Back to Journals » Drug Design, Development and Therapy » Volume 19
A Prospective, Randomized Trial Comparing Hydromorphone and Nalbuphine for Postcesarean Patient-Controlled Analgesia and Developing a Risk Prediction Model for Inadequate Analgesia
Authors Zhang K ![]() , Sun J, Zhang C, Jiao B, Zhang W, Yu S, Cao X, Zhou Z, Zhang G, Zhang X
, Sun J, Zhang C, Jiao B, Zhang W, Yu S, Cao X, Zhou Z, Zhang G, Zhang X ![]()
Received 2 July 2025
Accepted for publication 26 October 2025
Published 1 November 2025 Volume 2025:19 Pages 9759—9778
DOI https://doi.org/10.2147/DDDT.S551186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Tin Wui Wong
Kaiwen Zhang,1,* Jiaoli Sun,1,* Caixia Zhang,2 Bo Jiao,1 Wencui Zhang,1 Shangchen Yu,1 Xueqin Cao,1 Zhiqiang Zhou,1 Guanglei Zhang,1 Xianwei Zhang1
1Department of Anesthesiology and Pain Medicine,Hubei Key Laboratory of Geriatric Anesthesia and Perioperative Brain Health, and Wuhan Clinical Research Center for Geriatric Anesthesia, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Anesthesiology, Wuhan No. 1 Hospital, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guanglei Zhang, Department of Anesthesiology and Pain Medicine, Hubei Key Laboratory of Geriatric Anesthesia and Perioperative Brain Health, and Wuhan Clinical Research Center for Geriatric Anesthesia, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, No. 1095 Jiefang Avenue, Qiaokou District, Wuhan, Hubei Province, 430030, People’s Republic of China, Email [email protected] Xianwei Zhang, Department of Anesthesiology and Pain Medicine, Hubei Key Laboratory of Geriatric Anesthesia and Perioperative Brain Health, and Wuhan Clinical Research Center for Geriatric Anesthesia, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, No. 1095 Jiefang Avenue, Qiaokou District, Wuhan, Hubei Province, 430030, People’s Republic of China, Email [email protected]
Purpose: Effective postoperative analgesia is essential for maternal recovery following cesarean delivery. Hydromorphone and nalbuphine are commonly used opioids with differing pharmacologic properties, but direct comparisons in postcesarean patient-controlled analgesia (PCA) are limited. This study aimed to compare the analgesic efficacy and safety of hydromorphone versus nalbuphine and to develop a predictive model for inadequate analgesia.
Patients and Methods: In this prospective, randomized, double-blind clinical trial conducted from December 2024 to March 2025, 212 women undergoing elective cesarean section under spinal anesthesia were randomized (1:1) to receive hydromorphone (0.1 mg/mL) or nalbuphine (1 mg/mL) via standardized intravenous PCA. The primary outcome was the incidence of inadequate analgesia within 24 hours, defined as a numerical rating scale (NRS) score ≥ 4 at rest or during movement. Secondary outcomes included adverse events, PCA consumption, and recovery indicators. Multivariable logistic regression was used to identify predictors of inadequate analgesia, and a nomogram was constructed and internally validated.
Results: Nalbuphine was associated with a significantly lower incidence of inadequate analgesia than hydromorphone (14.2% vs 26.4%; P = 0.026), as well as reduced nausea and vomiting (18.9% vs 32.1%; P = 0.001) and pruritus (0% vs 5.7%; P = 0.029). Independent predictors of inadequate analgesia included PCA regimen (OR, 0.30; P = 0.026), gestational diabetes mellitus (OR, 4.40; P = 0.007), blood type AB (OR, 3.80; P = 0.043), and preoperative anxiety (OR, 0.20; P = 0.044). The predictive model showed good discrimination (AUC = 0.754).
Conclusion: Nalbuphine demonstrated superior analgesia and fewer adverse effects compared with hydromorphone for postcesarean PCA. The developed predictive model may support individualized pain management by identifying patients at risk for inadequate analgesia.
Keywords: postoperative analgesia, patient-controlled analgesia, hydromorphone, nalbuphine, predictive model
Introduction
Cesarean section (CS) is one of the most commonly performed surgical procedures worldwide, with its prevalence particularly prominent in China. A global survey conducted by the World Health Organization (WHO) during 2007–2008 reported a peak CS rate of 46.2%, placing China among the highest globally.1 While CS plays a vital role in managing dystocia, reducing perinatal mortality, and ensuring maternal safety.2 It is also associated with surgical trauma and intense postoperative pain, which can significantly hinder maternal recovery and adversely affect psychological well-being.3 Our own previous study found that the overall rate of inadequate analgesia after cesarean delivery was 24.25%.4 These findings underscore the urgent need to optimize postoperative analgesic strategies and identify patients at high risk for insufficient pain control.
To optimize postcesarean recovery and reduce opioid-related side effects, clinical guidelines recommend a multimodal analgesia strategy comprising neuraxial opioids, scheduled non-opioid agents such as NSAIDs and acetaminophen, and peripheral nerve blocks when indicated. Among these components, intravenous patient-controlled analgesia (PCA) remains a key modality,5 it offers stable plasma drug levels, flexible dose titration, and greater maternal autonomy, thereby facilitating individualized pain control and enhancing early postoperative recovery.6
While traditional opioids such as morphine and sufentanil are effective, their use in PCA is often limited by dose accumulation and an increased risk of adverse events such as respiratory depression, nausea, and vomiting.7 Consequently, there has been growing interest in alternative opioids such as nalbuphine and hydromorphone, due to their distinct pharmacological properties and potential safety advantages in postcesarean analgesia.
Nalbuphine, a κ-opioid receptor agonist and μ-opioid receptor antagonist, has demonstrated promising efficacy across both intravenous and neuraxial modalities. Compared with sufentanil, multiple randomized and retrospective studies have reported that nalbuphine provides comparable or superior analgesia, particularly in relieving resting pain, uterine contraction pain, and movement-related pain, while significantly reducing the incidence of nausea, vomiting, and pruritus, and enhancing maternal satisfaction.8–11 One randomized controlled trial showed that intravenous PCA with nalbuphine yielded superior pain relief over sufentanil without increasing total opioid consumption or adverse events.8 A large cohort study of multiparas similarly found better visceral pain control and fewer side effects with nalbuphine.9 In addition, several studies support its use in combination regimens—such as with sufentanil or dexmedetomidine—to enhance multimodal analgesia and accelerate recovery.10,11
Hydromorphone, a semisynthetic μ-opioid receptor agonist, is also increasingly used in the cesarean setting. When administered intrathecally, hydromorphone has been shown to be non-inferior to morphine for cesarean analgesia, with comparable pain scores, opioid requirements, and recovery quality.12 Beyond neuraxial use, both intravenous and epidural hydromorphone have proven effective in multimodal strategies, serving as either a primary or adjunct analgesic, alone or in combination with agents like butorphanol.13,14 A head-to-head randomized trial further demonstrated that hydromorphone was more effective than tramadol in controlling visceral pain after repeat cesarean delivery.15
Although both hydromorphone and nalbuphine have been widely used for postcesarean analgesia, direct comparisons in the context of intravenous patient-controlled analgesia remain limited, particularly due to the lack of large-scale, prospective randomized controlled trials. As a result, their relative efficacy, adverse effect profiles, and recovery outcomes have not been comprehensively evaluated. This randomized controlled trial was designed to systematically compare the clinical efficacy and safety profiles of hydromorphone and nalbuphine in postcesarean PCA, identify independent predictors of inadequate analgesia, and develop a concise, individualized risk prediction model to guide postoperative pain management. Compared with our previous predictive model,4 which lacked intervention-level comparisons, the current study enhances clinical applicability by implementing standardized interventions and directly evaluating commonly used opioid regimens.
Materials and Methods
Ethics Statement
This prospective, randomized, double-blind study was conducted in accordance with the Declaration of Helsinki and applicable national regulations. Ethical approval was granted by the Institutional Review Board of Tongji Hospital, Huazhong University of Science and Technology (Approval No.TJ-IRB202409103). The trial was registered at ClinicalTrials.gov (NCT06716359). Written informed consent was obtained from all participants prior to enrollment.
Study Design and Randomization
The study flowchart (Figure 1) illustrates the screening, randomization, and analysis procedures. The trial was conducted in the Department of Anesthesiology, Tongji Hospital, from December 2024 and March 2025. Eligible parturients were randomized to either the nalbuphine group (Group N, PCA concentration: 1 mg/mL; nalbuphine hydrochloride injection,Yichang Renfu Pharmaceutical Co., Ltd., Yichang, Hubei, China) or the hydromorphone group (Group H, PCA concentration: 0.1 mg/mL; hydromorphone hydrochloride injection,Yichang Renfu Pharmaceutical Co., Ltd., Yichang, Hubei, China). The equianalgesic dose ratio of hydromorphone to nalbuphine was set at approximately 1:10, based on a recent network meta-analysis of opioids used in patient-controlled analgesia, which provided comparative analgesic potencies for various intravenous opioids.16 This ratio aligns with clinical practice and literature-reported relative potencies. Randomization was performed using a computer-generated list (Microsoft Excel), and allocation was concealed in sealed opaque envelopes. PCA solutions were prepared by a pharmacist not involved in patient care. The PCA pumps were identical in appearance, volume, and labeling across groups, and patients were blinded to their group assignment. Both anesthesiologists and outcome assessors were blinded to group assignment.
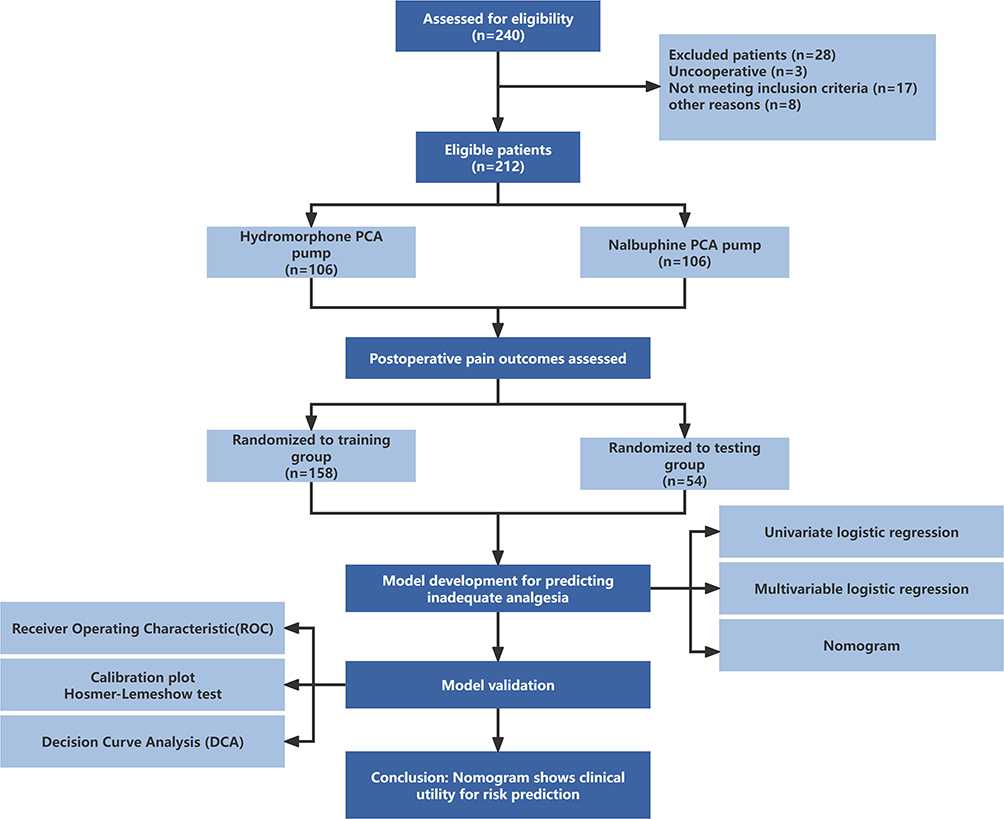 |
Figure 1 Study Design and Predictive Model Construction Flowchart. This flowchart illustrates the study design and analytical procedures. A total of 240 patients were initially enrolled. After applying inclusion and exclusion criteria and removing cases with incomplete data, 212 patients were included in the final analysis and randomized into two groups: hydromorphone PCA (n = 106) and nalbuphine PCA (n = 106). The dataset was further randomly divided into a training cohort (n = 158) and a validation cohort (n = 54) at a 3:1 ratio for model development and validation. Key analytical steps included univariate and multivariable logistic regression analyses, nomogram construction, and model performance evaluation via ROC curve, calibration plot, and DCA. Abbreviations: DCA, decision curve analysis; PCA, patient-controlled analgesia; ROC, receiver operating characteristic. |
Sample Size Calculation
Sample size was calculated using PASS software (version 11.0.7, NCSS, LLC, Kaysville, UT, USA) based on a two-sided chi-square test comparing two proportions. With 90% power to detect a significant intergroup difference at α = 0.05 and accounting for a 10% potential attrition rate, the required total sample size was estimated to be 212 patients. A total of 240 patients were assessed for eligibility.
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Age 18–50 years; (2) American Society of Anesthesiologists (ASA) physical status II–III; (3) Full-term singleton pregnancy scheduled for elective cesarean section via low transverse incision; (4) Voluntary participation with signed informed consent.
Exclusion Criteria
(1) History of central nervous system or psychiatric disorders; (2) History of substance or alcohol abuse; (3) Poor compliance or inability to complete follow-up; (4) Participation in another clinical trial within the past 3 months; (5) Severe obstetric complications during delivery; (6) Any other reason deemed inappropriate by the investigators.
Anesthesia and Analgesia Protocol
Baseline demographics and psychological status (Pain Catastrophizing Scale [PCS], Generalized Anxiety Disorder 7-item scale [GAD-7], and Edinburgh Postnatal Depression Scale 10-item version [EPDS-10]) were assessed after obtaining informed consent. Spinal anesthesia was performed at the L3–L4 interspace using 2.5–3 mL of 0.75% hyperbaric ropivacaine to achieve a T4–T5 sensory block. After fetal delivery, flurbiprofen axetil 50 mg and dexamethasone 5 mg were administered intravenously. PCA infusion was initiated postoperatively upon confirmation of adequate motor and sensory block regression. The PCA settings were: continuous infusion rate 2 mL/h, bolus 2 mL, lockout interval 15 minutes, maximum dose 10 mL/h, and total volume 100 mL. Diclofenac sodium suppository (50 mg) was administered as rescue analgesia if necessary.
Data Collection and Outcomes
Pain intensity was assessed using the Numeric Rating Scale (NRS), and all scores were self-reported by patients and recorded by blinded assessors. NRS scores were evaluated at four fixed timepoints within the first 24 hours after surgery: 4, 8, 12, and 24 hours postoperatively. At each timepoint, both static and dynamic (specifically turning) NRS scores were recorded. Inadequate analgesia was defined as NRS ≥4 at any single timepoint during the first 24 hours postoperatively, either at rest or during movement. Additional data collected within the first 24 hours postoperatively included PCA usage, adverse events, psychological assessments, and recovery indicators. Adverse effects (respiratory depression, rash, constipation, pruritus, nausea/vomiting) were documented and treated as needed. Additional postoperative outcomes included total PCA dosage, number of bolus attempts, use of rescue analgesics, Ramsay sedation score, analgesia satisfaction score (1–10), GAD-7 and EPDS-10 scores, time to first ambulation and breastfeeding, and length of hospital stay. All secondary outcomes except for length of hospital stay were assessed at the 24-hour postoperative timepoint.
Primary and Secondary Outcomes
Primary outcome: Incidence of inadequate analgesia within 24 hours, defined as:
Static inadequate analgesia: NRS ≥ 4 at rest at any single timepoint
Dynamic inadequate analgesia: NRS ≥ 4 during movement (turning) at any single timepoint
Overall inadequate analgesia: NRS ≥ 4 at any single timepoint, either at rest or during movement
Secondary outcomes included weight-adjusted PCA dosage, number of PCA boluses, rescue medication use, Ramsay sedation score, patient satisfaction, GAD-7 and EPDS-10 scores, time to first ambulation and breastfeeding, hospital stay duration, and incidence of adverse events.
Nomogram Construction and Model Validation
The dataset was randomly divided into a training set and a validation set in a 3:1 ratio using R software (version 4.2.3). Univariate logistic regression was performed to evaluate preoperative and intraoperative factors, and variables with a P value < 0.1 were entered into a multivariable logistic regression model. The optimal model was selected using forward stepwise selection based on the minimum Akaike Information Criterion (AIC).17 A nomogram was subsequently constructed. Model performance was evaluated using receiver operating characteristic (ROC) curves, calibration plots, and decision curve analysis (DCA).
Statistical Analysis
Statistical analyses were performed using SPSS software (version 21.0, IBM Corp., Armonk, NY, USA). Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± standard deviation (SD) and compared using the independent samples t-test. Non-normally distributed data were presented as median (interquartile range, IQR) and compared using the Mann–Whitney U-test. Categorical variables were summarized as counts (percentages) and compared using the chi-square test or Fisher’s exact test when appropriate (ie, when expected cell counts were <5). Multiple hypothesis testing correction was performed using the Benjamini-Hochberg procedure to control the false discovery rate (FDR). A P value < 0.05 was considered statistically significant.
Results
Patient Enrollment and Baseline Characteristics
A total of 240 parturients scheduled for elective cesarean delivery were assessed for eligibility. Among them, 28 patients were excluded, including 3 due to non-cooperation, 17 for not meeting the inclusion criteria, and 8 who underwent conversion to general anesthesia. Ultimately, 212 patients were enrolled and randomly assigned in a 1:1 ratio to either the hydromorphone PCA group (H group, n = 106) or the nalbuphine PCA group (N group, n = 106). All participants completed the prospective assessment of postoperative analgesic outcomes (Figure 1).
To ensure comparability between groups prior to outcome assessment, we analyzed the baseline demographic data, preoperative psychological status, and intraoperative variables. No significant differences were observed between the two groups, indicating well-balanced baseline characteristics (Table 1).
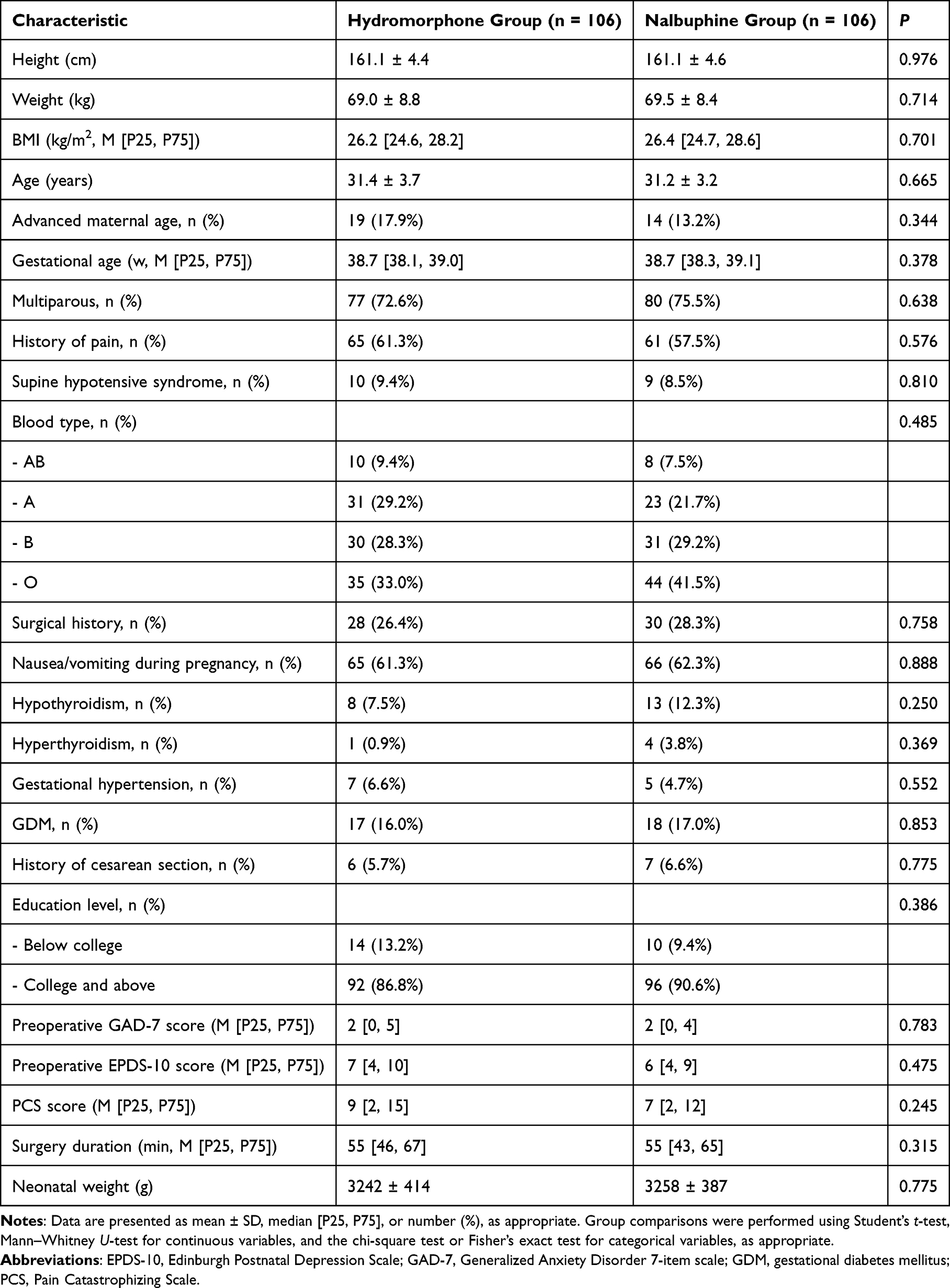 |
Table 1 Baseline Characteristics, Preoperative, and Intraoperative Data |
Postoperative Analgesic Outcomes
Postoperative analgesia was assessed by the incidence of inadequate analgesia (defined as NRS ≥ 4 within 24 hours), PCA usage, and the need for rescue analgesia.
Inadequate analgesia occurred predominantly during movement. A total of 28 out of 106 patients (26.4%) in the hydromorphone group (H group) experienced inadequate analgesia during movement, compared to 15 out of 106 patients (14.2%) in the nalbuphine group (N group), indicating a significantly higher incidence in the H group (RR = 1.87, 95% CI: 1.06–3.29; RD = 12.3%, 95% CI: 1.6%–23.0%; P = 0.026; Figure 2A). In contrast, the incidence of inadequate analgesia at rest was low and comparable between the two groups (1/106 in each group, 0.94%). The overall incidence of inadequate analgesia—defined as NRS ≥ 4 either at rest or during movement—was identical to the movement-related data, further highlighting the inferior efficacy of hydromorphone in controlling activity-related pain.
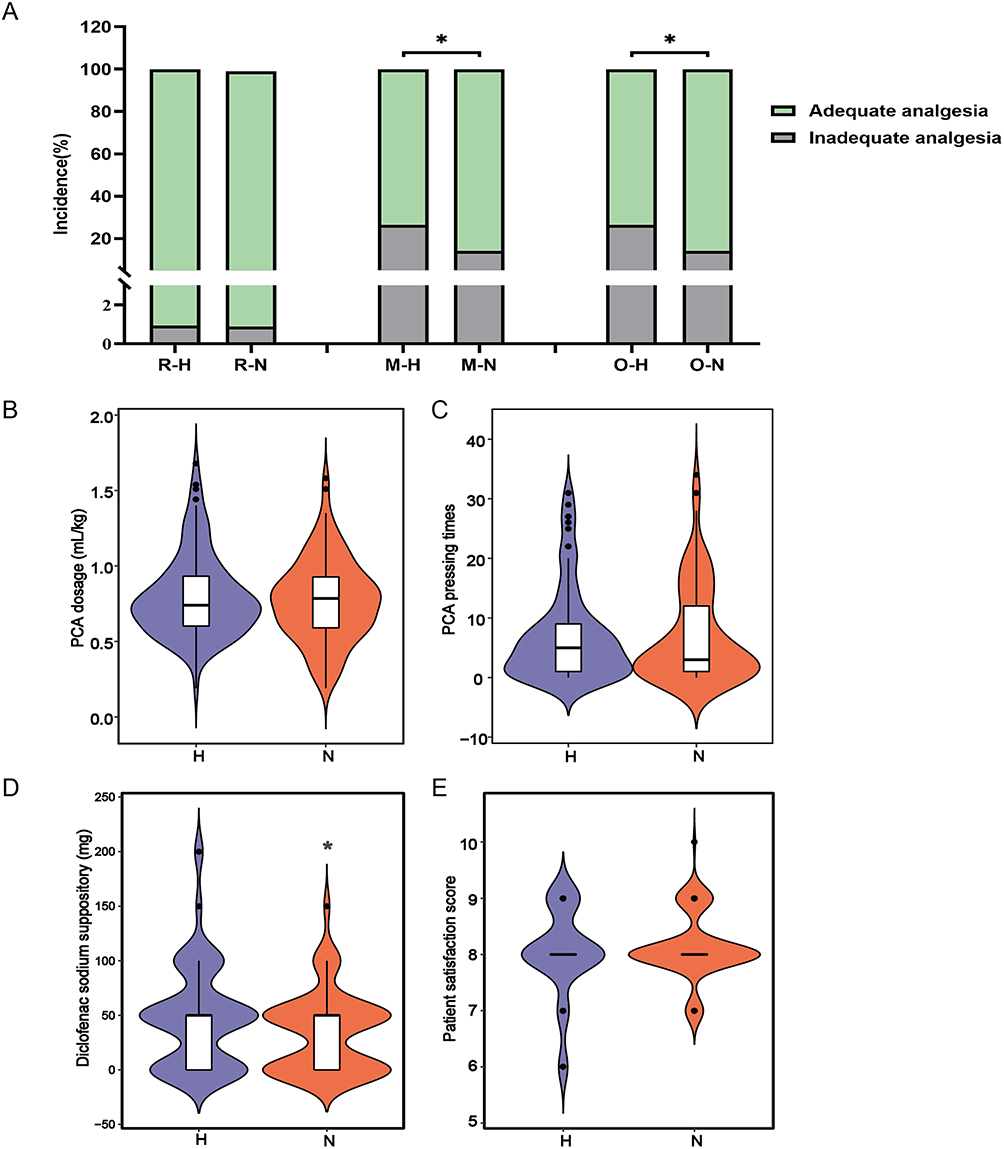 |
Figure 2 Postoperative pain and related outcomes. (A) Incidence of inadequate analgesia (NRS ≥ 4); (B) Total PCA dosage adjusted for body weight (mL/kg); (C) Number of PCA pressings; (D) Dosage of rescue diclofenac sodium suppository (mg); (fE) Patient satisfaction score (0–10). *P < 0.05 indicates a statistically significant difference. Abbreviations: H, Hydromorphone group; N, Nalbuphine group; M, Movement state; O, Overall (either resting or movement); R, Resting state. |
There were no statistically significant differences between the two groups in terms of PCA consumption (Figure 2B) and the number of PCA presses (Figure 2C). However, the use of diclofenac suppositories as rescue analgesia was significantly higher in the H group (P = 0.043; Figure 2D). Additionally, no significant differences were observed in patient satisfaction scores (Figure 2E).
Postoperative Recovery, Adverse Reactions, and Psychological Outcomes (Table 2)
Sedation and Recovery Indicators
The majority of patients in both groups had a Ramsay sedation score < 4 within 24 hours postoperatively, with no significant difference between groups (H group: 95.3% vs N group: 98.1%; P = 0.445; adjusted P = 0.761). Early ambulation (≤ 24 h) occurred in 56.6% of patients in the H group and 61.3% in the N group (P = 0.485; adjusted P = 0.761), while early breastfeeding initiation (≤ 24 h) was reported in 14.2% and 15.1% of patients, respectively (P = 0.846; adjusted P = 0.931). The distribution of hospital length of stay was similar between the two groups, with the majority discharged within 3 to 4 days (P = 0.590; adjusted P = 0.811).
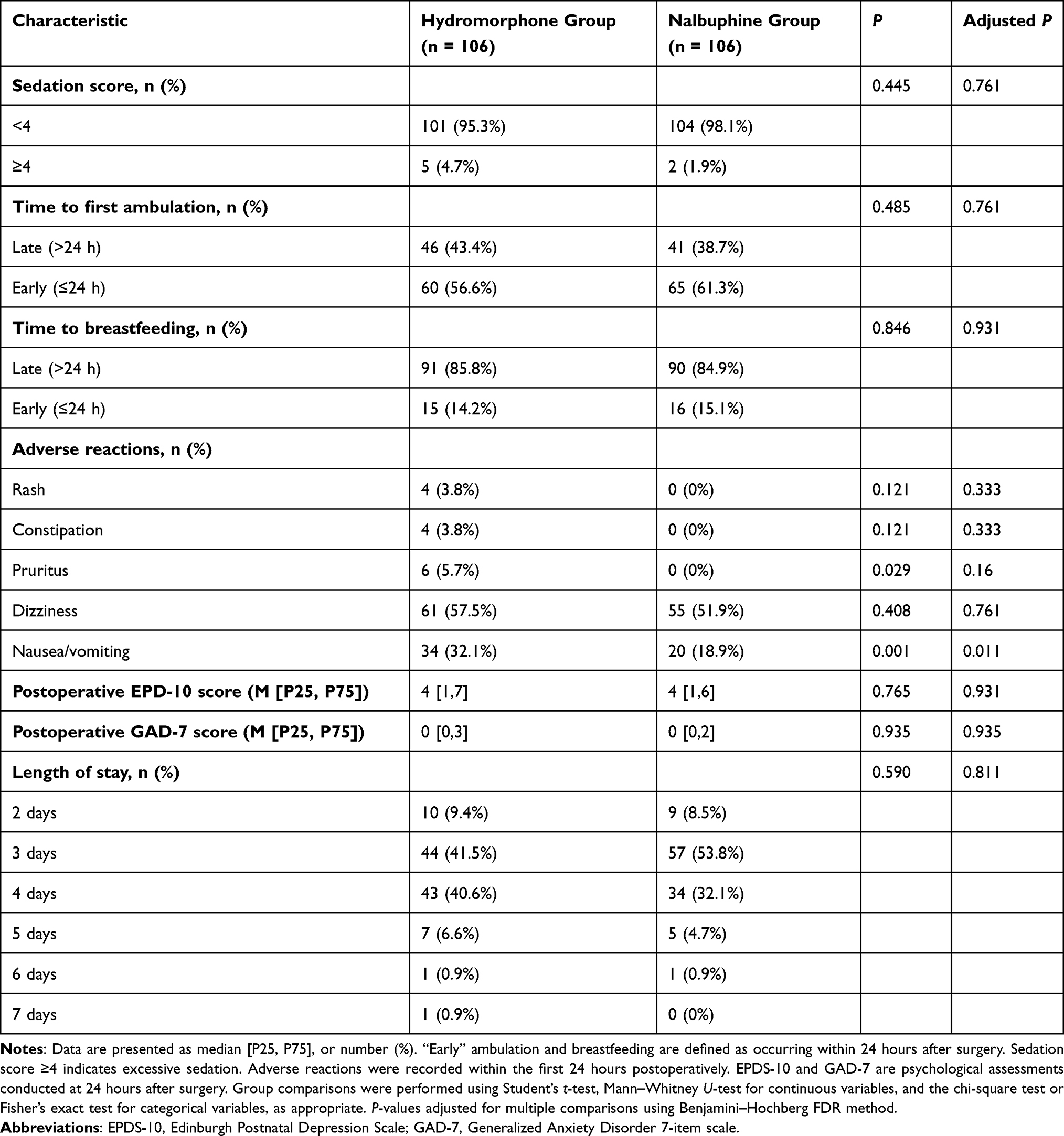 |
Table 2 Postoperative Recovery, Adverse Reactions, and Psychological Outcomes |
Adverse Reactions
The incidence of nausea and vomiting was significantly higher in the H group compared to the N group (32.1% vs 18.9%; P = 0.001), and this difference remained statistically significant after FDR correction (adjusted P = 0.011). Although pruritus was more frequent in the H group (5.7% vs 0%; P = 0.029), this difference did not remain significant after FDR adjustment (adjusted P = 0.16). Other adverse events, including rash (3.8% vs 0%) and constipation (3.8% vs 0%), showed non-significant differences between groups (P = 0.121; adjusted P = 0.333 for both). No significant difference was found in dizziness (57.5% vs 51.9%; P = 0.408; adjusted P = 0.761), and no cases of respiratory depression were reported in either group.
Psychological Outcomes
Postoperative psychological assessments showed no significant between-group differences. The median [IQR] EPDS-10 scores were 4 [1–7] in the H group and 4 [1–6] in the N group (P = 0.765; adjusted P = 0.931), while GAD-7 scores were 0 [0–3] and 0 [0–2], respectively (P = 0.935; adjusted P = 0.935).
Baseline Characteristics of Training and Validation Cohorts
Baseline characteristics were compared between the training and validation cohorts. A total of 158 patients were assigned to the training cohort, and 54 patients to the validation cohort. Details are presented in (Table 3).
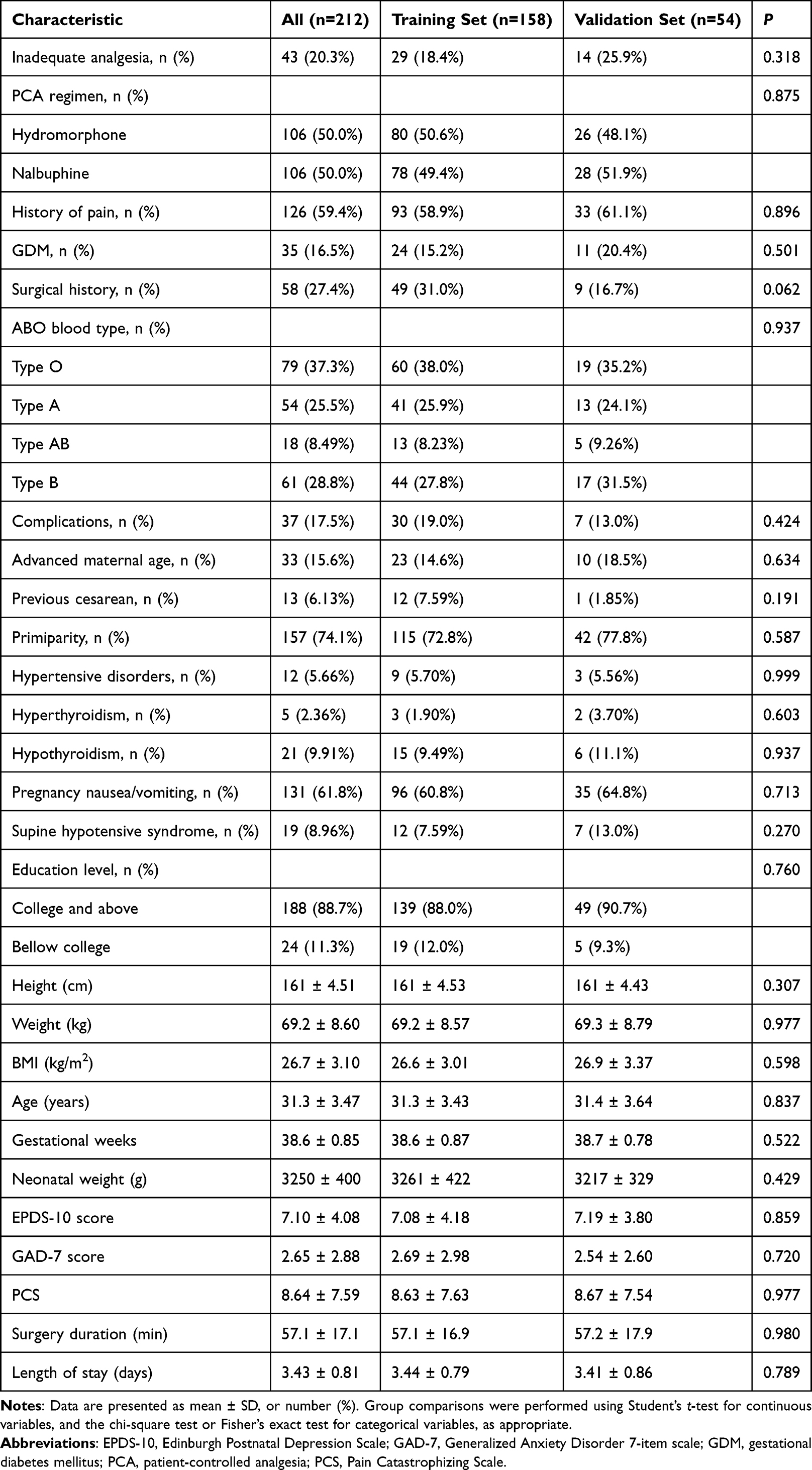 |
Table 3 Baseline Characteristics of Training and Validation Cohorts |
Predictive Factors for Postoperative Inadequate Analgesia
To identify independent predictors of inadequate postoperative analgesia—defined as a NRS score ≥4 at any time within 24 hours postoperatively, either at rest or during movement—a univariable logistic regression analysis was conducted including demographic, clinical, and perioperative variables (Table 4).
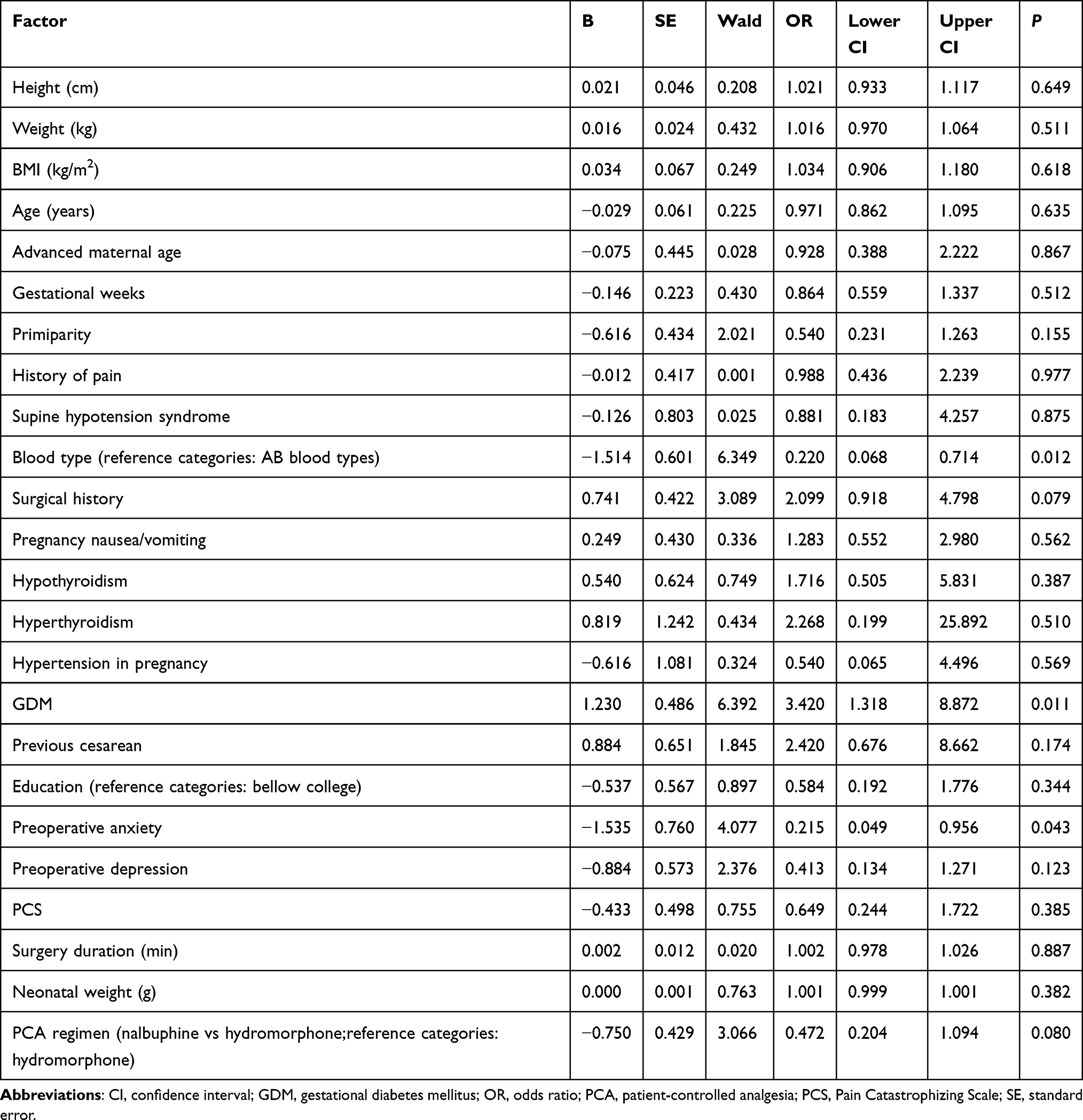 |
Table 4 Univariate Logistic Regression Analysis for Predicting Inadequate Postoperative Analgesia |
In the univariable analysis, gestational diabetes mellitus (GDM) (OR = 3.42, 95% CI: 1.32–8.87, P = 0.011), preoperative anxiety (OR = 0.22, 95% CI: 0.05–0.96, P = 0.043), and blood type AB (OR = 0.22, 95% CI: 0.07–0.71, P = 0.012) were significantly associated with inadequate analgesia. Variables with P < 0.1 were included in a multivariable logistic regression model (Figure 3). The final analysis identified the following independent predictors: PCA regimen (nalbuphine vs hydromorphone: OR = 0.30, 95% CI: 0.10–0.88, P = 0.026), preoperative anxiety (OR = 0.20, 95% CI: 0.04–0.90, P = 0.044), GDM (OR = 4.40, 95% CI: 1.55–12.7, P = 0.007), and blood type AB (OR = 3.80, 95% CI: 1.04–14.0, P = 0.043). Although surgical history did not reach statistical significance (OR = 2.10, 95% CI: 0.82–5.32, P = 0.121), the relatively high odds ratio suggests a potential association that may warrant further investigation. These findings highlight the importance of considering psychological, pharmacological, genetic, and metabolic factors when predicting analgesic outcomes following cesarean delivery. The significant variables were incorporated into the nomogram model to facilitate individualized risk assessment.
 |
Figure 3 Multivariable Logistic Regression for Predicting Inadequate Analgesia. The forest plot displays the independent predictors of inadequate analgesia (NRS ≥ 4 at rest or during movement within 24 hours postoperatively). Significant predictors included preoperative anxiety (OR = 0.2, 95% CI: 0.04–0.96, P = 0.044), PCA regimen (OR = 0.3, 95% CI: 0.14–0.88, P = 0.026), blood type AB (OR = 3.8, 95% CI: 1.04–14.03, P = 0.043), and gestational diabetes mellitus (OR = 4.4, 95% CI: 1.5–12.7, P = 0.007). A red dashed line represents the reference value (OR = 1). Abbreviations: CI, confidence intervals; GDM, gestational diabetes mellitus. OR, odds ratio. |
Construction of the Nomogram
To further evaluate the primary predictors of inadequate postoperative analgesia and provide intuitive clinical decision support, a multivariable logistic regression model was developed using stepwise selection based on the lowest Akaike information criterion (AIC = 139). The final model included GDM, Preoperative GAD-7 score, PCA regimen, and blood type AB. An interactive nomogram was subsequently constructed (Figure 4), which may offer practical reference for postoperative pain management and aid in identifying high-risk patients.
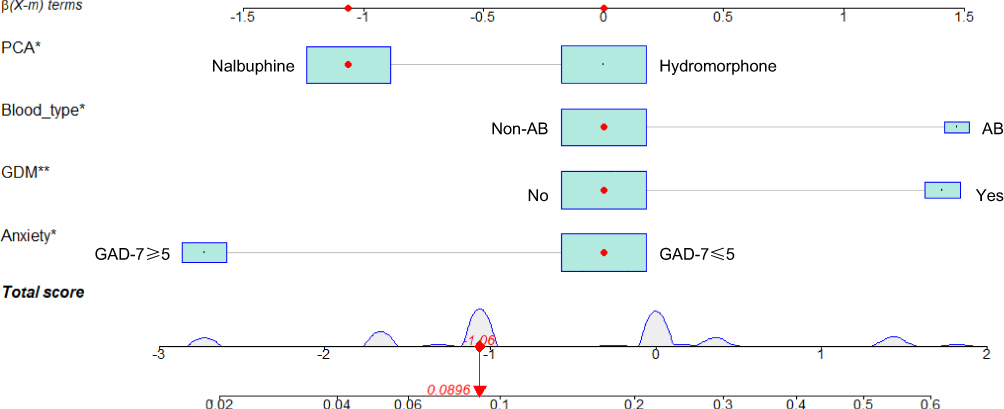 |
Figure 4 Interactive Nomogram for Predicting the Risk of Inadequate Postoperative Analgesia. This interactive nomogram visually represents a logistic regression model used to predict the risk of inadequate analgesia after cesarean section. The included predictors are PCA regimen (nalbuphine vs hydromorphone), preoperative anxiety score (GAD-7), GDM, and blood type AB. Each variable contributes a point value, and the total cumulative score corresponds to the predicted probability of inadequate analgesia, defined as NRS ≥ 4 at any time point within 24 hours postoperatively during rest or movement. The red dots indicate the specific values and point contributions for an example patient (ID 40). This tool supports individualized risk assessment and informs postoperative analgesia optimization. GAD-7, Generalized Anxiety Disorder 7-item scale.* P < 0.05; ** P < 0.01. P-values were derived from the multivariable logistic regression model. |
As shown in the figure, the β coefficient for the hydromorphone PCA regimen was positive, indicating a potential association with increased risk of inadequate analgesia, whereas the coefficient for nalbuphine was negative, suggesting a potential protective association. Both AB blood type and GDM exhibited positive β values, indicating their association with elevated risk. Preoperative anxiety also emerged as an important factor associated with inadequate analgesia, reflecting the complex impact of psychological status on pain perception and analgesic needs.
Based on the cumulative score from the nomogram, a higher total score corresponds to a greater predicted probability of inadequate analgesia. This model offers a quantitative tool for individualized risk prediction and underscores the importance of targeted clinical intervention among high-risk populations to optimize postoperative analgesic strategies.
Model Validation
To evaluate the performance of the predictive model across datasets, ROC curves, calibration plots, and DCA were generated for both the training and validation cohorts.
In the training cohort, the ROC curve (Figure 5A) demonstrated good discrimination, with an area under the curve (AUC) of 0.754 (95% CI: 0.651–0.857), a specificity of 0.589, and a sensitivity of 0.793. In the validation cohort (Figure 5B), the AUC was 0.659 (95% CI: 0.493–0.825), with a specificity of 0.675 and a sensitivity of 0.643. Although performance declined slightly, the model retained moderate discriminative ability. The drop in AUC may be attributed to the smaller sample size, distributional differences, or variations in predictor variables.
 |
Figure 5 Performance of the predictive model for inadequate postoperative analgesia in the training and validation cohorts. (A and B) ROC curves for the training (A) and validation (B) cohorts, demonstrating model discrimination (diagonal dashed line represents reference). (C and D) Calibration curves for the training (C) and validation (D) cohorts, assessing the agreement between predicted and observed probabilities. (E and F) DCA for the training (E) and validation (F) cohorts. The net benefit curves demonstrate clinical utility across a range of threshold probabilities (gray dashed line indicates the treat-all strategy; horizontal line represents the treat-none strategy). Abbreviation: AUC, area under the curve. |
Calibration was assessed via the Hosmer–Lemeshow test. In the training cohort, the Chi-square statistic was 1.21 with a P value of 0.998, and the calibration plot closely aligned with the ideal reference line (Figure 5C), indicating good model fit. In the validation cohort (Figure 5D), the calibration curve deviated in the moderate-to-high risk range. However, the Chi-square value of 11.25 (P = 0.260) suggested no significant miscalibration or overfitting, supporting reasonable model generalizability.
Decision curve analysis further supported the model’s clinical utility. In the training set (Figure 5E), the model provided greater net benefit than the “treat-all” and “treat-none” strategies across a risk threshold of 0.1 to 0.6. In the validation set (Figure 5F), the model demonstrated net clinical benefit between thresholds of 0.1 and 0.4, supporting its value in guiding individualized postoperative analgesia decisions in high-risk populations.
Discussion
This prospective study is the first to directly compare the postoperative analgesic efficacy and adverse reactions of hydromorphone and nalbuphine in women undergoing cesarean delivery. While most previous studies have focused on comparisons between nalbuphine and other opioids such as sufentanil, evidence regarding hydromorphone versus nalbuphine remains limited. Our findings fill this knowledge gap by providing head-to-head data in a clinical context where both agents are commonly used. In addition to efficacy and safety comparisons, we identified independent predictors of inadequate postoperative analgesia—defined as a NRS score ≥4 at rest or with movement within 24 hours postoperatively—including PCA regimen, GDM, blood type AB, and preoperative anxiety. Based on these variables, we developed a multivariable predictive model that demonstrated good discrimination and calibration. This model offers a quantitative tool for preoperative risk stratification and supports personalized perioperative pain management in cesarean delivery.
Analgesic Efficacy and Related Outcomes
With respect to analgesic outcomes, patients in the hydromorphone group experienced a significantly higher rate of inadequate analgesia compared to those in the nalbuphine group, suggesting superior analgesic performance of nalbuphine in the context of postcesarean pain management. To further illustrate the clinical benefit of nalbuphine, we quantified the absolute effect size and calculated the number needed to treat (NNT). Inadequate analgesia during movement occurred in 26.4% of patients in the hydromorphone group and 14.2% in the nalbuphine group, resulting in an absolute risk reduction (ARR) of 12.2%. This translates to a NNT of 9, indicating that for every nine patients treated with nalbuphine instead of hydromorphone, one additional case of inadequate postoperative analgesia could be prevented.
Although both hydromorphone and nalbuphine are opioid analgesics, they differ substantially in their mechanisms of action. Hydromorphone is a potent MOR agonist that exerts its analgesic effects by inhibiting nociceptive transmission in the central nervous system. However, MOR activation is also associated with common opioid-related adverse effects, including nausea, vomiting, pruritus, and respiratory depression. Furthermore, the clinical efficacy of hydromorphone is influenced by interindividual variability in MOR expression and the metabolic activity of enzymes such as CYP3A4 and UGT2B7, which are affected by both genetic factors and pregnancy-related physiological changes. These pharmacokinetic and pharmacodynamic variabilities may contribute to suboptimal analgesia in some patients.18
Nalbuphine, in contrast, is a KOR agonist and partial MOR antagonist. Its analgesic action primarily occurs at the spinal level, where KORs are densely expressed in the dorsal horn. KOR-mediated signaling is particularly effective in relieving visceral pain, such as that associated with postoperative uterine contractions. Postcesarean pain is multifaceted, involving both somatic incisional pain and visceral pain from uterine involution. Prior studies have shown that KOR agonists are particularly effective in addressing visceral pain, making nalbuphine especially suitable for postpartum patients. Moreover, its μ-antagonistic effect reduces the incidence of common opioid-related adverse effects, thereby enhancing safety while maintaining analgesic efficacy. Nalbuphine is also associated with a slower development of tolerance, providing more stable analgesic effects during continuous infusion.
The results of the multivariable logistic regression further support these mechanistic insights, as PCA regimen emerged as an independent predictor of inadequate analgesia (OR = 0.30, P = 0.026). This finding underscores the importance of tailoring postoperative analgesic strategies to pain characteristics, physiological status, and pharmacological profiles. Selecting agents with mechanisms more closely aligned to the predominant pain type and with lower interindividual variability may improve the quality of postoperative pain control.
Gestational Diabetes Mellitus and Postoperative Analgesia
This study identified GDM as an independent predictor of inadequate postoperative analgesia (defined as NRS ≥4), with a significantly higher incidence observed in patients with GDM. Although GDM is typically characterized as a transient hyperglycemic state, the associated metabolic disturbances, neuroinflammatory responses, and endocrine alterations may have lasting impacts on pain perception and responsiveness to analgesics.19 Prior studies have reported that patients with diabetes often experience more severe postoperative pain and require higher doses of opioids, likely due to hyperglycemia-induced peripheral nerve dysfunction and nociceptive sensitization.20–22
Mechanistically, hyperglycemia can activate the NF-κB pathway and elevate proinflammatory cytokines such as TNF-α and IL-6, contributing to neuroinflammation and decreased pain thresholds.23–27 In addition, oxidative stress and endothelial dysfunction may increase the sensitivity of nociceptive receptors such as transient receptor potential vanilloid 1 (TRPV1), amplifying pain signaling.28 Diabetes has also been shown to impair opioid receptor expression and G-protein coupling, thereby reducing the efficacy of opioid analgesics.29–31 Several clinical studies have reported positive correlations between perioperative glycated hemoglobin (HbA1c) levels and postoperative analgesic requirements, suggesting that higher glycemic burden is associated with intensified pain perception and analgesic needs.32,33
In the context of cesarean delivery, patients with GDM are more likely to undergo surgical intervention, yet their altered pain modulation and potential opioid resistance are often overlooked in perioperative management. The nomogram constructed in this study quantified the contribution of GDM to analgesic inadequacy, underscoring the importance of identifying GDM as a high-risk factor. Preoperative assessment of glycemic control and tailored intraoperative and postoperative analgesia protocols are warranted to optimize pain outcomes in this population.
Association Between Blood Type and Postoperative Analgesia Outcomes
ABO blood type, a common genetic trait, has been associated with various medical conditions, including hematological diseases,34–36 diabetes mellitus,37,38 and multiple types of cancer.39,40 In recent years, increasing attention has been directed toward its potential influence on postoperative analgesia outcomes. Our study demonstrated that patients with blood type AB had a significantly higher incidence of inadequate postoperative analgesia, suggesting a possible modulatory role of blood type in pain perception and response.
Although no consensus has been reached, and most findings remain exploratory, emerging evidence indicates that blood type may influence pain pathways through genetic and neurophysiological mechanisms. For instance, the synthesis of A and B antigens is catalyzed by specific glycosyltransferases—α-1,3-N-acetylgalactosaminyltransferase (GTA) and α-1,3-galactosyltransferase (GTB), respectively. Interestingly, these enzymes are not limited to hematologic expression; they also play roles in neural development and myelin maintenance by regulating glycosylation of neural glycoproteins, which are crucial for signal conduction and nerve repair. It has been postulated that the expression of GTA or GTB may influence other glycosylation pathways involved in sensory nerve integrity, thereby contributing to differential nociceptive processing across blood types.41 Moreover, blood type may modulate systemic inflammation and neural plasticity, both of which are critically involved in pain modulation following tissue injury or surgery. Individuals with certain blood types may exhibit heightened susceptibility to inflammatory responses, altered stress hormone profiles, or impaired resolution of neuroinflammation, thereby impacting their postoperative pain trajectories. These findings, though preliminary, highlight the need for further investigation into the molecular interplay between blood group antigens, neuroimmune signaling, and pain perception.42
Clinical studies have begun to support these hypotheses. One study reported that blood type was an independent predictor of pain intensity within 48 hours after cesarean delivery.43 A prospective pediatric cohort further found that children with blood types AB and B experienced higher pain scores and greater opioid requirements following adenotonsillectomy.44
Nevertheless, the association between blood type and analgesic outcomes may be confounded by psychological status, comorbidities, and anesthesia techniques.45,46 Despite these limitations, our findings underscore the potential relevance of blood type as a genetic modulator of analgesic response, warranting further investigation in larger cohorts and mechanistic studies.
Anxiety and Individualized Pain Management
Our findings indicate that preoperative anxiety, as assessed by the GAD-7 score, was an independent predictor of inadequate postoperative analgesia after cesarean delivery. Interestingly, both univariate and multivariable logistic regression analyses revealed that patients with higher preoperative anxiety scores experienced a lower incidence of inadequate analgesia and required less opioid consumption postoperatively. In the nomogram, preoperative anxiety emerged as one of the most influential predictors, underscoring the potential role of psychological factors in modulating postoperative pain perception and analgesic response.
At first glance, this result may appear paradoxical, as prior literature generally suggests that higher levels of anxiety are associated with increased pain sensitivity and poorer postoperative pain outcomes. However, several plausible explanations exist. One possibility is that patients with higher anxiety levels tend to report their pain more proactively or seek help earlier, leading to more timely and effective analgesia administration. Additionally, heightened anxiety may prompt more intensive monitoring or individualized care by medical staff, inadvertently resulting in better pain control. Another interpretation is that the structured perioperative environment and supportive care may mitigate anxiety-related hyperalgesia, especially in patients anticipating severe pain. These hypotheses warrant further investigation in larger cohorts.
These findings highlight the importance of tailoring pain management strategies based not only on physiological but also psychological profiles. For individuals with low anxiety levels—who may underreport pain or exhibit higher pain tolerance—greater attention to pain assessment and proactive intervention may be needed to avoid under-treatment. In contrast, patients with elevated anxiety may benefit from preoperative psychological counseling and enhanced communication, which could improve their coping capacity and optimize analgesic outcomes.
Interactive Nomogram and Its Clinical Implications
Based on the identified predictors, a risk prediction model for postoperative inadequate analgesia was developed and visualized using an interactive nomogram. This graphical tool enables clinicians to rapidly estimate an individual patient’s risk based on specific characteristics—such as PCA regimen, GDM, blood type AB, and preoperative anxiety score—and supports the implementation of personalized pain management strategies.
The nomogram enhances interpretability by illustrating how different variables interact and contribute to analgesic outcomes, thereby facilitating more informed and targeted clinical decision-making. Although the model’s performance in the validation cohort was slightly lower than in the training set, it demonstrated stable predictive value across ROC curves, calibration plots, and decision curve analysis, suggesting its potential utility and generalizability in real-world clinical practice.
Although the primary aim of this study was to compare the analgesic efficacy of hydromorphone and nalbuphine in a randomized controlled design, we also conducted an exploratory analysis to develop a risk prediction nomogram model for inadequate postoperative analgesia. Compared with our previous machine learning model based on 763 cesarean delivery patients and 42 perioperative variables,4 the current model included fewer predictors. This limitation partly stems from the relatively small sample size of this RCT and the low event rate of inadequate analgesia. To reduce the risk of overfitting and ensure model robustness, we adopted a simplified and clinically interpretable nomogram-based modeling strategy.
This model emphasized the inclusion of readily available and easily measurable perioperative variables to enhance its usability and bedside applicability. However, several limitations should be acknowledged. First, the study was conducted at a single center with a limited sample size, potentially restricting the generalizability of the model. Second, some associations—such as the role of blood type or preoperative anxiety—lack robust mechanistic evidence and should be interpreted with caution. Third, inadequate analgesia was defined solely based on an NRS score ≥ 4 within the first 24 hours postoperatively, without incorporating longer-term pain trajectories or multidimensional outcomes such as patient satisfaction. Fourth, the analgesic protocol used in this study did not incorporate regional techniques (eg, transversus abdominis plane [TAP] block or quadratus lumborum blocks) or standardized multimodal analgesia strategies that are increasingly adopted in enhanced recovery after cesarean delivery. This reflects the standard systemic PCA-based practice at our institution during the study period. Although this pragmatic design allowed us to isolate the effects of different systemic opioid regimens, it may limit the applicability of the findings to centers where regional techniques are routinely implemented. We have clearly acknowledged this limitation and recommend interpreting the results in the context of the analgesic approach employed. Furthermore, the model did not account for potential biological modulators, such as opioid receptor polymorphisms or interindividual metabolic variability, and has not been benchmarked against other prediction tools or analgesia strategies.
Future studies should aim to externally validate this model across larger and multicenter cohorts, integrate multi-omics data to explore mechanistic underpinnings, and assess the feasibility of incorporating the nomogram into clinical decision-making pathways to enhance its translational value.
Conclusion
This study demonstrated that nalbuphine provides more effective analgesia and fewer adverse effects than hydromorphone for postcesarean pain control. A predictive model incorporating PCA regimen, gestational diabetes, blood type AB, and preoperative anxiety was developed and validated, offering a practical tool for identifying patients at high risk of inadequate analgesia. These findings support the integration of both drug selection and patient-specific characteristics into postoperative pain management strategies to improve clinical outcomes and patient satisfaction.
Abbreviations
ARR, absolute risk reduction; AIC, Akaike information criterion; AUC, area under the receiver operating characteristic curve; BMI, body mass index; CI, confidence interval; CS, cesarean section; DCA, decision curve analysis; EPDS-10, Edinburgh Postnatal Depression Scale 10-item version; GAD-7, Generalized Anxiety Disorder 7-item scale; GDM, gestational diabetes mellitus; GTA, α-1,3-N-acetylgalactosaminyltransferase; GTB, α-1,3-galactosyltransferase; HbA1c, glycated hemoglobin; IQR, interquartile range; KOR, κ-opioid receptor; MOR, μ-opioid receptor; NNT, number needed to treat; NRS, numerical rating scale; OR, odds ratio; PCA, patient-controlled analgesia; PCS, pain catastrophizing scale; ROC, receiver operating characteristic; SD, standard deviation; TAP, transversus abdominis plane; TRPV1, transient receptor potential vanilloid 1; WHO, World Health Organization.
Data Sharing Statement
The data underlying this article are available from the corresponding author, Dr. Xianwei Zhang, upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of Tongji Hospital, Huazhong University of Science and Technology (Approval No. TJ-IRB202409103), and conducted in accordance with the Declaration of Helsinki and relevant national regulations. All participants provided written informed consent before enrollment. The trial was registered at ClinicalTrials.gov (Identifier: NCT06716359).
Acknowledgments
The authors thank the anesthesiology team at Tongji Hospital for their support in patient care and data acquisition during the trial. No writing assistance or external editorial support was used. All acknowledged individuals have provided permission for inclusion.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors would like to acknowledge the support of the National Natural Science Foundation of China (grant no. 81271235), the Hubei Provincial Natural Science Foundation of China (grant no. 2023AFB117), the Research Fund of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (grant no. 2019C03, 2023B26), the Special Project of Science and Technology Research Institute of National Health Commission (grant no. 2020045).
Disclosure
All authors declare that they have no competing interests to declare.
References
1. Lumbiganon P, Laopaiboon M, Gulmezoglu AM, et al. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007-08. Lancet. 2010;375(9713):490–499. doi:10.1016/S0140-6736(09)61870-5
2. Li HT, Luo S, Trasande L, et al. Geographic variations and temporal trends in cesarean delivery rates in China, 2008-2014. JAMA. 2017;317(1):69–76. doi:10.1001/jama.2016.18663
3. Nedeljkovic SS, Kett A, Vallejo MC, et al. Transversus abdominis plane block with liposomal bupivacaine for pain after cesarean delivery in a multicenter, randomized, double-blind, controlled trial. Anesthesia Analg. 2020;131(6):1830–1839. doi:10.1213/ANE.0000000000005075
4. Zhang K, Jiao B, Sun J, et al. Predicting high-risk factors for postoperative inadequate analgesia and adverse reactions in cesarean delivery surgery: a prospective study. International Journal of Surgery. 2025;111(6):3859–3875. doi:10.1097/JS9.0000000000002354
5. Bollag L, Lim G, Sultan P, et al. Society for obstetric anesthesia and perinatology: consensus statement and recommendations for enhanced recovery after cesarean. Anesthesia Analg. 2021;132(5):1362–1377. doi:10.1213/ANE.0000000000005257
6. Sun J, Li N, Liu B, et al. Efficacy and safety of patient-controlled intravenous analgesia after APS team standardized postoperative pain management: a 6-year experience of an acute pain service in 107802 Chinese patients. Heliyon. 2024;10(2):e24387. doi:10.1016/j.heliyon.2024.e24387
7. Santa Cruz Mercado LA, Liu R, Bharadwaj KM, et al. Association of intraoperative opioid administration with postoperative pain and opioid use. JAMA Surg. 2023;158(8):854–864. doi:10.1001/jamasurg.2023.2009
8. Sun S, Guo Y, Wang T, Huang S. Analgesic effect comparison between nalbuphine and sufentanil for patient-controlled intravenous analgesia after cesarean section. Front Pharmacol. 2020;11:574493. doi:10.3389/fphar.2020.574493
9. Zheng K, Chen B, Sun J. Nalbuphine may be superior to sufentanil in relieving postcesarean uterine contraction pain in multiparas: a retrospective cohort study. Drug Des Devel Ther. 2023;17:1405–1415. doi:10.2147/DDDT.S394664
10. Wang L, Wang Y, Ma Y, et al. Sufentanil combined with nalbuphine via patient-controlled intravenous analgesia after cesarean section: a retrospective evaluation. Drug Des Devel Ther. 2022;16:3711–3721. doi:10.2147/DDDT.S380292
11. Li WW, Zheng B, Shi R, Jiang YM, Liu YN, Wang ZW. Patient-controlled intravenous administration of dexmedetomidine with nalbuphine versus sufentanil for post cesarean delivery analgesia: a retrospective observational study. Kaohsiung J Med Sci. 2023;39(7):740–747. doi:10.1002/kjm2.12689
12. Sharpe EE, Molitor RJ, Arendt KW, et al. Intrathecal morphine versus intrathecal hydromorphone for analgesia after cesarean delivery: a randomized clinical trial. Anesthesiology. 2020;132(6):1382–1391. doi:10.1097/ALN.0000000000003283
13. Zhang Y, Xie S, Zhang G, Gong X. Analgesic effect of butorphanol tartrate combined with hydromorphone on patients with cesarean section: a prospective cohort study. Medicine. 2022;101(48):e31901. doi:10.1097/MD.0000000000031901
14. Cheng S, Bartolacci J, Armstrong K, et al. Intrathecal hydromorphone versus intrathecal morphine for postcesarean delivery analgesia: a randomized noninferiority trial. Anesthesia Analg. 2025. doi:10.1213/ANE.0000000000007580
15. Duan G, Bao X, Yang G, et al. Patient-controlled intravenous tramadol versus patient-controlled intravenous hydromorphone for analgesia after secondary cesarean delivery: a randomized controlled trial to compare analgesic, anti-anxiety and anti-depression effects. J Pain Res. 2019;12:49–59. doi:10.2147/JPR.S184782
16. Dinges HC, Schubert AK, Rucker G, et al. Equianalgesic potency ratios of opioids used in patient-controlled analgesia: a network meta-analysis. J Opioid Manag. 2022;18(6):567–586. doi:10.5055/jom.2022.0751
17. Yu L, Zhang X, Jiang F, et al. Development and validation of nomograms to predict preoperative anxiety and postoperative pain in patients undergoing gynecological surgery: an observational analysis. J Affect Disord. 2023;339:227–236. doi:10.1016/j.jad.2023.07.058
18. Alinejadfard M, Rajai Firouzabadi S, Mohammadi I, Oraee S, Golsorkh H, Mahdavi S. Efficacy and safety of hydromorphone for cancer pain: a systematic review and meta-analysis. BMC Anesthesiol. 2024;24(1):283. doi:10.1186/s12871-024-02638-y
19. Zhu WW, Yang HX, Wei YM, et al. Evaluation of the value of fasting plasma glucose in the first prenatal visit to diagnose gestational diabetes mellitus in China. Diabetes Care. 2013;36(3):586–590. doi:10.2337/dc12-1157
20. Nivatpumin P, Pangthipampai P, Dej-Arkom S, Aroonpruksakul S, Lertbunnaphong T, Ngam-Ek-Eu T. Gestational diabetes and intraoperative tubal sterilization are risk factors for high incidence of pain after cesarean delivery: a prospective observational study. Ann Palliat Med. 2022;11(4):1170–1178. doi:10.21037/apm-21-2139
21. Yang C, Li Y, Hu J, Wu J, Huang S. The relationship between pre-operative glycosylated haemoglobin and opioid consumption after caesarean section in women with gestational diabetes mellitus. Front Endocrinol. 2022;13:910914. doi:10.3389/fendo.2022.910914
22. Yang C, Geng WL, Hu J, Huang S. The effect of gestational diabetes mellitus on sufentanil consumption after cesarean section: a prospective cohort study. BMC Anesthesiol. 2020;20(1):14. doi:10.1186/s12871-019-0925-1
23. Park SH, Bahk JH, Oh AY, Gil NS, Huh J, Lee JH. Gender difference and change of alpha(1)-adrenoceptors in the distal mesenteric arteries of streptozotocin-induced diabetic rats. Korean J Anesthesiol. 2011;61(5):419–427. doi:10.4097/kjae.2011.61.5.419
24. Todorovic SM. Is diabetic nerve pain caused by dysregulated ion channels in sensory neurons? Diabetes. 2015;64(12):3987–3989. doi:10.2337/dbi15-0006
25. Zhang HH, Hu J, Zhou YL, et al. Promoted interaction of nuclear factor-kappab with demethylated purinergic P2X3 receptor gene contributes to neuropathic pain in rats with diabetes. Diabetes. 2015;64(12):4272–4284. doi:10.2337/db15-0138
26. Ye D, Fairchild TJ, Vo L, Drummond PD. High blood glucose and excess body fat enhance pain sensitivity and weaken pain inhibition in healthy adults: a single-blind cross-over randomized controlled trial. J Pain. 2023;24(1):128–144. doi:10.1016/j.jpain.2022.09.006
27. Poole DB, Cutler RS, Kelly WR, Collins JD. Eperythrozoon wenyoni anaemia in cattle. Vet Rec. 1976;99(24):481. doi:10.1136/vr.99.24.481
28. Johns EC, Denison FC, Norman JE, Reynolds RM. Gestational diabetes mellitus: mechanisms, treatment, and complications. Trends Endocrinol Metab. 2018;29(11):743–754. doi:10.1016/j.tem.2018.09.004
29. Karci A, Tasdogen A, Erkin Y, Aktas G, Elar Z. The analgesic effect of morphine on postoperative pain in diabetic patients. Acta anaesthesiologica Scandinavica. 2004;48(5):619–624. doi:10.1111/j.1399-6576.2004.00387.x
30. Weiner DA, Murphy JP, Gwam C, et al. Increased opioid consumption in diabetics with operative ankle fractures: a retrospective case-control study. Eur J Orthop Surg Traumatol. 2019;29(6):1319–1323. doi:10.1007/s00590-019-02428-0
31. Courteix C, Bourget P, Caussade F, et al. Is the reduced efficacy of morphine in diabetic rats caused by alterations of opiate receptors or of morphine pharmacokinetics? J Pharmacol Exp Ther. 1998;285(1):63–70. doi:10.1016/S0022-3565(24)37362-8
32. Koenig RJ, Peterson CM, Jones RL, Saudek C, Lehrman M, Cerami A. Correlation of glucose regulation and hemoglobin AIc in diabetes mellitus. New Engl J Med. 1976;295(8):417–420. doi:10.1056/NEJM197608192950804
33. Kim SH, Hwang JH. Preoperative glycosylated haemoglobin as a predictor of postoperative analgesic requirements in diabetic patients: a prospective observational study. Eur J Anaesthesiol. 2015;32(10):705–711. doi:10.1097/EJA.0000000000000282
34. O’Donnell J, Laffan MA. The relationship between ABO histo-blood group, factor VIII and von Willebrand factor. Transfus Med. 2001;11(4):343–351. doi:10.1046/j.1365-3148.2001.00315.x
35. He M, Wolpin B, Rexrode K, et al. ABO blood group and risk of coronary heart disease in two prospective cohort studies. Arterioscler Thromb Vasc Biol. 2012;32(9):2314–2320. doi:10.1161/ATVBAHA.112.248757
36. Chen Z, Yang SH, Xu H, Li JJ. ABO blood group system and the coronary artery disease: an updated systematic review and meta-analysis. Sci Rep. 2016;6(1):23250. doi:10.1038/srep23250
37. Fagherazzi G, Gusto G, Clavel-Chapelon F, Balkau B, Bonnet F. ABO and Rhesus blood groups and risk of type 2 diabetes: evidence from the large E3N cohort study. Diabetologia. 2015;58(3):519–522. doi:10.1007/s00125-014-3472-9
38. Walle M, Tesfaye A, Getu F. The association of ABO and Rhesus blood groups with the occurrence of type 2 diabetes mellitus: a comparative cross-sectional study. Medicine. 2023;102(35):e34803. doi:10.1097/MD.0000000000034803
39. Vasan SK, Hwang J, Rostgaard K, et al. ABO blood group and risk of cancer: a register-based cohort study of 1.6 million blood donors. Cancer Epidemiol. 2016;44:40–43. doi:10.1016/j.canep.2016.06.005
40. Li B, Tan B, Chen C, Zhao L, Qin L. Association between the ABO blood group and risk of common cancers. J Evid Based Med. 2014;7(2):79–83. doi:10.1111/jebm.12098
41. Simoni AH, Jerwiarz A, Randers A, Gazerani P. Association between ABO blood types and pain perception. Somatosens Mot Res. 2017;34(4):258–264. doi:10.1080/08990220.2018.1425675
42. Zhang JM, An J. Cytokines, inflammation, and pain. Int Anesthesiol Clin. 2007;45(2):27–37. doi:10.1097/AIA.0b013e318034194e
43. Jasim HH, Sulaiman S, Khan AH, SR UA. Factors affecting post caesarean pain intensity among women in the northern peninsular of Malaysia. J Clin Diagn Res. 2017;11(9):IC07–IC11. doi:10.7860/JCDR/2017/25364.10630
44. Shen L, Wu J, Xiao Q, et al. Association between ABO blood groups and postoperative pain in children after adenotonsillectomy: a prospective cohort study. BMC Anesthesiol. 2022;22(1):407. doi:10.1186/s12871-022-01953-6
45. Xu F, Yin JW, Xiong EF, et al. Correlation between preoperative anxiety and ABO blood types: evidence from a clinical cross-sectional study. Dis Markers. 2019;2019:1761693. doi:10.1155/2019/1761693
46. Nimmaanrat S, Thongkumdee W, Geater AF, Oofuvong M, Benjhawaleemas P. Is ABO blood group a predictive factor for the amount of opioid consumption in the first 24 hours after cesarean section? J Pain Res. 2021;14:3585–3592. doi:10.2147/JPR.S327230
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Effectiveness of Single-Dose Epidural Esketamine versus Hydromorphone in Thoracic and Upper Abdominal Surgery: A Randomized Trial
Song Y, Wang C, Huang N, He H, Hong W, Wu J, Yao M, Miao C, Liang C
Drug Design, Development and Therapy 2026, 20:580521
Published Date: 3 February 2026
Effect of Intrathecal Hydromorphone on the Duration and Efficacy of Postoperative Analgesia in Patients Undergoing Benign Anorectal Surgery: Protocol for a Randomized, Double-Blind, Controlled Trial
Cao Y, Zhou Y, Zhou D, Xiong C, Fu L, Chen X, Zhang X
Journal of Pain Research 2026, 19:569284
Published Date: 26 February 2026
Hydromorphone is Noninferior to Dexamethasone as an Adjuvant to Ropivacaine for Transversus Abdominis Plane Block After Laparoscopic Colorectal Cancer Surgery: A Randomized, Double-Blind Trial
Zhao L, Wang Y, Guo Q, An Q, Wu M, Fan C, Guo Z
Journal of Pain Research 2026, 19:581520
Published Date: 5 March 2026