Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Comparative Analysis of the Average Recommendation Time for the Incorporation of Biological Drugs for Cancer and Rheumatoid Arthritis
Authors Natividade MSD ![]() , Soares Lisboa E, Aragão E, de Castro CT
, Soares Lisboa E, Aragão E, de Castro CT ![]() , Damasceno de Barros R
, Damasceno de Barros R ![]() , Pereira M, Silva Miranda S, Souza LE, Almeida-Filho ND
, Pereira M, Silva Miranda S, Souza LE, Almeida-Filho ND
Received 3 April 2025
Accepted for publication 30 January 2026
Published 28 April 2026 Volume 2026:19 532154
DOI https://doi.org/10.2147/JMDH.S532154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David C. Mohr
Marcio Santos da Natividade,1 Erick Soares Lisboa,1 Erika Aragão,1 Caroline Tianeze de Castro,1 Rafael Damasceno de Barros,2 Marcos Pereira,1 Samilly Silva Miranda,1 Luís Eugênio Souza,1 Naomar de Almeida-Filho1
1Institute of Collective Health, Federal University of Bahia, Salvador, Bahia, Brazil; 2School of Nursing, Federal University of Bahia, Salvador, Bahia, Brazil
Correspondence: Marcio Santos da Natividade, Institute of Collective Health, Federal University of Bahia, Basílio da Gama Street, No Number, Canela Campus, Salvador, Bahia, 40.110-040, Brazil, Email [email protected]
Purpose: To compare the average time between the registration of a biological drug and its recommendation for incorporation for rheumatoid arthritis (RA) and cancer (CA) at national and international levels.
Methods: This retrospective, comparative study analyzed the time taken to incorporate biological drugs recommended by National Commission for the Incorporation of Technologies (CONITEC) in the Brazilian Unified Health System(SUS) for RA and CA from January 1, 2012, to March 28, 2024. The incorporation time in Brazil was compared to that of regulatory bodies in England and Australia for the same treatments. Kaplan-Meier curves and the Log rank test were used to estimate time differences between countries.
Results: In Brazil, biological drugs for RA took an average of 2,019 days from the National Health Surveillance Agency (ANVISA) approval to CONITEC’s incorporation recommendation. In England, the averages were 1,242 days for RA and 1,683 for CA, while in Australia, it was 744 days for RA and 1,315 for CA. Australia incorporated drugs faster than both England and Brazil.
Conclusion: The lengthy process in Brazil for incorporating biological technologies for RA and CA may hinder access, delaying treatment for many patients. This barrier is particularly significant for low-income individuals who rely exclusively on the SUS.
Keywords: national organizations in science and technology, health technology assessment, HTA, cancer, rheumatoid arthritis, unified health system, brazilian national commission for the incorporation of technologies, CONITEC
Introduction
The practice of Health Technology Assessment (HTA) emerged as a field of knowledge in the United States at the end of the 1970s, and its development as a scientific practice and part of health policy took place mainly in Europe, Australia, North America, and later in some developing countries.1
Health technology assessment and incorporation processes are not uniform across countries. Although there are some similarities in the foundations of public health systems, decision-making depends on, among other things, the level of evidence and the experience of the actors. In the search for efficacy, safety and cost-effectiveness, the time elapsed between the registration of a drug and its incorporation into the public system is a critical factor, as it can affect patients’ access to innovative treatments, especially for serious or chronic diseases, where delays can affect health and quality of life.1,2
HTA in Brazil, as an institutional practice, is essentially linked to the Unified Health System (in Portuguese: Sistema Único de Saúde – SUS), through initiatives of the Ministry of Health to promote the use of scientific evidence in the decision-making process for the incorporation of health technologies. In this sense, the National Commission for the Incorporation of Technologies in the SUS (in Portuguese: Comissão Nacional de Incorporação de Tecnologias no Sistema Único de Saúde – CONITEC) was created in 2011, with the function of supporting the Ministry of Health in decisions to incorporate technologies.1,3
The inclusion in the SUS of safe and effective medicines with an appropriate cost-effectiveness ratio expands access to these technologies, especially those with high added value, such as biopharmaceuticals. However, despite the progress made in the incorporation of biological medicines into the SUS, most of them have not been incorporated and are the subject of legal proceedings. The incorporation process can reduce the costs of the public health system by avoiding complications and hospitalizations, and promote the financial sustainability of the system.3–5
Rheumatoid arthritis (RA) and cancer (CA) are two of the diseases with the highest patient demand for biological medicines.6 Regarding RA, a chronic inflammatory disease that affects about 1% of the world’s population and about 0.3% of the Brazilian population, spending on biological drugs increased from R$1.4 billion in 2012 to R$1.9 billion in 2016, which shows the high cost of this technology.7–9 As for CA, it is the second leading cause of death by disease in Brazil, with an estimated 704,000 new cases of this disease in the country for the three-year period 2023–2025. Various treatments have been used for CA, including biological drugs such as monoclonal antibodies. The high cost of these biotechnologies has a significant economic impact on the SUS, especially through litigation.10,11 In this sense, the SUS faces major challenges in acquiring and making available pharmaceutical biotechnologies, especially for RA and CA. Understanding the time it takes for these technologies to be incorporated into the SUS is fundamental to ensure the integrality of the system in an equitable manner and to address health inequalities. Therefore, the aim of this study is to compare the average times between registration of a biological drug and recommendation for its incorporation for RA and CA at national and international levels.
Materials and Methods
This is a retrospective and comparative study of the time taken to incorporate the biological drugs recommended by CONITEC for RA and AC, from January 1, 2012 to March 28, 2024. The time taken in Brazil was compared with the time taken by the regulatory and drug incorporation bodies of the health systems in England and Australia to incorporate the same drugs for RA and CA.
To verify the time taken, the date of approval by ANVISA was taken into account, by consulting the drug registers on its website, and the date of publication by CONITEC of the regulation recommending the incorporation of the drug into the SUS, identified in each technical recommendation report, available on its website (Table 1).
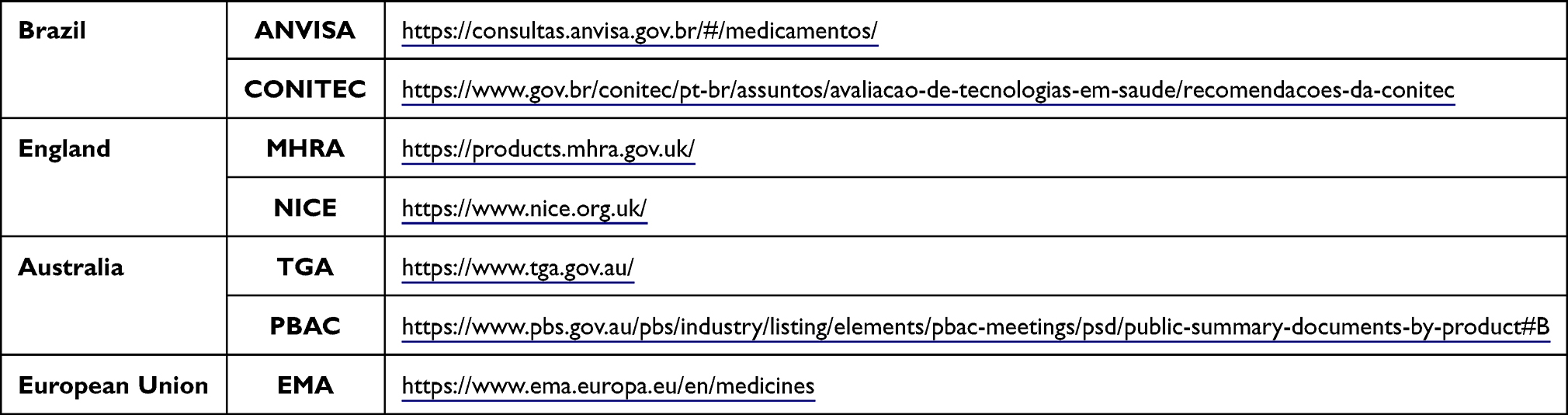 |
Table 1 Websites Consulted to Obtain Approval and Incorporation Dates for Oncology and Rheumatoid Arthritis Drugs |
Considering the same drugs consulted in Brazil, the time taken in England and Australia was verified for comparison purposes. These countries were chosen because they have public health systems that, like the SUS, provide universal services and are also references in the field of HTA, even cited by CONITEC in its recommendation reports.
For the Australian system, the date of approval of the drug’s registration by the Therapeutic Goods Administration (TGA) and the date of publication of the recommendation for incorporation into the public health system by the Pharmaceutical Benefits Advisory Committee (PBAC) were verified by consulting public documents on their respective websites (Table 1).
For England, data were collected from two regulatory agencies. The first was the European Medicines Agency (EMA), for drug registrations approved up to 2020, as the country was previously part of the European Union. The second agency was the UK’s Medicines & Healthcare Products Regulatory Agency (MHRA), which was consulted for drugs approved from 2021, after Brexit. Documents from the National Institute for Health and Care Excellence (NICE) were consulted to verify the publication date of the recommendation for incorporation into the UK public health system (Table 1).
Means, medians, minimums, maximums, and 1st and 3rd quartiles were calculated to analyze the data and estimate the time from approval of registration to recommendation for incorporation of the drugs. In addition, Kaplan-Meier curves and the Log rank test were used to estimate time differences between countries. All analyses were stratified by disease, and the analyses were performed using the R statistical program, version 4.3.2.
Results
During the period analyzed, CONITEC recommended the incorporation of 32 biological drugs for the treatment of RA and various types of CA, of which 11 (34.4%) were for RA and 21 (65.6%) for CA. Of the 32 incorporations analyzed, 26 different drugs were identified.
Australia consistently demonstrated the fastest incorporation of new drugs for both RA (744 ± 1,060 days) and CA (1,315 ± 1,333 days). England followed with a moderate pace (RA: 1,242 ± 1,246; CA: 1,683 ± 1,463), while Brazil experienced the longest delays, particularly in CA treatments (RA: 2,019 ± 1,757; CA: 3,898 ± 2,430). Overall, cancer drugs tend to take longer to integrate across all countries compared to rheumatoid arthritis treatments (Table 2 and Figure 1).
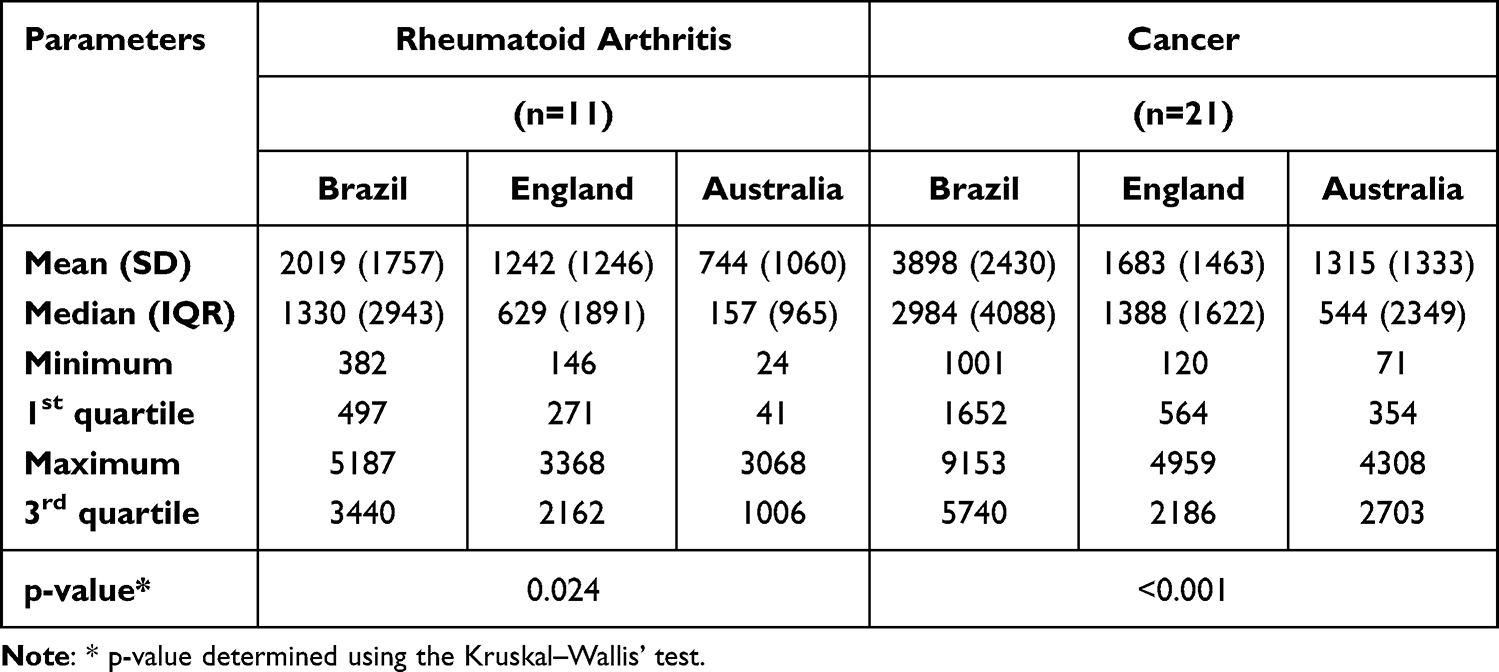 |
Table 2 Time Elapsed Between Regulatory Approval of Biological Drugs and Recommendation for Incorporation Into the Public Health System of Technologies for Rheumatoid Arthritis and Cancer (in Days), Brazil, England, and Australia |
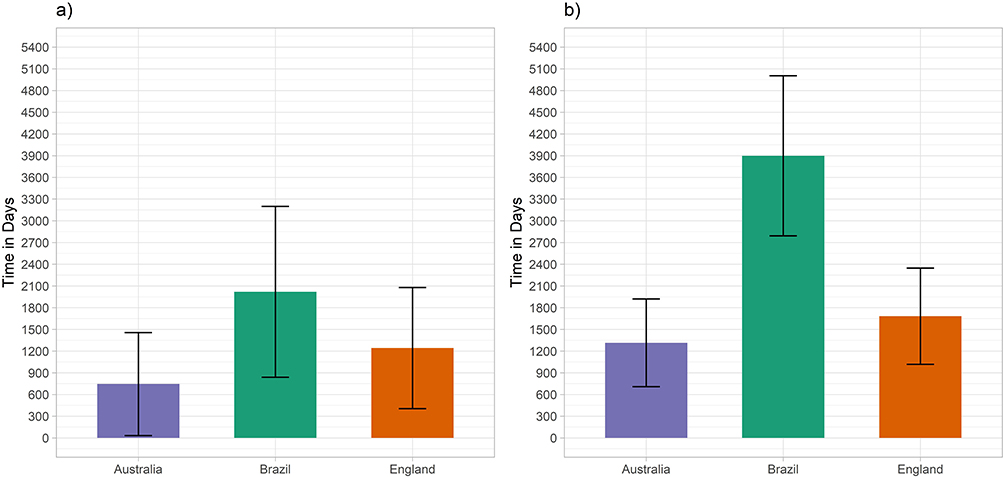 |
Figure 1 Drug incorporation timelines for (a) rheumatoid arthritis and (b) cancer in Brazil, England, and Australia. |
In the context of RA treatment, Australia demonstrated shorter incorporation timelines for nearly all drugs, with tofacitinib being incorporated the fastest. England showed slightly slower incorporation than Australia but generally followed a similar pattern, with certolizumab pegol being the quickest to be incorporated. Brazil experienced the slowest incorporation across all drugs, with rituximab having notably longer wait times (Figure 2a). Regarding CA treatment, Australia again exhibited quicker timelines for most drugs, particularly brentuximab vedotin. England displayed variable incorporation times, with ribociclib being the fastest incorporated drug. Brazil faced significant delays, especially with rituximab and trastuzumab (Figure 2b).
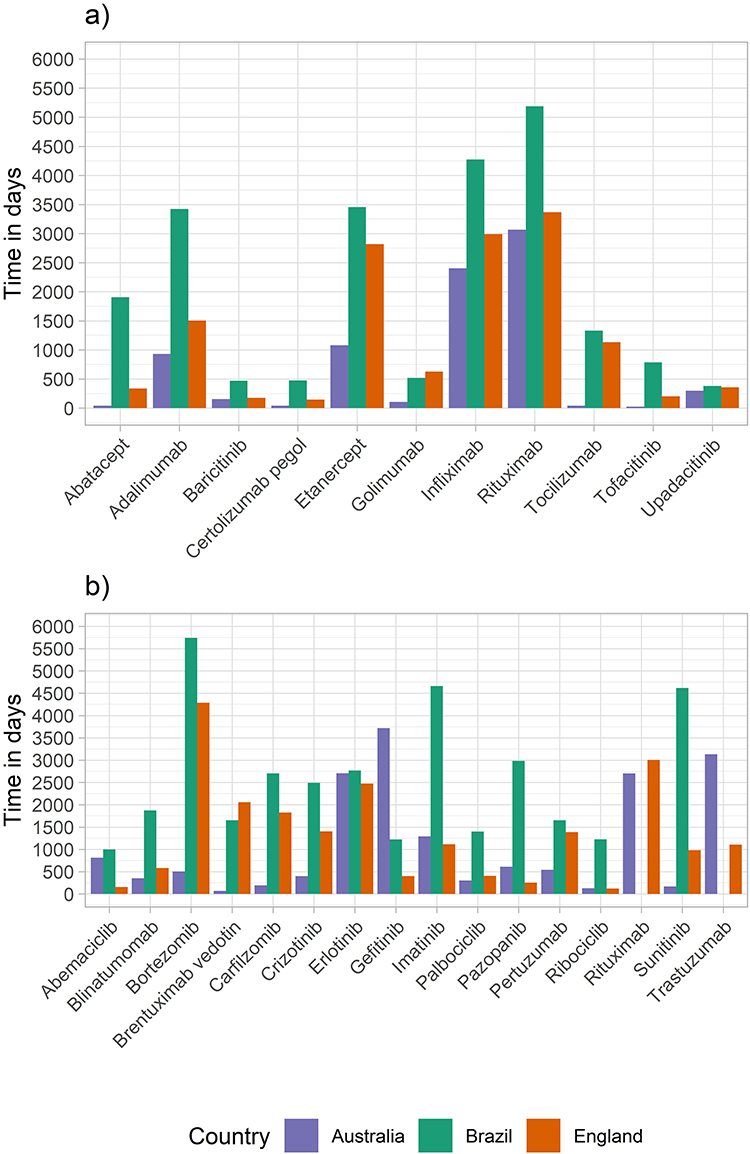 |
Figure 2 Drug incorporation timelines for (a) rheumatoid arthritis and (b) cancer in Brazil, England, and Australia, by drug. |
Figure 3 shows the number of days that elapsed between the approval of the drugs’ registration and the publication of the recommendation for their incorporation in each country. Overall, Australia issued recommendations for incorporation more quickly than England and Brazil (Figure 3a). The same pattern is observed in the analyses stratified by disease type, where there is a greater disparity in the time taken to incorporate oncology drugs between countries, with a significantly longer incorporation time for Brazil (Figure 3a–c).
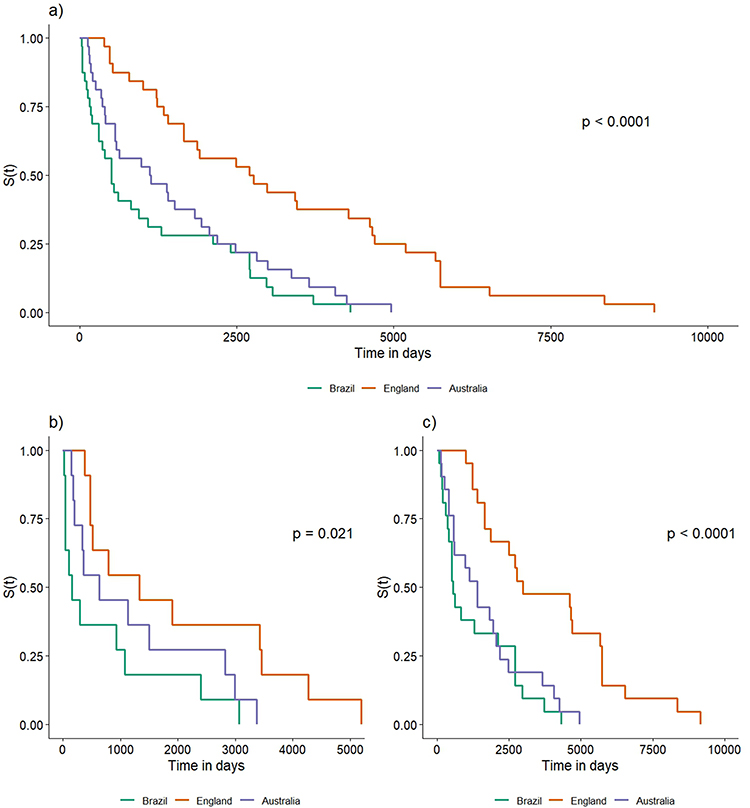 |
Figure 3 Comparison of time elapsed between regulatory approval of the drug and publication of the recommendation for incorporation into the public health system (a) overall, (b) rheumatoid arthritis, and (c) cancer (in days), between Brazil, Australia and England using the Kaplan-Meier curve. |
Discussion
Between January 2012 and March 2024, CONITEC recommended the incorporation of 32 biological drugs, 34.4% of them for the treatment of RA and 65.6% for different types of CA, corresponding to a total of 26 unique drugs. According to the respective Clinical Protocols and Therapeutic Guidelines (PCDT), these pathologies can be treated with some of the same biological drugs. Regarding the biological drugs used in oncology, the same drug may be recommended for incorporation by CONITEC for different types of CA at different times. An example is rituximab, which was recommended for incorporation into the SUS for the treatment of RA in 2012, for B-cell non-Hodgkin’s lymphoma in 2013, and for chronic lymphocytic leukemia in 2023.
The time between ANVISA’s approval of the drug’s registration and CONITEC’s publication of the recommendation for its incorporation was on average 1,879 days longer for oncology drugs than for RA drugs. In England, this difference was 441 days on average, and in Australia, 571 days. This means that in Brazil, it takes about three times longer for an oncology drug to be recommended for incorporation into the SUS than in the UK system, and about four times longer for RA drugs than in the Australian system.
The results show that patients in Brazil, especially those with CA, may face delays in access to modern treatments compared to patients in England and Australia, as the recommendation for incorporation does not immediately mean that the drug will be available in the public health system, as shown in the study by Capucho et al12 This could have a significant impact on survival, as a delay in treatment of just four weeks could increase CA-related mortality, and on the quality of life of Brazilian patients, as timely access to new treatments could better control the disease and improve, prevent or delay severe CA symptoms.13,14 In addition, the financial sustainability of the SUS can be affected by these delays, as prolonged illness and the need for additional treatment can increase health care costs.15 Inequalities in access to treatment can also exacerbate disparities in health outcomes, particularly affecting vulnerable populations.16,17
Australia presented the fastest incorporation of new drugs for RA and CA, highlighting the strength and agility of its healthcare and regulatory systems. This expedited access ensures that patients receive cutting-edge treatments earlier, potentially improving outcomes and quality of life. In contrast, Brazil’s broad delays, particularly for CA, underscore deep-rooted systemic barriers such as regulatory inefficiencies, underfunding, and infrastructural gaps. These delays can result in prolonged suffering, reduced survival rates, and an increased disease burden for patients who await innovative therapies.18 Across all countries, CA drugs typically face longer timelines for integration than RA treatments, likely due to their clinical complexity and cost. These extended timelines may compromise timely care, limit therapeutic options, and widen global health disparities.
The analysis of specific drugs further illuminates these systemic differences. In Australia, the rapid incorporation of novel agents like tofacitinib for RA and brentuximab vedotin for CA highlights a responsive and agile health technology assessment (HTA) process. In contrast, the significant delays for crucial drugs like rituximab and trastuzumab in Brazil underscore a system struggling to keep pace with therapeutic advancements. These are not niche medications but foundational treatments in their respective fields; extended delays in their availability can mean that Brazilian patients are denied the standard of care available elsewhere for years.
Disparities between countries may be the result of various factors, including differences in regulatory processes, financing and public health policies. In Brazil, universal access to health services and comprehensive therapeutic care is guaranteed by the Unified Health System (SUS),19 which is responsible for providing drug treatment to all those who need it (in the case of chronic diseases, about 45% of the Brazilian population.20
In Australia, access to medicines is provided through the Australian Pharmaceutical Benefits Scheme (PBS), which subsidizes a portion of the value of medicines included in the public health system and available to the population. Thus, despite the principle of universal access to health, not every public health good or service is completely free. Its national health system, called Medicare, is maintained through taxes and fees and is accessible to the entire population.20
In the British case, the National Health Service (NHS) covers the whole of the United Kingdom and its reference is universal access to health services. The NHS has undergone transformations since its creation in 1948, and in 2012, in the case of England, became NHS England, as an independent system. Although the majority of health actions and services are provided free of charge and public expenditure represents the largest share of funding, there are cost-sharing arrangements in the NHS.20,21
In Brazil, the National Health Surveillance Agency (in Portuguese: Agência Nacional de Vigilância Sanitária – ANVISA) is responsible for the registration of drugs, and in order for them to be registered, it is essential that a duly authorized company applies for registration, according to Law 6,360/1976.3 After this stage, for the registration of the drug to be approved, it undergoes a careful analysis to certify its quality, efficacy and safety. If, for any reason, it is not proven that the drug has the required quality, safety and efficacy, the application for registration is rejected and the drug cannot be offered to the population. Once the medicine is registered, it can be marketed and included in the SUS.22 The drugs available in the SUS are included in the National List of Essential Medicines (in Portuguese: Relação Nacional de Medicamentos Essenciais – RENAME), which is divided into the Basic, Strategic and Specialized Components of Pharmaceutical Assistance.23
While the Basic Component is responsible for the procurement of drugs and supplies for basic health care, the Strategic Component finances pharmaceutical assistance activities for strategic health programs, such as the control of endemic diseases and antiretroviral drugs for HIV/AIDS. The Specialized Component of Pharmaceutical Assistance finances the acquisition and distribution of exceptional drugs that are expensive for the health system and are used to treat rare and highly prevalent diseases, such as autoimmune diseases and CA, on an outpatient basis.23–25 This last component guarantees, through CONITEC, comprehensive outpatient drug treatment for all clinical conditions covered by the different lines of care defined in the PCDT.25
The PCDT are documents that establish and standardize the criteria for diagnosing a disease or health problem, the recommended treatment with drugs and/or other appropriate products, the recommended dosages, the methods of clinical control, and the monitoring and verification of therapeutic results. They are based on scientific evidence and take into account the efficacy, safety, efficiency and cost-effectiveness of the recommended technologies.26
It is important to note that oncology drugs in the SUS are not made available through these components, but through Medium and High Complexity Health Care, where the supply of the drug occurs through the facility qualified in oncology, after the technology is included in the chemotherapy procedures registered in the High Complexity Authorization subsystem of the Outpatient Information System (APAC-SIA). This is different from what happens in the Specialized Component, where the drugs indicated for the treatment of CA are not listed in RENAME.22
The institutionalization of the HTA process in the SUS with the creation of CONITEC has been an important step forward for Brazil in expanding access to medicines, among other things, as more people have been able to access innovative and expensive treatments through the SUS.12 However, this study found a long time lag between the registration of drugs in the country and their recommendation for use by CONITEC, an average of 2019 days for drugs used to treat RA and 3898 days for drugs used in oncology.
England is responsible for HTA through the National Institute for Health and Care Excellence (NICE), created in 1999, with four standing Technology Assessment Committees, with a high degree of autonomy, which aim to promote recommendations on issues related to the provision of public health services by the NHS in England. It should be noted that NICE delegates the preparation of technology assessment reports to be considered by the Technology Assessment Committee to independent academic groups. In the Australian case, the Pharmaceutical Benefits Advisory Committee (PBAC), established in 1953, has the objective of evaluating new medicines in order to advise the relevant Ministry on their inclusion. As such, its autonomy is limited, as the Ministry has the final say on its recommendations. In both cases, it can be seen that NICE and PBAC have a faster process for recommending biological drugs for RA and oncology than the CONITEC process, which may favor faster incorporation and availability of the drug to the population, such that earlier access to these technologies may increase patient survival.2,12,20 In this sense, delaying treatment for RA and CA can have a significant negative impact on patient outcomes. In RA, delays in treatment have been associated with worse disease outcomes, increased disability and reduced quality of life.27 In oncology, delays in starting drug therapy can compromise the efficacy of the treatment itself and increase the risk of disease recurrence, death, disabilities, and costs with palliative care.28–30
The longer time it takes to recommend the inclusion of these drugs in the SUS and, consequently, their availability, can significantly compromise the proper management and treatment of diseases and constitute a barrier to access to pharmacotherapeutic treatment by making it difficult to access effective therapies within an acceptable timeframe.28,29,31,32 In addition, the pattern found in this study suggests a greater delay in CONITEC’s analysis and recommendation of processes involving oncology drugs, resulting in a delay in making these technologies available to patients with serious conditions, for example, who may be more affected by the development of negative outcomes related to the late initiation of appropriate treatment. Therefore, although the creation and implementation of CONITEC was an important step forward, the results indicate the need to improve the process of making biological technologies available in the SUS, especially in the area of oncology.
HTA process is fundamental to the development and improvement of universal health systems such as the SUS, including expanding access to new technologies and reducing health disparities. Since its inception, CONITEC has been an essential part of this process. However, there is a need for greater agility in the timing of recommendations for the inclusion of biological medicines for RA and oncology.
It is important to acknowledge the limitations of this study. The analysis was focused on a specific set of biological drugs recommended by CONITEC during a defined period and may not be generalizable to all drug classes or timeframes. Furthermore, this study did not investigate the specific reasons for delays within each country’s process, such as the number of review cycles, price negotiations, or public consultation periods. Additionally, it relies exclusively on descriptive analysis, without attempting to evaluate the impact of potential confounding factors or investigate covariate relationships. Consequently, the findings should be viewed as observational patterns rather than causal inferences, which may restrict the depth of understanding regarding underlying drivers or associations. Also, as this is a bibliographic research, data on factors such as drug costs, patient compliance, and quality of life were not available.
Conclusion
Treatment with these technologies, especially for CA, is considered fundamental to improving the quality of life of those who need it, as it is a disease for which a delay in starting treatment can cause a serious deterioration in the condition and increased mortality. Developed countries such as England and Australia have paid special attention to the impact of neoplasms on the health of their populations. Thus, the long time it has taken Brazil to recommend the incorporation of biological technologies for the treatment of RA and CA of different types may be an obstacle or a barrier to access to these drugs in the SUS, prolonging the start of treatment for a large part of the Brazilian population, especially those with fewer resources and who use the SUS exclusively.
Abbreviations
HTA, Health Technology Assessment; CONITEC, National Commission for the Incorporation of Technologies in the Unified Health System; SUS, Brazilian Unified Health System; RENAME, National List of Essential Medicines; ANVISA, National Health Surveillance Agency; EMA, European Medicines Agency; MHRA, UK’s Medicines & Healthcare Products Regulatory Agency; (NICE), National Institute for Health and Care Excellence.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Novaes HMD, de Soárez PC. Health technologies assessment: origins, development, and current challenges. Int and Brazilian Scenarios Cad Saude Publica. 2020;36(8). doi:10.1590/0102-311X00006820
2. Lima SGG, de BC, de ACJC. Health technology assessment in Brazil–an international perspective. Cien Saude Colet. 2019;24:1709–9. doi:10.1590/1413-81232018245.17582017
3. Caetano R, Lopes LC, Santos GML, Osorio-de-Castro CGS. Incorporation and use of medicines in the Brazilian Unified National Health System: changes and risks of new Ministry of Health legislation. Cad Saude Publica. 2023;39.
4. Salerno MS, Matsumoto C, Ferraz I. Biofármacos no Brasil: características, importância e delineamento de políticas públicas para seu desenvolvimento. Available from: https://repositorio.ipea.gov.br/handle/11058/8522.
5. Aragão E, Loureiro S, Temporão JG. Trajetórias tecnológicas na indústria farmacêutica: desafios para a equidade no Brasil. Paim JS, Almeida Filho N, organizadores Saúde Coletiva: teoria e Prática Rio de Janeiro: medbook.
6. Zhang Y, Lin J, You Z, et al. Cancer risks in rheumatoid arthritis patients who received immunosuppressive therapies: will immunosuppressants work? Front Immunol. 2022;13:1050876. doi:10.3389/fimmu.2022.1050876
7. de Souza Neto AV, de Oliveira Souza M, Andrade GF. Biofármacos usados para o tratamento de artrite reumatoide: uma revisão de literatura: biopharmaceuticals used in the treatment of rheumatoid arthritis: a literature review. Health and Biosci. 2022;3(1):5–29. doi:10.47456/hb.v3i1.36997
8. Germano JL, Reis-Pardal J, Tonin FS, Pontarolo R, Melchiors AC, Fernandez-Llimos F. Prevalence of rheumatoid arthritis in South America: a systematic review and meta-analysis. Cien Saude Colet. 2021;26:5371–5382. doi:10.1590/1413-812320212611.3.05152020
9. Ferreira ML, Silva TB, Laine de Oliveira G. Expenditure on biological drugs for rheumatoid arthritis in the brazilian unified healthsystem between 2012 and 2016. JAFF. 2022;5(3). doi:10.22563/2525-7323.2020.v5.n.p.4-12
10. Rodrigues Filho FJ. Delineamento Do Perfil Das Tecnologias Incorporadas No SUS e a Análise Dos Gastos Públicos Com Biofármacos. Universidade Federal de Pernambuco. 2020.
11. Nepomuceno AF, Figueiredo M, Santos R, Souza T. Evaluation of the incorporation of monoclonal antibodies for cancer treatment in the unified health system. J Assist Farmacêutica Farmacoeconomia. 2020;5(2).
12. Capucho HC, Brito A, Maiolino A, Kaliks RA, Pinto RP. Incorporation of medicines in the Unified Health System (SUS): comparison between oncology and the specialized component of pharmaceutical care. Cien Saude Colet. 2022;27:2471–2479. doi:10.1590/1413-81232022276.16282021
13. Thibodeau S, Jalink M, Paulin G. Mortality due to cancer treatment delay: a systematic review and meta-analysis.
14. Sehdev S, Gotfrit J, Elias M, Stein BD. Impact of systemic delays for patient access to oncology drugs on clinical, economic, and quality of life outcomes in Canada: a call to action. Current Oncol. 2024;31(3):1460–1469. doi:10.3390/curroncol31030110
15. Ocké-Reis CO. Financial sustainability of the Brazilian Health System and health-related tax expenditures. Cien Saude Colet. 2018;23:2035–2042. doi:10.1590/1413-81232018236.05992018
16. Vaccarella S, Georges D, Bray F, et al. Socioeconomic inequalities in cancer mortality between and within countries in Europe: a population-based study. Lancet Reg. Health Eur. 2023:25. doi:10.1016/J.LANEPE.2022.100551.
17. Cancer Inequalities: home. Available from: https://cancer-inequalities.iarc.who.int/.
18. P HT, D KW, Thibodeau S, et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020;371:m4087. doi:10.1136/bmj.m4087
19. Brazil. Lei No 8.080, de 19 de Setembro de 1990. Available from: https://www.planalto.gov.br/ccivil_03/leis/l8080.htm.
20. de OLCF, do NMAA, IMSO L. Access to medication in universal health systems–perspectives and challenges. Saúde em Debate. 2020;43:286–298.
21. Filippon J, Giovanella L, Konder M, Pollock AM. “ Liberalizing” the English National Health Service: background and risks to healthcare entitlement. Cad Saude Publica. 2016;32:e00034716. doi:10.1590/0102-311X00034716
22. Brazil, Agência Nacional de Vigilância Sanitária - Anvisa. Registro de novos medicamentos: saiba o que é preciso — agência Nacional de Vigilância Sanitária - Anvisa. 2018. Available from: https://www.gov.br/anvisa/pt-br/assuntos/noticias-anvisa/2018/registro-de-novos-medicamentos-saiba-o-que-e-preciso.
23. Brazil. Conselho Nacional de Secretários de Saúde. Assistência Farmacêutica No SUS. Vol 7. Conselho Nacional de Secretários de Saúde (CONASS).
24. Vieira FS. Assistência farmacêutica no sistema público de saúde no Brasil. Rev Panam Salud Pública. 2010;27(2):149–156. doi:10.1590/s1020-49892010000200010
25. Brazil. Componente Especializado da Assistência Farmacêutica - CEAF — ministério da Saúde. Available from: https://www.gov.br/saude/pt-br/composicao/sectics/daf/ceaf.
26. Brazil. Protocolos Clínicos e Diretrizes Terapêuticas - PCDT — comissão Nacional de Incorporação de Tecnologias no Sistema Único de Saúde - CONITEC. Available from: https://www.gov.br/conitec/pt-br/assuntos/avaliacao-de-tecnologias-em-saude/protocolos-clinicos-e-diretrizes-terapeuticas/pcdt.
27. Naeem F, Khan SEA, Saeed MA, Farman S. Diagnostic and therapeutic delay in rheumatoid arthritis patients: impact on disease outcome. Pak J Med Sci. 2021;37(4):1001. doi:10.12669/pjms.37.4.3471
28. Indini A, Aschele C, Cavanna L, et al. Reorganisation of medical oncology departments during the novel coronavirus disease-19 pandemic: a nationwide Italian survey. Eur J Cancer. 2020;132:17–23. doi:10.1016/j.ejca.2020.03.024
29. Schwartz KM, Honstain C, Spruit JL, Harris M. Allogeneic hematopoietic stem cell transplant for acute lymphoblastic leukemia in a pediatric patient after Covid-19 infection complicated by MIS-C. J Pediatr Health Care. 2022;36(3):280–285. doi:10.1016/j.pedhc.2022.01.006
30. Barclay NL, Català M, Jödicke AM, et al. Collateral effects of the COVID-19 pandemic on endocrine treatments for breast and prostate cancer in the UK: a cohort study. Ther Adv Med Oncol. 2024;16:17588359241253115. doi:10.1177/17588359241253115
31. Wirtz VJ, Kaplan WA, Kwan GF, Laing RO. Access to medications for cardiovascular diseases in low-and middle-income countries. Circulation. 2016;133(21):2076–2085. doi:10.1161/CIRCULATIONAHA.115.008722
32. Chieffi AL, Barradas RDCB, Golbaum M. Legal access to medications: a threat to Brazil’s public health system? BMC Health Serv Res. 2017;17(1):499. doi:10.1186/s12913-017-2430-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combination of Methotrexate and Resveratrol Reduces Pro-Inflammatory Chemokines in Human THP-1 Cells
Al-Nasser MM, Al-Saeedi MJ, Alhowaiti SA, Shinwari Z, Alhamlan FS, Alothaid H, Alkahtani S, Al-Qahtani AA
Journal of Inflammation Research 2024, 17:8085-8098
Published Date: 2 November 2024