Back to Journals » Journal of Pain Research » Volume 18
Comparative Effectiveness of Optimized Versus Conventional Perioperative Care in Unilateral Biportal Endoscopy for Lumbar Degenerative Disease: A Single-Center Retrospective Study
Authors Cui M, Tan S, Liu Y, Wang X, Chen M, Tang Y, Ding L
Received 30 August 2025
Accepted for publication 14 October 2025
Published 30 October 2025 Volume 2025:18 Pages 5701—5714
DOI https://doi.org/10.2147/JPR.S559658
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Miaomiao Cui,1,* Shengzhi Tan,1,* Yu Liu,2 Xin Wang,1 Mengshi Chen,1 Yujuan Tang,1 Liping Ding1
1Department of Spinal Surgery II, Ninth Medical Center, PLA General Hospital, Chaoyang District, Beijing, 100101, People’s Republic of China; 2Department of Anesthesiology, Ninth Medical Center, PLA General Hospital, Chaoyang District, Beijing, 100101, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liping Ding, Department of Spinal Surgery II, Ninth Medical Center, PLA General Hospital, Chaoyang District, No. 9, Anxiang Beili, Chaoyang District, Beijing, 100101, People’s Republic of China, Email [email protected]
Objective: To analyze the effect of perioperative nursing optimization in patients with lumbar degenerative diseases treated with percutaneous unilateral biportal endoscopy (UBE).
Methods: This observational, retrospective cohort study analyzed the data of 105 patients with lumbar degenerative diseases who underwent UBE surgery in the Department of Spine Surgery of PLA General Hospital Ninth Medical Center from June 2022 to December 2024. According to different nursing optimization methods, 49 patients were assigned to the conventional group (conventional nursing intervention) and 56 patients were assigned to the intervention group (perioperative nursing optimization). The anxiety, depression, waist/leg pain, quality of life, self-care ability and functional disability of the patients were evaluated by the self-rating anxiety scale (SAS), self-rating depression scale (SDS), visual analogue score (VAS) for waist/leg pain, quality of life scale score (SF-36), Barthel score and disability index (ODI). The incidence of complications was compared between the two groups.
Results: The emotional state, quality of life, self-care ability, and functional impairment of the intervention group were more significantly improved after optimization than those of the conventional group (P< 0.05). The VAS score of waist/leg pain in the intervention group was significantly lower than that in the conventional group after surgery (P< 0.05). The total incidence of complications in the intervention group was 7.14%, and the total incidence of complications in the conventional group was 20.41%. The difference between the two groups was significant (P< 0.05).
Conclusion: The optimization of perioperative nursing in patients undergoing UBE surgery for lumbar degenerative diseases can relieve patients’ negative emotions such as perioperative anxiety and depression, reduce postoperative pain symptoms, improve quality of life, enhance self-care ability, improve functional impairment, and promote postoperative recovery.
Keywords: lumbar degenerative diseases, unilateral biportal endoscopy, optimization of perioperative nursing, pain symptoms, quality of life
Introduction
Lumbar degenerative diseases include spondylolisthesis, lumbar disc herniation, and lumbar spinal stenosis, which can cause low back and leg pain and neurogenic intermittent claudication. Severe cases require surgical treatment.1–3 In recent years, minimally invasive spinal endoscopic technology has flourished. Minimally invasive spinal surgery has seen remarkable advancements in recent years, with Unilateral Biportal Endoscopy (UBE) emerging as a prominent technique for the treatment of lumbar degenerative diseases. The rapid proliferation of this surgical modality is not merely anecdotal but is substantiated by significant growth in both academic research and clinical application. A bibliometric analysis published in 2022 revealed a steep increase in UBE-related publications, indicating a burgeoning interest and widespread academic validation within the surgical community.4 This academic momentum is mirrored by substantial market adoption; the global UBE market was valued at USD 941.3 million in 2024 and is projected to expand at a compound annual growth rate (CAGR) of 6.0% from 2025 to 2030, underscoring its escalating integration into clinical practice.5 Furthermore, numerous recent systematic reviews and meta-analyses have firmly established the clinical efficacy and safety of UBE. These studies consistently demonstrate that UBE achieves comparable, if not superior, outcomes to traditional open surgery and other minimally invasive techniques, with distinct advantages including reduced intraoperative blood loss, shorter hospital stays, and lower complication rates.6,7 Collectively, this body of evidence confirms that UBE is not only gaining traction but is solidifying its position as a mainstream surgical option for managing lumbar degenerative conditions. However, lumbar degenerative diseases are more common in the middle-aged and elderly population, whose physical functions gradually deteriorate, and most people have underlying diseases. Postoperative pain, swelling and other reasons will affect the rehabilitation effect.8 At the same time, we have found in clinical practice that patients’ doubts about the surgery and its efficacy can lead to negative emotional states. This aligns with contemporary paradigms in spine care, which emphasize a holistic patient care approach, recognizing that psychosocial factors significantly impact treatment outcomes.9 Such emotional distress can cause unstable vital signs and even temporary refusal of surgery, affecting surgical progress, prolonging operation times, and consequently increasing the incidence of complications like bleeding.10–12
During surgical treatment, the quality of nursing work will directly affect the surgical effect. Therefore, optimizing perioperative nursing is an important measure to ensure the smooth progress of the operation.13 This concept aligns with the principles of Enhanced Recovery After Surgery (ERAS), which is a multimodal, evidence-based approach designed to attenuate the surgical stress response and accelerate patient recovery. The successful application of ERAS protocols has been demonstrated across various surgical disciplines.14,15 Perioperative quality nursing services, embodying the core ERAS principle of being patient-centered, reflect the people-oriented concept. Through preoperative psychological counseling, patients can reduce their anxiety, fear and other negative psychological conditions and gain a sense of security and comfort. Close postoperative observation and early functional exercise are conducive to reducing the incidence of complications and promoting patient recovery.16,17 Our hospital applies such perioperative quality nursing services to patients undergoing unilateral biportal endoscopy, hoping to relieve the pain of patients with lumbar degenerative diseases and promote their rapid recovery.
Materials and Methods
Participants
This study is an observational, retrospective cohort study. A total of 105 patients with lumbar degenerative diseases who underwent UBE surgery in the Department of Spine Surgery of PLA General Hospital Ninth Medical Center from June 2022 to December 2024 were included in the study. The data retrieval from the electronic medical record system for this specific study was performed after obtaining ethical approval (Approval No.: 2025–05-15). The clinical data of the patients were retrieved from the electronic medical record system for retrospective analysis. Inclusion criteria: ① Patients diagnosed with lumbar degenerative diseases based on symptoms, signs, and imaging examinations; ② Patients meeting surgical indications who voluntarily undergo Unilateral Biportal Endoscopy (UBE) surgery; ③ Patient consciousness is clear, defined as a Glasgow Coma Scale (GCS) score of 15,18 and able to cooperate in completing scale assessments; ④ Patients whose symptoms have not been significantly relieved after more than 3 months of conservative treatment. “Significant relief” is operationally defined as meeting at least one of the following Minimal Clinically Important Difference (MCID) criteria: a decrease of ≥2.1 points in the Back Pain Visual Analogue Scale (BP-VAS) or ≥2.8 points in the Leg Pain VAS (LP-VAS),19 or a decrease of ≥10 points in the Oswestry Disability Index (ODI).20 Exclusion criteria: ① Patients with multi-segment lumbar lesions; ② Patients with lumbar instability or lumbar spondylolisthesis II° or above; ③ Patients with a history of spinal deformity and lumbar surgery; ④ Patients with lumbar infection, tumors, lumbar fractures, and severe medical diseases; ⑤ Patients with infectious diseases or abnormal immune mechanisms. A total of 105 patients with lumbar degenerative diseases were divided into groups. Patients were allocated to the conventional group (n=49) if they received surgery between June 2022 and March 2023, during which period conventional perioperative nursing was implemented. Patients in the intervention group (n=56) underwent surgery between April 2023 and December 2024, during which the optimized perioperative nursing protocol was introduced. The allocation was based solely on the timing of surgery relative to the implementation of the new nursing protocol, and there was no randomization or matching procedure applied. This study was approved by the hospital ethics committee (ethics approval number: 2025–05-15).
Nursing Methods
Throughout the study period, all UBE surgeries were performed by the same surgical team using consistent surgical techniques and equipment. The only systematic difference between the two periods was the implementation of the optimized nursing protocol.
The optimized nursing protocol, which was applied during the treatment period of the optimized group, adheres to the core principles of ERAS. The ERAS pathway is a multimodal, evidence-based approach aimed at attenuating the patient’s surgical stress response, thereby reducing complications, shortening hospital stays, and accelerating postoperative recovery. This protocol, therefore, integrates a series of optimized interventions that span the entire perioperative period, including preoperative patient education and preparation, intraoperative management, and postoperative rehabilitation, which are detailed below.
The conventional group received conventional nursing interventions, including (1) routine education upon admission, introduction of surgical information, including surgical method, fasting time, and preoperative functional exercise methods; (2) fasting for 8 hours before surgery, and close monitoring of vital signs during surgery; (3) lying flat for 6 hours after surgery, informing patients to eat and drink 6 hours after surgery, observing the recovery of lower limb muscle strength, closely observing vital signs and wound conditions, observing bowel movements, and encouraging self-urination; (4) following the doctor’s advice, giving patients drug treatment, maintaining electrolyte balance, conducting pain assessments, and giving timely drug analgesia; (5) eating a reasonable diet, enhancing nutrition, providing psychological care, introducing surgical conditions, treatment and nursing content, promptly relieving various concerns during the recovery period, and ensuring sleep; (6) health education, explaining functional exercise methods: actively moving the joint muscles of both lower limbs, doing straight leg raising exercises, and performing back muscle exercises 3 weeks after surgery.
The intervention group received optimized perioperative nursing intervention. (1) Preoperative nursing: ① Personalized health education. According to the patient’s acceptance level, the concept of rapid recovery was introduced to the patient or caregiver to obtain their cooperation. The operation was fully introduced, and the experience of similar patients’ rehabilitation was explained to relieve the patient’s fear of surgery and anxiety about postoperative recovery. The patient was guided to train the habit of urinating and defecating in bed. The patient was taught how to turn over and exercise the waist and back muscles, and to insist on doing prone position training every day, so that the patient would have a perceptual understanding, which would help improve the compliance of postoperative rehabilitation exercises. ② Psychological support. The nurse conducted an interview information survey on the patient and conducted motivational interviews with the patient and his family, namely narrative listening. The interview clarified the patient’s education level, understanding of the disease and surgery, family situation, etc. Listen to the narrative to reduce the sense of unfamiliarity, communicate face-to-face in an independent room, place green plants in the room, play relaxing music, and let the patient narrate the event in a calm state of mind. Pay attention to protecting the patient’s privacy and do not interrupt the narration. Finally, the patient was introduced to the matters related to the surgery. After the narration was completed, the patient was evaluated and sorted out, the patient’s psychological changes were recorded, the main factors of psychological pressure were analyzed, and targeted solutions were formulated. ③ Pain management: Considering that the pain levels of different patients with lumbar disc herniation vary, some patients who complain of obvious pain can be given preoperative analgesia. The oral medications used are celecoxib or loxoprofen sodium tablets.
Intraoperative Care: ① Intraoperative temperature management: Maintaining intraoperative normothermia is a critical component of our standardized patient care protocol, with a target core body temperature of ≥36.0°C.21,22 To achieve this, a multi-modal approach is implemented for all patients undergoing surgery. The ambient operating room temperature is maintained at a minimum of 21°C. Active warming is provided throughout the procedure using a forced-air warming (FAW) system, with warming blankets applied to the non-operative areas of the body to maximize surface area coverage.23 Furthermore, all intravenous fluids and surgical irrigation fluids are warmed to approximately 37°C prior to administration, a measure that is particularly crucial in endoscopic procedures requiring large volumes of irrigation fluid.24,25 As an objective measurement criterion, the patient’s core temperature is continuously monitored throughout the surgery via an esophageal or nasopharyngeal probe, allowing for timely adjustments to the warming interventions.21②Intraoperative urinary catheterization management: In accordance with ERAS principles and guidelines aimed at reducing catheter-associated urinary tract infections (CAUTI), routine intraoperative urinary catheterization is strictly avoided.26,27 A urinary catheter is placed only when specific clinical indications are present, such as an anticipated surgical duration exceeding 1.5 to 2 hours, the need for precise urine output monitoring for hemodynamic management, or pre-existing urinary retention.28 For patients who do not meet these criteria but where significant bladder filling is suspected during the procedure, a non-invasive portable bladder scanner is utilized as an objective measurement tool to assess bladder volume. This allows the clinical team to make an informed decision and avoid unnecessary catheterization.29 If a urinary catheter is deemed necessary and is placed intraoperatively, the protocol dictates its removal at the earliest possible opportunity, which is typically at the conclusion of the surgery or within the post-anesthesia care unit (PACU), to minimize infection risk and promote early patient mobility.
Postoperative bed-out exercise and rehabilitation exercises. The design of our postoperative rehabilitation protocol is enhanced by integrating contemporary movement-based approaches, such as the joint-by-joint training paradigm.30 This approach provides a stronger scientific rationale for our functional exercise progressions by emphasizing that the lumbar spine, a segment requiring high stability, is protected and functions optimally when the adjacent joints—primarily the hips and thoracic spine—possess full mobility. Therefore, the subsequent exercises, while targeting lumbar function, are conceptually aimed at restoring this crucial balance between proximal mobility and core stability. The content of postoperative rehabilitation exercises mainly includes straight leg raising training and lumbar spine function training. After the patient’s pain is relieved and the condition is stable, the nursing staff will give the patient straight leg raising training guidance, that is, let the patient lie on a hard bed, take a supine position, lift both lower limbs off the bed, straighten both lower limbs, until the patient’s lower limbs have radiating pain, hold for 5 to 10 seconds, and slowly put down both lower limbs. Repeat 10 to 15 times each time, 4 times/d. When training lumbar spine function, the five-point support method and the four-point support method can be implemented. The five-point support method is adopted, and the support points are the elbows, feet and head. The patient uses force to lift the lower limbs and trunk off the bed, and do hip joint and spine hyperextension training. After holding for 10 to 15 seconds, the body is slowly lowered. Repeat 15 to 20 times each time, 3 to 4 times/d; the four-point support method is adopted, and the heels and elbows are the four support points of the body. The patient uses force to lift the lower limbs and trunk off the bed, keeps the hip joints and spine hyperextension, and holds for about 15 seconds before the body is slowly lowered. Repeat 15 to 20 times each time, 3 to 4 times/d. During the rehabilitation process, the responsible nurse fully understands the patient’s lumbar spine function recovery and functional exercise progress, keeps good records, and provides timely feedback to the attending physician. At the same time, the nurse dynamically adjusts the exercise plan and intensity according to the patient’s specific situation.
Evaluation Indicators
The data for all outcome measures (SAS, SDS, VAS, SF-36, Barthel, ODI, and complications) were extracted retrospectively from the electronic medical records. These scores were routinely collected and documented by ward nurses during the patients’ hospitalization as part of standard clinical care. The nurses who administered the questionnaires and assessed the outcomes were not formally blinded to the patients’ group assignment, as the nursing protocol was an integral part of their treatment. However, the use of standardized and validated scales (SAS, SDS, VAS, etc) was intended to minimize assessment subjectivity.
- Emotional state: SAS and SDS scores were used to evaluate anxiety and depression in patients with lumbar degenerative diseases. Each scale has 20 items, with each item ranging from 1 to 4 points, and a standard score of 100 points. A SAS score of >50 points indicates anxiety, and an SDS score of >53 points indicates depression. The scores are positively correlated with the degree of anxiety and depression in patients. The evaluation time was before optimization and 3 days after optimization.
- Waist/leg pain: VAS was used to evaluate the waist/leg pain in patients with lumbar degenerative diseases. The VAS score was expressed from 0 to 10 points, with no pain as 0 and unbearable pain as 10. The score was positively correlated with the patient’s pain level. The evaluation time was before surgery, 3 days after surgery, and 3 months after surgery.
- Quality of life: The SF-36 score is used to evaluate the quality of life of patients with lumbar degenerative lesions. This research team selected five items closely related to the quality of life of patients, namely, emotion, physical, social, role, and cognitive function, for evaluation. Each dimension is assigned a score of 0–100, and the score is positively correlated with the quality of life of the patient. The evaluation time is before optimization and 3 months after optimization.
- Ability to take care of oneself: The Barthel score was used to evaluate the ability of patients with lumbar degenerative lesions to take care of themselves, ranging from 0 to 100 points. The score was positively correlated with the patient’s ability to take care of themselves. The evaluation time was before optimization and 3 months after optimization.
- Functional impairment: ODI consists of 10 items, including walking, standing, sitting, lifting, traveling, sexual life, social life, self-care, pain intensity, and sleep disturbance. Each item is assigned a score of 0–5 points, and the total score is 0–50 points. The scoring method is: actual score/50 (maximum possible score) × 100%. The higher the score, the more obvious the patient’s impairment. The evaluation time is before optimization and 3 months after optimization.
- Complications: Compare and count the complications between the two groups of patients.
- Patient global satisfaction: Patient global satisfaction with the perioperative care experience was assessed at the 3-month postoperative follow-up using a Numerical Rating Scale (NRS) ranging from 0 (“very dissatisfied”) to 10 (“very satisfied”). Higher scores indicate greater satisfaction.
Sample Size
As a retrospective study spanning a defined period (June 2022 to December 2024), the sample size was determined by the total number of eligible patients who underwent UBE surgery during this timeframe and met the inclusion criteria, rather than by a prospective power calculation. This approach allowed for the inclusion of all available cases, maximizing the statistical power for this single-center experience. A post-hoc power analysis was performed using G*Power software (version 3.1.9.7) for the primary outcome of the Oswestry Disability Index (ODI) at 3 months. With a sample size of 49 in the conventional group and 56 in the intervention group, an effect size (Cohen’s d) of 1.42, and an alpha level of 0.05, the achieved statistical power was calculated to be >0.99, indicating a sufficiently large sample to detect the observed clinically significant difference between groups.
Statistical Analysis
Statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The normality of distribution for continuous variables was assessed using the Shapiro–Wilk test, and homogeneity of variances was evaluated with Levene’s test. Continuous variables are presented as mean ± standard deviation. Between-group comparisons of continuous variables at single time points were performed using independent samples t-tests (for parametric data) or Mann–Whitney U-tests (for non-parametric data). Effect sizes for continuous variables were calculated using Cohen’s d, and 95% confidence intervals (CIs) for mean differences are reported. Categorical variables are presented as numbers (percentages) and were compared using Pearson’s chi-square tests or Fisher’s exact test, as appropriate. Effect sizes for categorical variables were calculated using the Phi coefficient or Cramer’s V, and 95% CIs for risk differences are reported. The primary outcomes of this study were the between-group differences in pain intensity (VAS), functional disability (ODI), and self-care ability (Barthel Index) at the 3-month follow-up. A Bonferroni correction for multiple comparisons was applied to these primary outcomes, setting the significance threshold at P < 0.017 (0.05/3) for this family of tests. Comparisons of complication rates and secondary outcomes (eg, emotional state, quality of life dimensions) were considered exploratory, and findings are interpreted with caution regarding the potential for Type I error inflation. To account for potential confounding effects, an analysis of covariance (ANCOVA) was conducted for the primary continuous outcomes (3-month VAS, ODI, and Barthel scores), adjusting for their respective baseline scores and key demographic variables (age, BMI). The evaluation timepoints for different outcomes were selected based on their clinical relevance: emotional state (SAS/SDS) was assessed preoperatively and at 3 days postoperatively to capture perioperative changes; pain (VAS) was assessed preoperatively, at 3 days, and 3 months to evaluate immediate and short-term recovery; while functional outcomes (ODI, Barthel, SF-36) were assessed preoperatively and at 3 months to reflect meaningful medium-term recovery. All tests were two-sided.
Results
Baseline Data
Table 1 shows the baseline data of the two groups of participants. The baseline characteristics, including age, gender, BMI, course of disease, surgical segment, and disease type, were compared between groups to assess homogeneity. Continuous variables (age, BMI, disease duration) were analyzed using independent samples t-tests, and categorical variables (gender, surgical segment, disease type) were analyzed using Pearson’s chi-square test or Fisher’s exact test as appropriate. The analyses revealed no statistically significant differences between the groups (all P > 0.05), indicating that the groups were comparable at baseline.
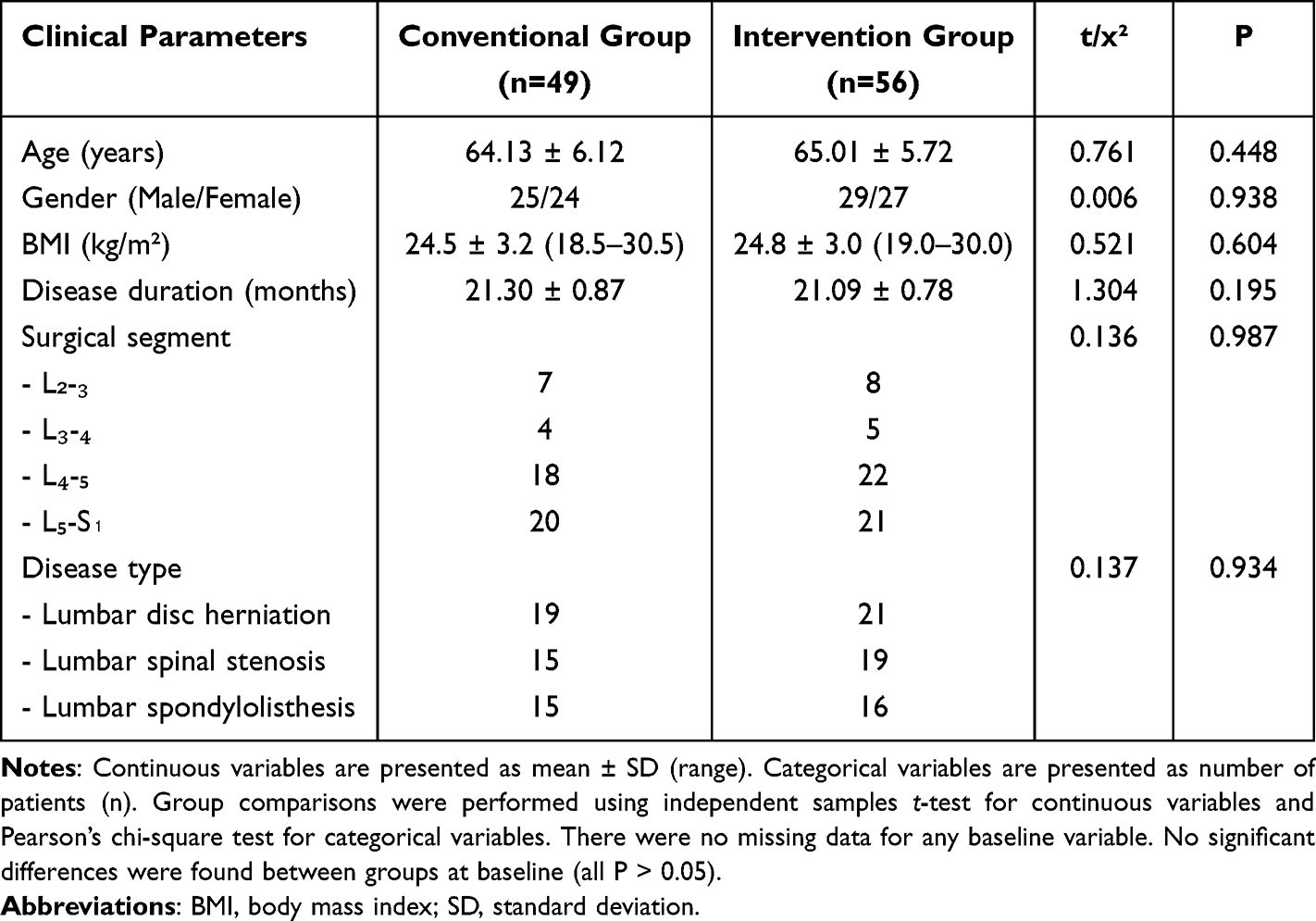 |
Table 1 Analysis of Baseline Data of the Two Groups |
Emotional State
According to the data in Table 2, the emotional state of both the intervention group and the conventional group improved after optimization. Specifically, the SAS and SDS scores of both the intervention group and the conventional group decreased after optimization, and the difference was significant compared with before optimization (P < 0.05). In addition, the SAS and SDS scores of the intervention group were significantly lower than those of the conventional group after optimization (P < 0.001), with large effect sizes (Cohen’s d for SAS: 4.24, 95% CI: 3.45 to 5.03; for SDS: 2.18, 95% CI: 1.65 to 2.71).
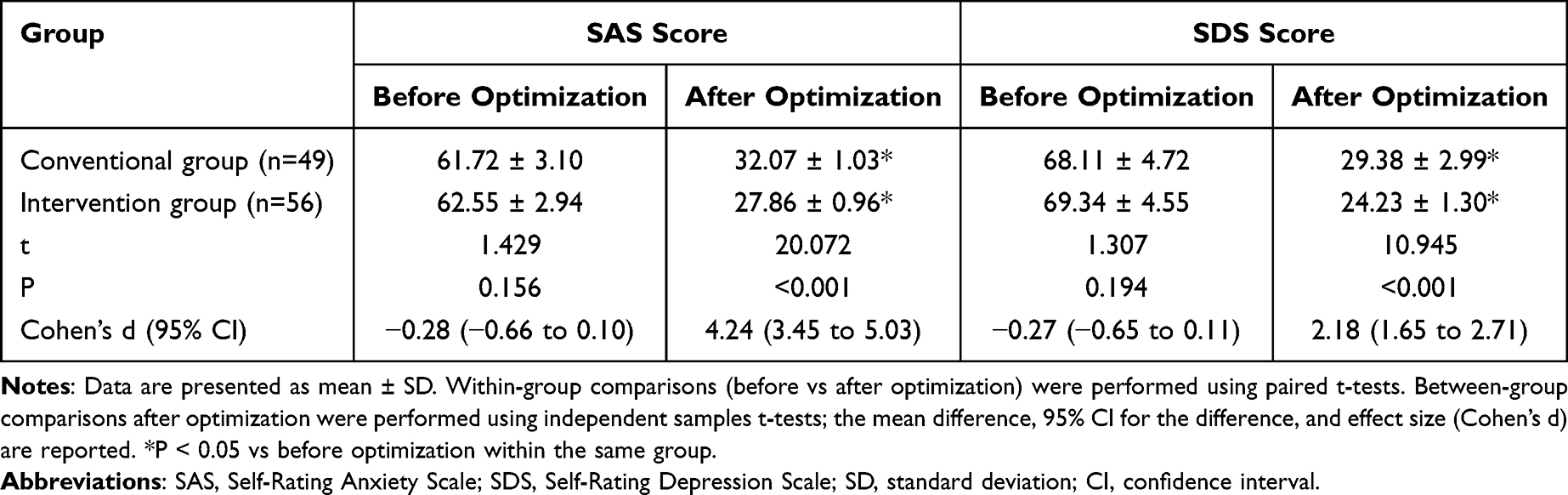 |
Table 2 Analysis of Emotional States of the Two Groups (Mean ± SD) |
Waist/Leg Pain
According to the data in Table 3, the waist and leg pain in both the intervention group and the conventional group were relieved after surgery. Specifically, the VAS scores of waist/leg pain in both the intervention group and the conventional group showed a downward trend after surgery, and the difference was significant compared with that before surgery (P < 0.05). In addition, the VAS scores of waist/leg pain in the intervention group were significantly lower than those in the conventional group at postoperative 3 days and 3 months (P < 0.001), with moderate to large effect sizes (for waist VAS at 3 days: d=0.93, 95% CI: 0.52 to 1.34; at 3 months: d=2.67, 95% CI: 2.00 to 3.34; for leg VAS at 3 days: d=1.65, 95% CI: 1.18 to 2.12; at 3 months: d=1.92, 95% CI: 1.41 to 2.43).
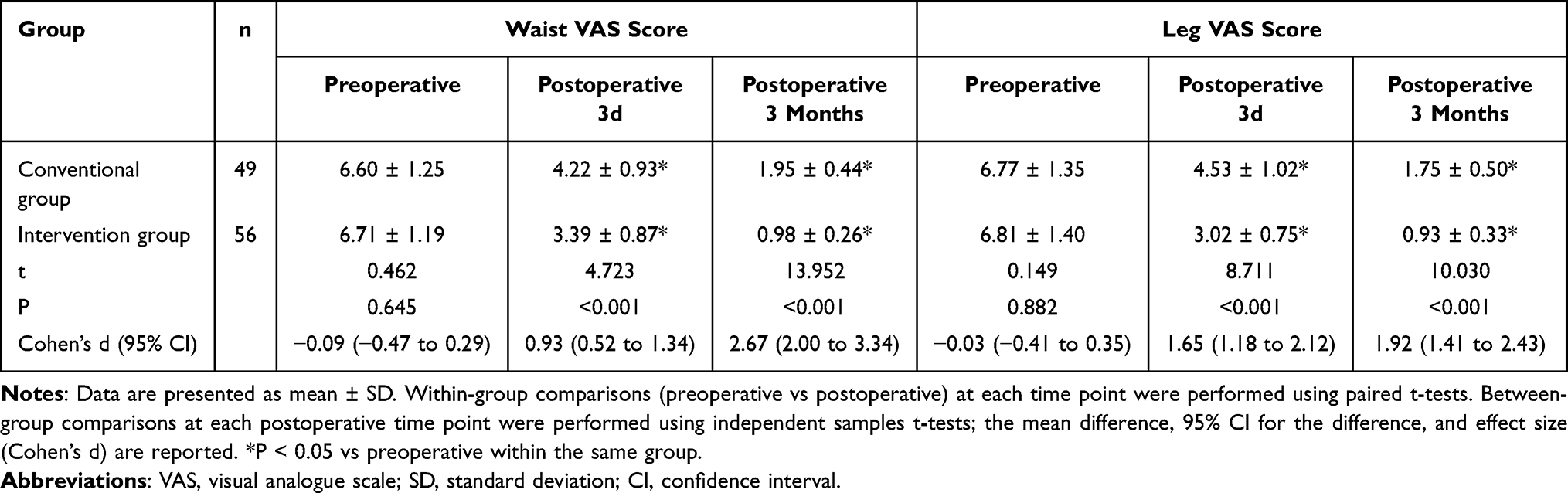 |
Table 3 Analysis of Waist/Leg Pain in the Two Groups (Mean ± SD) |
Quality of Life
According to the data in Table 4, the quality of life of both the intervention group and the conventional group was significantly improved after optimization. Specifically, the scores of the emotional, physical, social, role and cognitive function dimensions of the intervention group and the conventional group increased after optimization, and the difference was significant compared with before optimization (P < 0.05). In addition, the scores of each dimension of SF-36 in the intervention group increased significantly after optimization compared with the conventional group (P < 0.05), with moderate to large effect sizes (emotional: d=0.95, 95% CI: 0.54 to 1.36; physical: d=0.78, 95% CI: 0.38 to 1.18; social: d=0.75, 95% CI: 0.35 to 1.15; role: d=0.98, 95% CI: 0.57 to 1.39; cognitive: d=1.08, 95% CI: 0.66 to 1.50).
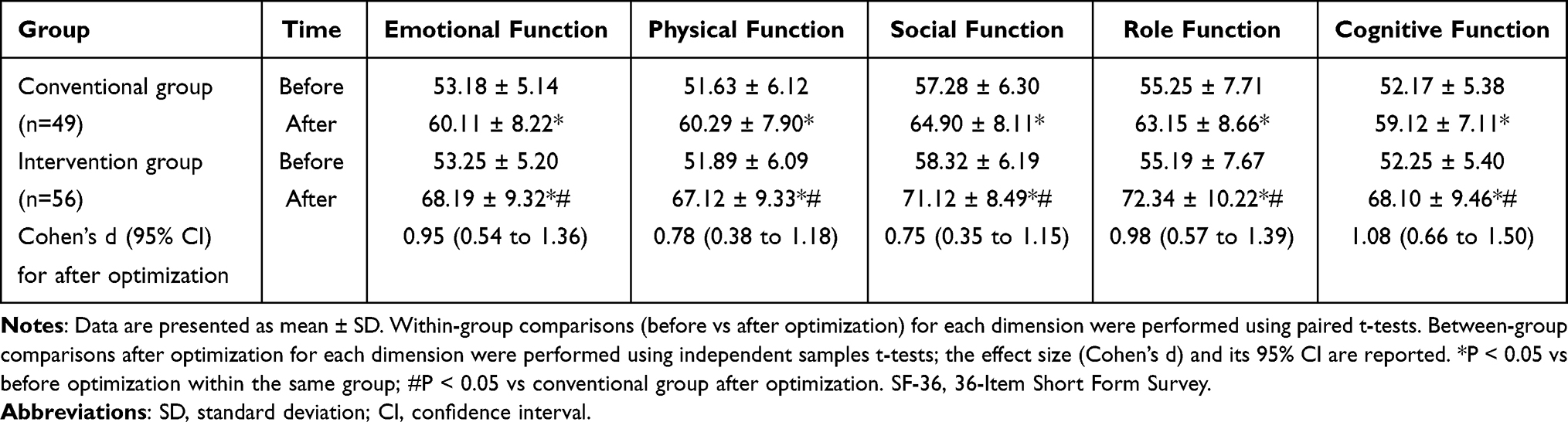 |
Table 4 Analysis of Quality of Life Between the Two Groups (Mean ± SD) |
Self-Care Ability and Functional Impairment
As shown in Table 5, the self-care ability and functional impairment of the intervention group and the conventional group were significantly improved after optimization. Specifically, after optimization, the Barthel scores of the intervention group and the conventional group increased, and the ODI decreased, which was significantly different from before optimization (P < 0.05). In addition, the Barthel score of the intervention group increased significantly compared with the conventional group, and the ODI decreased significantly compared with the conventional group (P < 0.001), with large effect sizes (for Barthel: d=1.68, 95% CI: 1.20 to 2.16; for ODI: d=1.42, 95% CI: 1.00 to 1.84).
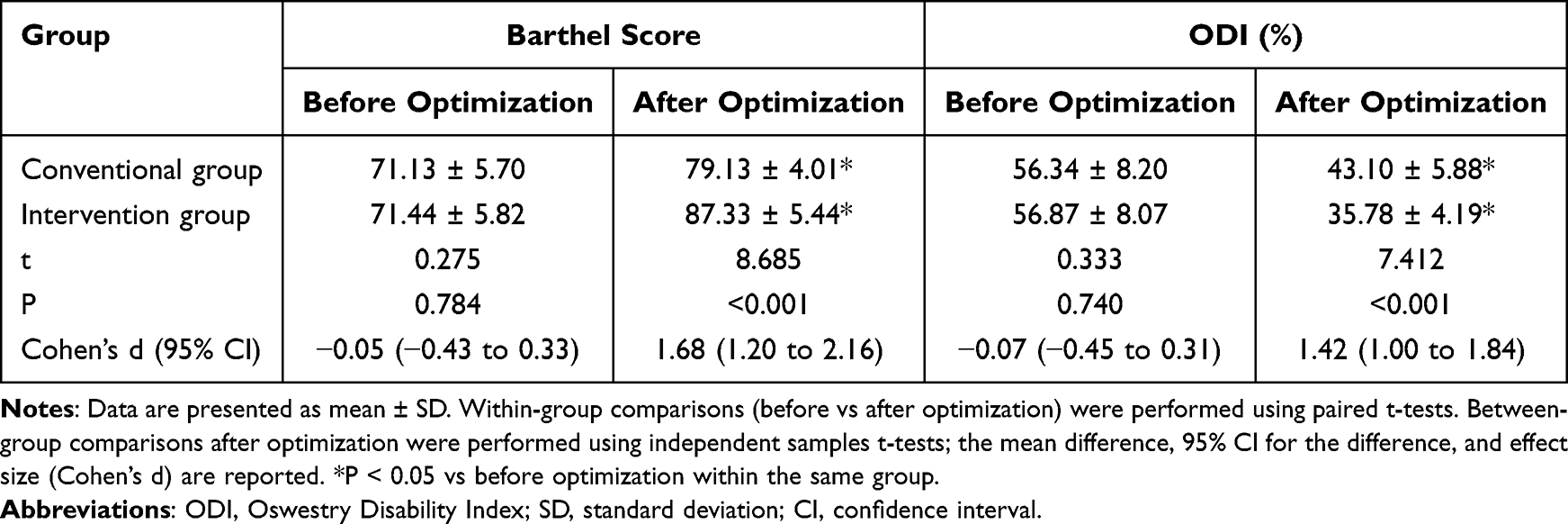 |
Table 5 Analysis of Self-Care Ability and Functional Disability Index Between the Two Groups (Mean ± SD) |
Analysis Adjusting for Potential Confounders
To strengthen the robustness of our findings and account for potential confounding effects, an analysis of covariance (ANCOVA) was performed on the primary continuous outcomes at the 3-month follow-up. The models were adjusted for baseline scores of the respective outcome, age, and BMI. The results of the ANCOVA, presented in Table 6, confirmed that the significant between-group differences in pain intensity (VAS), functional disability (ODI), and self-care ability (Barthel Index) remained statistically significant after adjusting for these covariates (all P < 0.001). The adjusted mean differences between the intervention and conventional groups were consistent with the unadjusted comparisons, indicating that the superior outcomes associated with the optimized nursing protocol were independent of the influence of baseline scores, age, and BMI.
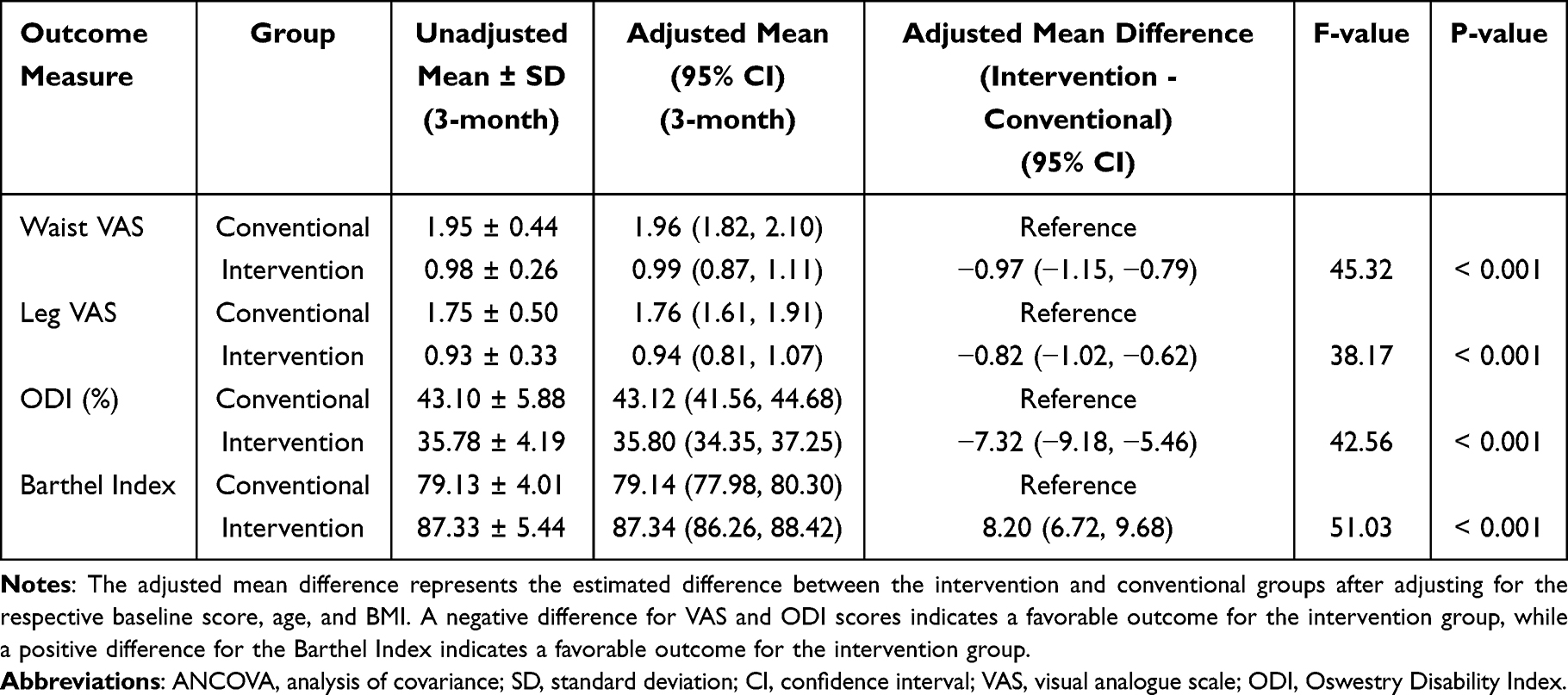 |
Table 6 Analysis of Covariance (ANCOVA) for Primary Outcomes at 3 months, Adjusted for Baseline Scores, Age, and BMI |
Complications
According to the data in Table 7 and Figure 1, the intervention group had secondary infection and bedsore-related postoperative complications, totaling 4 cases, with a total incidence of 7.14%. The conventional group had secondary infection, bedsore, delayed healing, and lower extremity venous thrombosis-related postoperative complications, totaling 10 cases, with a total incidence of 20.41%. The two groups were significantly different (P = 0.046). The risk difference was 13.27% (95% CI: 0.5% to 26.0%), with a small effect size (Phi = 0.195, 95% CI: 0.010 to 0.380).
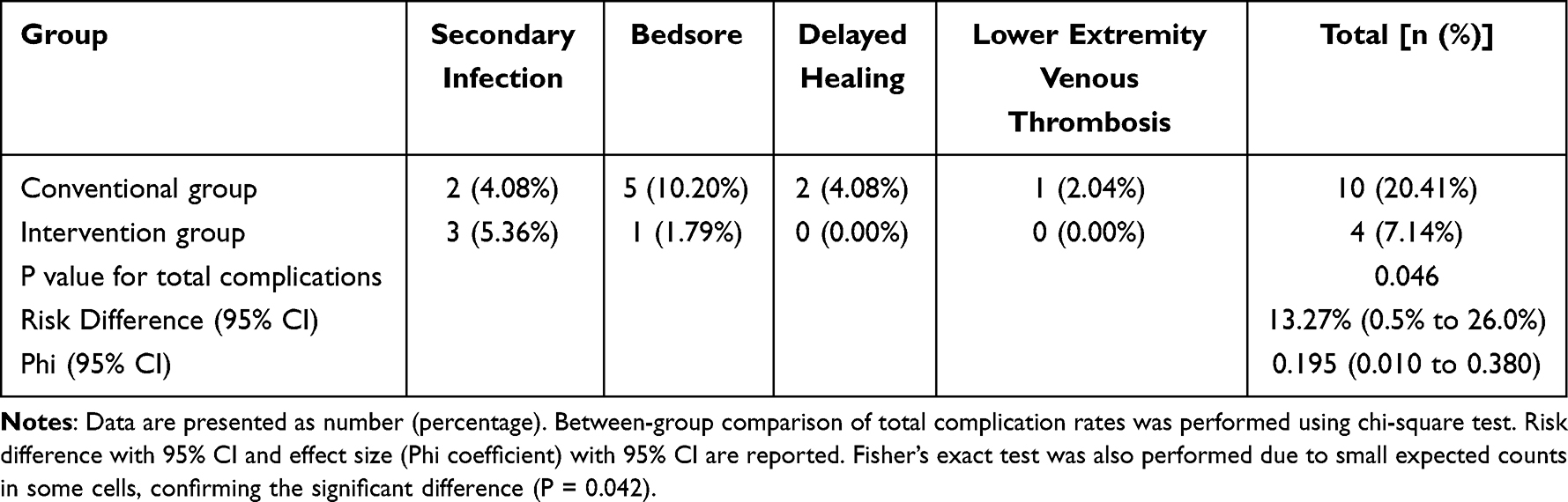 |
Table 7 Comparison of Complications Between the Two Groups [n (%)] |
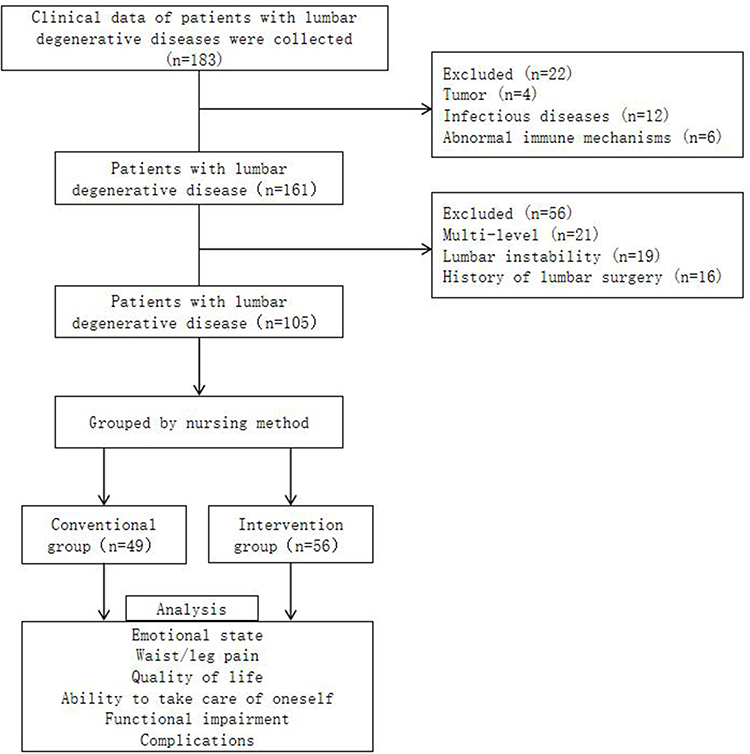 |
Figure 1 Case screening flow chart. |
Patient Global Satisfaction
The global satisfaction with the perioperative care experience was significantly higher in the intervention group compared to the conventional group at the 3-month follow-up (9.02 ± 0.76 vs 7.88 ± 1.05; mean difference: 1.14, 95% CI: 0.80 to 1.48; P < 0.001, Cohen’s d = 1.24) (Table 8). The results indicate a large effect size, suggesting that the optimized nursing protocol was associated with a substantially better patient-reported care experience.
 |
Table 8 Comparison of Patient Global Satisfaction Between the Two Groups (Mean ± SD) |
Discussion
Symptoms such as low back pain and walking dysfunction caused by lumbar degenerative diseases seriously affect the quality of life of patients. Surgical treatment mainly aims to relieve the structure that compresses the nerves, relieve clinical symptoms and improve function.31 In recent years, spinal endoscopy technology has flourished, and UBE has begun to gradually treat a variety of lumbar degenerative diseases such as lumbar spondylolisthesis, lumbar disc herniation, and lumbar spinal stenosis. However, postoperative rehabilitation depends on effective functional exercise.32 For patients with lumbar degenerative diseases undergoing surgical treatment, perioperative care is very important.
The implementation of routine perioperative care for patients with lumbar disc herniation, long-term bed rest and fasting will lead to a long recovery time and miss the best time for functional exercise, thus affecting the patient’s limb function recovery and postoperative recovery. In addition, long-term bed rest can easily lead to complications (pressure sores, venous thrombosis, etc)., affecting the patient’s prognosis.33 The optimized perioperative nursing strategy, grounded in a patient-centered and holistic framework, derives its effectiveness from the synergistic interplay of three core pillars: psychological intervention, multimodal pain management, and structured early rehabilitation. The core mechanism is not attributable to a single component but to their integrated, positive feedback loop. Firstly, psychological interventions actively mitigate the patient’s physiological and psychological stress response to surgery by down-regulating the neuroendocrine and immune systems, thereby reducing inflammatory mediators.34,35 This creates a favorable physiological state, enhancing the efficacy of multimodal pain management protocols. Secondly, effective pain control, achieved by minimizing opioid use and its side effects, serves as the essential prerequisite for early mobilization, breaking the cycle of pain-induced immobility.36 Finally, successful early rehabilitation prevents complications and provides powerful psychological reinforcement, boosting the patient’s sense of control and recovery confidence, which further improves their psychological state and adherence to the care plan.35,37 It is this tightly coupled, synergistic action—where psychological stability facilitates physical recovery, and physical progress reinforces psychological well-being—that explains the comprehensive improvements observed, transforming the care model from a series of isolated tasks into a dynamic, integrated recovery system.37,38 This study found that the VAS score of waist/leg pain in the intervention group was significantly lower than that in the conventional group after surgery (P < 0.05). The results of this study indicate that the optimization of perioperative nursing applied to patients undergoing UBE surgery can effectively reduce postoperative pain symptoms. In the management of patient pain, the early application of multi-step and multi-angle analgesia schemes and the use of combined preoperative and postoperative analgesia can further reduce the pain level of postoperative patients.39
This study found that the intervention group’s emotional state, quality of life, self-care ability, and functional impairment were more significantly improved after optimization than those of the conventional group. And the incidence of complications was lower (P < 0.05). This shows that perioperative nursing optimization can significantly reduce the negative emotions of patients undergoing low UBE surgery during the perioperative period, improve the quality of life, enhance the ability to take care of themselves, and promote the functional recovery of patients. The significant reduction in anxiety and depression scores observed in the intervention group may be attributed not only to the direct psychological support but also to the potential improvement in patients’ sleep quality. Our nursing interventions, such as ensuring a quiet and comfortable environment and alleviating preoperative anxiety, are conducive to better sleep. It is well-established that sleep plays a vital role in emotional regulation and recovery.40 Therefore, sleep optimization likely served as an important mediator in alleviating perioperative negative emotions, although this warrants direct measurement in future studies. In addition to guiding patients to undergo a comprehensive examination and make adequate preparations for the body before surgery, nursing staff should also provide health education and psychological intervention for patients, so that patients can be familiar with the relevant knowledge of the disease and surgical treatment, help patients correct previous misconceptions, strengthen their recognition of surgical treatment and nursing work, and improve the patient’s cooperation with treatment and nursing, which can significantly improve the patient’s negative emotions and also have a positive significance for improving treatment and nursing compliance.41,42 At the same time, appropriate analgesia and better anesthesia reduce patients’ discomfort, pain, and stress reactions.43 In addition, postoperative rehabilitation management is traditionally mainly completed by nurses, which can easily lead to blind functional exercise due to random guidance by nurses. Medical staff and nurses jointly implement functional exercise guidance for patients, which can provide timely feedback and adjust the functional exercise plan, thereby improving the effect of functional exercise.44–46 This approach aligns with contemporary spine care paradigms that emphasize promoting dynamic “posture change” and frequent movement over instructing static “posture correction”, which is crucial for effective functional recovery and preventing stiffness.47 Gonella41 et al found that perioperative nursing optimization can shorten the postoperative hospitalization time of colorectal cancer patients and reduce the incidence of complications. Yue43 et al applied perioperative nursing optimization services to patients and found that this nursing model can significantly reduce postoperative pain, reduce the use of opioids, and promote gastrointestinal function recovery. Furthermore, patients who received the optimized care reported significantly higher global satisfaction with their perioperative experience, underscoring the patient-centered value of the protocol beyond purely clinical outcomes.
However, this study has several limitations. First, its retrospective and non-randomized design inherently carries risks of selection bias and unmeasured confounding. Although baseline characteristics were comparable between groups, we cannot exclude the possibility that temporal trends or other unmeasured factors influenced the outcomes. Second, the study was conducted at a single center with a relatively small sample size, which may introduce center-specific biases and limit the generalizability of the findings to a broader population. Third, the follow-up duration was short, preventing a comprehensive evaluation of the long-term effects of the nursing optimization on patient recovery and quality of life. Future multicenter, prospective studies with longer follow-up are needed to validate these findings.
Conclusion
In summary, this study demonstrates that the implementation of an optimized perioperative nursing protocol for patients undergoing UBE surgery for lumbar degenerative diseases is associated with significant improvements in key patient-centered outcomes. Specifically, the optimization led to a notable alleviation of perioperative anxiety and depression, reduced postoperative pain, enhanced quality of life, improved self-care ability, and promoted functional recovery, alongside a lower incidence of complications compared to conventional care. These findings underscore the integral role of structured, patient-centric nursing within the enhanced recovery framework for spinal endoscopic surgery. Future research should aim to validate these findings through a prospective, randomized controlled trial design to robustly address potential selection bias and confounding. Such a study should incorporate a priori power calculation, longer-term follow-up (eg, 12 months) to assess the durability of benefits, and a cost-effectiveness analysis to evaluate the economic impact of the nursing optimization protocol.
Abbreviations
SAS score, self-rating anxiety scale score; ODI, oswestry disability index; SDS score, self-rating depression scale score; SF-36 score, quality of life scale score; VAS score, visual analogue score; UBE, unilateral biportal endoscopy.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of Ninth Medical Center, PLA General Hospital (ethics approval number: 2025-05-15), with a waiver of informed consent granted by the institutional ethics committee. This study is a retrospective analysis of anonymized medical records; it did not involve any direct interaction with human subjects or animal models. All data were obtained from routine clinical practice in accordance with the principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was not funded by any funding.
Disclosure
Miaomiao Cui and Shengzhi Tan are co-first authors for this study. The authors declared that they have no conflicts of interest regarding this work.
References
1. Kgomotso EL, Hellum C, Fagerland MW, et al. Decompression alone or with fusion for degenerative lumbar spondylolisthesis (Nordsten-DS): five year follow-up of a randomised, multicentre, non-inferiority trial. BMJ. 2024;386:e079771. doi:10.1136/bmj-2024-079771
2. Kögl N, Petr O, Löscher W, Liljenqvist U, Thomé C. Lumbar disc herniation—the significance of symptom duration for the indication for surgery. Dtsch Arztebl Int. 2024;121(13):440–448. doi:10.3238/arztebl.m2024.0074
3. Zhu L, Sun Y, Kang J, et al. Effect of acupuncture on neurogenic claudication among patients with degenerative lumbar spinal stenosis: a randomized clinical trial. Ann Intern Med. 2024;177(8):1048–1057. doi:10.7326/M23-2749
4. Chu P, Wu Y, Liu Y, Wu X, Fan G. Global and current research trends of unilateral biportal endoscopy/biportal endoscopic spinal surgery: a bibliometric analysis. World Neurosurg. 2022;162:e497–e508.
5. Grand View Research. Unilateral biportal endoscopy market size, share & trends analysis report by product (UBE systems, UBE kits), by region (North America, Europe, Asia Pacific, Latin America, MEA), and segment forecasts, 2025–2030. 2024.
6. Li K, Liu S, Tang R, Zhang Y, Liu J, Guo M. A systematic review and meta-analysis of full-endoscopic versus biportal-endoscopic transforaminal lumbar interbody fusion for lumbar spinal stenosis. Front Surg. 2025;12.
7. Ding Y, Chen J, Ma J, Gao K, Zhang Y, Zhao C. Comparison of efficacy and safety between unilateral biportal endoscopic transforaminal lumbar interbody fusion and minimally invasive transforaminal lumbar interbody fusion for lumbar degenerative diseases: a meta-analysis of comparative studies. BMC Musculoskelet Disord. 2024;25(1):324. doi:10.1186/s12891-024-08146-x
8. Stephens ME, CM O, Westrup AM, et al. Utility of machine learning algorithms in degenerative cervical and lumbar spine disease: a systematic review. Neurosurg Rev. 2022;45(2):965–978. doi:10.1007/s10143-021-01624-z
9. Dhahbi W, Padulo J, Bešlija T, Cheze L. Dynamic posture change in non-specific low back pain management: a paradigm shift utilizing the joint-by-joint training approach. New as J Med. 2024;2(3):17–23.
10. Bogaert L, Thys T, Depreitere B, et al. Rehabilitation to improve outcomes of lumbar fusion surgery: a systematic review with meta-analysis. Eur Spine J. 2022;31(6):1525–1545. doi:10.1007/s00586-022-07158-2
11. Wen DJ, Tavakoli J, Tipper JL. Lumbar total disc replacements for degenerative disc disease: a systematic review of outcomes with a minimum of 5 years follow-up. Global Spine J. 2024;14(6):1827–1837. doi:10.1177/21925682241228756
12. Van Isseldyk F, Padilla-Lichtenberger F, Guiroy A, et al. Endoscopic treatment of lumbar degenerative disc disease: a narrative review of full-endoscopic and unilateral biportal endoscopic spine surgery. World Neurosurg. 2024;188:e93–e107. doi:10.1016/j.wneu.2024.05.047
13. Bonus CG, Hatcher D, Northall T, Montayre J. Enhancing culturally responsive care in perioperative settings for older adult patients: a qualitative interview study. Int J Nurs Stud. 2025;161:104925. doi:10.1016/j.ijnurstu.2024.104925
14. Rezaee ME, Mahon KM, Trock BJ, et al. ERAS for ambulatory TURBT: enhancing bladder cancer care (EMBRACE) randomised controlled trial protocol. BMJ Open. 2024;14(6):e076763. doi:10.1136/bmjopen-2023-076763
15. Yang Q, Wang L, Zhang X, et al. Impact of an enhanced recovery after surgery program integrating cardiopulmonary rehabilitation on post-operative prognosis of patients treated with CABG: protocol of the ERAS-CaRe randomized controlled trial. BMC Pulm Med. 2024;24(1):512. doi:10.1186/s12890-024-03286-1
16. Ma L, Yu Y, Zhao BJ, Yu YN, Li Y. Effect of information-motivation-behavioral skills model based perioperative nursing on pain in patients with gallstones. World J Gastrointest Surg. 2024;16(7):2232–2241. doi:10.4240/wjgs.v16.i7.2232
17. Yu Z, Jia W, Sun X, Zhang S, Tan J, Feng L. Effect of Roy’s adaptation, model-based, perioperative nursing service on patients: a clinical observational study. Altern Ther Health Med. 2023;29(1):118–123.
18. Jagoda AS, Cantrill SV, Wears RL, et al. Clinical features of head injury patients presenting with a Glasgow Coma Scale score of 15 and who require neurosurgical intervention. Ann Emerg Med. 2006;48(2):220–225.
19. Parker SL, Mendenhall SK, Shau DN, et al. Utility of minimum clinically important difference in assessing pain, disability, and health state after transforaminal lumbar interbody fusion for degenerative lumbar spine disease. J Neurosurg Spine. 2011;14(5):598–604. doi:10.3171/2010.12.SPINE10472
20. Shebib R, Bailey JF, Inman M, et al. Randomized controlled trial of a 12-week digital care program in improving low back pain. Npj Digit Med. 2019;2:1. doi:10.1038/s41746-018-0076-7
21. Sessler DI, Kurz A. Guideline on patient warming. 3M Health Care. 2018.
22. New jersey department of health. SCIP-Inf-10: surgery patients perioperative temperature management. 2013.
23. Spruce L. Maintaining normothermia: implementing AORN’s updated patient temperature management guideline. AORN J. 2019;110(5):478–485.
24. Kim KT, Lee S, Kim YB, Kwak YH, Kim HJ. Effect of warmed irrigation fluid on core body temperature during percutaneous endoscopic lumbar discectomy: a randomized controlled trial. J Orthop Surg Res. 2022;17(1):324. doi:10.1186/s13018-022-03217-y
25. Jin Y, Yang J. Warming of irrigation fluids for prevention of perioperative hypothermia during arthroscopy: a systematic review and meta-analysis. J Arthrosc Relat Surg. 2018;34(2):643–650.
26. Chinese medical association anesthesiology branch. expert consensus on perioperative management of spine surgery in China (2023 Edition). 2023.
27. Agency for Healthcare Research and Quality (AHRQ). Toolkit for Reducing CAUTI in Hospitals; 2018.
28. National health commission of the People’s Republic of China. Clinical pathway for accelerated recovery of total knee arthroplasty. 2023.
29. Tee TS, Saiman MK, Saiman D, Soe HH, Mohsin SS. The use of bladder scanner to reduce urinary catheterization. J Clin Nurs. 2010;19(21–22):3141–3146.
30. Dhahbi W, Materne O, Chamari K. Rethinking knee injury prevention strategies: joint-by-joint training approach paradigm versus traditional focused knee strengthening. Biol Sport. 2025;42(4):59–65. doi:10.5114/biolsport.2025.148544
31. Ruffilli A, Manzetti M, Cargeli A, et al. Unveiling timetable for physical therapy after single-level lumbar surgery for degenerative disc disease: insights from a systematic review and meta-analysis. J Clin Med. 2024;13(9):2553. doi:10.3390/jcm13092553
32. Reis JPG, Pinto EM, Teixeira A, et al. Unilateral biportal endoscopy: review and detailed surgical approach to extraforaminal approach. EFORT Open Rev. 2025;10(3):151–155. doi:10.1530/EOR-24-0137
33. Kannan V, Ullah N, Geddada S, et al. Impact of “enhanced recovery after surgery” (ERAS) protocols vs. traditional perioperative care on patient outcomes after colorectal surgery: a systematic review. Patient Saf Surg. 2025;19(1):4. doi:10.1186/s13037-024-00425-9
34. Sun BF, Chen QP. Mechanism and influence of excessive inflammatory response in perioperative period of abdominal surgery. World Chin J Digestol. 2017;25(2):178–184. doi:10.11569/wcjd.v25.i2.178
35. Fidelis P, Xiong LP, Zhang Y, Zhao TT, Zhang CY, et al. From operating room to recovery: evidence and gaps in cardiac surgical nursing integrative psychological support. Ann Card Anaesth. 2025;28(1):1–10. doi:10.4103/aca.aca_168_24
36. He Y, Li M, Liu Y, et al. Comprehensive review on personalized pain assessment and multimodal interventions for postoperative recovery optimization. J Pain Res. 2025;18:1–20. doi:10.2147/JPR.S481853
37. Walsh CA, Cleary S, Stelmach W, Zheng Z, et al. Patient engagement in perioperative settings: a mixed method systematic review. J Clin Nurs. 2023;32(11–12):2356–2374.
38. Santa-Maria CA,Claydon-Mueller LS, Weiss O, Zhang J, Rushton A, Khanduja V, et al. Prehabilitation for patients undergoing orthopedic surgery: a systematic review and meta-analysis. JAMA Netw Open. 2023;6(4):e238721.
39. Patel J, Snyder K, Brooks AK. Perioperative pain optimization in the age of the opioid epidemic. Curr Opin Anaesthesiol. 2024;37(3):279–284.
40. Bouzouraa E, Dhahbi W, Ferchichi A, et al. Single-night sleep extension enhances morning physical and cognitive performance across time of day in physically active university students: a randomized crossover study. Life. 2025;15(8):1178. doi:10.3390/life15081178
41. Gonella F, Massucco P, Perotti S, et al. Prehab, ERAS, rehab: a patient care continuum around colo-rectal surgery: prehabilitation combined with ERAS and rehabilitation to reduce morbidity and hospital stay. Eur J Surg Oncol. 2024;50(12):108688. doi:10.1016/j.ejso.2024.108688
42. Bignami E, Leoni B, Domenichetti T, Panizzi M, Diego LA, Bellini V. ERAS and the challenge of the new technologies. Minerva Anestesiol.
43. Yue TM, Sun BJ, Xu N, et al. Improved postoperative pain management outcomes after implementation of enhanced recovery after surgery (ERAS) protocol for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS-HIPEC). Ann Surg Oncol. 2024;31(6):3769–3777. doi:10.1245/s10434-024-15120-3
44. Mangone L, Mereu F, Zizzo M, et al. Outcomes before and after implementation of the ERAS (enhanced recovery after surgery) protocol in open and laparoscopic colorectal surgery: a comparative real-world study from northern Italy. Curr Oncol. 2024;31(6):2907–2917. doi:10.3390/curroncol31060222
45. Salenger R, Ad N, Grant MC, et al. Maximizing minimally invasive cardiac surgery with enhanced recovery (ERAS). Innovations. 2024;19(4):371–379. doi:10.1177/15569845241264565
46. Tidadini F, Trilling B, Sage PY, et al. Five-year oncological outcomes after enhanced recovery after surgery (ERAS) compared to conventional care for colorectal cancer: a retrospective cohort of 981 patients. Tech Coloproctol. 2024;29(1):9. doi:10.1007/s10151-024-03036-9
47. Dhahbi W, Ben Saad H. Revolutionizing “text neck syndrome” management: paradigm shifting from “posture correction” to “posture change”. Acta Kinesiologica. 2024;18(3):37–40. doi:10.51371/issn.1840-2976.2024.18.3.06
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.