Back to Journals » Psychology Research and Behavior Management » Volume 17
Communal Riots and Its Psychological Impact: A Systematic Review Study in Indian Context
Authors Irshad S ![]()
Received 12 February 2024
Accepted for publication 22 April 2024
Published 13 May 2024 Volume 2024:17 Pages 1991—1998
DOI https://doi.org/10.2147/PRBM.S455783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Seema Irshad
Department of Clinical Neurosciences, College of Medicine, King Faisal University, Al-Ahsa, Kingdom of Saudi Arabia
Correspondence: Seema Irshad, Division of Psychology, Department of Clinical Neurosciences, College of Medicine, King Faisal University, Al-Ahsa, 31982, Kingdom of Saudi Arabia, Tel +966-13-589-7883 ; +966-538010765, Email [email protected]; [email protected]
Objective: In the Indian setting, communal riots characterized by intergroup violence have been common and have had an impact on the lives of both people and communities. The goal of this systematic review is to investigate the psychological effects of Indian communal riots in depth. Through a comprehensive review of the literature, the study aims to identify recurring themes, patterns, and variances in the psychological effects encountered by victims of community violence.
Methods: The researcher searched Science Direct, PubMed, Web of Science, Google Scholar, and PsycINFO for research published between the year 2000 and the year 2022 in each of these databases. The Newcastle–Ottawa Scale was employed to evaluate the study’s quality.
Results: After identifying 1189 publications in all, 195 of them were chosen for full-text examination, and 41 research were ultimately included. Twenty studies examined depression and mental health with a prevalence rate of 49%. Five studies (12%) examined post-traumatic stress disorder. In places devastated by riots, the prevalence of post-traumatic stress disorder varied from 4% to 41%. Other studies investigated anxiety, alcohol abuse, and homelessness. However, two studies revealed that group activities could lower depression and suicide rates, perhaps as a result of increased social cohesiveness and group catharsis among subpopulations.
Conclusion: The researcher investigated the connection between collective activities and mental health in this systematic review, providing strong evidence that riots, protests, and other collective actions—even peaceful ones—can harm mental health outcomes. Thus, healthcare providers must be aware of the psychological and emotional effects of riots, revolutions, and demonstrations. It is essential to do more study on this newly identified sociopolitical driver of mental health.
Keywords: communal riots, psychological well-being, systematic review
Over 180 nations, or 99% of the world’s population, have experienced collective activities including protests, riots, and revolutions over the past few decades.1,2 Globally, they are growing,3,4 however, it’s still not quite understood how group action affects mental health. Much more research has been done on the impact of armed conflicts, terrorist attacks, natural catastrophes, and man-made disasters on the mental health of huge populations.5–8 These researches demonstrate higher levels of resilience and psychopathology in the face of widespread community trauma, although it is yet unknown how collective behaviors relate to healthcare professionals. A different area of study is required since collective activities vary from further significant population events in nature. As a result, we thoroughly examined studies on global collective action and mental health.
India is a multi-religious country. In the nation, various religions and their adherents can be found. India is a secular nation, so it emphasizes the equality of people and humanity. However, on occasion, because of careless mistakes and flaws, our nation experiences some issues that degrade and humiliate mankind. Communal riots are one of them. One of the biggest issues with human rights now is communal violence or conflict between groups who define themselves by their differences from one another. But compared to earlier decades, the violence that has persisted over the last 20 years is different. The current sectarian violence is not the fault of any one extremist organization, but rather of the governments that use inter-group animosity to achieve power. These systemic causes of intergroup conflict pose a challenge to the foundational values of democracy and equality. Identity politics is the root cause of current racial violence. Identity politics, whether based on race, sex, caste, class, language, religion, or national or regional origin, emphasize the group aspect of rights, experiences, and identities. In many instances, the political-culture forces involved in identity politics want to impose their political dominance, cultural hegemony, and major legal changes. Communal riots are fairly common throughout the country as a result of all these conflicts. Mumbai, Moradabad, Meerut, Gujarat, and Aligarh are the areas of India that are most sensitive.
Religious festivals and places of worship have been the most apparent root of conflicts between communities. However, various economic and political causes have deepened and aggravated the split between the two populations beneath the pattern of injured religious sentiments. These have included controversial British colonial practices, economic sanctions imposed on Muslim textile workers in the 1930s, and other types of economic rivalry existing before separation. In 1969, there was the deadliest communal violence since independence, marking the start of the state’s partisan involvement and the emergence of a link between politicians and criminals. Political parties play a crucial role in building positive links between the communities. Political parties are organizations where people are free to express their opinions and ideals publicly. The democratic social structure and political parties give people the chance to express their opinions.
From Table 1 we can see communal riots have increased in India between 2019–2020. A major increase can be seen in communal/religious incidents and riots ie 96%.
 |
Table 1 Rioting Offences (Courtesy: NCRB Data, 2020) |
With a particular focus on understanding the psychological effects of these events on individuals and communities, the goal of this systematic review and synthesis of the literature on communal riots in the Indian context is to identify patterns, common themes, and variances in psychological outcomes associated with communal violence in India.
Methods
Search Strategy and Selection Criteria
Our study protocol was pre-specified and registered in PROSPERO (PROSPERO: CRD42023480295). We adhered to the PRISMA standards,9 which are the recommended reporting elements for meta-analyses and systematic reviews. This systematic review is conducted on communal riots and their psychological impact on the Indian population so all study was chosen based on the Indian context. Studies that were written in English and distributed in scholarly journals were selected. All study types, including cross-sectional and longitudinal, qualitative and quantitative, were covered in this investigation.
The research needed to provide a report any psychiatric diagnoses, admissions, prescriptions, symptoms, or distress of those directly or indirectly impacted by a recognized collective action to fulfil the requirements for inclusion in the outcome. Studies based on labor conflicts were left out because they sought to alter how resources or positions were distributed within an organization. Events involving protracted, paramilitary wars orchestrated by states or individuals with state-like characteristics were also disregarded.
Searches were conducted in Science Direct, PubMed, Web of Science, Google Scholar and PsycINFO for studies released between the beginning of each database’s existence from 2000 to 2022. We also looked through the references in the retrieved publications to find other studies. Search terms included “riots”, “protest”, “unrest”, “civil disorders”, “demonstration”, “revolution”, and “campaign”, as well as terms for social movements that use collective activities as a strategy, such as “social movement”, “political movement”, and “socio-political movement”. These were used to find prospective publications addressing group activity and mental health results, in addition to phrases like “mental health”, “mental disorders”, “behavioral symptoms”, and “psychological”. An illustration of the thorough search plan is shown in Table 2.
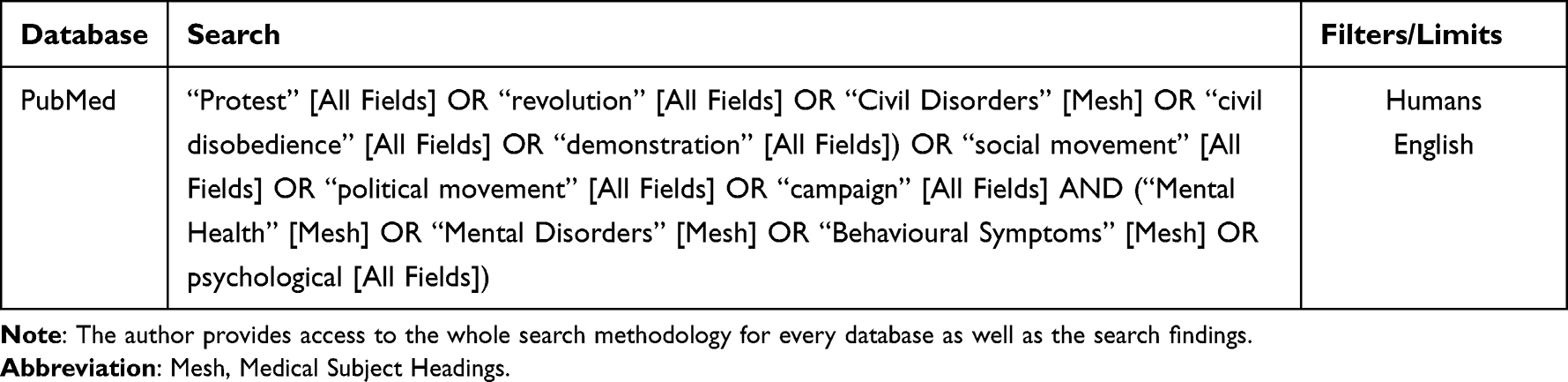 |
Table 2 Electronic Search Strategy for PubMed |
After retrieving, the published articles were independently reviewed by the researcher for inclusion, and any disagreements were settled. The researcher first looked at the titles and abstracts to evaluate if the publications fit the inclusion requirements. The complete texts of the articles were carefully reviewed after the first two rounds of screening, and those that met the exclusion criteria were eliminated.
Evidence Grading
The Newcastle-Ottawa Scale (NOS), which is advised by the Cochrane Collaboration for the assessment of non-randomized trials, was used by the author to independently grade the standard of methodology across all included research.10 Concerning earlier adaptations,11,12 the NOS was updated for the evaluation of cross-sectional research quality.
Synthesis of Results
The data have been summarized by outcomes related to mental health. The researcher prioritized findings from longitudinal studies first, and where none were available, we evaluated cross-sectional studies with high NOS values under systematic review procedures.13 We prioritized data based on random samples taken from the general population when determining the incidence of mental health outcomes.
Results
Description of Studies
There were 1189 items found in the first search. We found 41 papers after implementing the prerequisites for inclusion and exclusion and looking through the research contained in the reference lists (Figure 1). A total of 23,132 persons were involved in this study, which included 16 cross-sectional, 4 systematic reviews, 4 surveys, 3 observational, 3 exploratory, 3 epidemiological, 3 explanatory mixed methods, and 5 qualitative research (not including time series and qualitative studies without a sample size specification). Table 2 and “Supplementary Table 1” summarise the study designs and main findings from all the selected research.
 |
Figure 1 PRISMA Flow Diagram. Note: This diagram shows the systematic process we followed to include papers captured by our search. |
Sample Characteristics
Eight studies used random samples, some drawn from the general population,14,15 others by sex,16,17 remaining from affected communities.18,19 This research includes a representative sample study that illustrates the nation’s diversity, considering factors such as age, gender, ethnicity, urban-rural distribution, and socioeconomic status. Inclusivity is vital, encompassing various geographic regions: Northern, Southern, Eastern, and Western India. Moreover, urban and rural populations, as well as tribal communities, are also included for a comprehensive view. The number of study participants ranged from 17 to 22,377, with ten studies having participants greater than 5000, twelve investigations involving over than 300–850 individuals, six studies recruiting a population of more than 150, as well as two studies with less than 100 participants.
Examination of Mental Health Outcomes
From Table 3 we can check that the most often examined outcome was depression and mental health concerns, which were noted in a third of the studies (n = 20, 48.78%), followed by post-traumatic stress disorder (PTSD) (n = 5, 12.19%) and anxiety disorder/anxiety symptoms (n = 6, 14.63%). Other effects included an increase in alcohol use disorder, homelessness, and a high chance of poverty. (Table 3).
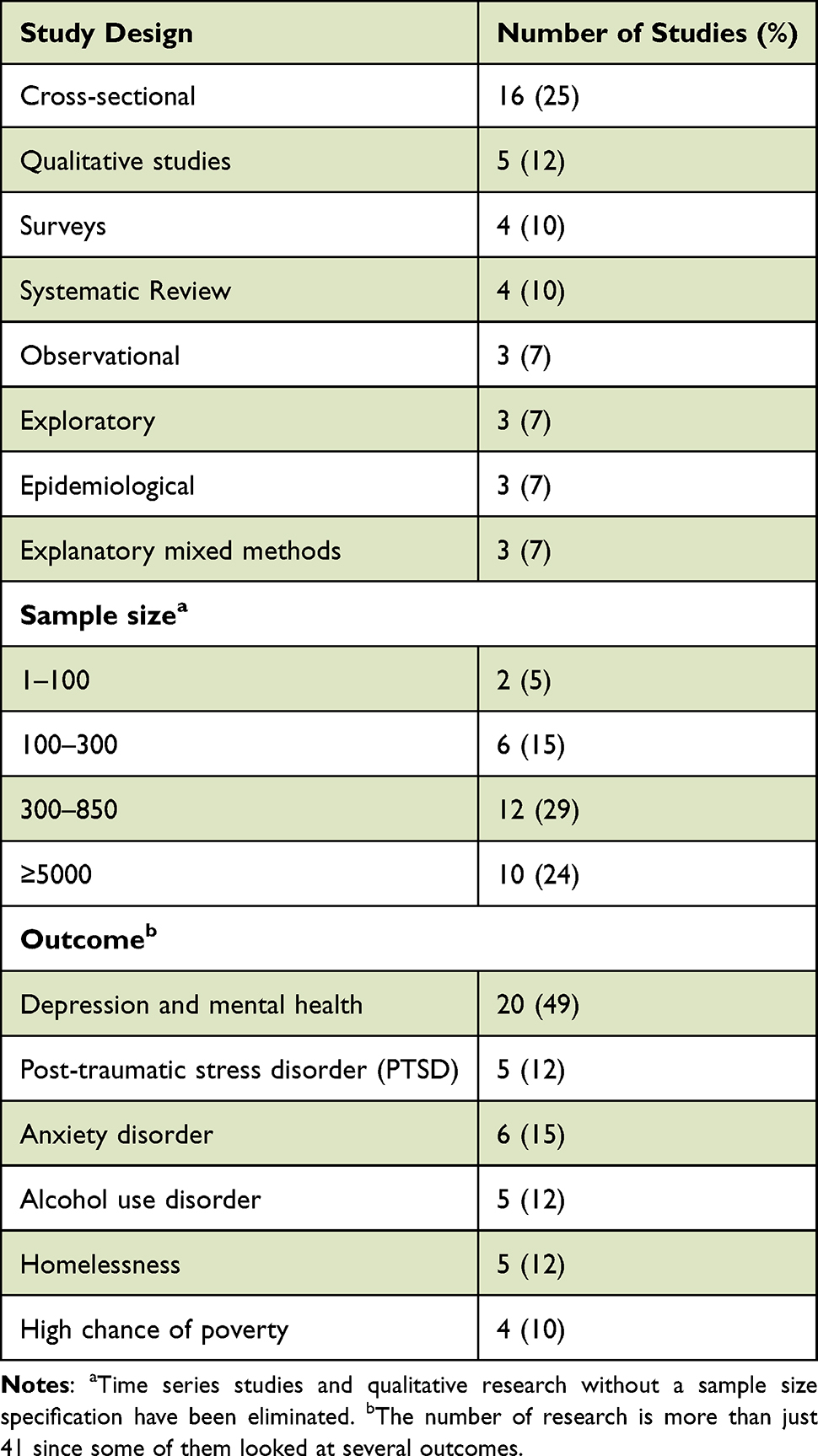 |
Table 3 Outcome of the Systematic Review |
Discussion
This is, as far as we are aware, the first comprehensive analysis of collective activities and mental health. The two most often researched mental health consequences of mass actions, riots, and social unrest are depression and PTSD.15,20–22 Notably, the frequency of depression and PTSD after mass gatherings appears to be equivalent to those who have been victims of violence, riots and social unrest in both the general population and among victims of violence.15,20,23,24 Individual characteristics (such as poor socioeconomic status, female sex, psychological resilience, health status, and social support), the nature of the event itself (such as being exposed to violence, coverage in the media, and level of engagement), and post-event situations (such as loss of personal as well as social resources), Unemployment rates were indicators of risk for psychopathology following collective actions.14,16,25–28
According to some evidence (n = 5; 12% of the included studies), collective acts might also linked to enhanced mental health, including a reduction in depression and suicides.18,29–32 This conclusion might be clarified by the fact that when individuals voice their frustrations collectively, it can be cathartic. Additionally, stronger social links among subpopulations that are either in favor of or against the collective action’s cause might improve social bonds, which in turn could mitigate the negative effects of the stressful environment.18,31,32
Therefore, different means must be used for nonviolent collective action to affect health. The effect of riots on mental health might be explained by the stressors and stress assessment processes.33 Stress reactivity refers to an increased risk of mental illness following stress exposure, whereas stressors are operationalized as external pressures that test a person’s potential for adaptation.14,34,35 The first domain of the Research Domain Criteria matrix36 recognizes the significance of stress reactivity in the appearance of mental diseases. As an outcome, exposure to stress and an individual’s stress response might be seen as the causes of threat for mental health illnesses after collective activities.14,18 Conflicts between individuals and the interruption of healthcare services are examples of how collective activities may create stress.37,38 Similar to this, the function of social relationships in reducing stress may help to explain the protective impact of social support.39–41
Strengths and Limitations
Although completing small-scale investigations cannot indicate the incidence of psychological morbidities in this research, this review has methodically documented existing data, highlighted the research gap, and highlighted the necessity for more in-depth research. However, there are some limitations to our review. In comparison to the population in India, the population that some researchers we synthesized addressed is small. In addition, the majority of the research was cross-sectional, and the techniques and instruments employed varied widely. Therefore, it is impossible to generalize the results of these investigations. Cross-study comparisons are challenging since various mental health metrics were used in the research. According to Galea and Maxwell (2009), validated standardized measures or diagnostic interviews should be used in future research to evaluate mental health. Lastly, even though Higgins and Green (2012a) of the Cochrane Collaboration suggest using the NOS to assess the excellence of non-randomized research, the NOS was only intended for cohort and case-2 studies. However, to evaluate cross-sectional research, the NOS has been adjusted in light of earlier evaluations.11,12 Another limitation of this study is that the articles included in the review were screened by a single reviewer. The lack of additional reviewers may have increased the likelihood of bias or oversight in the selection of papers, despite attempts to assure completeness and correctness in the screening process. Multiple reviewers might improve the robustness and dependability of the literature review process in future research.
In conclusion, according to this systematic study, within the previous three decades, there has been very little community-based research on issues related to mental health among indigenous groups. Of them, even fewer studies focused exclusively on tribal communities. A limited range of mental health issues, primarily alcoholism, anxiety, depression and suicide were explored by these investigations. Despite the rise in collective activities throughout the world and their known effects on mental health,3 collective actions are frequently underappreciated as a sociopolitical factor influencing mental health. The assessment of how communal activities affect mental health and the underlying mechanisms has just recently started in the literature. Therefore, it would be appropriate to research this new area of study.
Funding
This research was funded by the Deanship of Scientific Research, King Faisal University, Al-Hasa, Saudi Arabia (Grant No. GrantA119).
Disclosure
The author declares no conflicts of interest in this work.
References
1. Tarrow SG. Power in Movement: Social Movements and Contentious Politics. New York: Cambridge University Press; 2011.
2. Banks AS, Wilson KA. Cross-National Time-Series Data Archive. Jerusalem: Databanks International; 2017.
3. Ortiz I, Burke S, Berrada M, et al. World Protests 2006–2013. New York: Initiative for Policy Dialogue and Friedrich-Ebert-Stiftung; 2013.
4. Stephan MJ, Chenoweth E. Why civil resistance works: the strategic logic of nonviolent conflict. Int Sec. 2008;33(1):7–44. doi:10.1162/isec.2008.33.1.7
5. Charlson F, Van Ommeren M, Flaxman A, et al. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet. 2019;394(10194):240–248. doi:10.1016/S0140-6736(19)30934-1
6. Galea S, Maxwell A. Methodological challenges in studying the mental health consequences of disasters. In: Neria Y, Galea S, Norris FH, editors. Mental Health and Disasters. Cambridge: Cambridge University Press; 2009:579–593.
7. Galea S, Nandi A, Vlahov D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol Rev. 2005;27(1):78–91. doi:10.1093/epirev/mxi003
8. Perlman SE, Friedman S, Galea S, et al. Short-term and medium-term health effects of 9/11. Lancet. 2011;378(9794):925–934. doi:10.1016/S0140-6736(11)60967-7
9. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Br Med J. 2009;339(jul21 1):b2. doi:10.1136/bmj.b2700
10. Higgins JPT, Green S. Tools for assessing methodological quality or risk of bias in non-randomized studies [Online]; 2012a. Available from: http://handbook-5-1.cochrane.org/chapter_13/13_5_2_3_tools_for_assessing_methodological_quality_or_risk_of.htm.
11. Anglin RE, Samaan Z, Walter SD, et al. Vitamin D deficiency and depression in adults: systematic review and meta-analysis. Br J Psychiatry. 2012;202(2):100–107. doi:10.1192/bjp.bp.111.106666
12. Patra J, Bhatia M, Suraweera W, et al. Exposure to second-hand smoke and the risk of tuberculosis in children and adults: a systematic review and meta-analysis of 18 observational studies. PLoS Med. 2015;12(6):e1001835. doi:10.1371/journal.pmed.1001835
13. JAMA. Instructions for authors [Online]; 2018. Available from: https://jamanetwork.com/journals/jama/pages/instructions-for-authors#SecSystematicReviews.
14. Pandey G, Moghal S, Barodia R, Carey W. COVID-19 and its effects on the mental health of people living in Urban Slums in India. J Inf Knowl Manag. 2022;21(Supp 1):2240003. doi:10.1142/S0219649222400032
15. Srivastava S, Purkayastha N, Chaurasia H, et al. Socioeconomic inequality in psychological distress among older adults in India: a decomposition analysis. BMC Psychiatry. 2021;21(1):179. doi:10.1186/s12888-021-03192-4
16. Sathyanath MS, Kundapur R. Epidemiological correlates of psychological distress in a rural community of South India: a Cross-sectional Study. Indian J Community Med. 2020;45(2):240–243. doi:10.4103/ijcm.IJCM_129_19
17. Gupta A, Coffey D. Caste, religion, and mental health in India. Popul Res Policy Rev. 2020;39(6):1119–1141. doi:10.1007/s11113-020-09585-9
18. Subbaraman R, Nolan L, Shitole T, et al. The psychological toll of slum living in Mumbai, India: a mixed methods study. Soc Sci Med. 2014;119:155–169. doi:10.1016/j.socscimed.2014.08.021
19. Thomas A, John Sergenti E. Economic growth and ethnic violence: an empirical investigation of Hindu–Muslim riots in India. J Peace Res. 2010;47(5):535–546. doi:10.1177/0022343310373032
20. Reddy V. Mental health issues and challenges in India: a review. Int J Soc Sci Manag Entrep. 2019;3(2): 72–78.
21. Böge K, Zieger A, Mungee A, et al. Perceived stigmatization and discrimination of people with mental illness: a survey-based study of the general population in five metropolitan cities in India. Indian J Psychiatry. 2018;60(1):24–31. doi:10.4103/psychiatry.IndianJPsychiatry_406_17
22. Bhavnani RR, Lacina B. The effects of weather-induced migration on sons of the Soil Riots in India. World Politics. 2015;67(4):760–794. doi:10.1017/s0043887115000222
23. Maheshwari R, Steel Z. Mental health, service use and social capital among Indian-Australians: findings of a wellbeing survey. Australas Psychiatry. 2015;20(5):384–389. doi:10.1177/1039856212458980
24. de Jong K, van de Kam S, Ford N, et al. Conflict in the Indian Kashmir Valley II: psychosocial impact. Confl Health. 2008;2(1):11. doi:10.1186/1752-1505-2-11
25. Jena R, Pradhan B, Beydoun G. Earthquake vulnerability assessment in Northern Sumatra province by using a multi-criteria decision-making model. Int J Disaster Risk Reduct. 2020;46:101518. doi:10.1016/j.ijdrr.2020.101518
26. Pai S, Sajjan K. Communal mobilization and riots in Western Uttar Pradesh: muzaffarnagar and Shamli Districts. In: Everyday Communalism: Riots in Contemporary Uttar Pradesh (Delhi, 2018; Online Edn). Oxford Academic; 2019. doi10.1093/oso/9780199466290.003.0006
27. Gangopadhyay P, Nilakantan R. Estimating the effects of climate shocks on collective violence: ARDL evidence from India. J Dev Stud. 2018;54(3):441–456. doi:10.1080/00220388.2016.1269890
28. Lakhan R, Ekúndayò OT. National sample survey organization survey report: an estimation of the prevalence of mental illness and its association with age in India. J Neurosci Rural Pract. 2015;6(01):51–54. doi:10.4103/0976-3147.143194
29. Farooqui N, Ahmad A. Communal violence, mental health and their correlates: a cross-sectional study in two riot affected districts of Uttar Pradesh in India. J Muslim Minor Aff. 2021;41(3):510–521. doi:10.1080/13602004.2021.1999139
30. Bhargava R, Gupta N. Social unrest and its impact on mental health. Ind J Soc Psych. 2020;36(1):3–4. doi:10.4103/ijsp.ijsp_27_20
31. Chauhan SK, Dhar M. Prevalence and predictors of mental health disorder among the adolescent living in the slums of Lucknow, India: a cross-sectional study. Community Ment Health J. 2020;56(3):383–392. doi:10.1007/s10597-019-00452-2
32. Mathias K. Shadows and light: examining community mental health competence in North India; 2016.
33. Silvanus V, Subramanian P. Epidemiological study of mental morbidity in an urban slum community in India for the development of a community mental health program. Nepal Med Coll J. 2012;14(1):13–17.
34. Gopikumar V. Understanding the Mental Ill Health - Poverty - Homelessness Nexus in India: strategies that promote distress alleviation and social inclusion; 2014.
35. Jaffrelot C. Communal riots in Gujarat: the state at risk? 2003.
36. Copland I. The production and containment of communal violence: scenarios from Modern India, South Asia. J South Asian Stud. 2010;33(1):122–150. doi:10.1080/00856401003592503
37. Basu H. Contested practices of control: psychiatric and religious mental health care in India. Curare. 2009;32(1):2.
38. Irshad S, Begum N. COVID-19 and its psychological impact on working parents. Technium Social Sciences Journal. 2021;24:389–399.
39. Gupte J, Justino P, Tranchant J-P. Households amid Urban Riots: the economic consequences of civil violence in India. J Conflict Resol. 2014;58(8):1445–1473. doi:10.1177/0022002714547886
40. Bhadra S. Psychosocial support for the children affected by communal violence in Gujarat, India. J Appl Psychoanal Stud. 2012;9(3):212–232. doi:10.1002/aps.1327
41. Thara R, Padmavati R, Aynkran JR, John S. Community mental health in India: a vision beckoning fulfillment? Can J Community Mental Health. 2008;21(2):131–137. doi:10.7870/cjcmh-2002-0021
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.