Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Comparative Effectiveness of Non-Pharmacological Interventions for Postpartum Depression and Anxiety: A Network Meta-Analysis
Authors Zhu Y ![]() , Yang W, Li N
, Yang W, Li N ![]() , Yang J, Yang J, Zheng Y, Chen W, Yang Y, Liu Y
, Yang J, Yang J, Zheng Y, Chen W, Yang Y, Liu Y ![]() , Zhao Y
, Zhao Y
Received 1 July 2025
Accepted for publication 18 November 2025
Published 16 December 2025 Volume 2025:21 Pages 2817—2834
DOI https://doi.org/10.2147/NDT.S549504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Yuqin Zhu,1,* Weicheng Yang,1,* Na Li,2 Jinfeng Yang,1 Jinqi Yang,1 Yan Zheng,1 Wen Chen,1 Yunchang Yang,1 Yunlu Liu,1 Yan Zhao1
1Sports Medicine Key Laboratory of Sichuan Province, School of Sports Medicine and Health, Chengdu Sport University, Chengdu, Sichuan, People’s Republic of China; 2The National Clinical Research Center for Geriatrics, West China Hospital of Sichuan University, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunlu Liu, Sports Medicine Key Laboratory of Sichuan Province, School of Sports Medicine and Health, Chengdu Sport University, Chengdu, Sichuan, People’s Republic of China, Email [email protected] Yan Zhao, Sports Medicine Key Laboratory of Sichuan Province, School of Sports Medicine and Health, Chengdu Sport University, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Background: Postpartum depression (PPD), a prevalent perinatal mood disorder characterized by persistent depressive and anxiety symptoms, significantly impacts maternal-infant health. The COVID-19 pandemic has further increased the global burden of PPD, emphasizing the need for effective and accessible interventions. Although non-pharmacological interventions are widely used, their comparative efficacy remains uncertain.
Methods: We searched the Cochrane Library, Web of Science, EMBASE, PubMed, Scopus, CNKI, VIP Database, and Wanfang Database (inception to September 1, 2024) for randomized controlled trials (RCTs). Interventions included acupuncture (ACU), exercise (EXE), psychotherapy (PSY), exercise combined with psychotherapy (ECP), and music therapy (MT). Primary (depression) and secondary (anxiety) outcomes were pooled using mean differences (MD) with 95% credible intervals (CrI). Risk of bias was assessed via Cochrane RoB2. (PROSPERO: CRD42020166801).
Results: Thirty-five RCTs were included (n=4047). Meta-analyses for depressive symptoms (5 interventions, n=4047) showed a statistically significant improvement in the non-pharmacological intervention group compared with the control group (standard care, no intervention, or placebo et al), particularly for the ECP (95% CrI − 2.3 to − 0.85), followed by ACU (95% CrI − 1.8 to − 0.44) and EXE (95% CrI − 1.7 to − 0.48). Similarly, for anxiety symptoms (5 interventions, n=863), the overall effect of the non-pharmacological interventions was superior to that of the control group, with ECP again being the most effective modality (95% CrI − 2.3 to − 0.18), followed by EXE (95% CrI − 2.0 to − 0.0021) and ACU (95% CrI − 0.96 to − 0.052).
Conclusion: This study demonstrates the promise of non-pharmacological interventions, particularly exercise, acupuncture, and ECP, for alleviating PPD symptoms, positioning ECP as a potential first-line intervention for mild to moderate cases.
Keywords: postpartum depression, anxiety, network meta-analysis, non-pharmacological intervention
Introduction
Postpartum depression (PPD) represents one of the most prevalent complications during the perinatal period.1 Current research suggests multifactorial origins contributing to the pathophysiology of PPD, involving inflammatory mechanisms, neuroendocrine alteration, potential neurodegenerative processes, as well as a complex interplay between genetic susceptibility factors and environmental determinants.2 Accumulating studies have established that PPD contributes to severe outcomes, including anhedonia, persistent insomnia, impaired maternal-infant bonding, and thoughts of infant harm or maternal suicidality.3,4 These clinical manifestations not only compromise maternal health but also exert profound detrimental effects on offspring development, particularly affecting emotional regulation, social competence, and cognitive acquisition.5 A large-scale meta-analysis encompassing 296284 participants from 56 countries quantified the global pooled prevalence of PPD at 17.7%, with subgroup analyses revealing geographical disparities - notably, low- and middle-income countries demonstrate elevated prevalence rates ranging from 19% to 25%.6 Moreover, some studies analyzing the prevalence of postnatal depression during the COVID-19 pandemic have reported nearly a two-fold higher incidence compared with the pre-pandemic period, underscoring the exacerbating impact of global crises on maternal mental health.2 These epidemiological patterns indicate that PPD represents a significant global public health concern.
Given the persistently elevated prevalence of PPD and its biopsychosocial impact on maternal-child relationships, untreated cases could impose substantial emotional and physical burdens on families and society.7 Consequently, the timely implementation of evidence-based intervention strategies during perinatal windows emerges as both a clinical imperative and public health necessity. Currently, the pharmacotherapeutic approaches for PPD employ a neurochemical strategy, comprising serotonergic modulators including selective serotonin reuptake inhibitors (SSRIs; eg, sertraline, paroxetine), serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants targeting broader monoaminergic systems, and novel neurosteroid-based therapeutics exemplified by brexanolone.8–10 While SSRIs demonstrate favorable maternal tolerability, their trans- mammary passage necessitates rigorous risk-benefit analysis concerning potential neonatal neurobehavioral complications.11 Brexanolone, despite its efficacy in rapid remission, presents implementation challenges, such as a 60-hour intravenous infusion, high costs, and dose-dependent adverse effects necessitate intensive monitoring.12 Consequently, pharmacotherapy adherence barriers persist, with patients declining treatment due to teratogenicity misconceptions, lactation safety, and so on.13 In addition, PPD frequently coexists with bipolar affective disorder and exhibits overlapping symptoms, complicating the diagnostic process. This challenge may lead to inappropriate pharmacological intervention strategies; selecting the wrong medication could exacerbate depressive symptoms and elevate maternal suicide risk.14
In recent years, non-pharmacological interventions for PPD have gained significant traction among patients, with therapies such as psychotherapy, pram walking, yoga, music therapy and acupuncture being increasingly adopted either as mono- or complementary interventions. Non-pharmacological approaches offer several benefits: they generally have fewer side effects, making them especially suitable for breastfeeding mothers;15 psychotherapy aids in improving negative emotions and fosters sustained psychological resilience;16 physical activities like yoga and walking enhance endorphin release and cardiovascular health, which synergistically improves emotional regulation;17,18 and acupuncture demonstrates neurobiological benefits through neuroplasticity modulation and anti-inflammatory mechanisms that may ameliorate depressive symptoms.19 Importantly, these interventions can be customized to meet the unique needs of each patient while reducing reliance on psychotropic medications, thereby mitigating risk of adverse pharmacological effects on both mothers and infants.20 Thus, non-pharmacological interventions present a safe and effective alternative for PPD patients.
Although numerous systematic reviews have supported the efficacy of non-pharmacological interventions for PPD, existing meta-analyses remain limited by small sample sizes, methodological heterogeneity, and insufficient exploration of heterogeneity sources.21–23 Exercise intervention studies frequently encounter difficulties in blinding participants due to postpartum physiological characteristics, introducing potential bias,20 whereas acupuncture trials frequently suffer from small sample sizes and insufficient subgroup analyses to differentiate intervention protocols (eg, acupoint combinations or intervention frequency).24 Traditional pairwise meta-analyses are limited to direct comparisons between two interventions, which constrains the ability to comprehensively evaluate multiple options. In contrast, network meta-analysis (NMA) integrates both direct and indirect evidence to estimate and compare the relative effectiveness of several interventions within a single analytical framework. The Bayesian model is commonly used in NMAs because they offer greater flexibility than frequentist methods, such as incorporating prior information and modeling complex study structures.25 Therefore, this study employs a Bayesian NMA to systematically compare and rank non-pharmacological interventions for PPD with respect to depressive and anxiety symptoms, providing comparative evidence to inform clinical decision-making and support personalised treatment strategies.
Materials and Methods
Study Registration
This study adhered to the PRISMA extension for Network Meta-Analyses (PRISMA-NMA) checklist, the Cochrane Handbook for Systematic Reviews of Interventions, and relevant NMA methodological guidelines. The NMA has been prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD42020166801.
Eligibility Criteria
Participants
The participants included primiparous or multiparous postpartum women who were diagnosed with PPD based on a systematic clinical interview or a validated depression assessment scale.
Interventions
This study included the following non-pharmacological interventions (Table 1).
 |
Table 1 Types of Non-Pharmacological Intervention |
Comparator
Any of the above-mentioned non-pharmacological interventions or the control group; the control group was defined as receiving any form of control intervention (eg, usual care, waitlist controls, non-intervention controls, and placebo).
Outcomes
The study should assess symptoms of depression or anxiety, and available data should be provided. Additionally, the assessment of primary outcomes should utilize valid and specialized scales, listed as follows: (1) Depression symptoms: Edinburgh Postnatal Depression Scale, Beck Depression Inventory, Hamilton Rating Scale for Depression; Self-Rating Depression Scale. (2) Anxiety symptoms: Self-Rating Anxiety Scale, Beck Anxiety Inventory, State-Trait Anxiety Inventory.
Study Designs
This systematic review exclusively included randomized controlled trials (RCTs) without imposing restrictions on blinding procedures or allocation concealment. Grey study sources (eg, dissertations) were systematically searched to mitigate publication bias. All eligible studies investigating non-pharmacological interventions were published in either English or Chinese, thereby enhancing the methodological rigor and comprehensiveness of the present network meta-analysis.
Exclusion Criteria
In this study, the following studies were excluded (Table 2). Studies were excluded if they met any of the following conditions.
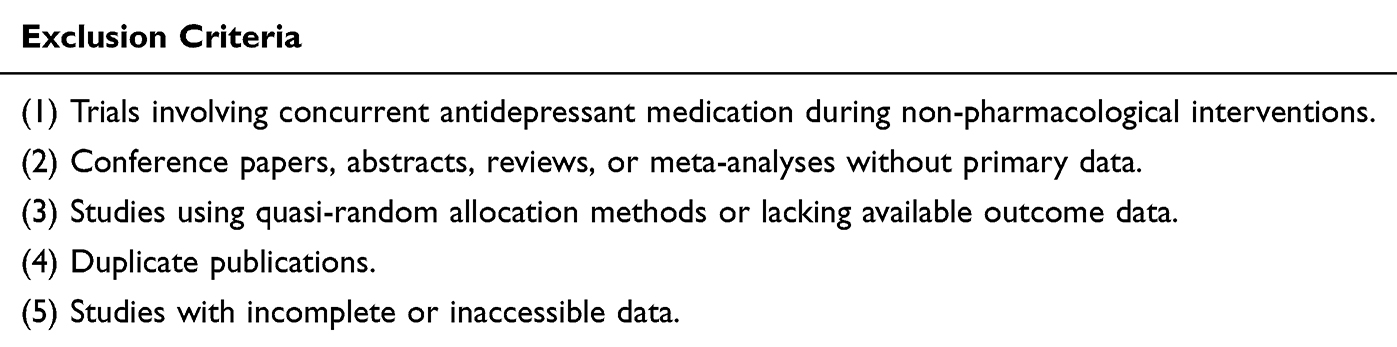 |
Table 2 Exclusion Criteria Used for Study Selection |
Information Sources
This study retrieved The Cochrane Library, Web of Science, EMBASE, PubMed, Scopus, China National Knowledge Infrastructure (CNKI), VIP Database, and Wanfang Database for relevant studies published from database inception to September 1, 2024. Two reviewers independently performed the study search using a predefined search strategy combining free-text terms with medical subject headings.
Search Strategy
This study combined different search terms using Boolean logic (AND [between categories], OR [within categories]). Two independent reviewers systematically executed the study search following predetermined exclusion criteria. To maximize data completeness, the search encompassed both conventionally unavailable studies and non-indexed gray study. The detailed search protocol is presented in Supplementary Table S1.
Selection Process
All retrieved records were imported into EndNote X9 to remove duplicate studies. Two reviewers independently screened all titles and abstracts, strictly adhering to the inclusion and exclusion criteria, and obtained full manuscripts of studies identified as potentially relevant. During the study screening and data extraction process, the two reviewers discussed and resolved any issues. If any problems were not resolved, they were addressed through consensus with a third reviewer. The flowchart of study selection was created according to the PRISMA guidelines.26,27
Data Collection Process
For studies meeting the inclusion criteria, two researchers extracted participants’ characteristics using a data collection form created in Excel. A standardized data extraction form was designed to facilitate comparison and analysis. In cases where a study reported multiple depression or anxiety scores at different time points (eg, mid- intervention, follow-up), only the scores obtained at the assessment point after the intervention phase were used. For studies with missing data, efforts were made to contact the corresponding authors via Email or phone to obtain complete data.
Data Items
The extracted data were as follows: (1) General information: First author’s name, publication year, country, intervention duration, and follow-up information. (2) Baseline data: Number of patients, age, duration of intervention (weeks), frequency of intervention, initial and final scores on the adopted scales, and assessment endpoint for outcome measures. (3) Intervention strategies: Acupuncture; exercise combined with psychotherapy; exercise; psychotherapy; music therapy. (4) Primary and secondary outcome measures: Depression and anxiety.
Study Risk of Bias Assessment
Two independent reviewers independently assessed the risk of bias in randomized trials using the Cochrane risk of bias tool, version 2 (RoB2). After completing their individual evaluations, the reviewers discussed their assessments to resolve any discrepancies. The RoB2 tool examines bias across six distinct domains: (1) Bias arising from the randomization process. (2) Bias due to deviations from intended intervention. (3) Bias due to missing outcome data. (4) Bias in measurement of the outcome. (5) Bias in the selection of the reported result. (6) Bias in overall assessment.28 Each domain was rated as follows: (1) low risk of bias, (2) unclear risk of bias, (3) high risk of bias. Any conflicts in evaluation between the two reviewers were resolved through consultation with a third reviewer.
Effect Measures
As outcomes of depression and anxiety in this meta-analysis were continuous data, standardized mean differences (SMD) was utilized to unify the effect sizes across studies according to the Cochrane Handbook. Specifically, the mean changes and SD from each included study were converted into SMD, allowing for comparisons of results on the same scale.29 Furthermore, as this study included various types of interventions, Bayesian random effects and network meta-regression were employed to assess the transferability of the data.
Synthesis Methods
Pairwise Meta-Analysis
In this study, all RCTs were grouped according to Mesh terms. A pairwise meta-analysis was conducted for depression and anxiety. Statistical analyses were performed in R software (version 4.3.2) within a Bayesian framework, using JAGS software (version 4.3.1) for direct and indirect comparisons. Data analysis was carried out using the GeMTC, metafor, and meta packages in R.30 For the Bayesian estimation, four parallel Markov chains were run with 20,000 burn-in (adaptation) iterations followed by 50,000 sampling iterations per chain. Convergence of the Bayesian models was assessed using the Brooks–Gelman–Rubin diagnostic statistic (potential scale reduction factor, PSRF < 1.05), along with visual inspections of trace and density plots to ensure the stability and reliability of the model estimates.
Summary of the Network
In the network diagram, the size of the points represents the sample size, with larger points indicating a larger sample size. In head-to-head comparisons, the width of the connecting lines is proportional to the number of trials comparing the two interventions. The absence of a connecting line indicates no direct comparative relationship between the trials, allowing for network analysis through indirect comparisons.
Assessment of Consistency in Network
To assess the overall consistency of the network meta-analysis, both consistency and inconsistency models were used for evaluation. The Deviance Information Criterion (DIC) values of the two models were compared, and the model with the lower DIC value was selected. Subsequently, the node-splitting method was employed to determine if there was statistical local inconsistency between direct and indirect comparisons (P-value > 0.05 indicates local consistency). If no inconsistency was found, the consistency model was considered acceptable.31
Assessment of Intervention Effectiveness Ranking
The ranking plots were generated based on the effectiveness of the non-pharmacological interventions in improving depression and anxiety. The P-values for the intervention rankings were calculated using the point estimates and standard errors derived from the network analysis. To assess the probability of each intervention being the most effective, the P-score method was applied. This method estimates the effect sizes of pairwise intervention comparisons, assuming their point estimates are normally distributed. The P-values range from 0 to 1, with higher values indicating a higher ranking of intervention effectiveness, and lower values indicating a lower ranking.32
Assessment of Heterogeneity
Heterogeneity was assessed using Cochran’s Q statistic and I2 values, categorized as follows: 0% indicating no heterogeneity, 25% representing low heterogeneity, 50% indicating moderate heterogeneity, and 75% reflecting high heterogeneity.33 In the presence of significant heterogeneity, a random-effects model was applied for data synthesis; otherwise, a fixed-effects model was used.
Reporting Bias Assessment
To assess the deviation of the findings from the true value, a funnel plot was generated using R (version 4.3.2). A symmetric funnel plot indicated the absence of reporting bias, while an asymmetric plot suggested the presence of reporting bias. The results of the funnel plot were verified by two researchers, with each researcher independently evaluating the potential bias. In the case of any disagreements regarding the trial results, the final decision was made by a third researcher.
Results
Study Selection
This study identified a total of 2804 records across eight databases. After the removal of duplicates, 1903 unique entries remained. Titles and abstracts were screened, and availability of full texts was assessed, resulting in 202 articles selected for further evaluation. Following a thorough full-text review, 35 studies met the inclusion criteria and were included in the final analysis.34–68 The study selection process adhered strictly to the PRISMA guidelines (Figure 1).26,27
 |
Figure 1 Illustrates the process of study identification through databases and registries. The diagram shows the total number of records identified through database searching and other sources, the number of records after duplicates were removed, the number of records screened and excluded, the number of full-text articles assessed for eligibility, and the number of studies included in the final qualitative and quantitative synthesis. |
Study Characteristics
A total of 35 studies, conducted between 1991 and 2024, involving a total of 4047 participants. The detailed characteristics of these studies, including authors, publication year, country, interventions, sample size, mean age, intervention specifics, are summarized in Supplementary Table S2.
These studies were conducted across multiple countries, with 16 studies from China,38–40,45,46,48–58 5 from Australia,34,35,59–61 4 from the United States,36,47,62,63 2 each from Canada and the United Kingdom,41–44 and 1 study each from France, Iran, Turkey, Brazil, South Korea, and Switzerland.37,64–68 Intervention types varied, including acupuncture (6 studies, 17.1%), exercise therapy (6 studies, 17.1%), psychotherapy (15 studies, 42.9%), exercise combined with psychotherapy (5 studies, 14.3%), and music therapy (3 studies, 8.6%). All studies reported depression severity, while 9 studies reported anxiety symptoms. In terms of intervention specifics, the durations typically ranged from 4 to 12 weeks, with a frequency of 1–7 sessions per week. The sample sizes across these studies varied from 10 to 349 participants, with the majority of the participants being adult women aged between 20 and 40 years.
Risk of Bias in Studies
The results of the risk of bias assessment are presented in Figure 2. In the domain of randomization process, 33 studies (94.3%) demonstrated low risk as they employed explicit methodologies such as sealed envelope methods or random number tables for group allocation. Only two studies (5.7%) were rated as high risk due to insufficient descriptions of randomization procedures and allocation concealment.
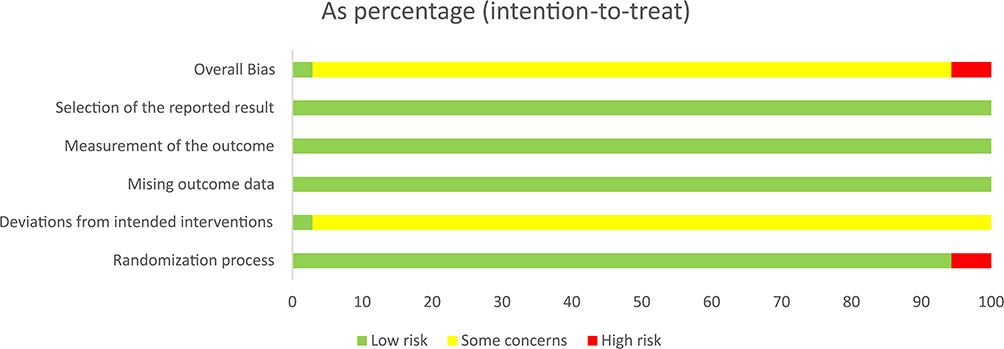 |
Figure 2 Present the risk of bias assessment results for all included studies in this review. Green indicates no significant risk of bias, yellow represents insufficient information to assess the risk of bias or incomplete reporting, and red signifies a clear risk of bias in the included studies. |
Regarding deviations from intended interventions, one study (2.9%) utilizing acupuncture versus sham acupuncture with double-blinding was classified as low risk. Notably, the non-pharmacological nature of the interventions posed challenges in blinding implementation across other studies. The remaining 34 studies (97.1%) were deemed to have potential risks owing to inadequate descriptions of analytical methods for addressing intervention deviations.
For missing outcome data, all studies exhibited complete reporting with no attrition bias (low risk). In the measurement of the outcome domain, standardized methodologies and statistical protocols were consistently reported, resulting in a unanimous low-risk assessment. Selection of reported result bias was rated as low risk as predefined outcomes specified in the study protocols were fully reported.
Quality appraisal revealed that two studies (5.7%) were classified as low quality due to high risk of bias, while the remaining 32 studies (91.4%) were rated as moderate quality.
Network Meta-Analysis Results
Network Geometry
Among the 35 included studies, all were two-arm trials. The network plots (Figure 3A and B), generated using R (Version 4.3.2), summarized the effects of non-pharmacological interventions on depressive and anxiety symptoms in PPD. Six interventions were evaluated: psychotherapy, music therapy, exercise therapy, acupuncture, exercise combined with psychotherapy, and control intervention. In direct comparisons, the thickness of the connecting lines reflected the number of trials comparing the two interventions. The absence of a connecting line indicated no direct comparison between the interventions, allowing for network analysis through indirect comparisons.
 |
Figure 3 (A) A network graph comparing various non-pharmacological interventions for their effects on depressive symptoms in patients with PPD. (B) A network graph comparing various non-pharmacological interventions for their effects on anxiety symptoms in patients with PPD. In panels (A and B), each circle represents an intervention: ACU, EXE, PSY, ECP, MT and CON. The size of each circle is proportional to the number of studies evaluating that intervention. The lines connecting the circles represent direct comparisons between interventions, with the width of the line indicating the number of studies comparing the two interventions. Thicker lines represent a greater number of studies. The figure provides a visual representation of the network of interventions and their comparisons for both depressive and anxiety symptoms. Abbreviations: CON, Control group; ACU, Acupuncture group; ECP, Exercise combined with psychotherapy group; EXE, Exercise therapy group; PSY, Psychotherapy group; MT, Music therapy group. |
Convergence Test
The convergence of the MCMC model for depressive and anxiety symptoms was assessed. The trace plots of all parameters showed good mixing, the density plots exhibited unimodal distributions, and the Gelman-Rubin convergence factors were close to 1 (Figures 4 and 5). These results indicate that the model has adequately converged and the parameter estimates are reliable.
 |
Figure 4 Trace plots and density plots for depressive trajectories and convergence diagnostics. (A and B) Trace plots of the posterior distributions for anxiety symptoms across different interventions, including acupuncture (d.CON.ACU), exercise (d.CON.EXE), music therapy (d.CON.MT), psychotherapy (d.CON.PSY), and exercise combined with psychotherapy (d.PSY.ECP). Trace of sd.d (bottom of (B) represents the trace plot for the standard deviation of the parameters (sd.d), which is used for assessing the variability in the model and ensuring convergence of the model. (C) Convergence diagnostics for the model, showing the trace plots (left) and density plots (right) of the standard deviations (sd.d) and other parameters. The red dashed lines indicate the 97.5% quantile, and the median value is shown by the solid line. Convergence is confirmed when the trace plot stabilizes and the density plot forms a clear distribution. Abbreviations: CON, Control group; ACU, Acupuncture group; ECP, Exercise combined with psychotherapy group; EXE, Exercise therapy group; PSY, Psychotherapy group; MT, Music therapy group. |
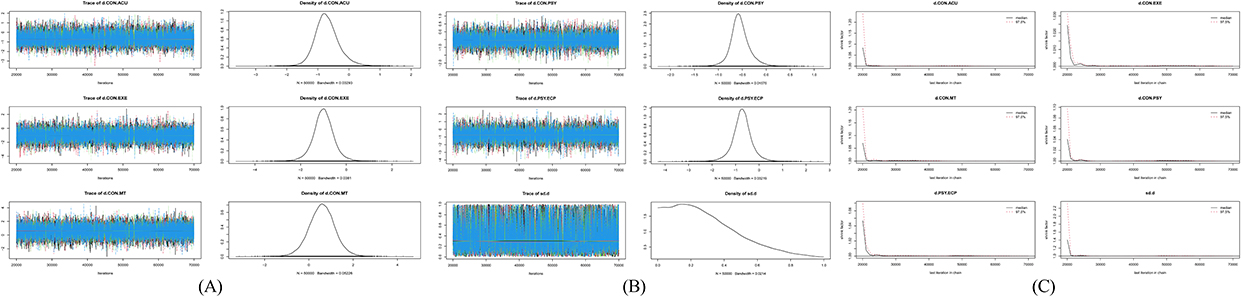 |
Figure 5 Trace plots and density plots for anxiety trajectories and convergence diagnostics. (A and B) Trace plots of the posterior distributions for anxiety symptoms across different interventions, including acupuncture (d.CON.ACU), exercise (d.CON.EXE), music therapy (d.CON.MT), psychotherapy (d.CON.PSY), and exercise combined with psychotherapy (d.PSY.ECP). Trace of sd.d (bottom of (B) represents the trace plot for the standard deviation of the parameters (sd.d), which is used for assessing the variability in the model and ensuring convergence of the model. (C) Convergence diagnostics for the model, showing the trace plots (left) and density plots (right) of the standard deviations (sd.d) and other parameters. The red dashed lines indicate the 97.5% quantile, and the median value is shown by the solid line. Convergence is confirmed when the trace plot stabilizes and the density plot forms a clear distribution. Abbreviations: CON, Control group; ACU, Acupuncture group; ECP, Exercise combined with psychotherapy group; EXE, Exercise therapy group; PSY, Psychotherapy group; MT, Music therapy group. |
Consistency and Heterogeneity Analysis
For the network meta-analysis of depressive symptoms in this review, the ratio was found to be very close to 1, and the DIC value (66.9) was lower than that of the inconsistent model (67.73). All p-values from the node-splitting analyses were ≥0.05, indicating no evidence of local inconsistency. Therefore, the consistency model was selected for the subsequent network meta-analysis. At this stage, I2 was 6%, and the total model heterogeneity was also 6%.
Similarly, the odds ratio approximated unity (≈1). The DIC value of the consistency model (15.2) was comparatively lower than the inconsistency model (17.9). No evidence of local inconsistency emerged from node-splitting tests (p≥ 0.05), supporting the selection of the consistency model. Moderate heterogeneity was observed (I2, 21%; total model heterogeneity: 21%).
Depressive Symptoms
Overall, a total of 35 RCTs involving 4047 participants evaluated the effects of six non-pharmacological interventions on depressive symptoms in patients with PPD. As shown in the forest plot (Figure 6), four non-pharmacological interventions were statistically significantly effective in improving depressive symptoms compared to the control group. These interventions included acupuncture (MD, −1.1, 95% CrI −1.8 to −0.44), exercise combined with psychotherapy (MD, −1.5, 95% CrI −2.3 to −0.85), exercise therapy (MD, −1.1, 95% CrI −1.7 to −0.48), and psychotherapy (MD, −0.93, 95% CrI −1.3 to −0.60).
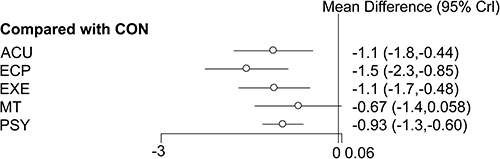 |
Figure 6 Forest plot of network meta-analysis results for depressive outcomes. This forest plot illustrates the mean differences (95% credible intervals, CrI) for various interventions compared with the control group. Each intervention is represented by a horizontal line with a point estimate (hollow circle) and the 95% credible interval (horizontal line). The mean differences indicate the effect size of each intervention relative to the control group, with negative values suggesting a reduction in symptoms compared to the control. The intervals represent the uncertainty around the point estimate, and a wider interval suggests more uncertainty. The closer the interval is to zero, the less certain the effect is. |
Anxiety Symptoms
A total of 9 RCTs, including 863 participants, assessed the effects of six non-pharmacological interventions on anxiety symptoms in patients with PPD. As shown in the forest plot (Figure 7), three non-pharmacological interventions were found to significantly improve anxiety symptoms compared to the control group. These interventions were exercise combined with psychotherapy (MD, −1.3, 95% CrI −2.3 to −0.18), exercise therapy (MD, −1.0, 95% CrI −2.0 to −0.0021), and psychotherapy (MD, −0.56, 95% CrI −0.96 to −0.052).
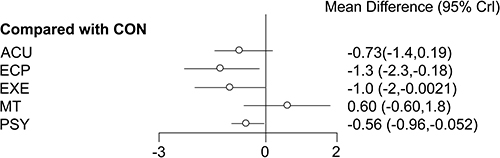 |
Figure 7 Forest plot of network meta-analysis results for anxiety outcomes. This forest plot illustrates the mean differences (95% credible intervals, CrI) for various interventions compared with the control group. Each intervention is represented by a horizontal line with a point estimate (hollow circle) and the 95% credible interval (horizontal line). The mean differences indicate the effect size of each intervention relative to the control group, with negative values suggesting a reduction in symptoms compared to the control. The intervals represent the uncertainty around the point estimate, and a wider interval suggests more uncertainty. The closer the interval is to zero, the less certain the effect is. |
Effectiveness Rankings of Interventions
Table 3 and Figure 8 present the probability rankings of different interventions for improving depressive symptoms in patients with PPD. The results indicate that exercise combined with psychotherapy ranks highest in effectiveness (p-score, 0.92), followed by acupuncture (p-score, 0.64) and exercise therapy (p-score, 0.62). Similarly, Table 3 and Figure 9 show the probability rankings of interventions for improving anxiety symptoms in patients with PPD. The findings demonstrate that exercise combined with psychotherapy remains the most effective intervention (p-score, 0.89), followed by exercise therapy (p-score, 0.76) and acupuncture (p-score, 0.61).
 |
Table 3 Interventions Ranking |
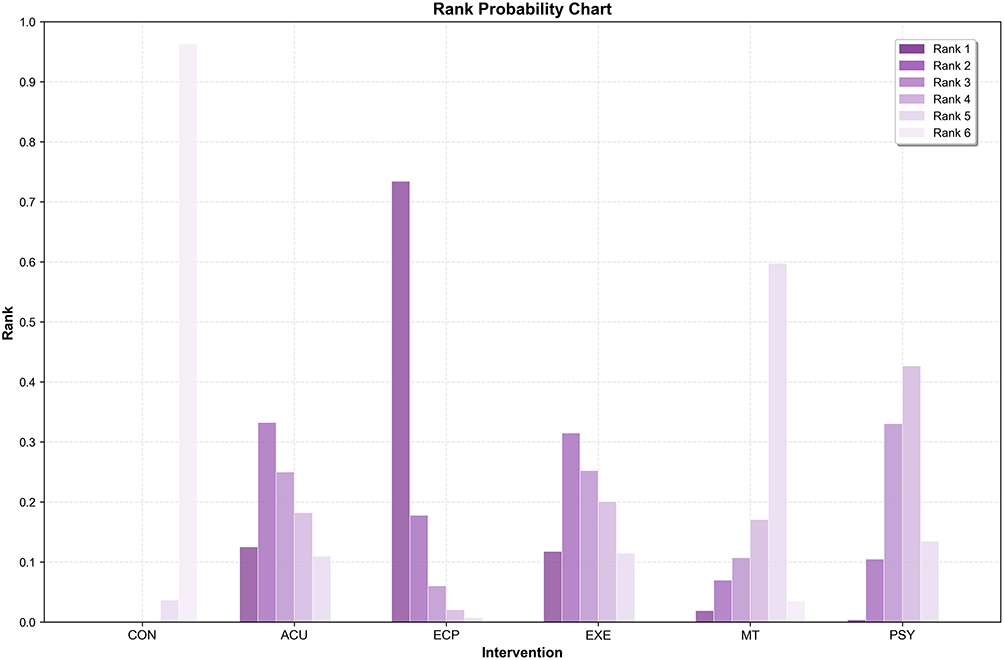 |
Figure 8 The ranking of each intervention in improving depressive symptoms. The horizontal axis represents each intervention, the vertical axis represents the probability of the intervention under that ranking, and the height of the bar then characterizes the probability value (0–1). |
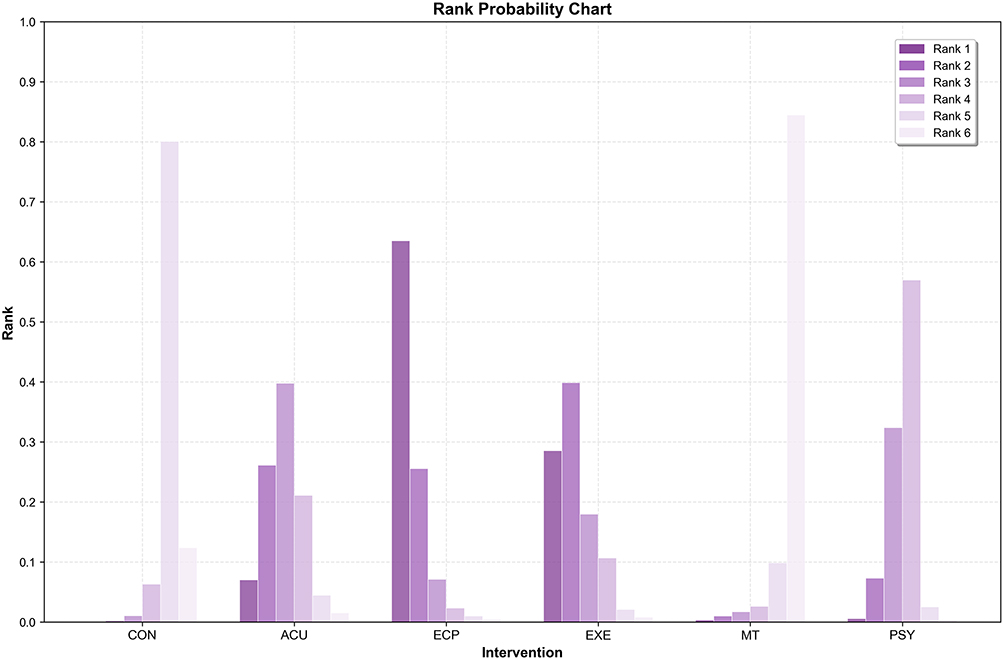 |
Figure 9 The ranking of each intervention in improving anxiety symptoms. The horizontal axis represents each intervention, the vertical axis represents the probability of the intervention under that ranking, and the height of the bar then characterizes the probability value (0–1). |
Reporting Bias
The funnel plot for depressive symptoms appears asymmetrical, suggesting the potential presence of publication bias (Figure 10).
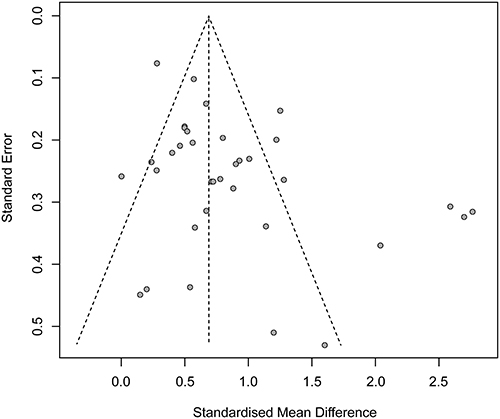 |
Figure 10 Reporting bias in depressive symptoms. This funnel plot displays the relationship between the standardized mean difference (x-axis) and standard error (y-axis) for the studies included in the network meta-analysis. Each dot represents a study, with the position along the x-axis indicating the effect size (standardized mean difference) and the position along the y-axis representing the standard error. The dashed lines represent the expected distribution for studies with no publication bias, where studies with larger sample sizes are expected to cluster near the top of the plot and those with smaller sample sizes spread out at the bottom. The symmetry of the plot suggests that publication bias is unlikely, while asymmetry may indicate the presence of such bias. |
Discussion
Summary of Findings
Despite the growing adoption of non-pharmacological interventions in PPD management, the lack of reliable clinical guidelines continues to impede their standardized implementation, while their therapeutic features and comparative efficacy remain insufficiently investigated. To our knowledge, this study constitutes the first NMA systematically evaluating the non-pharmacological interventions in ameliorating both depressive and anxiety symptoms among individuals with PPD. Distinct from prior pairwise meta-analyses, our review encompassed 35 RCTs involving 4047 participants, which rigorously assessed five non-pharmacological interventions: acupuncture, exercise therapy, psychotherapy, music therapy, and a combination of ECP. The results demonstrated statistically significant improvements across all five interventions in alleviating depressive and anxiety symptoms in individuals with PPD.
The rank order probability analysis for depressive symptom improvement revealed ECP as the most effective intervention, followed by acupuncture, exercise therapy, and psychotherapy, with music therapy demonstrating the lowest efficacy. These finding suggest that ECP could be an optimal therapeutic approach for PPD management, potentially due to the synergistic benefits derived from combining exercise and psychotherapy components, which appear to enhance overall intervention outcomes. Meanwhile, the ranking probability analysis demonstrated that ECP exhibited the highest potential for alleviating anxiety symptoms, followed by exercise therapy, acupuncture and music therapy, while psychotherapy showed comparatively limited effectiveness. The current findings demonstrate the therapeutic advantages of ECP as a combined intervention. Additionally, the results provide support for the potential effectiveness of exercise therapy and acupuncture as viable non-pharmacological intervention alternatives for the management of PPD-related symptoms.
Interpretation
Key mechanisms of PPD include a sharp decline in estradiol levels after childbirth, sustained elevation of cortisol levels during pregnancy and postpartum, and dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis.69–71 Additionally, reduced oxytocin and serotonin levels are closely linked to depressive symptoms.72
Current perspective on PPD intervention suggests that integrated intervention approaches combining multiple therapeutic modalities can simultaneously address both physiological and psychological factors, thereby offering a more comprehensive and multidimensional intervention strategy. Li Li’s research, demonstrated that a combined intervention of yoga and psychological counselling for primiparous women with PPD not only significantly alleviated depressive symptoms but also improved mental health, promoted postpartum body shape recovery and pelvic floor function restoration, and enhanced the patients’ quality of life.50 The rank probability analysis conducted in this study further validates the superior efficacy of ECP, showing significantly improvements in both depressive and anxiety symptoms compared to other interventions. These findings position ECP as a potentially optimal intervention strategy for PPD. Future high-quality mechanistic studies are needed to elucidate ECP’s neurobiological mechanisms and strengthen the evidence base for its clinical application.
The methodological quality of the included studies was “good”, and the risk of bias was generally manageable; however, the quality of evidence remained insufficient. According to the bias risk chart (Figure 2), most studies had low risk in “randomization process” and “selection of reported results”. However, concerns were observed in “overall bias” and “deviations from intended interventions”, with some studies showing higher risks, particularly in “randomization process” and “deviations from intended interventions”. The main issue was the lack of blinding of both participants and investigators, which impacted the quality of the evidence. Previous systematic reviews have shown that blinding is the most common factor affecting the quality of evidence in studies involving exercise, psychotherapy, acupuncture, and other interventions.73,74 Indeed, blinding is often difficult to implement when the investigators are directly involved in the intervention. Therefore, we recommend that both investigators and participants be blinded in future studies. Code names can be assigned to different groups, ensuring that neither the investigators nor the participants know the group allocations, thus enabling double blinding and improving the quality of evidence. Studies have suggested that acupuncture may alleviate depressive symptoms and exert antidepressant effects through modulation of the HPA axis.75 The neuroendocrine mechanisms provide a theoretical foundation for acupuncture’s application in PPD intervention, with clinical studies providing empirical validation. As shown in the study by Zhang et al, while both acupuncture group and control group demonstrated therapeutic effects on depression and anxiety symptoms, the acupuncture group exhibited significantly superior outcomes.58 To further evaluate the efficacy of acupuncture, this review included five RCTs investigating various acupuncture modalities, including scalp acupuncture, dry needling and electroacupuncture. Rank probability analysis indicated that acupuncture ranked second and third for improving depressive and anxiety symptoms, respectively. These findings align with previous RCTs and meta-analyses.73 Nevertheless, due to variability in intervention efficacy and heterogeneity in acupoint selection, additional high-quality studies are warranted to establish optimal intervention parameters and elucidate the underlying mechanisms.
Accumulating evidence suggests that exercise therapy may alleviate depressive and anxiety symptoms in PPD patients by modulating HPA axis dysfunction and enhancing the secretion of oxytocin and serotonin.76–78 These neurobiological mechanisms provide a theoretical support for clinical application, while the high practicality and safety of exercise therapy further enhance its clinical utility. For instance, by conducting a 12-week study, Armstrong et al found that stroller walking interventions significantly improved both physical fitness levels and depressive symptoms in PPD patients, providing early empirical evidence for exercise therapy in PPD management.34 Meta-analytic evidence confirms that both low- and moderate-intensity exercise effectively alleviate depressive symptoms in women with PPD.74 Notably, a recent meta-analysis indicates optimal therapeutic effects are achieved with moderate-intensity exercise performed 3–4 times weekly, with 35–45 minute sessions.79 Our findings regarding exercise therapy align closely with these established conclusions, further validating its efficacy and clinical value in PPD management.
Psychological therapy addresses PPD-related psychosocial challenges by enhancing role adaption and interpersonal functioning.80 Various evidence-based psychological interventions have been widely employed in PPD intervention, particularly interpersonal therapy (IPT) and cognitive behavioral therapy (CBT). For instance, Seo et al developed a CBT-based application that demonstrated efficacy in promoting healthy behaviors and alleviated depressive symptoms among postpartum mothers.67 Nevertheless, while psychological therapy shows significant potential for PPD management, its therapeutic effects may vary depending on individual differences and intervention adherence. Although our study confirmed the effectiveness of psychological interventions, the outcomes were comparatively less robust than those of ECP, acupuncture, and exercise therapy.
Emerging evidence indicates that music stimulation, as a form of environmental enrichment, upregulates brain-derived neurotrophic factor (BDNF) in key brain regions including the prefrontal cortex, amygdala, hypothalamus and hippocampus, thereby alleviating depressive and anxiety-like behaviors,81,82 A RCT demonstrated that music therapy significantly reduced anxiety symptoms in both mothers and infants compared to control group,83 Nevertheless, research examining music therapy’s efficacy for mothers with PPD remains limited, resulting in the inclusion of only a small number of relevant studies in our analysis. Although music therapy did not achieve high ranking in our evaluation, its potential role in emotion regulation warrants further investigation, particularly its combined effects when integrated with other non-pharmacological interventions.
Strengths and Limitations
This study represents the first NMA to systematically evaluate the efficacy of five distinct non-pharmacological interventions for the treatment of PPD. Our comprehensive study search across seven authoritative databases ensured source diversity and methodological rigor. The analysis exclusively incorporated RCTs meeting stringent design criteria to guarantee high-quality evidence. The results suggest that, compared to the control group, these interventions exert their antidepressant and anxiolytic effects. Importantly, these evidence-based results empower both patients and healthcare providers to make informed clinical decisions regarding PPD management.
This NMA have several limitations that warrant consideration: (1) Clinical heterogeneity may exist across the included non-pharmacological interventions due to variations in treatment protocols. (2) Most of the trials in this review lacked long-term follow-up data, therefore it was not possible to assess the long-term effects of these interventions. (3) While this review primarily focused on single intervention effects (with the exception of ECP), the therapeutic potential of combined non-pharmacological interventions remains underexplored. Future research should systematically examine multimodal intervention strategies to determine their synergistic effectiveness in PPD management.
Conclusion
This study underscores the potential of non-pharmacological interventions in managing PPD. The findings indicate that exercise, acupuncture, and ECP show promising effects in improving depression and anxiety symptoms, suggesting a role for ECP as a first-line intervention for mild to moderate PPD. In contrast, music therapy demonstrated more modest benefits, necessitating further validation through rigorously designed RCTs. Given the multifactorial etiology of PPD, future research should prioritize the development of multimodal intervention strategies to support personalized intervention. However, these conclusions should be interpreted with caution due to methodological heterogeneity, limited long-term follow-up, and generalizability constraints of the included studies. Therefore, further high-quality, large-scale, multicenter randomized controlled trials are warranted to substantiate these findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in dratting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Sichuan Province [2022NSFSC1529] and the Excellence Research Project of the Institute of Sports Medicine and Health, Chengdu Sport University[2025-A027].
Disclosure
The authors declare that they have no competing interests.
References
1. Stewart DE, Vigod S. Postpartum depression. New Engl J Med. 2016;375(22):2177–2186. doi:10.1056/NEJMcp1607649
2. Worthen RJ, Beurel E. Inflammatory and neurodegenerative pathophysiology implicated in postpartum depression. Neurobiol Dis. 2022;165:105646. doi:10.1016/j.nbd.2022.105646
3. Dimcea DA, Petca RC, Dumitrașcu MC, Șandru F, Mehedințu C, Petca A. Postpartum depression: etiology, treatment, and consequences for maternal care. Diagnostics. 2024;14(9):865. doi:10.3390/diagnostics14090865
4. Wan Mohamed Radzi C, Salarzadeh Jenatabadi H, Samsudin N. Postpartum depression symptoms in survey-based research: a structural equation analysis. BMC Public Health. 2021;21(1):27. doi:10.1186/s12889-020-09999-2
5. Soe NN, Wen DJ, Poh JS, et al. Pre- and post-natal maternal depressive symptoms in relation with infant frontal function, connectivity, and behaviors. PLoS One. 2016;11(4):e0152991. doi:10.1371/journal.pone.0152991
6. Hahn-Holbrook J, Cornwell-Hinrichs T, Anaya I. Economic and health predictors of national postpartum depression prevalence: a systematic review, meta-analysis, and meta-regression of 291 studies from 56 countries. Front Psychiatr. 2018;9:8. doi:10.3389/fpsyt.2018.00008
7. Zhao XH, Zhang ZH. Risk factors for postpartum depression: an evidence-based systematic review of systematic reviews and meta-analyses. Asian J Psychiatr. 2020;53:102353. doi:10.1016/j.ajp.2020.102353
8. Dennis CL, Singla DR, Brown HK, et al. Postpartum depression: a clinical review of impact and current treatment solutions. Drugs. 2024;84(6):645–659. doi:10.1007/s40265-024-02038-z
9. Meltzer-Brody S, Gerbasi ME, Mak C, et al. Indirect comparisons of relative efficacy estimates of zuranolone and selective serotonin reuptake inhibitors for postpartum depression. J Med Econ. 2024;27(1):582–595. doi:10.1080/13696998.2024.2334160
10. Lanza Di Scalea T, Wisner KL. Antidepressant medication use during breastfeeding. Clin Obstet Gynecol. 2009;52(3):483–497. doi:10.1097/GRF.0b013e3181b52bd6
11. Sie SD, Wennink JM, van Driel JJ, et al. Maternal use of SSRIs, SNRIs and NaSSAs: practical recommendations during pregnancy and lactation. Arch Dis Child Fetal Neonatal Ed. 2012;97(6):F472–476. doi:10.1136/archdischild-2011-214239
12. Faden J, Citrome L. Intravenous brexanolone for postpartum depression: what it is, how well does it work, and will it be used? Ther Adv Psychopharmacol. 2020;10:2045125320968658. doi:10.1177/2045125320968658
13. Chabrol H, Teissedre F, Armitage J, Danel M, VJJoR W, Psychology I. Acceptability of psychotherapy and antidepressants for postnatal depression among newly delivered mothers. J Reprod Infant Psychol. 2004;22:12–15 doi:10.1080/02646830310001643094.
14. Rihmer Z, Gonda X. Antidepressant-resistant depression and antidepressant-associated suicidal behaviour: the role of underlying bipolarity. Depress Res Treat. 2011;2011:906462. doi:10.1155/2011/906462
15. Singh B, Olds T, Curtis R, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. Br J Sports Med. 2023;57(18):1203–1209. doi:10.1136/bjsports-2022-106195
16. Stuart S. Interpersonal psychotherapy for postpartum depression. Clin Psychol Psychother. 2012;19(2):134–140. doi:10.1002/cpp.1778
17. Steinberg H, Sykes EA. Introduction to symposium on endorphins and behavioural processes; review of literature on endorphins and exercise. Pharmacol Biochem Behav. 1985;23(5):857–862. doi:10.1016/0091-3057(85)90083-8
18. Daley AJ, Macarthur C, Winter H, Winter H. The role of exercise in treating postpartum depression: a review of the literature. J Midwifery Women’s Health. 2007;52(1):56–62. doi:10.1016/j.jmwh.2006.08.017
19. Yang NN, Lin LL, Li YJ, et al. Potential mechanisms and clinical effectiveness of acupuncture in depression. Curr Neuropharmacol. 2022;20(4):738–750. doi:10.2174/1570159X19666210609162809
20. Ji M, Li R, Xu Y. Meta-analysis of the effect of different exercise modalities in the prevention and treatment of perinatal depression. J Affective Disorders. 2024;350:442–451. doi:10.1016/j.jad.2024.01.076
21. Wang X, Qiu Q, Shen Z, Yang S, Shen X. A systematic review of interpersonal psychotherapy for postpartum depression. J Affective Disorders. 2023;339:823–831. doi:10.1016/j.jad.2023.07.067
22. Huang R, Yang D, Lei B, et al. The short- and long-term effectiveness of mother-infant psychotherapy on postpartum depression: a systematic review and meta-analysis. J Affective Disorders. 2020;260:670–679. doi:10.1016/j.jad.2019.09.056
23. Stamou G, García-Palacios A, Botella C. Cognitive-Behavioural therapy and interpersonal psychotherapy for the treatment of post-natal depression: a narrative review. BMC psychol. 2018;6(1):28. doi:10.1186/s40359-018-0240-5
24. Li S, Zhong W, Peng W, Jiang G. Effectiveness of acupuncture in postpartum depression: a systematic review and meta-analysis. Acupuncture Med. 2018;36(5):295–301. doi:10.1136/acupmed-2017-011530
25. Rosenberger KJ, Duan R, Chen Y, Lin L. Predictive P-score for treatment ranking in Bayesian network meta-analysis. BMC Med Res Method. 2021;21(1):213. doi:10.1186/s12874-021-01397-5
26. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71 doi:10.1136/bmj.n71.
27. Rethlefsen ML, Kirtley S, Waffenschmidt S, et al. PRISMA-S: an extension to the PRISMA statement for reporting literature searches in systematic reviews. Syst Rev. 2021;10(1):39. doi:10.1186/s13643-020-01542-z
28. Hartling L, Hamm M, Milne A, et al. AHRQ methods for effective health care. In: Validity and Inter-Rater Reliability Testing of Quality Assessment Instruments. Rockville (MD): Agency for Healthcare Research and Quality (US); 2012.
29. Andrade C. Understanding the basics of meta-analysis and how to read a forest plot: as simple as it gets. J Clini Psych. 2020;81(5). doi:10.4088/JCP.20f13698
30. Neupane B, Richer D, Bonner AJ, Kibret T, Beyene J. Network meta-analysis using R: a review of currently available automated packages. PLoS One. 2014;9(12):e115065. doi:10.1371/journal.pone.0115065
31. van Valkenhoef G, Dias S, Ades AE, Welton NJ. Automated generation of node-splitting models for assessment of inconsistency in network meta-analysis. Res Synth Methods. 2016;7(1):80–93. doi:10.1002/jrsm.1167
32. Rücker G, Schwarzer G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med Res Method. 2015;15:58. doi:10.1186/s12874-015-0060-8
33. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
34. Armstrong K, Edwards H. The effects of exercise and social support on mothers reporting depressive symptoms: a pilot randomized controlled trial. Int J Ment Health Nurs. 2003;12(2):130–138. doi:10.1046/j.1440-0979.2003.00229.x
35. Armstrong K, Edwards H. The effectiveness of a pram-walking exercise programme in reducing depressive symptomatology for postnatal women. Int J Nurs Pract. 2004;10(4):177–194. doi:10.1111/j.1440-172X.2004.00478.x
36. Buttner MM, Brock RL, O’Hara MW, Stuart S. Efficacy of yoga for depressed postpartum women: a randomized controlled trial. Complement Ther Clin Pract. 2015;21(2):94–100. doi:10.1016/j.ctcp.2015.03.003
37. Chabrol H, Teissedre F, Saint-Jean M, Teisseyre N, Rogé B, Mullet E. Prevention and treatment of post-partum depression: a controlled randomized study on women at risk. Psychol med. 2002;32(6):1039–1047. doi:10.1017/S0033291702006062
38. Chen CH, Tseng YF, Chou FH, Wang SY. Effects of support group intervention in postnatally distressed women. A controlled study in Taiwan. J Psychosom Res. 2000;49(6):395–399. doi:10.1016/S0022-3999(00)00180-X
39. Chen YY. Integrating acupuncture regimen for mild to moderate depression postpartum clinical research [Master’s thesis]. Guangzhou University of Chinese Medicine; 2019.
40. Chung KF, Yeung WF, Zhang ZJ, et al. Randomized non-invasive sham-controlled pilot trial of electroacupuncture for postpartum depression. J Affective Disorders. 2012;142(1–3):115–121. doi:10.1016/j.jad.2012.04.008
41. Daley AJ, Blamey RV, Jolly K, et al. A pragmatic randomized controlled trial to evaluate the effectiveness of a facilitated exercise intervention as a treatment for postnatal depression: the PAM-PeRS trial. Psychol med. 2015;45(11):2413–2425. doi:10.1017/S0033291715000409
42. Dennis CL, Hodnett E, Kenton L, et al. Effect of peer support on prevention of postnatal depression among high risk women: multisite randomised controlled trial. BMJ. 2009;338 doi:10.1136/bmj.a3064.
43. Dennis CL, Grigoriadis S, Zupancic J, Kiss A, Ravitz P. Telephone-based nurse-delivered interpersonal psychotherapy for postpartum depression: nationwide randomised controlled trial. Br J Psychiatry. 2020;216(4):189–196. doi:10.1192/bjp.2019.275
44. Forsyth J, Boath E, Henshaw C, Brown H. Exercise as an adjunct treatment for postpartum depression for women living in an inner city-A pilot study. Health Care Women Int. 2017;38(6):635–639. doi:10.1080/07399332.2017.1295049
45. Gui Y, Xu X. Effectiveness of group mindfulness-based yoga in patients with postpartum depression. Nurs Pract Res. 2020;17(22):92–93 doi:10.3969/j.issn.1672-9676.2020.22.036.
46. Guo CG, Jiashu, Xu X. Cognitive behavioural therapy combined with systemic family therapy improves mild to moderate postpartum depression. Chin Foreign Women’s Health Res. 2017;48–50 doi:10.3969/i.issn.2096-0417.2017.22.034.
47. Gjerdingen DK, McGovern P, Pratt R, Johnson L, Crow S. Postpartum doula and peer telephone support for postpartum depression: a pilot randomized controlled trial. J Prim Care Community Health. 2013;4(1):36–43. doi:10.1177/2150131912451598
48. Heh SS, Huang LH, Ho SM, Fu YY, Wang LL. Effectiveness of an exercise support program in reducing the severity of postnatal depression in Taiwanese women. Birth. 2008;35(1):60–65. doi:10.1111/j.1523-536X.2007.00192.x
49. Hou Y, Hu P, Zhang Y, et al. Combined cognitive behavior therapy with systematic family therapy inpatients with mild to moderate post-partum depression. Chin Mental Health J. 2012;26(10):741–747 doi:10.3969/i.issn.1000-6729.2012.10.005.
50. Li L, Gao L. Effects of yoga combined with psychological counseling on mental health, body type and pelvic floor function recovery of primiparas with postpartum depression. Chin J Health Psychol. 2019;27(01):118–123 doi:10.13342/j.cnki.cjhp.2019.01.035.
51. Li Q, Li M, Yang J. Analysis of the effect of psychological intervention on postpartum depression in second-born pregnant women. Health Edu Health Promotion. 2020;15(03):307–309+339 doi:10.16117/j.cnki.31-1974/r.202003028.
52. Li P. A preliminary study on the mechanism and the intervention effect of mindfulness-based music therapy on postpartum depression [Master’s thesis]. Hebei medical university; 2019.
53. Liu C, Chen H, Zhou F, et al. Positive intervention effect of mobile health application based on mindfulness and social support theory on postpartum depression symptoms of puerperae. BMC Women’s Health. 2022;22(1):413. doi:10.1186/s12905-022-01996-4
54. Ngai FW, Wong PW, Leung KY, Chau PH, Chung KF. The Effect Of Telephone-Based Cognitive-Behavioral Therapy On Postnatal Depression: A Randomized Controlled Trial. Psychother Psychosom. 2015;84(5):294–303. doi:10.1159/000430449
55. Wang C, Liu S, Xu W. Clinical effect of applying Chinese five elements music therapy onpostpartum depression on the basis of psychological care. Chin J Conval Med. 2018;27(01):15–17 doi:10.13517/j.cnki.ccm.2018.01.005.
56. Xu S. clinical observation on acupuncture in treating postpartum depression [Master’s thesis]. Guangzhou University of Chinese Medicine; 2010.
57. Yang Y. Study on the difference of clinical curative effect and theinfluence of intestinal flora in the treatment of postpartumdepression by “Tiao Ren Tong Du” Acupuncture [Master’s thesis]. Guangzhou University of Chinese Medicine; 2021.
58. Zhang K. Observation on the clinical effect of acupuncture treatment of postpartum depression [Master’s thesis]. Heilongjiang University of Chinese Medicine; 2017.
59. Milgrom J, Danaher BG, Gemmill AW, et al. Internet cognitive behavioral therapy for women with postnatal depression: a randomized controlled trial of mumMoodBooster. J Med Internet Res. 2016;18(3):e54. doi:10.2196/jmir.4993
60. Milgrom J, Negri LM, Gemmill AW, McNeil M, Martin PR. A randomized controlled trial of psychological interventions for postnatal depression. Br J Clin Psychol. 2005;44(4):529–542. doi:10.1348/014466505X34200
61. Norman E, Sherburn M, Osborne RH, Galea MP. An exercise and education program improves well-being of new mothers: a randomized controlled trial. Physical Ther. 2010;90(3):348–355. doi:10.2522/ptj.20090139
62. O’Hara MW, Scott S, Gorman Laura L, Amy W. Efficacy of interpersonal psychotherapy for postpartum depression. Arch Gen Psychiatry. 2000;57(11):1039–1045. doi:10.1001/archpsyc.57.11.1039
63. Perkins R, Spiro N, Waddell G. Online songwriting reduces loneliness and postnatal depression and enhances social connectedness in women with young babies: randomised controlled trial. Public Health. 2023;220:72–79. doi:10.1016/j.puhe.2023.04.017
64. Jannati N, Mazhari S, Ahmadian L, Mirzaee M. Effectiveness of an app-based cognitive behavioral therapy program for postpartum depression in primary care: a randomized controlled trial. Int J Med Inform. 2020;141:104145. doi:10.1016/j.ijmedinf.2020.104145
65. Özkan S, Kücükkelepce DS, Korkmaz B, Yılmaz G, Bozkurt MA. The effectiveness of an exercise intervention in reducing the severity of postpartum depression: a randomized controlled trial. Perspect Psychiatr Care. 2020;56(4):844–850. doi:10.1111/ppc.12500
66. Ribeiro MKA, Alcântara-Silva TRM, Oliveira JCM, et al. Music therapy intervention in cardiac autonomic modulation, anxiety, and depression in mothers of preterms: randomized controlled trial. BMC psychol. 2018;6(1):57. doi:10.1186/s40359-018-0271-y
67. Seo JM, Kim SJ, Na H, Kim JH, Lee H. Effectiveness of a mobile application for postpartum depression self-management: evidence from a randomised controlled trial in South Korea. Healthcare. 2022;10(11):2185. doi:10.3390/healthcare10112185
68. Sjömark J, Svanberg AS, Larsson M, et al. Effect of internet-based cognitive behaviour therapy among women with negative birth experiences on mental health and quality of life - a randomized controlled trial. BMC Pregnancy Childbirth. 2022;22(1):835. doi:10.1186/s12884-022-05168-y
69. Frokjaer VG, Pinborg A, Holst KK, et al. Role of serotonin transporter changes in depressive responses to sex-steroid hormone manipulation: a positron emission tomography study. Biol Psychiatry. 2015;78(8):534–543. doi:10.1016/j.biopsych.2015.04.015
70. Glynn LM, Sandman CA. Evaluation of the association between placental corticotrophin-releasing hormone and postpartum depressive symptoms. Psychosomatic Med. 2014;76(5):355–362. doi:10.1097/PSY.0000000000000066
71. Brummelte S, Galea LA. Postpartum depression: etiology, treatment and consequences for maternal care. Horm Behav. 2016;77:153–166. doi:10.1016/j.yhbeh.2015.08.008
72. Stuebe AM, Grewen K, Meltzer-Brody S. Association between maternal mood and oxytocin response to breastfeeding. J Women’s Health. 2013;22(4):352–361. doi:10.1089/jwh.2012.3768
73. Tong P, Dong LP, Yang Y, Shi YH, Sun T, Bo P. Traditional Chinese acupuncture and postpartum depression: a systematic review and meta-analysis. J Chin Med Assoc. 2019;82(9):719–726. doi:10.1097/JCMA.0000000000000140
74. He L, Soh KL, Huang F, et al. The impact of physical activity intervention on perinatal depression: a systematic review and meta-analysis. J Affective Disorders. 2023;321:304–319. doi:10.1016/j.jad.2022.10.026
75. Li P, Zhao J, Wei X, et al. Acupuncture may play a key role in anti-depression through various mechanisms in depression. ChinMed. 2024;19(1):135. doi:10.1186/s13020-024-00990-2
76. Clark PJ, Amat J, McConnell SO, et al. Running reduces uncontrollable stress-evoked serotonin and potentiates stress-evoked dopamine concentrations in the rat dorsal striatum. PLoS One. 2015;10(11):e0141898. doi:10.1371/journal.pone.0141898
77. Kim TK, Lee JE, Kim JE, et al. G9a-mediated regulation of OXT and AVP expression in the basolateral amygdala mediates stress-induced lasting behavioral depression and its reversal by exercise. Mol Neurobiol. 2016;53(5):2843–2856. doi:10.1007/s12035-015-9160-z
78. Naghibi S, Barzegari A, Shariatzadeh M, et al. Voluntary physical activity increases maternal care and reduces anxiety- and depression-related behaviours during the postpartum period in mice. Brain Res. 2022;1784:147880. doi:10.1016/j.brainres.2022.147880
79. Xu H, Liu R, Wang X, Yang J. Effectiveness of aerobic exercise in the prevention and treatment of postpartum depression: meta-analysis and network meta-analysis. PLoS One. 2023;18(11):e0287650. doi:10.1371/journal.pone.0287650
80. Reay RE, Mulcahy R, Wilkinson RB, Owen C, Shadbolt B, Raphael B. The development and content of an interpersonal psychotherapy group for postnatal depression. Int J Group Psychother. 2012;62(2):221–251. doi:10.1521/ijgp.2012.62.2.221
81. Angelucci F, Ricci E, Padua L, Sabino A, Tonali PA. Music exposure differentially alters the levels of brain-derived neurotrophic factor and nerve growth factor in the mouse hypothalamus. Neurosci lett. 2007;429(2–3):152–155. doi:10.1016/j.neulet.2007.10.005
82. Papadakakis A, Sidiropoulou K, Panagis G. Music exposure attenuates anxiety- and depression-like behaviors and increases hippocampal spine density in male rats. Behav Brain Res. 2019;372:112023. doi:10.1016/j.bbr.2019.112023
83. Schlez A, Litmanovitz I, Bauer S, Dolfin T, Regev R, Arnon S. Combining kangaroo care and live harp music therapy in the neonatal intensive care unit setting. Isr Med Assoc J. 2011;13(6):354–358.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Utility of Zuranolone for Postpartum Depression: A Narrative Review
Giannopoulos A, Singh J, Deligiannidis KM
Neuropsychiatric Disease and Treatment 2025, 21:93-105
Published Date: 25 January 2025