Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Community Pharmacists’ Knowledge and Counseling Competence on GLP-1 Receptor Agonists in Obesity and Type 2 Diabetes Care in Türkiye: A Cross-Sectional Study
Authors Bayram-Ozgur D ![]() , Demirtürk E, Sar Y
, Demirtürk E, Sar Y
Received 16 December 2025
Accepted for publication 23 January 2026
Published 3 March 2026 Volume 2026:19 587750
DOI https://doi.org/10.2147/DMSO.S587750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Donald McClain
Dilara Bayram-Ozgur,1 Ecenur Demirtürk,1 Yigitcan Sar1,2
1Department of Pharmacology, Faculty of Pharmacy, Acibadem Mehmet Ali Aydinlar University, Istanbul, Türkiye; 2Department of Pharmacology, Institute of Health Sciences, Istanbul University, Istanbul, Türkiye
Correspondence: Dilara Bayram-Ozgur, Acibadem Mehmet Ali Aydinlar University, Kerem Aydınlar Campus, Kayisdagi Cad. No: 32, Atasehir, Istanbul, 34752, Türkiye, Tel +902165004036, Email [email protected]
Purpose: The use of glucagon-like peptide-1 receptor agonists (GLP-1 RAs), including liraglutide and semaglutide, has expanded rapidly due to their effectiveness in weight management and glycemic control. Rising public interest, off-label cosmetic use, and prescription-free requests highlight the critical role of community pharmacists in ensuring appropriate patient counselling, safe dispensing, and rational use of these agents. This study aimed to assess the knowledge, attitudes, and practices of community pharmacists regarding GLP-1 RAs in Türkiye.
Patients and Methods: A cross-sectional survey was conducted among 500 community pharmacists in Türkiye between January and April 2025. Data were collected using a structured, literature-based questionnaire covering sociodemographic characteristics, attitudes, knowledge, and professional practices. Knowledge was evaluated using a 25-item scoring system. Statistical analyses included descriptive statistics, chi-square tests, independent samples t-tests, and one-way ANOVA, with significance set at p< 0.05.
Results: Requests for semaglutide and liraglutide were primarily for weight loss purposes (82.6% and 79.4%, respectively), and these agents were often sought without a prescription (over 60%) or medical recommendation (over 35%). The mean knowledge score was 15.8± 4.3. Differences were observed across gender, professional experience, and pharmacy setting (p< 0.05), with higher scores among female pharmacists, those with more than 16 years of experience, and those working in shopping mall pharmacies. Although most respondents correctly identified both medications as GLP-1 RAs (85.6% for semaglutide; 83.6% for liraglutide), gaps remained in regulatory awareness and consistency of routine counselling. A substantial proportion perceived misuse, with over 60% reporting concerns for both medications.
Conclusion: Community pharmacists demonstrate moderate knowledge and active involvement in counselling for GLP-1 RAs; however, gaps persist in addressing off-label demand and safety-related patient guidance. Targeted pharmacist education and clearer regulatory communication may enhance safe and evidence-based use of GLP-1 RAs.
Plain Language Summary: People around the world are showing great interest in new medicines called GLP-1 receptor agonists. These medicines, such as liraglutide and semaglutide, were first created to help people manage type 2 diabetes, but they are now widely used for weight loss. Because public demand is rising quickly—often without medical advice—community pharmacists are becoming the first professionals people turn to for information.
We conducted a survey with 500 community pharmacists in Türkiye to understand how much they know about these medicines and how they guide people who want to use them. Pharmacists told us that most people request these medicines mainly for weight loss, and many ask for them without a prescription. Pharmacists also reported that they often have to explain how to use the injections, how to store them safely at home, and what side effects to expect.
Our results show that pharmacists have a moderate level of knowledge. Many understand the basic information, but some important gaps remain, especially around official approval, correct dosing, and safety recommendations. Pharmacists with more experience tended to know more, and those working in busy locations such as shopping malls reported higher patient demand.
These findings highlight how important pharmacists are in helping people make safe and informed choices. As interest in weight loss medicines continues to grow, pharmacists need clear guidance, reliable training, and strong public health communication to support responsible use. Improving knowledge and counselling may help prevent misuse and protect the wellbeing of people seeking these treatments.
Keywords: medication misuse, off-label use, pharmacovigilance, pharmacy practice assessment, weight-loss pharmacotherapy
Introduction
Defined by a body mass index (BMI) ≥30 kg/m2, obesity now affects over 890 million adults globally, with projections suggesting this figure could exceed 1.02 billion by 2030 if effective interventions are not implemented.1 As obesity complications such as type 2 diabetes mellitus and cardiovascular diseases are associated with increased obesity related morbidity and mortality, the treatment of obesity with effective weight management strategies, including pharmacotherapy, is crucial.2,3
Glucagon-like peptide-1 (GLP-1) receptor agonists, particularly liraglutide and semaglutide, have emerged as highly effective agents due to their combined benefits on glycaemic control and weight reduction.4 Initially approved for type 2 diabetes management, both medications demonstrated robust weight-loss effects in large-scale clinical trials, which ultimately supported their regulatory approval for chronic weight management at higher doses.5,6 In Türkiye, liraglutide was officially approved for obesity treatment by the Turkish Medicines and Medical Devices Agency for use in patients with a BMI ≥30 kg/m2, or ≥27 kg/m2 with at least one weight related comorbidity.7 Semaglutide formulated for glycemic control in type 2 diabetes was approved in Türkiye in 2022.8 However, although a different formulation of the same active ingredient was approved in 2023 specifically for the treatment of obesity, this formulation is not currently available for sale in community pharmacies in Türkiye, thereby limiting access to an approved pharmacological option for obesity management.9 Nevertheless, mirroring global patterns, off-label semaglutide use for weight loss has increased substantially, driven by public interest and social media promotion.10
This rapid rise in off-label use has raised multiple safety, ethical, and regulatory concerns. Increased demand has contributed to periodic drug shortages, rising prices, and potential inequities in access.11,12 At the same time, interest in semaglutide for cosmetic weight loss has been amplified by online trends and non-medical information sources, as demonstrated in analyses of Google search patterns.10 Pharmacovigilance investigations have further highlighted safety concerns related to its inappropriate use, including misuse signals detected in the FDA Adverse Event Reporting System.11 Moreover, recent evidence indicates that public support for off-label Ozempic prescribing carries important policy implications, reflecting increasing societal pressure on prescribers and pharmacists.12
Community pharmacists are licensed healthcare professionals who serve as the most accessible point of contact between patients and the healthcare system, particularly in medication dispensing, counselling, and pharmacovigilance activities. They play a pivotal role in ensuring the rational use, safe dispensing, and patient counselling of GLP-1 receptor agonists. Their responsibilities include educating patients about approved indications, correct administration techniques, expected therapeutic outcomes, potential side effects, and contraindications.13 However, international evidence suggests that pharmacists’ preparedness for weight management services varies considerably. A recent systematic review highlighted several barriers—including knowledge gaps, limited training, and workflow and staffing constraints—that may hinder pharmacists’ ability to deliver comprehensive weight management services.13 Studies conducted in Lebanon and China similarly revealed deficiencies in pharmacists’ or healthcare professionals’ understanding of GLP-1 receptor agonists, underscoring the need for improved education and guidance.14,15 Research from Jordan also showed that reliance on non-scientific information sources can contribute to community-level misconceptions and misuse of GLP-1 medications.16
Despite the growing clinical importance and widespread public attention toward GLP-1 receptor agonists, data on community pharmacists’ knowledge, attitudes, and professional practices—particularly in Türkiye—remain limited. This gap is critical, given pharmacists’ frontline role in medication counselling and their direct involvement in preventing inappropriate or unsafe use of these high-demand therapies. Therefore, this study aims to evaluate the knowledge levels, attitudes, and professional practices of community pharmacists in Türkiye regarding the use of GLP-1 receptor agonists, specifically liraglutide and semaglutide, in the context of weight management.
Materials and Methods
Study Design and Setting
This study employed a cross-sectional and descriptive design to evaluate community pharmacists’ knowledge, attitudes, and practices regarding the use of liraglutide and semaglutide in Türkiye. Data were collected between January and April 2025 from pharmacists working in community pharmacies across multiple provinces. The study focused on practicing pharmacists who routinely provide pharmaceutical care and patient counselling services. An overview of the applied study methodology is presented in the flowchart in Figure 1.
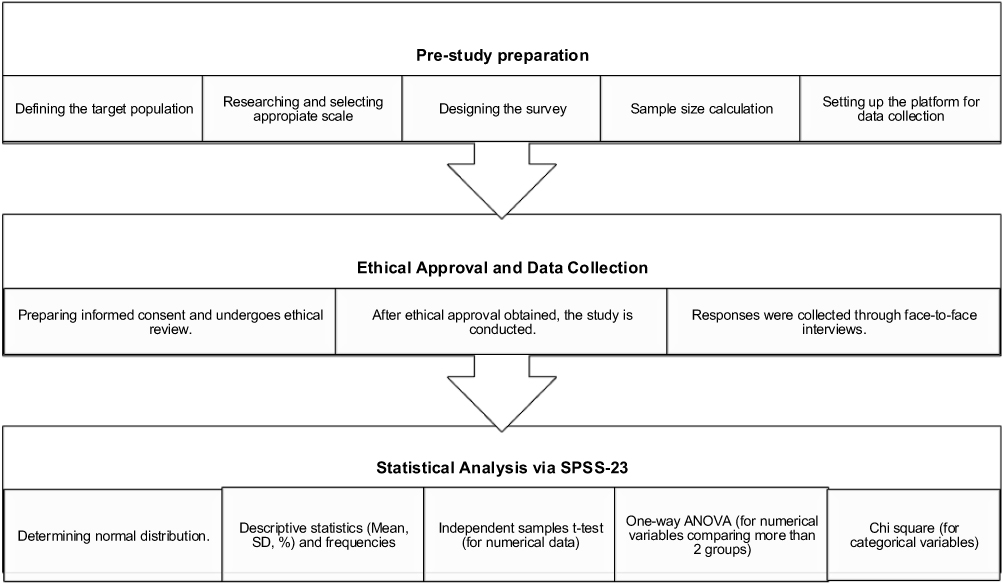 |
Figure 1 Flowchart of overview of the applied study methodology. Abbreviation: SD, standard deviation. |
Participants and Sampling
The target population consisted of licensed community pharmacists actively working in community pharmacies in Türkiye. A convenience sampling technique was used. Potential participants were approached in person at their community pharmacies and invited to participate in the study by the researchers. Inclusion criteria were: (1) being a registered community pharmacist, (2) actively working in a community pharmacy during the study period, and (3) providing voluntary informed consent. Exclusion criteria were limited to individuals who declined to participate or did not complete the questionnaire.
Sample Size Determination
The sample size was determined using Cochran’s formula to ensure adequate statistical precision. A 95% confidence level, 5% margin of error, and an assumed population proportion of 50%—commonly recommended when the true prevalence is unknown—were applied.17 Based on the total number of registered community pharmacists in Türkiye (n = 26,177), reported in the Turkish Pharmacists’ Association’s national report, the minimum required sample size was calculated as 379. This calculation ensured sufficient statistical power for the study.18
Data Collection Procedure
Data were collected through a structured, face-to-face questionnaire administered by trained researchers. Each questionnaire was completed individually by the participant at their own community pharmacy during working hours. To minimize the risk of mutual influence during data collection, questionnaires were administered one participant at a time, and participants completed the questionnaire without discussing the questions or their responses with others during completion. Participants were instructed to answer all questions based solely on their own knowledge and professional experience and were asked not to consult external information sources while completing the questionnaire. Before data collection, participants were informed about the study objectives, voluntary participation, anonymity, and confidentiality. Each survey took approximately 5–7 minutes to complete. No personally identifiable information was collected.
Questionnaire Development
The questionnaire was developed by the researchers and included selected items adapted from previous studies in the relevant literature.19–21 The questionnaire included 50 questions in four sections and applied in Turkish. The first section included questions on the sociodemographic characteristics of the participants, such as age, gender, and years of professional experience as a community pharmacist (≤1 year, 2–5 years, 6–10 years, 11–15 years, and ≥16 years). The second section assessed attitudes and pharmacy practices. The third section included knowledge-based items evaluating pharmacists’ understanding of the regulatory approval status, mechanisms of action, dosing, storage requirements, side effects, and contraindications of semaglutide and liraglutide. This section contains 25 questions. Correct answers were scored as 1, while incorrect answers were scored as 0. A participant can receive an average score between 0 and 25, with a higher score indicating a higher level of knowledge. In the last section, there are questions about pharmacists’ thoughts and experiences regarding the misuse of these drugs (Supplement Table 1).
Content validity was ensured through expert review. Two clinical pharmacists and one endocrinologist independently evaluated the questionnaire items for relevance, clarity, and appropriateness. Additionally, a biostatistician reviewed the questionnaire to confirm methodological suitability and the logical structure of the measurement domains. Based on expert feedback, the wording of several items was refined to improve clarity, while no items were removed.
A pilot study was conducted with 20 community pharmacists to assess the clarity, comprehensibility, and flow of the questionnaire. Based on the pilot study results, no substantial modifications were required, and the final version of the questionnaire was used for data collection.
The internal consistency of the knowledge section of the questionnaire was evaluated using Cronbach’s alpha coefficient, which demonstrated acceptable reliability (Cronbach’s α= 0.70).
Ethical Considerations
Ethical approval for this study was obtained from the Acibadem University Medical Research Ethics Committee (Decision No: 2024–19/703). The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The questionnaire was administered anonymously, and no personally identifiable information was collected. Participation was entirely voluntary, and informed consent was obtained from all participants prior to the commencement of the survey. Drug names are presented using their generic names; however, brand names are mentioned in parentheses in a few survey questions for clarity. This study has no conflict of interest with any pharmaceutical company.
Statistical Analysis
Prior to analysis, the dataset was reviewed to improve data quality and consistency. Records were screened for missing or implausible values, and missing observations were handled by imputing the mean value of the relevant group. The distributional properties of the continuous variables were evaluated using skewness and kurtosis statistics. Values falling within the range of −2 to +2 were considered indicative of approximate normality.22 Based on these criteria, all scale scores demonstrated acceptable distributional characteristics, allowing the use of parametric statistical methods.
Descriptive statistics were summarized using frequencies and percentages for categorical variables, and means with standard deviations for continuous variables. Comparisons between two independent groups were conducted using the independent samples t-test. Assumptions of variance homogeneity were assessed using Levene’s test, and test statistics were interpreted accordingly. For comparisons involving more than two groups, one-way analysis of variance (ANOVA) was applied, followed by post-hoc analyses when statistically significant differences were detected. Associations between categorical variables were examined using the chi-square test, with consideration of expected cell counts and degrees of freedom. A two-sided p value of less than 0.05 was accepted as the threshold for statistical significance (Figure 1).
Results
A total of 500 community pharmacists participated in the study. The demographic and professional characteristics of the respondents are presented in Table 1. The majority were female (72.6%), and the most common age group was 20–30 years (45.6%), followed by 31–40 years (20.4%). Most pharmacists held a bachelor’s degree (77.0%), and 34.2% had 16 years or more professional experience. The largest proportion of pharmacies were located near hospitals or healthcare facilities (33.8%), followed by street-front pharmacies (30.6%) (Table 1).
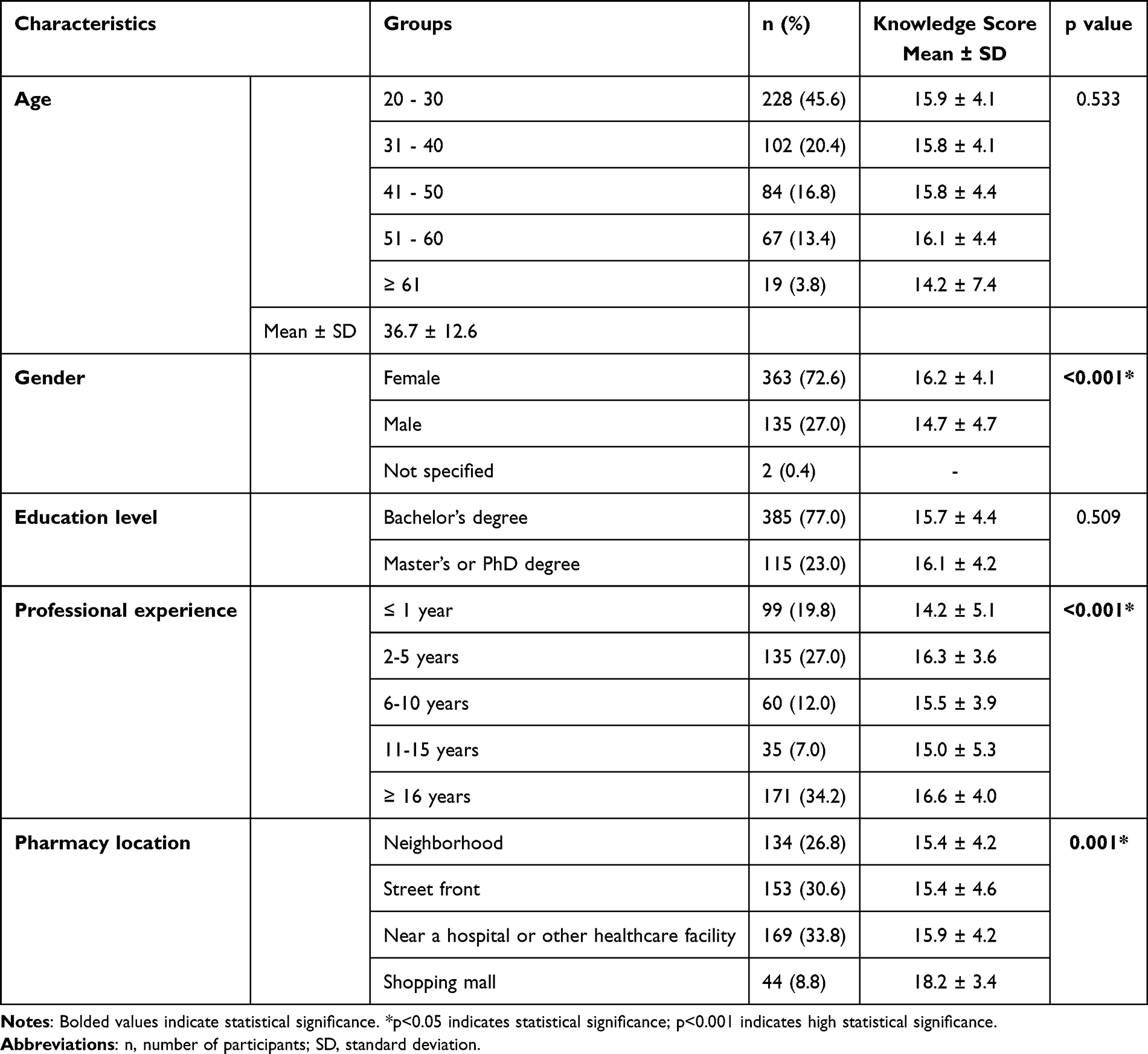 |
Table 1 Distribution of Participants Based on Demographic Characteristics, Educational Background, Professional Experience, and Pharmacy Location, Along with an Analysis of the Impact of These Demographic Variables on Participants’ Pharmacological Knowledge Levels |
Pharmacy Practices and Patient Demand
On average, pharmacists reported 2.73 weekly patient inquiries for semaglutide and 2.13 for liraglutide, with corresponding mean weekly dispensing volumes of 1.76 boxes for semaglutide and 1.38 boxes for liraglutide.
Pharmacists stated that both medications were predominantly requested for weight-loss purposes (semaglutide 82.6%, liraglutide 79.4%). A considerable proportion also reported prescription-free requests (semaglutide 62.6%; liraglutide 64.6%) and requests without any medical advice (41.8% and 35.2%, respectively). These patterns are illustrated in Figure 2.
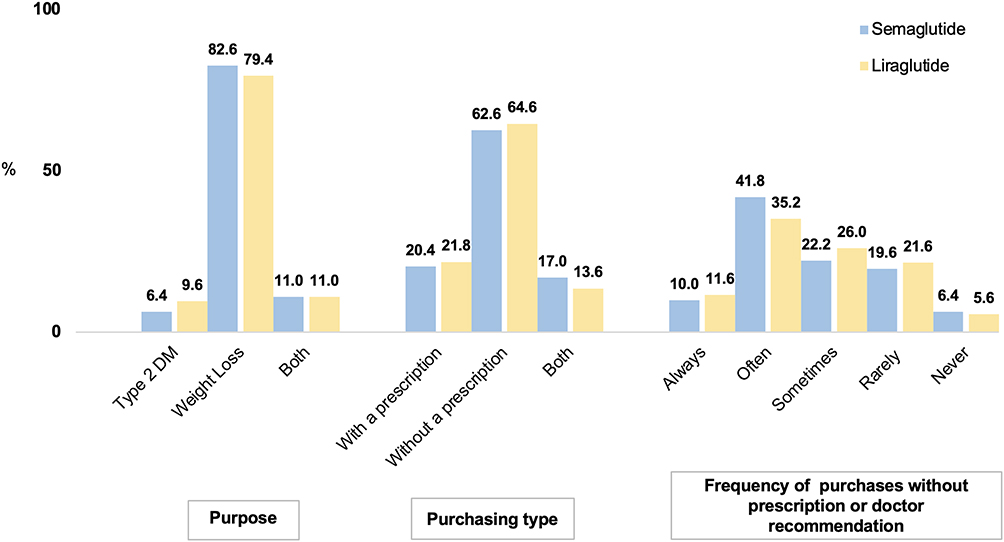 |
Figure 2 Distribution of participants based on their pharmacy practices regarding semaglutide and liraglutide. Abbreviation: DM, diabetes mellitus. |
No statistically significant association was found between pharmacy location and the intended purpose of medication use (p > 0.05). However, descriptive data indicated that pharmacies located in shopping malls more frequently reported weight-loss–related requests (97.2%), whereas neighborhood and street-front pharmacies reported requests more often related to type 2 diabetes (75.0%).
Pharmacists’ Counselling Behaviors
Pharmacists’ self-reported counselling practices varied. More than half indicated that they always explained the correct method of using injection pens (51.0%), while a small proportion (3.6%) reported never providing such information. Most respondents also stated that they regularly informed patients about timing of administration (53.2%) and storage conditions (74.2%). Regarding safety counselling, 45.6% of pharmacists reported that they “always” informed patients about potential side effects, and 45.0% stated that they routinely asked about other comorbidities or medications (Figure 3).
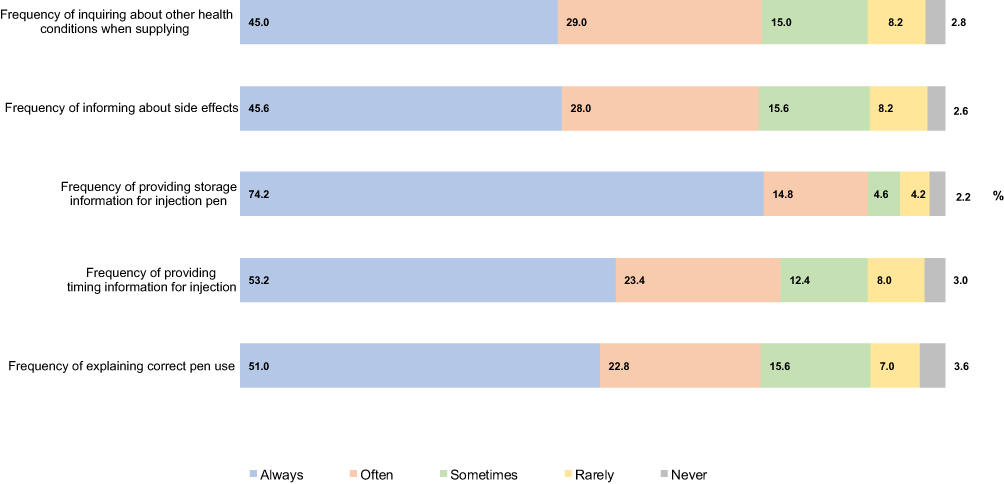 |
Figure 3 Distribution of participants’ responses regarding attitudes towards pharmacy practice. Abbreviation: n, number of participants. |
Evaluation of Participants’ Knowledge Regarding Semaglutide and Liraglutide
The internal consistency of the 25-item knowledge section was acceptable, with a Cronbach’s alpha coefficient of 0.70. Participants’ responses demonstrated notable gaps in regulatory and clinical knowledge. More than half (50.4%) incorrectly believed that the formulation of semaglutide approved for glycemic control has also been approved by the US FDA for weight loss. Similarly, 27.4% incorrectly stated that the Turkish Ministry of Health has approved this formulation for weight management. In contrast, 58.8% correctly identified that the liraglutide formulation indicated for weight loss is approved by the US FDA, and 38.2% correctly recognized its approval by the Turkish Ministry of Health. Regarding dosing knowledge, 71.0% responded “yes” to the weekly dose escalation statement for liraglutide based on a fixed titration schedule. Additionally, the majority (85.2%) correctly answered “no” to whether unused injectable pens can be stored at room temperature (25°C) (Table 2).
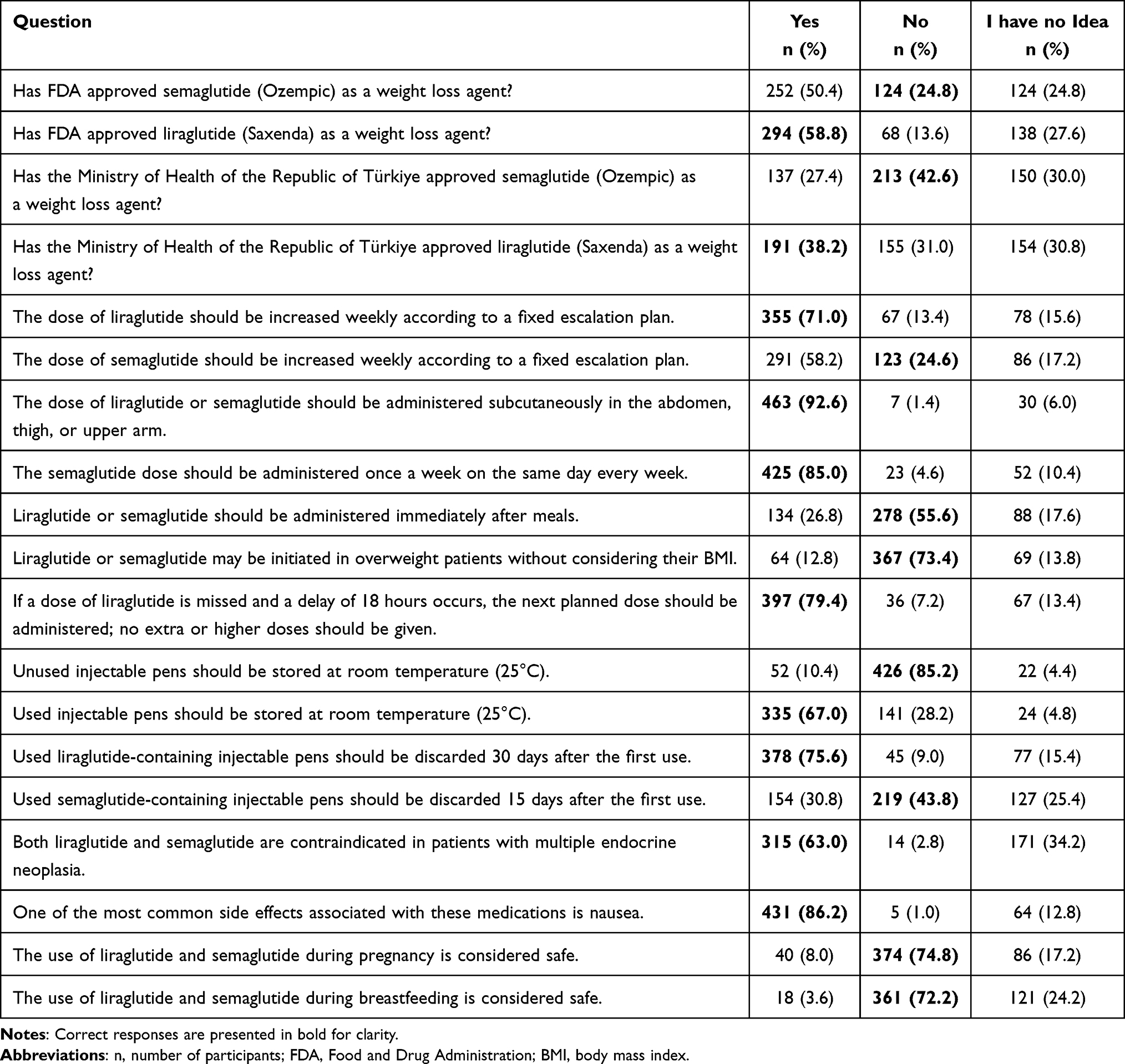 |
Table 2 Distribution of Participants According to Their Answers to Questions Related to Knowledge Levels About Liraglutide and Semaglutide |
The majority of participants correctly selected “GLP-1 receptor agonist” as the drug class for both medications, with response rates of 85.6% and 83.6%, respectively. Additionally, 22.0% of participants responded “I have no idea” when asked about the recommended starting weekly dose of semaglutide for weight loss, while 22.8% selected the same response for liraglutide (Table 3).
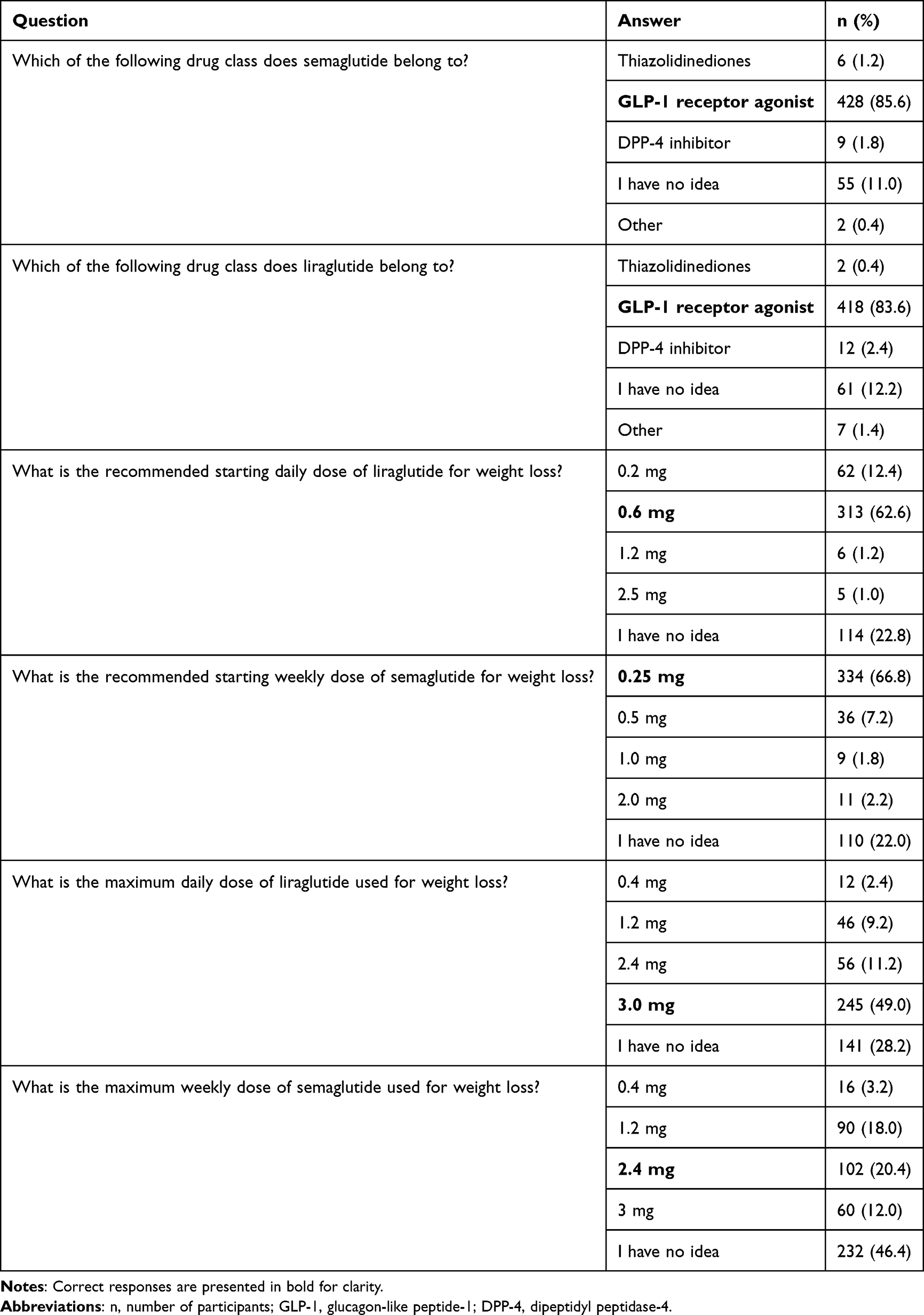 |
Table 3 Distribution of Participants Based on Their Responses to Questions Assessing Their Pharmacological Knowledge of Liraglutide and Semaglutide |
Knowledge Scores
The mean knowledge score was 15.8 ± 4.3 (range: 0–25). Female pharmacists scored significantly higher than male pharmacists (16.2 ± 4.1 vs 14.7 ± 4.7, p<0.05). A significant association was found between pharmacy location and knowledge scores (p=0.001). Pharmacists working in shopping mall pharmacies had the highest mean knowledge score (18.2 ± 3.4), whereas those in street-front, neighborhood, and near-hospital pharmacies scored lower, with no significant differences among these groups (Table 1). Professional experience also influenced knowledge scores (p < 0.001). Pharmacists with ≥16 years of experience scored significantly higher compared with pharmacists with <1 year or 11–15 years of experience, while those with 2–5 years of experience scored higher than those with <1 year.
Participants’ Perceptions of Misuse of Liraglutide and Semaglutide
A substantial proportion of pharmacists perceived misuse, with 61.4% reporting concerns about semaglutide and 60.2% expressing similar concerns for liraglutide. One-way ANOVA revealed a significant association between knowledge scores and perceptions of misuse (p < 0.05), and post hoc analysis showed significant differences between participants who responded “yes” and those in the “other” category. Additionally, 60.8% reported that they had not encountered attempts to obtain these medications illegally.
Discussion
This study provides comprehensive insights into community pharmacists’ knowledge, attitudes, and professional practices regarding the use of liraglutide and semaglutide for weight management. Pharmacists reported substantial patient interest in both medications, frequently motivated by weight-loss expectations and often occurring without prescriptions or medical recommendations. Although many pharmacists reported providing counselling on administration, safety, and storage, notable gaps were identified in regulatory awareness, dosing knowledge, and consistency across counselling domains. Differences in knowledge scores based on gender, professional experience, and pharmacy setting, as well as high levels of perceived misuse, further highlight the complexity of pharmacists’ roles in guiding the rational use of GLP-1 receptor agonists. These findings indicate that targeted educational strategies focusing on regulatory approval status, dosing schedules, and approved indications may help address the specific knowledge gaps identified in this study.
The increased demand observed in the present study aligns with global patterns indicating heightened public interest in GLP-1 receptor agonists for weight loss. Infodemiology analyses have shown that interest in semaglutide for cosmetic or rapid weight loss has risen sharply, driven in part by online trends and non-medical information sources.10 Similar concerns about inappropriate or unsupervised use have emerged in pharmacovigilance reports, where non-indicated use and safety issues were frequently noted.11 These patterns reinforce the need for consistent pharmacist-led education and monitoring—an area where our findings indicate both strengths and areas for improvement.
In this study, the mean knowledge score of 15.8 ± 4.3 out of 25 indicates a moderate understanding among pharmacists, consistent with findings from Saudi Arabia, where similar educational gaps were noted.23 Studies from high-income countries also reflect knowledge deficiencies, even among trained professionals. A US study emphasized the importance of continuous education to address gaps in prescribing and patient counseling on GLP-1 agonists.24 This suggests a global need for updated training on the evolving indications of these agents. Gender and experience were significant factors in knowledge variation. Female and more experienced pharmacists performed better overall, aligning with previous research.25,26 Interestingly, younger pharmacists scored higher on drug-specific items, possibly reflecting exposure to updated curricula, similar to previous findings showing recent graduates better understood administration techniques.19 These findings suggest that professional development initiatives may benefit from being tailored according to pharmacists’ experience levels, with differentiated training approaches addressing both foundational regulatory knowledge and evolving clinical practices.
Over 60% of participants believed that these medications were being misused for weight loss. This aligns with international studies: in Jordan, public support for unsupervised use of GLP-1 agents was reported.16 The FAERS database has raised concerns about semaglutide misuse, with Chiappini et al identifying it as a high-risk substance for off-label abuse.11 In Denmark, semaglutide was reportedly prescribed for non-diabetic patients before obesity-specific approval.12 In Türkiye, media and social media have likely fueled public demand despite the unavailability of the obesity-specific formulation. Also, in the current study, most pharmacists reported high demand for semaglutide and liraglutide for weight loss, often without prescription. Although their effectiveness—especially semaglutide’s superior weight loss outcomes—partly explains this, it also raises public health concerns.6 High demand may be enabling inappropriate access and use in ineligible populations. These results highlight the need for clearer regulatory guidance and practical support tools to assist pharmacists in managing off-label requests and mitigating potential misuse.
Consistent with the literature, our findings demonstrate that pharmacists play an essential frontline role in guiding patients about appropriate administration, storage conditions, and potential adverse effects.13,14 Only about half of the pharmacists consistently provided counseling on injection technique, storage, and administration timing; even fewer addressed potential side effects. These rates are lower than international benchmarks. For instance, US pharmacists routinely counsel on GLP-1 use, including adverse effect management.27 Reduced counseling here may reflect workload or regulatory barriers. Standardized counselling frameworks or checklists may therefore help ensure more consistent delivery of key safety and administration information across different practice settings.
The high proportion of pharmacists reporting requests without prescriptions raises additional ethical and legal concerns. In Türkiye, prescribing regulations for these medications are clear, yet consumer-driven demand may place pharmacists in challenging positions when balancing patient expectations against rational and evidence-based dispensing. Similar challenges have been reported internationally, where pharmacists express discomfort when patients request GLP-1 receptor agonists solely for weight loss or without meeting approved criteria.16 Taken together, these findings highlight the need for enhanced pharmacist training in obesity management, comprehensive counselling on GLP-1 receptor agonists, and improved public awareness regarding appropriate use. As these medications continue to gain widespread attention, supported by robust clinical evidence demonstrating their efficacy for chronic weight management ensuring safe, equitable, and evidence-based access becomes increasingly important.4–6 Community pharmacists are in a key position to reduce misuse by reinforcing correct indications, monitoring potential adverse effects, and providing guideline-based patient counselling. Empowering pharmacists with clear practice-oriented guidance may strengthen their ability to navigate ethical dilemmas and uphold evidence-based dispensing practices.
This study has several limitations that should be acknowledged. First, the use of convenience sampling restricts the generalizability of the findings to all community pharmacists in Türkiye, as those who participated may differ from pharmacists who declined or were not reached. Second, the reliance on self-reported data introduces potential recall and social desirability biases, which may have led some participants to overestimate their counselling practices or knowledge levels. Third, the cross-sectional design precludes any causal interpretations between pharmacists’ characteristics and their knowledge or behaviours. Additionally, the study did not include observational or objective assessments of counselling performance, which may not fully align with pharmacists’ self-reported practices. Finally, although the sample size was large and geographically diverse, it may not fully capture regional variations in patient demand, prescribing patterns, or pharmacy workflows across all provinces in Türkiye.
Conclusion
This study highlights the essential role of community pharmacists in Türkiye in supporting the safe and rational use of liraglutide and semaglutide. While pharmacists demonstrate moderate knowledge and active engagement in patient counselling, the findings reveal persistent challenges related to off-label demand, prescription-free requests, and variability in counselling practices. Differences in knowledge across pharmacy settings and experience levels further emphasize the need for targeted professional development. Strengthening pharmacist education, updating clinical guidance, and enhancing public awareness regarding appropriate use of GLP-1 receptor agonists may contribute to reducing misuse and promoting more effective obesity and diabetes management in Türkiye.
Data Sharing Statement
The data supporting this research are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study received approval from the Acibadem Mehmet Ali Aydinlar University Medical Research Ethics Committee (Decision No: 2024-19/703). The participants provided written informed consent. Only the pharmacists who gave consent were included in the study. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Author Contributions
Conceptualization: DBO, ED; Methodology: DBO, ED, YS; Formal analysis: YS; Data curation: DBO, YS; Writing – original draft: DBO, ED; Writing – review & editing: DBO, ED, YS. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work has been supported by Acibadem Mehmet Ali Aydinlar University Scientific Research Projects Coordination Unit under grant number # TLO-2025-2276.
Disclosure
Dilara Bayram-Ozgur reports grants from Acibadem Mehmet Ali Aydinlar University Scientific Research Projects Coordination Unit during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Lingvay I, Cohen RV, le Roux CW, Sumithran P. Obesity in adults. Lancet. 2024;404(10456):972–13. doi:10.1016/S0140-6736(24)01210-8
2. Abdelaal M, le Roux CW, Docherty NG. Morbidity and mortality associated with obesity. Ann Transl Med. 2017;5(7):161. doi:10.21037/atm.2017.03.107
3. Kinlen D, Cody D, O’Shea D. Complications of obesity. QJM. 2018;111(7):437–443. doi:10.1093/qjmed/hcx152
4. Xie Z, Yang S, Deng W, Li J, Chen J. Efficacy and safety of liraglutide and semaglutide on weight loss in people with obesity or overweight: a systematic review. Clin Epidemiol. 2022;14:1463–1476. doi:10.2147/CLEP.S391819
5. Mehta A, Marso SP, Neeland IJ. Liraglutide for weight management: a critical review of the evidence. Obes Sci Pract. 2017;3(1):3–14. doi:10.1002/osp4.84
6. Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMoa2032183
7. Turkish Medicines and Medical Devices Agency (TMMDA). Summary of product characteristics – Liraglutide 6 mg/mL solution for injection (pre-filled pen). Ankara: TMMDA; 2024. Available from: https://titck.gov.tr/storage/Archive/2025/kubKtAttachments/saxendakubtemiz_10_03_2025.pdf.
8. Turkish Medicines and Medical Devices Agency (TMMDA). Summary of product characteristics – Ozempic 0.5 mg solution for injection in pre-filled pen. Ankara: TMMDA; 2024. Available from: https://titck.gov.tr/storage/Archive/2023/kubKtAttachments/ozempic0.5kubtemiz_ac5c506-4191-4f47-8ed4-c9b36dec0055.pdf.
9. Turkish Medicines and Medical Devices Agency (TMMDA). Wegovy 0.5 mg solution for injection in pre-filled pen – summary of product characteristics (SmPC). Ankara: TMMDA; 2025. Available from: https://titck.gov.tr/storage/Archive/2025/kubKtAttachments/WEGOVY0.5KB_17_02_2025.pdf.
10. Han SH, Safeek R, Ockerman K, et al. Public interest in the off-label use of glucagon-like peptide 1 agonists (Ozempic) for cosmetic weight loss: a Google Trends analysis. Aesthet Surg J. 2023;44(1):60–67. doi:10.1093/asj/sjad211
11. Chiappini S, Vickers-Smith R, Harris D, et al. Is there a risk for semaglutide misuse? Focus on the Food and Drug Administration’s FDA Adverse Events Reporting System (FAERS) pharmacovigilance dataset. Pharmaceuticals. 2023;16(7):994. doi:10.3390/ph16070994
12. Callaghan T, Motta M, Stein M, Goidel K. The prevalence and consequences of support for off-label Ozempic prescriptions. Health Econ Policy Law. 2025;1–14. doi:10.1017/S1744133124000306
13. Supsongserm P, Thin SM, Nerapusee O, Sorofman BA, Watcharadamrongkun S, Kittisopee T. Factors contributing to pharmacists’ intention to provide weight management service in community pharmacy settings: a systematic review. Pharm Pract. 2023;21(2):2790.
14. Hijazi MA, Shatila H, El-Lakany A, Al Rifai H, Aboul-Ela M, Naja F. Role of community pharmacists in weight management: results of a national study in Lebanon. BMC Health Serv Res. 2020;20(1):386. doi:10.1186/s12913-020-05258-7
15. Liu B, Wu X, Zou X, Sheng J, Yu J. Knowledge, attitude and practice toward liraglutide and semaglutide among endocrinology medical staff. Sci Rep. 2025;15(1):11533. doi:10.1038/s41598-025-96545-y
16. Abutaima R, Barakat M, Sawan HM, Al Omari SM, Mhaidat NM. Knowledge, attitudes, and practices towards the use of GLP-1 receptor agonists for weight loss among the general population in Jordan: a cross-sectional study. PLoS One. 2024;19(12):e0314407. doi:10.1371/journal.pone.0314407
17. Cochran WG. Sampling Techniques.
18. Fidan Ü, Türker M, Durak Albayrak Ö. Eczanelerde Ekonomik ve Finansal Durum Araştırması. TEB Yayınları; 2019. Available from: https://www.teb.org.tr/versionsView/1248.
19. Al-Samiry AH, Mohammed SI, Khalaf NM. Proficiency and knowledge of community pharmacists in the use of liraglutide and semaglutide as weight reduction agents. Al-Rafidain J Med Sci. 2024;6(1):20–24. doi:10.54133/ajms.v6i1.413
20. Peterson GE, Pollom RD. Liraglutide in clinical practice: dosing, safety and efficacy. Int J Clin Pract. 2010;64(167):35–43. doi:10.1111/j.1742-1241.2010.02498.x
21. Pillarisetti L, Agrawal DK. Semaglutide: double-edged sword with risks and benefits. Arch Intern Med Res. 2025;8(1):1–13. doi:10.26502/aimr.0189
22. Hair J, Alamer A. Partial least squares structural equation modeling (PLS-SEM) in second language and education research: guidelines using an applied example. Res Methods Appl Linguist. 2022;1(3):100027. doi:10.1016/j.rmal.2022.100027
23. Alhomoud IS, Aldakhil SA, Alhosan RF, et al. Knowledge, counseling practice, perceived barriers, and clinical decision-making of community pharmacists in Saudi Arabia regarding glucagon-like peptide-1 receptor agonists and sodium-glucose cotransporter 2 inhibitors. Diabetes Metab Syndr Obes. 2025;18:3093–3107. doi:10.2147/DMSO.S552287
24. Garvey WT, Mahle CD, Bell T, Kushner RF. Healthcare professionals’ perceptions and management of obesity & knowledge of glucagon, GLP-1, GIP receptor agonists, and dual agonists. Obes Sci Pract. 2024;10(3):e756. doi:10.1002/osp4.756
25. Aldhobaib AY, Rabbani SI, Mobark MA. Knowledge, attitude and practice about a newer class of antidiabetic drug (glucagon-like peptide-1 receptor agonist) among the health care professionals of Qassim University, Saudi Arabia. J Pharm Res. 2021;20(4):58–66. doi:10.18579/jopcr/v20i4.MS21083
26. Keijsers CJ, Leendertse AJ, Faber A, Brouwers JR, de Wildt DJ, Jansen PA. Pharmacists’ and general practitioners’ pharmacology knowledge and pharmacotherapy skills. J Clin Pharmacol. 2015;55(8):936–943. doi:10.1002/jcph.500
27. Meece J. The role of the pharmacist in managing type 2 diabetes with glucagon-like peptide-1 receptor agonists as add-on therapy. Adv Ther. 2017;34(3):638–657. doi:10.1007/s12325-017-0491-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.