Back to Journals » Infection and Drug Resistance » Volume 13
Community-Acquired Methicillin-Resistant Staphylococcus aureus ST59 in a Chinese Adult with Meningitis: A Case Report from China
Authors Chen F, Chen Y ![]() , Zhao X, Wang J
, Zhao X, Wang J ![]()
Received 11 March 2020
Accepted for publication 14 June 2020
Published 29 June 2020 Volume 2020:13 Pages 2011—2016
DOI https://doi.org/10.2147/IDR.S253407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eric Nulens
Fayu Chen,1 Yan Chen,2 Xiaofei Zhao,3 Jianfeng Wang4
1Department of General Practice, The Affiliated Hospital of Hangzhou Normal University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of General Practice, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Clinical Laboratory, The Affiliated Hospital of Hangzhou Normal University, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Respiratory Diseases, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Jianfeng Wang
Department of Respiratory Diseases, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
Tel +86 571 8662 0306
Email [email protected]
Abstract: Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) infections are reported worldwide and are associated with serious outcomes. The majority of CA-MRSA infections are soft tissue and skin infections, and cases with meningitis caused by CA-MRSA are rare. Here, we reported a 53-year-old male patient with meningitis due to CA-MRSA infection, as confirmed by cerebrospinal fluid examination. Whole-genome sequencing data revealed an ST59 CA-MRSA strain encoding PVL and SCCmec IV. Linezolid was administered in this case, and the patient recovered, with no signs of relapse during the one-year follow-up. We present the first case of PVL-positive ST59 CA-MRSA meningitis, with severe manifestations in China.
Keywords: methicillin-resistant Staphylococcus aureus, community-acquired, meningitis, whole-genome sequencing, ST59
Introduction
Staphylococcus aureus is a widely distributed microorganism present in human and animal skin, nasal cavities, and the throat, intestine and stomach; it is also found in carbuncles, purulent oral cavities, sewage and other environments. S. aureus is one of the most important pathogens of nosocomial and community infections and may cause a broad range of infections. Since the first methicillin-resistant S. aureus (MRSA) was discovered by Jevons in the United Kingdom, MRSA infection has mostly spread worldwide. The clinical and bacteriological properties of community-acquired methicillin-resistant S. aureus (CA-MRSA) are different from those of hospital-acquired MRSA.1 Despite its rarity, meningitis due to CA-MRSA has been associated with serious and occasionally fatal outcomes. Overall, our knowledge of the epidemiological and molecular characteristics of CA-MRSA lineages is limited. In this study, we present the first case report of CA-MRSA ST59 meningitis in China.
Case Report
A 53-year-old male patient was hospitalized in the respiratory outpatient department of our hospital. He had fever with headache for half a month, slight cough, and sore muscles and joints. The patient did not have diabetes or immunosuppressive diseases, and there was no history of hypertension. Considering that no signs of pneumonia were found by thoracic CT, the patient was given cefixime sustained-release capsules plus clarithromycin sustained-release capsules for 4 days. However, the fever with headache remained, and he was admitted to the neurology department.
The patient was treated with a three-day course of ceftriaxone, with no signs of improvement. Brain magnetic resonance imaging (MRI) showed a high T2WI signal and T2 flair in the left lateral ventricle, and DWI indicated no significant diffusion restriction. The lesion was not enhanced. Brain MRI showed left paraventricular demyelination (Figure 1). A lumbar puncture was performed, and cerebrospinal fluid (CSF) examination demonstrated a nucleated cell count of 2120 cells/µL, neutrophil percentage of 95%, glucose level of 2.29 mmol/L, protein level of 57.3 mg/dL, and adenosine deaminase activity of 1.5 U/L. The ratio between CSF and blood glucose levels was 0.47. The CSF samples were centrifuged, and the sediment was smeared and stained with Gram, ink, fluorescence and anti-acid stains. No acid-fast bacilli, cryptococci or fungi were detected in the CSF smears; the Xpert MTB/RIF assay was also negative. Hepatitis B surface antigen (HbsAg), hepatitis B core antibody (HbcAb) and hepatitis B e-antigen (HbeAb) were positive, and upper-abdomen enhanced CT showed cirrhosis of the liver, multiple small cysts of the liver, gallstones and cholecystitis. The Child-Pugh score of liver cirrhosis was class A.
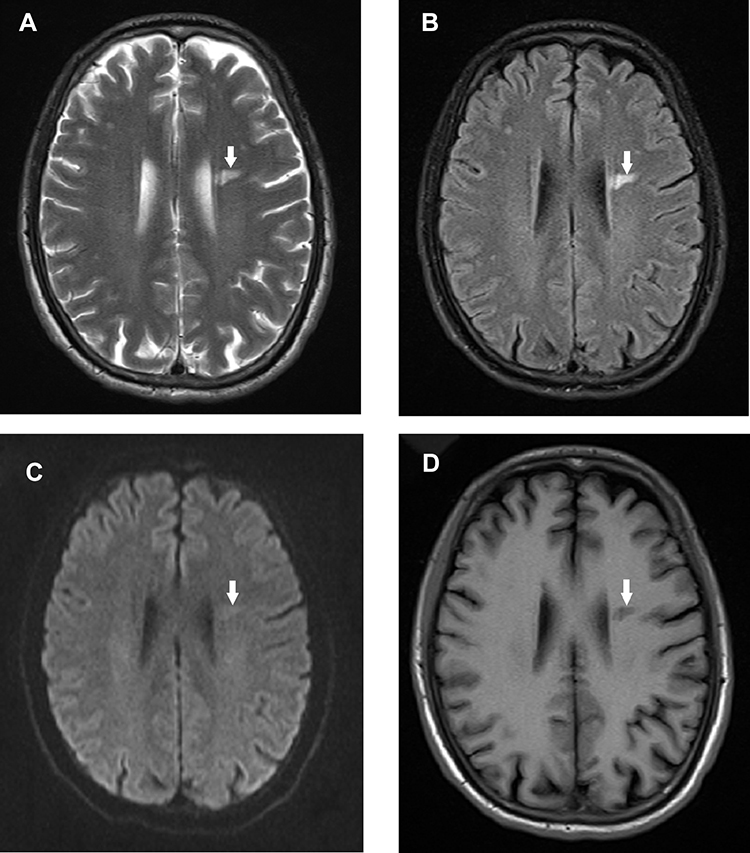 |
Figure 1 The axial T2WI image shows a small strip of a hypersignal lesion near the left lateral ventricle (A). The lesion presented hyperintensity on FLAIR (B) and no significant diffuse obstruction on DWI (C). No significant enhancement (D) was observed in the GD-DTPA enhanced sequence. |
CSF culture vials were incubated in an automated culture system (Bact/ALERT Virtuo™, bioMérieux, France). The bacteria primarily grew under both anaerobic and aerobic conditions. After the CSF culture became positive, 10 µL of fluid was plated on Columbia blood agar, and S. aureus isolate SA17 was cultured. Microbiological identification was performed by matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) mass spectrometry using a MALDI/TOF Biotyper (Bruker Italia, Milan, Italy). Antimicrobial susceptibility testing was performed using E-test strips in three replicates, revealing that the isolate was methicillin-resistant S. aureus.
After multidisciplinary discussion, the patient received antibiotic treatment with 0.6 g linezolid bid intravenously for 17 days, and the patient’s platelet counts decreased to 27×109/L. The time course of linezolid administration and the onset of thrombocytopaenia are illustrated in Figure 2. When linezolid was stopped, his platelet counts gradually increased. The patient recovered well, his symptoms and signs improved significantly, and the results of CSF re-examination were normal.
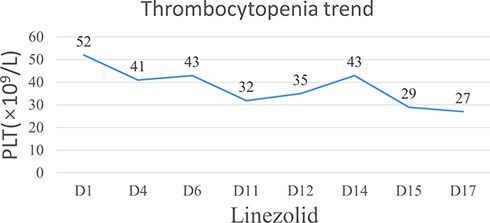 |
Figure 2 The time course of linezolid administration and the onset of thrombocytopaenia. |
S. aureus strain SA17 was detected as a result of routine hospital laboratory procedures. This study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of The Affiliated Hospital of Hangzhou Normal University, Hangzhou, China. Written informed consent, which included publication of the case details, was obtained from the patient.
Results of Phenotypic and Genotypic Characterization
S. aureus SA17 was found to be sensitive to non-beta-lactam antibiotics, including gentamicin, ciprofloxacin, moxifloxacin, tetracycline, minocycline, tigecycline, rifampicin, trimethoprim-sulfamethoxazole (TMP-SMX), teicoplanin and vancomycin, but was resistant to clindamycin and erythromycin. Based on the D-zone test, this isolate showed inducible clindamycin resistance.
Whole-genome sequencing of S. aureus SA17 was performed using the Illumina HiSeq X Ten platform (Illumina, San Diego, CA, USA) with a 150-bp paired-end protocol. The trimmed sequence reads were de novo assembled using Unicycler v0.4.7 with the Pilon v1.23 option for modification of the assembled reads. The genome sequence was further examined by in silico multilocus sequence typing (MLST) and staphylococcal cassette chromosome mec (SCCmec), staphylococcal protein A gene (spa), and Panton-Valentine leukocidin (PVL) element determination. In silico MLST analysis and bacterial source tracking using the core genome MLST (cgMLST) strategy were performed by the BacWGSTdb server.2
The draft genome sequence of S. aureus SA17 consisted of 58 contigs, comprising 2,769,666 bases, and the PGAP server predicted a total of 2730 protein-coding sequences. The overall G+C content of this strain is 32.8%. In total, 59 tRNA genes and 18 rRNA operons were identified. This strain belongs to sequence type 59 (ST59) and spa type t437, harbours a novel variant of staphylococcal cassette chromosome mec element (SCCmec) type IV (90.77% identity to SCCmec IVa) and νSaα and νSaβ pathogenicity islands and is positive for the lukF and lukS Panton-Valentine leukocidin (PVL) pathogenic determinant. The strain carries two β-lactam resistance genes (blaZ and mecA), aminoglycoside resistance genes [ant(6)-Ia and aph(3ʹ)-III], and macrolide resistance genes [erm(B)]. Several virulence factors were found in the genome, including staphylococcal complement inhibitor (scn), aureolysin (aur), gamma-haemolysin (hlgA, hlgB, and hlgC), and enterotoxin (seb, sek and seq). The phylogenetic relationship between S. aureus SA17 and 10,521 S. aureus strains currently deposited in the NCBI GenBank database was analysed. Our data suggest that S. aureus SA17 can be further classified as a separate clone and that its closest relative is an ST59 CA-MRSA strain (SA957, SCCmec V) recovered from the blood sample of a patient with severe sepsis and acute respiratory failure in China, differing by 86 cgMLST loci (Figure 3). Previous studies have confirmed that the majority of ST59 CA-MRSA strains belong to two clones, PVL-negative SCCmec IV and PVL-positive SCCmec V, in Asia-Pacific countries. Our present study highlights the emergence of a novel variant of the SCCmec type ST59 CA-MRSA in China. According to our genomic epidemiological analysis, the assumed basis of virulence in the S. aureus SA17 strain can be explained in a fashion different than that reported for Asia-Pacific strains, that is, by a combination of acquisition of CA-MRSA-characteristic genes encoding PVL and SCCmec IV and possible enhanced expression of virulence genes.
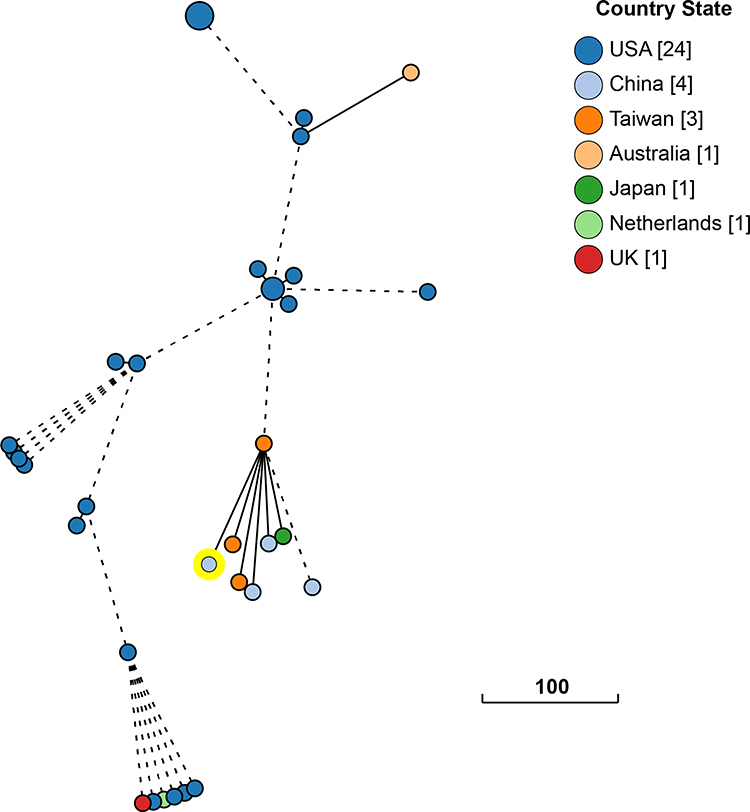 |
Figure 3 Phylogenetic relationship between S. aureus SA17 and closely related S. aureus ST59 strains currently deposited in the NCBI GenBank database. The lines connecting the circles indicate the clonal relationships between different isolates. The scale bar represents a pairwise allelic difference of 100 cgMLST loci. |
Discussion
Staphylococcus aureus, belonging to the family Staphylococcaceae, is a gram-positive, catalase-positive, and bacitracin-resistant coccus.3 S. aureus can survive in different harsh environments and is resistant to many disinfectants.4 Methicillin-resistant S. aureus (MRSA) was first clinically identified from patients hospitalized in the 1960s and was characterized by resistance to all penicillins, cephalosporins, and even carbapenems.4 MRSA is rapidly spreading worldwide, and it has been one of the most common nosocomial bacterial pathogens.5,6 MRSA-associated infections are potentially damaging and fatal.7
MRSA is generally considered to be a typical nosocomial pathogen.1 However, community-acquired MRSA (CA-MRSA) strains have been reported from patients in different areas beginning in the 1990s.3 In the past, CA-MRSA infections often occurred in patients who frequently contacted health-care facilities or in specific groups of patients, such as intravenous drug users. However, the epidemiology of community-based infections caused by MRSA has changed dramatically in the past decade.6 Indeed, CA-MRSA may occur without any underlying diseases and usually presents with soft tissue and skin infection.8 Spontaneous meningitis caused by CA-MRSA is rare and usually present in older patients with immunodeficiency or diabetes mellitus.7 In China, reports on CA-MRSA meningitis patients are very scarce.
Molecular epidemiological investigation of MRSA is essential for monitoring the occurrence and development of epidemic clones and for determining intervention policies.9 Healthcare-associated MRSA (HA-MRSA) and CA-MRSA have different clinical and molecular characteristics. CA-MRSA infection usually manifests as cellulitis or abscesses, whereas HA-MRSA often causes pneumonia and sepsis.10 In contrast to HA-MRSA clones that carry SCCmec type I, II or III,11 CA-MRSA lineages have been characterized by the presence of small-sized SCCmec types IV and V and of genes encoding Panton-Valentine leukocidin (PVL) in many cases.12 At present, there are five dominant CA-MRSA lineages, ST1-IV, ST8-IV, ST30-IV, ST59-IV/V, and ST80-IV, and each is prevalent in different geographical locations.13 ST59 was first reported in Taiwan in 2004, and the emergence of CA-MRSA is becoming a growing public health concern.14 In China, ST59 constitutes an epidemic lineage of CA-MRSA isolates in recent decades. Furthermore, in various animal infection models, ST59 CA-MRSA isolates have been observed to have significantly more pronounced virulence than HA-MRSA clones ST5 and ST239.15 In general, ST59 needs to be rapidly discriminated from other MRSA STs. STs can be rapidly predicted with high accuracy by using machine learning algorithms and MALDI-TOF MS.16–18 For ST59 isolates, the loss of a large portion of the β-haemolysin-converting prophage, increased expression of α-toxin and evolutionary acquisition of PVL possibly contribute to its enhanced pathogenic potential. In this case, the possible upregulated expression of virulence genes may cause meningitis in immunocompetent patients.
The Infectious Diseases Society of America has recommended 2 weeks of vancomycin therapy for MRSA meningitis; alternative antimicrobials recommended are cotrimoxazole and linezolid.7 Interestingly, according to a literature review, all reported patients with CA-MRSA central nervous system infections showed complete remission without neurological sequelae when treated with linezolid, whereas those treated with vancomycin without linezolid had severe complications or died.19 The vancomycin concentration in CSF is only approximately 20% of the serum concentration.20 Linezolid and co-trimoxazole have better CSF penetration than vancomycin, and the drug concentrations in CSF are approximately 65% and 50% of their serum level, respectively. Despite the high dose of vancomycin, low levels of the drug are found in CSF. Hence, rifampicin and cotrimoxazole have been used in the early stage of treatment, with linezolid being added when fever persisted. After multidisciplinary discussion, linezolid was used in this case, and the patient recovered with no signs of relapse during the one-year follow-up.
Conclusion
Meningitis caused by community-acquired methicillin-resistant S. aureus is rare. The disease requires timely diagnosis and effective antibiotics. We present the first case of PVL-positive ST59 CA-MRSA meningitis with severe manifestations in China.
Data Sharing Statement
The genome sequence of S. aureus SA17 (Biosample ID: SAMN12612975) can be accessed at DDBJ/ENA/GenBank under accession number VSRP00000000. The version described in this paper is the first version, VSRP01000000.
Disclosure
All authors declare that they have no conflicts of interest.
References
1. Yonezawa R, Kuwana T, Kawamura K, Inamo Y. Invasive community-acquired methicillin-resistant Staphylococcus aureus in a Japanese girl with disseminating multiple organ infection: a case report and review of Japanese pediatric cases. Case Rep Pediatr. 2015;2015:291025. doi:10.1155/2015/291025
2. Ruan Z, Feng Y. BacWGSTdb, a database for genotyping and source tracking bacterial pathogens. Nucleic Acids Res. 2016;44(D1):D682–D687. doi:10.1093/nar/gkv1004
3. Lakhundi S, Zhang K. Methicillin-resistant Staphylococcus aureus: molecular characterization, evolution, and epidemiology. Clin Microbiol Rev. 2018;31(4).
4. Gajdacs M. The continuing threat of methicillin-resistant Staphylococcus aureus. Antibiotics (Basel, Switzerland). 2019;8(2):52.
5. Turner NA, Sharma-Kuinkel BK, Maskarinec SA, et al. Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research. Nat Rev Microbiol. 2019;17(4):203–218. doi:10.1038/s41579-018-0147-4
6. Stryjewski ME, Chambers HF. Skin and soft-tissue infections caused by community-acquired methicillin-resistant Staphylococcus aureus. Clin Infect Dis. 2008;46(Suppl 5):S368–S377. doi:10.1086/533593
7. Kumari VH, Babu AR, Srinivas D, Siddaiah N, Somanna S. Methicillin-resistant Staphylococcus aureus central nervous system infections–analysis and outcome. Br J Neurosurg. 2015;29(3):413–418. doi:10.3109/02688697.2015.1006168
8. Pereira NM, Shah I, Ohri A, Shah F. Methicillin resistant Staphylococcus aureus meningitis. Oxf Med Case Reports. 2015;2015(11):364–366. doi:10.1093/omcr/omv064
9. Hadyeh E, Azmi K, Seir RA, Abdellatief I, Abdeen Z. Molecular characterization of methicillin resistant Staphylococcus aureus in west bank-palestine. Front Public Health. 2019;7:130. doi:10.3389/fpubh.2019.00130
10. Wang HK, Huang CY, Huang YC. Clinical features and molecular characteristics of childhood community-associated methicillin-resistant Staphylococcus aureus infection in a medical center in northern Taiwan, 2012. BMC Infect Dis. 2017;17(1):470. doi:10.1186/s12879-017-2560-0
11. Santosaningsih D, Santoso S, Setijowati N, et al. Prevalence and characterisation of Staphylococcus aureus causing community-acquired skin and soft tissue infections on Java and Bali, Indonesia. Trop Med Int Health. 2018;23(1):34–44. doi:10.1111/tmi.13000
12. Otto M. Basis of virulence in community-associated methicillin-resistant Staphylococcus aureus. Annu Rev Microbiol. 2010;64:143–162. doi:10.1146/annurev.micro.112408.134309
13. Qu T, Feng Y, Jiang Y, et al. Whole genome analysis of a community-associated methicillin-resistant Staphylococcus aureus ST59 isolate from a case of human sepsis and severe pneumonia in China. PLoS One. 2014;9(2):e89235. doi:10.1371/journal.pone.0089235
14. Wang CC, Lo WT, Chu ML, Siu LK. Epidemiological typing of community-acquired methicillin-resistant Staphylococcus aureus isolates from children in Taiwan. Clin Infect Dis. 2004;39(4):481–487. doi:10.1086/422642
15. Wu S, Huang J, Zhang F, et al. Prevalence and characterization of food-related methicillin-resistant Staphylococcus aureus (MRSA) in China. Front Microbiol. 2019;10:304. doi:10.3389/fmicb.2019.00304
16. Camoez M, Sierra JM, Dominguez MA, Ferrer-Navarro M, Vila J, Roca I. Automated categorization of methicillin-resistant Staphylococcus aureus clinical isolates into different clonal complexes by MALDI-TOF mass spectrometry. Clin Microbiol Infect. 2016;22(2):
17. Wang HY, Lee TY, Tseng YJ, et al. A new scheme for strain typing of methicillin-resistant Staphylococcus aureus on the basis of matrix-assisted laser desorption ionization time-of-flight mass spectrometry by using machine learning approach. PLoS One. 2018;13(3):e0194289. doi:10.1371/journal.pone.0194289
18. Wang HY, Lien F, Liu TP, Chen CH, Chen CJ, Lu JJ. Application of a MALDI-TOF analysis platform (ClinProTools) for rapid and preliminary report of MRSA sequence types in Taiwan. PeerJ. 2018;6:e5784. doi:10.7717/peerj.5784
19. Fernandez-Ruiz M, Cervera C, Pitart C, et al. Community-acquired methicillin-resistant Staphylococcus aureus meningitis complicated by cerebral infarction. Role of antibiotic combination of linezolid plus levofloxacin. Intern Med. 2010;49(18):1971–1974. doi:10.2169/internalmedicine.49.3942
20. Munckhof WJ, Krishnan A, Kruger P, Looke D. Cavernous sinus thrombosis and meningitis from community-acquired methicillin-resistant Staphylococcus aureus infection. Intern Med J. 2008;38(4):283–287. doi:10.1111/j.1445-5994.2008.01650.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.