Back to Journals » Journal of Pain Research » Volume 18
Comparative Effectiveness of Pharmacological, Non-Pharmacological, and Combined Strategies for Pain Relief During Colonoscopy: A Bayesian Network Meta-Analysis of Randomized Trials
Authors Huang X ![]() , Tian S
, Tian S ![]() , Xu L, Chen J, Wang H, Mai T
, Xu L, Chen J, Wang H, Mai T ![]() , Shi L, Wang H, Cai M, Fang F
, Shi L, Wang H, Cai M, Fang F
Received 23 July 2025
Accepted for publication 12 November 2025
Published 19 November 2025 Volume 2025:18 Pages 6165—6179
DOI https://doi.org/10.2147/JPR.S554665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert B. Raffa
Xiaonan Huang,1,* Shan Tian,2,* Lifan Xu,1,* Juhan Chen,1,* Hao Wang,3 Tingting Mai,1 Lei Shi,1 Han Wang,4 Mengcheng Cai,5 Fanfu Fang1
1Department of Rehabilitation Medicine, Changhai Hospital, Naval Medical University, Shanghai, People’s Republic of China; 2Department of Acupuncture and Massage, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 3Department of Colorectal Surgery, Changhai Hospital, Naval Medical University, Shanghai, People’s Republic of China; 4School of Health Science and Engineering, University of Shanghai for Science and Technology, Shanghai, People’s Republic of China; 5Department of Rehabilitation Medicine, Naval Medical Center, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fanfu Fang, Changhai Hospital, Naval Medical University, 168 Changhai Road, Yangpu District, Shanghai, 200433, People’s Republic of China, Email [email protected] Mengcheng Cai, Changhai Hospital, Naval Medical University, 168 Changhai Road, Yangpu District, Shanghai, 200433, People’s Republic of China, Email [email protected]
Background: Colonoscopy is the gold standard for colorectal cancer screening, but procedural pain remains a major barrier to patient compliance. Various pharmacological and non-pharmacological interventions have been developed to improve patient comfort, yet the comparative effectiveness of these strategies remains unclear.
Methods: We systematically searched five databases for randomized controlled trials published between 2004 and 2024 that evaluated analgesic interventions for colonoscopy and performed a Bayesian random-effects network meta-analysis. We analyzed two pre-specified subnetworks—non-pharmacological and pharmacological/combined—according to intervention type. The primary outcome was pain on a visual analogue scale.
Results: 40 RCTs (5614 participants, 32 interventions) were included. Compared to blank control: 1) Combined physical intervention + analgesia/sedation (MD = − 2.7, 95% CrI: − 5.3 to − 0.15) and water perfusion/CO2 insufflation (MD = − 1.9, 95% CrI: − 2.8 to − 0.99) significantly reduced pain; 2) Among non-pharmacological interventions, CO2 insufflation, water perfusion, and visual distraction showed significant advantages; 3) Among pharmacological/combined interventions, pethidine + benzodiazepines + non-pharmacological (MD = − 5.1, 95% CrI: − 8.6 to − 1.7) and propofol-based strategies were most effective. SUCRA rankings identified combined physical intervention + analgesia/sedation, propofol, and water perfusion/CO2 as top overall interventions.
Conclusion: Multimodal strategies that combine pharmacological agents, especially pethidine or propofol, with non-pharmacological techniques such as CO2 insufflation and water perfusion provide the most effective pain relief during colonoscopy.
Keywords: colonoscopy, pain relief, network meta-analysis, nonpharmacologic interventions, randomized controlled trials
Introduction
According to recent statistics, there were approximately 1.92 million new cases of colorectal cancer (CRC) worldwide in 2022, accounting for 10.2% of all malignancies, with 904,000 deaths representing 9.3% of cancer-related mortality. CRC ranks third in incidence and second in mortality among all cancers globally.1 Notably, the incidence of CRC among individuals under the age of 50 has been steadily increasing, with the median age at diagnosis for early-onset CRC in the United States declining from 72 to 66 years.2 Furthermore, it is projected that by 2030, the annual global incidence of CRC will reach 2.2 million cases, with China’s share likely to further increase.3
Colonoscopy remains the gold standard for CRC screening, enabling early detection of 45–75% of colorectal cancers and reducing CRC-related mortality by nearly 50%.4 Regular colonoscopic screening every 2–3 years substantially increases the likelihood of early diagnosis and can slow disease progression. However, data indicate that as many as 16–20% of routine colonoscopies are prematurely terminated due to intolerable pain. This discomfort—primarily resulting from colonic traction, abdominal distension, and spasm—significantly impairs patient compliance, as fear of pain leads many patients to avoid recommended repeat examinations.5 Poor adherence to colonoscopy due to anticipated or experienced pain can reduce lesion detection, delay diagnosis, and worsen outcomes, underscoring the need for effective, scalable analgesia.6
To address the wide range of adjunctive analgesic approaches used to improve patient tolerance during colonoscopy, we designed our analysis at the strategy level rather than at the level of individual interventions. We conducted a network meta-analysis, which integrates both direct and indirect comparisons to evaluate multiple strategies when head-to-head trials are limited.7 Before analysis, all trial arms were pre-classified into three strategy types: non-pharmacological,8 pharmacological, and combined approaches integrating both.9 Because pharmacological trials typically employed placebo controls whereas non-pharmacological trials often used blank controls, we structured the evidence into two subnetworks, non-pharmacological and pharmacological/combined, to respect heterogeneous control types, minimize transitivity violations, and reduce network sparsity.10 Accordingly, this review evaluates analgesia at the strategy level—non-pharmacological, pharmacological, and combined—rather than single agents, to inform resource-sensitive, patient-tailored practice.
Methodology
Study Design
This Bayesian network meta-analysis was conducted and reported in accordance with the PRISMA-NMA guidelines.11 The protocol was prospectively registered in PROSPERO (www.crd.york.ac.uk, CRD42024586361).
Search Strategy
This study systematically reviewed randomized controlled trials (RCTs) evaluating analgesic interventions for colonoscopy. Comprehensive literature searches were conducted in five databases: Web of Science, PubMed, Embase, Cochrane CENTRAL, and ClinicalTrials.gov. Boolean operators were used to combine MeSH terms and free-text keywords, and the search strategy was constructed according to the PICOS framework, with the study type limited to RCTs (for detailed search strategies, see Table 1s). The search covered publications from November 7, 2004, to November 7, 2024, without language restrictions; non-English articles were included after translation. Reference management was performed using EndNote 20 to remove duplicates, followed by an additional manual deduplication step. Titles and abstracts were screened to exclude irrelevant studies, and the full texts of the remaining articles were reviewed for eligibility and systematically assessed to determine the final inclusion set.
Based on preliminary literature review, we observed that analgesic strategies in colonoscopy include pharmacological, non-pharmacological, and combined interventions, with numerous possible permutations. Therefore, for all included studies, we initially grouped similar intervention types before analysis, and then categorized them into two major groups: (1) interventions containing only non-pharmacological modalities, and (2) interventions involving pharmacological agents or combined treatments. This approach aimed to ensure greater objectivity and clarity in the network meta-analysis, and to provide clinically relevant guidance for analgesic strategies during colonoscopy.
Inclusion and Exclusion Criteria
First, we included studies involving complete colonoscopy procedures, regardless of whether anesthesia was used, and excluded trials focused solely on rectal or colonic insufflation. Studies involving sequential upper and lower gastrointestinal endoscopy (ie, combined gastroscopy and colonoscopy) were also excluded. Second, with respect to interventions, we excluded studies where differences in operator expertise (among endoscopists or anesthesiologists) or variations in endoscopic equipment could affect pain outcomes. All external patient analgesic interventions—both pharmacological and non-pharmacological—were eligible for inclusion. Regarding outcome measures, only studies reporting pain scores as a primary or secondary outcome were included. We also collected data on secondary outcomes that may indirectly reflect pain, such as anxiety and patient satisfaction, as well as dosages of sedatives or analgesics used in studies involving such medications. Finally, to minimize bias arising from temporal differences in operator or equipment proficiency, we limited our review to RCTs published within the past 20 years, and excluded any non-randomized clinical studies. Study selection was performed independently by two reviewers (HXN and XLF). Any disagreements were resolved through discussion, or if necessary, in consultation with a third reviewer (TS).
Data Extraction Procedures
For each eligible study, two reviewers (HXN and XLF) independently extracted the following data: inclusion and exclusion criteria, patient demographic characteristics (including sex and age), intervention details, intervention duration, and dosage. Patient outcomes assessed in this study included pain scores measured by the Visual Analogue Scale (VAS), Numerical Rating Scale (NRS), and all other potential indicators reflecting pain severity, such as intubation success rate, sedative and analgesic usage, anxiety levels, and patient satisfaction, along with their corresponding means and standard deviations. When studies reported median and interquartile range, these values were converted to mean and standard deviation using established methods,12,13 Adverse events related to analgesic interventions were also recorded. In studies reporting pain at multiple time points, the pain score corresponding to the moment of greatest discomfort during the procedure was prioritized for analysis. If intra-procedural pain scores were not available, the first pain score assessed immediately after the procedure was used.
Risk of Bias
For all included RCTs, two reviewers (HXN and XLF) independently assessed the risk of bias using the Cochrane Risk of Bias tool 2.0 (version: ROB2_cluster_beta_v3).14 Discrepancies were resolved by discussion or, if necessary, in consultation with a third reviewer.
Statistical Analysis
To compare the effectiveness and safety of different analgesic interventions during colonoscopy, a network meta-analysis was performed using the gemtc package in R (version 4.3.3). A Bayesian random-effects network meta-analysis was used to estimate the relative effects of all interventions. This approach, utilizing a design-by-treatment interaction model, assessed the consistency assumption across the entire network, while node-splitting methods evaluated local inconsistency between direct and indirect evidence within each closed loop of the network.15
The relative effectiveness of interventions was comprehensively evaluated using the gemtc and netmeta packages in R. First, data were organized into tables containing study IDs, group sample sizes, means, standard deviations, and other relevant continuous variables. The mtc.network function was used to construct the network evidence map. For statistical modeling, a consistency model was applied, assuming that direct and indirect comparisons yield consistent results. Parameters were estimated using the Markov chain Monte Carlo (MCMC) algorithm, with four chains, 10,000 burn-in iterations, 50,000 sampling iterations, and a thinning interval of 10 to reduce autocorrelation. Model convergence was evaluated with trace plots, density plots, and the Gelman-Rubin statistic. Heterogeneity was assessed using a random-effects model, and quantified by the I2 statistic; I2 > 50% was considered indicative of substantial heterogeneity. Local inconsistency was examined using the node-splitting method by comparing direct and indirect evidence; a P < 0.05 was considered indicative of significant inconsistency. Global inconsistency was assessed using the design-by-treatment interaction model via the mtc.anohe function. Treatment ranking was determined using the surface under the cumulative ranking curve (SUCRA), with values ranging from 0 to 1, where higher values indicate better ranking.16 The rank.probability function was used to generate rank probability matrices, and cumulative probability plots and rankograms were created using the ggplot2 package.
Equity, Diversity and Inclusion Statement
Our study included RCTS of colonoscopy pain studies with no exclusion criteria for sex, race, ethnicity, and socioeconomic level. Our research team consisted of individuals working in Shanghai, China, including three women and four men from different disciplines (pain management, colorectal surgery, rehabilitation, and medical research).
Results
Study Selection
A total of 6820 records were identified from five databases (see Tables 2s–4s for search strategies). After automatic and manual deduplication using EndNote, 2237 duplicates were removed. The titles and abstracts of the remaining 4583 records were screened, leaving 181 articles for full-text review. Following the exclusion of 141 studies upon full-text assessment, 40 articles were ultimately included in the network meta-analysis17–56 (see Figure 1 for the study selection flowchart). Of these, 35 were two-arm studies, three were three-arm studies, and two were four-arm studies, encompassing a total of 5614 participants. Among these, 3070 were male (54.68%), with a mean age of 58.36 years.
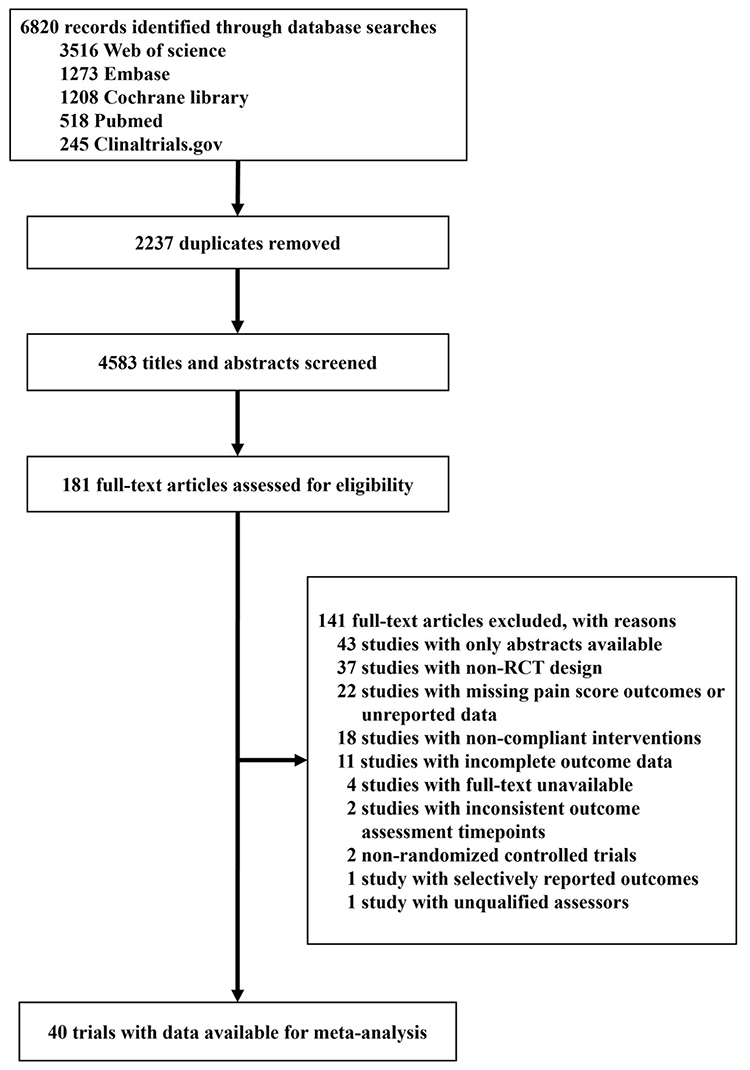 |
Figure 1 Flow chart of studies identified and included in the network meta-analysis. |
Across the 40 included studies, 32 different interventions were identified. The most frequently used were blank control (22 studies), fentanyl combined with midazolam (8), water perfusion (7), virtual reality (VR, 5), electrical stimulation/electroacupuncture (4), propofol (4), visual distraction (3), music (3), placebo (3), CO2 (2), abdominal compression (2), fentanyl plus propofol (2), music plus fentanyl and propofol (2), and pethidine plus midazolam (2). The remaining interventions—including various combinations of CO2, dezocine, diazepam, pethidine, propofol, VR, music, nalbuphine, pentazocine, and dezocine—each appeared in one study. Of the included RCTs, 22 studies evaluated non-pharmacological interventions only, 17 involved pharmacological or combined interventions, and one study included non-pharmacological, pharmacological, and combined interventions. Detailed data for each study are provided in Table 5s.
Network Geometry
The 40 included RCTs were initially categorized into 12 groups (Figure 2a), including one blank control group and one placebo group, the specific intervention methods included in each category are shown in Table 6s. In the non-pharmacological subgroup, 22 non-pharmacological RCTs and the non-pharmacological arm of one mixed-intervention study were divided into nine groups, including blank control and placebo (Figure 2b). For pharmacological interventions, 17 RCTs (plus the pharmacological arm of one mixed study) were also divided into nine groups, including a placebo group (Figure 2c).
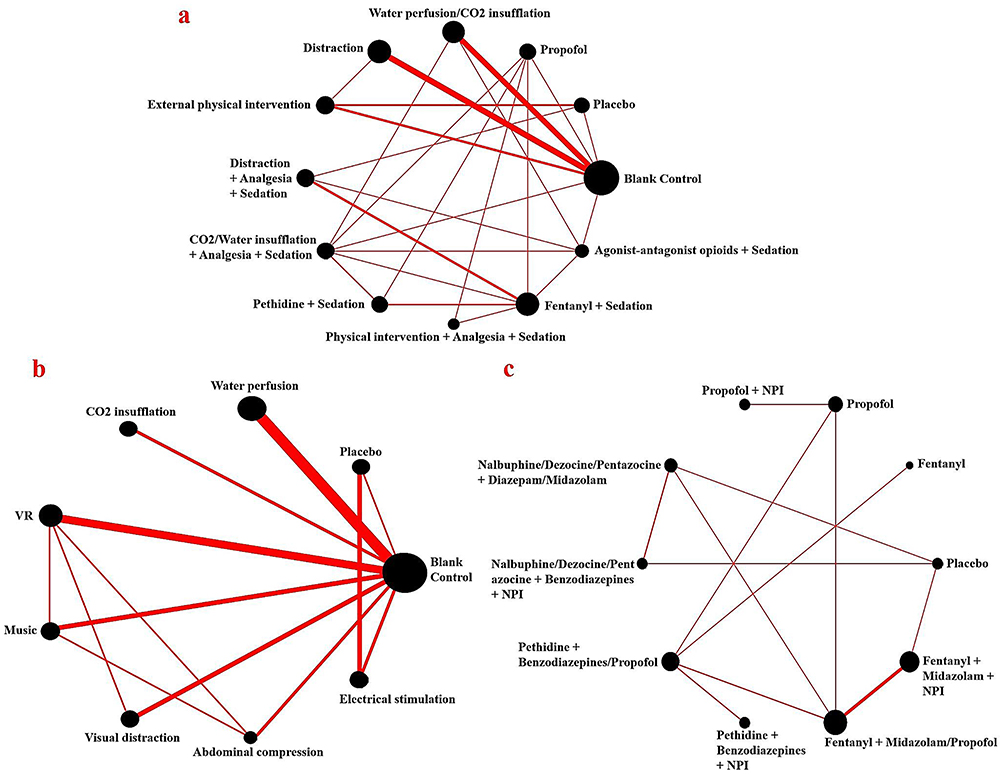 |
Figure 2 The network structure diagram. (a) All intervention measures; (b) Non-pharmacological intervention measures; (c) Pharmacological and combined intervention measures. Each node represents an intervention and is weighted by the number of studies that received the intervention. Each line connecting the nodes is weighted by the number of studies that included a pairwise comparison. Abbreviations: NPI, Non-pharmacological intervention. |
Risk of Bias
For the primary outcome, most studies were rated as having “some concerns” for risk of bias (n = 23, 57.5%). High risk of bias was identified in 4 studies (10%), while 13 studies (32.5%) were judged as low risk. The greatest risks were observed in the domains of measurement of outcomes and deviations from intended interventions. Full details of the risk of bias assessment are provided in Figure 1s.
Bayesian Model results for Pain Scores
Following network construction, a Bayesian random-effects consistency model was used for statistical analysis. The model specified a normal likelihood function and identity link, assuming consistency between direct and indirect comparisons. Four Markov chains were run with 10,000 burn-in iterations and 50,000 sampling iterations (thinning interval = 10) for parameter estimation. Gelman-Rubin diagnostic plots and trace plots confirmed adequate convergence of all parameters (potential scale reduction factors <1.05), indicating satisfactory model fit for all three comparison sets. Node-splitting and random-effects models were applied to assess local inconsistency within each evidence loop. The inconsistency tests for all interventions revealed that most pairwise comparisons did not show significant inconsistency; after separating analyses by pharmacological and non-pharmacological interventions, all pairwise comparisons were consistent (see Figures 2s–4s). Finally, the global heterogeneity of the three networks was evaluated using the design-by-treatment interaction model, revealing high overall heterogeneity, with I2 values of 95.71%, 93.75%, and 99.62%, respectively.
All Intervention Measures
Compared to blank control, both physical interventions combined with analgesia and sedation (MD = −2.7, 95% CrI: −5.3 to −0.15) and water perfusion/CO2 insufflation (MD = −1.9, 95% CrI: −2.8 to −0.99) demonstrated significant reductions in pain scores. In addition, distraction alone (MD = −0.97, 95% CrI: −1.8 to −0.19) was also associated with a statistically significant reduction in pain (Figure 5s). Other interventions—including propofol (MD = −2.1, 95% CrI: −4.3 to 0.082), pethidine plus sedatives (MD = −1.7, 95% CrI: −3.7 to 0.43), and fentanyl plus sedatives (MD = −1.4, 95% CrI: −3.3 to 0.49)—showed a trend toward pain relief, though these results did not reach statistical significance (Table 1). The league table of all interventions uses orange shading to indicate that the intervention listed in the row is more effective than that in the column, while blue indicates the opposite. We divided the yellow and blue shading into four tiers. For yellow: the first tier applies when MD exceeds 3 points. The second tier applies when MD is below 3 points and the 95% CrI has a lower bound greater than 0 and an upper bound greater than 3 points. The third tier applies when the 95% CrI has a lower bound greater than 0 and an upper bound between 1 and 3 points. The fourth tier applies when MD is below 3 points and the 95% CrI has a lower bound less than or equal to 0. For blue, the rules are the reverse. Calculation methods are detailed in Figure 8s.
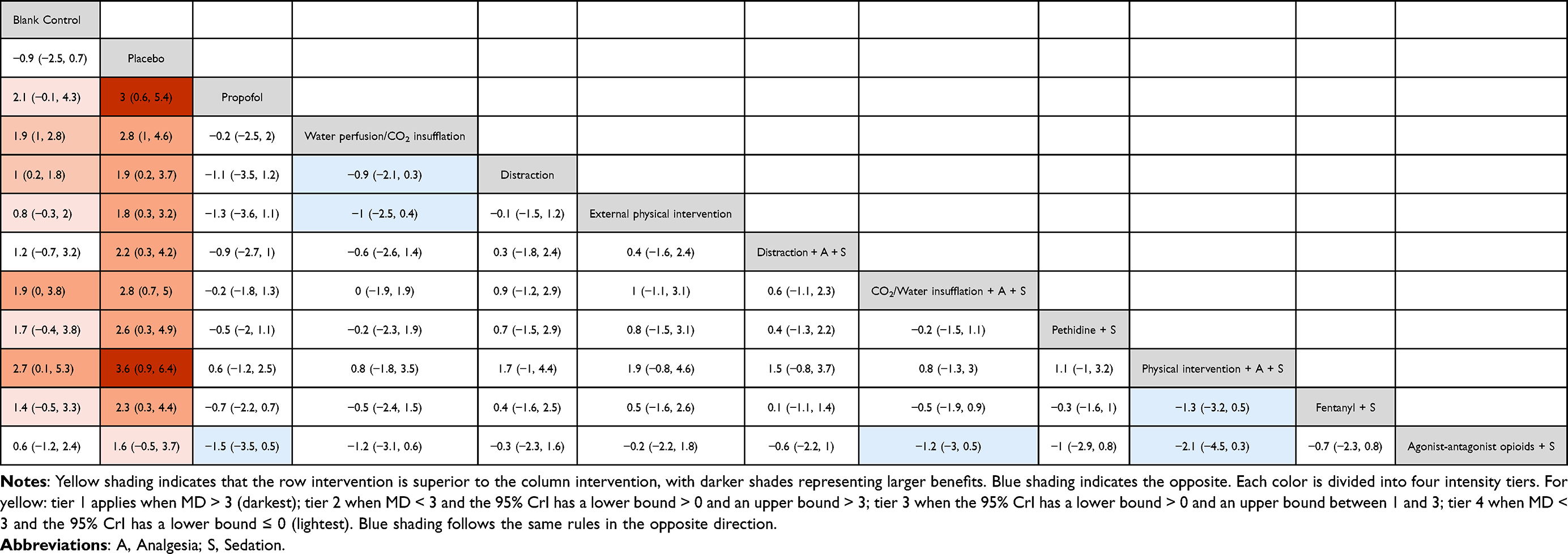 |
Table 1 League Tables of All Mean Differences and 95% Confidence Intervals by All Interventions |
Non-Pharmacological Intervention Measures
CO2 insufflation (MD = −1.9, 95% CrI: −3.7 to −0.14), water perfusion (MD = −1.7, 95% CrI: −2.7 to −0.70), and visual distraction (MD = −1.2, 95% CrI: −2.6 to −0.30) each showed significant advantages for pain relief (Figure 6s). Other interventions—including music (MD = −1.3, 95% CrI: −2.7 to 0.17), electrical stimulation (MD = −1.0, 95% CrI: −2.9 to 0.82), virtual reality (VR; MD = −0.73, 95% CrI: −1.9 to 0.36), and abdominal compression (MD = −0.53, 95% CrI: −2.2 to 1.2) did not reach statistical significance. The league table further presents pairwise comparisons among non-pharmacological interventions (Table 2).
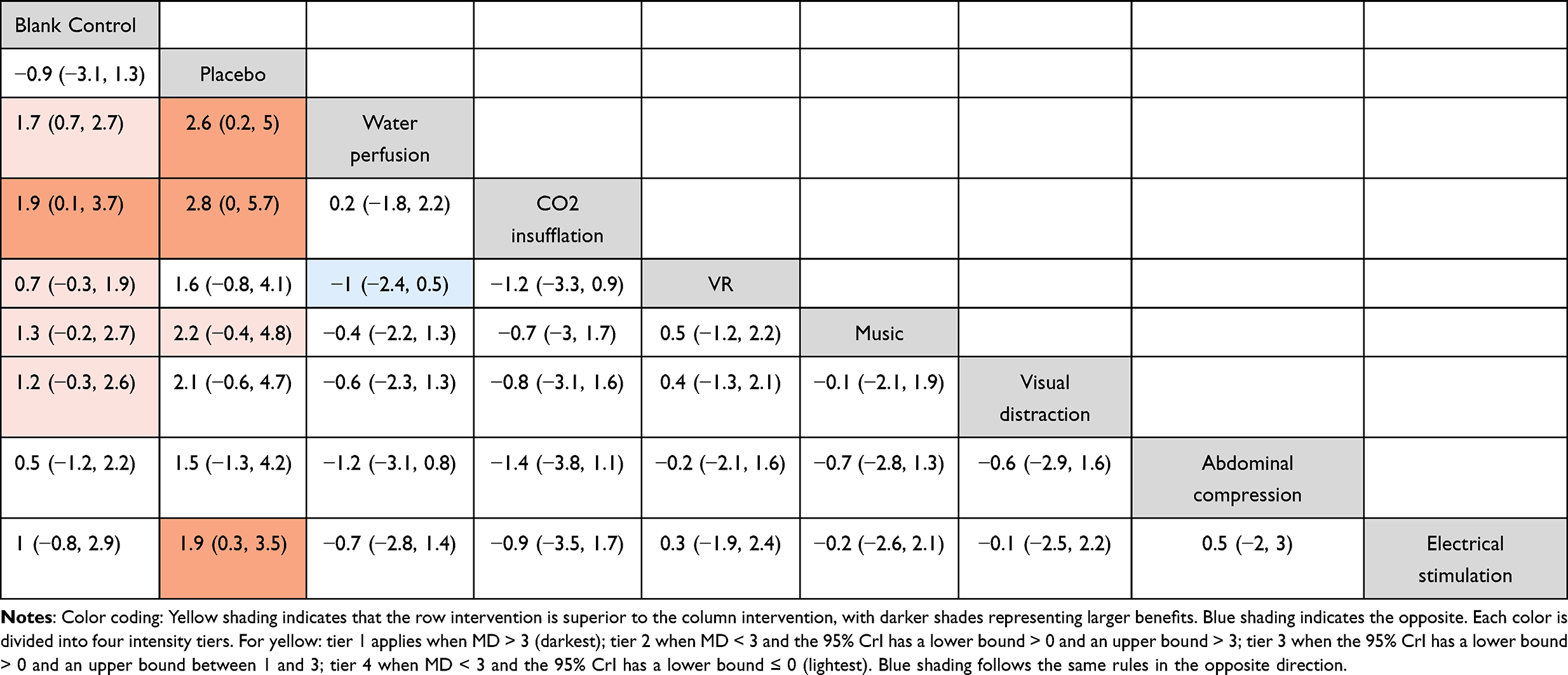 |
Table 2 League Tables of All Mean Differences and 95% Confidence Intervals by Nonpharmacological Interventions |
Pharmacological and Combined Intervention Measures
The most effective pain relief was observed with pethidine plus benzodiazepines and non-pharmacological interventions (MD = −5.1, 95% CrI: −8.6 to −1.7). Similarly, propofol combined with non-pharmacological interventions was associated with significant pain reduction (MD = −4.4, 95% CrI: −8.1 to −0.75). Other interventions with significant advantages included propofol alone (MD = −3.9, 95% CrI: −7.0 to −0.80), pethidine plus benzodiazepines/propofol (MD = −3.7, 95% CrI: −6.7 to −0.84), and fentanyl plus midazolam plus non-pharmacological interventions (MD = −2.9, 95% CrI: −5.2 to −0.61) (Figure 7s). Fentanyl plus midazolam/propofol (MD = −2.3, 95% CrI: −4.7 to 0.016) demonstrated a trend toward pain reduction but did not reach statistical significance. Finally, combinations involving nalbuphine, dezocine, or pentazocine (with benzodiazepines and non-pharmacological interventions, or with diazepam/midazolam) were less effective (Table 3).
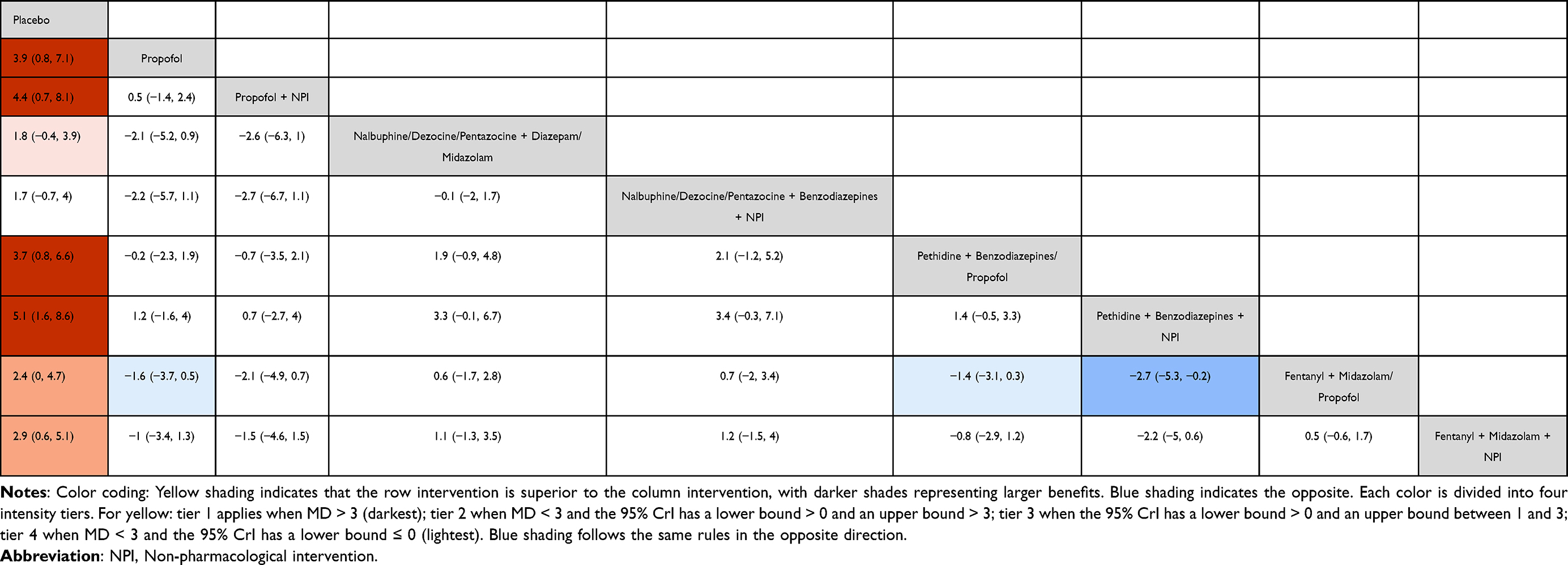 |
Table 3 League Tables of All Mean Differences and 95% Confidence Intervals by Pharmacological and Combined Interventions |
Superiority of Ranking
Figure 3 presents the SUCRA curves for all interventions. For all interventions combined (Figure 3a), the top three in terms of probability of being the best for pain relief were physical intervention plus analgesia and sedation (92.8%), propofol (81.2%), and water perfusion/CO2 insufflation (76.7%). Additionally, CO2/water perfusion plus analgesia and sedation (75.2%) and pethidine plus sedatives (66.8%) also showed high efficacy. For non-pharmacological interventions (Figure 3b), SUCRA analysis identified CO2 insufflation (88.0%) as the most effective strategy, followed by water perfusion (85.9%), with music (70.3%) and visual distraction (66.5%) also ranking highly. Finally, among pharmacological and combined interventions (Figure 3c), pethidine plus benzodiazepines and non-pharmacological interventions ranked highest (97.4%) for pain relief, followed by propofol plus non-pharmacological interventions (86.2%) and propofol alone (76.8%). Pethidine plus benzodiazepines/propofol (73.1%) and fentanyl plus midazolam plus non-pharmacological interventions (57.2%) were next in efficacy.
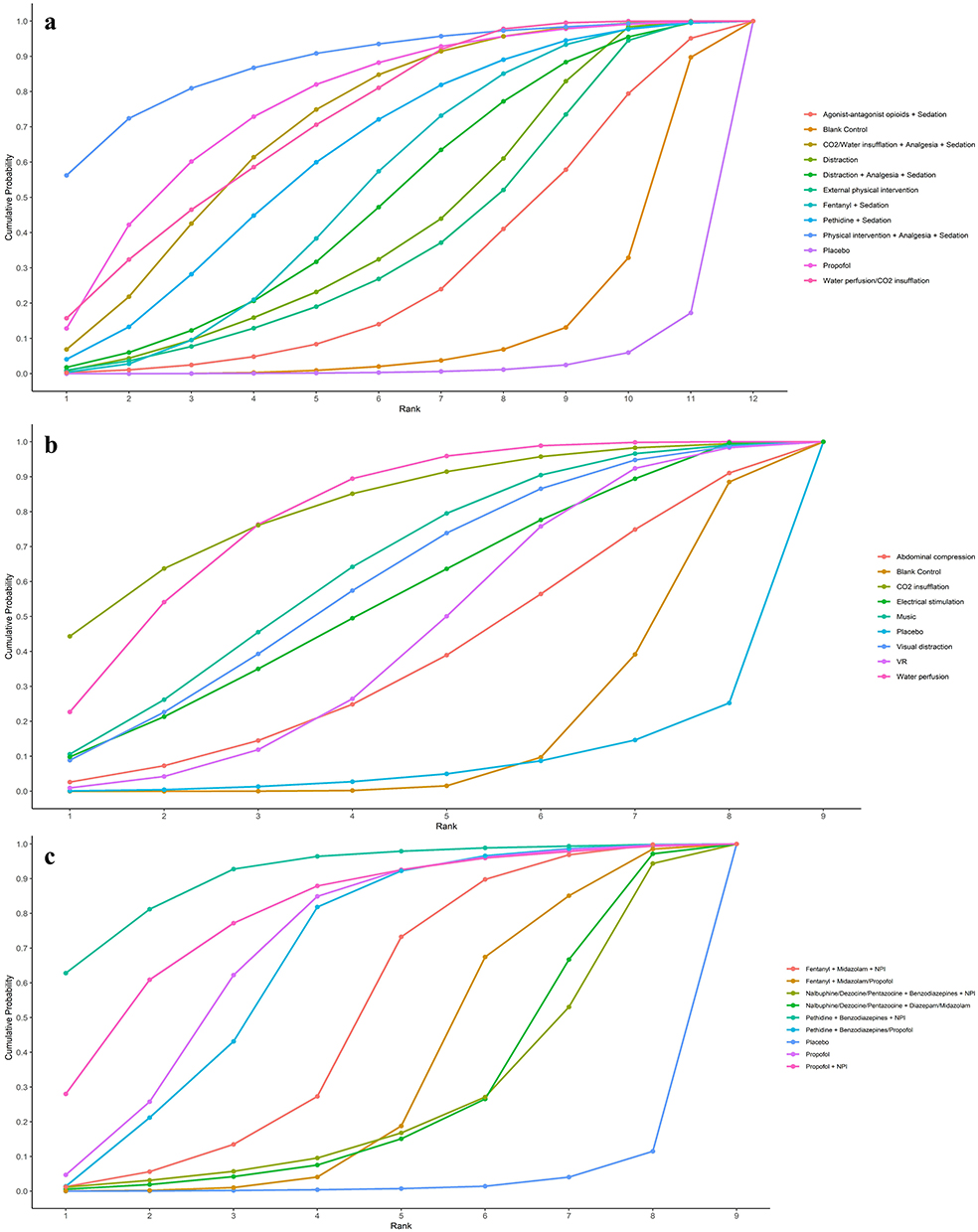 |
Figure 3 Probability of ranking for each intervention for outcomes. (a) All intervention measures; (b) Non-pharmacological intervention measures; (c) Pharmacological and combined intervention measures. Abbreviations: NPI, Non-pharmacological intervention. |
Discussion
In this comprehensive network meta-analysis of analgesic interventions for colonoscopy, multimodal strategies that combine pharmacological sedation, opioid analgesics, and non-pharmacological approaches yielded the most pronounced pain relief. Notably, the combination of pethidine with benzodiazepine sedatives and adjunctive physical interventions (such as CO2 insufflation or water perfusion) was associated with the highest efficacy. Deep sedation with propofol alone also emerged as one of the most effective single interventions, underscoring the potent analgesic and amnesic effects of deep sedation. Among non-pharmacological interventions, CO2 insufflation and water-aided techniques demonstrated significant analgesic benefits, ranking highest among standalone strategies. By contrast, standard moderate sedation regimens (such as fentanyl combined with midazolam) showed significant pain reduction compared to placebo but were less effective than multimodal drug-based strategies, possibly due to variation in drug dosing—some studies used minimum dosages, while others utilized patient-controlled sedation. Importantly, many pairwise differences had overlapping credible intervals, indicating some uncertainty regarding the precise rank order. Overall, combinations of analgesic modalities delivered the greatest pain relief, highlighting the need for individualized pain management by anesthesiologists and endoscopy nurses, particularly in older patients undergoing surveillance after colorectal cancer surgery, where careful attention to both drug dosages and non-pharmacological approaches is warranted.
Colonoscopy-related pain primarily arises from two sources: mechanical stretching caused by the endoscope and luminal distension due to insufflation. The non-pharmacological interventions examined in this study directly address these pain mechanisms. Replacing air with CO2 for insufflation alleviates discomfort, as CO2 is rapidly absorbed from the bowel, reducing luminal distension and bloating.57 There is evidence that water perfusion and CO2 insufflation, compared to air, significantly reduce colonoscopy-related pain and discomfort.58 Our analysis confirmed that CO2 insufflation resulted in significantly lower pain scores and improved patient comfort compared to air. Similarly, water-aided techniques (including water immersion and water exchange) reduce pain by minimizing mesenteric traction, maintaining minimal luminal distension, and facilitating easier advancement with fewer loop formations, thereby improving tolerance.59 These mechanisms explain why CO2 and water perfusion ranked as top non-pharmacological interventions in our study.
In terms of pharmacological options, deep sedation with propofol was highly effective. Previous studies have shown that patients report greater satisfaction with propofol compared to traditional benzodiazepine/opioid sedation, and there is a growing preference for propofol for colonoscopy sedation due to its rapid onset and potent analgesic effects.26 Importantly, propofol has a safety profile comparable to traditional sedation, with meta-analyses showing no increase in cardiopulmonary complications compared to midazolam-fentanyl regimens.60 Although propofol requires more intensive anesthesia support or monitoring, it represents an excellent option for providing a pain-free colonoscopy experience where resources allow. Among combined interventions, pethidine plus benzodiazepines with CO2 or water perfusion was also highly effective. Fentanyl plus midazolam remains one of the most widely used sedation regimens worldwide, with well-established efficacy and safety. Although our network meta-analysis showed a trend toward pain reduction for this combination (MD = −2.3, 95% CrI: −4.7 to 0.016), this did not reach statistical significance. This finding does not imply a lack of efficacy—extensive evidence supports its use over unsedated colonoscopy—but likely reflects variability in dosing regimens and sedation protocols among studies.26,29,31,43 In clinical practice, standard dosing of opioid and benzodiazepine combinations remains an effective method for moderate sedation during colonoscopy, though its analgesic efficacy may be inferior to propofol.
While other non-pharmacological interventions (such as distraction techniques and transcutaneous nerve stimulation) did not demonstrate significant pain reduction, they nonetheless contributed to improved patient tolerance. Music therapy and audiovisual distraction have been validated as simple, low-risk approaches to reduce anxiety and discomfort during colonoscopy. A recent meta-analysis concluded that music during colonoscopy enhances the patient experience and significantly reduces both pain and anxiety.61 Our analysis similarly identified VR, music, and visual distraction as higher-ranking non-pharmacological strategies. By engaging patient attention and alleviating anxiety, distraction techniques likely enhance pain tolerance and procedure tolerability. Additionally, our results indicate that electrical stimulation and acupuncture, although not statistically significant, may offer supplementary analgesia. When combined with pharmacological interventions, these effects may be additive; for example, adjunctive use of TENS or acupuncture with sedation and analgesia could lower required drug doses and improve overall comfort. In clinical application, the number and type of combined interventions may be limited by available resources, but our findings highlight that multimodal analgesia is highly effective for colonoscopy.
Significant heterogeneity (I2 > 90%) was observed among studies, likely attributable to the large number of indirect comparisons, variations in intervention techniques (eg, water perfusion methods), non-standardized drug dosages, and differences in pain measurement timing and scales. Despite this heterogeneity, our network meta-analysis showed good overall consistency, with node-splitting analysis revealing no significant differences between direct and indirect evidence.
We stratified the analyses into non-pharmacological and pharmacological/combined subnetworksto improve clinical interpretability. First, control types differed across trials: sedative or analgesic studies typically used placebo controls such as saline, whereas non-pharmacological studies generally used blank controls such as no additional intervention with standard air insufflation. Mixing these would conflate expectation effects and risk bias. Second, placing all interventions into a single network would create an overly complex, sparsely connected geometry and yield imprecise or unstable estimates. Accordingly, Table 1 pools all interventions and necessarily includes both blank and placebo nodes with more indirect paths, whereas Table 3 restricts the evidence to pharmacological and combined arms with placebo as the primary comparator. Because control expectations and network connectivity differ, posterior estimates can legitimately shift without implying bias; for example, the effect for propofol versus placebo appears as 3.0 in all-interventions network and 3.9 in pharmacological/combined subnetwork, reflecting network geometry and evidence composition, which showed no important local inconsistency after subnetworking despite high global heterogeneity.
Our findings provide clear evidence-based guidance to improve patient comfort during colonoscopy. Key non-pharmacological methods—such as CO2 insufflation and water-assisted techniques—are simple, cost-effective, and significantly reduce discomfort. CO2 insufflation is especially recommended, as it has been proven to lessen post-procedure pain and bloating compared to traditional air insufflation. Water-assisted methods (immersion or exchange) further reduce pain and are particularly valuable in settings with limited access to sedation or anesthesia. Where deep sedation is not feasible, moderate sedation with benzodiazepines and opioids remains effective. Combining pharmacological and non-pharmacological strategies can further enhance comfort.
Several limitations of this study should be acknowledged. Significant heterogeneity existed among included studies, likely resulting from differences in patient populations, intervention protocols, sedation regimens, and pain assessment methods. Additionally, interventions were grouped into broader categories to ensure feasibility, which may have masked differences between specific techniques or drug regimens. Our analysis focused only on procedural pain outcomes and did not assess other important endpoints such as anxiety, patient satisfaction, cecal intubation rate, or adenoma detection rate.
Conclusion
This network meta-analysis provides a comprehensive comparison of pharmacological, non-pharmacological, and combined interventions for pain management during colonoscopy. Our results demonstrate that combined interventions—particularly pethidine plus midazolam/propofol with CO2 or water perfusion—are the most effective strategies for alleviating procedure-related pain. Among pharmacological approaches, pethidine plus midazolam/propofol and propofol alone showed the greatest analgesic efficacy. CO2 insufflation and water perfusion were the most effective non-pharmacological options and can significantly reduce pain even in the absence of sedation. In settings with anesthesia support, multimodal strategies should be prioritized to maximize pain relief and completion. Where such resources are limited, CO2 insufflation or water-aided methods provide effective, scalable options. Framing decisions at the strategy level aligns analgesia with local resources and patient preferences.
Funding
National Key Research and Development Program of China, 2019YFC1711803; National Health Commission of the People’s Republic of China, SZ2024HL010.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Zhang Jinzhu YM, Xishan W. A comparison and reflection on the epidemiology and disease burden of colorectal cancer in China, the United States, and the world. Chinese J Colorectal Dis. 2024;13(2):89–93. doi:10.3877/cma.j.issn.2095-3224.2024.02.001
3. Ikuta KS, Swetschinski LR, Robles Aguilar G, et al. Global mortality associated with 33 bacterial pathogens in 2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2022;400(10369):2221–2248. doi:10.1016/S0140-6736(22)02185-7
4. Bernardo WM, Averbach M, Moura EGH. Critical appraisal of the clinical trial: effect of colonoscopy screening on risks of colorectal cancer and related death. Arq Bras Cir Dig. 2023;36:e1719. doi:10.1590/0102-672020230002e1719
5. Bugajski M, Wieszczy P, Hoff G, et al. Modifiable factors associated with patient-reported pain during and after screening colonoscopy. GUT. 2018;67(11):1958–1964. doi:10.1136/gutjnl-2017-313905
6. Denberg TD, Melhado TV, Coombes JM, et al. Predictors of nonadherence to screening colonoscopy. J Gen Intern Med. 2005;20(11):989–995. doi:10.1111/j.1525-1497.2005.00164.x
7. Shim S, Yoon BH, Shin IS, et al. Network meta-analysis: application and practice using Stata. Epidemiol Health. 2017;39:e2017047. doi:10.4178/epih.e2017047
8. Ahmed JF, Ashrafian H, Darzi A, et al. The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis. Ther Adv Gastroenterol. 2025;18:17562848251378236. doi:10.1177/17562848251378236
9. Sinonquel P, Jans A, Bisschops R. Painless colonoscopy: fact or fiction? Clin Endosc. 2024;57(5):581–587. doi:10.5946/ce.2024.001
10. Lunny C, Higgins JPT, White IR, et al. Risk of bias in network meta-analysis (RoB NMA) tool. BMJ. 2025;388:e079839. doi:10.1136/bmj-2024-079839
11. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/m14-2385
12. Luo D, Wan X, Liu J, et al. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
13. Wan X, Wang W, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135. doi:10.1186/1471-2288-14-135
14. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
15. Higgins JP, Jackson D, Barrett JK, et al. Consistency and inconsistency in network meta-analysis: concepts and models for multi-arm studies. Res Synth Methods. 2012;3(2):98–110. doi:10.1002/jrsm.1044
16. watt J, Del Giovane C. Network meta-analysis. Methods Mol Biol. 2022;2345:187–201. doi:10.1007/978-1-0716-1566-9_12
17. Wong JC, Yau KK, Cheung HY, et al. Towards painless colonoscopy: a randomized controlled trial on carbon dioxide-insufflating colonoscopy. ANZ J Surg. 2008;78(10):871–874. doi:10.1111/j.1445-2197.2008.04683.x
18. Leung JW, Mann SK, Siao-Salera R, et al. A randomized, controlled comparison of warm water infusion in lieu of air insufflation versus air insufflation for aiding colonoscopy insertion in sedated patients undergoing colorectal cancer screening and surveillance. Gastrointest Endosc. 2009;70(3):505–510. doi:10.1016/j.gie.2008.12.253
19. Geyer M, Guller U, Beglinger C. Carbon dioxide insufflation in routine colonoscopy is safe and more comfortable: results of a randomized controlled double-blinded trial. Diagn Ther Endosc. 2011;2011:378906. doi:10.1155/2011/378906
20. Radaelli F, Paggi S, Amato A, et al. Warm water infusion versus air insufflation for unsedated colonoscopy: a randomized, controlled trial. Gastrointest Endosc. 2010;72(4):701–709. doi:10.1016/j.gie.2010.06.025
21. Amer-Cuenca JJ, Goicoechea C, Girona-López A, et al. Pain relief by applying transcutaneous electrical nerve stimulation (TENS) during unsedated colonoscopy: a randomized double-blind placebo-controlled trial. Eur J Pain. 2011;15(1):29–35. doi:10.1016/j.ejpain.2010.05.006
22. Pohl J, Messer I, Behrens A, et al. Water infusion for cecal intubation increases patient tolerance, but does not improve intubation of unsedated colonoscopies. Clin Gastroenterol Hepatol. 2011;9(12):1039–43.e1. doi:10.1016/j.cgh.2011.06.031
23. Toros AB, Ersoz F, Ozcan O. Does a fitted abdominal corset makes colonoscopy more tolerable? Dig Endosc. 2012;24(3):164–167. doi:10.1111/j.1443-1661.2011.01207.x
24. Szura M, Pach R, Matyja A, et al. Carbon dioxide insufflation during screening unsedated colonoscopy: a randomised clinical trial. Eur J Cancer Prev. 2015;24(1):37–43. doi:10.1097/cej.0000000000000047
25. Umezawa S, Higurashi T, Uchiyama S, et al. Visual distraction alone for the improvement of colonoscopy-related pain and satisfaction. World J Gastroenterol. 2015;21(15):4707–4714. doi:10.3748/wjg.v21.i15.4707
26. Schroeder C, Kaoutzanis C, Tocco-Bradley R, et al. Patients prefer propofol to midazolam plus fentanyl for sedation for colonoscopy: results of a single-center randomized equivalence trial. Dis Colon Rectum. 2016;59(1):62–69. doi:10.1097/dcr.0000000000000512
27. Azevedo R, Leitão C, Pinto J, et al. Can water exchange improve patient tolerance in unsedated colonoscopy a prospective comparative study. GE Port J Gastroenterol. 2018;25(4):166–174. doi:10.1159/000484093
28. Pontone S, Palma R, Donato G, et al. Efficacy of sedation by midazolam in association with meperidine or fentanyl and role of patient distress during elective colonoscopy. Gastroenterol Nurs. 2020;43(3):258–263. doi:10.1097/sga.0000000000000456
29. Veldhuijzen G, Klaassen NJM, Van Wezel RJA, et al. Virtual reality distraction for patients to relieve pain and discomfort during colonoscopy. Endosc Int Open. 2020;8(7):E959–e66. doi:10.1055/a-1178-9289
30. Joan Gan CY, Chan KK, Tan JH, et al. Smartphone-controlled patch electro-acupuncture versus conventional pain relief during colonoscopy: a randomized controlled trial. ANZ J Surg. 2021;91(6):E375–e81. doi:10.1111/ans.16870
31. Brix LD, Pedersen ASB. Effect of music intervention in colonoscopy-naïve adults: a randomised controlled trial. Br J Nurs. 2022;31(10):526–532. doi:10.12968/bjon.2022.31.10.526
32. Cakir SK, Evirgen S. Three distraction methods for pain reduction during colonoscopy: a randomized controlled trial evaluating the effects on pain and anxiety. J Perianesth Nurs. 2023;38(5):e1–e7. doi:10.1016/j.jopan.2023.02.007
33. Huang X, Wang H, Shi L, et al. Effect of transcutaneous electrical nerve stimulation based on wrist-ankle acupuncture theory for pain relief during colonoscopy without anesthesia: a randomized controlled trial. Endoscopy. 2024;57(02):158–165. doi:10.1055/a-2373-0513
34. Shamali M, Vilmann P, Johansen NR, et al. Virtual reality intervention to improve quality of care during colonoscopy: a hybrid type 1 randomized controlled trial. Gastrointest Endosc. 2024;100(5):914–922.e2. doi:10.1016/j.gie.2024.05.023
35. Hirani AAA, Ismail FW, Abdulaziz F, et al. The effects of music therapy on patients undergoing colonoscopy in a tertiary care hospital at karachi, pakistan: a comparative study. J Pain Palliat Care Pharmacother. 2024:1–11. doi:10.1080/15360288.2024.2357551
36. Hayee BH, Dunn J, Loganayagam A, et al. Midazolam with meperidine or fentanyl for colonoscopy: results of a randomized trial. Gastrointestinal Endoscopy. 2009;69(3):681–687. doi:10.1016/j.gie.2008.09.033
37. Hsieh Y-H, Chou A-L, Lai -Y-Y, et al. Propofol alone versus propofol in combination with meperidine for sedation during colonoscopy. J Clin Gastroenterol. 2009;43(8):753–757. doi:10.1097/MCG.0b013e3181862a8c
38. Leung FW, Jackson G, Okamoto KE, et al. A proof-of-concept RCT of water vs. air method in scheduled, unsedated colonoscopy in united states veterans - final report demonstrating significantly improved outcomes in unsedated colonoscopy by the water method. Gastroenterology. 2010;138(5):S56–S57. doi:10.1016/S0016-5085(10)60256-9
39. Hsieh Y-H, Lin H-J, Tseng K-C. Limited water infusion decreases pain during minimally sedated colonoscopy. World J Gastroenterol. 2011;17(17):2236–2240. doi:10.3748/wjg.v17.i17.2236
40. Bayupurnama P, Ratnasari N, Indrarti F, et al. The water-aided method in routine unsedated colonoscopy: a randomized controlled trial (RCT) in diagnostic cases in indonesian patients presidential poster. Am J Gastroenterol. 2012;107:S733–S34. doi:10.14309/00000434-201210001-01802
41. Chen Y, Wu W, Yao Y, et al. Transcutaneous electric acupoint stimulation at Jiaji points reduce abdominal pain after colonoscopy: a randomized controlled trial. Int J Clin Exp Med. 2015;8(4):5972–5977.
42. Jiang X, Li X, Zhou Hui L. Effects of visual and audiovisual distraction on pain and anxiety among patients undergoing colonoscopy. Gastroenterol Nurs. 2015;38(1):55–61. doi:10.1097/sga.0000000000000089
43. Ko SY. The effectiveness of music interventions on anxiety level, pain level and satisfaction for Chinese adult patients undergoing colonoscopy. 2016.
44. Adigun TA, Akere A, Ayandipo OO, et al. A comparison of propofol - fentanyl with midazolam - pentazocine combination for sedation and analgesia during colonoscopy in Ibadan Nigeria. J Clin Sci. 2019;16(1):1–6. doi:10.4103/jcls.jcls_38_18
45. Hsieh Y-H, Tseng C-W, Koo M, et al. Feasibility of sedation on demand in Taiwan using water exchange and air insufflation: a randomized controlled trial. J Gastroenterol Hepatol. 2020;35(2):256–262. doi:10.1111/jgh.14839
46. Cakir SK, Evirgen S. The effect of virtual reality on pain and anxiety during colonoscopy: a randomized controlled trial. Turk J Gastroenterol. 2021;32(5):451–457. doi:10.5152/tjg.2021.191081
47. Han C, Xu T, Sheng L, et al. Improving the discomfort and satisfaction of colonoscopy by distraction with smartphones A prospective randomized controlled study. Medicine. 2021;100(9):e23799. doi:10.1097/md.0000000000023799
48. Liu Q, Zang Y, Zang W, et al. Implementation of virtual reality technology to decrease patients’ pain and nervousness during colonoscopies: a prospective randomised controlled single-blinded trial. Clin Med. 2022;22(3):237–240. doi:10.7861/clinmed.2022-0001
49. Sun D-J, You Y-X, He X-J, et al. Effects of light music played by piano intervention on satisfaction, anxiety, and pain in patients undergoing colonoscopy: a randomized controlled trial. Medicine. 2022;101(52):e32339. doi:10.1097/md.0000000000032339
50. Tani A, Tartarisco G, Vagheggini G, et al. Binaural beats reduce feeling of pain and discomfort during colonoscopy procedure in not-sedated patients: a randomized control trial. Complementary Ther Clin Pract. 2022;48:101605. doi:10.1016/j.ctcp.2022.101605
51. Veisman I, Duchan MT, Lahat A, et al. Unsedated colonoscopy utilizing virtual reality distraction: a pilot-controlled study. Surg Endoscopy Other Interventional Techniq. 2024;38(9):5060–5067. doi:10.1007/s00464-024-10999-1
52. Chen Y, Du B, Yang C, et al. Insufflation of carbon dioxide at colonoscopy elevates degree of comfort in elderly patients: a randomized controlled trial. Chinese J Gastroenterol. 2012;17(5):288–292. doi:10.3969/j.issn.1008-7125.2012.05.008
53. Cao Y, Wang P. Impact of water infusion colonoscopy on abdominal pain and inflammatory response in elderly patients. Chinese J Gastroenterol. 2017;22(1):40–42. doi:10.3969/j.issn.1008-7125.2017.01.009
54. He T, Liu C, Lu Z-X, et al. Effect of wrist-ankle acupuncture on propofol dosage during painless colonoscopy: a randomized controlled prospective study. World J Clin Cases. 2022;10(12):3764–3772. doi:10.12998/wjcc.v10.i12.3764
55. Ni YF, Lian QQ, Jiang PW, et al. Application of acupuncture analgesia in colonoscopy. Zhongguo Zhen Jiu. 2008;27(10):766–768.
56. De Silva AP, Niriella MA, Nandamuni Y, et al. Effect of audio and visual distraction on patients undergoing colonoscopy: a randomized controlled study. Endoscopy Int Open. 2016;4(11):E1211–E14. doi:10.1055/s-0042-117630
57. Mallette K, Dhalla S. Carbon dioxide versus room air insufflation in colonoscopy: a comparative study. Digestive System. 2017;1(2). doi:10.15761/DSJ.1000108
58. Holme Ø, Bretthauer M. Pain and sedation during colonoscopy - a never ending story. Endosc Int Open. 2016;4(5):E538–9. doi:10.1055/s-0042-106085
59. Arnaert S, Persyn D, Cool M, et al. Unsedated or on-demand minimally sedated water-aided outpatient colonoscopy in colorectal cancer screening and surveillance: a step forward or backward? experience from daily practice in a regional (Nonacademic) hospital. Diagnostics. 2024;14(22):2596. doi:10.3390/diagnostics14222596
60. Wadhwa V, Issa D, Garg S, et al. Similar risk of cardiopulmonary adverse events between propofol and traditional anesthesia for gastrointestinal endoscopy: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2017;15(2):194–206. doi:10.1016/j.cgh.2016.07.013
61. Saab O, Al-Obaidi H, Merza N, et al. The impact of visual distraction interventions on patients’ pain and anxiety during colonoscopy: a systematic review and meta-analysis of randomized controlled trials. J Clin Gastroenterol. 2024. doi:10.1097/mcg.0000000000002086
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.