions to patient follow-up work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Shanghai (Project’s number:23ZR1462800).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Chen YK, Boden KA, Schreiber KL. The role of regional anaesthesia and multimodal analgesia in the prevention of chronic postoperative pain: a narrative review. Anaesthesia. 2021;Suppl 76(Suppl S1):8–10. doi:10.1111/anae.15256
2. Bialka S, Copik M, Daszkiewicz A, et al. Comparison of different methods of postoperative analgesia after thoracotomy-a randomized controlled trial. J Thorac Dis. 2018;10(8):4874–4882. doi:10.21037/jtd.2018.07.88
3. Ezhevskaya AA, Mlyavykh SG, Anderson DG. Effects of continuous epidural anesthesia and postoperative epidural analgesia on pain management and stress response in patients undergoing major spinal surgery. Spine. 2013;38(15):1324–1330. doi:10.1097/BRS.0b013e318290ff26
4. Li YW, Li HJ, Li HJ, et al. Effects of two different anesthesia-analgesia methods on incidence of postoperative delirium in elderly patients undergoing major thoracic and abdominal surgery: study rationale and protocol for a multicenter randomized controlled trial. BMC Anesthesiol. 2015;15:144. doi:10.1186/s12871-015-0118-5
5. Pirie K, Doane MA, Riedel B, Myles PS. Analgesia for major laparoscopic abdominal surgery: a randomised feasibility trial using intrathecal morphine. Anaesthesia. 2022;77(4):428–437. doi:10.1111/anae.15651
6. Waurick R, Van Aken H. Update in thoracic epidural anaesthesia. Best Pract Res Clin Anaesthesiol. 2005;19(2):201–213. doi:10.1016/j.bpa.2004.12.001
7. Chestnut DH. Efficacy and safety of epidural opioids for postoperative analgesia. Anesthesiology. 2005;102(1):221–223. doi:10.1097/00000542-200501000-00031
8. Choi H, Huh J, Kim M, Moon SW, Kim KS, Hwang W. Opioid-free using ketamine versus opioid-sparing anesthesia during the intraoperative period in video-assisted thoracoscopic surgery: a randomized controlled trial. J Pers Med. 2024;14(8). doi:10.3390/jpm14080881
9. Feenstra ML, Jansen S, Eshuis WJ, van Berge Henegouwen MI, Hollmann MW, Hermanides J. Opioid-free anesthesia: a systematic review and meta-analysis. J Clin Anesth. 2023;90:111215. doi:10.1016/j.jclinane.2023.111215
10. Li K, Chai Z, Deng C, et al. Effects of epidural esketamine versus sufentanil on labor analgesia and postpartum depression: a retrospective cohort study. BMC Anesthesiol. 2025;25(1):6. doi:10.1186/s12871-024-02846-6
11. Yang Y, Zhang Y, Zhou G, Yang Z, Yan H, Zhang J. Efficacy of epidural esketamine on postoperative sleep quality after laparoscopic and robotic lower abdominal surgeries: a study protocol for randomised, double-blind, controlled trial. BMJ Open. 2024;14(2):e081589. doi:10.1136/bmjopen-2023-081589
12. Prabhakar P, Mariappan R, Moorthy RK, Nair BR, Karuppusami R, Lionel KR. Adding ketamine to epidural morphine does not prolong postoperative analgesia after lumbar laminectomy or discectomy. J Neurosurg Anesthesiol. 2024;36(3):244–251. doi:10.1097/ANA.0000000000000914
13. Schnider TW, Minto CF, Gambus PL, et al. The influence of method of administration and covariates on the pharmacokinetics of propofol in adult volunteers. Anesthesiology. 1998;88(5):1170–1182. doi:10.1097/00000542-199805000-00006
14. Yan H, Chen W, Chen Y, et al. Opioid-free versus opioid-based anesthesia on postoperative pain after thoracoscopic surgery: the use of intravenous and epidural esketamine. Anesth Analg. 2023;137(2):399–408. doi:10.1213/ANE.0000000000006547
15. Ni L, Yao S, Wu Y, et al. Epidural dexmedetomidine or esketamine versus fentanyl to decrease ropivacaine use for labor analgesia: a randomized non-inferiority study. Heliyon. 2024;10(9):e30218. doi:10.1016/j.heliyon.2024.e30218
16. Lai HC, Hsieh CB, Wong CS, Yeh CC, Wu ZF. Preincisional and postoperative epidural morphine, ropivacaine, ketamine, and naloxone treatment for postoperative pain management in upper abdominal surgery. Acta Anaesthesiol Taiwan. 2016;54(3):88–92. doi:10.1016/j.aat.2016.10.004
17. Subramaniam B, Subramaniam K, Pawar DK, Sennaraj B. Preoperative epidural ketamine in combination with morphine does not have a clinically relevant intra- and postoperative opioid-sparing effect. Anesth Analg. 2001;93(5):1321–1326. doi:10.1097/00000539-200111000-00059
18. Luo H, Yang Y, He Z, et al. Esketamine as an epidural adjuvant for postoperative analgesia in gynecological malignancy surgery: a randomized trial. J Pain Res. 2025;18:4349–4359. doi:10.2147/jpr.S533143
19. Grape S, El-Boghdadly K, Jaques C, Albrecht E. Efficacy and safety of neuraxial hydromorphone: a systematic review and meta-analysis with trial sequential analysis. J Clin Anesth. 2024;99:111664. doi:10.1016/j.jclinane.2024.111664
20. Gorlin AW, Rosenfeld DM, Maloney J, Wie CS, McGarvey J, Trentman TL. Survey of pain specialists regarding conversion of high-dose intravenous to neuraxial opioids. J Pain Res. 2016;9:693–700. doi:10.2147/jpr.S113216
21. Liu SS, Bieltz M, Wukovits B, John RS. Prospective survey of patient-controlled epidural analgesia with bupivacaine and hydromorphone in 3736 postoperative orthopedic patients. Reg Anesth Pain Med. 2010;35(4):351–354. doi:10.1097/aap.0b013e3181e6ac3a
22. Nguyen MN, Zimmerman LH, Meloche K, et al. Hydromorphone vs fentanyl for epidural analgesia and anesthesia. Am J Surg. 2016;211(3):565–570. doi:10.1016/j.amjsurg.2015.12.003
23. Olofsen E, Kamp J, Henthorn TK, et al. Ketamine psychedelic and antinociceptive effects are connected. Anesthesiology. 2022;136(5):792–801. doi:10.1097/aln.0000000000004176
24. Domino EF. Taming the ketamine tiger. 1965. Anesthesiology. 2010;113(3):678–684. doi:10.1097/ALN.0b013e3181ed09a2
25. Goodarzi M. Comparison of epidural morphine, hydromorphone and fentanyl for postoperative pain control in children undergoing orthopaedic surgery. Paediatr Anaesth. 1999;9(5):419–422. doi:10.1046/j.1460-9592.1999.00370.x
26. Ummenhofer WC, Arends RH, Shen DD, Bernards CM. Comparative spinal distribution and clearance kinetics of intrathecally administered morphine, fentanyl, alfentanil, and sufentanil. Anesthesiology. 2000;92(3):739–753. doi:10.1097/00000542-200003000-00018
27. Ziemann-Gimmel P, Goldfarb AA, Koppman J, Marema RT. Opioid-free total intravenous anaesthesia reduces postoperative nausea and vomiting in bariatric surgery beyond triple prophylaxis. Br J Anaesth. 2014;112(5):906–911. doi:10.1093/bja/aet551
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Opioid-Free Anesthesia with Esketamine Combined with Iliac Fascia Block in Elderly Patients Undergoing Hip Surgery
Luo LL, Xiao R, Zhang JP, Xi WF, Xu GH, Yuan H
Drug Design, Development and Therapy 2025, 19:3337-3349
Published Date: 28 April 2025
A Prospective, Randomized Trial Comparing Hydromorphone and Nalbuphine for Postcesarean Patient-Controlled Analgesia and Developing a Risk Prediction Model for Inadequate Analgesia
Zhang K, Sun J, Zhang C, Jiao B, Zhang W, Yu S, Cao X, Zhou Z, Zhang G, Zhang X
Drug Design, Development and Therapy 2025, 19:9759-9778
Published Date: 1 November 2025
Effect of Intrathecal Hydromorphone on the Duration and Efficacy of Postoperative Analgesia in Patients Undergoing Benign Anorectal Surgery: Protocol for a Randomized, Double-Blind, Controlled Trial
Cao Y, Zhou Y, Zhou D, Xiong C, Fu L, Chen X, Zhang X
Journal of Pain Research 2026, 19:569284
Published Date: 26 February 2026
Hydromorphone is Noninferior to Dexamethasone as an Adjuvant to Ropivacaine for Transversus Abdominis Plane Block After Laparoscopic Colorectal Cancer Surgery: A Randomized, Double-Blind Trial
Zhao L, Wang Y, Guo Q, An Q, Wu M, Fan C, Guo Z
Journal of Pain Research 2026, 19:581520
Published Date: 5 March 2026
Efficacy and Safety of Ultrasound-Guided Erector Spinae Plane Block at Different Injection Depths for Percutaneous Kyphoplasty: A Randomized Controlled Trial
Liu Y, Yu Y, Gao X, Wang Q, Wang Y, Xia X
Drug Design, Development and Therapy 2026, 20:601168
Published Date: 16 June 2026