Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Comparable Improvements in Heart Rate Recovery Following Short-Term High-Intensity and Moderate-Intensity Interval Training in Patients with Cardiovascular Disease
Authors Song Q, Chang J, Bai B, Abudoukelimu M, Jiang Z, Zhu J, Lin Z, Guo J, Ma H ![]() , Hu D
, Hu D
Received 29 August 2025
Accepted for publication 8 December 2025
Published 23 December 2025 Volume 2025:18 Pages 8185—8196
DOI https://doi.org/10.2147/JMDH.S560641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Qianqian Song,1,2,* Jinna Chang,3,* Bingqing Bai,1 Mayila Abudoukelimu,1 Zhongxing Jiang,1 Junshuo Zhu,4 Zhaoqin Lin,1 Jianjun Guo,2 Huan Ma,1 Dayi Hu2,5
1Department of Cardiac Rehabilitation, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 2Center for Sports-Medicine Integrative Innovation, Capital University of Physical Education and Sports, Beijing, People’s Republic of China; 3Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, People’s Republic of China; 4School of Medicine South China University of Technology, Guangdong, People’s Republic of China; 5Institute of Cardiovascular Diseases, Peking University People’s Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dayi Hu, Center for Sports-Medicine Integrative Innovation, Capital University of Physical Education and Sports, Beijing, China; Institute of Cardiovascular Diseases, Peking University People’s Hospital, Beijing, People’s Republic of China, Email [email protected] Huan Ma, Department of Cardiac rehabilitation, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China, Email [email protected]
Objective: Heart rate recovery (HRR) is a validated prognostic marker in cardiovascular disease (CVD). This study evaluated and compared the effects of 4-week high-intensity interval training (HIIT) and moderate-intensity interval training (MIIT) on post-exercise HRR in patients with CVD.
Methods: A total of 1,020 CVD patients undergoing cardiac rehabilitation (Jan 2021-May 2024) were screened, and 209 who completed 12 sessions and cardiopulmonary exercise tests were included (HIIT: 82; MIIT: 127). The mean ages were 55.2 (HIIT) and 52.9 years (MIIT), with females comprising 34.1% and 34.6%, respectively. The MIIT protocol included four 8-min cycling bouts (RPE 12– 14) with 2-min active recovery, while HIIT involved 20– 25 × 30-s high-intensity bouts (RPE 14– 15) alternating with 30-s low-intensity recovery.
Results: Both interventions significantly improved HRR (HIIT: 3.1± 8.7 bpm, P = 0.002; MIIT: 3.0± 10.0 bpm, P = 0.001), with no between-group difference (P = 0.816). Peak VO2 similarly increased in both groups (HIIT: 3.3± 2.8; MIIT: 3.0± 3.6 mL·kg− 1·min− 1; P < 0.001). Other related measures were also notably improved (P < 0.05). Multivariable regression analysis revealed that the change in HRR was inversely associated with the change in resting heart rate in both HIIT (β = − 0.227, P = 0.04) and MIIT (β = − 0.318, P < 0.001) cohorts.
Conclusion: Both short-term HIIT and MIIT comparably enhance HRR in patients with CVD, highlighting the clinical applicability of interval training as an efficient option for patients with limited time availability. However, the retrospective design limits causal inference and requires confirmation in future studies.
Keywords: cardiovascular disease, high-intensity interval training, moderate-intensity interval training, heart rate recovery
Introduction
Cardiovascular disease (CVD) remains the leading cause of mortality worldwide, accounting for approximately 19 million deaths annually, or nearly one-third of all death,1 placing a substantial burden on healthcare systems. The rising prevalence of metabolic risk factors such as hypertension, diabetes, obesity, dyslipidemia, and physical inactivity continues to drive CVD incidence while impairing long-term quality of life.2,3 Psychological comorbidities, including anxiety and depression, further exacerbate cardiovascular pathology and worsen prognosis.4,5
In addition to conventional risk factor management, an increasing body of evidence highlights autonomic dysfunction as a key pathophysiological mechanism in CVD progression.6,7 HRR is a well-established noninvasive marker of autonomic regulation during the post-exercise period, reflecting the coordinated process of rapid parasympathetic reactivation and gradual sympathetic withdrawal.8 Impaired or delayed HRR, particularly within the first minute after exercise, indicates autonomic imbalance driven primarily by reduced vagal reactivation.9 Importantly, delayed HRR has been identified as an independent predictor of major adverse cardiovascular events, hospital readmission, and all-cause mortality in patients with CVD.10,11 These combined burdens highlight the urgent need for effective strategies to improve outcomes and reduce disease progression in patients with CVD.
While pharmacological therapies and invasive interventions,12,13 address certain aspects of CVD, structured exercise training represents a cornerstone for modulating autonomic function.14 Cardiac rehabilitation (CR) demonstrates efficacy in restoring autonomic balance in patients with acute coronary syndrome, characterized by attenuated sympathetic overactivity and enhanced parasympathetic tone.15 Notably, parasympathetic reactivation is postulated as a primary mechanism underpinning the cardioprotective effects of CR.16
Current CR guidelines predominantly recommend moderate-intensity continuous training (MICT), which involves sustained aerobic exercise performed at a prescribed moderate workload over a continuous duration.17,18 In recent years, however, accumulating evidence has supported high-intensity interval training (HIIT) as a safe and effective alternative.19 HIIT involves alternating short bouts of high-intensity exercise with active recovery and has been shown in randomized trials and meta-analyses to be superior or at least non-inferior to MICT in improving cardiovascular function and cardiorespiratory fitness.20,21 Similar advantages have been observed for autonomic recovery, where HIIT appears to outperform or match MICT in enhancing HRR, a key marker of autonomic reactivation.22,23 Collectively, these findings highlight HIIT as a time-saving and efficient training modality capable of eliciting meaningful cardiovascular and autonomic benefits in cardiac rehabilitation, underscoring the importance of exploring alternative interval-based approaches. Moderate-intensity interval training (MIIT) lies between the two modalities, incorporating moderate-intensity intervals with recovery phases. It offers a hybrid training approach, and its moderate intensity may provide a more favorable balance between training efficacy and patient tolerance.24
However, the application of MIIT in patients with cardiovascular disease remains limited, and evidence specifically addressing its effects on HRR is insufficient. Direct comparisons between MIIT and HIIT are also lacking, which results in insufficient clarity in the guidance regarding the autonomous recovery strategies based on intermittent training in cardiac rehabilitation. Moreover, considering that most existing studies have intervention periods ranging from 8 to 12 weeks,25 real-world CR programs an urgent need to explore efficient and feasible short-term rehabilitation strategies.26 Several studies have demonstrated that short-term interventions can already elicit meaningful improvements in patients with CVD.20,27 Therefore, this study aims to address these unmet needs by evaluating the effects of a short-term HIIT and MIIT intervention on HRR and cardiopulmonary function in patients with CVD, and by directly comparing the two modalities to clarify their relative efficacy.
We hypothesized that both HIIT and MIIT would improve HRR and cardiopulmonary function in patients with CVD. Furthermore, during short-term intervention, MIIT would demonstrate beneficial effects comparable to those of HIIT, providing an efficient and feasible alternative exercise modality for cardiac rehabilitation.
Materials and Methods
Design and Participants
This retrospective cohort study screened 1,020 CVD patients participating in cardiac rehabilitation at Guangdong Provincial People’s Hospital between 2021 and 2024. Based on predefined eligibility criteria, 209 patients who completed all 12 prescribed training sessions and both pre- and post-intervention cardiopulmonary exercise testing (CPET) were included in the analysis. Key inclusion criteria comprised: (1) age 18–76 years; (2) coronary artery disease (eg, stable angina, post-percutaneous coronary intervention, or post-coronary artery bypass grafting), valvular heart disease after surgical or transcatheter treatment; (3) completion of 12 supervised outpatient rehabilitation sessions (HIIT: n=82; MIIT: n=127) in one month; and (4) provision of written informed consent for data use. Exclusions were primarily due to missing CPET or psychological assessment data (Figure 1). The study complied with the Declaration of Helsinki and was approved by the hospital’s Ethics Committee (Approval No: KY2023-514).
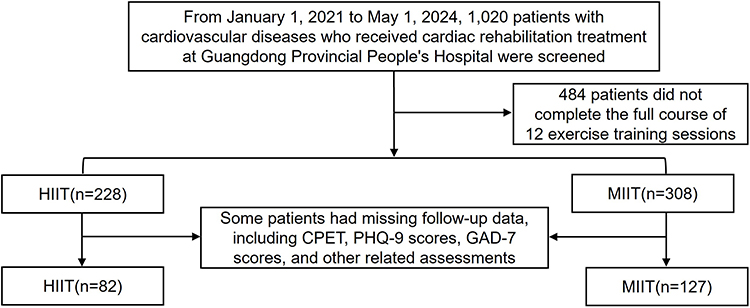 |
Figure 1 Study enrollment. |
It should be noted that the 209 patients were allocated to the HIIT or MIIT group as part of routine clinical decision-making prior to the initiation of cardiac rehabilitation, rather than by the research team. The assignment was jointly determined by the cardiology director and rehabilitation physicians based on individualized clinical assessments, including baseline cardiopulmonary function, exercise tolerance, and risk stratification, to ensure safety and appropriateness of the prescribed training program. The researchers subsequently performed a retrospective analysis of the clinical records and outcome data to evaluate the effects of the two training modalities. Furthermore, no adverse cardiovascular events (eg, angina or syncope) occurred during training in either group, and session adherence was better. As this study employed a retrospective design and non-randomized group assignment, selection bias may exist. To minimize bias, all patients received a standardized rehabilitation program, and age, sex, BMI, and baseline differences were controlled for in the analysis, with outcome assessments performed by blinded evaluators.
Sample Size and Power Justification
An a priori power analysis was conducted in G*Power (version 3.1) for an ANCOVA design with two groups (F-tests, fixed effects, main effects and interactions), assuming an effect size of f = 0.25, α = 0.05, power = 0.80, and five covariates (group, age, sex, BMI, baseline), which indicated a required total sample size of N = 134. Our final analytic sample of N = 209 exceeded this requirement, indicating adequate statistical power to detect clinically meaningful effects.
Cardiopulmonary Exercise Test
Standardized CPET was performed on all patients before and after the intervention using identical equipment and protocols to ensure data comparability. Tests were conducted on electronically braked cycle ergometers with individualized incremental ramp protocols, adjusted for each patient’s clinical status and exercise tolerance. The protocol continued until volitional exhaustion or meeting predefined termination criteria (symptoms, electrocardiography abnormalities, or blood pressure limits). HRR was calculated as the reduction in heart rate from peak exercise to 1 minute after exercise cessation (HRR1min = Peak HR − HR at 1 min post-exercise), which reflects early parasympathetic reactivation. Throughout testing, real-time monitoring included 12-lead electrocardiography, blood pressure, oxygen saturation, and HR. HR data were acquired via a computerized automated system to ensure measurement precision.
HIIT and MIIT Protocols
All exercise interventions were performed at the CR Center of Guangdong Provincial People’s Hospital. Participants underwent a 4-week, supervised cycling program comprising 12 sessions (3 sessions/week) under the guidance of a multidisciplinary team of cardiologists, rehabilitation therapists, and nurses. Exercise intensity was individually prescribed according to baseline CPET-derived peak VO2 and maximal work rate (WR).
The MIIT protocol consisted of a 5-min warm-up followed by four cycles of 8-min continuous cycling at 40–55% WR (RPE 12–14) interspersed with 2-min active recovery. The target WR was progressively increased from 40% to 55% in 4-session increments while maintaining the same session structure, and the total session duration was approximately 50 min including a cool-down period.
The HIIT protocol consisted of a 5-min warm-up followed by 20–25 repeated bouts of 30-s high-intensity cycling at 80–90% WR (RPE 14–15) alternated with 30-s low-intensity recovery. Training load was progressively increased every four sessions by raising both exercise intensity (80%, 85%, 90% WR) and the number of repetitions (20 to 25 cycles) to ensure a consistent overload stimulus, and the total session duration was approximately 40–45 min including a cool-down period, see Figure 2 for details.
 |
Figure 2 Exercise protocols of HIIT and MIIT in CR. |
Psychological Symptom Assessment
Psychological symptoms were assessed at baseline and post-intervention using validated self-report scales. Depressive symptoms were measured with the Patient Health Questionnaire-9 (PHQ-9). Anxiety symptoms were evaluated with the Generalized Anxiety Disorder-7 (GAD-7).28,29 All assessments were conducted under researcher supervision to ensure data accuracy and confidentiality.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean ± SD and categorical variables as number (percentage). Normality was assessed using the Shapiro–Wilk test. Within-group changes from baseline to post-intervention were analyzed using paired t-tests or Wilcoxon signed-rank tests with Cohen’s d as the effect size indicator. Between-group comparisons were performed using independent samples t-tests or Mann–Whitney U-tests when appropriate. ANCOVA was applied with post-intervention values as dependent variables, group as a fixed factor, and baseline values, age, sex, and BMI as covariates, with partial η2 reported as the effect size. ANCOVA assumptions were verified, including the normality and homogeneity of residuals (Supplement Tables S4–12 and Figure S1–S4). A sensitivity analysis using a linear mixed-effects model was conducted to confirm the robustness of the primary findings.
Multivariable linear regression models were used to identify predictors of HRR change, including a pooled model incorporating group × predictor interaction terms. Candidate predictors were selected based on physiological relevance and prior evidence. Regression results are reported as standardized coefficients (β) with 95% confidence intervals (CIs) and p-values. Pearson or Spearman correlation analyses, as appropriate, were further used to examine the association. All tests were two-tailed with a significance level of p < 0.05.
Results
Study Patients
Baseline demographic, clinical, and medication characteristics were similar between the two groups (Table 1). There were no significant differences in age (55.2 ± 12.1 vs 52.9 ± 13.3 years, p = 0.18), sex distribution (34.1% vs 34.6% female, p = 0.941), height, body weight, BMI, or resting hemodynamic parameters, including resting HR, SBP, and DBP (all p > 0.05). The prevalence of comorbidities, including CAD (p = 0.653), valvular heart disease (p = 0.413), diabetes (p = 0.473), hypertension (p = 0.340), hyperlipidemia (p = 0.301), and previous cardiac surgery (p = 0.269), was also comparable between groups. Likewise, the use of statins (p = 0.727), beta-receptor blockers (p = 0.764), ACEIs/ARBs (p = 0.882), hypoglycemic drugs (p = 0.158), and SSRIs (p = 0.639) did not differ significantly between groups.
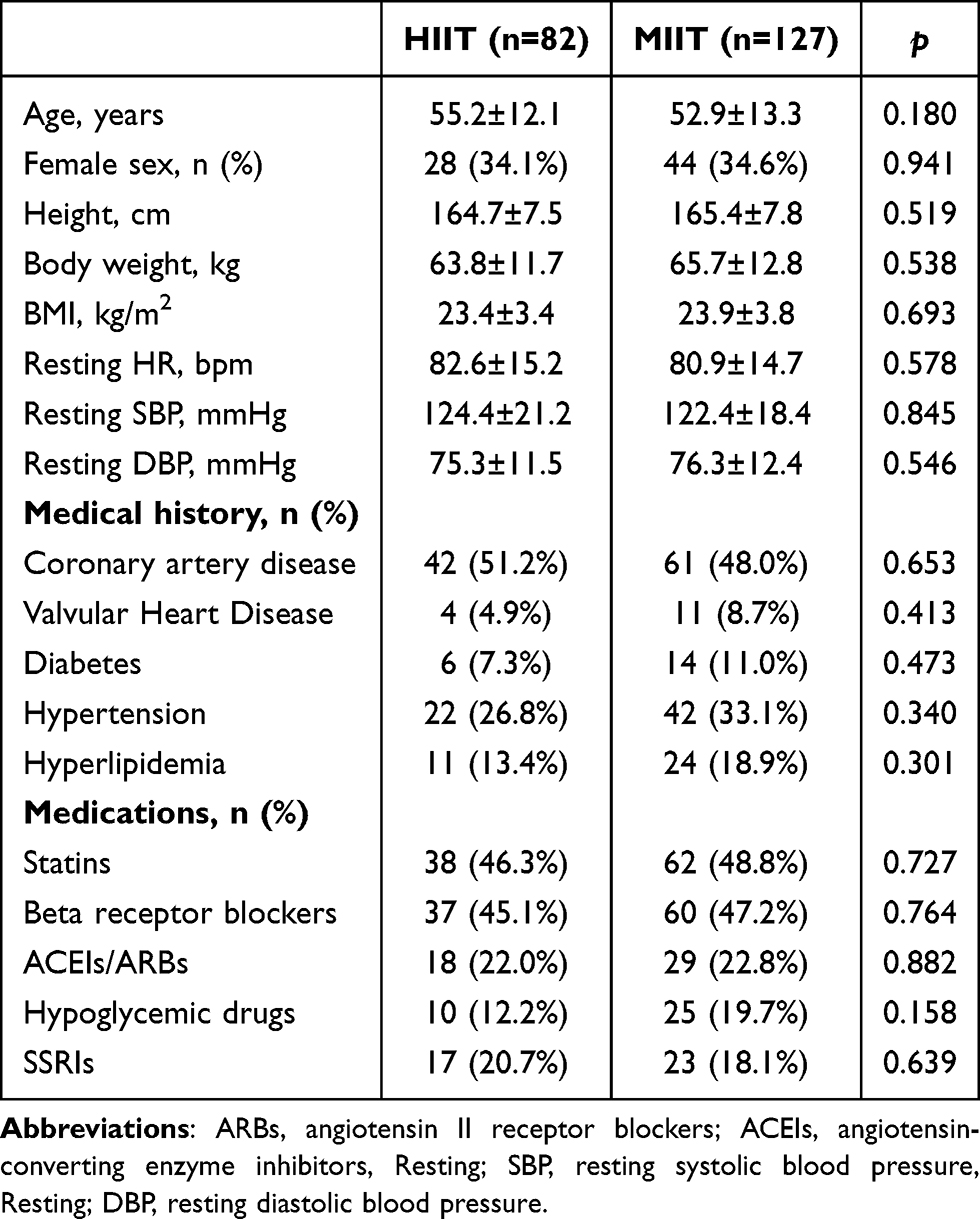 |
Table 1 Baseline Characteristics of Study Patients |
These findings confirm that baseline demographic characteristics, comorbidities, and medication use were well balanced between the HIIT and MIIT groups, minimizing the potential influence of confounding factors on subsequent outcomes.
Heart Rate Parameters
After the 4-week intervention (Table 2), both groups exhibited significant improvements in HRR. The mean change was 3.1 ± 8.7 bpm in the HIIT group (p = 0.002) and 3.0 ± 10.0 bpm in the MIIT group (p = 0.001), with no significant difference between groups (p = 0.816). Resting HR decreased markedly in both groups, with reductions of 7.0 ± 12.9 bpm in the HIIT group (p < 0.001) and 4.6 ± 13.8 bpm in the MIIT group (p < 0.001). The magnitude of reduction did not differ significantly between groups (p = 0.249).
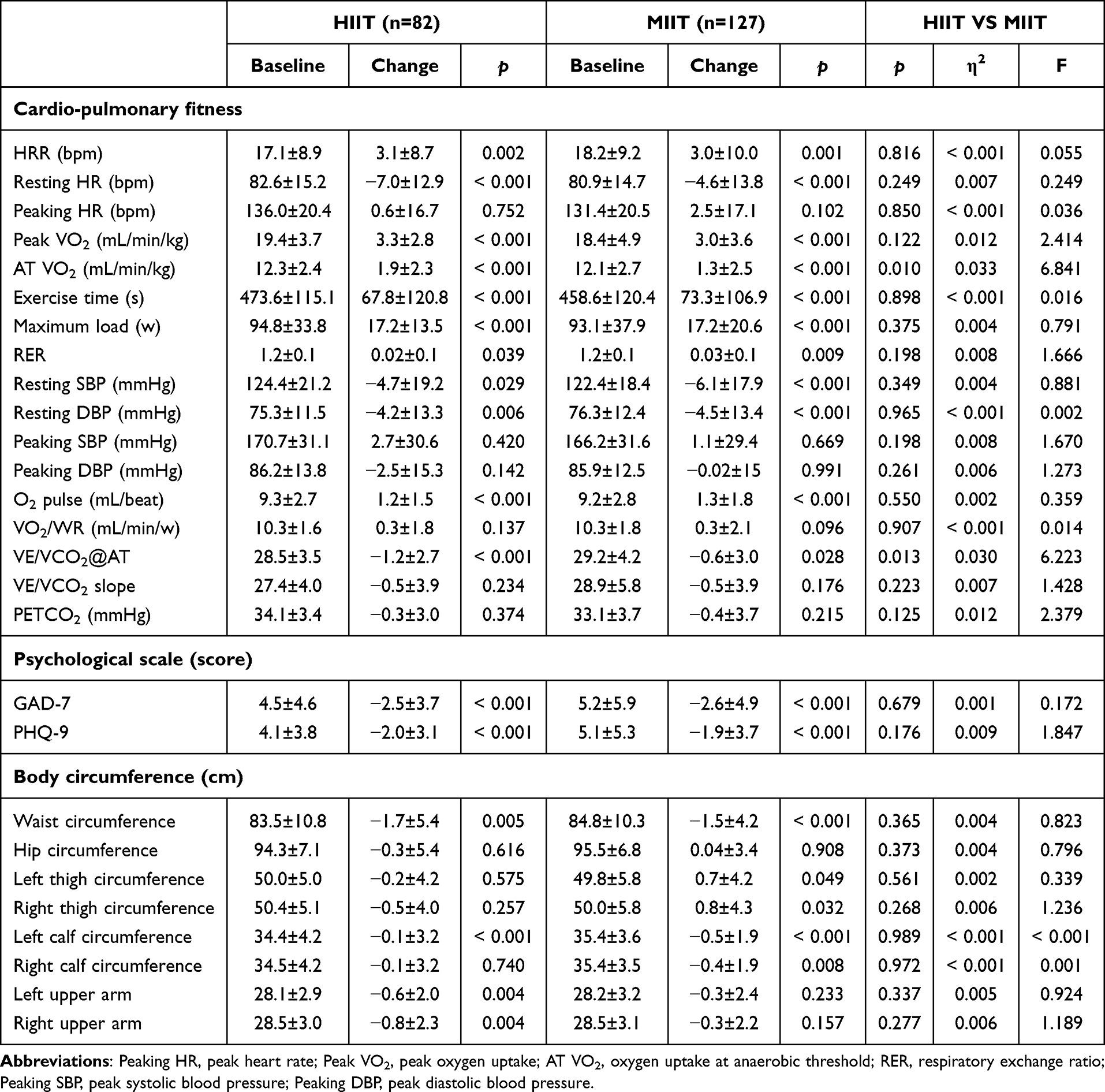 |
Table 2 Pre- and Post-Intervention Changes in CPET, Psychological Scores, and Body Circumference in HIIT and MIIT Groups |
Cardiopulmonary Exercise Capacity
After the 4-week intervention (Table 2), both groups demonstrated significant improvements in key Cardio-pulmonary fitness parameters. Peak VO2 increased by 3.3 ± 2.8 mL·kg−1·min−1 in the HIIT group (p < 0.001) and 3.0 ± 3.6 mL·kg−1·min−1 in the MIIT group (p < 0.001), with no significant difference between groups (p = 0.122). AT VO2 also improved in both groups, with mean increases of 1.9 ± 2.3 mL·kg−1·min−1 in HIIT and 1.3 ± 2.5 mL·kg−1·min−1 in MIIT (both p < 0.001). The increase was significantly greater in the HIIT group than in the MIIT group (p = 0.01). Regarding exercise tolerance, exercise time increased significantly in both groups, with changes of 67.8 ± 120.8 s in HIIT and 73.3 ± 106.9 s in MIIT (both p < 0.001). Maximum load increased by an average of 17.2 w in both groups (p < 0.001). Resting SBP decreased significantly in both groups, with reductions of 4.7 ± 19.2 mmHg in HIIT (p = 0.029) and 6.1 ± 17.9 mmHg in MIIT (p < 0.001). Resting DBP also declined significantly, with reductions of 4.2 ± 13.3 mmHg in HIIT (p = 0.006) and 4.5 ± 13.4 mmHg in MIIT (p < 0.001). VE/VCO2@AT decreased significantly in both groups, with reductions of 1.2 ± 2.7 in HIIT (p < 0.001) and 0.6 ± 3.0 in MIIT (p = 0.028). The reduction was significantly greater in the HIIT group than in the MIIT group (p = 0.013).
Psychological Scale Assessment
Both interventions significantly reduced anxiety and depression scores compared with baseline (Table 2). For anxiety, GAD-7 scores decreased by 2.5 ± 3.7 in the HIIT group (p < 0.001) and by 2.6 ± 4.9 in the MIIT group (p < 0.001). For depression, PHQ-9 scores decreased by 2.0 ± 3.1 in the HIIT group (p <0.001) and by 1.9 ± 3.7 in the MIIT group (p < 0.001). The magnitude of reduction did not differ significantly between groups (p>0.05).
Consistent with the descriptive findings, repeated-measures ANCOVA demonstrated significant time effects across all outcomes (partial η2 = 0.04–0.32, all p < 0.001), without significant group × time interactions (all p > 0.05; Supplement Table S1). Effect-size analysis further showed moderate-to-large within-group improvements in both interventions (Cohen’s d = 0.30–1.18), particularly for increases in peak VO2 and decreases in resting HR (Supplement Table S2).
Body Circumferences
Significant reductions in waist circumference were observed in both groups after the intervention (Table 2). In the HIIT group, waist circumference decreased by 1.7 ± 5.4 cm (p = 0.005), whereas in the MIIT group, it decreased by 1.5 ± 4.2 cm (p < 0.001). The magnitude of reduction did not differ significantly between groups (p = 0.493).
Predictors of HRR Change
Multiple linear regression models were developed to identify determinants of ΔHRR, adjusting for covariates that included changes in resting HR, peaking HR, GAD-7, PHQ-9, exercise time, maximum load, peak VO2, and AT VO2 (Table 3). The analysis showed that the change in resting HR was the only consistent independent predictor of HRR improvement across all cohorts. In the HIIT group, the regression coefficient was β = -0.227 (95% CI −0.302 to −0.007, p = 0.04); in the MIIT group, β = -0.318 (95% CI −0.352 to −0.109, p < 0.001); and in the overall cohort, β = -0.286 (95% CI −0.295 to −0.110, p < 0.001). The pooled model including the group × predictor interaction confirmed that the reduction in resting HR remained the most robust and consistent predictor of HRR improvement across intervention modalities, independent of training intensity (Supplement Table S3).
 |
Table 3 Predictors of HRR Change in HIIT, MIIT, and Overall Cohort |
Correlation Analysis Between HRR and Resting HR
A significant negative correlation was observed between changes in HRR and resting HR in the overall sample (r = −0.268, P < 0.001; Figure 3). This association persisted in subgroup analyses for both the MIIT group (r = −0.282, P = 0.001) and the HIIT group (r = −0.255, P = 0.021).
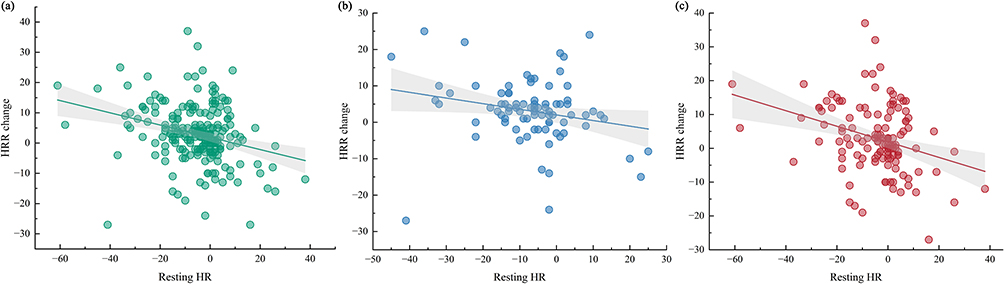 |
Figure 3 HRR-resting HR relationship analysis. (a) Overall cohort: Resting HR was significantly and inversely associated with HRR change; (b) HIIT group: Resting HR showed a significant inverse relationship with HRR change; (c) MIIT group: Resting HR was significantly and inversely correlated with HRR change. |
Discussion
The primary finding of this study was that both short-term HIIT and MIIT significantly improved HRR, with comparable magnitudes of improvement between the two training modalities, thereby offering clinicians two equally effective options for enhancing this important prognostic marker. Notably, the intervention period was only 4 weeks, whereas most previous trials typically lasted 8–12 weeks or longer. Furthermore, this study is the first to demonstrate, within a short-term HIIT and MIIT intervention, the pivotal role of resting heart rate in HRR improvement, highlighting its central importance in mediating post-exercise cardiac autonomic recovery.
Most prior trials employed longer-term training or focused on continuous protocols, whereas the present study uniquely compared two structured interval modalities over a short period. The present study found that MIIT and HIIT produced comparable improvements in HRR after a 4-week intervention. This may be because early improvements in HRR are primarily driven by rapid adaptations in autonomic regulation rather than relying on slower structural or peripheral cardiovascular remodeling. Aerobic training can promote parasympathetic reactivation while suppressing sympathetic excitability within a short period, thereby accelerating post-exercise heart rate recovery.27,30 Among these mechanisms, the potential advantage of HIIT has been attributed to its repeated high-intensity stimuli, which may more effectively trigger vagal reactivation and sympathetic withdrawal.31 MIIT may induce similar autonomic adaptations by providing an equivalent training load at moderate intensities through structured intervals, thereby reducing acute physiological stress while maintaining sufficient stimulus for adaptation.32
Resting HR has been recognized as an independent risk factor for both cardiovascular-specific and all-cause mortality.33 In this study, both the HIIT and MIIT groups exhibited a significant reduction in resting HR after the short-term intervention, reinforcing existing evidence that aerobic exercise effectively decreases resting HR.34,35 Lower resting HR is typically associated with better exercise capacity and enhanced cardiac vagal modulation.36 Enhanced vagal tone and reduced sympathetic activity are well-established mechanisms underlying exercise-induced decreases in resting HR,27,37,38 which in turn facilitate faster HRR recovery. Furthermore, multivariable regression consistently identified reductions in resting HR as the strongest independent predictor of HRR improvement across HIIT, MIIT, and the overall cohort. This robust association supports the concept that resting HR is a sensitive physiological marker reflecting dynamic autonomic adaptations.
Both HIIT and MIIT effectively enhanced overall exercise capacity in patients with CVD. Significant increases in peak VO2 and AT VO2 were observed in both groups. These improvements may be attributed to exercise-induced enhancements in mitochondrial function, microcirculatory remodeling, and increased skeletal muscle oxygen extraction efficiency.39,40 Previous studies have shown that short-term high-intensity training (3 weeks) is more effective than moderate-intensity continuous training in improving the AT, with particularly pronounced effects during the early adaptive phase of training.41 Consistent with these findings, the present study also observed that HIIT was superior to MIIT in enhancing AT VO2., but their clinical significance remains uncertain due to the short intervention duration. Longer-term follow-up and extended intervention studies are needed.
Moreover, both HIIT and MIIT significantly improved exercise time, maximal workload, RER, and O2 pulse, accompanied by reductions in resting systolic and diastolic blood pressure. These findings are consistent with previous cardiac rehabilitation studies demonstrating similar enhancements in exercise capacity and cardiac efficiency,42,43 as well as comparable improvements in blood pressure.44 Previous studies have shown that reductions in VE/VCO2 slope or VE/VCO2@AT following exercise-based cardiac rehabilitation are associated with better survival and lower hospitalization risk in patients with cardiovascular disease.45 The reductions in VE/VCO2@AT observed in both groups in this study, particularly in the HIIT group, suggest that HIIT may provide additional benefits by further optimizing ventilation–perfusion matching.
Given that waist circumference is a representative indicator of abdominal and visceral fat burden, it has been widely used to predict the risk of cardiovascular events such as hypertension, heart failure, and atherosclerosis.46,47 It is worth noting that both groups demonstrated significant reductions in waist circumference following the intervention. In addition, both interval training modalities significantly reduced GAD-7 and PHQ-9 scores, effectively alleviating anxiety and depressive symptoms. Consistent with previous studies, regular aerobic exercise can improve mental health through multiple mechanisms, including increasing neurotransmitter levels such as BDNF and enhancing autonomic nervous system function.48 These findings underscore the added value of interval training in providing metabolic and psychological benefits, which may contribute to improved quality of life and long-term outcomes in CVD patients.
In summary, short-term HIIT and MIIT produced clinically meaningful and comparable improvements in HRR and multiple cardiopulmonary indicators. For patients with limited exercise tolerance, insufficient cardiac functional reserve, or more conservative participation willingness, MIIT can provide adequate training stimulus while reducing acute physiological load, indicating favorable feasibility and suitability.24 In contrast, HIIT is more appropriate for individuals who can tolerate higher exercise intensities and may lead to additional improvements in exercise capacity and prognosis-related outcomes. Therefore, selecting interval training strategies based on functional status and individualized goals can enhance the precision and overall clinical benefit of CR.
Notably, the retrospective design represents the primary limitation of this study, as it may introduce selection bias and restrict causal inference. In addition, the wide age range of participants and variability in disease severity may introduce confounding effects. Furthermore, the relatively small sample size may have limited the statistical power to detect modest associations. Therefore, nonsignificant results should be interpreted with caution, given that a lack of significance may reflect insufficient power rather than the absence of a true effect. The intervention period was also relatively short, and long-term effects on HRR and clinical outcomes were not evaluated. Moreover, autonomic function was assessed solely through HRR without complementary measures such as heart rate variability or baroreflex sensitivity. Finally, all participants were recruited from a single cardiac rehabilitation center, which may limit the generalizability of the findings. Future studies with longer intervention durations, larger and more diverse multicenter cohorts, and mechanistic evaluations involving multimodal autonomic assessments are needed to confirm the sustainability of HRR improvements and clarify the underlying physiological pathways. These research directions will help strengthen the overall quality of evidence.
Conclusion
This study compared the effects of short-term HIIT and MIIT on HRR in patients with CVD and demonstrated that both training modalities significantly enhanced HRR and multiple cardiopulmonary indicators with comparable clinical benefits. These findings support interval training as a time-efficient and practical rehabilitation strategy, with MIIT offering better feasibility for those with limited exercise tolerance and HIIT providing potential additional benefits in individuals capable of higher workloads. This study supports the integration of HRR-targeted interval training into routine cardiac rehabilitation practice. Future multicenter, longer-term, and mechanistic studies incorporating multimodal autonomic assessments are needed to confirm the durability and physiological basis of these improvements, as well as their impact on long-term clinical outcomes.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author, Dr. Huan Ma, upon reasonable request.
Ethics Approval and Informed Consent
This study adhered to established ethical guidelines. The experimental procedures were approved by the Ethics Committee of Guangdong Provincial People’s Hospital (Ethics No. KY2023-514) and were in accordance with the ethical standards specified by the Helsinki Declaration of 1975 (revised in 2008). The patients/participants provided their written informed consent to participate in this study.
Acknowledgments
The authors sincerely thank all participants and the clinical rehabilitation team at Guangdong Provincial People’s Hospital for their valuable assistance with patient management and data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project is supported by grants from the Guangzhou Municipal Science and Technology Program key projects (2023B03J1249), the Su Ke’an Pharmaceutical Research and Development Project (202460), and the China Heart House-Chinese Cardiovascular Association TCM fund (CCA-TCM-032; 202342).
Disclosure
The authors declare no conflicts of interest and no financial relationships with any commercial entities related to this research.
References
1. Di Cesare M, Perel P, Taylor S, et al. The heart of the world. Global Heart. 2024;19(1):11. doi:10.5334/gh.1288
2. Rus M, Crisan S, Andronie-Cioara FL, et al. Prevalence and risk factors of metabolic syndrome: a prospective study on cardiovascular health. Medicina. 2023;59(10). doi:10.3390/medicina59101711
3. Vaduganathan M, Mensah GA, Turco JV, Fuster V, Roth GA. The global burden of cardiovascular diseases and risk: a compass for future health. J American College Cardiol. 2022;80(25):2361–2371. doi:10.1016/j.jacc.2022.11.005
4. Blatch Armon D, Buhayer A, Miteva K, et al. Depression and cardiovascular disease: mind the gap in the guidelines. Eur Heart J. 2025. doi:10.1093/eurheartj/ehaf479
5. Rezaee M, Darroudi H, Etemad L, et al. Anxiety, a significant risk factor for coronary artery disease: what is the best index. BMC Psychiatry. 2024;24(1):443. doi:10.1186/s12888-024-05798-w
6. Goldberger JJ, Arora R, Buckley U, Shivkumar K. Autonomic nervous system dysfunction: JACC focus seminar. J American College Cardiol. 2019;73(10):1189–1206. doi:10.1016/j.jacc.2018.12.064
7. Putranto R, Shatri H, Faisal E, Poespitasari VI, Megantara MA. A narrative review of heart rate variability and psychosomatic disorders: a promising tool for assessment and treatment. Heart Mind. 2025;9(5):387–97. doi:10.4103/hm.HM-D-24-00146
8. Peçanha T, Bartels R, Brito LC, Paula-Ribeiro M, Oliveira RS, Goldberger JJ. Methods of assessment of the post-exercise cardiac autonomic recovery: a methodological review. Int J Cardiol. 2017;227:795–802. doi:10.1016/j.ijcard.2016.10.057
9. Okutucu S, Karakulak UN, Aytemir K, Oto A. Heart rate recovery: a practical clinical indicator of abnormal cardiac autonomic function. Expert Review of Cardiovascular Therapy. 2011;9(11):1417–1430. doi:10.1586/erc.11.149
10. Velmeden D, Söhne J, Schuch A, et al. Role of heart rate recovery in chronic heart failure: results from the myovasc study. J American Heart Association. 2025;14(10):e039792. doi:10.1161/jaha.124.039792
11. Qiu S, Cai X, Sun Z, et al. Heart rate recovery and risk of cardiovascular events and all-cause mortality: a meta-analysis of prospective cohort studies. J American Heart Association. 2017;6(5). doi:10.1161/jaha.117.005505
12. Salavatian S, Spinelli JC, Schaefer JA, Libbus I, Mahajan A, Armour JA. Cardiopulmonary nerve stimulation as a novel therapy for cardiac autonomic nervous system modulation. Front Neurosci. 2024;18:1377171. doi:10.3389/fnins.2024.1377171
13. Shanks J, Ramchandra R. Angiotensin II and the cardiac parasympathetic nervous system in hypertension. Int J Mol Sci. 2021;22(22). doi:10.3390/ijms222212305
14. Jolly MA, Brennan DM, Cho L. Impact of exercise on heart rate recovery. Circulation. 2011;124(14):1520–1526. doi:10.1161/circulationaha.110.005009
15. Eser P, Jaeger E, Marcin T, Herzig D, Trachsel LD, Wilhelm M. Acute and chronic effects of high-intensity interval and moderate-intensity continuous exercise on heart rate and its variability after recent myocardial infarction: a randomized controlled trial. Ann Phys Rehabil Med. 2022;65(1):101444. doi:10.1016/j.rehab.2020.09.008
16. Piepoli MF, Hoes AW, Agewall S, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the sixth joint task force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016;252:207–274. doi:10.1016/j.atherosclerosis.2016.05.037
17. Verdicchio C, Freene N, Hollings M, et al. A clinical guide for assessment and prescription of exercise and physical activity in cardiac rehabilitation. A CSANZ position statement. Heart Lung Circul. 2023;32(9):1035–1048. doi:10.1016/j.hlc.2023.06.854
18. Ambrosetti M, Abreu A, Corrà U, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: from knowledge to implementation. 2020 update. A position paper from the secondary prevention and rehabilitation section of the european association of preventive cardiology. Eur J Preventive Cardiol. 2021;28(5):460–495. doi:10.1177/2047487320913379
19. Ribeiro PAB, Boidin M, Juneau M, Nigam A, Gayda M. High-intensity interval training in patients with coronary heart disease: prescription models and perspectives. Ann Phys Rehabil Med. 2017;60(1):50–57. doi:10.1016/j.rehab.2016.04.004
20. Taylor JL, Holland DJ, Keating SE, et al. Short-term and long-term feasibility, safety, and efficacy of high-intensity interval training in cardiac rehabilitation: the FITR heart study randomized clinical trial. JAMA Cardiol. 2020;5(12):1382–1389. doi:10.1001/jamacardio.2020.3511
21. Sert H, Gulbahar Eren M, Gurcay B, Koc F. The effectiveness of a high-intensity interval exercise on cardiometabolic health and quality of life in older adults: a systematic review and meta-analysis. BMC Sports Sci Med Rehab. 2025;17(1):128. doi:10.1186/s13102-025-01176-5
22. Villelabeitia-Jaureguizar K, Vicente-Campos D, Senen AB, Jiménez VH, Garrido-Lestache MEB, Chicharro JL. Effects of high-intensity interval versus continuous exercise training on post-exercise heart rate recovery in coronary heart-disease patients. Int J Cardiol. 2017;244:17–23. doi:10.1016/j.ijcard.2017.06.067
23. Currie KD, Rosen LM, Millar PJ, McKelvie RS, MacDonald MJ. Heart rate recovery and heart rate variability are unchanged in patients with coronary artery disease following 12 weeks of high-intensity interval and moderate-intensity endurance exercise training. Appl Physiol Nutr Metab. 2013;38(6):644–650. doi:10.1139/apnm-2012-0354
24. Maaloul R, Ben Dhia I, Marzougui H, et al. Is moderate-intensity interval training more tolerable than high-intensity interval training in adults with obesity? Biol Sport. 2023;40(4):1159–1167. doi:10.5114/biolsport.2023.123323
25. Stefanakis M, Batalik L, Antoniou V, Pepera G. Safety of home-based cardiac rehabilitation: a systematic review. Heart Lung. 2022;55:117–126. doi:10.1016/j.hrtlng.2022.04.016
26. Sugiharto F, Nuraeni A, Trisyani Y, Melati Putri A, Aghnia Armansyah N. Barriers to participation in cardiac rehabilitation among patients with coronary heart disease after reperfusion therapy: a scoping review. Vascular Health Risk Management. 2023;19:557–570. doi:10.2147/vhrm.S425505
27. Besnier F, Labrunée M, Richard L, et al. Short-term effects of a 3-week interval training program on heart rate variability in chronic heart failure. A randomised controlled trial. Ann Phys Rehabil Med. 2019;62(5):321–328. doi:10.1016/j.rehab.2019.06.013
28. Li Y, Cen J, Wu J, et al. The degree of anxiety and depression in patients with cardiovascular diseases as assessed using a mobile app: cross-sectional study. J Med Internet Res. 2023:
29. Bolgeo T, Di Matteo R, Simonelli N, et al. Psychometric properties and measurement invariance of the 7-item general anxiety disorder scale (GAD-7) in an Italian coronary heart disease population. J Affective Disorders. 2023;334:213–219. doi:10.1016/j.jad.2023.04.140
30. La Rovere MT, Mortara A, Sandrone G, Lombardi F. Autonomic nervous system adaptations to short-term exercise training. Chest. 1992;101(5 Suppl):299s–303s. doi:10.1378/chest.101.5_supplement.299s
31. Coretti M, Donatello NN, Bianco G, Cidral-Filho FJ. An integrative review of the effects of high-intensity interval training on the autonomic nervous system. Sports Med Health Sci. 2025;7(2):77–84. doi:10.1016/j.smhs.2024.08.002
32. Sasso JP, Ivanchikov S, Coates K, et al. Investigating the role of exercise pattern in acute cardiovagal recovery. Med Sci Sports Exercise. 2025;57(3):579–589. doi:10.1249/mss.0000000000003580
33. Seravalle G, Quarti Trevano F, Grassi G. Heart rate as a predictor of cardiovascular risk. Minerva Medica. 2021;112(1):130–143. doi:10.23736/s0026-4806.20.06695-1
34. Reimers AK, Knapp G, Reimers CD. Effects of exercise on the resting heart rate: a systematic review and meta-analysis of interventional studies. J Clin Med. 2018;7(12). doi:10.3390/jcm7120503
35. Coswig VS, Barbalho M, Raiol R, Del Vecchio FB, Ramirez-Campillo R, Gentil P. Effects of high vs moderate-intensity intermittent training on functionality, resting heart rate and blood pressure of elderly women. J Transl Med. 2020;18(1):88. doi:10.1186/s12967-020-02261-8
36. Gourine AV, Ackland GL. Cardiac Vagus and Exercise. Physiology. 2019;34(1):71–80. doi:10.1152/physiol.00041.2018
37. Munk PS, Butt N, Larsen AI. High-intensity interval exercise training improves heart rate variability in patients following percutaneous coronary intervention for angina pectoris. Int J Cardiol. 2010;145(2):312–314. doi:10.1016/j.ijcard.2009.11.015
38. Carnevali L, Sgoifo A. Vagal modulation of resting heart rate in rats: the role of stress, psychosocial factors, and physical exercise. Front Physiol. 2014;5:118. doi:10.3389/fphys.2014.00118
39. Christensen PM, Jacobs RA, Bonne T, Flück D, Bangsbo J, Lundby C. A short period of high-intensity interval training improves skeletal muscle mitochondrial function and pulmonary oxygen uptake kinetics. J Appl Physiol. 2016;120(11):1319–1327. doi:10.1152/japplphysiol.00115.2015
40. Mølmen KS, Almquist NW, Skattebo Ø. Effects of exercise training on mitochondrial and capillary growth in human skeletal muscle: a systematic review and meta-regression. Sports Med. 2025;55(1):115–144. doi:10.1007/s40279-024-02120-2
41. Wang Z, Wang J. The effects of high-intensity interval training versus moderate-intensity continuous training on athletes’ aerobic endurance performance parameters. Eur J Appl Physiol. 2024;124(8):2235–2249. doi:10.1007/s00421-024-05532-0
42. Astorino TA, Allen RP, Roberson DW, Jurancich M. Effect of high-intensity interval training on cardiovascular function, VO2max, and muscular force. J Strength Conditioning Res. 2012;26(1):138–145. doi:10.1519/JSC.0b013e318218dd77
43. Nam H, Jeon HE, Kim WH, Joa KL, Lee H. Effect of maximal-intensity and high-intensity interval training on exercise capacity and quality of life in patients with acute myocardial infarction: a randomized controlled trial. Eur J Phys Rehabil Med. 2024;60(1):104–112. doi:10.23736/s1973-9087.23.08094-2
44. Li L, Liu X, Shen F, et al. Effects of high-intensity interval training versus moderate-intensity continuous training on blood pressure in patients with hypertension: a meta-analysis. Medicine. 2022;101(50):e32246. doi:10.1097/md.0000000000032246
45. Poggio R, Arazi HC, Giorgi M, Miriuka SG. Prediction of severe cardiovascular events by VE/VCO2 slope versus peak VO2 in systolic heart failure: a meta-analysis of the published literature. Am Heart J. 2010;160(6):1004–1014. doi:10.1016/j.ahj.2010.08.037
46. Ross R, Neeland IJ, Yamashita S, et al. Waist circumference as a vital sign in clinical practice: a consensus statement from the IAS and ICCR working group on visceral obesity. Nat Rev Endocrinol. 2020;16(3):177–189. doi:10.1038/s41574-019-0310-7
47. Powell-Wiley TM, Poirier P, Burke LE, et al. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143(21):e984–e1010. doi:10.1161/cir.0000000000000973
48. Rawliuk T, Thrones M, Cordingley DM, Cornish SM, Greening SG. Promoting brain health and resilience: the effect of three types of acute exercise on affect, brain-derived neurotrophic factor and heart rate variability. Behav Brain Res. 2025;493:115675. doi:10.1016/j.bbr.2025.115675
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.