Back to Journals » Infection and Drug Resistance » Volume 19
Combating Antimicrobial Resistance: A Pharmacist-Led PDCA Stewardship Program in a Tertiary Hospital
Authors Li C ![]() , Han B
, Han B ![]() , Lv L
, Lv L ![]() , Jiang H
, Jiang H ![]() , Zhang M, Chen N, Xin C, Ying Y, Yang B
, Zhang M, Chen N, Xin C, Ying Y, Yang B ![]()
Received 27 December 2025
Accepted for publication 3 March 2026
Published 12 March 2026 Volume 2026:19 592120
DOI https://doi.org/10.2147/IDR.S592120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Chengle Li,1 Bing Han,1 Lisong Lv,1 Hong Jiang,1 Mingwan Zhang,1 Nanmei Chen,1 Chuanwei Xin,1 Yin Ying,2,* Bo Yang1,*
1Department of Pharmacy, Tongde Hospital of Zhejiang Province Affiliated to Zhejiang Chinese Medical University, Hangzhou, 310012, People’s Republic of China; 2Editorial Department, Zhejiang Journal of Traditional Chinese Medicine, Zhejiang Academy of Traditional Chinese Medicine, Hangzhou, 310012, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bo Yang, Department of Pharmacy, Tongde Hospital of Zhejiang Province Affiliated to Zhejiang Chinese Medical University, Hangzhou, 310012, People’s Republic of China, Tel +86 571 8997 2240, Fax +86 571 8997 2242, Email [email protected]
Background: Antimicrobial resistance (AMR) is a critical global health threat driven by inappropriate antimicrobial use. Reducing antimicrobial consumption and optimizing prescribing are fundamental goals of Antimicrobial Stewardship Programs (ASPs). This study aimed to implement and evaluate a pharmacist-led, multidimensional ASP based on the Plan-Do-Check-Act (PDCA) cycle to reduce Antibacterial Use Density (AUD) and improve prescribing quality.
Methods: A quasi-experimental study was conducted from October 2023 to September 2024 in a tertiary hospital. Led by a multidisciplinary ASP team and guided by the PDCA cycle, the intervention comprised: 1) an innovative “ 1+X” ward-based clinical pharmacist model to standardize surgical antimicrobial prophylaxis (SAP); 2) promoting precision diagnostics via Therapeutic Drug Monitoring (TDM) and droplet digital PCR (ddPCR); 3) establishing regular multidisciplinary case discussions; and 4) integrating informatics-driven alerts into the prescribing system. Data on AUD, SAP quality, diagnostic utilization, and cost were extracted from the hospital information system and analyzed.
Results: Hospital-wide AUD significantly decreased by 25.06%, from 49.68 to 37.23 DDDs/100 patient-days (p< 0.001). A resource-concentrating strategy led to greater AUD reduction in six high-consumption medical departments than in others (23.26 vs. 5.17 DDDs/100 patient-days, p< 0.05). The “ 1+X” model improved duration rationality for Type I incisions from 50.54% to 78.44% (p< 0.001). TDM utilization increased 7.7-fold, and ddPCR showed rapid clinical adoption. Access antibiotic use increased nearly five-fold. Total antimicrobial cost decreased by 7.8%.
Conclusion: A pharmacist-led, PDCA-based ASP integrating differentiated strategies and precision diagnostics effectively reduced antimicrobial consumption, optimized prescribing structure, improved SAP quality, and generated economic benefits. This model provides a replicable framework for sustainable antimicrobial stewardship in hospitals.
Keywords: antimicrobial stewardship, antibacterial use density, PDCA cycle, clinical pharmacist, precision diagnostics
A Letter to the Editor has been published for this article.
Introduction
The discovery of antibiotics is hailed as one of the greatest medical achievements of the 20th century, transforming once-lethal infections such as pneumonia and sepsis into treatable conditions. However, their widespread and often inappropriate use has led to the growing global public health threat of bacterial antimicrobial resistance.1 According to authoritative estimates, antimicrobial resistance directly caused 1.27 million deaths globally in 2019, and was associated with approximately 4.95 million additional deaths, highlighting a health burden far exceeding prior expectations.2 In this context, promoting the rational use of antimicrobials has become a core task for healthcare institution management.
To scientifically quantify management effectiveness, the World Health Organization recommends the use of Antibacterial Use Density (AUD) as a key evaluation indicator. This metric effectively eliminates variations in drug specifications and dosages, objectively reflecting the frequency of use and exposure level of drugs, and is more accurate and sensitive than the “use rate”.3 Nevertheless, due to multiple constraining factors such as clinical prescribing habits, insufficient support from pathogen diagnostic technologies, and a lack of management refinement, the AUD in many Chinese healthcare institutions remains high, posing a serious challenge to optimizing antimicrobial use structures.4 Compounding these challenges is diagnostic limitations, including the slow turnaround time of conventional microbiology and the lack of rapid molecular tools for pathogen and resistance gene identification, which delay targeted therapy and perpetuate empirical broad-spectrum use.
To address this challenge systematically, this study introduces the “Plan-Do-Check-Act” (PDCA) cycle, a classic quality management tool. Its closed-loop, spiral-upward model provides a proven pathway for continuous improvement in healthcare quality. While the PDCA cycle has been extensively applied in general healthcare quality improvement, its specific application to multidimensional, pharmacist-led antimicrobial stewardship interventions remains underexplored in the literature. Despite the widespread endorsement of ASPs, a critical gap remains in the availability of structured, replicable implementation frameworks that effectively integrate multiple evidence-based strategies into a cohesive and sustainable hospital-wide program. Based on this framework, this study aims to construct and implement a pharmacist-led Antimicrobial Stewardship Program (ASP). Core strategies include: establishing a multidisciplinary ASP team; promoting the application of Therapeutic Drug Monitoring (TDM) and droplet digital polymerase chain reaction (ddPCR) in key clinical departments; creating a standardized intervention mechanism involving “designated clinical pharmacists conducting ward rounds”; and supplementing these with standardized education and an intelligent informatics-based alert system. By evaluating the effect of this comprehensive intervention model on reducing the AUD in inpatients, this study aims to provide practical evidence for the refined management of antimicrobials in hospitals. The specific objectives were to assess the program’s impact on reducing overall and department-specific Antibacterial Use Density (AUD), to evaluate improvements in the quality of surgical antimicrobial prophylaxis (SAP), to monitor the adoption of precision diagnostic tools (TDM and ddPCR), and to analyze structural changes in antimicrobial prescribing patterns according to the WHO AWaRe classification.
Methods
Study Design
This quasi-experimental, action research study was conducted at Tongde Hospital of Zhejiang Province Affiliated to Zhejiang Chinese Medical University, a large tertiary teaching hospital in China. The study implemented a single pharmacist-led PDCA cycle (Figure 1) over a 12-month period (October 2023 to September 2024), with a 6-month pre-intervention baseline phase (October 2023 to March 2024), a 6-month active intervention phase (April 2024 to September 2024), and embedded planning and analysis phases. Antimicrobial consumption data were extracted from the hospital’s upgraded Business Intelligence (BI) system (implemented from September 2023). The baseline AUD calculated from this system differs from a prior publication,4 as discussed in the Limitations.
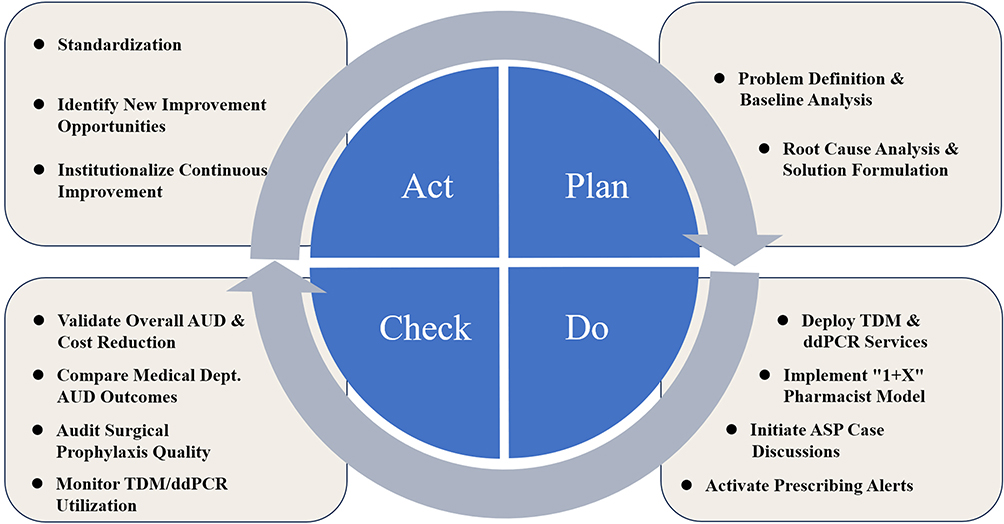 |
Figure 1 Flowchart of the pharmacist-led PDCA cycle for reducing AUD. |
The Ethics Committee of Tongde Hospital of Zhejiang Province waived the requirement for ethics approval and informed consent for this study. This waiver was granted because the research focused solely on the methodological study of management processes and quality improvement, did not involve any patient privacy or identifiable information, and the exemption was not considered to adversely affect the rights or health of the subjects.
Plan
Problem Definition & Baseline Analysis
We retrospectively collected and analyzed data from the pre-intervention baseline period (October 2023 to March 2024) to quantify the problem and establish benchmarks. The primary outcomes for this analysis were the overall Antibacterial Use Density (AUD), expressed in Defined Daily Doses (DDDs) per 100 patient-days, and the cumulative DDDs of antimicrobial agents. This provided a clear, quantitative picture of the antimicrobial consumption landscape before any intervention.
Root Cause Analysis & Solution Formulation
Following the established framework of an Antimicrobial Stewardship Program (ASP), a multidisciplinary ASP team was convened. The team comprised representatives from the Medical Administration Department, the Hospital Infection Control Department, physicians specializing in infectious diseases, clinical pharmacists, microbiologists, and radiologists. The team conducted a systematic root cause analysis using a fishbone diagram (Ishikawa diagram, Figure 2) to identify the underlying factors contributing to the high AUD. Ultimately, based on the consensus regarding the primary root causes, a set of targeted countermeasures was selected and integrated, including: (1) Promoting the application of Therapeutic Drug Monitoring (TDM) and droplet digital polymerase chain reaction (ddPCR) rapid molecular pathogen diagnostics (eg, dPCR) in key clinical departments. (2) Implementing complex case discussions within the ASP framework to guide optimal therapy. (3) Establishing a “1+X” ward-based clinical pharmacist model. (4) Developing informatics-driven alerts within the hospital’s prescribing system.
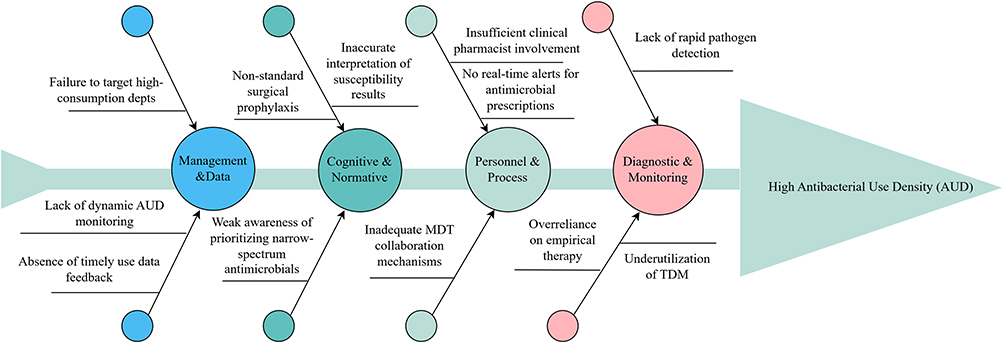 |
Figure 2 Fishbone diagram identifying causes of high AUD. |
Do
Promoting the Application of TDM and ddPCR in Key Clinical Departments
To enable clinicians to perform precise assessments of drug efficacy, ASP team successfully established an Antimicrobial Drug Blood Concentration Monitoring Program. We compiled and published the Zhejiang Provincial Tongde Hospital Therapeutic Drug Monitoring (TDM) Standard Manual to guide physicians and nurses in performing standardized sampling procedures. The hospital laboratory is now equipped to monitor the plasma concentrations of twenty-three commonly used antibiotics, including carbapenems, β-lactams, vancomycin, and tigecycline. Based on the TDM results, clinical pharmacists collaborate directly with physicians to optimize antibiotic selection, dosage, and dosing frequency.
Furthermore, we developed a novel droplet digital PCR (ddPCR) assay for the rapid quantification of pathogens and antimicrobial resistance (AMR) genes. This assay utilizes specific primers and fluorescent probes designed to target conserved nucleic acid regions of 13 pathogenic microbial genera and 7 bacterial AMR genes. The ddPCR platform provides absolute quantification of target nucleic acids in patient samples, making it particularly suitable for the rapid detection of common isolates and AMR genes in patients with suspected bloodstream infections in the Intensive Care Unit (ICU).
Implementing Complex Case Discussions Within the ASP Framework to Guide Optimal Therapy
A core intervention was the formal implementation of bi-weekly to monthly multidisciplinary ASP case discussion rounds. These sessions were led by the Medical Administration Department and clinical pharmacists, with integral input from infectious disease physicians, microbiologists, and radiologists. Clinical pharmacists took responsibility for proactively identifying and submitting cases for discussion, as well as facilitating the proceedings. Cases were selected based on pre-defined criteria, such as infections with multidrug-resistant organisms or failure of initial empiric therapy. During structured discussions, the team reviewed diagnostic data and collaboratively formulated a consensus recommendation for therapy optimization.
Establishing a “1+X” Ward-Based Clinical Pharmacist Model
To fully leverage the role of clinical pharmacists as pivotal forces in promoting rational antimicrobial use, our hospital innovatively implemented a “1+X” ward-based clinical pharmacist model. This model required clinical pharmacists to support multiple (X) surgical departments, building upon their base responsibilities in one permanently assigned internal medicine department. This structure was specifically designed to enhance pharmacist engagement within the surgical system.
A key focus of the “1+X” model was the standardization of surgical antimicrobial prophylaxis (SAP), where baseline data revealed two predominant issues: unnecessarily high prophylaxis usage rates and prolonged duration beyond recommended guidelines. Through this model, clinical pharmacists actively engaged in surgical ward rounds, preoperative discussions, and postoperative follow-up. They conducted prospective audit and feedback on SAP for all Type I, II, and III incisions, with particular emphasis on rationalizing prescription indications and enforcing a ≤24-hour duration protocol. Furthermore, clinical pharmacists provided structured feedback to department heads regarding adherence to SAP guidelines, focusing specifically on justification of use and appropriate duration. This established a continuous “feedback-improvement-re-feedback” cycle aimed at sustaining optimized antimicrobial prophylaxis practices.
Developing Informatics-Driven Alerts Within the Hospital’s Prescribing System
To enhance prescribing decision-support, we implemented two key informatics-driven interventions within the hospital’s computerized physician order entry (CPOE) system. A real-time Antimicrobial Use Density (AUD) alert was integrated. Upon prescribing any antimicrobial agent, the system automatically calculates and displays the daily AUD value for that specific order. For instance, when a physician prescribes “Meropenem 1g q8h IV”, the system immediately prompts with “The AUD for this order is 1”. This provides clinicians with instant, quantitative feedback on the intensity of their antimicrobial selection. Concurrently, a default duration alert system was established, assigning predefined courses of 24 hours for surgical prophylaxis and 72 hours for empirical therapy. As the prescribed duration approaches this limit, the system triggers an automated alert requiring the physician to actively reassess the patient’s clinical status before extending therapy, thereby preventing unnecessarily prolonged antimicrobial exposure.
Check
In accordance with the established plan, the impact of the PDCA cycle was evaluated by comparing pre- and post-implementation data for both primary and secondary outcomes. The primary outcome was the change in the overall Antibacterial Use Density (AUD), measured in Defined Daily Doses (DDDs) per 100 patient-days, while secondary outcomes included the consumption volume of key antimicrobial agents and the utilization rates of droplet digital PCR (ddPCR) and Therapeutic Drug Monitoring (TDM) in targeted clinical departments.
All statistical analyses were performed using SPSS statistical software (version 25.0). Data are presented as numbers and percentages. Differences between groups were assessed using the Chi-square test and the Student’s t-test, with a p-value of <0.05 considered statistically significant.
Act
In the final phase of the cycle, the findings and statistical results from the Check phase were systematically fed back to the multidisciplinary ASP team for review. This forum served to discuss and resolve problems identified during the evaluation. Based on these discussions, the team formulated concrete recommendations and defined the key focus areas for the subsequent intervention cycle.
Successful measures, such as the “1+X” ward-based clinical pharmacist model and the informatics-driven alert protocol, were integrated into the hospital’s official standard operating procedures (SOPs) to ensure sustainability. Simultaneously, unresolved challenges and new opportunities for improvement were identified, establishing a clear agenda for the next PDCA cycle and thereby institutionalizing a culture of continuous quality enhancement in antimicrobial stewardship.
Results
Hospital-Wide Reduction in Antimicrobial Use
The implementation of the pharmacist-led PDCA cycle across all clinical departments was associated with a significant reduction in antimicrobial consumption at the institutional level. As summarized in Table 1, the overall hospital-wide Antibacterial Use Density (AUD) decreased from 49.68 DDDs per 100 patient-days in the pre-intervention period to 37.23 DDDs per 100 patient-days in the post-intervention period. This represents a relative reduction of 25.06% in the primary outcome measure. A paired t-test conducted on the AUD values from all 34 departments confirmed that this reduction was statistically significant (t = 3.71, p < 0.001).
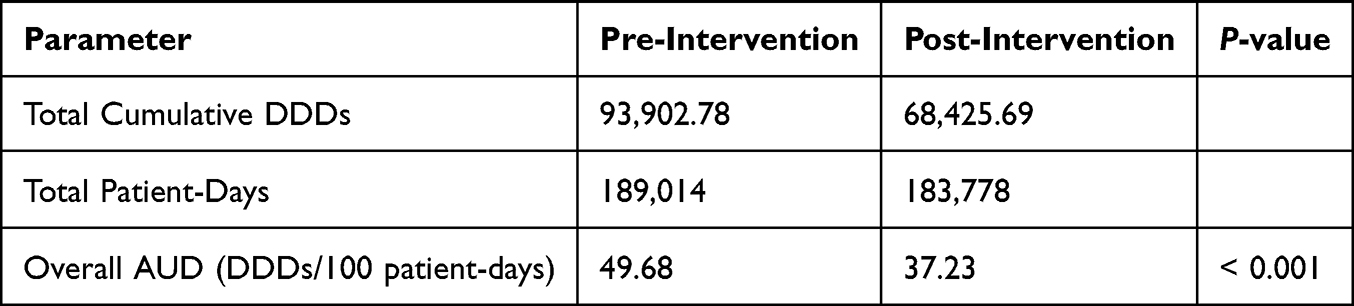 |
Table 1 Hospital-Wide Antimicrobial Use Outcomes Before and After Intervention |
Enhancement of Diagnostic and Monitoring Stewardship
The sequential implementation of advanced diagnostic tools during the intervention period successfully established a new foundation for precision antimicrobial therapy. As illustrated in Figure 3, the clinical adoption of both TDM and ddPCR services demonstrated a strong and sustained upward trajectory following their introduction.
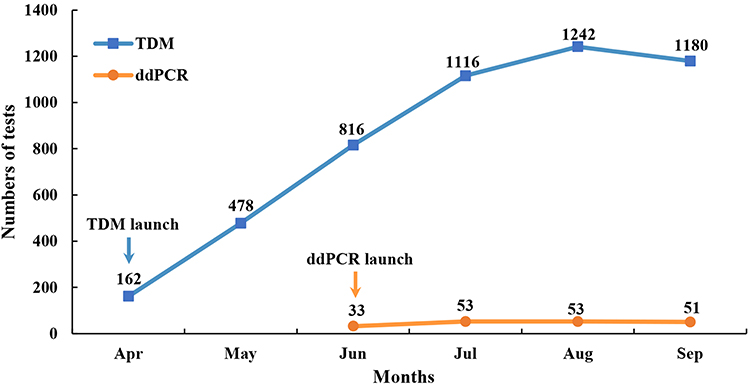 |
Figure 3 Monthly utilization of newly established TDM and ddPCR services. |
A Therapeutic Drug Monitoring (TDM) program was launched in April 2024. The service exhibited remarkable and consistent growth, with monthly test volumes increasing from 162 in the launch month to a peak of 1242 tests in August, representing a 7.7-fold increase and confirming its successful integration into routine clinical practice.
The droplet digital PCR (ddPCR) service for rapid pathogen identification was introduced in June 2024. It demonstrated immediate clinical utility, with test volumes increasing by 61% from June to July and maintaining at a stable, elevated level thereafter, underscoring its established role in the rapid diagnostic workflow.
Effectiveness of the Resource-Concentrating Strategy in Medical Departments
A resource-concentrating strategy was implemented in medical departments based on a Pareto analysis of baseline antimicrobial consumption. This analysis identified six key departments responsible for approximately 80% of total medical antimicrobial consumption: Hematology, Pulmonary and Critical Care Medicine, Infectious Diseases, Pediatrics, Emergency Intensive Care Unit, and Nephrology (Figure 4). These departments were designated as high-priority intervention targets.
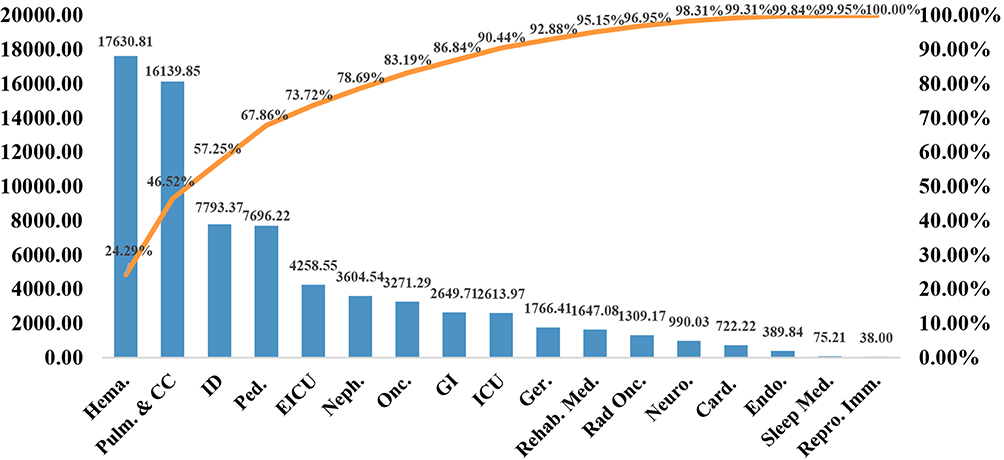 |
Figure 4 Pareto Chart of Baseline Antimicrobial Consumption in Medical Departments. The Orange curve indicates the cumulative percentage of total antimicrobial consumption. Abbreviations: Hema., Hematology; Pulm. and CC, Pulmonary and Critical Care Medicine; Ped., Pediatrics; ID, Infectious Diseases; EICU, Emergency Intensive Care Unit; Neph., Nephrology; Onc., Oncology; GI, Gastroenterology; ICU, Intensive Care Medicine; Ger., Geriatrics; Rehab. Med., Rehabilitation Medicine; RT, Radiotherapy; Neuro., Neurology; Card., Cardiology; Endo., Endocrinology; Sleep Med., Sleep Medicine; Reprod. Immunol., Reproductive Immunology. |
The targeted approach demonstrated significant effectiveness. As shown in Table 2, the key departments exhibited a substantial reduction in mean AUD from 109.76 to 86.50 DDDs/100 patient-days, representing an absolute reduction of 23.26 DDDs/100 patient-days. In comparison, the other medical departments showed a more modest decline from 24.51 to 19.34 DDDs/100 patient-days, with an absolute reduction of 5.17 DDDs/100 patient-days.
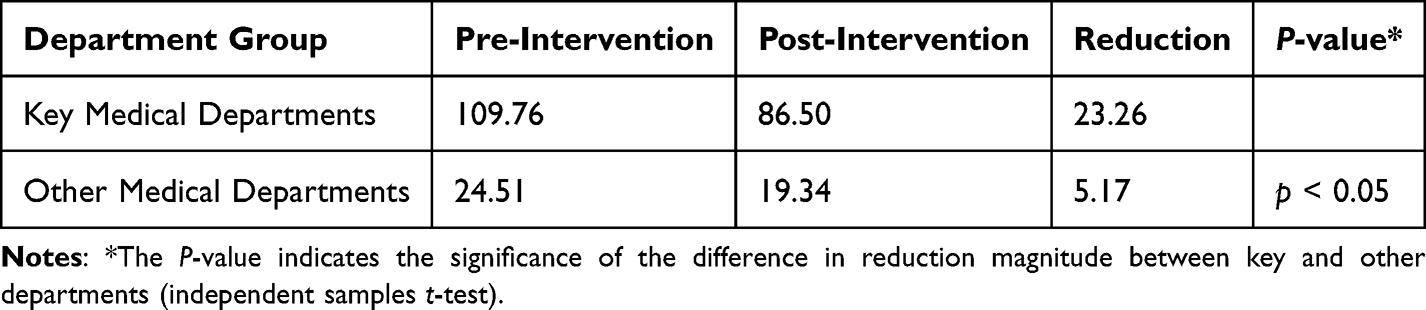 |
Table 2 Comparative Analysis of AUD Reduction Between Key and Other Medical Departments |
The difference in the magnitude of AUD reduction between the two groups was statistically significant (23.16 vs. 5.17 DDDs/100 patient-days; t = 2.59, p < 0.05). This result confirms that the resource-concentrating strategy effectively enhanced the intervention impact in high-priority medical departments.
Effectiveness of the “1+X” Model on Antimicrobial Use and Prophylaxis Quality in Surgical Departments
The “1+X” ward-based clinical pharmacist model significantly optimized antimicrobial use within the surgical system. The aggregate AUD for all 17 surgical departments decreased from 36.98 DDDs/100 patient-days at baseline to 31.94 DDDs/100 patient-days post-intervention, representing a relative reduction of 13.63% (t = 3.41, p < 0.001).
The intervention achieved marked enhancements in surgical antimicrobial prophylaxis quality across all wound types (Table 3). The most pronounced improvement was observed in duration rationality, which increased substantially for Type I incisions (from 50.54% to 78.44%, χ2 = 158.2, p < 0.001) and Type III incisions (from 70.77% to 91.46%, χ2 = 49.6, p < 0.001). Type II incisions also demonstrated significant improvement (from 62.86% to 69.31%, χ2 = 13.8, p < 0.001).
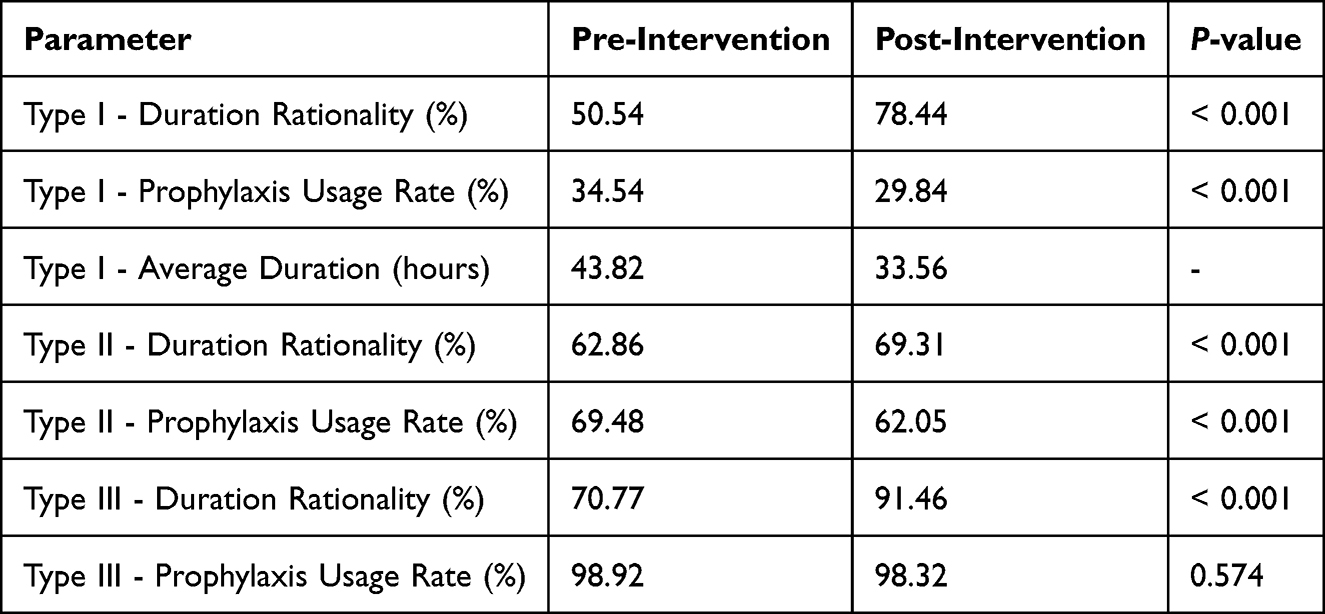 |
Table 3 Quality Metrics of Surgical Antimicrobial Prophylaxis Before and After Intervention |
Notably, the average prophylaxis duration for Type I incisions was reduced from 43.82 to 33.56 hours, representing a 23.4% decrease in antimicrobial exposure. Concurrently, prophylaxis usage rates decreased significantly for Type I incisions (from 34.54% to 29.84%, χ2 = 16.5, p < 0.001) and Type II incisions (from 69.48% to 62.05%, χ2 = 30.6, p < 0.001), while remaining appropriately high for Type III incisions.
Economic Impact and Structural Optimization of Antimicrobial Utilization
The total acquisition cost of antimicrobial agents decreased by 7.8%, from 13.16 million RMB to 12.13 million RMB over the six-month intervention period. More significantly, the cost per patient admission decreased from 1097 RMB to 947 RMB (13.7% reduction), demonstrating improved economic efficiency in patient care.
Structural analysis using the WHO AWaRe classification framework revealed fundamental improvements in prescribing quality (Figure 5). The proportion of AUD attributed to Access group medications increased substantially from 1.71% to 9.71%, representing a 5.7-fold increase in the utilization of first-line, narrow-spectrum agents. Concurrently, the utilization of Watch group antimicrobials decreased from 76.41% to 66.58% of total AUD, indicating reduced reliance on broad-spectrum agents. Most notably, antifungal drug utilization decreased by 45.5% in AUD, reflecting enhanced diagnostic stewardship and appropriate use of antifungal therapy. A parallel optimization was observed in the structure of antimicrobial expenditure.
 |
Figure 5 Comparative Impact on Antimicrobial Use and Expenditure: Structural Optimization Based on WHO AWaRe Classification. (A) Overall AUD, (B) AUD composition, (C) total expenditure, and (D) expenditure composition, before versus after intervention. |
Discussion
This study, through the implementation of a pharmacist-led PDCA cycle, successfully achieved a significant 25.06% reduction in the overall hospital Antibacterial Use Density (AUD). This success was not limited to a mere decrease in usage intensity but was accompanied by a structural optimization of prescribing behaviors, a substantial enhancement of diagnostic and monitoring capabilities, and considerable economic benefits, collectively forming a multi-dimensional benchmark for quality improvement.
Differentiated Intervention Pathways: A Data-Driven and Embedded Strategy
The observed hospital-wide reduction in AUD robustly validates the high applicability and effectiveness of the PDCA cycle as a classical management tool for implementing refined antimicrobial stewardship within a complex hospital setting.5 The success of this model can be attributed to its structured, closed-loop mechanism, which facilitated a systematic transition from problem identification to sustainable solution. Crucially, our approach transcended a simplistic, one-size-fits-all mandate. Instead, it was predicated on a thorough root cause analysis (as illustrated in Figure 2), which directly informed the development and execution of differentiated intervention pathways tailored to the distinct challenges of medical and surgical departments.
Within the medical department system, we applied the Pareto principle to strategically direct our limited stewardship resources toward six key clinical departments responsible for approximately 80% of total antimicrobial consumption. The result was a significantly greater reduction in AUD in these key departments compared to others (23.26 vs. 5.17 DDDs/100 patient-days). This strongly validates the considerable value of a data informed, resource concentrating strategy. This approach is supported by the work of Johnson et al, whose findings demonstrate that operationalizing stewardship to focus on specific high yield clinical scenarios is an effective method for achieving substantial, system-wide antibiotic reductions.6
In the surgical system, the innovative “1+X” ward-based clinical pharmacist model represented a strategic reorganization of pharmacy resources to address a systemic gap in surgical care. While clinical pharmacists in China typically undergo specialized training and subsequently collaborate with a fixed set of internal medicine departments,7 our model strategically extended this mandate by requiring pharmacists to proactively expand their services into multiple (X) surgical departments while maintaining their primary responsibilities. This approach was specifically designed to overcome the traditional under-engagement of clinical pharmacists in the surgical system8 and to shift the stewardship focus from merely reducing consumption volumes to fundamentally improving the quality of Surgical Antimicrobial Prophylaxis (SAP). The model proved highly effective, significantly improving the rationality rates of prophylaxis duration for Type I and III incisions and substantially shortening the average prophylaxis time. It also reduced the aggregate AUD across surgical departments, a finding in line with the 29% DDD reduction reported in a recent single-centre, pharmacist-led orthopaedic internal fixation programme.9 These outcomes demonstrate that the formal integration of pharmacists into the surgical workflow was a critical success factor. By institutionalizing a mechanism for continuous, on-site guidance and audit, the model directly addressed the deeply rooted problem of prolonged SAP, underscoring its indispensable role in standardizing antimicrobial prophylaxis practices in surgery.10,11
Paradigm Shift Towards Precision Therapy: The Role of Diagnostics and Pharmacists
This study marks a pivotal transition from empirical to precision antimicrobial therapy at our institution, a shift aligned with evolving antimicrobial stewardship paradigms.12 This transition was facilitated by the successful establishment and rapid clinical adoption of TDM and ddPCR. The exponential growth in TDM utilization provides a scientific basis for the individualized dosing of critical drugs like vancomycin and β-lactams, thereby enhancing efficacy and minimizing toxicity, a principle strongly advocated in contemporary pharmacokinetic guidance.13 Concurrently, the clinical value of the ddPCR platform is strongly supported by our recent findings in a high-risk cohort.14 In a study of 400 patients with hematologic malignancies and sepsis, ddPCR demonstrated a significantly higher pathogen detection rate (49.33% vs. 17.50%, P < 0.01) and a drastically reduced time-to-result (4.06 hours vs. 72.47 hours for blood culture, P < 0.01). Most importantly, this rapid diagnostic advantage translated into superior patient outcomes, including a lower 28-day mortality (HR=0.55, P=0.01) and a significant reduction in antibiotic use density (AUD). The integration of these advanced diagnostic tools, now with robust outcome data, represents a cornerstone of modern antimicrobial stewardship and aligns with the international consensus on the critical importance of diagnostic stewardship.15
Crucially, the pharmacist served as the central orchestrator of this multifaceted intervention. From convening the ASP team and leading ward rounds to providing real-time feedback and education, pharmacists effectively bridged the gap between management policy and clinical practice. Their pivotal role, as demonstrated in this study, corroborates the global recognition of pharmacists as essential drivers of successful ASPs.9,16
Structural Optimization and Economic Implications: Beyond Volume Reduction
Our study revealed profound improvements in prescribing patterns that extend far beyond the mere reduction in consumption volume. Through the WHO AWaRe classification framework, we observed a striking near five-fold increase in the utilization of Access group antibiotics (from 1.71% to 9.71% of total AUD). This dramatic shift clearly indicates that our interventions effectively promoted “de-escalation” therapy and optimized the antimicrobial use structure, which is a fundamental objective of any Antimicrobial Stewardship Program (ASP).17 The significant increase in first-line, narrow-spectrum agents was complemented by a decrease in the proportional use of Watch group antibiotics, reflecting a move towards more targeted and sustainable prescribing practices.
Concurrently, the total acquisition cost of antimicrobial agents decreased by 7.8%, and the cost per patient admission saw a more substantial reduction of 13.7%. This synergy between optimized prescribing and economic outcomes demonstrates that the program achieved not simple cost-cutting, but an enhancement of therapeutic value. The concurrent optimization of both the AUD and cost structures signifies a strategic reallocation of resources towards more rational and cost-effective treatment regimens, underscoring the financial sustainability of high-quality antimicrobial stewardship.18,19
Limitations and Future Directions
Despite the positive outcomes, this study has several limitations that should be acknowledged. First, its single-center, quasi-experimental design limits the generalizability of the findings, which requires validation in hospitals of different levels and types. Additionally, as noted in the Methods section, the baseline AUD reported here differs from a prior publication4 due to a hospital-wide BI system upgrade. This upgrade implemented a refined algorithm that excludes antimicrobials administered via topical routes from AUD calculations, providing a more precise estimate of systemic antibacterial exposure and representing a methodological improvement rather than an inconsistency in data. Second, the PDCA cycle constituted a multi-faceted intervention bundle, making it difficult to precisely quantify the individual contribution of each specific component (eg, TDM, pharmacist ward rounds, informatics alerts). Furthermore, due to the study’s time constraints, we were unable to evaluate the long-term sustainability of this management model or its impact on more distal outcomes, such as bacterial resistance rates.
Future research should aim to design more rigorous multicenter randomized controlled trials to disentangle the effects of the individual interventions. Concurrently, long-term follow-up studies are warranted to observe whether the optimized trends identified here can be sustained and to ultimately assess the model’s impact on critical clinical outcomes, such as patient mortality and infection relapse rates, as well as on antimicrobial resistance patterns.
Conclusion
In conclusion, this pharmacist-led, PDCA-based Antimicrobial Stewardship Program successfully demonstrated a multi-dimensional improvement in antimicrobial use within a tertiary hospital. The intervention achieved a significant reduction in consumption intensity alongside a fundamental optimization of prescribing patterns, confirmed by a structural shift towards narrower-spectrum agents and enhanced surgical prophylaxis quality, all while generating substantial economic benefits. The proven effectiveness of the innovative “1+X” pharmacist model and the strategic integration of precision diagnostic tools establish this comprehensive approach as a replicable and sustainable blueprint for other healthcare institutions. This model provides a viable pathway for strengthening hospital antimicrobial stewardship and contributing to the global fight against antimicrobial resistance.
Acknowledgments
We thank all the medical staff involved in this project.
Funding
This work was supported by Zhejiang Provincial Kang’enbei Hospital Management Soft Science Research Project (2024ZHA-KEB316).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Endale H, Mathewos M, Abdeta D. Potential causes of spread of antimicrobial resistance and preventive measures in one health perspective-a review. Infect Drug Resist. 2023;16:7515–11. doi:10.2147/IDR.S428837
2. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
3. Yin D, Tang Y, Wang S, et al. Use of multiple metrics and clustering analysis to assess antimicrobial use in Shanxi hospitals, China: a cross-sectional study based on 25 general hospitals. Front Public Health. 2025;13:1464613. doi:10.3389/fpubh.2025.1464613
4. Xin C, Yang B, Pang L, et al. Antimicrobial stewardship reduces antibiotic use density and cost in a Chinese tertiary hospital. Sci Rep. 2025;15(1):23609. doi:10.1038/s41598-025-06622-5
5. Zhang H, Wang Y, Diao R, et al. The practice and evaluation of antifungal stewardship programs at a tertiary first-class hospital in China. BMC Infect Dis. 2024;24(1):506. doi:10.1186/s12879-024-09405-x
6. Johnson MC, Hulgan T, Cooke RG, et al. Operationalising outpatient antimicrobial stewardship to reduce system-wide antibiotics for acute bronchitis. BMJ Open Qual. 2021;10(3):e001275. doi:10.1136/bmjoq-2020-001275
7. Huang H, Yin Z, Du J, et al. Development of a self-assessment tool to evaluate the readiness of pharmacy departments for internship training in China: a two-phase study. BMC Med Educ. 2024;24(1):1129. doi:10.1186/s12909-024-06088-5
8. Ierano C, Thursky K, Peel T, et al. Influences on surgical antimicrobial prophylaxis decision making by surgical craft groups, anaesthetists, pharmacists and nurses in public and private hospitals. PLoS One. 2019;14(11):e0225011. doi:10.1371/journal.pone.0225011
9. Zhou X, Gong J, Su D, et al. Effect of pharmacist intervention on antibiotic prophylaxis in orthopedic internal fixation: a retrospective study. Res Social Adm Pharm. 2023;19(2):301–307. doi:10.1016/j.sapharm.2022.10.002
10. Fésüs A, Benkő R, Matuz M, et al. The effect of pharmacist-led intervention on Surgical Antibacterial Prophylaxis (SAP) at an orthopedic unit. Antibiotics. 2021;10(12):1509. doi:10.3390/antibiotics10121509
11. Elnour AA, Al-Khidir IY, Elkheir H, et al. Double blind randomized controlled trial for subjects undergoing surgery receiving surgical antimicrobial prophylaxis at tertiary hospital: the clinical pharmacist’s interventions. Pharm Pract. 2022;20(4):2727. doi:10.18549/PharmPract.2022.4.2727
12. Hibbard R, Mendelson M, Page SW, et al. Antimicrobial stewardship: a definition with a One Health perspective. NPJ Antimicrob Resist. 2024;2(1):15. doi:10.1038/s44259-024-00031-w
13. O’Jeanson A, Nielsen EI, Friberg LE. Therapeutic drug monitoring (TDM) of β-lactam/β-lactamase inhibitor (BL/BLI) drug combinations: insights from a pharmacometric simulation study. J Antimicrob Chemother. 2025;80(1):79–86. doi:10.1093/jac/dkae375
14. Zheng B, Xin C, Liu Y, et al. Optimizing clinical indicators in hematologic malignancies and sepsis using ddPCR: a retrospective study. Infect Dis Ther. 2025;14(10):2299–2320. doi:10.1007/s40121-025-01207-1
15. Morrissey CO. Diagnosis and management of invasive fungal infections due to non-aspergillus moulds. J Antimicrob Chemother. 2025;80(Supplement_1):i17–i39. doi:10.1093/jac/dkaf005
16. Dighriri IM, Alnomci BA, Aljahdali MM, et al. The role of clinical pharmacists in Antimicrobial Stewardship Programs (ASPs): a systematic review. Cureus. 2023;15(12):e50151. doi:10.7759/cureus.50151
17. Dyar OJ, Huttner B, Schouten J, et al. What is antimicrobial stewardship? Clin Microbiol Infect. 2017;23(11):793–798. doi:10.1016/j.cmi.2017.08.026
18. Huebner C, Flessa S, Huebner NO. The economic impact of antimicrobial stewardship programmes in hospitals: a systematic literature review. J Hosp Infect. 2019;102(4):369–376. doi:10.1016/j.jhin.2019.03.002
19. Krishnamoorthy Y, Govindan D, Karunakaran M, et al. Global impact of antimicrobial stewardship programs in Healthcare: an umbrella review of effectiveness, cost-efficiency, and implementation strategies. J Infect Chemother. 2025;31(8):102753. doi:10.1016/j.jiac.2025.102753
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Quality Control Circle Practices to Reduce Specimen Rejection Rates
Li B, Cai X, Zhan L, Zhang X, Lin Y, Zeng J
Journal of Multidisciplinary Healthcare 2024, 17:4925-4935
Published Date: 26 October 2024
Applying Value-Based Healthcare Principles in Optimizing Post-Operative Oral Antibiotic Prophylaxis: A Pre-Post Intervention Study in a Single Center in Saudi Arabia
Youssef SA, Alshurtan KS, Alodayli RM, Alzinati HM, Mustafa SY
Infection and Drug Resistance 2026, 19:595284
Published Date: 7 May 2026