Back to Journals » Cancer Management and Research » Volume 18

Common Bile Duct Diameter in Bladder Urothelial Carcinoma: A Case-Control Study
Authors Dadkhah A, Zolfaghari M, Bagheri SM, Soltani S, Fooladi Z, Emami M
Received 8 November 2025
Accepted for publication 21 June 2026
Published 24 June 2026 Volume 2026:18 580011
DOI https://doi.org/10.2147/CMAR.S580011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Shari Youngblood
Adeleh Dadkhah,1 Masoome Zolfaghari,1 Seyed Morteza Bagheri,1 Sepideh Soltani,2 Zahra Fooladi,1 Masoud Emami3
1Department of Radiology, School of Medicine, Iran University of Medical Sciences, Tehran, Iran; 2Department of Radiation Oncology, School of Medicine, Iran University of Medical Sciences, Tehran, Iran; 3Department of Radiology, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran
Correspondence: Masoome Zolfaghari, Department of Radiology, School of Medicine, Iran University of Medical Sciences, Tehran, Iran, Email [email protected]
Background: Although sporadic case reports have suggested an association between bladder urothelial carcinoma and common bile duct (CBD) dilation, no comprehensive study has investigated this association. This study aimed to compare CBD size in patients with urothelial carcinoma and matched controls.
Methods: In this retrospective case-control study, we analyzed 63 patients diagnosed with urothelial carcinoma alongside a control group of 63 individuals who were matched for age, gender distribution, smoking habits, and opium use. Demographic and clinical data were extracted from patient records. An experienced radiologist who was blinded to the study objectives measured the diameter of the CBD using CT scans.
Results: The mean CBD diameter was larger in patients with urothelial carcinoma compared with the control group (6.81± 2.77 vs 5.40± 1.43, p = 0.004). Furthermore, individuals with tumor recurrence (8.58± 3.45 vs 6.15± 2.17, p = 0.005) or metastases (8.35± 4.16 vs 6.52± 2.38, p = 0.049) exhibited significantly higher CBD diameters compared with those without. However, regression analysis identified tumor recurrence (OR=7.63 [1.64– 35.60]) and abnormal CRP (OR=9.85 [1.46– 66.62]) as the only significant risk factors for abnormal CBD diameter.
Conclusion: Patients with urothelial carcinoma demonstrated larger CBD diameters than matched controls, with greater dilation observed among those with tumor recurrence. These findings suggest a potential association between urothelial carcinoma and CBD diameter; however, given the observational design and limited sample size, the results should be considered exploratory and hypothesis-generating. Further large-scale prospective studies are required to validate these findings, clarify underlying mechanisms, and determine their clinical significance.
Keywords: urothelial carcinoma, CT imaging, common bile duct, bladder cancer, bile ducts
Introduction
Bladder cancer is among the most prevalent cancers worldwide. It ranks as the tenth most common cancer globally and the seventh most common in men, with its incidence rising, particularly in developing countries.1,2 Urothelial carcinoma is the most prevalent subtype of bladder cancer and is characterized by a high risk of recurrence and progression.3 Smoking is considered one of the major risk factors for bladder cancer. Other reported risk factors include environmental and occupational factors, family history, opium consumption, red meat, obesity, and infection with Schistosomiasis haematobium.4,5
Beyond its localized effects, bladder cancer may involve other organs due to its pathophysiology or associated treatments. Studies have indicated that the most common site of metastasis is the lymph nodes, with initial regional involvement progressing to the common iliac and paraaortic lymphatic chains.6–8 The liver, bone, lungs, and peritoneum have also been reported as common distant metastatic sites.7 However, involvement of the biliary system in bladder urothelial carcinoma appears to be uncommon and has mainly been described in isolated case reports.9–11
A limited number of reports have described biliary obstruction or biliary tract involvement in patients with metastatic bladder urothelial carcinoma.9–11 Clinical observation at Hasheminejad Hospital in Tehran, a kidney and urinary tract subspecialty center, suggested a number of patients with bladder urothelial carcinoma had an increased diameter of the common bile duct. Possible explanations for non-obstructive CBD dilation may include advanced patient age, a higher prevalence of opium use, metastatic involvement of the biliary system, effects of medical treatments or the secretion of cytokines or inflammatory mediators that may affect the wall of the common bile duct and contribute to its dilation; however, these mechanisms remain hypothetical.
A number of patients with bladder urothelial carcinoma who had a dilated CBD on CT scan underwent Endoscopic Retrograde Cholangiopancreatography (ERCP) or Magnetic Resonance Cholangiopancreatography (MRCP), but these investigations did not identify an anatomical obstructive cause.
Given the extensive retroperitoneal lymphatic network and the communication of hepatic and biliary lymphatic drainage with paraaortic and peripancreatic lymphatic pathways, biliary tract involvement in advanced urothelial carcinoma is biologically plausible.12,13 These observations suggest that urothelial carcinoma may affect the biliary system through direct metastatic spread or through indirect inflammatory, paraneoplastic, or treatment-related mechanisms. However, no comprehensive study has investigated a possible association between bile duct dilation and bladder urothelial carcinoma.
Given the limited available evidence, we hypothesized that patients with bladder urothelial carcinoma may have a larger common bile duct diameter compared with individuals without the disease. Clarifying this potential association may improve understanding of hepatobiliary findings encountered in these patients and help guide future investigations regarding their clinical significance. Therefore, this study compared the mean CBD diameter between patients diagnosed with bladder urothelial carcinoma and a control group.
Materials and Methods
Study Design and Setting
This retrospective case-control study was conducted at Shahid Hasheminejad Hospital, a referral academic hospital affiliated with the Iran University of Medical Sciences, from March 2023 to March 2024. All participants provided informed consent before enrollment. All methods were performed in accordance with the relevant guidelines and regulations. The Iran University of Medical Sciences ethics committee approved the study (IR.IUMS.FMD.REC.1402.207).
Participants
This study evaluated CBD diameter in patients with bladder urothelial carcinoma (case group) and individuals without urothelial carcinoma (control group). The sample size was calculated using G*Power software (version 3.1.9.2). With a 95% confidence level, 80% statistical power, and an effect size of 0.5, the required sample size was 63 participants per group.
The case group included patients with histopathologically confirmed bladder urothelial carcinoma who underwent abdominopelvic CT scans with CBD measurement during the study period, selected through convenience sampling. The control group consisted of outpatients who underwent abdominopelvic CT imaging during the same study period for non-hepatobiliary and non-oncologic indications. Based on available medical records, these individuals had no recent hospitalization for major medical conditions and no documented history of bladder urothelial carcinoma, other malignancies, or liver and biliary diseases. Absence of malignancy and hepatobiliary pathology was also confirmed through review of medical records and CT imaging findings. The control group was individually matched 1:1 to the case group based on age (± 5 years), gender, smoking status, and opium use as common confounders associated with increased CBD diameter.
Participants in both groups were required to be ≥18 years old, have complete medical records, and show no visible stones or obstructive lesions within the CBD. Additional criteria for the case group included a histopathological diagnosis of bladder urothelial carcinoma, while the control group required no history of malignancy. Exclusion criteria included other malignancies (except bladder urothelial carcinoma in the case group), liver or biliary tract disease, CBD stones or obstructive lesions, abnormal bilirubin levels, incomplete records, or inadequate imaging data. Patients with abnormal bilirubin levels were excluded to reduce the likelihood of occult biliary obstruction or hepatobiliary dysfunction independently affecting CBD diameter.
Data Collection and Imaging Review
Demographic variables (age and sex), clinical information (smoking, opium use, drug history, C-reactive protein (CRP), history of chemotherapy, and radiotherapy), and tumor characteristics (grade, multifocality, tumor recurrence, metastasis) were extracted from patient records. Tumor recurrence was defined as reappearance of histopathologically confirmed urothelial carcinoma after prior treatment or documented remission. Metastasis was defined as radiologically or histopathologically confirmed spread of urothelial carcinoma beyond the primary tumor site. CBD diameter was measured on abdominopelvic CT scans by an experienced radiologist, blinded to the study objectives, following standard measurement protocols. All CT scans were performed using a 16-slice GE CT scanner with 2.5-mm slice thickness. Imaging was obtained with and without intravenous contrast enhancement, including portal venous phase acquisitions when contrast was administered. Images were reconstructed and reviewed using the Picture Archiving and Communication System (PACS). CBD diameter was measured manually on oblique coronal reconstructed images oriented parallel to the long axis of the common bile duct, with measurements obtained at the mid-CBD level.
Statistical Analysis
All statistical analyses were conducted using SPSS software (version 25, IBM Corporation, NY, USA). We used frequency to report qualitative variables and mean ± standard deviation (SD) to report quantitative variables. There were no missing data for any variables. The Kolmogorov–Smirnov test, Q-Q plot, and P-P plot were applied to assess the normality of quantitative variables.
CBD diameter was compared between patients with urothelial carcinoma and the control group, as well as within urothelial carcinoma subgroups using the Mann–Whitney U and Kruskal Wallis tests. The independent t-test was applied to compare age, which followed a normal distribution. The Chi-square and Fisher’s exact tests were used to assess relationships between categorical variables.
Based on thresholds of 10 mm for individuals over 60 years and 8 mm for those under 60 years, CBD diameter was categorized as normal or abnormal.14 Univariate regression analysis was performed to evaluate the association between potential predictors and abnormal CBD diameter. Variables with p<0.05 in the univariate analysis were subsequently included in a multivariable logistic regression model to identify independent predictors of abnormal CBD diameter. P-values < 0.05 were considered statistically significant.
Results
Sixty-three patients with urothelial carcinoma and 63 controls, matched for age, sex, smoking status, and opium use, were studied. There were 57 males (90.5%) and 6 females (9.5%) in each group. 71.4% of the subjects in each group were smokers, and the frequency of opium use in each group was 30.2%. The mean age of participants was 63.86±13.43 in the urothelial carcinoma group and 63.83±13.66 in the control group (p = 0.981), Table 1.
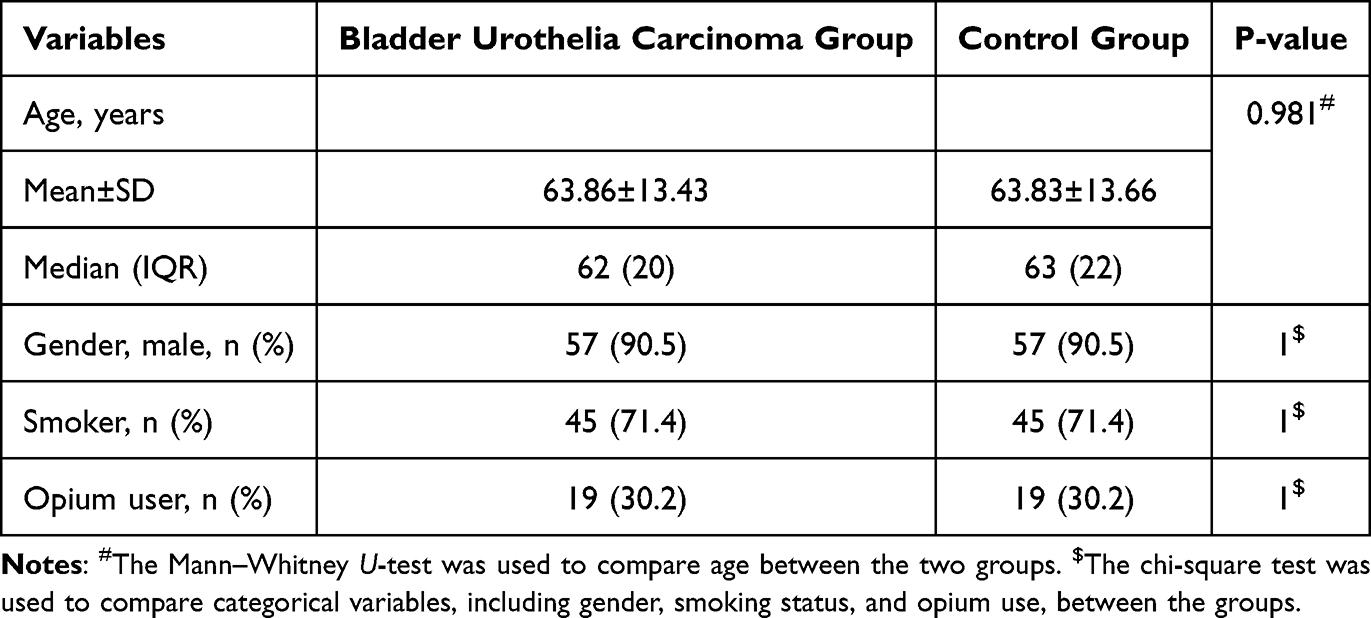 |
Table 1 Comparison of Demographic and Lifestyle Variables Between the Bladder Urothelial Carcinoma Group and the Control Group |
Among the 63 patients with bladder urothelial carcinoma, 52 (82.5%) had high-grade disease. Multifocal tumors were observed in 25 (39.7%) cases, and 17 (27%) experienced tumor recurrence. Metastasis occurred in 10 (15.9%) patients, while only one had a multicentric tumor. All participants in the urothelial carcinoma group were receiving analgesic treatment. Additionally, 62 participants (98.4%) were receiving antibiotic therapy. Among these, 57 participants (90.5%) were prescribed standard-spectrum antibiotics, while 5 (7.9%) received broad-spectrum antibiotics. Regarding inflammatory markers, 6 patients (9.5%) had abnormal CRP levels, whereas 57 (90.5%) had CRP levels within the normal range.
The mean diameter of the CBD in patients with bladder urothelial carcinoma (6.81±2.77) was significantly higher than that in the control group (5.40±1.43). The median (interquartile range) CBD diameter was significantly higher in patients with bladder urothelial carcinoma than in the control group (6 [3] vs 5[2]; Z=−2.846, p = 0.004, r=0.25, Figure 1).
 |
Figure 1 Distribution of common bile duct (CBD) diameter in patients with bladder urothelial carcinoma and in the control group. |
When comparing CBD diameter between patients with high-grade and low-grade urothelial carcinoma, the high-grade group had a larger diameter, but the difference was not statistically significant (p = 0.26), Table 2. Similarly, there was no significant difference in CBD diameter between patients with multifocal tumors and those without (p = 0.26). However, patients with a history of tumor recurrence had a significantly larger CBD diameters than those without recurrence (median 6.75, mean 8.58 vs median 6, mean 6.15, p = 0.005). Due to the presence of only one patient with a multicentric tumor, no comparison of CBD diameter could be made for this subgroup. Finally, the mean CBD diameter in patients with metastatic urothelial carcinoma was significantly larger than in those with non-metastatic urothelial carcinoma (median 7, mean 8.35 vs median 6, mean 6.52, p = 0.049), Table 2.
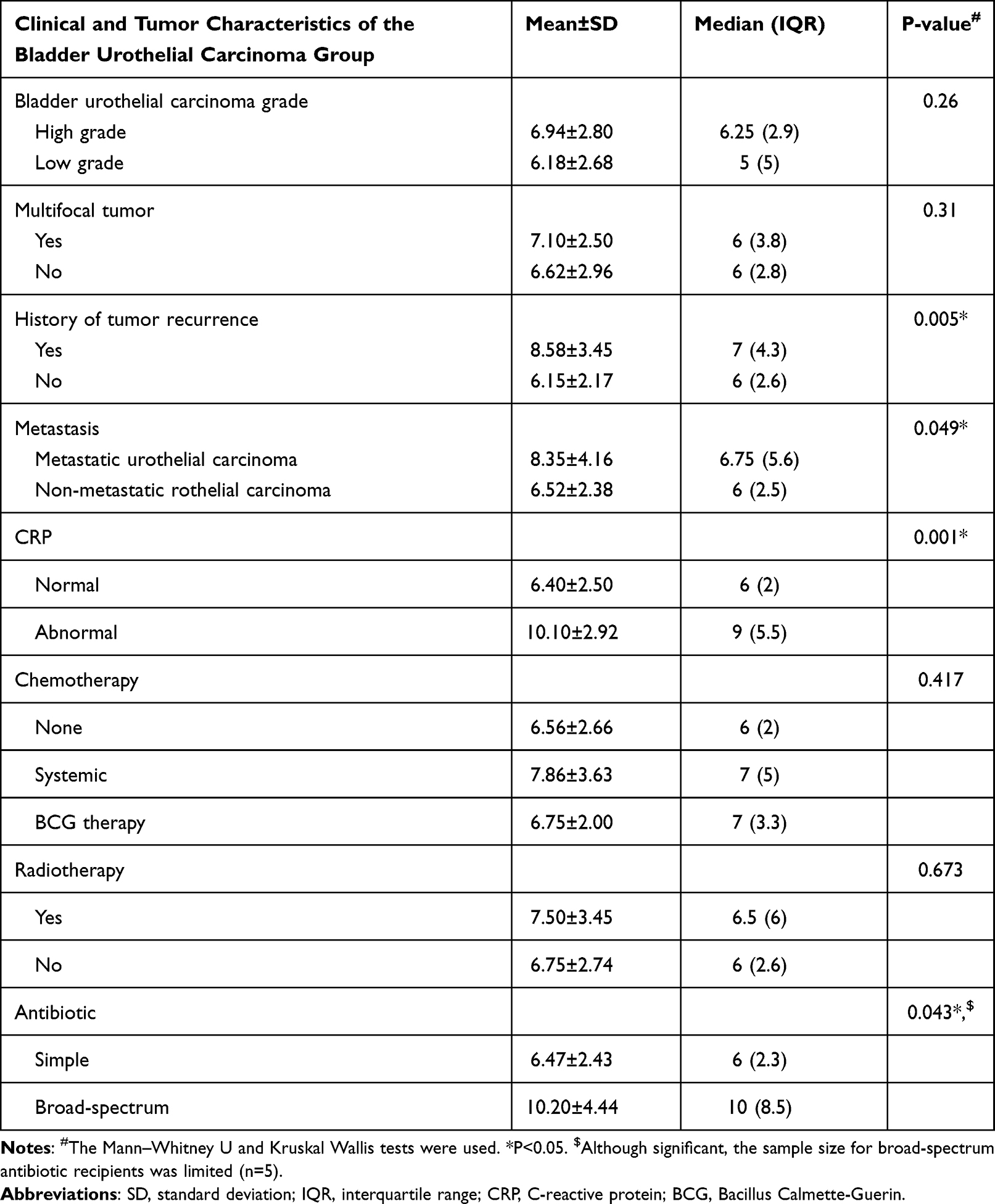 |
Table 2 Clinical Factors Associated with Common Bile Duct Diameter in Patients with Bladder Urothelial Carcinoma |
In patients with urothelial carcinoma, univariate regression analysis using dichotomized CBD diameter (normal vs abnormal) showed that a history of tumor recurrence (OR = 7.35 [95% CI: 1.30–80.10], p = 0.006) and abnormal CRP (OR = 9.33 [95% CI: 1.72–50.76], p = 0.010) in the case group were the only significant risk factors for an abnormal CBD diameter.
While the CBD diameter was significantly larger in patients with metastatic disease compared with those without, metastasis did not emerge as a statistically significant predictor of an abnormal CBD diameter in the regression analysis (OR = 2.41 [95% CI: 0.11–51.40], p = 0.265). Furthermore, factors such as age, gender, smoking, opium use, tumor grade, multifocality, systemic chemotherapy, BCG therapy, and radiotherapy were not found to be significant risk factors for an abnormal CBD diameter, Table 3.
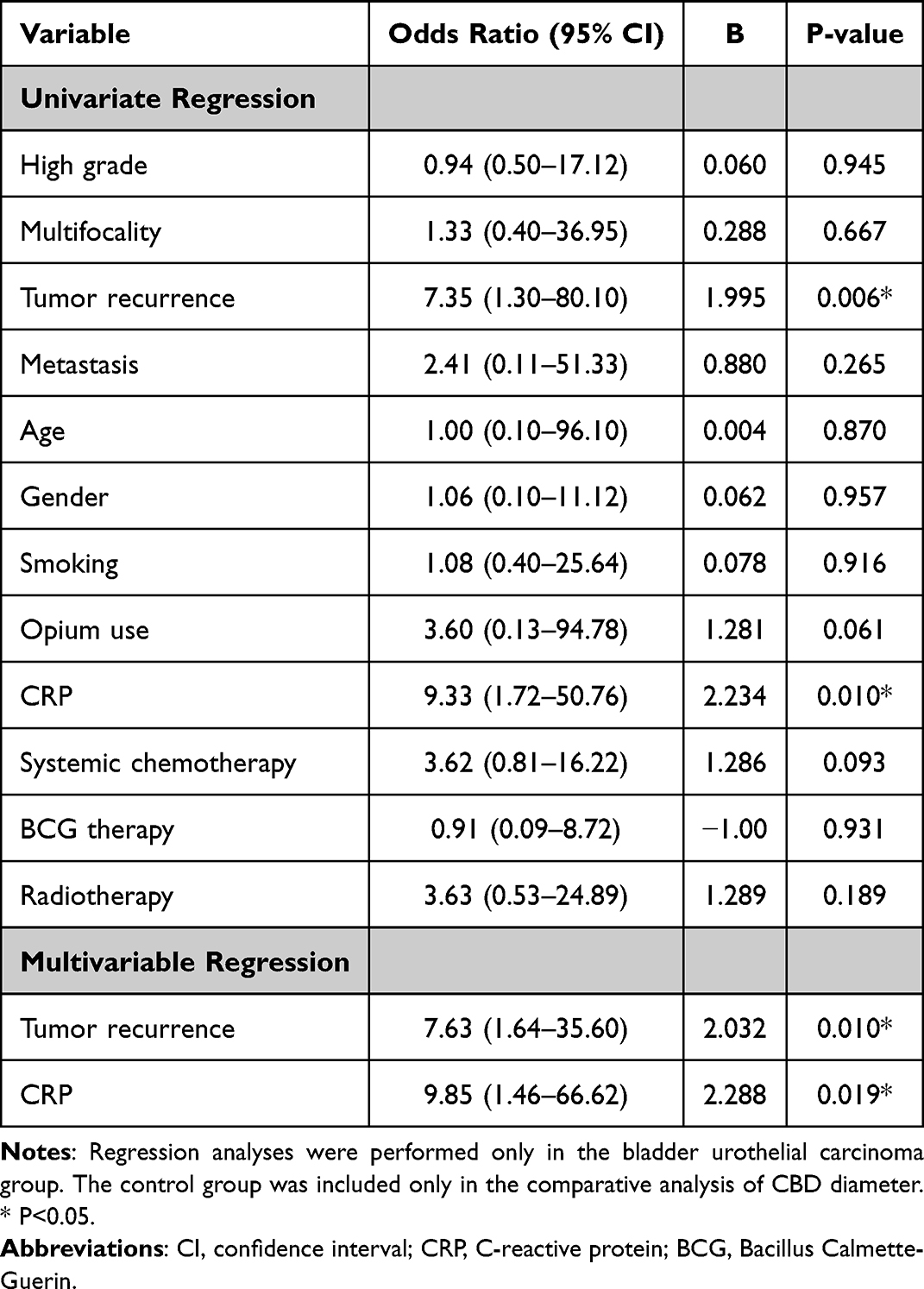 |
Table 3 Univariate and Multivariable Regression Analyses of Factors Associated with Common Bile Duct Diameter in Patients with Bladder Urothelial Carcinoma |
Multivariable regression analysis revealed that patients with a history of tumor recurrence had a 7.63-fold and those with abnormal CRP levels had a 9.85-fold increased likelihood of presenting with an abnormal CBD diameter (p = 0.010, 0.019, respectively), Table 3.
Discussion
Principal Findings
We investigated the relationship between bladder urothelial carcinoma and CBD diameter, comparing 63 patients with urothelial carcinoma with 63 matched controls. Patients with bladder urothelial carcinoma exhibited a significantly larger mean CBD diameter than the control group, without any visible stones or obstructive lesions along the CBD or increased bilirubin levels. By matching for confounding factors such as age, sex, smoking, and opium use, the observed difference in CBD diameter can be more confidently attributed to the presence of bladder urothelial carcinoma. Although the absolute mean difference in CBD diameter between groups was modest (approximately 1.4 mm), the difference persisted despite matching for major confounders. All CT scans were obtained using the same scanner, and measurements were performed by a blinded experienced radiologist to minimize technical bias. Nevertheless, the clinical significance of a difference of this magnitude should be interpreted cautiously in the context of well-characterized physiologic variability in CBD diameter. Recent large-scale MRCP-based population studies have demonstrated that CBD diameter is strongly age-dependent, with upper reference limits extending to approximately 8 mm in individuals younger than 65 years and up to 10–11 mm in older populations, even in the absence of biliary pathology.15,16 Reported upper reference limits vary across studies and populations, particularly in older individuals, in whom values exceeding the traditionally accepted threshold may still be considered physiologic. In addition, CT- and MRCP-based studies have shown variability in CBD measurements depending on imaging modality, measurement location, and observer-related factors, further contributing to a broad normal range.15,17 Functional factors, including sphincter of Oddi tone and transient fluctuations in biliary flow, may also influence short-term variation in duct caliber.18 Therefore, although the observed difference between groups may reflect a true association, its magnitude lies within a physiologic range that is inherently wide, particularly in older populations, emphasizing the need for cautious interpretation and prospective validation using standardized imaging protocols and age-stratified reference values.
We also found that a history of tumor recurrence and abnormal CRP levels were strongly associated with an increased CBD diameter in patients with urothelial carcinoma, as shown by both univariate and multivariable regression analyses. While metastasis was linked to a larger CBD diameter, it did not emerge as a statistically significant predictor in the regression model.
Although tumor recurrence and abnormal CRP remained statistically significant in the multivariable model, these findings should be interpreted cautiously. The relatively small number of abnormal CBD events and the limited sample size may have reduced model stability, contributing to wide confidence intervals and potential overestimation of effect sizes. Differences between univariate and multivariable regressions likely reflect adjustment for coexisting variables, possible collinearity among disease-related factors, and reduced statistical power after stratification. For example, metastasis was associated with larger mean CBD diameter in subgroup analysis but did not remain a significant independent predictor in regression analysis, possibly due to limited event numbers and insufficient precision. Therefore, while the regression findings suggest potential associations, they should be considered exploratory and hypothesis-generating rather than definitive.
Comparison with Previous Literature
Previous studies on the relationship between bladder urothelial carcinoma and biliary dilation are limited to rare case reports of biliary metastasis. Ling et al documented gallbladder infiltration by urothelial cancer in a patient with renal pelvic urothelial carcinoma.9 Similarly, Hong et al reported a case of jaundice in a patient with bladder urothelial carcinoma, where imaging and histopathology revealed metastatic spread to the bile duct wall.10 Fakhoury et al described a patient with ureteral urothelial carcinoma presenting with biliary obstruction, confirmed as metastatic involvement of urothelial origin.11 While these reports highlight the potential for urothelial cancers to involve the biliary system, our study systematically demonstrates an association between bladder urothelial carcinoma and increased CBD diameter without biliary metastasis in a larger cohort, providing statistically significant evidence of this relationship.
Potential Mechanisms
The mechanism by which bladder urothelial carcinoma may influence the common bile duct is not well understood and is likely multifactorial. Possible mechanisms include systemic inflammation, treatment-related effects, and other unidentified mechanisms. Further investigation is needed to clarify these potential pathways.
A plausible explanation for the observed association is the systemic inflammatory response often triggered by malignancies such as urothelial carcinoma. Cancer-associated inflammation involves the release of cytokines and growth factors that can affect distant organs. Specifically, mediators like interleukins and tumor necrosis factor have been shown to alter biliary physiology, potentially contributing to bile duct dilation.19,20 This aligns with our finding that abnormal CRP levels, a marker of systemic inflammation, were significantly associated with increased CBD diameter in patients with urothelial carcinoma. These results suggest that inflammation may play a critical role in the biliary changes observed in bladder urothelial carcinoma, emphasizing the systemic impact of this malignancy beyond its primary site. However, this finding should be interpreted with caution because only a small proportion of patients had abnormal CRP levels. The limited number of cases with elevated CRP may have increased statistical instability and contributed to wide confidence intervals, reducing the precision and generalizability of the observed association. Therefore, although the results may support a possible link between systemic inflammation and CBD dilation in urothelial carcinoma, they should be considered preliminary and require confirmation in larger studies with more robust inflammatory marker representation.
In addition to inflammatory mechanisms, medication-related effects may also contribute to physiologic variation in CBD diameter and should be considered when interpreting imaging findings. Patients with urothelial carcinoma may receive various systemic therapies and supportive medications that could potentially influence hepatobiliary physiology or biliary motility.21 Although the present study excluded patients with overt biliary obstruction and abnormal bilirubin levels, detailed treatment and medication histories were not consistently available; therefore, residual confounding related to pharmacologic exposure cannot be completely excluded.
Metastasis is another important factor to consider. While bladder urothelial carcinoma typically metastasizes to lymph nodes, lungs, liver, and bone,7 rare cases of biliary system involvement have been documented.11 Metastatic spread to the bile ducts can directly cause obstruction, leading to dilation. However, in our study, all patients with anatomical obstructive lesions along the bile ducts or patients with increased bilirubin levels were excluded. Therefore, it does not seem that the cause of the increase in CBD diameter in these patients is tumor metastasis to the bile ducts. The observed discrepancy between the univariate and multivariable analyses may be explained by confounding between metastasis and other covariates, as well as reduced statistical power in the adjusted model due to the limited number of events.
We found that patients with a history of tumor recurrence had a significantly larger CBD diameters compared with those without recurrence. This suggests that more aggressive or advanced disease may exert a greater impact on the biliary system. However, participants with a history of tumor recurrence also tended to be older, raising the possibility of a cumulative effect of age and cancer recurrence on CBD diameter. This finding underscores the importance of vigilant, long-term monitoring in elderly patients with urothelial carcinoma, as both age-related and disease-specific factors may contribute to biliary changes over time.
Clinical Implications
Understanding the mechanisms behind increased CBD diameter in patients with bladder urothelial carcinoma may have potential clinical implications. If future studies confirm that systemic inflammation or metastasis contributes to bile duct changes, monitoring CBD diameter may serve as a potential noninvasive marker of disease progression or systemic involvement. Regular imaging and CBD measurements could assist in disease monitoring and early detection of aggressive disease. At present, however, these findings are exploratory and do not establish CBD diameter as a validated biomarker for clinical decision-making. Further prospective studies are required before such applications can be considered.
On the other hand, awareness that some patients with bladder urothelial carcinoma may demonstrate larger CBD diameters in the absence of clear obstructive pathology could assist clinicians in contextual interpretation of imaging findings. However, this observation alone should not replace standard diagnostic evaluation or preclude invasive investigations such as ERCP when clinically indicated.
Limitations
Despite the potential clinical relevance of these findings, several limitations should be considered. First, the retrospective case-control design limits causal inference and does not permit evaluation of temporal relationships between urothelial carcinoma progression and changes in CBD diameter over time.
Second, although major confounders such as age, sex, smoking, and opium use were matched, residual confounding from unmeasured variables cannot be excluded. These variables may include comorbidities, medication exposure, prior cholecystectomy status, body mass index, and other hepatobiliary influences. Furthermore, detailed baseline tumor staging information, including NMIBC versus MIBC classification and complete TNM staging, was not consistently available in the accessible medical records because of the retrospective nature of the study and incomplete baseline staging documentation. Therefore, the relationship between tumor stage and CBD diameter could not be evaluated comprehensively. In addition, due to the retrospective nature of the study, the temporal relationship between CT imaging and acute illness, hospitalization status, medication exposure (particularly opioids/analgesics), or oncologic treatments such as chemotherapy, intravesical BCG, and radiotherapy could not be consistently established. Therefore, some degree of CBD dilation may reflect treatment-related or systemic inflammatory effects rather than a purely malignancy-specific phenomenon. Third, the relatively small sample size, particularly within subgroup analyses such as recurrence, metastasis, and abnormal CRP, as well as the limited number of abnormal CBD events, may have reduced statistical power and limited the stability of the logistic regression model. In particular, the small number of outcome events raises the possibility of model overfitting, resulting in wide confidence intervals and reduced precision of effect estimates. Therefore, the results of the multivariable analysis should be interpreted cautiously and considered exploratory rather than confirmatory.
Fourth, while participants with abnormal bilirubin or visible obstructive lesions were excluded, more comprehensive biochemical cholestatic markers such as alkaline phosphatase, gamma-glutamyl transferase, and detailed liver function profiles were not uniformly available, which may have limited exclusion of subtle hepatobiliary dysfunction. Finally, although CBD measurements were performed by an experienced radiologist blinded to study objectives, CT-based measurement may still be influenced by physiologic variation, imaging phase, technical factors, and potential measurement variability. These limitations suggest that the findings should be interpreted cautiously and validated through larger prospective multicenter studies with standardized imaging and biochemical assessment.
Conclusions
In this exploratory case-control study, we aimed to investigate whether bladder urothelial carcinoma is associated with increased common bile duct diameter compared with matched controls. Our findings suggest that patients with bladder urothelial carcinoma may have larger CBD diameters, with greater dilation observed more frequently among those with tumor recurrence and metastatic disease, although only recurrence and abnormal CRP remained independently associated with abnormal CBD diameter in multivariable analysis.
These findings should be considered hypothesis-generating rather than conclusive, as the observational design does not establish causality or immediate clinical applicability. While the observed associations may suggest possible links between urothelial carcinoma, disease activity, systemic inflammation, and biliary ductal changes, the single-center case-control design and relatively limited sample size restrict definitive interpretation. Further multicenter prospective studies with larger populations and longitudinal follow-up are needed to validate these findings, clarify underlying mechanisms, and determine whether they hold broader biological or clinical significance.
Data Sharing Statement
Datasets are not publicly available but are accessible upon reasonable request from the corresponding author.
Ethics Approval and Consent to Participate
The study protocol complies with the Declaration of Helsinki and The Iran University of Medical Sciences ethics committee approved the study (IR.IUMS.FMD.REC.1402.207). Informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Artificial Intelligence Disclosure
During the preparation of this work authors used OpenAI ChatGPT4 to paraphrase and harmonize text. After using this tool, the authors reviewed and edited the content as needed and took full responsibility for the content of the publication.
Disclosure
The authors declare no competing interests.
References
1. Ferlay J, Ervik M, Lam F, et al. Global cancer observatory: cancer today. Lyon: International Agency for Research on Cancer; 2020. Available from: https://gco.iarc.who.int/today.
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–10. doi:10.3322/caac.21492
3. Redondo-Gonzalez E, de Castro LN, Moreno-Sierra J, et al. Bladder carcinoma data with clinical risk factors and molecular markers: a cluster analysis. Biomed Res Int. 2015;2015:168682. doi:10.1155/2015/168682
4. Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of bladder cancer. Med Sci. 2020;8(1):15.
5. Kalan Farmanfarma K, Mahdavifar N, Salehiniya H. Bladder cancer in Iran: an epidemiological review. Res Rep Urol. 2020;12:91–103. doi:10.2147/RRU.S232417
6. Vikram R, Sandler CM, Ng CS. Imaging and staging of urothelial carcinoma: part 1, lower urinary tract. AJR Am J Roentgenol. 2009;192(6):1481–1487. doi:10.2214/AJR.08.1318
7. Shinagare AB, Ramaiya NH, Jagannathan JP, Fennessy FM, Taplin M-E, Van den Abbeele AD. Metastatic pattern of bladder cancer: correlation with the characteristics of the primary tumor. AJR Am J Roentgenol. 2011;196(1):117–122. doi:10.2214/AJR.10.5036
8. Husband JE, Reznek RH. An overview of imaging in oncology. In: Husband JE, Reznek RH, editors. Imaging in Oncology. London: Taylor & Francis; 2004:1–12.
9. Ling XY, Kevric J, DuGuesclin A, Teague J, Perera M, Penington E. Metastatic urothelial carcinoma presenting as acute cholecystitis. Urol Ann. 2019;11(3):331–333. doi:10.4103/UA.UA_144_18
10. Hong SP, Park SW, Lee SJ, et al. Bile duct wall metastasis from micropapillary variant urothelial carcinoma of the urinary bladder mimicking primary hilar cholangiocarcinoma. Gastrointest Endosc. 2002;56(5):756–758. doi:10.1016/S0016-5107(02)70135-1
11. Fakhoury J, Braha J. Metastatic transitional cell carcinoma masquerading as cholangiocarcinoma. Am J Gastroenterol. 2014;109(Suppl 2):S313. doi:10.14309/00000434-201410002-01052
12. Mirilas P, Skandalakis JE. Surgical anatomy of the retroperitoneal spaces, part III: retroperitoneal blood vessels and lymphatics. Am Surg. 2010;76(2):139–144. doi:10.1177/000313481007600203
13. Morine Y, Shimada M. The value of systematic lymph node dissection for intrahepatic cholangiocarcinoma from the viewpoint of liver lymphatics. J Gastroenterol. 2015;50(9):913–927. doi:10.1007/s00535-015-1071-2
14. Piyawong W, Lekhavat V. Normal measurement of diameters of the common bile ducts in different aged groups. J Med Assoc Thai. 2016;99(Suppl 4):S153–8.
15. Beyer G, Kasprowicz F, Hannemann A, et al. Definition of age-dependent reference values for the diameter of the common bile duct and pancreatic duct on MRCP: a population-based, cross-sectional cohort study. Gut. 2023;72(9):1738–1744. doi:10.1136/gutjnl-2021-326106
16. Wu CC, Ho YH, Chen CY. Effect of aging on common bile duct diameter: a real-time ultrasonographic study. J Clin Ultrasound. 1984;12(8):473–478. doi:10.1002/jcu.1870120804
17. Kasemassawachanont A, Chuangsuwanich N, Lertpipopmetha W, et al. Correlation between axial and coronal common bile duct diameters in computed tomography: a retrospective study of 1064 patients. Egypt J Radiol Nucl Med. 2025;56(1):5. doi:10.1186/s43055-025-01421-4
18. Barreto SG, Toouli J. Physiology and pathophysiology of function of sphincter of oddi. In: The Pancreas: An Integrated Textbook of Basic Science, Medicine, and Surgery. Wiley Online Library; 2023:56–64.
19. Le Vee M, Gripon P, Stieger B, Fardel O. Down-regulation of organic anion transporter expression in human hepatocytes exposed to the proinflammatory cytokine interleukin 1β. Drug Metab Dispos. 2008;36(2):217–222. doi:10.1124/dmd.107.016907
20. Kosters A, Karpen SJ. The role of inflammation in cholestasis: clinical and basic aspects. Semin Liver Dis. 2010;30(2):186–194. doi:10.1055/s-0030-1253227
21. Wang D, Sun K, Wang T, et al. Adverse effects and toxicity of immune checkpoint inhibitors for patients with urothelial carcinoma. Front Pharmacol. 2021;12:710943. doi:10.3389/fphar.2021.710943
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.