")
Back to Journals » Infection and Drug Resistance » Volume 16
Community-Acquired Urinary Tract Infection Among Sexually Active Women: Risk Factors, Bacterial Profile and Their Antimicrobial Susceptibility Patterns, Arba Minch, Southern Ethiopia
Authors Seid M, Markos M, Aklilu A , Manilal A, Zakir A, Kebede T, Kulayta K, Endashaw G
Received 17 February 2023
Accepted for publication 7 April 2023
Published 18 April 2023 Volume 2023:16 Pages 2297—2310
DOI https://doi.org/10.2147/IDR.S407092
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Mohammed Seid,1 Mesafint Markos,1 Addis Aklilu,1 Aseer Manilal,1 Abdurezak Zakir,1 Teshome Kebede,2 Kebede Kulayta,3 Gessila Endashaw4
1Department of Medical Laboratory Science, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 2Arba Minch General Hospital, Arba Minch, Ethiopia; 3Department of Medical Laboratory Science, Arba Minch College of Health Sciences, Arba Minch, Ethiopia; 4Department of Nursing, Arba Minch University, Arba Minch College of Health Sciences, Arba Minch, Ethiopia
Correspondence: Mohammed Seid, Email [email protected]
Background: Globally, urinary tract infections (UTIs) are a common health issue among women. Investigating risk factors associated with culture-proven UTIs and the antimicrobial resistance profile of uropathogens would provide insight into planning prevention and control measures.
Objective: To identify the risk factors associated with UTIs among sexually active women and determine antimicrobial susceptibility patterns of uropathogenic bacterial isolates.
Methods: A case-control study was conducted from February to June 2021, involving 296 women (62 case group and 234 control group in a ratio of 4:1). Cases were defined as culture-confirmed UTIs, and controls were non-UTIs. A semi-structured questionnaire was used to collect demographic, clinical, and behavioral data. The antimicrobial susceptibility test was done by the Kirby-Bauer disc diffusion method. The data were analyzed using SPSS version 25. Bivariable and multivariable logistic regressions were used to identify risk factors, and the strength of association was measured by adjusted odds ratios and a 95% confidence interval used at P-values < 0.05.
Results: The results revealed that recent coitus and frequency of coitus more than three times per week (P=0.001) were independent predictors of UTIs. Swabbing from back to front, a history of UTI and a delay in voiding were also independent predictors (P < 0.05). On the other hand, a daily water intake of 1 to 2 litres reduced the risk of UTI (P= 0.001). The predominant uropathogenic isolate was Escherichia coli (35.48%). Over 60% of isolates were resistant to cotrimoxazole, penicillin, cephalosporin, and fluoroquinolones. The most effective antibiotics included piperacillin-tazobactam, aminoglycosides, carbapenem, and nitrofurantoin. 85% and 50% of isolates were MDR and ESBL producers, respectively.
Conclusion: The finding indicates the importance of public intervention targeting the identified risk factors and the resistance phenotype to reduce the burden of UTIs with antimicrobial resistance in the study area.
Keywords: risk factors, adolescents and young women, bacteriuria, symptomatic UTIs, uropathogens, antimicrobial resistance, ESBL producing, case-control, Ethiopia
Introduction
Urinary tract infection is one of the most pressing problems confronting the global healthcare system, and it is significantly more prevalent in women.1,2 It is evident that by the age of 24, one-third of women would experience at least one episode of UTI requiring antimicrobial treatment, and 40 to 50% of them would experience at least one episode of UTI during their lifetime.3 On the other hand, recurrent UTIs necessitate multiple clinical visits and antimicrobial treatment in 25 to 50% of women.4,5 The treatment of UTIs is estimated to account for 15% of all antimicrobial use in humans. The management of UTIs has become a public health concern due to the emergence of drug-resistant uropathogens.6,7 Among the various risky subpopulations, adolescent and young adult women are particularly vulnerable to developing UTIs.
Nevertheless, it is difficult to accurately estimate the incidence of UTIs since they are not reportable diseases. The problem may be further complicated because, in most outpatient settings, a positive urine culture result is not required to diagnose based on symptoms.8 However, studies indicate that despite UTI symptoms, women do not seek medical intervention. Therefore, the accurate picture of UTIs is likely to be underestimated in the literature.9
The pathogenesis of UTIs in sexually active young women is intricate and is influenced by several host-related biological and behavioral factors and the virulence of the uropathogens.10 A variety of bacterial pathogens cause UTIs, predominantly Escherichia coli (80–90%), followed by Staphylococcus saprophyticus (5–16%).6,7 Besides, other faecal pathogens, including Klebsiella pneumoniae, Proteus mirabilis, and Enterococcus faecalis, have also been implicated.11,12 In addition, the emerging multidrug-resistant uropathogens (including the extended-spectrum beta-lactamase (ESBL) producers and carbapenem-resistant Enterobacteriaceae) are imposing the most significant challenge on public health worldwide.7,13 The negative consequences of UTIs extend beyond the clinical and economic burdens of the illness and include the personal, social, and psychological effects that hurt the quality of life.6 Besides, managing UTIs has been further complicated due to the emergence of drug-resistant uropathogens.9
With all these in mind, the main objective of this case-control study is to identify risk factors affecting the prevalence of culture-confirmed UTIs among sexually active women attending outpatient clinics of the title hospital in Arba Minch, southern Ethiopia. In addition, as a secondary objective, the study determined the bacterial profile and antimicrobial susceptibility pattern among the case group.
Materials and Methods
Study Setting and Design
This case-control study was conducted from February 1 to July 31, 2021, in the Arba Minch General Hospital, Arba Minch, southern Ethiopia. The hospital has 200 beds and more than 251 health professionals, providing preventive, curative, and rehabilitative services for the population of 200,747.
Study Participants
All young and adolescent women who visited Arba Minch General Hospital were the source population. Therefore, the study population comprised sexually active women (adolescents and young women) aged 15–24.
The case group consisted of 62 participants with culture-confirmed UTs. Culture-confirmed UTIs were defined as the presence of significant bacteriuria as per the Kass count (ie, > 105 colony-forming units (CFU)/mL in the mid-stream urine culture) in conjunction with one or more symptoms of UTI (frequency, urgency, dysuria, hematuria, fever (>38°C), chills, or back or flank pain, vomiting, or nausea) as per the guidelines.14
Control Group
A total of 234 adolescents and young women attending the title hospital for non-UTI reasons were selected by a systematic random sampling technique. Participants were selected at the interval of the Kth unit, among them attending each service unit. They were recruited from the source population, from which the cases arose at the same time interval. For every case, four controls of a similar age (within 5 years) were included.
Sample Size Determination and Sampling Techniques
The sample size was computed for an unmatched case-control study by OpenEpi version 3.03 using a double population proportion formula. The sample size was calculated with the following assumptions: a 95% confidence interval (Zα/2 = 1.96), a case-to-control ratio of 1:4, the proportion of women who had sexual intercourse for more than three times per week in the control group (0.20) as reported previously,15 and 90% power (Z β = 1.28) to detect a three-fold risk difference between the case and the control groups. The final sample size was calculated to be 282 (57 cases and 225 controls); after adding a 5% non-response rate, the final sample size was consolidated as 296 (62 cases and 234 controls).
Eligibility
The inclusion criteria for both groups were: 14 to 24 years; and provided written informed consent or age-specific assent collected from the guardian. However, subjects who were pregnant, had urinary tract anomalies, were currently menstruating, were admitted for more than 72 hrs., were on the course of antibiotics within the last weeks before the beginning of the study, were severely ill, had asymptomatic bacteriuria, and diabetics were excluded.
Ascertainment of Outcome and Assessment of Exposure
The primary outcome variable in this study was a culture-confirmed symptomatic UTI. Exposures of interest in this study were sexual behaviour, hygiene habits, birth control methods, and hydration status of the body in the previous 4 weeks. The timeframe of four months was chosen because it was most relevant to UTI risk and minimized recall issues.
Data Collection Procedures
A standard, pre-tested, semi-structured questionnaire was developed after a comprehensive literature review16–18 for data collection. The data was collected by trained collectors closely overseen by supervisors. The information on sexual behaviour covered in this study included the following questions: 1) During the last year, have you ever had coitus? (ie, vaginal or anal). (The variable was dichotomized as yes and no.); 2) When was your most recent coitus? (within the last month or so); 3) In response to the above questions: At your last time of coitus, did you micturate rapidly after sex? (within 15 minutes) (yes and no.); 4) Does your partner wash his genitals before coitus? (yes, usually/sometimes and no, occasionally/never); 5) Sexual intercourse frequency was assessed using the following questions: How often do you have coitus? (per week in the previous 30 days). Do you have a habit of delaying micturating voluntarily? (usually, sometimes, occasionally, and never). Participants were also asked to provide the amount of daily water consumption (less than 1 litre, 1–2 liters, or above 2 litres).
Laboratory Analysis
Urine Specimen Collection and Processing
Ten to twenty mL of first voided midstream urine samples were collected under aseptic conditions into 50 mL of sterile FalconTM tubes. Collected samples were labelled and immediately transported at ambient temperature within 2 hours to the Medical Microbiology and Parasitology Laboratory following appropriate safety precautions and standard operating procedures.19
Cultivation and Identification of Bacterial Isolates
Urine samples were plated directly onto a series of media such as 5% sheep blood agar, cysteine-lactose electrolyte deficient agar and MacConkey agar using calibrated loops (0.01 mL). The plates were incubated aerobically at 35–37°C for 24–48 hours. Following incubation, plates were inspected for bacterial growth. According to Kass count, the samples with prominent bacterial growth were considered culture-positive.19 Results interpretation: if the pure culture is at a concentration of 105 colony forming units (CFU)/mL and for cultures containing two organisms, one in low numbers (10,000 CFU/mL) and the other over 10,000 colonies, sub-culture was done for the dominant organism assuming organism in lower numbers is unlikely to be causing disease. Samples with a significant colony count were further processed for isolation and identification using colony morphology, Gram staining, and biochemical reactions.19
Antimicrobial Susceptibility Testing
The antibiotic susceptibility test was carried out on Mueller Hinton agar by adopting the Kirby-Bauer disk diffusion method according to the CLSI (Clinical and Laboratory Standards Institute) guidelines.20 Isolates were tested against the following antimicrobial agents: erythromycin (15 µg), ceftriaxone (30 µg), cefotaxime (30 µg), ceftazidime (30 µg), cefepime (30 µg), ampicillin (10 µg), piperacillin (100 µg), piperacillin-tazobactam (110 µg), amoxicillin-clavulanic acid (20/10 µg), tetracycline (30 µg), linezolid (30 µg), levofloxacin (5 µg), norfloxacin (10 µg), ciprofloxacin (5 µg), imipenem (10 µg), meropenem (10 µg)), nitrofurantoin (300 μg), vancomycin (30µg) and trimethoprim-sulfamethoxazole (1.25/23.75 μg). Categorization of antimicrobial susceptibility results as susceptible, intermediate, or resistant and detection of ESBL producers by disc synergy test was done as per the standard procedures.20 In this study, multi-drug resistance (MDR) was extrapolated as the resistance of at least three or more different classes of antibiotics.21
Quality Control and Data Quality Assurance
Strict measures were taken from the pre-analytical to the post-analytical phase. The questionnaire was pretested, and laboratory analyses were conducted using standard operating procedures. Culture media was tested for sterility and performance by incubating 5% of the batch. The quality of culture media was tested by using quality control strains such as Staphylococcus aureus (ATCC 25923), Escherichia coli (ATCC 25922) and P. aeruginosa (ATCC 27853).
Data Management and Statistical Analysis
Data were analyzed using IBM Statistical Package for Social Science (SPSS) version 25 (IBM, USA). Descriptive statistics of the basic demographic data were generated for the overall study participants enrolled in the study and the groups identified as cases and controls. We checked differences between groups for categorical variables with chi-square tests or Fisher’s exact tests and for continuous variables with Student’s t-tests or Mann–Whitney tests with a significance level of alpha = 0.05. Both bivariable and multivariable logistics were used to estimate crude and adjusted odds ratios with 95% confidence intervals for the association between risk factors and UTI. Bivariable conditional logistic regression for each variable was analyzed, and any risk factors with (a P-value < 0.25) were considered a candidate for multivariable logistic regression. The final model was selected considering the highest level of explicative ability measured by PseudoR2. Finally, the estimated adjusted odds ratios (OR; 95% confidence interval) were used to ascertain the degree of association between independent variables and UTI. All tests were two-tailed, and a P-value of less than 0.05 was considered statistically significant.
Ethical Consideration
The study was conducted in accordance with the ethical principle of the declaration of Helsinki. The study was approved by the Institutional Research Ethics Review Board of the College of Medicine and Health Science of Arba Minch University (Ref. AMU/9/31/42). All participants were informed about the objective and purpose of the study, and written/verbal informed consent was obtained from each participant. For participants under 18, an age-specific equivalent form (assent) was used to obtain informed consequences from the guardian or family. There was no risk associated with the process of urine sample collection or interviewing participants. The data collected during laboratory screening or interviewing were kept confidential. Positive cultures were informed to the physician for immediate care.
Results
Population Characteristic
After applying eligibility criteria, a total of 296 study participants were enrolled (ie, 62 culture-confirmed cases of UTIs and 234 women without UTIs), with a response rate of 100%. The mean age of the study participants was 20.75±5.1. 75.8% were urban dwellers (73.07% in the case group and 59.67% in the control group). In addition, 20.96% of the cases and 27.3% of the control group are comprised of individuals pursuing a diploma or higher level of education.
A greater proportion (ie, 40.32%) of the case group participants had a history of UTIs than the control group (28.63%). Overall, 53.4% of women had sexual intercourse within the past three months (case group: 50.58% and control group: 50.58%). Recent sexual intercourse (within the past 30 days) was reported frequently among the case group (54.84%). Women with multiple sexual partners were 29.02 and 24.12% in the cases and controls, respectively. Engaging in sexual intercourse three or more times per week was reported by 87.09% of participants in the cases and 60% in the control group. The rate of contraceptive use was 26.9% in the case group and 22.7% in the control group. The chi-square test of independence showed no significant difference between the case and control groups (P > 0.05). Details on the participant’s characteristics are shown in Table 1.
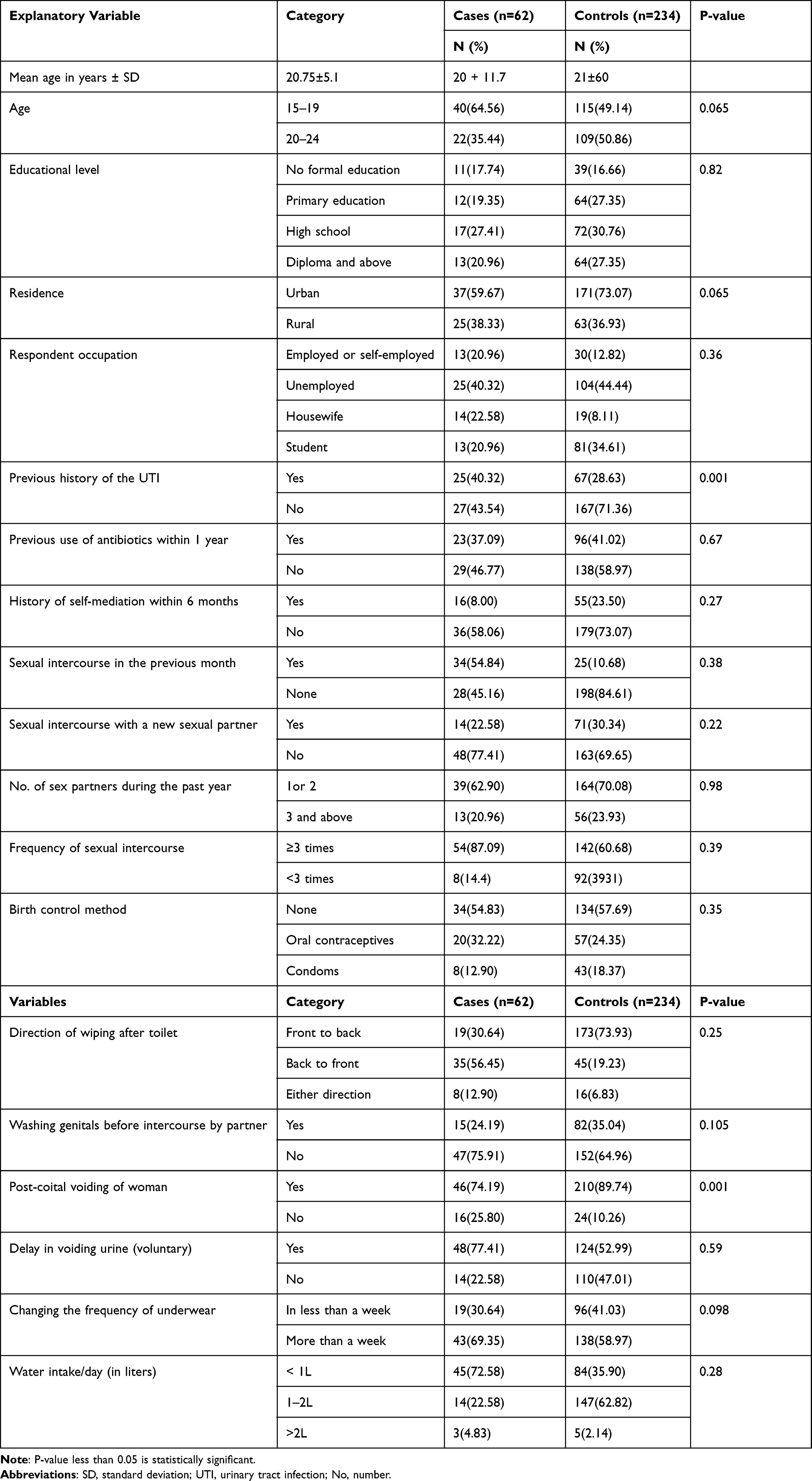 |
Table 1 Soci-Demographic and Hygiene and Behavioural Characteristics of Study Participants in the Case Group (n=62) and Control Group (n=234), Southern Ethiopia, 2021 |
Bacterial Profile of UTIs
Among the diverse bacterial uropathogens, 75.81% were Gram-negative bacilli, whereas 21.19% were Gram-positive cocci. Candida albicans were identified in two participants. The ranking of identified bacteria in decreasing order was: E. coli (35.48%), K. pneumoniae (20.97%), S. saprophyticus (16.13%), P. mirabilis (11.29%), S. aureus and P. aeruginosa (each 4.84%) and Enterobacter species, and Enterococcus species (each 3.23%). Of the culture-positive samples, species of Enterobacteriaceae were generally observed to be the predominant group (72.58%) (Table 2).
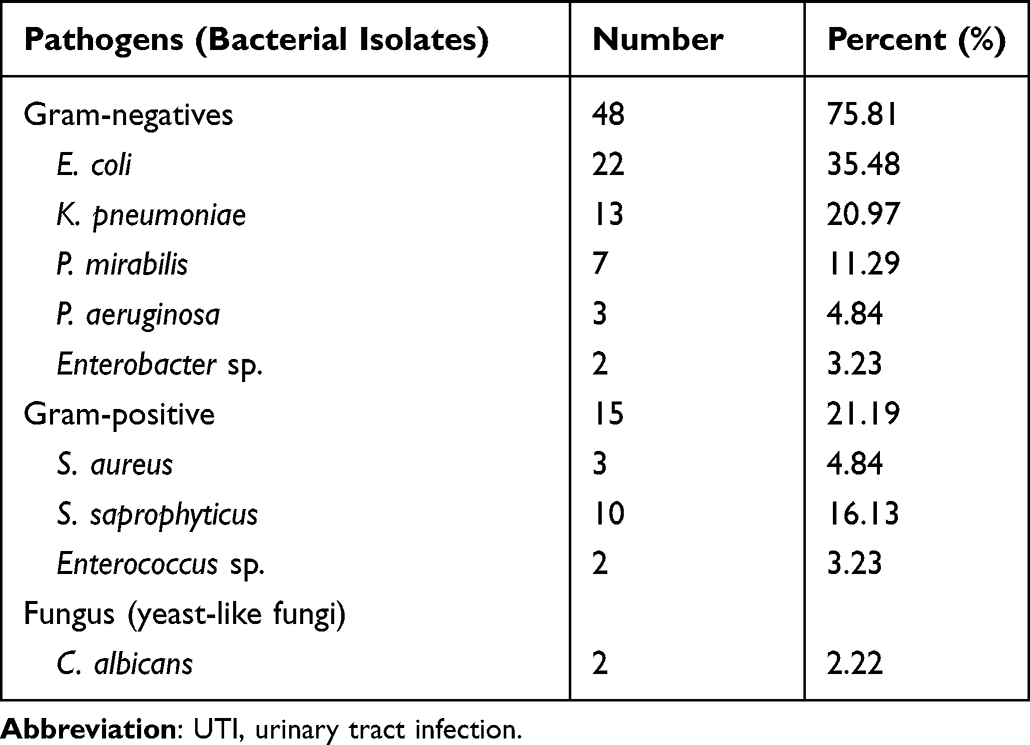 |
Table 2 Bacteria Isolated from Culture-Confirmed UTIs Among Sexually Active Women Attending Arba Minch General Hospital, Southern Ethiopia (February – July 2021) |
Antimicrobial Susceptibility Patterns
The antimicrobial susceptibility profile of all the bacterial isolates is shown in Table 3 and Table 4. The percentage of resistance to at least one or more antimicrobials was 77.41% (n = 48). The overall resistance towards antimicrobial has been detected for all first-line and second-line antimicrobials agents, and cotrimoxazole, penicillin cephalosporins, and fluoroquinolones were the class of antimicrobials for which the observed resistance ranges from 25% to 88.6%. The observed resistance to penicillin-class drugs was 88.63%. Of which resistance to ampicillin was 82.22%, to piperacillin and penicillin G was 86.66%, whereas resistance for cephalosporin class drug was 76.19%, 76.19%, and 36.17% to cefuroxime, ceftriaxone, and cefepime, respectively. With regard to the beta-lactamase inhibitors combination class, isolates resistant to amoxicillin/clavulanic acid and piperacillin/tazobactam were 61.36% and 48.88%, respectively. The resistance level to fluoroquinolone drugs was: 65.95 to 66.66% to ciprofloxacin and 59.57% to 66.66% to norfloxacin, but resistance to levofloxacin was only 25.53%. Regarding the most effective antimicrobials, nitrofurantoin, linezolid, amikacin, imipenem, and meropenem retained the highest percentage of the susceptible agent with the low level of resistance, corresponding to 31.42, 6.66, 12.76, 12.76 and 8.51%, respectively (Table 3 and Table 4).
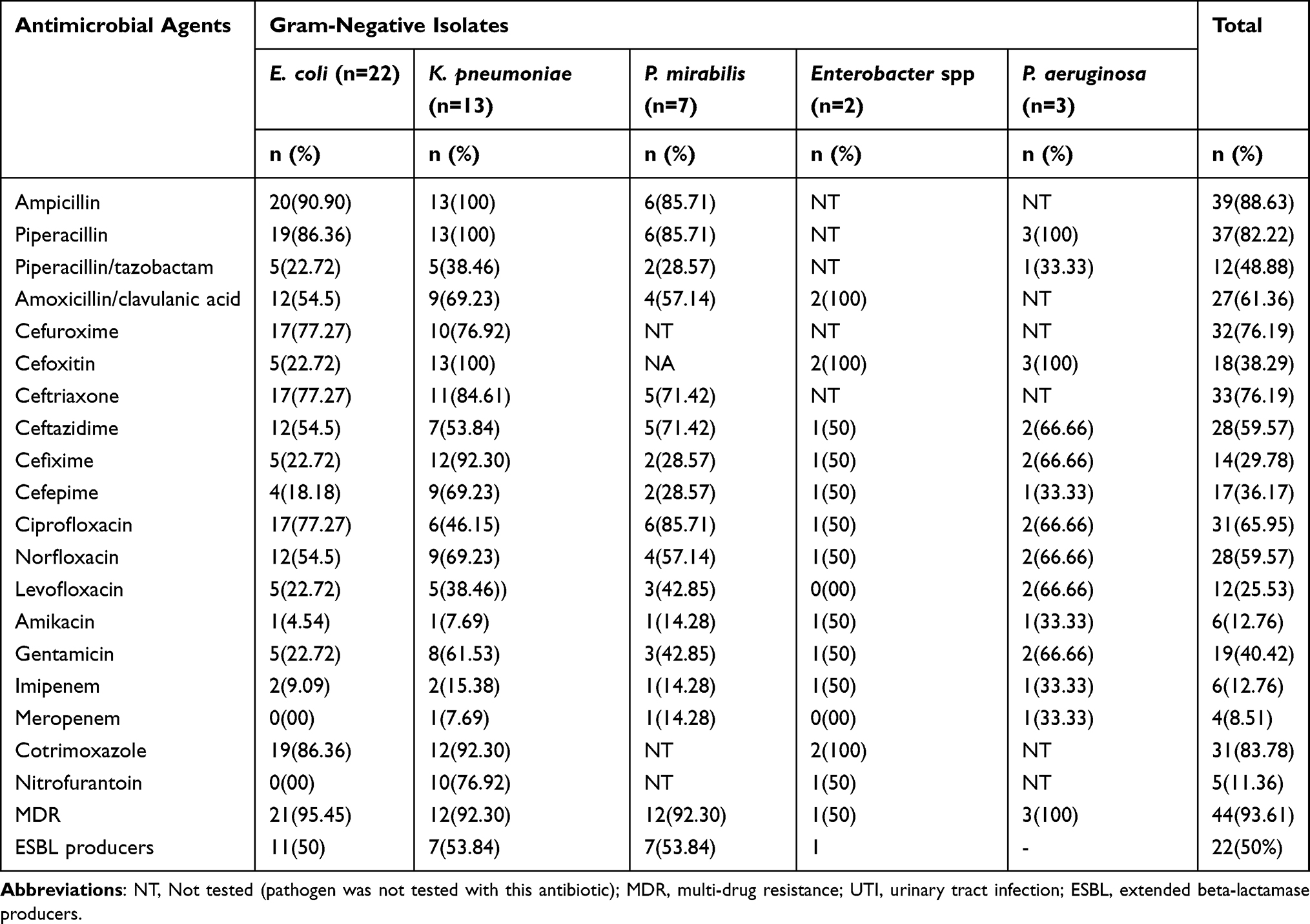 |
Table 3 Antimicrobial Susceptibility Pattern of Gram-Negative Bacteria Isolated from Culture-Confirmed UTIs Among Sexually Active Women Attending Arba Minch General Hospital, Southern Ethiopia (February – July 2021) |
 |
Table 4 Antimicrobial Susceptibility Pattern of Gram-Positive Bacteria Isolated from Culture-Confirmed UTIs Among Sexually Active Women Attending Arba Minch General Hospital, Southern Ethiopia (February – July 2021) |
Concerning specific Gram-negative isolates, E. coli and P. mirabilis showed high resistance levels to penicillin-class, such as 88% for ampicillin, 60% for each piperacillin, and 50% for amoxicillin-clavulanic acid. About 80% of isolates, including E. coli, K. pneumoniae, P. mirabilis, and Enterobacter sp., were resistant to third-generation cephalosporins, ceftriaxone, and ceftazidime, whereas cefoxitin and cefixime were relatively active cephalosporin compounds. A similar picture of moderate resistance was noted against gentamicin (40.42%) and levofloxacin (25.53%). Invariably, all the isolates of P. aeruginosa were resistant to piperacillin, whereas resistance to cefoxitin, ceftazidime, and cefixime was 66.6% each. However, only 33.33% of bacteria were resistant to amoxicillin/clavulanic acid, imipenem, meropenem, and cefepime. In contrast, isolates of E. coli were 100% susceptible to intravenous carbapenems, except for 9.09% resistance to imipenem. The antibiotics of the carbapenem class were among the most effective agents against K. pneumoniae, where 7 and 15.38% of isolates were resistant to meropenem and imipenem, respectively.
Multidrug resistance was found in 85.48% of Gram-negative bacteria and 95.45% of Gram-positive bacteria. The overall prevalence of ESBL-producing Enterobacteriaceae was 50% (22/44). The prevalence of ESBL-confirmed isolates was 53.84, 50, and 42.85% in K. pneumoniae, E. coli, and P. mirabilis, respectively.
Isolates of Gram-positive bacteria showed the highest level of resistance to penicillin and ampicillin (each 86.66%), tetracyclines (76.92%), and cotrimoxazole (86.66%). On the other hand, moderate level resistance was noted for erythromycin, ciprofloxacin, cefixime, and norfloxacin (each 66.66%). The antibiotics with the lowest resistance rates were linezolid (6.6%), nitrofurantoin (13.33%), amikacin (15.38%), and levofloxacin (26.66%). Two to three isolates of S. aureus exhibited resistance to ampicillin, penicillin, and amoxicillin/clavulanic acid, but only a single isolate showed resistance to nitrofurantoin and linezolid. Isolates of S. saprophyticus were resistant to ampicillin (100%), cotrimoxazole and penicillin (each 80%) and 70% to fluoroquinolone drugs. According to this study, isolates of Enterococcus species showed 100% resistance to all the penicillin derivatives and 50% resistance to vancomycin. No linezolid-resistant Enterococcus spp. and S. saprophyticus isolates were identified (Table 4).
Risk Factors for Symptomatic UTIs
In this study, various socio-demographic, clinical, and behavioural factors that play a role in escalating UTIs among women were considered and assessed using bivariable and multivariable logistic analyses. More than ten variables in the binary logistic regression had a significant relationship with UTIs (P < 0.05). In addition, age, residence, medical history (history of UTIs and self-medication), sexual behaviour (recent sexual practice, frequency of coitus, number of sexual partners in the previous year, coitus with a new partner, not urinating after sexual intercourse), the direction of wiping after toileting, voluntary delay in voiding urine, and water intake/day (in litres) were statistically significant and therefore included in the further analysis.
In multivariable logistic regression analysis, the strongest association was noted between UTI and sexual behaviour (coitus in the past 30 days and frequency of coitus). It was found that participants with recent coitus are 6.6 times more prone to develop UTI (adjusted OR = 6.61, 95% CI: 2.55, 12.01, P < 0.001). Likewise, the risk increased ninefold in those who reported recent coitus more than three times per week (adjusted OR = 9.17, 95% CI: 2.1, 11.01, P < 0.001). Women who did not micturate after coitus, on the other hand, had a marginally higher risk of UTI (P = 0.047).
Women with a history of UTI within the previous six months were twice as likely to develop a subsequent UTI than their peers (adjusted OR = 2.21; 95% CI, 1.54, 13.12). Analysis of the toilet hygiene habits of the study participants revealed that the direction of wiping after toileting was an independent predictor of UTI (P < 0.001). Women who reported wiping in either direction (back-to-front or front-to-back) had a twofold higher risk of developing UTI than those who only reported wiping from front-to-back (adjusted OR = 2.04, 95% CI: 1.10, 9.32). However, women who only wring their hands backwards have a six-fold increased risk of UTI (adjusted OR = 6.21, 95% CI: 2.90, 10.11) (P < 0.001). On the one hand, a delay in voiding habit (voluntary) was significantly associated with UTI (adjusted OR = 3.04, 95% CI: 1.59, 5.88) (P < 0.001). On the other hand, maintaining body hydration by drinking 1–2 litres of water per day was associated with a 75% lower risk of UTI when compared to a daily water intake of 1 litre (adjusted OR = 0.25, 95% CI: 0.06, 0.76), (P < 0.001) (Table 5).
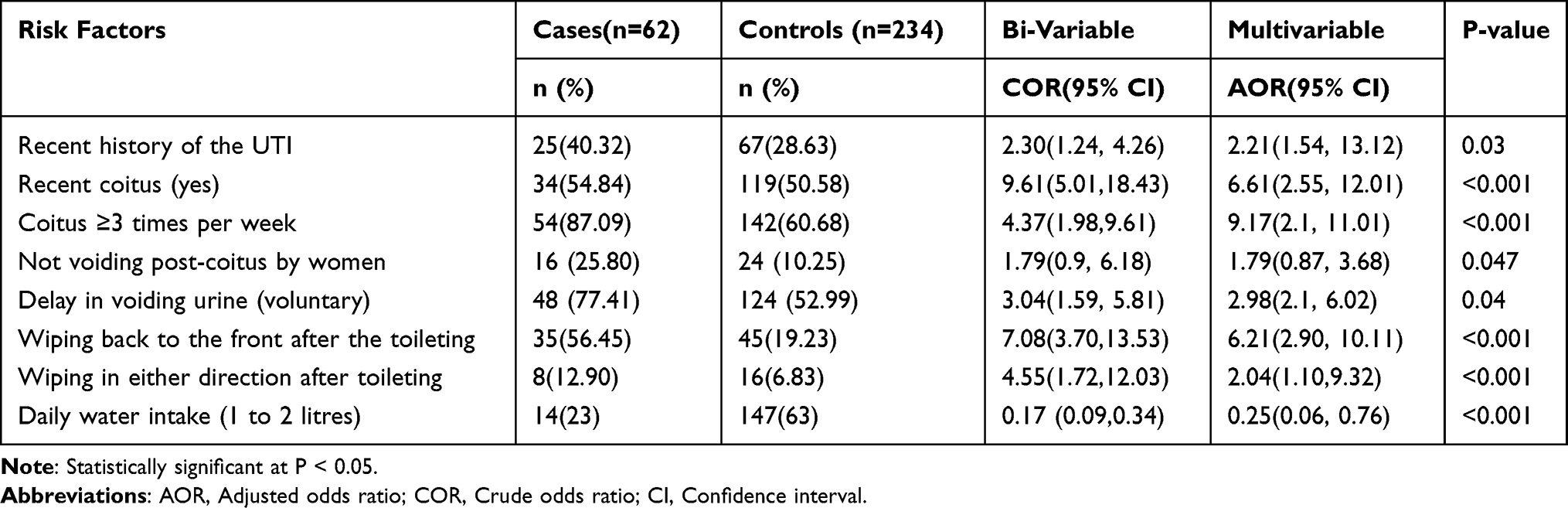 |
Table 5 Bi-Variable and Multivariable Analysis of the Risk Factors Associated with Culture-Confirmed UTIs Among Sexually Active Women in Southern Ethiopia from February – July 2021 |
Discussion
The analysis of sexual behavior data from 286 women aged 15–24 (62 cases of UTI and 234 controls) revealed a strong association between UTI and coitus (increased odds of UTIs observed following recent and frequent coitus). After accounting for age, residence, history of UTI, hospitalization, not wiping from front to back direction, not voiding after coitus, delay in voiding and increasing daily water intake variables, recent coitus and coitus for > 3 times/ weeks increase the odds of UTI by six and nine-fold respectively. This institution-based case-control study was designed to overcome the stigma of examining sexual behaviour and genital hygiene practices in Ethiopia and identifying risk factors associated with UTIs. The analysis was exhaustive and included data from numerous participants. To the best of our knowledge, this is the first case-control study to provide insight into risk factors associated with UTIs among sexually active women and to strengthen the existing prevention and control programs for UTIs in the country.
This study confirms a previously reported association between acute and recurrent urinary tract infections.8,17 This finding highlights the contribution of coitus to the burden of UTI morbidity and supports the theory of ascending route UTI among sexually active women.11,15,18 There are several factors underlings this observation. First, the close proximity of the urethral meatus to the anus and the shorter urethra facilitates the entry of bacteria into the bladder.10 During coitus, bacteria in the vaginal area or the male partner’s penile are pushed up into the urethra and transmitted to the bladder, where urine in the bladder offers the perfect environment for the bacteria to multiply and cause an infection.22 Alternatively, these observations could reflect that the introduction of bacteria into the short urethra may be facilitated by poor genital hygiene habits, including male partners who do not wash their genitals pre-coitus, women who do not void after coitus, and heterosexual vaginal and anal intercourse.8,10,23 Some of these factors showed strong associations in bivariable logistic regression in this study. As recent and frequent coitus was a significant risk factor for UTI, this study explored the possibility that hygiene practices, such as how the male partner washed the genital were risk factors for UTI. While this study demonstrated a marginally protective effect of post-sexual intercourse urinating by women, it did not demonstrate any protective effect of washing genitals pre-coitus by male partners. Given the inadequate sample size, the finding may be underpowered, as the primary objective was not to assess these associations. Individuals with previous UTIs have a twofold greater risk for future UTIs than those with no history, confirming the conclusion of previous studies.5,12 The possible explanation may be that women with low income may develop recurrent UTIs, leading to increased exposure to antimicrobial treatment and infection with resistance strains.4,7 One of the critical observations in this regard was that improper toilet hygiene habits were associated with an increased risk of symptomatic UTI. The finding supports the hypothesis that women in the habit of wiping their genitals in either direction or only from back to front after defecating are more likely to get UTIs than women who wipe from front to back. The finding was in agreement with a previous report.1,15,24 One hypothesis to explain this association could be that the practice of wiping from back to front increases the chance of soiling the genitals with faecal microorganisms.24 This study showed the link between holding urine on several occasions and UTIs and supported the conclusions drawn by several other observational studies, stating “any delay in voiding increases the risk of UTI in adolescents and young adult women”.25,26 The finding supports the hypothesis that if a woman delays urination by holding urine regularly for various reasons, it increases her chances of suffering from UTI multifold. The finding suggests the timely voiding or urination in peri- and postmenopausal women to prevent UTIs, as indicated in previously published guidelines.2 The importance of concise attention to the timely voiding of urine has to be sharply considered in developing public policies aiming reduction of the UTI burden.3,4 The evidence generated from this study showed the reverse association between increased daily water intake and UTIs, and it was in agreement with the result of the systemic review and RCTs that showed an increased daily fluid intake by > 1.5 litre/ day reduced UTIs.27–29 The finding can be explained by the fact that increasing daily water intake can flush out of the urinary tract and making more difficult for micro-organisms to inhabit the urinary tract.28 However, the heterogeneity of effect size across different studies, particularly for non-standard reporting of the volume of water intake and the frequency, suggests that findings must be interpreted with caution.29 Although finding from previous studies established a link between frequent changing of underwear and reduced risk of UTIs,22 this study failed to find this association. Further analysis of the risk factor data also showed the absence of an association between UTI and participants’ ages, residence, contraceptive use, number of sexual partners, and previous antimicrobial use. This may be because of difficulties eliciting sufficient information on these exposures variables, methodology and geographical differences.
The findings of this study showed that the spectrum and bacterial profile of UTI among women aged 15–24 years were predominantly caused by Gram-negative bacilli followed by Gram-positive cocci and a few fungi. The finding confirms the results of previous studies.8,11,12 E. coli was the commonest bacteria isolated in nearly one-third of study participants, followed by K. pneumoniae (20.97%) and S. saprophyticus (16.13%). This was in agreement with the profile of uropathogens reported in the literature.30 The higher prevalence of E. coli in UTI of sexually active women may be explained by the bacterial virulence ability to attachment to the uroepithelium and suggest the faecal contamination as a potential source of infection attributed to the toilet hygiene and sexual practice of the study participants observed in the current study and previous similar study.9 However, the isolates of E. coli as the predominant among sexually active women contrasts with the previous findings, which report S. saprophyticus.3,13
Based on the results of the antimicrobial resistance pattern, this study confirmed the risk associated with UTIs due to antibiotic resistance as a public health concern in the study setting. The finding supports the conclusion correlating the inappropriate use of broad-spectrum drugs with the increase in the rate of drug resistance pathogens.13,31,32 Although the guidelines of the Infectious Disease Society of America recommend nitrofurantoin and fluoroquinolones, such as ciprofloxacin and cotrimoxazole, for uncomplicated and complicated UTI,33 results in the current study revealed an alarming rate of resistance to these classes of drugs. However, the high resistance levels (exceeding 85%) against the penicillin group of drugs, cotrimoxazole, 2nd and some 3rd generation cephalosporins likely reflect the broader use of these agents in clinical practice. This finding, with other previous similar studies, may preclude these agents from the empirical treatment of UTI in clinical practice. However, the low level of resistance recorded for piperacillin/tazobactam, cefixime, cefepime, nitrofurantoin, amikacin, imipenem, meropenem, and levofloxacin suggest these drugs are reasonably highly active agents for uropathogens in the current study setting.
Similarly, linezolid, gentamicin, and amoxicillin/clavulanic acid were the most active drugs against Gram-positive UTI isolates.34 Again, the findings were in agreement with previous studies. Cotrimoxazole has been used for more than decades for the empirical treatment of UTI, but many national and international guidelines recommend its use only when local resistance rates are <20%,35 which is not in the case of most of the isolates evaluated in this study, where the resistance rate was 86%.
The overall prevalence of MDR in this study was 85.48% and agreed with previous reports published abroad.36 Extended-spectrum-lactamase-producing bacteria have recently emerged in ambulatory settings associated with community-acquired UTIs.13,36 Results also revealed the presence of 50% of ESBL-producing Enterobacteriaceae, of which K. pneumoniae, E. coli, and P. mirabilis accounted for 53.84, 50, and 42.85%, respectively. This was almost similar to the results of ESBL-producing uropathogens reported from Sri Lanka (40.2%),34 Pakistan (66%)37 and Bangladesh.36
The overall antibiogram of UTI in this study matches with the reports from the national level during surveillance.38 Considering the close association between ESBL production and fluoroquinolone co-resistance, as reported in the previous study, the detection of both ESBL-producing pathogens and fluoroquinolones resistance in this study may be used to explain the public health risk associated with the possible co-resistant UTIs pathogens. Therefore, in these cases, antibiotics must be tailored according to the antibiogram, ie, using carbapenems for empirical treatment in certain situations. The finding also reinforces revising the guidelines for the management of UTIs. Overall, resistance to commonly prescribed drugs warrants implementing an antibiotic stewardship program and an antimicrobial resistance surveillance system.
Limitations
The findings of this study should be interpreted in light of the following limitations. Like other observational studies, association measured in case-control studies may not represent causal effect relationships. Many confounding factors may influence an unmatched case-control study design, affecting the association between the outcome and the exposure variable. Further, this study does not show the magnitude of recurrent UTI due to the limitation of the study design. The study was facility-based and may not be representative of the larger group in the population. Moreover, there may be social desirability bias since the study assessed the lifestyle and sexual behaviour of the participants.
The strengths of this study include the microbiological screening of midstream urine from both and control to rule out asymptomatic UTI, the recruitment of participants from the general hospital; the inclusion of confounders; medical history, contraceptive methods use, hygiene and inadequate water intake; which may increase the risks of UTI. However, the study was subjected to the following limitation: exposure to several risk factors was assessed based on the self-response, and the molecular characterization of the resistance determinants in the individual isolates was not performed, only to the extent of the presence/absence of ESBLs.
Implications of the Study
This study complements the literature on risk factors for UTI among women aged 14–24 in southern Ethiopia. The modifiable risk factor associated with UTIs justifies the rationale of including health education in reproductive health as a potential public health intervention for the reduction of risk associated with UTIs.
The high rates of antimicrobial resistance observed against first-line drugs (eg cotrimoxazole) limits the use of these drugs in clinical practice, and it also suggests the importance of implementing antimicrobial resistance surveillance and stringent antimicrobial stewardship programs. Therefore, the observation may be implicated in recognizing the possible role of the patient’s own normal flora in the pathogenesis of UTI, guiding clinicians’ appropriate diagnosis and empirical antibiotic treatment. At the same time, the high rate of drug-resistant isolates (MDR and ESBL positive) in community-acquired UTIs highlighted the spread of these pathogens in the community setting, implying the importance of effective control measures. The antibiogram data in this study may be used to develop treatment guidelines in the local context. The detection of resistant bacteria to new parenteral classes of drugs in the absence of their use in Ethiopia is a new insight which justifies further study to evaluate the possible risk factors using a robust design involving molecular techniques.
Conclusion
The finding from this study confirmed that the association between UTI and recent heterosexual intercourse and the effect has a dose-response relationship with frequency. Additional independent risk factor includes a recent history of UTI and not wiping from front to back direction after toileting, and delay in voiding. The common bacterium isolated in this study was E. coli. The finding highlighted a sharp rise in the rate of antimicrobial resistance against the class of antimicrobials commonly used for empirical treatment. However, aminoglycosides, nitrofurantoin and carbapenems were the most active drugs.
Abbreviations
AOR, Adjusted Odds Ratio; CLSI, Clinical and Laboratory Standards Institute. ESBL, Extended Spectrum Beta-Lactamase; HPF, High Power Field; SNNP, South Nation Nationality People; SPSS, Statistical Package for Social Science, UTI, Urinary Tract Infection; WHO, World Health Organization; MDR, multi-drug resistance; COR, crude odds ratio; AOR, adjusted odds ratio; ESBL, Extended-spectrum β-lactamase.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors are greatly indebted to Yetnayet Tadele, Mistru Gibe, Liulsege Yirgu, Zenit Elias, Moges Molla, and Meron Assefa for assistance during the data collection. In addition, the authors would like to thank the CEO, medical director, and the staff (clinicians and others) of Arba Minch General Hospital for assistance with study participant enrollment. Thanks to other staff in the Department of Medical Laboratory Science for the comment and guidance in developing the study protocols, data collection and data analysis. Finally, we are very grateful to all of the study participants.
Funding
No specific grant was received for this research from any funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harrington RD, Hooton TM. Urinary tract infection risk factors and gender. J Gend Specif Med. 2000;3:27–34.
2. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13:269–284. doi:10.1038/nrmicro3432
3. Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Disease-a-Month. 2003;49:53–70. doi:10.1067/mda.2003.7
4. Foxman B. Recurring urinary tract infection: incidence and risk factors. Am J Public Health. 1990;80:331–333. doi:10.2105/AJPH.80.3.331
5. Al-Badr A, Al-Shaikh G. Recurrent urinary tract infections management in women. Sultan Qaboos Univ Med J. 2013;13:359–367. doi:10.12816/0003256
6. Alós JI. Epidemiología y etiología de la infección urinaria comunitaria. Sensibilidad antimicrobiana de los principales patógenos y significado clínico de la resistencia [Epidemiology and etiology of urinary tract infections in the community. Antimicrobial susceptibility of the main pathogens and clinical AQ8 AQ7 significance of resistance]. Enferm Infecc Microbiol Clin. 2005;23(Suppl 4):3–8. Spanish. doi:10.1157/13091442
7. Bader MS, Loeb M, Brooks AA. An update on the management of urinary tract infections in the era of antimicrobial resistance. Postgrad Med. 2017;129:242–258. doi:10.1080/00325481.2017.1246055
8. Almukhtar SH. Urinary tract infection among women aged (18–40) years old in Kirkuk City, Iraq. Open Nurs J. 2018;12. doi:10.2174/1874434601812010248
9. Abou Heidar NF, Degheili JA, Yacoubian AA, Khauli RB. Management of urinary tract infection in women: a practical approach for everyday practice. Urol Ann. 2019;11:339–346. doi:10.4103/UA.UA_104_19
10. Klein RD, Hultgren SJ. Urinary tract infections: microbial pathogenesis, host-pathogen interactions and new treatment strategies. Nat Rev Microbiol. 2020;18:211–226. doi:10.1038/s41579-020-0324-0
11. Hooton TM, Scholes D, Stapleton AE, et al. A prospective study of asymptomatic bacteriuria in sexually active young women. N Engl J Med. 2000;343. doi:10.1056/NEJM200010053431402
12. Vincent CR, Thomas TL, Reyes L, White CL, Canales BK, Brown MB. Symptoms and risk factors associated with first urinary tract infection in college age women: a prospective cohort study. J Urol. 2013;189:904–910. doi:10.1016/j.juro.2012.09.087
13. Erdem I, Kara Ali R, Ardic E, Elbasan Omar S, Mutlu R, Topkaya AE. Community-acquired lower urinary tract infections: etiology, antimicrobial resistance, and treatment results in female patients. J Glob Infect Dis. 2018;10:129–132. doi:10.4103/jgid.jgid_86_17
14. Jancel T, Dudas V. Management of uncomplicated urinary tract infections. West J Med. 2002;176:51–55. doi:10.1136/ewjm.176.1.51
15. Amiri FN, Rooshan MH, Ahmady MH, Soliamani MJ. Hygiene practices and sexual activity associated with urinary tract infection in pregnant women. East Mediterr Health J. 2009;15:104–110. doi:10.26719/2009.15.1.104
16. Agyei WK, Epema EJ, Lubega M. Contraception and prevalence of sexually transmitted diseases among adolescents and young adults in Uganda. Int J Epidemiol. 1992;21:981–988. doi:10.1093/ije/21.5.981
17. Buckley RM, McGuckin M, MacGregor RR. Urine bacterial counts after sexual intercourse. N Engl J Med. 1978;298:321–324. doi:10.1056/NEJM197802092980607
18. Elster AB, Lach PA, Roghmann KJ, McAnarney ER. Relationship between frequency of sexual intercourse and urinary tract infections in young women. South Med J. 1981;74:704–708. doi:10.1097/00007611-198106000-00018
19. Cheesbrough M. District Laboratory Practice in Tropical Countries, Part.
20. Weinstein MP; Clinical Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing.
21. Magiorakos A-P, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18:268–281. doi:10.1111/j.1469-0691.2011.03570.x
22. Hooton TM, Roberts PL, Stamm WE. Effects of recent sexual activity and use of a diaphragm on the vaginal microflora. Clin Infect Dis. 1994;19:274–278. doi:10.1093/clinids/19.2.274
23. Lema VM. Urinary tract infection in young healthy women following heterosexual anal intercourse: case reports. Afr J Reprod Health. 2015;19:134–139.
24. Persad S, Watermeyer S, Griffiths A, Cherian B, Evans J. Association between urinary tract infection and postmicturition wiping habit. Acta Obstet Gynecol Scand. 2006;85:1395–1396. doi:10.1080/00016340600936977
25. Jagtap S, Harikumar S, Vinayagamoorthy V, Mukhopadhyay S, Dongre A. Comprehensive assessment of holding urine as a behavioral risk factor for UTI in women and reasons for delayed voiding. BMC Infect Dis. 2022;22:521. doi:10.1186/s12879-022-07501-4
26. Welk B, Hickling D. Frequent urinary tract infections in a premenopausal woman. CMAJ. 2016;188:522–523. doi:10.1503/cmaj.150893
27. Lean K, Nawaz RF, Jawad S, Vincent C. Reducing urinary tract infections in care homes by improving hydration. BMJ Open Qual. 2019;8(3):e000563. PMID: 31363503; PMCID: PMC6629391. doi:10.1136/bmjoq-2018-000563
28. Scott AM, Clark J, Mar CD, Glasziou P. Increased fluid intake to prevent urinary tract infections: systematic review and meta-analysis. Br J Gen Pract. 2020;70:e200–e207. doi:10.3399/bjgp20X708125
29. Hooton TM, Vecchio M, Iroz A, et al. Effect of increased daily water intake in premenopausal women with recurrent urinary tract infections: a randomized clinical trial. JAMA Intern Med. 2018;178:1509–1515. doi:10.1001/jamainternmed.2018.4204
30. Saber S, Yasmin N, Alam MT, Hossain MM, Alam RF. Study on urinary tract infection among females of reproductive age group in tertiary care teaching hospital, Dhaka, Bangladesh. Eur J Med Health Sci. 2021;3:85–89. doi:10.24018/ejmed.2021.3.1.680
31. Belete MA, Saravanan M, Systematic A. Review on drug resistant urinary tract infection among pregnant women in developing countries in Africa and Asia; 2005–2016. Infect Drug Resist. 2020;13:1465–1477. doi:10.2147/IDR.S250654
32. Parvin US, Hossain MA, Musa AK, et al. Pattern of aerobic bacteria with antimicrobial susceptibility causing community acquired urinary tract infection. Mymensingh Med J. 2009;18:148–153.
33. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the infectious diseases Society of America and the European Society for microbiology and infectious diseases. Clin Infect Dis. 2011;52:e103–e120. doi:10.1093/cid/ciq257
34. Tillekeratne LG, Vidanagama D, Tippalagama R, et al. Extended-spectrum ß-lactamase-producing enterobacteriaceae as a common cause of urinary tract infections in Sri Lanka. Infect Chemother. 2016;48:160–165. doi:10.3947/ic.2016.48.3.160
35. Critchley IA, Cotroneo N, Pucci MJ, Jain A, Mendes RE. Resistance among urinary tract pathogens collected in Europe during 2018. J Glob Antimicrob Resist. 2020;23:439–444. doi:10.1016/j.jgar.2020.10.020
36. Islam MA, Islam MR, Khan R, et al. Prevalence, etiology and antibiotic resistance patterns of community-acquired urinary tract infections in Dhaka, Bangladesh. PLoS One. 2022;17:e0274423. doi:10.1371/journal.pone.0274423
37. Sohail M, Khurshid M, Saleem HGM, Javed H, Khan AA. Characteristics and antibiotic resistance of urinary tract pathogens isolated from Punjab, Pakistan. Jundishapur J Microbiol. 2015;8:e19272. doi:10.5812/jjm.19272v2
38. Addis T, Mekonnen Y, Ayenew Z, Fentaw S, Biazin H. Bacterial uropathogens and burden of antimicrobial resistance pattern in urine specimens referred to Ethiopian Public Health Institute. PLoS One. 2021;16:e0259602. doi:10.1371/journal.pone.0259602
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.