Back to Journals » Journal of Pain Research » Volume 19
Comparative Effectiveness of Mind–Body Exercise Modalities on Pain Intensity and Fatigue in Patients with Non-Neuropathic Cancer-Related Pain: A Systematic Review and Network Meta-Analysis
Authors Yuan Z, Shi J, Xiang W, Yu H, Wang B, Chen Q, Yuan H, Xiao P ![]() , Weng H
, Weng H
Received 31 January 2026
Accepted for publication 10 June 2026
Published 18 June 2026 Volume 2026:19 599922
DOI https://doi.org/10.2147/JPR.S599922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rocío de la Vega
Zhoushuai Yuan,1,2,* Jian Shi,3,* Weinie Xiang,1,4 Hairui Yu,1 Biru Wang,5 Qiang Chen,6 Huijuan Yuan,7 Ping Xiao,1 Huajuan Weng1,4
1Department of Rehabilitation Medicine, The Affiliated Hospital of Jiujiang University, Jiujian, Jiangxi, People’s Republic of China; 2Division of Exercise and Movement Science, Institute for Sport Science, University of Göttingen, Göttingen, Germany; 3Department of Rehabilitation Medicine, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 4Jiujiang Key Laboratory of Modern Scientific Research on Traditional Chinese Medicine Rehabilitation Technology, Jiujiang university, Jiujiang, Jiangxi, People’s Republic of China; 5Department of Rehabilitation Medicine, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China; 6Department of Rehabilitation, Shangrao Municipal Hospital, Shangrao, Jiangxi, People’s Republic of China; 7Center for Disease Control and Prevention of Lianxi District, Jiujiang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huajuan Weng, Department of Rehabilitation Medicine, The Affiliated Hospital of Jiujiang University, Jiujian, Jiangxi, People’s Republic of China, Email [email protected]
Purpose: Cancer-related pain (CRP) is a prevalent issue among cancer survivors, especially during extended periods of survivorship. Existing therapeutic approaches for CRP present certain limitations. To investigate safe and accessible non-pharmacological interventions that may reduce both pain and fatigue, we performed a network meta-analysis (NMA) to compare various Mind–Body Exercises (MBEs) in cancer survivors experiencing CRP, excluding cases of neuropathic pain.
Patients and Methods: We systematically searched eight databases for randomized controlled trials (RCTs) assessing MBEs in adult patients with CRP. Data extraction was conducted using standardized forms. The Cochrane Risk of Bias tool was employed to evaluate study quality, and the certainty of evidence was appraised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework. The primary outcome was pain intensity, with fatigue as the secondary outcome. Both pairwise meta-analyses and the NMA were performed using random-effects models. Treatment rankings were derived from the surface under the cumulative ranking curve (SUCRA).
Results: Fourteen eligible RCTs, comprising 1070 participants, were included in the analysis. For pain intensity, Qigong had the highest SUCRA value (98.6%) and was associated with greater reductions in pain than Pilates (SMD = − 2.16, 95% CI: − 3.90 to − 0.42), dance (SMD = − 2.31, 95% CI: − 4.27 to − 0.35), and yoga (SMD = − 2.36, 95% CI: − 4.07 to − 0.64). Taichi was also associated with greater pain reduction than standard exercise (SMD = − 1.18, 95% CI: − 1.88 to − 0.48). For fatigue, Qigong ranked first based on SUCRA (94.7%) and showed a favorable effect compared with usual care (SMD = − 1.30, 95% CI: − 2.59 to − 0.01).
Conclusion: Within the limited and mainly breast cancer–based evidence, Qigong showed the most favorable ranking probabilities for pain intensity and fatigue in patients with predominantly non-neuropathic CRP. However, these findings should be interpreted with caution and regarded as exploratory rather than definitive evidence of clinical superiority. Taichi showed relatively more stable evidence for pain relief, although the overall certainty of evidence remained limited.
Keywords: mind-body exercises, cancer-related pain, cancer pain, fatigue, exercise
Introduction
Cancer represents a major global health burden and is among the leading causes of mortality, responsible for roughly one in six deaths worldwide, as reported in 2020.1,2 Advances in early detection and therapeutic approaches have led to a growing population of cancer survivors, with an increasing number achieving long-term survival.3 Despite these improvements, CRP persists as one of the most common and disabling symptoms experienced by survivors and is widely acknowledged as a critical factor influencing their quality of life (QoL).4 CRP encompasses pain resulting directly from the primary tumor, metastatic spread, or adverse effects of cancer treatments.5 In addition to limiting physical functioning, CRP is linked to heightened symptom burden—such as fatigue and depressive symptoms—greater psychological distress, reduced engagement in social activities, and overall diminished QoL.6,7
It should be noted that CRP is not a uniform condition. From a pathophysiological standpoint, it can be broadly categorized into two principal types: nociceptive pain and neuropathic pain.8 Nociceptive pain arises mainly from tissue damage and associated inflammatory processes, while neuropathic pain results from injury or disease affecting the somatosensory nervous system, whether peripheral or central.9 Because of differences in biological mechanisms, clinical manifestations, and therapeutic outcomes, predominantly non-neuropathic CRP should be distinguished from neuropathic pain when evaluating non-pharmacological interventions.6,9,10 Consequently, the International Association for the Study of Pain (IASP) has emphasized the importance of tailored, mechanism-based treatment approaches for patients with CRP.10 Nevertheless, existing research has largely concentrated either on broadly defined CRP populations or specifically on neuropathic cancer pain, particularly within RCTs and systematic reviews assessing drug-based and neuromodulatory interventions.11–13 In comparison, evidence on active, non-pharmacological interventions for predominantly non-neuropathic CRP remains limited. This notable gap in evidence regarding non-neuropathic CRP served as a key motivation for focusing on this specific patient subgroup in the current investigation.
Although opioids are the cornerstone of the management of CRP, analgesic responses are suboptimal in a substantial proportion of patients, and long-term use is limited by adverse effects such as dependence, constipation, nausea, and cognitive impairment.14–17 Mind–body exercises (MBEs), which combine movement sequences with mind-focused components such as breath regulation, relaxation, meditation, or emotion regulation, have attracted increasing attention in cancer pain rehabilitation because of their favorable safety profile, non-invasive nature, and feasibility for long-term practice.18–21 Notably, the multicomponent features of MBEs may provide a plausible rationale for alleviating both CRP and cancer-related fatigue. These two symptoms share partially overlapping biological underpinnings, including peripheral inflammatory activation, inflammation-related signaling within the central nervous system and dysregulation of related brain networks.22–26 Therefore, MBEs may contribute to symptom relief through neuromodulatory, anti-inflammatory, and psychophysiological pathways, particularly in CRP predominantly driven by nonneuropathic mechanisms.27–29
Although current studies report that MBEs can improve cancer-related symptoms, there are critical limitations in the existing evidence. First, most prior trials and evidence syntheses have focused on broadly defined CRP populations, with few explicitly distinguishing nociceptive from neuropathic pain. Because treatment response can differ by underlying pain mechanism, pooling heterogeneous pain phenotypes may bias effect estimates and reduce the precision and interpretability of conclusions.30,31 Second, available systematic reviews typically evaluate a single-intervention or single-outcome, providing limited comparative insight across different MBEs and rarely assessing pain and cancer-related fatigue within a unified analytic framework. Third, although network meta-analyses have examined MBEs for CRP, these reviews commonly include patients with heterogeneous CRP etiologies and aggregate diverse interventions (eg., meditation, mindfulness, relaxation training) under the umbrella of MBEs. Consequently, both the target population and intervention scope differ significantly from the present focus on CRP predominantly driven by nonneuropathic mechanisms and accompanied by cancer-related fatigue. Taken together, it remains unclear how different types of MBEs compare in their relative effectiveness for reducing pain intensity and improving fatigue among patients with CRP predominantly driven by nonneuropathic mechanisms.32
To address these limitations, we performed a NMA comparing multiple Mind–Body Exercise modalities for reducing the intensity of CRP and cancer-related fatigue among patients with CRP predominantly driven by nonneuropathic mechanisms, to better inform rehabilitation and pain management decisions.
Material and Methods
Protocol and Registration
The protocol for this systematic review and NMA was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO: CRD420251179880, https://www.crd.york.ac.uk/PROSPERO/view/CRD420251179880) before data extraction. The review was reported in accordance with the PRISMA guidelines, the completed PRISMA checklist is provided in Appendix 1.33
Literature Retrieval
We conducted comprehensive searches across eight databases: PubMed, Web of Science (WOS), Embase, Cochrane Library, VIP Chinese Journal Database (CQVIP), China National Knowledge Infrastructure (CNKI), Wanfang Data, and the Chinese Biomedical Literature Service System (SinoMed). All available records from the inception of each database up to September 2025 were included.
For English-language databases, search strategies were formulated by combining controlled vocabulary with free-text keywords, such as Medical Subject Headings (MeSH) in PubMed and Emtree in Embase. For Chinese databases, strategies were developed based on the SinoMed controlled vocabulary and adjusted accordingly to ensure relevance. Terms related to MBEs were derived from the approach outlined by Shi et al,34 while CRP search terms were informed by the methodology of Wang et al35 These approaches were adopted to enhance search sensitivity and reduce the likelihood of omitting pertinent studies. Detailed search strategies are available in Appendix 2.
Eligibility Criteria
Inclusion Criteria
Trials primarily enrolling patients with neuropathic cancer pain were excluded, particularly those in which pain was mainly attributable to chemotherapy-induced peripheral neuropathy or other treatment-related neuropathic pain. This was done to avoid mixing pain phenotypes with distinct pathophysiological mechanisms, thereby reducing additional heterogeneity and potential bias in effect estimates.10,36 Pain etiology was adjudicated based on the information reported in the original studies, including eligibility criteria, reported pain condition, cancer treatment history, pain descriptors, and validated neuropathic pain screening tools when available. Studies explicitly focusing on chemotherapy-induced peripheral neuropathy (CIPN), chemotherapy-related neuropathic pain, post-surgical neuropathic pain, or studies with clear neuropathic pain descriptors, such as numbness, burning pain, tingling, electric shock-like pain, allodynia, or hypoesthesia, were excluded. When tools such as DN4, LANSS, or painDETECT were reported, the original tool results were used to support classification. Studies without explicit evidence of predominant neuropathic pain were considered eligible as cancer-related pain. If chemotherapy exposure was reported but neuropathic symptoms or pain phenotype were unclear, the study was classified as unclear pain etiology and further examined in sensitivity analyses. Per trial decisions are summarized in Appendix 3 and Table S1.
MBEs were defined as active exercise-based interventions that combine physical movement components with mind-focused or psychosocial components, such as breath regulation, relaxation, attentional focus, meditation, emotional regulation, positive affective engagement, or structured social interaction.21 Interventions without an active movement component, including standalone meditation, mindfulness or relaxation training were excluded.
Control groups were classified according to their actual content in the original studies. UC referred to routine care or education without additional structured exercise; PC referred to wait-list, no-treatment, or maintenance of usual activities and SE referred to structured conventional exercise or rehabilitation without core Mind–Body components.
We excluded studies in which neuropathic pain was explicitly described in the text, such as numbness or burning pain, or in which patients had CIPN. If neuropathic pain screening tools were reported, classification was based on the original study reports. Studies in which neuropathic pain could not be clearly ruled out were included in the main analysis and further examined in sensitivity analyses.
- Adults (≥18 years) with CRP attributable to the primary tumor, metastases, or cancer treatments, in whom pain was non-neuropathic-predominant according to trial description;10
- Without restrictions on sex, race/ethnicity, cancer type, or cancer stage;
- Intervention: Mind–Body Exercise modalities (eg. Taichi, Qigong, Yoga, Pilates, Dance etc).;34,37
- Comparators: usual care (UC), standard exercise (SE) or passive control (PC).
- At least the following outcomes were reported: pain intensity (primary outcome) or cancer-related fatigue (secondary outcome).
- Study design: RCTs.
- Intervention duration: ≥4 weeks.38
Exclusion Criteria
- Full texts or primary outcome data were unavailable or could not be obtained (eg., incomplete reporting of key outcomes);
- Duplicate publications or overlapping datasets;
- Trials in which the study population primarily comprised chemotherapy-induced peripheral neuropathy (CIPN) or other explicitly described treatment-related neuropathic pain were excluded;10
- Non-randomized study designs (eg., observational experiments etc);
- Participants were<18 years of age or the population did not have CRP;
- Publication types not eligible for inclusion, including conference abstracts, study protocols, reviews, book chapters, and retracted articles.
Data Extraction
Two reviewers (HRY and BRW) independently performed data extraction with a standardized form. All extracted data were subsequently cross-checked and verified by the corresponding author. For multidimensional instruments, we extracted only the domain-specific subscale or item that directly corresponded to the prespecified outcomes, namely cancer-related pain and fatigue.
To minimize potential bias from baseline imbalances, change-from-baseline values were utilized for analysis. When necessary data could not be directly obtained from the published text, corresponding authors were contacted to request additional information. For outcomes presented only in graphical form, numerical data were extracted using Origin 2021. In cases where variability was reported as standard errors (SEs), confidence intervals (CIs), or interquartile ranges (IQRs), these were converted to standard deviations (SDs) following the guidelines outlined in Cochrane Handbook.39
For studies reporting outcomes at multiple time points (either at the end of treatment or during treatment), the assessment closest to 8 weeks was prioritized to improve comparability across trials. The 8-week time point was selected as a pragmatic reference point based on the distribution of intervention durations in the included trials, rather than as an assumed optimal intervention duration. If two time points were equidistant from 8 weeks (eg., 6 and 10 weeks), the longer duration was selected to capture a more complete intervention exposure.40,41
Risk of Bias Assessment
Two independent reviewers (QC and PX) assessed the methodological quality and potential bias of the included trials with the Cochrane risk-of-bias assessment tool. Each study was classified as a low, high, or unclear risk of bias cross domains of selection, performance, detection, attrition, reporting, and other potential sources of bias. Any discrepancies in assessment were discussed. In cases where consensus could not be achieved, a third reviewer was consulted to arbitrate, and the final decision was based on the majority opinion.
Assessment of Evidence Quality
The quality of evidence for primary and secondary outcomes was assessed by the GRADE system.42 According to the GRADE approach, evidence derived from RCTs is initially considered to be of high certainty. This rating may be lowered based on evaluations across five domains: risk of bias, inconsistency, imprecision, indirectness, and publication bias. Each domain was categorized as having no serious limitations, serious limitations, or very serious limitations. Following an assessment of these domains, the overall certainty of the evidence was graded as high, moderate, low, or very low. Two independent reviewers (QC and HJY) performed the GRADE evaluations. Any discrepancies of assessment for GRADE were resolved through consultation with a third reviewer.
Data Synthesis and Analysis
Pairwise meta-analyses were conducted in Stata 16.0 using the meta command suite to synthesize direct head-to-head evidence. Network meta-analysis (NMA) was performed using a frequentist framework in Stata 16.0 with the network command to synthesize direct and indirect comparisons. Continuous outcomes of effectiveness were summarized with standardized mean differences (SMD) and 95% confidence intervals (CI) using a random-effects model. For studies that did not report the standard deviation (SD) of change, we imputed it from the baseline and post-intervention values, assuming a correlation coefficient of 0.5 between the two measurements.43 To harmonize the direction of different scales, mean values from scales in which higher scores indicated more severe symptoms were multiplied by −1 (with the SD left unchanged) before standardization.44 In this review, a negative SMD indicates greater improvement in pain or fatigue for the row intervention compared with the column intervention. Correlations induced by multiple-arm trials were accounted for using multivariate distributions. We calculated the surface under the cumulative ranking curve (SUCRA) to rank the effectiveness of the different interventions for each target outcome.
Consistency is a key assumption for estimating the agreement between direct and indirect comparisons. Global inconsistency was assessed using a design-by-treatment interaction model. Local inconsistency was explored using node-splitting by comparing direct and indirect evidence within specific comparisons. The hypothesis of transitivity was assessed using the standard PICOS framework; we compared the distribution of baseline characteristics, duration of interventions, type of control group, risk of bias, and other relevant factors. We examined global heterogeneity in NMA using the tau-squared (τ2) statistic and assessed heterogeneity for pairwise meta-analysis with the I2 statistic. Moreover, we evaluated potential publication bias using comparison-adjusted funnel plots and Egger’s regression test.
Results
Search results
The research identified totally 1861 records. After deduplication and title/abstract screening, 1,531 records were excluded. 51 full-text articles were evaluated for eligibility and 14 Studies were included in the NMA (see Figure 1).
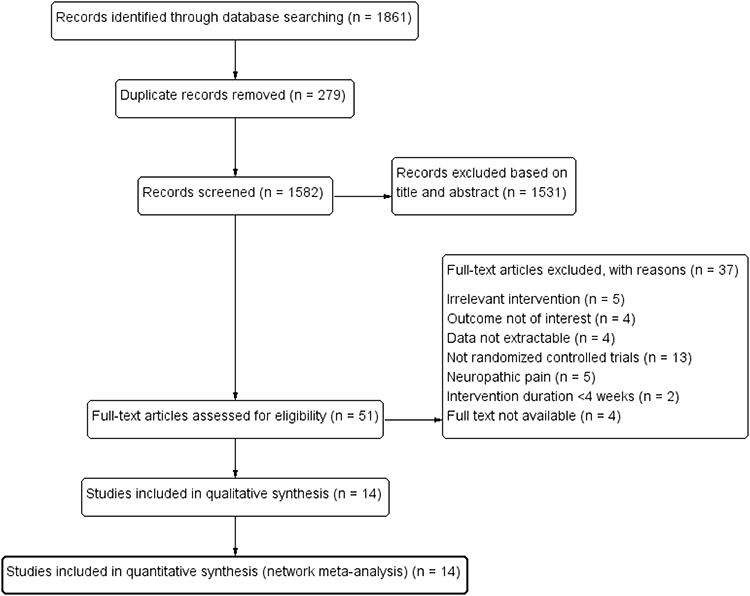 |
Figure 1 PRISMA flow diagram of the selection process for studies evaluating the efficacy of Mind–Body Exercises in patients with Cancer-related pain. |
Study Characteristics
We identified 14 studies from 8 countries, published between 2009 and 2024, comprising a total of 1,070 adult participants (>18 years old). The interventions evaluated were Pilates (4 RCTs), yoga (6 RCTs), Taichi (2 RCTs), Qigong (1 RCT), and dance (1 RCT). The intervention duration ranged from 4 to 16 weeks, with 8-week programs being the most common (5/14). Pain intensity was assessed using the Visual Analog Scale (VAS), Numeric Rating Scale (NRS), Constant-Murley Score, Brief Pain Inventory (BPI), and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30). Fatigue was measured using the Revised Piper Fatigue Scale (RPFS), Brief Fatigue Inventory (BFI), Functional Assessment of Cancer Therapy (FACT), VAS, Myeloproliferative Neoplasm Symptom Assessment Form (MPN-SAF), and EORTC QLQ-C30. Eleven studies focused on breast cancer, whereas the remaining three studies included patients with lung cancer, myeloproliferative neoplasms and cancer. Detailed study characteristics are summarized in Table 1.
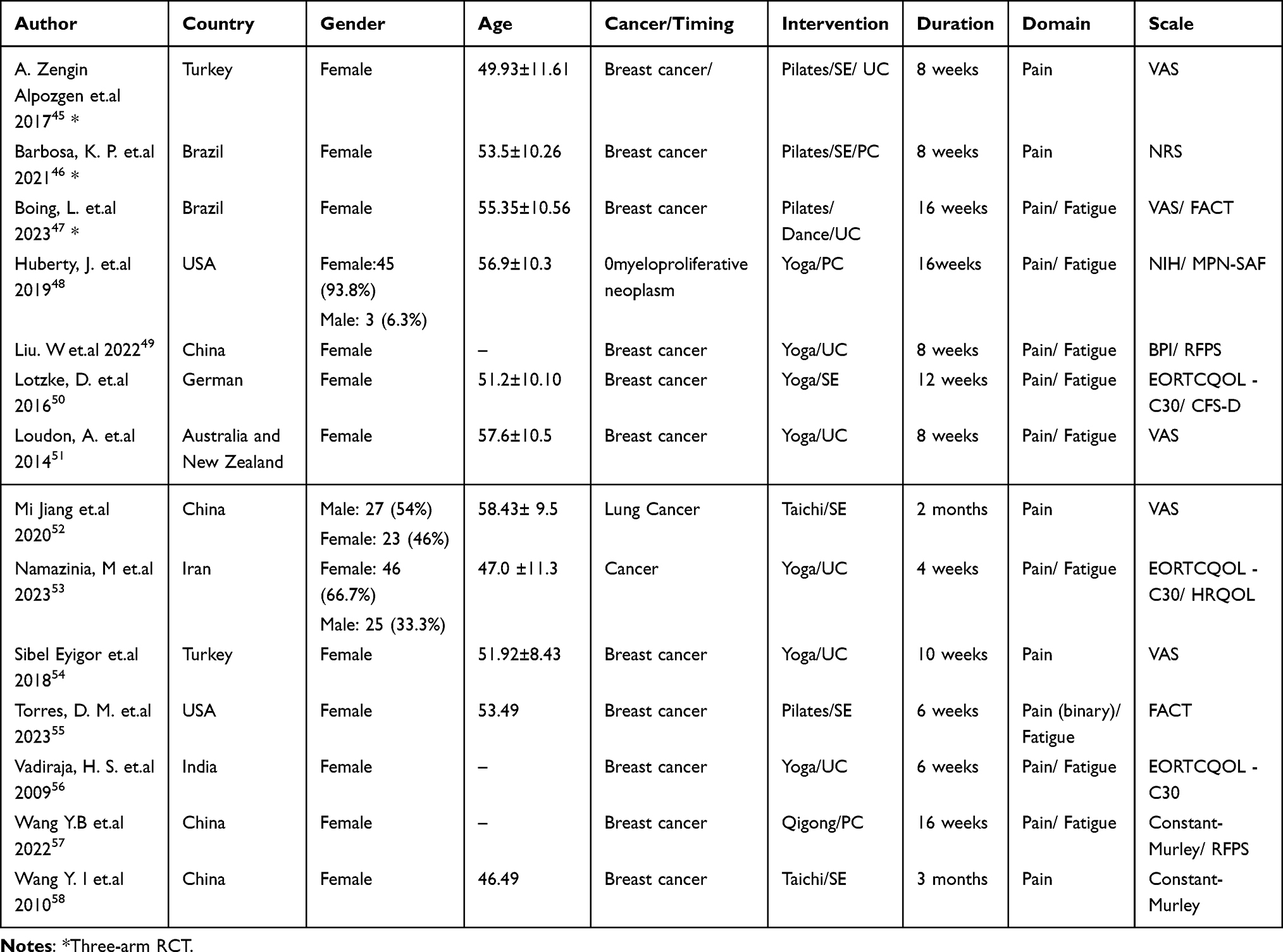 |
Table 1 Principal Characteristics of Included Studies |
Quality Appraisal of Literature
Due to the inherent nature of exercise-based interventions, all included trials were rated as having a high risk of bias for blinding of participants and personnel (performance bias).59 For blinding of outcome assessment (detection bias), only the trial by Torres et al55 explicitly reported that their outcome assessors were not blinded, and it was therefore rated as high risk. The remaining studies were rated as unclear or low risk. The outcomes of included Studies were showed in Figures 2 and 3.
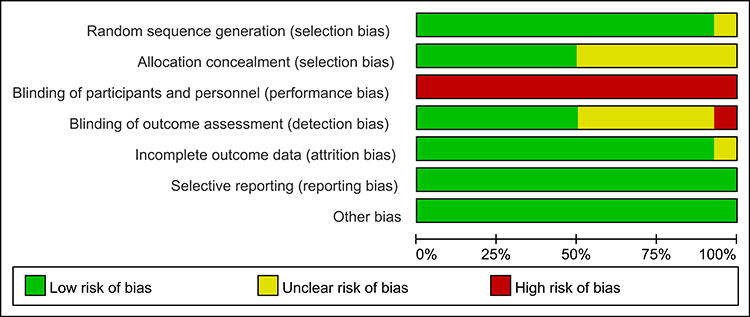 |
Figure 2 Percentage of studies evaluating the efficacy of mind–body exercise in patients with cancer pain, classified as low, unclear, or high risk of bias for each domain of the Cochrane Risk of Bias tool. |
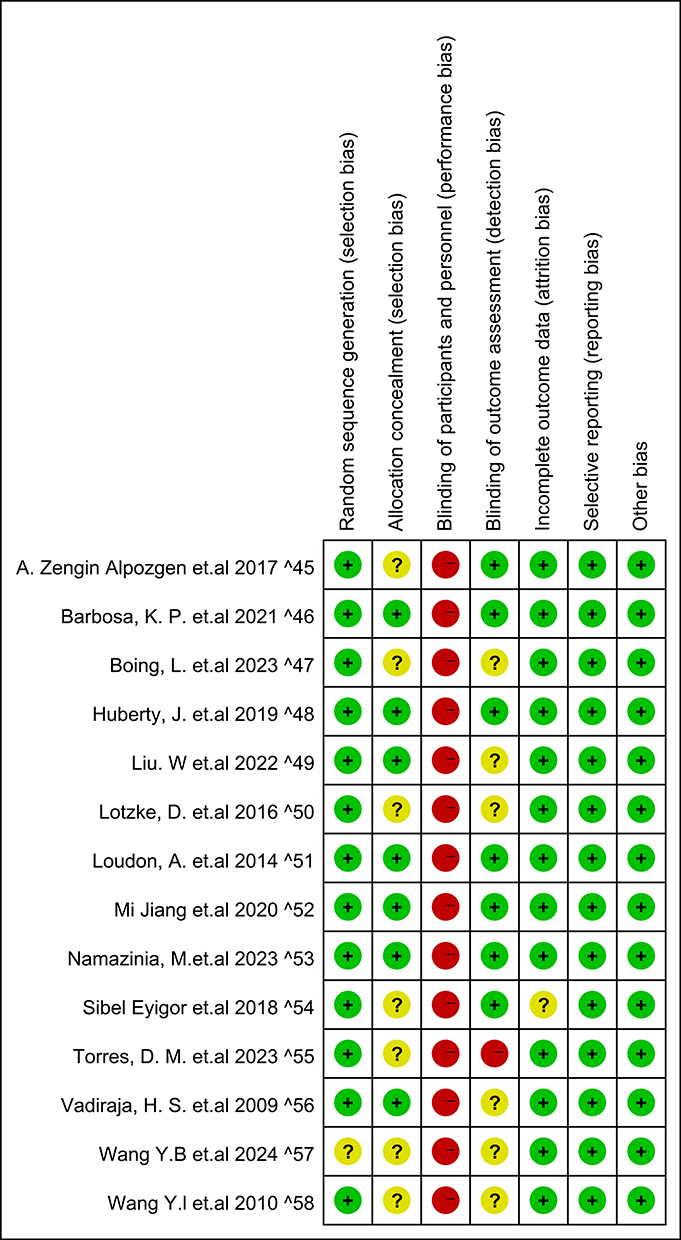 |
Figure 3 Methodological quality summary: Review authors’ judgments about each methodological quality item for each included study. Green and “+” (Low risk of bias), Yellow and “?” (Unclear risk of bias), Red and “-” (High risk of bias). |
Certainty of Evidence (GRADE)
We conducted GRADE assessments for all direct pairwise meta-analyses to evaluate the certainty of evidence for each outcome. For pain intensity (Table 2), only the comparison of Qigong versus PC was rated as low-certainty evidence; all other comparisons were rated as very low-certainty evidence, primarily due to risk of bias and very serious imprecision. A similar pattern was observed for fatigue (Table 3), where only the comparison of Qigong versus PC was rated as low-certainty evidence, and all remaining comparisons were rated as very low-certainty evidence. For more information, detailed GRADE assessments are provided in Appendix 4, Tables S2 and S3.
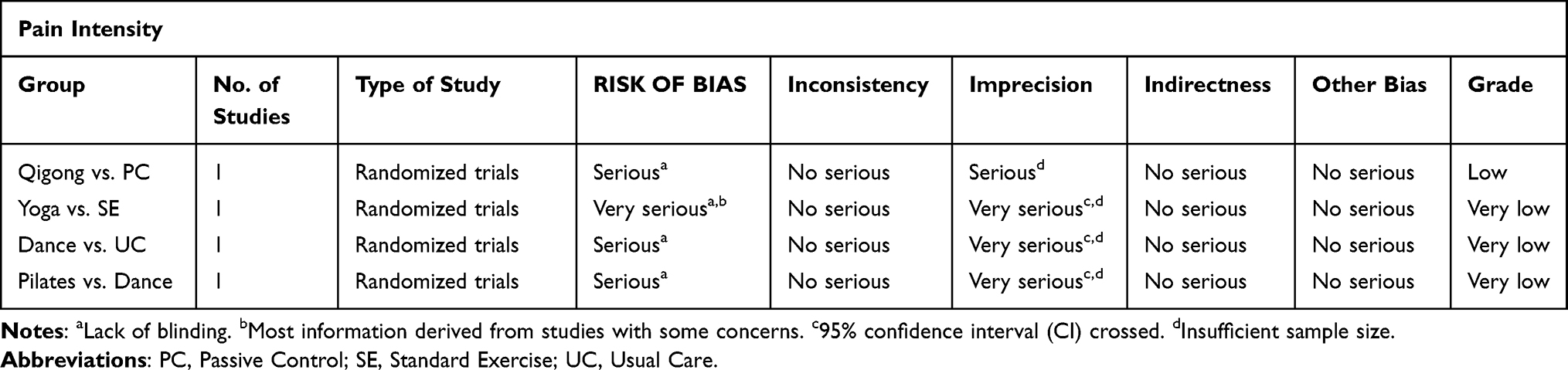 |
Table 2 GRADE Assessment for Pain Intensity |
 |
Table 3 GRADE Assessment for Fatigue |
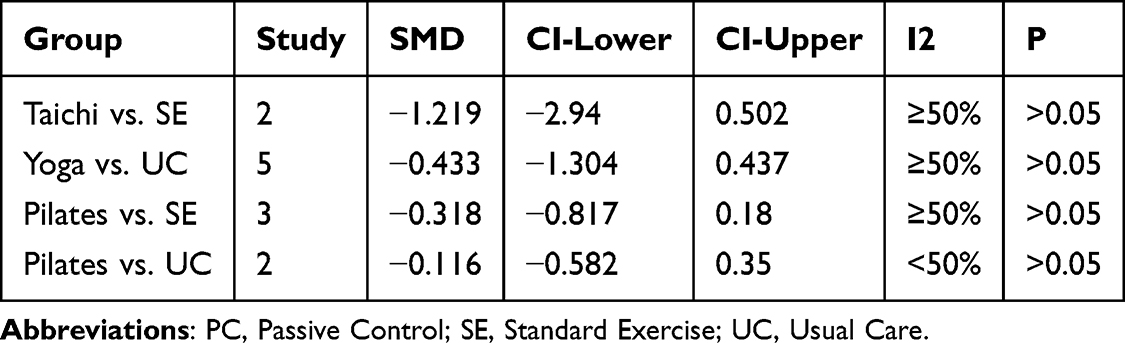 |
Table 4 Pairwise Meta-Analysis of Direct Comparisons Supported by Two or More Studies |
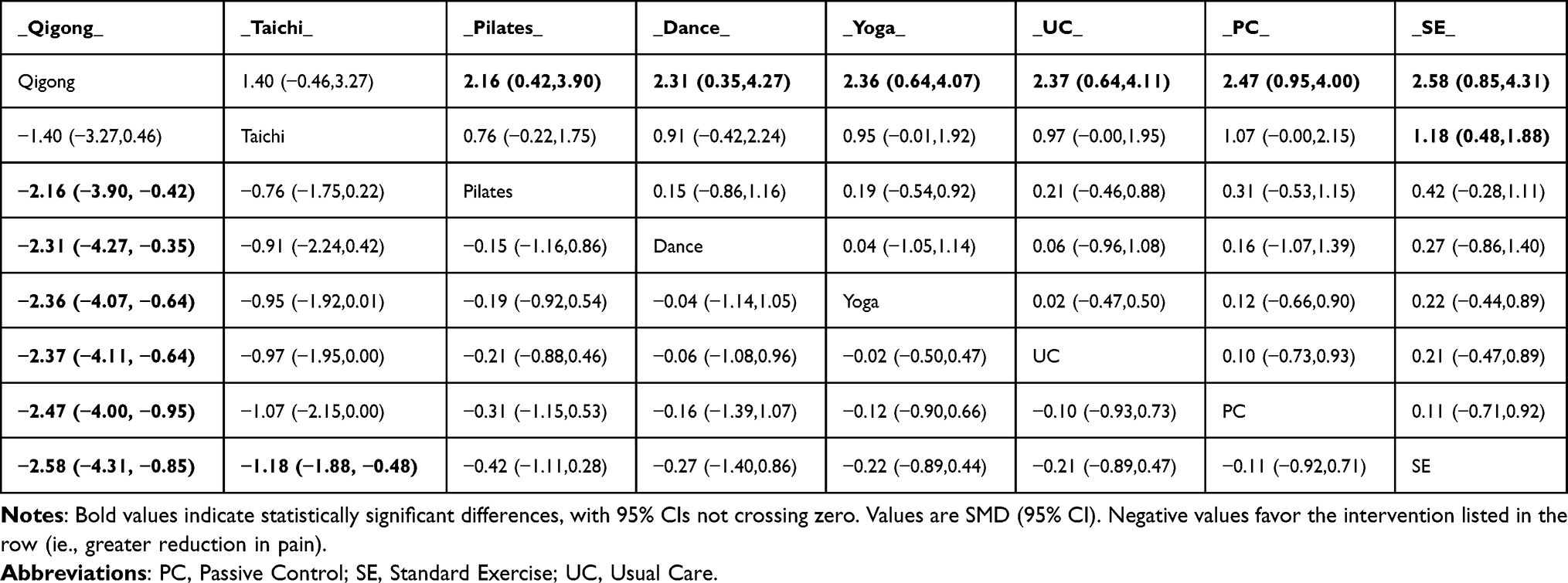 |
Table 5 League Table on Pain Intensity |
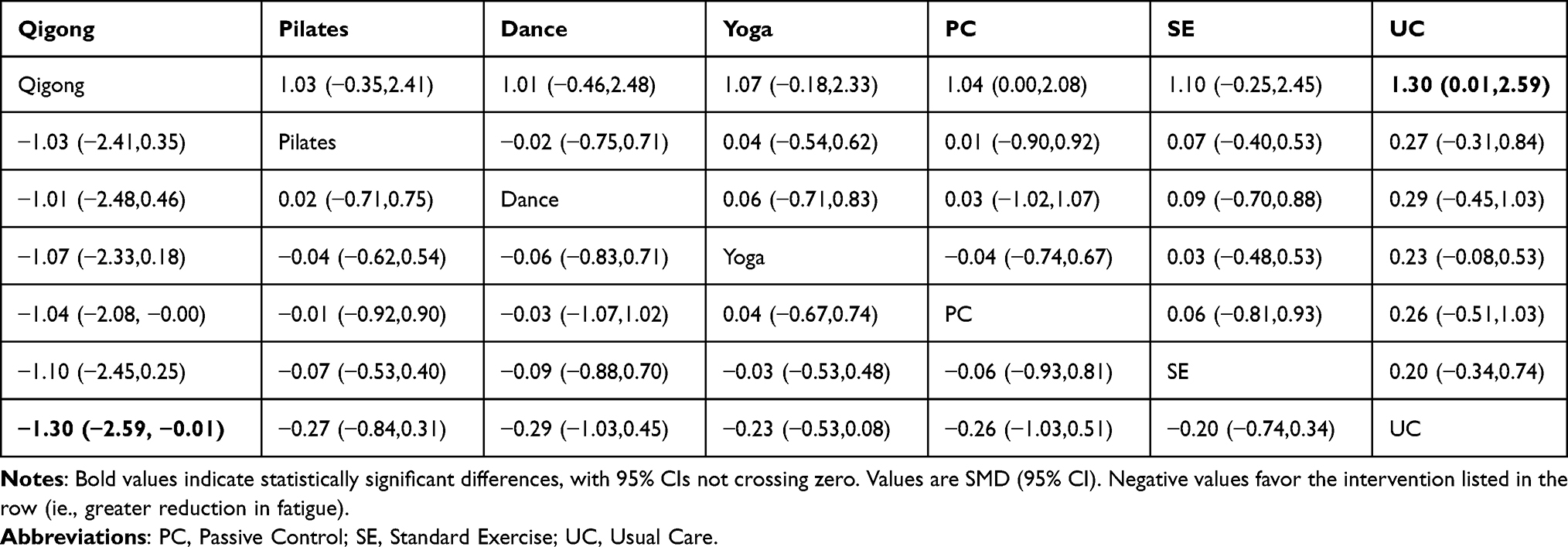 |
Table 6 League Table on Fatigue |
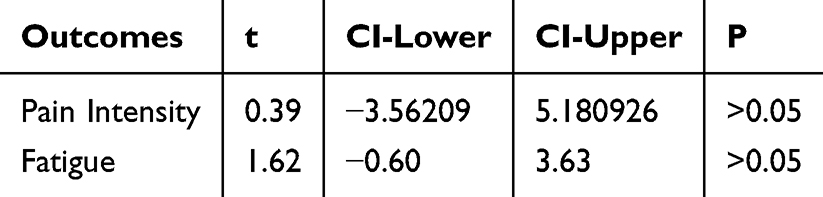 |
Table 7 The Outcomes of Egger’s Test |
Pair Comparison Meta-Analysis
For pain intensity, Qigong showed a statistically significant improvement compared with PC (1 RCT, SMD = –1.043, 95% CI: –1.991 to –0.09). In contrast, the comparison between yoga and standard exercise showed a minimal effect size near zero, with no statistically significant difference (1 RCT, SMD = 0.002, 95% CI: –0.407 to 0.41). Other direct comparisons, each informed by a single study, did not show statistically significant differences. Direct comparisons supported by two or more studies were further synthesized using pairwise meta-analysis and are presented in Table 4. Detailed results are provided in Appendix 4 and Table S4.
For fatigue, Qigong showed a significant improvement compared with PC (SMD = −2.482, 95% CI: −3.708 to −1.255). No statistically significant differences were observed for the other comparisons of interventions. The comparison of Yoga vs. PC, based on a single study, suggested an almost no effect on fatigue (SMD = 0.039, 95% CI: −0.531 to 0.609). Detailed results are also provided in in Appendix 4 and Table S5.
Network-Meta Analysis
Figure 4 presents the network plot for pain intensity, including 13 RCTs (10 two-arm RCTs and 3 three-arm RCTs). In the pain network, closed loops were present. The global inconsistency test indicated no evidence of inconsistency (χ2 = 0.39, P > 0.05), and node-splitting analyses similarly showed no significant local inconsistency across comparisons (all P > 0.05). Therefore, the consistency model was considered appropriate and was used for the primary analysis. Between-study heterogeneity was observed in the random-effects consistency model (τ = 0.45, see Appendix 3 and Table S6).
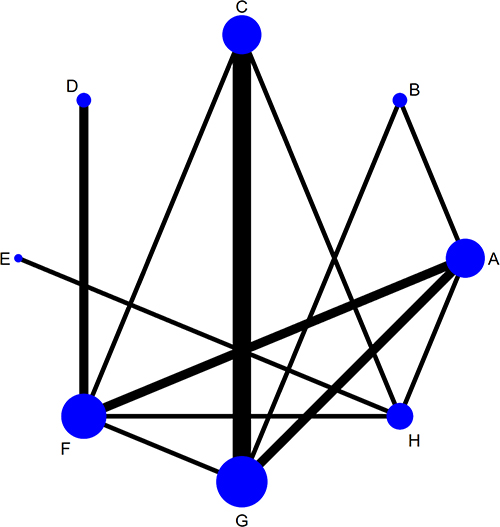 |
Figure 4 Network of evidence for pain intensity: Node size is the number of participants include each intervention, and line thickness is the number of studies contributing to each comparison. (A) Pilates, (B) Dance, (C) Yoga, (D) Taichi, (E) Qigong, (F) control group (Standard Exercise), (G) control group (Usual Care), (H) control group (Passive control). |
Figure 5 presents the network plot for fatigue. In total 9 studies were included (8 2-Arms-RCT and 1 3-Arms-RCT) and closed loops were present. The global inconsistency test suggested no inconsistency (χ2 = 0.01, P > 0.05), and node-splitting analyses showed no significant local inconsistency (all P > 0.05). Accordingly, the consistency model was adopted for the primary analysis. Between-study heterogeneity was low to moderate (τ = 0.21, see Appendix 3 and Table S6).
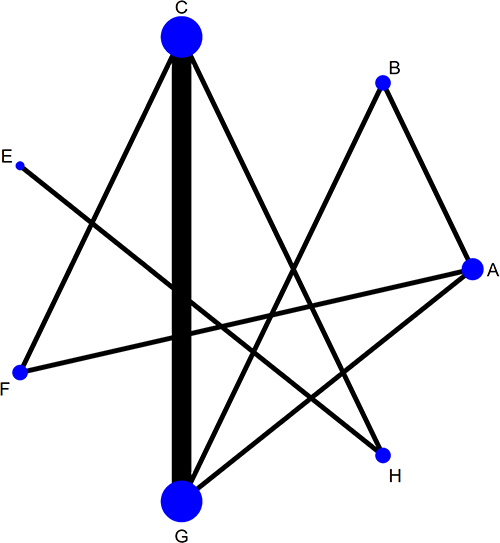 |
Figure 5 Network of evidence for cancer-related fatigue: Node sizes are proportional to the number of studies, and edge thickness reflects the number of direct comparisons; (A) Pilates, (B) Dance, (C) Yoga, (E) Qigong, (F) control group (Standard Exercise), (G) control group (Usual Care), (H) control group (Passive control). |
Pain Intensity
The league-table estimates showed that Qigong was associated with greater reductions in pain intensity than the control groups and several active interventions, including Pilates (SMD = −2.16, 95% CI: −3.90 to −0.42), Dance (SMD = −2.31, 95% CI: −4.27 to −0.35), and Yoga (SMD = −2.36, 95% CI: −4.07 to −0.64). Taichi was also associated with a greater reduction in pain intensity than SE (SMD = −1.18, 95% CI: −1.88 to −0.48). No statistically significant differences were observed in the remaining comparisons. Notably, the certainty of evidence was rated as very low for most comparisons, and only the comparison between Qigong and PC was judged as low certainty according to the GRADE system. Therefore, these findings should be interpreted with caution. Detailed results are shown in Table 5.
In the ranking analysis, Qigong had the highest SUCRA value for pain intensity (98.6%). However, given that most comparisons were supported by single trials and the certainty of evidence was predominantly very low, SUCRA rankings should be considered supportive rather than definitive (see Figure 6).
 |
Figure 6 SUCRA-based ranking probabilities of interventions for pain intensity. Abbreviations: PC, passive control; SE, Standard Exercise; UC, Usual Care. |
Fatigue
The NMA of fatigue showed that Qigong trended more favorably than UC (SMD = −1.30, 95% CI: −2.59 to −0.01). There were no statistically significant differences in other intervention-control comparisons (see in Table 6). However, these results should be interpreted with care due to the very low certainty according to GRADE. In the exploratory ranking analysis, Qigong ranked first for fatigue (94.7%) based on SUCRA; nevertheless, given the sparse evidence base and predominantly very low certainty, this ranking should be interpreted with caution. Detailed results were presented in Figure 7.
 |
Figure 7 SUCRA-based ranking probabilities of interventions for cancer-related fatigue. Abbreviations: PC, passive control; SE, Standard Exercise; UC, Usual Care. |
Sensitivity Analysis
We performed sensitivity analyses by fitting a fixed-effect model and comparing the results with those from the random-effects model. Overall, findings were generally consistent across models (see Appendix 5 Tables S7 and S8, Figures S1 and S2). In addition, because the pain etiology in Liu et al49 and Namazinia et al53 could not be clearly determined, specifically whether the pain was chemotherapy-induced neuropathic pain, we conducted a further sensitivity analysis excluding these two studies to assess the robustness of the primary results (see Appendix 5, Tables S9 and S10, Figures S3 and S4). Moreover, Namazinia et al53 used laughter yoga as the intervention, which may be considered controversial within the MBE classification. Therefore, we excluded this study alone in an additional sensitivity analysis. The findings after exclusion were largely unchanged compared to the main analysis, although the ranking of yoga in terms of treatment effectiveness changed (see Appendix 5 and Tables S12 and S13, Figures S6 and S7).
To assess the potential influence of measurement heterogeneity related to outcome scales, we performed a sensitivity analysis excluding the studies by Wang YB57 and Wang YI,58 which used the Constant-Murley pain component. Because the only Qigong study used this measure, the Qigong node was no longer estimable in the sensitivity analysis. Among the remaining interventions, Taichi showed statistically significant advantages over several comparators, and the overall pattern of results was broadly consistent with the primary analysis. The detailed results are presented in Appendix 5 Table S11 and Figure S5. The ranking of Qigong could not be verified in this sensitivity analysis.
Publication Bias
Potential publication bias was explored using comparison-adjusted funnel plots (Figures 8 and 9) and Egger’s regression test. Funnel plots suggested that most studies were symmetrically distributed around the vertical line, and clustered near the center, indicating no significant small-study effects. Consistently, Egger’s test (see in Table 7) did not detect statistically significant asymmetry for either outcome, which suggests no evidence of publication bias.
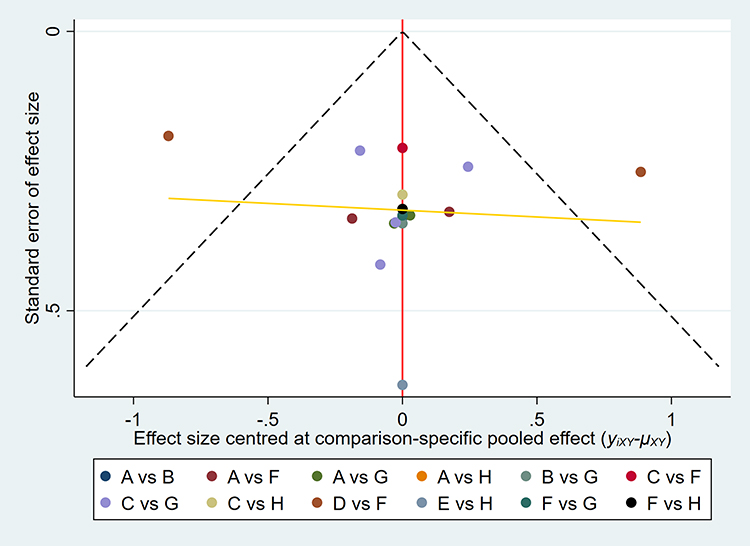 |
Figure 8 Pain Intensity: Funnel plot assessing the publication bias of the included trials. The red line represents the null hypothesis that individual study effects equal the comparison-specific pooled estimate; (A) Pilates, (B) Dance, (C) Yoga, (D) Taichi, (E) Qigong, (F) control group (Standard Exercise), (G) control group (Usual Care), (H) control group (Passive control).The red vertical line indicates the comparison-adjusted null line. The dashed lines represent the pseudo 95% confidence limits of the funnel plot. The yellow line represents the fitted regression line used to visually assess funnel plot asymmetry and potential small-study effects. |
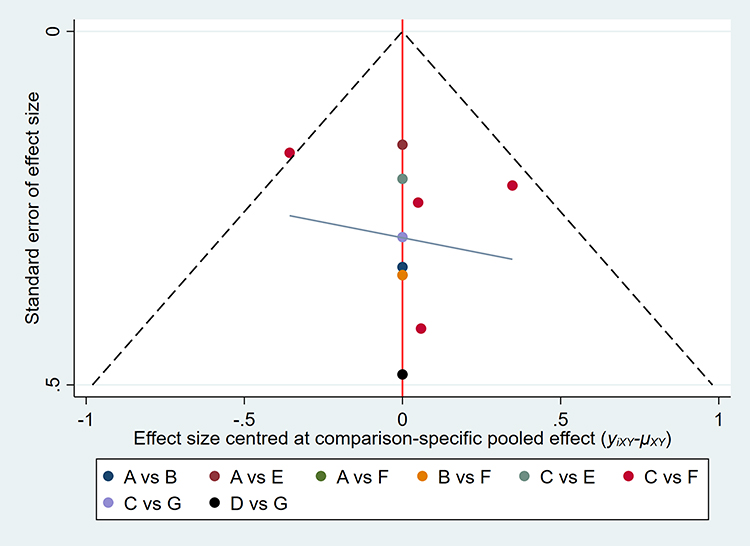 |
Figure 9 Fatigue: Funnel plot assessing the publication bias of the included trials. The red line represents the null hypothesis that individual study effects equal the comparison-specific pooled estimate; (A) Pilates, (B) Dance, (C) Yoga, (E) Qigong, (F) control group (Standard Exercise), (G) control group (Usual Care), (H) control group (Passive control). The red vertical line indicates the comparison-adjusted null line. The dashed lines represent the pseudo 95% confidence limits of the funnel plot. The grey line represents the fitted regression line used to visually assess funnel plot asymmetry and potential small-study effects. |
Discussion
Main Findings
The SUCRA suggested that Qigong showed the most favorable ranking probabilities for pain intensity and cancer-related fatigue, followed by Taichi. Furthermore, sensitivity analyses using fixed-effect models and excluding potentially problematic studies, including laughter yoga and studies with unclear pain etiology, produced broadly similar results to the primary analysis. However, because most included studies were conducted in patients with breast cancer, these findings should be interpreted primarily in the context of breast cancer populations rather than generalized to all cancer types. Additionally, the Qigong result for pain intensity was based on one study using the Constant-Murley pain component and could not be verified in sensitivity analysis. Because this measure is shoulder-specific rather than a dedicated cancer pain scale, measurement heterogeneity may have influenced the estimate. Moreover, the effect size for Qigong versus passive control was unusually large for a behavioral intervention. This may reflect single-study evidence, small sample size, sparse evidence, measurement differences, and possible overestimation rather than a stable effect. Therefore, although Qigong showed a favorable ranking, this finding should be interpreted as exploratory. In contrast, Taichi showed relatively more robust results across sensitivity analyses and may provide more stable evidence for pain relief in the current network. Taken together, the available evidence remains limited, and the comparative effectiveness estimates should be regarded as preliminary. Although no significant inconsistency was detected in either network meta-analysis, heterogeneity across trials was still observed (pain: τ = 0.45; fatigue: τ = 0.21). This heterogeneity may be attributed to clinical and methodological differences across trials, such as variations in cancer type/stage and outcome measures/scales.60 Although no significant inconsistency was detected in either network meta-analysis, heterogeneity across trials was still observed (pain: τ = 0.45; fatigue: τ = 0.21). This heterogeneity may be attributed to clinical and methodological differences across trials, such as variations in cancer type/stage and outcome measures/scales.
Effect in Different Comparisons on Pain Intensity
Although the overall network-level analyses demonstrated consistency, certain discrepancies persisted between some direct comparisons and the estimates derived from NMA. When interpreting ranking outcomes, it remains crucial to evaluate the agreement between direct head-to-head comparisons and network-derived estimates. Specifically, for the comparison of yoga versus usual care, the direction of the effect estimate obtained from pairwise meta-analysis conflicted with that from the NMA. This inconsistency may be attributable to instability in the direct comparison itself. Regarding pain intensity, the reversal in effect direction was primarily influenced by the trial conducted by Loyzet et al,50 which reported no significant benefit at 12 weeks but observed improvement at the 3-month follow-up. Prior research indicates that the benefits of yoga for pain relief may become more evident with longer practice duration; however, early low adherence among beginners, combined with variations in intervention dosage and follow-up timing across studies, could partially account for the inconsistency between short-term and follow-up effects.48,61 It should be noted, however, that the trial by Loyzet et al50 documented a high dropout rate during extended follow-up, which may undermine the robustness of the direct estimate. In contrast, provided the transitivity assumption is reasonably satisfied, NMA integrates evidence from across the entire network and can mitigate the impact of fluctuations from individual studies on the overall estimates.62,63
Effect in Different Comparisons on Fatigue
For fatigue, the observed discrepancy appears to stem from a small feasibility study in which the certainty of direct evidence was rated as very low.48 A limited sample size not only increases the variance of direct effect estimates but also reduces statistical power to detect genuine effects. Furthermore, fatigue was measured using a single item from the MPN-SAF—a scale designed for myeloproliferative neoplasms—rather than a validated multidimensional fatigue instrument. This approach may have constrained sensitivity and responsiveness, thereby diminishing the reliability of the direct evidence. Consequently, NMA—supported by a wider array of indirect comparisons—may offer a more stable indication of the overall trend of yoga on fatigue, although conclusions should still be drawn with caution.
Comparisons with External Evidences on Fatigue
Overall, the pooled effect directions for both pain intensity and fatigue were largely consistent with prior evidence, though discrepancies persisted in specific SUCRA rankings and in the classification of MBE interventions across studies. Regarding fatigue, our findings indicate that Qigong may offer benefits for cancer-related fatigue, synthesizing results from several RCTs, many of which primarily involved breast cancer survivors.64,65 It is important to note that the populations in earlier studies differed from those targeted in the present analysis, particularly in terms of cancer type and treatment setting. Consequently, these bodies of evidence should be viewed as complementary rather than directly comparable. On one hand, cancer-related fatigue is believed to share common biological and behavioral mechanisms across tumor types, and the consistent direction of effects across diverse cancer populations lends biological plausibility to our results. On the other hand, given the heterogeneity in cancer types, treatments, and symptom burden, the efficacy of Qigong for fatigue in patients with CRP should be validated through more adequately powered, high-quality RCTs specifically in this population. Taken together, our findings provide preliminary support for including Qigong as a component of a comprehensive symptom management strategy in CRP, while also highlighting the necessity for further targeted investigation.
Comparisons with External Evidences on Pain Intensity
In contrast to the fatigue outcome, the evidence base for pain intensity primarily relies on a previously published NMA focused on CRP.32 Overall, both NMAs indicate a generally consistent trend, suggesting that Qigong may offer greater benefits compared to other interventions. However, notable distinctions exist in terms of target populations, scope of interventions, classification approaches, and ranking results. Consequently, the current study should be regarded as complementing and refining the existing evidence rather than merely replicating it. It is important to note that the earlier NMA included certain patients with pain characteristics indicative of neuropathic mechanisms, such as pain associated with chemotherapy-induced peripheral neuropathy. In contrast, following relevant methodological guidelines, we deliberately excluded populations where neuropathic pain was likely to be predominant. This decision was based on the understanding that cancer pain with a predominantly neuropathic origin tends to exhibit greater heterogeneity in pathophysiology and symptom presentation, and its response to MBEs may differ from pain driven primarily by non-neuropathic mechanisms. Including populations with predominantly neuropathic pain within the same network could introduce additional heterogeneity and reduce the interpretability of treatment rankings. Therefore, our objective was to estimate relative effects within a more homogeneous clinical context.
Given this background, it is not surprising that the treatment rankings between the two studies are not entirely consistent. In the present analysis, Qigong and Taichi were ranked first and second, respectively, with Taichi estimated to be more favorable than standard exercise. In contrast, the previous NMA ranked standard exercise ahead of Taichi. Considering that SUCRA rankings are sensitive to network structure, sample size, and imprecision in effect estimates, such ranking differences likely reflect variations in population definitions and intervention classifications across studies rather than contradictory conclusions. Collectively, the previous NMA provided broader evidence across a wider definition of CRP and a more diverse range of complementary therapies, while the current study evaluated active MBEs modalities within a more narrowly defined population and intervention framework. Despite these differences, both bodies of evidence converge on a similar clinical implication: Qigong appears to be a promising option for managing symptoms in CRP, although further adequately powered head-to-head trials are warranted to strengthen comparative certainty.66
Type of Cancer-Related Pain
To offer a theoretical basis for our population selection and its potential impact on intervention outcomes, the subsequent section examines CRP through a multi-level framework derived from modern pain science. In this view, CRP is not a singular signal originating from a single site; instead, it constitutes a multidimensional brain-based experience formed by interacting layers. These layers encompass peripheral sources (such as nociceptive input from tumor invasion of bone or viscera, or direct nerve damage), spinal and supraspinal regulatory mechanisms (including central sensitization and neuro-immune-glial interactions), as well as psychological and social elements like emotional distress, sleep disruption, and pain catastrophizing.67–70
Compared to non-neuropathic cancer pain, neuropathic cancer pain is more strongly defined by persistent abnormal nerve discharges and maladaptive changes in peripheral and central neural pathways. This indicates that processes at the peripheral source level play a relatively larger role in shaping the pain experience.71,72 In nociceptive cancer pain, sustained pain and its amplification are often influenced by central regulatory mechanisms and psychosocial contributors, frequently occurring alongside inflammation, functional impairment, and behavioral factors.73,74 Although both pain phenotypes may share common downstream processes (eg., central sensitization), the proportion of “modifiable” pain attributable to central and psychosocial levels is not necessarily the same.
This may help explain why Qigong showed more evident benefits in non-neuropathic cancer pain than would be expected in predominantly neuropathic pain. Within this framework, non-pharmacological interventions may act mainly by modulating central processing and psychosocial factors, rather than reversing structural peripheral nerve damage.
The Effect of Mind-Body Exercises in Cancer-Related Pain
Although MBEs are not expected to directly reduce tumor size or repair existing nerve damage, their main effects likely involve central pain regulation and psychosocial factors. MBEs may help relieve pain by enhancing physical function, balance, and walking ability, while reducing muscle tension and abnormal biomechanical stress. They may also influence central sensitization through breath and attention regulation, emotional relief, sleep improvement, inflammation modulation, and autonomic nervous system activity.26,29,75 This suggests that the part of pain that MBEs can change may be greater in nociceptive or non-neuropathic cancer pain, where ongoing pain is more influenced by adaptive central processes and psychosocial factors.67,76 In predominantly neuropathic cancer pain, although central and psychosocial factors remain relevant, persistent abnormal nerve signals and maladaptive peripheral and central neural changes may play a larger role, potentially limiting the effects of MBEs.77–79
The aforementioned mechanistic insights offer a rationale for excluding patient populations in which neuropathic mechanisms predominantly drive cancer pain, and they aid in interpreting the observed variations in treatment efficacy rankings. From a symptom-cluster perspective, pain and fatigue may share common upstream inflammatory and neuroinflammatory pathways, providing an additional explanatory framework for the concurrent benefits of Qigong on both outcomes.
Potential Mechanisms of Traditional Chinese Mind-Body Exercises on Pain and Fatigue
A growing body of evidence indicates that CRP frequently co-occurs with cancer-related fatigue, sleep disturbances, and symptoms of depression and anxiety, forming relatively stable symptom clusters.80–83 From this viewpoint, pain and fatigue can be understood as interacting comorbid conditions that mutually influence each other.84,85 Mechanistically, cancer and its treatments can chronically activate the immune system, leading to sustained mild-to-moderate elevations in circulating proinflammatory signals such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α).86,87 These inflammatory mediators may compromise the integrity of blood–brain barrier tight junctions, increasing blood–brain barrier permeability and facilitating the transfer of peripheral inflammatory signals into the central nervous system. This process promotes microglial activation, triggers neuroinflammation, and disrupts brain networks involved in energy regulation, motivation, and affective processing.88–93 Within this framework, interventions that modulate inflammatory and neuroinflammatory pathways may simultaneously impact the pain–fatigue symptom cluster. Emerging evidence suggests that traditional Chinese MBEs may lower levels of pro-inflammatory cytokines (eg., IL-6 and TNF-α), reduce systemic inflammatory load, and potentially attenuate signaling from peripheral to central inflammatory pathways.59,94,95 Furthermore, neuroimaging studies indicate that traditional Chinese MBEs practice may decrease activation in brain regions associated with affective–cognitive pain processing, such as the cingulate cortex and insula.96,97 This downregulation may reduce the affective/cognitive amplification of pain and subsequently alleviate the subjective experience of fatigue.95,98 Therefore, Qigong and Taichi may improve both pain and fatigue through a pathway involving systemic inflammation, neuroinflammation, and modifications in brain network processing.
Strengths and Limitations
To maintain precise definitions for both interventions and target populations, we excluded trials where neuropathic pain was the predominant feature of CRP. This approach reduces heterogeneity that can arise from pooling diverse cancer pain phenotypes, a limitation present in some prior analyses. Furthermore, this study provides a systematic comparison of five prevalent MBE modalities: Taichi, Qigong, yoga, Pilates, and dance. We employed NMA to synthesize both direct and indirect evidence, enabling estimation of the relative efficacy of these interventions. A comprehensive search across multiple databases was conducted to maximize study inclusion and minimize potential selection bias. Finally, to enhance cross-study comparability and strengthen network estimates, we prioritized pain and fatigue outcome assessments closest to the 8-week time point for trials reporting data at multiple intervals.
Several limitations should be noted. First, the majority of included RCTs lacked long-term follow-up data. Consequently, our findings predominantly reflect short-term effects, and the durability of the observed benefits requires confirmation in future research. Second, although trials explicitly describing predominantly neuropathic cancer pain were excluded, most primary studies did not systematically phenotype pain using validated tools such as DN4, LANSS, or painDETECT. Thus, potential misclassification of mixed nociceptive–neuropathic pain cannot be fully excluded. Third, most included studies were conducted in patients with breast cancer, and fatigue was analyzed only as a secondary outcome within this pain-defined population. Moreover, the fatigue network was based on fewer studies than the pain network, and fatigue was not reported in all eligible trials. Therefore, the findings, particularly those for fatigue, should be generalized with caution to all cancer types or to all patients with cancer-related fatigue. Fourth, blinding of participants and personnel was generally not feasible in exercise-based interventions, contributing to risk of bias and low or very low certainty of evidence. Fifth, several intervention nodes were supported by few trials, and most direct comparisons relied on a single study. In particular, the Qigong rankings for pain and fatigue were supported by only one RCT per outcome, which may have reduced the stability of the SUCRA-based rankings. For pain intensity, the Qigong ranking was mainly based on one study using the Constant-Murley pain component. Because this measure is shoulder-specific rather than a dedicated cancer pain scale, measurement heterogeneity may have affected comparability. Moreover, the Qigong node could not be verified after excluding studies using this measure. Finally, differences in outcome scales, intervention dose, supervision level, treatment timing, cancer type, pain characteristics, and control group content may have influenced the stability of the estimates. Accordingly, the SUCRA rankings and comparative effectiveness estimates should be interpreted with caution.
Conclusion
Within the limited and mainly breast cancer–based evidence, Qigong showed the highest-ranking probabilities for pain intensity and cancer-related fatigue among patients with cancer-related pain. However, these rankings were based on single trials, a sparse network, and low- to very low-certainty evidence. Therefore, the Qigong findings should be interpreted with caution and regarded as hypothesis-generating rather than definitive evidence of clinical superiority. Taichi showed relatively more stable evidence for pain relief, although the certainty of evidence based on GRADE remained limited. Further multicenter, adequately powered RCTs with standardized pain phenotyping, validated outcome measures, and longer follow-up are warranted to confirm these findings and to further evaluate the clinical application of MBEs in cancer-related pain management.
Abbreviations
MBEs, Mind-Body Exercises; CRP, Cancer-related pain; NMA, Network meta-analysis; RCTs, Randomized controlled trials; GRADE, Grading of Recommendations Assessment, Development and Evaluation; SUCRA, Surface under the cumulative ranking curve; QoL, Quality of life; SE, Standard errors; CIs, Confidence intervals, IQRs, Interquartile ranges; SDs, Standard deviations.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its Supplementary Information Files.
Ethics Approval
This systematic review and network meta-analysis was registered in PROSPERO.
Acknowledgments
The authors thank the editor and the reviewers for their time and valuable feedback.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Open access funding was provided by the affiliated hospital of Jiujiang University and Jiujiang Key Laboratory of Modern Scientific Research on Traditional Chinese Medicine Rehabilitation Technology.
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Laversanne M, Sung H. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians. 2024;74(3):229–22. doi:10.3322/caac.21834
2. WHO. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer.
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics 2022. CA: A Cancer Journal for Clinicians. 2022;72(1):7–33. doi:10.3322/caac.21708
4. Bennett MI, Kaasa S, Barke A, Korwisi B, Rief W, Treede RD. The IASP classification of chronic pain for ICD-11: chronic cancer-related pain. Pain. 2019;160(1):38–44. doi:10.1097/j.pain.0000000000001363
5. Ragaban F, Purohit O, Del Fabbro E. Methadone in cancer-related neuropathic pain: a narrative review. Current Oncology. 2024;31(12):7613–7624. doi:10.3390/curroncol31120561
6. Mestdagh F, Steyaert A, Lavand’homme P. Cancer pain management: a narrative review of current concepts, strategies, and techniques. Current Oncology. 2023;30(7):6838–6858. doi:10.3390/curroncol30070500
7. Badger TA, Segrin C, Crane TE, et al. Social determinants of health and symptom burden during cancer treatment. Nursing Research. 2023;72(2):103–113. doi:10.1097/NNR.0000000000000636
8. Caraceni A, Shkodra M. Cancer Pain Assessment and Classification. Cancers. 2019;11(4):510. doi:10.3390/cancers11040510
9. Bernetti A, Agostini F, de Sire A, et al. Neuropathic pain and rehabilitation: a systematic review of international guidelines. Diagnostics. 2021;11(1):74. doi:10.3390/diagnostics11010074
10. Danon N, Al-Gobari M, Burnand B, Rodondi P-Y. Are mind–body therapies effective for relieving cancer-related pain in adults? A systematic review and meta-analysis. Psycho-Oncology. 2022;31(3):345–371. doi:10.1002/pon.5821
11. Brami C, Bao T, Deng G. Natural products and complementary therapies for chemotherapy-induced peripheral neuropathy: a systematic review. Critical Reviews in. Critical Reviews in Oncology/Hematology. 2016;98:325–334. doi:10.1016/j.critrevonc.2015.11.014
12. Cheung DST, Yeung WF, Chau PH, et al. Improving chemotherapy-induced peripheral neuropathy in cancer patients using a combined qigong and self-administered acupressure intervention: a randomized controlled trial. ESMO Open. 2025;10(9):105565. doi:10.1016/j.esmoop.2025.105565
13. Papadopoulou M, Stamou M, Bakalidou D, et al. Non-pharmacological interventions on pain and quality of life in chemotherapy induced polyneuropathy: systematic review and meta-analysis. In Vivo. 2023;37(1):47–56. doi:10.21873/invivo.13053
14. Häuser W, Welsch P, Radbruch L, Fisher E, Bell RF, Moore RA. Cannabis-based medicines and medical cannabis for adults with cancer pain. The Cochrane Database of Systematic Reviews. 2023;6(6):Cd014915. doi:10.1002/14651858.CD014915.pub2
15. Kistemaker KRJ, Sijani F, Brinkman DJ, et al. Pharmacological prevention and treatment of opioid-induced constipation in cancer patients: a systematic review and meta-analysis. Cancer Treatment Reviews. 2024;125:102704. doi:10.1016/j.ctrv.2024.102704
16. Chung M, Kim HK, Abdi S. Update on cannabis and cannabinoids for cancer pain. Current Opinion in Anaesthesiology. 2020;33(6):825–831. doi:10.1097/ACO.0000000000000934
17. Lawson McLean A, Kahr J, Régis J, Kamp MA, Senft C. Epidemiology of resistant cancer pain: prevalence, clinical burden, and treatment gaps. Stereotactic and Functional Neurosurgery. 2025;2025:1–13.
18. Bhargav H, Vidyasagar PD, Venugopal S, et al. Development, validation, and feasibility testing of a yoga module for opioid use disorder. Advances in Mind-Body Medicine. 2021;35(3):20–30.
19. Teng Y, Tao S, Chen J, et al. Tai Chi’s synergistic modulation on autonomic nervous activity and central autonomic networks in functional constipation patients: a randomized controlled trial. Scientific Reports. 2025;15(1):23560. doi:10.1038/s41598-025-04088-z
20. Hale FB, Harris AL. Understanding the health benefits of tai chi practice for managing pain after breast cancer treatment. Nursing for Women’s Health. 2025;29(3):200–204. doi:10.1016/j.nwh.2024.11.004
21. Zhang X, Zong B, Zhao W, Li L. Effects of Mind-Body Exercise on Brain Structure and Function: a Systematic Review on MRI Studies. Brain Sciences. 2021;11(2):205. doi:10.3390/brainsci11020205
22. Calapai F, Mondello E, Mannucci C, et al. Pain biomarkers in cancer: an overview. Current Pharmaceutical Design. 2021;27(2):293–304. doi:10.2174/1381612826666201102103520
23. Xu T, Wang J, Wu Y, et al. Ac4C Enhances the translation efficiency of vegfa mRNA and mediates central sensitization in spinal dorsal horn in neuropathic pain. Advanced Science. 2023;10(35):e2303113. doi:10.1002/advs.202303113
24. Wei P, Liu Y, Tong J, Zhang Q, Qiu Z, Xu X. Advances in neuroimaging of breast cancer pain: an overview. Journal of Pain Research. 2025;18:4975–4988. doi:10.2147/JPR.S540502
25. Thong MSY, van Noorden CJF, Steindorf K, Arndt V. Cancer-related fatigue: causes and current treatment options. Current Treatment Options in Oncology. 2020;21(2):17. doi:10.1007/s11864-020-0707-5
26. Medeiros Torres D, Jorge Koifman R, da Silva Santos S. Impact on fatigue of different types of physical exercise during adjuvant chemotherapy and radiotherapy in breast cancer: systematic review and meta-analysis. Support Care Cancer. 2022;30(6):4651–4662. doi:10.1007/s00520-022-06809-w
27. Craft LL, Perna FM. The benefits of exercise for the clinically depressed. Primary Care Companion to. The Journal of Clinical Psychiatry. 2004;6(3):104–111.
28. O’Higgins CM, Brady B, O’Connor B, Walsh D, Reilly RB. The pathophysiology of cancer-related fatigue: current controversies. Supportive Care in. Cancer. 2018;26(10):3353–3364.
29. van Dam K. Individual Stress Prevention through Qigong. International Journal of Environmenta lResearch and Ppublic Health. 2020;17(19):7342.
30. Sun F, Li L, Wen X, Xue Y, Yin J. The effect of tai chi/qigong on depression and anxiety symptoms in adults with cancer: a systematic review and meta-regression. Complement Ther Clin Pract. 2024;56:101850. doi:10.1016/j.ctcp.2024.101850
31. Sun J, Chen D, Qin C, Liu R. The effect of mind-body exercise in lung cancer patients: a meta-analysis of RCTs. Supportive Care in Cancer. 2023;31(12):650. doi:10.1007/s00520-023-08092-9
32. He X, Liang G, Zou Z, et al. What are the optimal mind-body therapies for cancer-related pain? A network meta-analysis. Translational Exercise Biomedicine. 2025;2(2):105–127. doi:10.1515/teb-2025-0009
33. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:1.
34. Shi J, Hu Z-Y, Wen Y-R, et al. Optimal modes of mind-body exercise for treating chronic non-specific low back pain: systematic review and network meta-analysis. Frontiers in Neuroscience. 2022;16:1046518. doi:10.3389/fnins.2022.1046518
35. Wang J, Lv M, Li H, Guo D, Chu X. Effects of Exercise in Adults With Cancer Pain: a Systematic Review and Network Meta-Analysis. Journal of Pain and Symptom Management. 2025;69(1):82–101. doi:10.1016/j.jpainsymman.2024.08.033
36. Yoon SY, Oh J. Neuropathic cancer pain: prevalence, pathophysiology, and management. The Korean Journal of Internal Medicine. 2018;33(6):1058–1069. doi:10.3904/kjim.2018.162
37. Zhu Y, Zhang Z, Du Z, Zhai F. Mind-body exercise for patients with stable COPD on lung function and exercise capacity: a systematic review and meta-analysis of RCTs. Scientific Reports. 2024;14(1):18300. doi:10.1038/s41598-024-69394-4
38. Zhou X, Yang Y, Zhai L, Gan J, Li C, Zhu Y. Comparative efficacy of different exercise therapies for cardiorespiratory fitness in breast cancer survivors: a systematic review and Bayesian network meta-analysis. Sports Medicine - Open. 2025;11(1):67. doi:10.1186/s40798-025-00872-3
39. Higgins JP, Li T, Deeks JJ. Chapter 6: choosing effect measures and computing estimates of effect. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.5. Cochrane; 2024. Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook/current/chapter-06#section-6-2-7.
40. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. The Lancet. 2018;391(10128):1357–1366. doi:10.1016/S0140-6736(17)32802-7
41. Cheng Y-C, Huang W-L, Chen W-Y, Huang Y-C, Kuo P-H, Tu Y-K. Comparative efficacy and tolerability of nutraceuticals for depressive disorder: a systematic review and network meta-analysis. Psychological Medicine. 2025;55:e134. doi:10.1017/S0033291725000996
42. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
43. Feliciano JL, Waldfogel JM, Sharma R, et al. Pharmacologic interventions for breathlessness in patients with advanced cancer: a systematic review and meta-analysis. JAMA Network Open. 2021;4(2):e2037632. doi:10.1001/jamanetworkopen.2020.37632
44. Higgins JP, Li T. Chapter 6: choosing effect measures and computing estimates of effect. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, ea PMJ, editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.5. Cochrane; 2024. Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook/current/chapter-06#section-6-1.
45. Alpozgen AZ, Ozdincler AR, Karanlik H, Agaoglu FY, Narin AN. Effectiveness of Pilates-based exercises on upper extremity disorders related with breast cancer treatment. European Journal of Cancer Care. 2017;26(6):8.
46. Barbosa KP, da Silva LGT, Garcia PA, et al. Effectiveness of Pilates and circuit-based exercise in reducing arthralgia in women during hormone therapy for breast cancer: a randomized, controlled trial. Support Care Cancer. 2021;29(10):
47. Boing L, Fretta TB, Lynch BM, et al. Mat Pilates and belly dance: effects on patient-reported outcomes among breast cancer survivors receiving hormone therapy and adherence to exercise. Complementary Therapies in Clinical Practice. 2023;50:101683. doi:10.1016/j.ctcp.2022.101683
48. Huberty J, Eckert R, Dueck A, et al. Online yoga in myeloproliferative neoplasm patients: results of a randomized pilot trial to inform future research. BMC Complementary and Alternative Medicine. 2019;19(1):121. doi:10.1186/s12906-019-2530-8
49. Liu W, Liu J, Ma L, Chen J. Effect of mindfulness yoga on anxiety and depression in early breast cancer patients received adjuvant chemotherapy: a randomized clinical trial. Journal of Cancer Research and Clinical Oncology. 2022;148(9):
50. Lotzke D, Wiedemann F, Rodrigues Recchia D, et al. Iyengar-yoga compared to exercise as a therapeutic intervention during (neo)adjuvant therapy in women with stage I-III breast cancer: health-related quality of life, Mindfulness, spirituality, life satisfaction, and cancer-related fatigue. Evidence-Based Complementary and Alternative Medicine. 2016;2016. doi:10.1155/2016/5931816
51. Loudon A, Barnett T, Piller N, Immink MA, Williams AD. Yoga management of breast cancer-related lymphoedema: a randomised controlled pilot-trial. BMC Complementary and Alternative Medicine. 2014;14:214. doi:10.1186/1472-6882-14-214
52. Jiang M, Zhao H, Liu J, Zhao X, Jin L, Pan R. Does Tai Chi improve antioxidant and anti-inflammatory abilities via the KEAP1-NRF2 pathway and increase blood oxygen level in lung cancer patients: a randomized controlled trial? European Journal of Integrative Medicine. 2020;37:101161. doi:10.1016/j.eujim.2020.101161
53. Namazinia M, Mazlum SR, Mohajer S, Lopez V. Effects of laughter yoga on health-related quality of life in cancer patients undergoing chemotherapy: a randomized clinical trial. BMC Complementary and Alternative Medicine. 2023;23(1):192. doi:10.1186/s12906-023-04028-2
54. Eyigor S, Uslu R, Apaydın S, Caramat I, Yesil H. Can yoga have any effect on shoulder and arm pain and quality of life in patients with breast cancer? A randomized, controlled, single-blind trial. Complementary Therapies in Clinical Practice. 2018;32:40–45. doi:10.1016/j.ctcp.2018.04.010
55. Torres DM, Fireman KD, Fabro EAN, et al. Effectiveness of mat pilates on fatigue in women with breast cancer submitted to adjuvant radiotherapy: randomized controlled clinical trial. Support Care Cancer. 2023;31(6):11.
56. Vadiraja HS, Rao RM, Hongasandra NR, Nagarathna R, Rekha M, Vanitha N. Effects of yoga on symptom management in breast cancer patients: a randomized controlled trial. International Journal of Yoga. 2009;2(2):
57. Wang YB, Cheng ZG, Zhang L, et al. Intervention effects of Baduanjin and fancy diabolo on postoperative breast cancer patients. Journal of Hebei North University. 2022;38(2):16–19.
58. Wang YL, Sun XY, Wang YB, et al. Effects of tai chi exercise on postoperative upper-limb function and quality of life in patients with breast cancer. China Sport Science and Technology. 2010;5:125–128.
59. Zeng Y, Luo T, Xie H, Huang M, Cheng ASK. Health benefits of qigong or tai chi for cancer patients: a systematic review and meta-analyses. Complementary Therapies in. Medicine. 2014;22(1):173–186.
60. Mbuagbaw L, Rochwerg B, Jaeschke R, et al. Approaches to interpreting and choosing the best treatments in network meta-analyses. Systematic Reviews. 2017;6(1):79. doi:10.1186/s13643-017-0473-z
61. Bower JE, Garet D, Sternlieb B, et al. Yoga for persistent fatigue in breast cancer survivors: a randomized controlled trial. Cancer. 2012;118(15):3766–3775. doi:10.1002/cncr.26702
62. Lin L, Xing A, Kofler MJ, Murad MH. Borrowing of strength from indirect evidence in 40 network meta-analyses. Journal of Clinical Epidemiology. 2019;106:41–49. doi:10.1016/j.jclinepi.2018.10.007
63. Chaimani A, Caldwell DM, Li T, Higgins JP, S G. Chapter 11: undertaking network meta-analyses In: Higgins TJ, Chandler J, Cumpston M, et al. editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.5. Cochrane; 2024: Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook/current/chapter-11?utm_source=chatgpt.com#section-11-2-3.
64. Ee C, Kay S, Reynolds A, Lovato N, Lacey J, Koczwara B. Lifestyle and integrative oncology interventions for cancer-related fatigue and sleep disturbances. Maturitas. 2024;187:108056. doi:10.1016/j.maturitas.2024.108056
65. Tan TW, Hsu MF, Chung YC. Effects of Qigong on Cancer-Related Fatigue, Sleep Disturbance, Cognitive Impairment, and Quality of Life in Breast Cancer Survivors: a Systematic Literature Review and Meta-Analysis. The Journal of. Nursing. 2024;71(6):72–82.
66. Meng T, Hu SF, Cheng YQ, et al. Qigong for women with breast cancer: an updated systematic review and meta-analysis. Complementary Therapies in. Medicine. 2021;60:102743.
67. Mulvey MR, Paley CA, Schuberth A, King N, Page A, Neoh K. Neuropathic pain in cancer: what are the current guidelines? Current Treatment Options in. Oncology. 2024;25(9):1193–1202. doi:10.1007/s11864-024-01248-7
68. Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron. 2006;52(1):77–92. doi:10.1016/j.neuron.2006.09.021
69. Donnelly CR, Andriessen AS, Chen G, et al. Central nervous system targets: glial cell mechanisms in chronic pain. Neurotherapeutics. 2020;17(3):846–860. doi:10.1007/s13311-020-00905-7
70. Wang WL, Hao YH, Pang X, Tang YL. Cancer pain: molecular mechanisms and management. Molecular Biomedicine. 2025;6(1):45. doi:10.1186/s43556-025-00289-0
71. Devor M. Neuropathic pain and injured nerve: peripheral mechanisms. British Medical Bulletin. 1991;47(3):619–630. doi:10.1093/oxfordjournals.bmb.a072496
72. Kocot-Kępska M, Zajączkowska R, Mika J, Wordliczek J, Dobrogowski J, Przeklasa-Muszyńska A. Peripheral mechanisms of neuropathic pain—the role of neuronal and non-neuronal interactions and their implications for topical treatment of neuropathic pain. Pharmaceuticals. 2021;14(2):77. doi:10.3390/ph14020077
73. Nishigami T, Manfuku M, Lahousse A. Central sensitization in cancer survivors and its clinical implications: state of the art. Journal of Clinical Medicine. 2023;12(14):4606. doi:10.3390/jcm12144606
74. Cao B, Xu Q, Shi Y, et al. Pathology of pain and its implications for therapeutic interventions. Signal Transduction and Targeted Therapy. 2024;9(1):155. doi:10.1038/s41392-024-01845-w
75. Ficarra S, Thomas E, Bianco A, et al. Impact of exercise interventions on physical fitness in breast cancer patients and survivors: a systematic review. Breast Cancer. 2022;29(3):402–418. doi:10.1007/s12282-022-01347-z
76. Lozano-Ondoua AN, Symons-Liguori AM, Vanderah TW. Cancer-induced bone pain: mechanisms and models. Neuroscience Letters. 2013;557:52–59. doi:10.1016/j.neulet.2013.08.003
77. Huang Y, Tan T, Liu L, et al. Exercise for reducing chemotherapy-induced peripheral neuropathy: a systematic review and meta-analysis of randomized controlled trials. Frontiers in Neurology. 2023;14:1252259. doi:10.3389/fneur.2023.1252259
78. Wayne PM, Lee M, Novakowski J, et al. Tai Chi and Qigong for cancer-related symptoms and quality of life: a systematic review and meta-analysis. Journal of Cancer Survivorship. 2018;12(2):256–267. doi:10.1007/s11764-017-0665-5
79. Vieira WF, Real CC, Martins DO, Chacur MJC. The role of exercise on glial cell activity in neuropathic pain management. Cells. 2025;14(7):487. doi:10.3390/cells14070487
80. Miaskowski C, Barsevick A, Berger A, et al. Advancing symptom science through symptom cluster research. Expert Panel Proceedings and Recommendations. Journal of the National Cancer Institute. 2017;109(4):djw253. doi:10.1093/jnci/djw253
81. Bjerkeset E, Röhrl K, Schou-Bredal I. Symptom cluster of pain, fatigue, and psychological distress in breast cancer survivors: prevalence and characteristics. Breast Cancer Research and Treatment. 2020;180(1):63–71. doi:10.1007/s10549-020-05522-8
82. Theobald DE. Cancer pain, fatigue, distress, and insomnia in cancer patients. Clinical Cornerstone. 2004;6(Suppl 1D):S15–21. doi:10.1016/S1098-3597(05)80003-1
83. Knefel M, Zeilinger EL, Erfurth A, et al. Affective temperament, fatigue, and pain in cancer patients. Journal of Affective Disorders. 2023;340:80–87. doi:10.1016/j.jad.2023.08.003
84. He X, Msn N, Choi KC, Wkw S. Effects of a 16-week dance intervention on the symptom cluster of fatigue-sleep disturbance-depression and quality of life among patients with breast cancer undergoing adjuvant chemotherapy: a randomized controlled trial. International Journal of Nursing Studies. 2022;133:104317. doi:10.1016/j.ijnurstu.2022.104317
85. Lahousse A, Ivakhnov S, Nijs Ph DJ, et al. The mediating effect of perceived injustice and pain catastrophizing in the relationship of pain on fatigue and sleep in breast cancer survivors: a cross-Sectional study. Pain Medicine. 2022;23(7):1299–1310. doi:10.1093/pm/pnac006
86. Xiao C, Peng G, Conneely KN, et al. DNA methylation profiles of cancer-related fatigue associated with markers of inflammation and immunometabolism. Molecular Psychiatry. 2025;30(1):76–83. doi:10.1038/s41380-024-02652-z
87. Laird BJA, Scott AC, Colvin LA, et al. Cancer pain and its relationship to systemic inflammation: an exploratory study. Pain. 2011;152(2):460–463. doi:10.1016/j.pain.2010.10.035
88. Galvis D, Zavala E, Walker JJ, et al. Modelling the dynamic interaction of systemic inflammation and the hypothalamic-pituitary-adrenal (HPA) axis during and after cardiac surgery. Journal of the Royal Society. 2022;19(189):20210925.
89. Smith AM, Leeming A, Fang Z, et al. Mindfulness-based stress reduction alters brain activity for breast cancer survivors with chronic neuropathic pain: preliminary evidence from resting-state fMRI. Journal of Cancer Survivorship. 2021;15(4):518–525. doi:10.1007/s11764-020-00945-0
90. Lin WY, Hsieh JC, Lu CC, Ono Y. Altered metabolic connectivity between the amygdala and default mode network is related to pain perception in patients with cancer. Scientific Reports. 2022;12(1):14105. doi:10.1038/s41598-022-18430-2
91. Zhou X, Tan Y, Chen J, et al. Altered functional connectivity in pain-related brainregions and its correlation with pain duration in bone metastasis with cancer pain. Disease Markers. 2022;2022:3044186. doi:10.1155/2022/3044186
92. Vande Vyvere T, De Groote A, De Groef A, et al. Morphological and functional brain changes in chronic cancer-related pain: a systematic review. The Anatomical Record. 2024;307(2):285–297. doi:10.1002/ar.25113
93. Bower JE. The role of neuro-immune interactions in cancer-related fatigue: biobehavioral risk factors and mechanisms. Cancer. 2019;125(3):353–364. doi:10.1002/cncr.31790
94. Alvarenga-Filho H, Sacramento PM, Ferreira TB, et al. Combined exercise training reduces fatigue and modulates the cytokine profile of T-cells from multiple sclerosis patients in response to neuromediators. Journal of Neuroimmunology. 2016;293:91–99. doi:10.1016/j.jneuroim.2016.02.014
95. Irwin MR, Hoang D, Olmstead R, et al. Tai Chi compared with cognitive behavioral therapy and the reversal of systemic, cellular and genomic markers of inflammation in breast cancer survivors with insomnia: a randomized clinical trial. Brain, Behavior, and Immunity. 2024;120:159–166. doi:10.1016/j.bbi.2024.05.022
96. Shen C-L, Watkins BA, Kahathuduwa C, et al. Tai chi improves brain functional connectivity and plasma lysophosphatidylcholines in postmenopausal women with knee osteoarthritis: an exploratory pilot study. Frontiers in Medicine. 2022;8:775344. doi:10.3389/fmed.2021.775344
97. Du Y, Gao Y, Wu G, et al. Exploration of the relationship between hippocampus and immune system in schizophrenia based on immune infiltration analysis. Frontiers in Immunology. 2022;13:878997. doi:10.3389/fimmu.2022.878997
98. Yu WL, Li XQ, Tang WJ, Li Y, Weng XC, Chen YZ. fMRI study of pain reaction in the brain under state of “Qigong”. The American Journal of Chinese Medicine. 2007;35(6):937–945. doi:10.1142/S0192415X07005405
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.