Back to Journals » Journal of Pain Research » Volume 14
Common and Contrasting Characteristics of the Chronic Soft-Tissue Pain Conditions Fibromyalgia and Lipedema
Authors Angst F, Benz T ![]() , Lehmann S, Sandor P, Wagner S
, Lehmann S, Sandor P, Wagner S
Received 14 April 2021
Accepted for publication 4 August 2021
Published 17 September 2021 Volume 2021:14 Pages 2931—2941
DOI https://doi.org/10.2147/JPR.S315736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Felix Angst,1 Thomas Benz,1,2 Susanne Lehmann,1 Peter Sandor,1 Stephan Wagner3
1Research Department, Rehaklinik Bad Zurzach, Bad Zurzach, Switzerland; 2ZHAW Zurich University of Applied Sciences, School of Health Professions, Institute of Physiotherapy, Winterthur, Switzerland; 3Department of Angiology, Rehaklinik Bad Zurzach, Bad Zurzach, Switzerland
Correspondence: Felix Angst
Rehaklinik Bad Zurzach, Zurzach Care Group, Quellenstrasse 34, Bad Zurzach, 5330, Switzerland
Tel +41 56 269 51 51
Fax +41 56 269 51 70
Email [email protected]; [email protected]
Objective: To examine the common and specific characteristics of fibromyalgia and lipedema, two chronic soft-tissue pain syndromes without curative therapy options.
Methods: Diseases’ characteristics were compared using the findings of extensive literature and the empiric data from two cohorts, both fulfilling standardized diagnostic criteria. Outcome was measured by various socio-demographics, the generic Short Form 36 (SF-36), the Fibromyalgia Severity Questionnaire (FSQ), and the 6-minute walk distance (6MWD). Empiric SF-36 data were compared to specific population-based norms and between the diagnostic groups, using standardized mean differences (SMD).
Results: Female participants with fibromyalgia (n = 77) and lipedema (n = 112) showed comparable education levels and living situations. Lipedema cases were, on average, 3.9 years younger and BMI 6.3kg/m2 more obese. Women with fibromyalgia smoked more, did less sport, had more comorbidities, and worked less. Compared to the norms, health in fibromyalgia was worse than expected by SMD = – 1.60 to – 2.35 and in lipedema by – 0.44 to – 0.82 on the SF-36. The score differences between the two conditions ranged from SMD = – 0.96 to – 1.34 (all p < 0.001) on the SF-36 and the FSQ. For the inpatients (n = 77 fibromyalgia, n = 38 lipedema), the 6MWD was comparable (SMD = – 0.09, p = 0.640). These findings were consistent with detailed data from the literature reviewed.
Discussion: Fibromyalgia and lipedema share characteristics of clinical phenomenology and comorbid conditions. Disease perception is more pronounced in fibromyalgia than in lipedema, especially in social and role dysfunction, whereas the walking distance was similar for both syndromes. This difference may be explicable by limited coping skills in fibromyalgia.
Keywords: fibromyalgia, lipedema, diagnosis, outcome measures, SF-36
Introduction
Chronic pain localized in soft tissue presents challenges for diagnosis and management. Subsumed under “other musculoskeletal” diseases, chronic soft tissue pain ranked eighth after lumbar and neck pain and migraine in the global burden of diseases, quantified by years lived with disability.1 With an estimated mean point prevalence of 2.7% in the general population worldwide (range 0.4% to 9.3%), fibromyalgia emerges as one of the most important differential diagnoses for chronic soft tissue pain in clinical practice.2
The prevalence of lipedema is unclear because precisely quantified survey data are lacking.3 Estimates vary widely between 0.1% and 9.7%.3,4 Distinguishing lipedema from other chronic pain disorders is essential because it is responsive to complex decongestive therapy, in contrast to other chronic soft tissue pain conditions, such as fibromyalgia, which are often difficult to treat.3–5 While the diagnosis of lipedema is relatively obvious in stages II and III (see below), differentiation from other soft tissue pain syndromes may be difficult in stage I, where the skin surface is even and subcutaneous fat structure normal.3,4
Both fibromyalgia and lipedema are characterized by pain localized in soft tissue; they are found mainly in women in middle-age, who are often co-affected by overweight and symptoms of depression.6,7 Both diseases are chronic, persist over decades and are not curatively treatable, which contributes to a high individual and public health burden. No examiner-based or “objective” signs, such as abnormal laboratory or imaging findings, can be identified to specify one condition from the other.4,8 The two syndromes may often be confused or misdiagnosed. To date and to the best of our knowledge, there is no literature dealing with the differential diagnosis between the two conditions.
The aim of the study was to characterize and compare fibromyalgia and lipedema using the diagnostic criteria, clinical characteristics and data obtained from literature research, and the comprehensive health-related quality of life profiles of two empiric cohorts using cross-sectional comparison. The hypothesis was that there is a substantial overlap in the phenomenological expression of the two syndromes.
Methods
Case Definition/Diagnostic Criteria
The definition of fibromyalgia has an unsettled history. The American College of Rheumatology (ACR) diagnostic criteria of fibromyalgia syndrome have been comprehensively debated and undergone several revisions in the past 30 years.9–11 While palpatoric examination of so-called “tender points” (≥11 of 18 had to be positive) was crucial for diagnosis for two decades (1990–2010), the current criteria dating from 2016, the latest in a succession of revisions, are based on two self-administered anamnestic scores, the Widespread Pain Index (WPI) and the Symptom Severity Score (SSS), together subsumed in the Fibromyalgia Survey Questionnaire (FSQ).9–11 The WPI counts the number of painful body parts from 0 to 19. The SSS ranges from 0 to 12 and is the sum of 3 dimensional items scaled 0=absent, 1=mild, 2=moderate, 3=severe/always and referring to: Daily fatigue, waking unrefreshed, cognitive symptoms plus 3 binary yes/no items regarding the presence (=1)/absence (=0) of headache, pain and cramps in the lower abdomen, and depression. The diagnosis of fibromyalgia requires chronic pain (≥3 months) in 4 of 5 body regions (the 4 quadrants and the spine, assessed by the WPI) together with either (WPI≥7 and SSS≥5) or (WPI 4–6 and SSS≥9).11
Lipedema is characterized by abnormal, disproportional but symmetric deposition of subcutaneous fat in the extremities, leading to a disproportionate, hyper-convex enlargement of the legs, and, rarely, also the arms.3,4 Feet and hands are always spared, leading to the “cuff” sign – in contrast to lymphedema. Subcutaneous edema, although a component of the name of the disease and present in many cases, is also frequently absent, especially in non-obese women, and is not a necessary condition for diagnosis. Lipedema is always associated with daily spontaneous pain and allodynia, which are mandatory for a diagnosis. Pain severity ranges from disturbing heavy legs, pain on contact to permanent and disabling pain.3,4,12–14 Lipedema almost exclusively affects women and is probably due to hormonal factors (estrogen) and/or a genetic predisposition. It is not necessarily linked to obesity, but it may be induced and further aggravated by weight gain, and obesity is a frequent comorbidity. Most histological and etio-patho-physiological factors of the condition remain unknown. Diagnosis is based solely on anamnesis and clinical signs.4,12,13 To date, no technical or objective, examiner-based tests have been established to confirm the diagnosis. The stages of lipedema, which are based on morphology and not on pain levels, are:3,4,13
Stage I: Skin surface even, subcutis thickened, subcutaneous fat structure normal.
Stage II: Skin surface uneven, subcutaneous fat structure with rough texture.
Stage III: Tissue hardened with deforming fat lobe; secondary lymphedema possible.
Patient Sampling
The fibromyalgia patients were consecutively referred by their family physician, internist or rheumatologist to the Zurzach Interdisciplinary Pain (Schmerz) Program (ZISP) for standardized, inpatient, multidisciplinary rehabilitation.5,15 The program consists of a range of active physical therapies, education and coping instructions, psychotherapy, and various complementary therapies.5,15
The lipedema patients were consecutively referred by their family physician, internist or angiologist to the angiology department of the Rehaklinik Bad Zurzach, Bad Zurzach, Switzerland for outpatient consultation leading to a decision either to pursue outpatient management or to begin inpatient treatment.14 For the outpatients, the examination aimed to establish a plan for the management of their condition by the local angiologist, family doctor, and relevant therapists outside our clinic. Inpatient treatment comprised intensive complex decongestive lymphatic therapy and comprehensive rehabilitation, mainly through aquatic and land-based physiotherapy.
The inclusion criteria for the study were a confirmed diagnosis of 1) fibromyalgia according to the ACR criteria of 2016 or 2) lipedema stage I–III diagnosed by the head of the angiology department (SW) according to the diagnostic criteria in the S1 guidelines of the German Society of Phlebology (DGP).4,11 The German S1 guidelines are in line with the UK Best Practice Guidelines and the Dutch guidelines and apply the same diagnostic criteria.16,17 Thus, both diagnoses were standardized and necessary for inclusion in one of the cohorts, irrespective of the earlier admission diagnosis of the family physician, internist, rheumatologist or angiologist. Furthermore, for inclusion in the fibromyalgia cohort, the ACR 2016 criteria were measured on the FSQ and assessed as fulfilled or not by means of the SPSS statistical software (see below). A patient diagnosed with lipedema retained the diagnosis, despite a possible diagnosis of fibromyalgia based on the FSQ; in that case, (secondary) fibromyalgia was taken as a comorbidity. Women with predominant generalized pain and unclear signs of lipedema, however, were not classified as lipedema cases. Since lymphedema may co-occur in stage III of lipedema, persons with lipolymphedema were also included in the lipedema (leading diagnosis) cohort. Lymphedema extends to the foot, whereas lipedema does not (cuff sign). The Stemmer sign is mostly positive in lymphedema but is always negative in lipedema (stage I–III).4
Exclusion criteria were:4,11,14 1) Fibromyalgia: Chronic pain (predominately back pain or widespread pain) not fulfilling the ACR 2016 criteria. 2) Lipedema: Other type of edema with predominantly non-lipedema component (such as lymphedema, edema due to venous, heart or renal insufficiency, etc.). 3) Lipedema: A body mass index (BMI)>50.0 reflecting severe obesity, which, unlike lipedema alone, has a major impact on health. 4) Both disorders: Assessment impossible due to the patient’s insufficient knowledge of the German language, insufficient psycho-intellectual abilities, or severe somatic illness.
The study was approved by the ethics committee of Aarau, Canton Aargau, Switzerland (EK AG 2008/026) and written informed consent was obtained from all study participants.
Literature Search
The literature on fibromyalgia and lipedema was searched focusing on the specific clinical descriptions of the two disorders. The keyword search included the disorder (fibromyalgia or lipedema) and the clinical characteristics. Predefined inclusion and exclusion criteria were not applied and no specific published guideline for systematic reviews was followed. Data describing the clinical characteristics most precisely were selected and included in this paper.
Measures
Sociodemographic and disease-relevant data were recorded using a standardized questionnaire that has proved its worth in several previous studies.18 All necessary medical records were obtained to enable confirmation of the diagnosis, evaluation of the inclusion and exclusion criteria, and the comorbid conditions.
The Short Form 36 (SF-36) is the most widely used questionnaire globally for the self-assessment of generic health and quality of life by 8 scales and 2 summary scales.19–21 It is not condition-specific and enables comparison of comprehensively measured health in people with different diagnoses as well as in the healthy. We used the validated German translation of the revised version 2.20,21 From a representative German general population survey normative values can be retrieved, which are stratified by sex, age (5-year classes), and the presence or absence of comorbid conditions.22
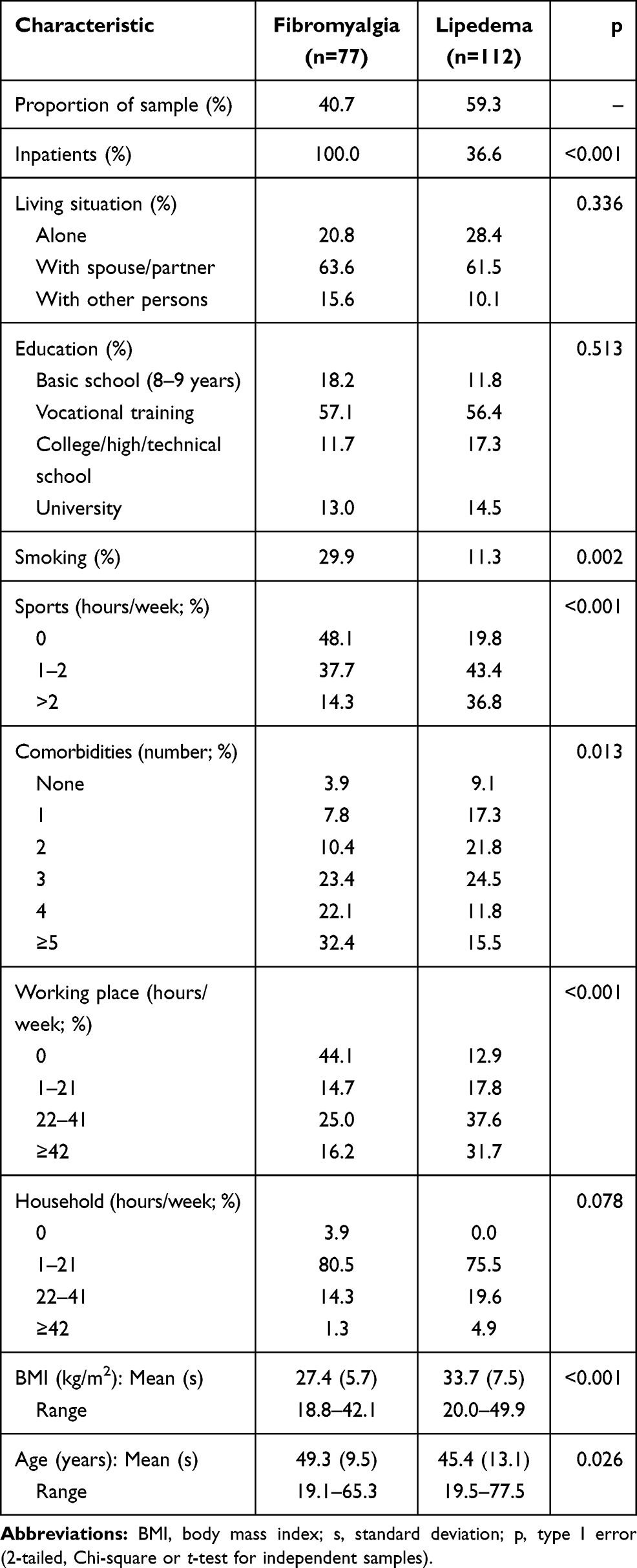 |
Table 1 Socio-Demographic and Disease-Relevant Data (n=189) |
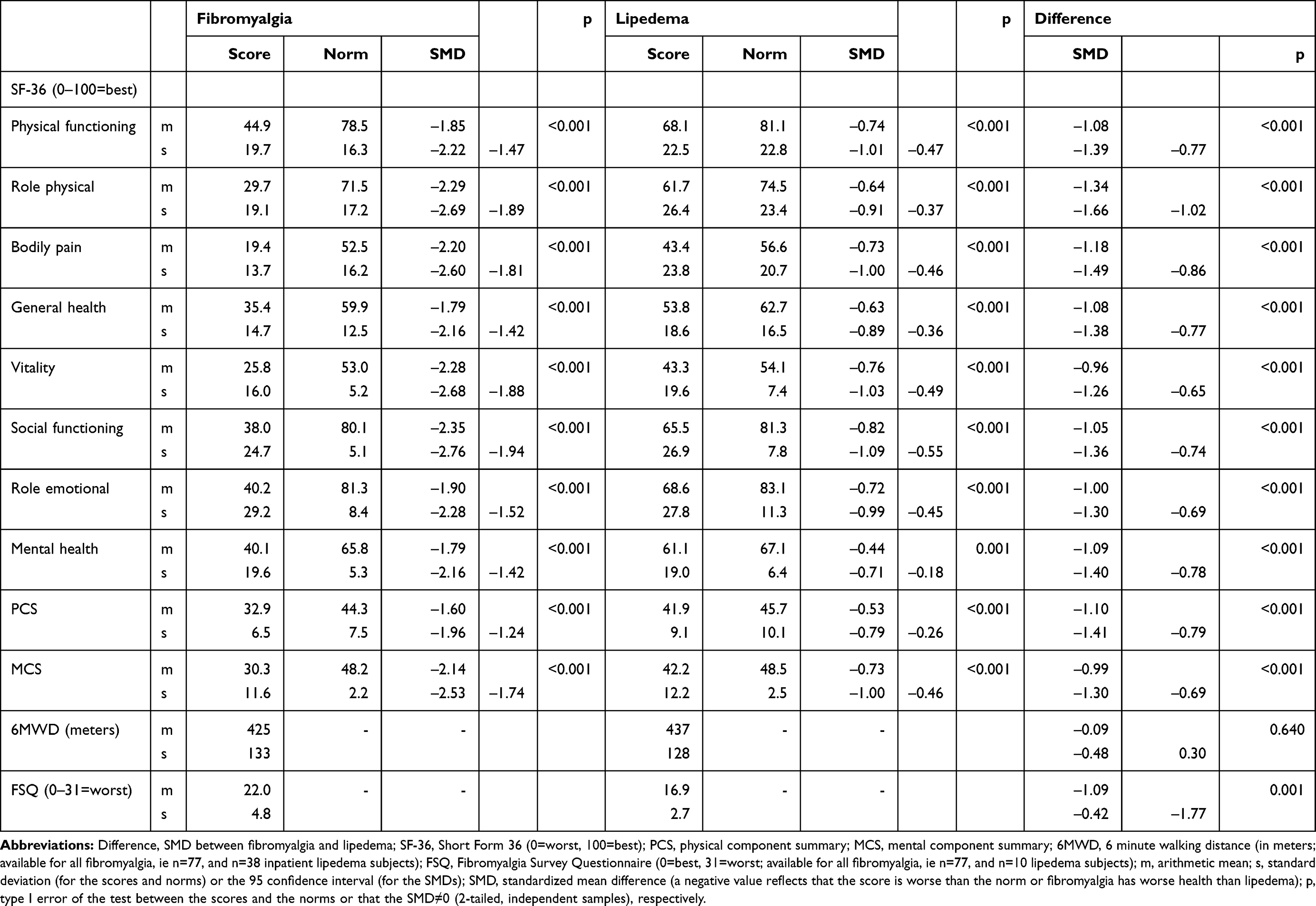 |
Table 2 Score Data of Fibromyalgia (n=77) and Lipedema (n=112) |
As an examiner-based measure of functional capacity, the 6-minute Walking Distance (6MWD) test was applied, one of the most frequently used, best validated, and responsive functional performance tests.23–25 Due to practical reasons and the time constraints on ambulatory consultations, the 6MWD was performed only by inpatients (all fibromyalgia and a subgroup of lipedema).
The FSQ score is the sum of the WPI (0 to 19 painful locations) and the SSS (0 to 12=most symptoms) resulting in a score ranging from 0=no symptoms to 31=maximum symptoms of fibromyalgia.11 Administration/Reporting of the FSQ is recommended to quantify the disease severity.11 A score <12 excludes the diagnosis of fibromyalgia. The FSQ was administered to a subgroup of lipedema in order to examine diagnostic overlap.
Analysis
The cross-sectional measurement took place on admission to the multidisciplinary rehabilitation program, ie, before therapy. While all those with fibromyalgia received inpatient treatment, a large number of the women with lipedema examined were referred for a consultation to the specialist (angiologist: S.W.) for further outpatient management at home. Since lipedema occurs only in females, women from the fibromyalgia cohort were also selected for analysis in order to match comparison by gender.
For the SF-36, more than 50% of the items had to be completed to determine a specific scale, which defines the original “missing rule”.20,21 The SF-36 original scaling is from 0=worst health, maximum symptoms/disability to 100=best health, no symptoms, full function. This means that 0 reflects maximum and 100 no pain. The walking distance of the 6MWD was quantified in meters.
The SF-36 and 6MWD score differences were quantified by standardized mean differences (SMD), as used in our earlier comparison of lipedema and lymphedema.14 This method was applied in both the comparison of fibromyalgia with lipedema and the comparison within each of the conditions with the corresponding SF-36 normative scores. The SMD is the difference between two scores divided by their pooled standard deviation, which equals the square root of the weighted mean of the two variances, where the weights are the sample sizes of the two groups.26 Exclusion of zero by the 95% confidence intervals (95% CI) of the SMD implies that the difference is statistically significant. The corresponding type I error p is the same as that obtained by the t-test. All analyses were performed using the statistical software package IBM SPSS 25.0 for Windows® (SPSS Inc., Chicago, IL, USA).
In determining sample sizes, the differences were compared to minimal clinically important differences (MCID).14,26 The level of SMD=0.30 constitutes the lower limit of the range 0.30–0.50 currently considered to indicate MCIDs.27 In order to reach statistical significance for an SMD=0.30, the total sample should be n≥174 (minimal degrees of freedom=174–2=172), ideally equally distributed, ie, n≥87 for each group.26,27 In other words, above that level, differences become subjectively perceptible on the group level. Moreover, exponentially increasing sample sizes would be needed for significance of smaller differences: n≥124 for each group for an SMD=0.25, for example.26
Results
Socio-Demographic and Disease-Relevant Data (Table 1)
All fibromyalgia participants (n=77) and 36.6% of those with lipedema (n=112) were admitted to inpatient treatment. Compared to the lipedema participants, those with fibromyalgia were on average and statistically significantly (p < 0.001) older by 3.9 years, less likely to be obese (BMI 6.3 kg/m2 lower), more frequently smokers, did less sport, were more affected by comorbidities (median 4 versus 2) and worked fewer hours in the work place. Obesity (BMI ≥30.0 kg/m2) was prevalent in 88.4% of the lipedema group but just 33.3% of the fibromyalgia participants (p < 0.001). In their living situations (alone or with spouse/partner), education levels, and hours spent working in the household the two cohorts were statistically comparable.
Outcome Data and Comparison to the Norm (Table 2)
Women with fibromyalgia reported, on average, very poor levels of health and quality of life on the SF-36 (Table 2). On the possible scale of 0=worst to 100=best health, all scores were far below the median of 50, ranging from a mean score of 44.9 for Physical function, and 40.1 for Mental health down to 19.4 for Bodily pain. The comparative levels for lipedema were 68.1, 61.1, and 43.4. Lipedema participants reported most symptoms on Vitality (mean 43.3) and least impairment in Role emotional (68.8).
Compared to the individually matched normative values from the general population, the SF-36 score levels of those with fibromyalgia were statistically significantly (all p < 0.001) far worse than expected, with SMDs ranging from –1.79 for SF-36 General and Mental health, to –2.20 for Bodily pain down to –2.35 for Social functioning. Those differences were much less marked but still statistically significant (all p≤0.001) in lipedema, ranging from –0.44 for SF-36 Mental health and –0.73 for Bodily pain to –0.82 for Social functioning.
Outcome of the Comparison Between Fibromyalgia and Lipedema (Table 2)
Fibromyalgia participants reported far worse health and quality of life on all scales of the SF-36, with scores ranging from mean score point difference=–17.6/SMD=–0.96 on SF-36 Vitality, to –24.0/–1.18 on Bodily pain down to –31.9/–1.34 on Role physical (all p < 0.001) with an overall differential of around one pooled standard deviation on the all-inclusive the summary scores. The same was true on the FSQ (–5.1/SMD=–1.09).
In contrast, the results on the 6MWD were almost equal for the two disorders, with a mean of 425 meters for fibromyalgia (n=77) and 437 meters for lipedema (n=38 inpatients with lipedema), SMD=–0.09 (p=0.640). Although those n=38 lipedema inpatients reported worse health when compared to the whole lipedema group, their scores revealed that they were nonetheless in better health than those with fibromyalgia (results not shown in Table 2): SF-36 Physical functioning, mean of the inpatient lipedema subgroup 56.5, standard deviation 23.7, SMD to fibromyalgia –0.54 (95%-CI: –0.92, –0.16), p=0.004. The corresponding data for SF-36 Role physical were: 48.2, 24.9, SMD=–0.86 (–1.25, –0.47), p < 0.001. SF-36 Bodily pain: 33.0, 22.2, SMD=–0.79 (–1.18, –0.40), p < 0.001. SF-36 Mental health: 61.0 (the same as for all n=112 with lipedema), 22.7, SMD=–1.00 (–1.40, –0.61), p < 0.001.
Comparison of Fibromyalgia and Lipedema with the Findings of the Literature Review (Table 3)
The literature review findings regarding the clinical characteristics and outcome data of the two disorders were combined with the main results of the empiric cohort data and are presented together in Table 3. The aim of this approach is to provide a concise overview of the common and the specific characteristics of fibromyalgia and lipedema instead of extensive descriptions in the discussion, which would blow up the text and unable to handle. None of the studies reviewed compared the two conditions at the same time as ours did. To illustrate the disease-associated severity of pain, disability, depression, etc., the scaling of the empiric data from the two cohorts (Table 2) from 0=worst to 100=best was converted to the common numeric rating scale (NRS) for severity where 0=best and 10=worst, since this was the scaling often used in the literature.
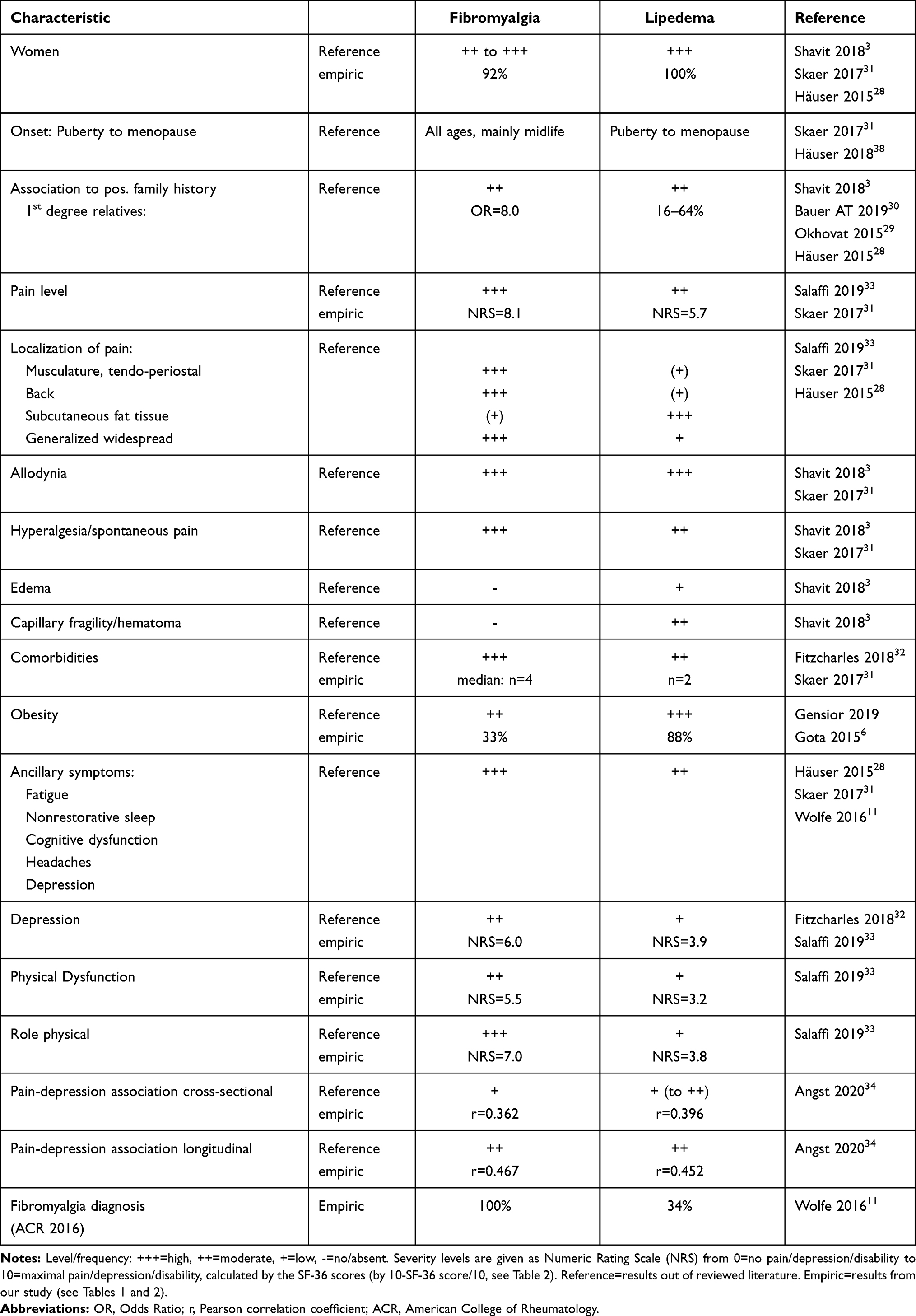 |
Table 3 Summary of Characteristics of Fibromyalgia and Lipedema |
Discussion
Our cross-sectional outcome study compared fibromyalgia and lipedema using descriptive potentially disease-relevant data and standardized measures, namely the SF-36, the 6MWD, and the FSQ, together with clinical and outcome data from the literature. The hypothesis of a substantial syndromal overlap between the conditions was confirmed, with implications for both diagnostics and disease management.
Both these chronic pain syndromes mainly affect women during their reproductive life span and are characterized by diffuse, spontaneous, widespread soft-tissue pain and allodynia. A hereditary risk was reported for both conditions (Table 3).3,28–30 Both diseases show relatively high comorbidity rates, especially associations with depression, fatigue, headache and functional, vegetative symptoms, but also with obesity.6,11,28,31–33 Significantly more symptoms and lower function levels than expected from the general population norms were observed in our cohorts. Compared to the population-based normative values, participants with fibromyalgia reported worse health by around 2 pooled standard deviations, and those with lipedema by 2/3 pooled standard deviations of the SMDs on all SF-36 scales. In both conditions, the greatest distance from the norms was on the SF-36 Social functioning and the smallest on the SF-36 Mental health. More than one-third of the women with lipedema also fulfilled the ACR 2016 diagnostic criteria for fibromyalgia. In addition, the associations between pain and depression were very similar in both the cross-sectional and the longitudinal assessments of the two disorders.34 Furthermore, our fibromyalgia and lipedema patients reported comparable living situations and education levels, both of which are important predictors of ability to work.35
Nevertheless, the women with fibromyalgia worked less than those with lipedema, especially at the work place and somewhat in the household. Regarding the two modifiable health determinants assessed, sport and smoking, more harmful health behavior was found in the fibromyalgia than in the lipedema group. The third partially modifiable factor, obesity, was much more in prevalent lipedema, but the total number of comorbidities was far higher in fibromyalgia. Physical and mental health and quality of life were much poorer in fibromyalgia than in lipedema on all SF-36 dimensions and on the FSQ by an average SMD of one pooled standard deviation. The greatest difference between the conditions was in SF-36 Role physical.
The latter finding is in line with the study of Salaffi.33 In patients with fibromyalgia SF-36 Role physical was the most severely affected health dimension. Among different musculoskeletal disorders, the largest differences were between fibromyalgia and low back pain and shoulder pain across all SF-36 scales. This is in line with lower SF-36 scores in fibromyalgia when compared to various other pain conditions, such as osteoarthritis of hip and knee, whiplash associated disorders, rheumatoid arthritis and other musculoskeletal disorders.36 Fibromyalgia participants also experienced much higher pain levels (SMD=–1.18) and more pain localizations (FSQ results) than those with lipedema (Table 3). In lipedema, pain is distinctively localized in subcutaneous fat tissue in the edema-affected limbs. For patients with fibromyalgia, pain is experienced in different types of tissue, is more diffuse and is distributed throughout the body, including the back.11
Although the levels of pain and other signs and symptoms are, on average, worse in fibromyalgia than in lipedema, an overlap between disorders in single cases is possible. The distances measured by the 6MWD were comparable. Compared to the performance on the examiner-based 6MWD (mean distance difference=–12 meters, SMD=–0.09, p=0.640), results on the SF-36 Physical functioning were much worse self-rated in the fibromyalgia group than in the inpatient lipedema group (mean score difference=–23.2 points, SMD=–0.54, p=0.004). Five of the ten (50%) items of the SF-36 Physical functioning scale address walking performance. This leads to the hypothesis that the mismatch between subjective and “objective” ratings may also be observed in other health dimensions, such as pain, social function, vitality, and depression (SF-36 Mental health), where persons with fibromyalgia judge themselves sicker than expected, a phenomenon consistently reported in the literature.15,37,38 This phenomenon might point to a relatively unrealistic, pessimistic self-assessment of physical function in fibromyalgia. The discordance between the subjective and objective assessments of physical function was shown to be associated with catastrophizing, which is highly prevalent in fibromyalgia.37 This is consistent with the typical clinical observation of a discrepancy in fibromyalgia patients between subjectively pronounced impairment and only mildly abnormal signs in physical examination. This may originate in the complex mechanisms of pain centralization and activation of the hypothalamic-pituitary-adrenal axis with sympathetic overactivity.38 For lipedema, comparable research and findings are lacking.
Despite pain and esthetic problems, younger women with lipedema are assessed as having relatively high functionality on the SF-36 Role physical, ie, only SMD=–0.69 lower than the norm compared to fibromyalgia (SMD=–2.29). It can be hypothesized that people with lipedema perceive themselves as having higher self-competence and self-efficacy in coping with their disease because of the strict adherence and self-discipline demanded by regular complex decongestive therapy. This hypothesis is supported by a comparison of lipedema and lymphedema patients, where the two groups had almost the same scores on the SF-36 Role physical, SF-36 Role emotional, and the Freiburg Lymphedema Quality-of-Life Everyday life (performance) scale, whereas on all other health dimensions, especially pain and physical function, lipedema patients scored statistically significantly worse.34 Cross-sectional social flexibility and social connectedness were found to be consistently and significantly positively associated with health and quality of life in lipedema.39
A strength of our study is that it is the first comparing the chronic soft pain conditions fibromyalgia and lipedema by empiric data measured by standardized outcome instruments. Both cohorts were strictly defined according to standardized diagnostic criteria. Data from a comprehensive and valid assessment of health and quality of life involving more than n=100 patients with lipedema are new in the scientific literature. The standardized self-assessment by the SF-36 was supplemented by a functional performance test, the 6MWD. The SF-36 scores reported were compared to sex-, age-, and presence of comorbidities-specific population norms. All differences were standardized by SMDs for ease of comparison across different health dimensions and diagnostic groups. An extensive literature research was performed to characterize and compare both syndromes. None of the studies reviewed compared the two conditions at the same time.
As a limitation, self-assessment included only the SF-36 and not other dimensions of chronic pain, such as pain coping, specific affective health dimensions, or further functional performance tests. However, depression was measured by the SF-36 Mental health scale, which has high content and construct validity for depression, as extensively demonstrated in our earlier study.34 While the lipedema cohort was large, that of fibromyalgia was relatively small. Only part of the lipedema cohort was examined using the 2016 ACR fibromyalgia criteria and only the inpatient participants with lipedema performed the 6MWD test. Moreover, the patients with fibromyalgia were not systematically evaluated for comorbid lipedema, due to the different clinical settings in the hospital of the two conditions.
Conclusions
Fibromyalgia and lipedema are two widespread, chronic soft-tissue pain conditions that are very similar in their localization, pain characteristics, gender distribution, clinical phenomenology, comorbid conditions, and absence of curative therapy options. The two conditions are distinct entities. The main distinguishing feature is that persons with lipedema report localized pain (in the legs most often) and show a disproportional subcutaneous fat pattern, whereas those with fibromyalgia report generalized pain (in at least 4/5 body regions, with almost all having back pain, see ACR criteria). The concomitant symptoms are often the same and reflect the chronic pain syndrome. Distinguishing fibromyalgia from stage I lipedema or other differential diagnostic conditions can be challenging but is essential for correct therapy allocation. The patient’s perception of disease severity is stronger in fibromyalgia than in lipedema, especially in the social and role dysfunction dimensions, whereas the walking distance was similar for both conditions. These observed inconsistent findings and parallel results in the literature suggest that the self-assessment of disease severity is more pessimistic and possibly unrealistically negative in fibromyalgia when compared to disorders, possibly due to limitations in the individual’s pain coping skills. Future research should include pain coping dimensions and additional functional performance tests.
Data Sharing Statement
All data and material are freely available. Please contact the corresponding author to request data.
Ethics Approval and Consent to Participate and for Publication
The study was approved by the ethics committee of Aarau, Canton Aargau, Switzerland (EK AG 2008/026) and written informed consent was obtained from all study participants. The study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable. The data do not contain any personal data.
Acknowledgments
This study was supported by the Zurzach Rehabilitation Foundation SPA, Bad Zurzach, Switzerland. We thank all patients for their voluntary participation in the study. We further thank Elizabeth Kyrke for the linguistic editing of the text.
Funding
There are no sources of funding to declare.
Disclosure
Dr Stephan Wagner reports personal fees from Essity Switzerland, personal fees from Sigvaris Switzerland, personal fees from Berro Switzerland/Juzo Germany, outside the submitted work.
There are no conflicts of interests or competing interests to declare.
References
1. GBD 2016 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Lond Engl. 2017;390(10100):1260–1344. doi:10.1016/S0140-6736(17)32130-X.
2. Queiroz LP. Worldwide epidemiology of fibromyalgia. Curr Pain Headache Rep. 2013;17(8):356. doi:10.1007/s11916-013-0356-5
3. Shavit E, Wollina U, Alavi A. Lipoedema is not lymphoedema: a review of current literature. Int Wound J. 2018;15(6):921–928. doi:10.1111/iwj.12949
4. Reich-Schupke S, Schmeller W, Brauer WJ, et al. S1 guidelines: lipedema. J Dtsch Dermatol Ges J Ger Soc Dermatol JDDG. 2017;15(7):758–767. doi:10.1111/ddg.13036
5. Angst F, Verra M, Lehmann S, Brioschi R, Aeschlimann A. Clinical effectiveness of an interdisciplinary pain management programme compared with standard inpatient rehabilitation in chronic pain: a naturalistic, prospective controlled cohort study. J Rehabil Med. 2009;41(7):569–575. doi:10.2340/16501977-0381
6. Gota CE, Kaouk S, Wilke WS. Fibromyalgia and obesity: the association between body mass index and disability, depression, history of abuse, medications, and comorbidities. J Clin Rheumatol Pract Rep Rheum Musculoskelet Dis. 2015;21(6):289–295. doi:10.1097/RHU.0000000000000278
7. Gensior MHL, Cornely M. [Pain in lipoedema, fat in lipoedema and its consequences: results of a patient survey based on a pain questionnaire]. Handchir Mikrochir Plast Chir. 2019;51(4):249–254. doi:10.1055/a-0942-9607. German
8. Bennett RM, Schein J, Kosinski MR, Hewitt DJ, Jordan DM, Rosenthal NR. Impact of fibromyalgia pain on health-related quality of life before and after treatment with tramadol/acetaminophen. Arthritis Rheum. 2005;53(4):519–527. doi:10.1002/art.21319
9. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the multicenter criteria committee. Arthritis Rheum. 1990;33(2):160–172. doi:10.1002/art.1780330203
10. Wolfe F, Clauw DJ, Fitzcharles M-A, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010;62(5):600–610. doi:10.1002/acr.20140
11. Wolfe F, Clauw DJ, Fitzcharles M-A, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319–329. doi:10.1016/j.semarthrit.2016.08.012
12. Halk AB, Damstra RJ. First Dutch guidelines on lipedema using the international classification of functioning, disability and health. Phlebology. 2017;32(3):152–159. doi:10.1177/0268355516639421
13. Wollina U, Heinig B. Differential diagnostics of lipedema and lymphedema: a practical guideline. Z Rheumatol. 2018;77(9):799–807. doi:10.1007/s00393-018-0546-y
14. Angst F, Lehmann S, Aeschlimann A, Sandòr PS, Wagner S. Cross-sectional validity and specificity of comprehensive measurement in lymphedema and lipedema of the lower extremity: a comparison of five outcome instruments. Health Qual Life Outcomes. 2020;18(1):245. doi:10.1186/s12955-020-01488-9
15. Angst F, Brioschi R, Main CJ, Lehmann S, Aeschlimann A. Interdisciplinary rehabilitation in fibromyalgia and chronic back pain: a prospective outcome study. J Pain. 2006;7(11):807–815. doi:10.1016/j.jpain.2006.03.009
16. Dutch Society for Dermatology and Venereology (NDVD). Dutch lipoedema guideline; 2014. Available from: https://diseasetheycallfat.tv/wp-content/uploads/2015/08/Dutch-lipoedemaguideline-2014.pdf.
17. Wounds UK. Best Practice Guidelines: The Management of Lipoedema. London: Wounds UK, 2017. Available from: https://www.guidelines.co.uk/skin-and-wound-care/wounds-uk-lipoedema-guideline/453516.article. Accessed August 31, 2021
18. Angst F, Aeschlimann A, Steiner W, Stucki G. Responsiveness of the WOMAC osteoarthritis index as compared with the SF-36 in patients with osteoarthritis of the legs undergoing a comprehensive rehabilitation intervention. Ann Rheum Dis. 2001;60(9):834–840.
19. Busija L, Pausenberger E, Haines TP, Haymes S, Buchbinder R, Osborne RH. Adult measures of general health and health-related quality of life: medical Outcomes Study Short Form 36-Item (SF-36) and Short Form 12-Item (SF-12) Health Surveys, Nottingham Health Profile (NHP), Sickness Impact Profile (SIP), Medical Outcomes Study Short Form 6D (SF-6D), Health Utilities Index Mark 3 (HUI3), Quality of Well-Being Scale (QWB), and Assessment of Quality of Life (AQoL). Arthritis Care Res. 2011;63 Suppl 11:S383–S412. doi:10.1002/acr.20541
20. Bullinger M, Kirchberger I. Fragebogen zum Gesundheitszustand: SF-36; Handanweisung [The SF-36 questionnaire to assess health status. A manual]. Hogrefe: Verlag für Psychologie; 1998.
21. Ware JE, Snow KK, Kosinski M, Gandek B; New England Medical Center Hospital, Health Institute. SF-36 Health Survey: Manual and Interpretation Guide.
22. Kurth B-M, Ellert U. The SF-36 questionnaire and its usefulness in population studies: results of the German health interview and examination survey 1998. Soz Praventivmed. 2002;47(4):266–277. doi:10.1007/BF01326408
23. Bennell K, Dobson F, Hinman R. Measures of physical performance assessments: self-Paced Walk Test (SPWT), Stair Climb Test (SCT), Six-Minute Walk Test (6MWT), Chair Stand Test (CST), Timed Up & Go (TUG), Sock Test, Lift and Carry Test (LCT), and Car Task. Arthritis Care Res. 2011;63 Suppl 11:S350–S370. doi:10.1002/acr.20538
24. Butland RJ, Pang J, Gross ER, Woodcock AA, Geddes DM. Two-, six-, and 12-minute walking tests in respiratory disease. Br Med J Clin Res Ed. 1982;284(6329):1607–1608. doi:10.1136/bmj.284.6329.1607
25. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102.
26. Borenstein M. Effect sizes for continuous data. In: The Handbook of Research Synthesis and Meta-Analysis.
27. Angst F, Aeschlimann A, Angst J. The minimal clinically important difference raised the significance of outcome effects above the statistical level, with methodological implications for future studies. J Clin Epidemiol. 2017;82:128–136. doi:10.1016/j.jclinepi.2016.11.016
28. Häuser W, Ablin J, Fitzcharles M-A, et al. Fibromyalgia. Nat Rev Dis Primer. 2015;1:15022. doi:10.1038/nrdp.2015.22
29. Okhovat J-P, Alavi A. Lipedema: a review of the literature. Int J Low Extrem Wounds. 2015;14(3):262–267. doi:10.1177/1534734614554284
30. Bauer A-T, von Lukowicz D, Lossagk K, et al. New insights on lipedema: the enigmatic disease of the peripheral fat. Plast Reconstr Surg. 2019;144(6):1475–1484. doi:10.1097/PRS.0000000000006280
31. Skaer TL, Kwong WJ. Illness perceptions and burden of disease in fibromyalgia. Expert Rev Pharmacoecon Outcomes Res. 2017;17(1):9–15. doi:10.1080/14737167.2017.1270207
32. Fitzcharles M-A, Perrot S, Häuser W. Comorbid fibromyalgia: a qualitative review of prevalence and importance. Eur J Pain Lond Engl. 2018;22(9):1565–1576. doi:10.1002/ejp.1252
33. Salaffi F, Di Carlo M, Carotti M, Farah S, Ciapetti A, Gutierrez M. The impact of different rheumatic diseases on health-related quality of life: a comparison with a selected sample of healthy individuals using SF-36 questionnaire, EQ-5D and SF-6D utility values. Acta Bio-Medica. 2019;89(4):541–557. doi:10.23750/abm.v89i4.7298
34. Angst F, Benz T, Lehmann S, et al. Extended overview of the longitudinal pain-depression association: a comparison of six cohorts treated for specific chronic pain conditions. J Affect Disord. 2020;273:508–516. doi:10.1016/j.jad.2020.05.044
35. Clay FJ, Fitzharris M, Kerr E, McClure RJ, Watson WL. The association of social functioning, social relationships and the receipt of compensation with time to return to work following unintentional injuries to Victorian workers. J Occup Rehabil. 2012;22(3):363–375. doi:10.1007/s10926-012-9354-4
36. Hoffman DL, Dukes EM. The health status burden of people with fibromyalgia: a review of studies that assessed health status with the SF-36 or the SF-12. Int J Clin Pract. 2008;62(1):115–126. doi:10.1111/j.1742-1241.2007.01638.x
37. Estévez-López F, Álvarez-gallardo IC, Segura-Jiménez V, et al. The discordance between subjectively and objectively measured physical function in women with fibromyalgia: association with catastrophizing and self-efficacy cognitions. The al-Ándalus project. Disabil Rehabil. 2018;40(3):329–337. doi:10.1080/09638288.2016.1258737
38. Häuser W, Fitzcharles M-A. Facts and myths pertaining to fibromyalgia. Dialogues Clin Neurosci. 2018;20(1):53–62.
39. Dudek JE, Białaszek W, Ostaszewski P. Quality of life in women with lipoedema: a contextual behavioral approach. Qual Life Res Int J Qual Life Asp Treat Care Rehabil. 2016;25(2):401–408. doi:10.1007/s11136-015-1080-x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.