")
Back to Journals » Infection and Drug Resistance » Volume 13
Colonization by Pseudomonas aeruginosa and Staphylococcus aureus of Antral Biopsy Specimens from Gastritis Patients Uninfected with Helicobacter Pylori
Authors Kachuei V, Talebi Bezmin Abadi A , Rahimi F , Forootan M
Received 22 March 2020
Accepted for publication 30 April 2020
Published 13 May 2020 Volume 2020:13 Pages 1411—1417
DOI https://doi.org/10.2147/IDR.S254967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Vida Kachuei,1 Amin Talebi Bezmin Abadi,1 Farid Rahimi,2 Mojgan Forootan3
1Department of Bacteriology, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran; 2Research School of Biology, The Australian National University, Canberra, Australia; 3Gastroenterology and Liver Diseases Research Center, Research Institute for Gastroenterology and Liver Diseases, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Correspondence: Amin Talebi Bezmin Abadi
Department of Bacteriology, Faculty of Medical Sciences, Tarbiat Modares University, P.o. Box 14115-111, Tehran, Iran
Tel +98 21 8288-4883
Email [email protected]
Purpose: Roles and incidence of some microorganisms that transiently or permanently colonize the human stomach are still unknown despite advances in gastroenterology. We aimed to examine the incidence of four microorganisms, Helicobacter pylori, Pseudomonas aeruginosa, Staphylococcus aureus, and Staphylococcus epidermidis, in the antral biopsy specimens of patients with gastroduodenal conditions.
Patients and Methods: Patients (67 females, 33 males; mean age = 49.5 years) were initially examined and diagnosed by a gastroenterologist at the Mehrad Hospital, Tehran, Iran. We enrolled those who underwent the upper gastrointestinal endoscopy because of gastroduodenal conditions. Two antral biopsy samples were taken by endoscopy; the first sample was used for the “rapid urease test” to confirm H. pylori. The second was used for DNA extraction and PCR analyses with specific, corresponding primer sets to establish the presence of the four microorganisms. Our study was approved by the Ethics Committee at the Tarbiat Modares University, Tehran.
Results: Based on pathology and endoscopy findings, we divided the patients into three groups: 62 presented with gastritis, 18 with duodenal ulcer, and 20 gastric ulcer. The number of patients with P. aeruginosa but without H. pylori significantly differed from the number of those co-infected with both microorganisms (P = 0.03). Additionally, a similar significance was found between the incidence of S. aureus in patients without H. pylori and those with both infections (P = 0.04). Our results indicated that a significant number of patients with gastritis were colonized with P. aeruginosa or S. aureus without being co-infected with H. pylori (P < 0.001). Interestingly, the incidence of colonization by P. aeruginosa of patients without H. pylori (45/49, 91.8%) was higher than that by S. aureus (28/49, 57%).
Conclusion: The number of patients without H. pylori but with P. aeruginosa or with S. aureus infection significantly differed from that with both infections, respectively. Our study thus shows that patients without H. pylori infection are prone to be colonized by P. aeruginosa or S. aureus, indicating that targeted antibiotic regimens are necessary for clinically treating them.
Keywords: gastritis, Helicobacter pylori, microbiota, PCR, Pseudomonas aeruginosa, Staphylococcus aureus
Introduction
The cumulative epidemiological knowledge about Helicobacter pylori as a pathogenic gastric colonizer of humans has profoundly changed the general mindset in the field:1,2 surprisingly, only small proportions of infected subjects, mainly in the developing countries, end up with severe gastroduodenal diseases such as gastric cancer. Thus, field investigators have started studying other bacterial species that could potentially permanently or transiently colonize the human stomach and potentially cause gastroduodenal diseases.3,4 Prevotella, Neisseria, Staphylococcus, and Streptococcus have been reportedly found in the stomach; however, some of these bacteria were found also in the esophagus with less-studied clinical relevance.5–7 Evidence suggests that colonization by some species, for example, Streptococcus salivarius, which have urease activity, generates a less acidic environment, thus favoring H. pylori colonization.8 Hansson et al have described that the production of acid in the antrum is increased mainly after gastritis whereas the risk of gastric cancer is slightly reduced.9 With the exception of H. pylori, the clinical relevance of other bacteria in gastroduodenal disorders has not been fully understood. Like the patchy gastric distribution of H. pylori that changes with changing acidic output in some patients,10 other bacterial species also may transiently colonize the human stomach likely with unmanifested clinical outcomes. To unravel non-Helicobacter species, Andersson et al investigated six patients (three with and three without H. pylori (non-pylori) infection) using barcoded pyrosequencing; surprisingly, they found diverse bacterial populations in subjects without H. pylori.11 Pyrosequencing is a synthesis-based sequencing method that involves measuring deoxynucleotide incorporation to primer-guided complementary DNA sequences by measuring the release of pyrophosphate.12 Llorca et al showed that the presence or absence of H. pylori infection in pediatric subjects could change the composition of the gastrointestinal microbial communities.13 Schulz et al reported that colonization by H. pylori affects the composition of the bacterial communities in the oral cavity.14 Many researchers so far have focused on specific roles of H. pylori in initiating or exacerbating some gastroduodenal disorders; not many have directly investigated the coexistence of the certain microorganisms in the human stomach in the absence or presence of H. pylori.15 Some researchers have studied pediatric populations or colonization of the oral cavity;16–18 thus, our understanding of gastric microbiota in adults is limited.
Here, we sought to determine the prevalence of Pseudomonas aeruginosa, Staphylococcus aureus, and Staphylococcus epidermidis in the antral biopsy samples of patients positive or negative for H. pylori. These microorganisms frequently colonize the human stomach.11,19-21 Iran has a high prevalence of H. pylori infection (40–90%)22,23 and provides a novel population sample for conducting such a study.
Patients and Methods
Study Design, Sample Collection, and Ethics
Biopsy samples were collected at the gastroenterology unit of Mehrad Hospital, Tehran from January 2018 to March 2019. Patients were candidates for the upper gastrointestinal endoscopy because of gastroduodenal complaints, including epigastric pain. Participation in the study was voluntary, and subjects were informed that they could disenroll whenever they wished. The participants signed the informed consent forms, and the study protocols were reviewed and approved by the Clinical Research Ethics Committee of Tarbiat Modares University, Tehran (IR.MODARES.REC.1397.244). Our study was conducted in accordance with the Declaration of Helsinki.24 The exclusion criteria included being under 18 or older than 80 years of age, having autoimmune diseases, history of abdominal surgery 3 months before endoscopy, history of antibiotic treatment against H. pylori, active gastric bleeding, taking antacid medications 2 weeks before endoscopy, and pregnancy. Gastroscopic endoscopy was performed by an expert gastroenterologist, and the reports were subsequently sent to our laboratory within 2 to 3 weeks. All clinical documents were kept confidential. In brief, two antral biopsy specimens were taken; the first one was used for rapid urease test (RUT) testing, and the second specimen was kept in sterile 1.5-mL Eppendorf tubes containing the thioglycolate broth (Merck, Germany) at 4°C for transporting to the laboratory for subsequent microbiological testing. Microbiology included genetically identifying and confirming the four bacterial species, that is, H. pylori, S. epidermidis, S. aureus, and P. aeruginosa.
DNA Extraction, PCR, and RUT
Genomic DNA was extracted using a commercial kit (QIAGEN, Germany) according to the manufacturer’s instructions. To confirm H. pylori infection in the biopsy samples, we used the glmM-specific primer sets described previously.25 For the three other microorganisms, DNA was amplified using their corresponding universal primer sets as detailed in Table 1. We designed and confirmed by sequencing the primers for amplifying aap (Gene ID: 2828035), which is specific for a genetic region of S. epidermidis. We used PA431C (GenBank accession No. NP_253925) amplification to confirm the presence of P. aeruginosa. In parallel, we used nuc (thermonuclease gene specific for S. aureus) to confirm the presence of S. aureus in the samples.26,27 PCR amplification was done in 20 µL using a T100 PCR machine (Bio-Rad, Berkeley, California). Optimal PCR conditions for each primer set are summarized in Table 1.
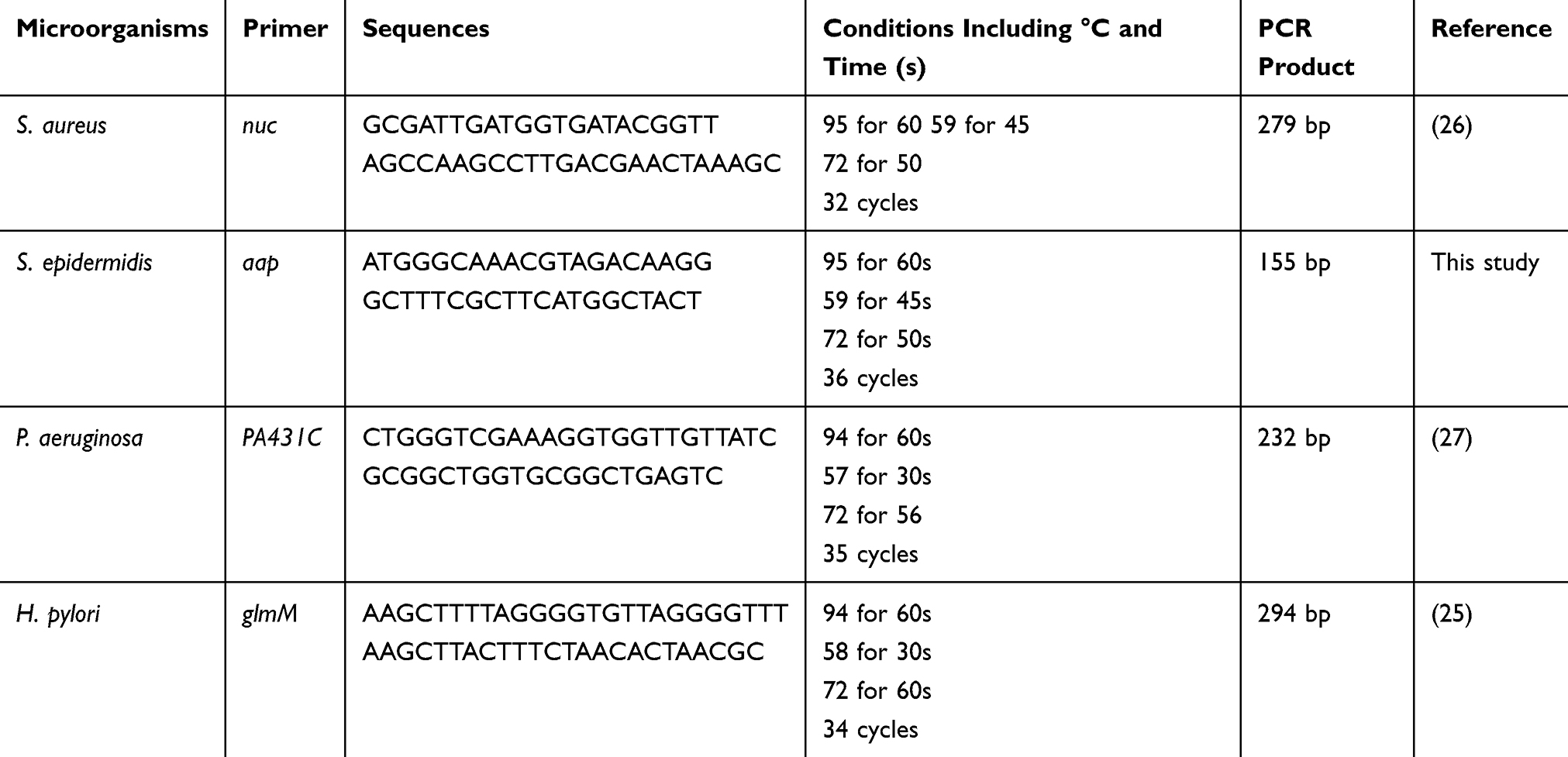 |
Table 1 Primer Sequences and PCR Conditions |
PCR products were checked by gel electrophoresis in 1.5% (w/v) agarose (Sina-clon, Tehran, Iran) in Tris/borate/EDTA (TBE) buffer. Gels were stained with GelRed® and subjected to UV transillumination (Biometra, Germany) and imaging. We included previously diagnosed clinical samples as positive controls, and negative controls by excluding the DNA template to ensure experimental quality.
RUT was used to confirm H. pylori biochemically. We included the samples positive for both glmM PCR and RUT in our first group (H. pylori positive). For the second group, we included only the samples that were negative for both RUT and glmM PCR.
Statistical Analyses
The IBM SPSS 18.0 software was used for statistical analyses. The status of each subject as positive or negative for H. pylori was independently determined and reported using the Student’s t-test. A p-value of <0.05 was deemed to be statistically significant.
Results
We examined the antral biopsy specimens from 100 patients. Patients included 67 females and 33 males, averaging 49.5 years of age. Patients with positive RUT and positive glmM PCR were categorized as definitely positive for H. pylori. Only two patients had negative RUT but positive glmM; these patients were excluded from the study. Altogether, 49 patients were negative and 51 were positive for H. pylori (35 F, 16 M). We repeated 10% of the PCR experiments in a double-blinded approach to double-check the consistency and integrity of our experiments and results. Unsurprisingly, the reported findings from the two independent operators were consistent.
Table 2 shows the prevalence of the three different microorganisms among the two groups, positive or negative for H. pylori. Of the total biopsy samples, 46% were positive for S. aureus, 44% positive for S. epidermidis, and 83% positive for P. aeruginosa (Table 2 and Figures 1 and 2). The concurrent colonization by Gram-negative and Gram-positive bacteria was found in 13% of samples.
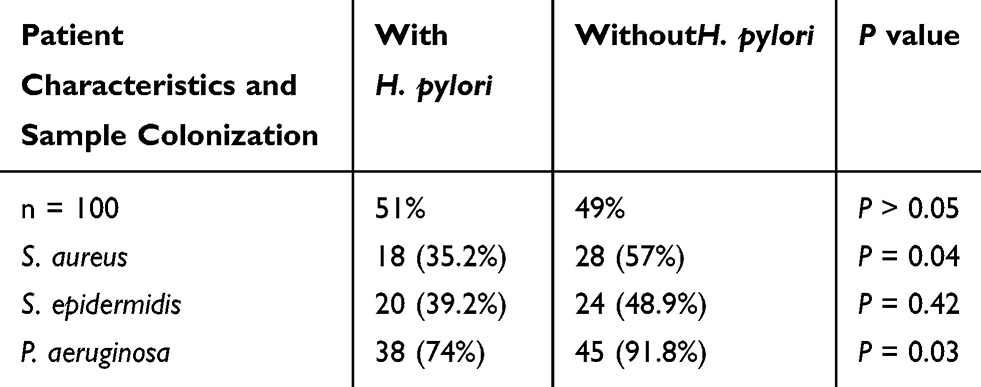 |
Table 2 Distribution of the Three Microorganisms Among Subjects Positive or Negative for H. Pylori |
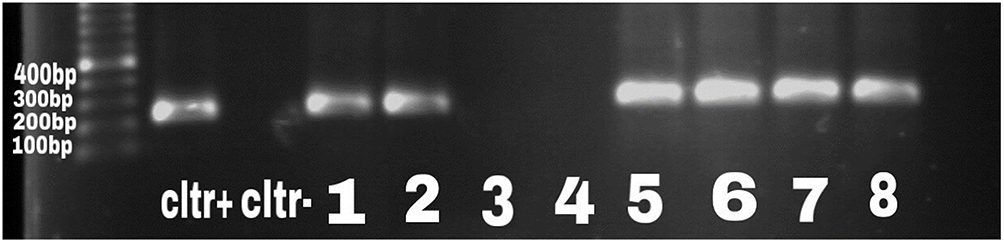 |
Figure 1 Gel electrophoresis for PA431C gene to determine the prevalence of P. aeruginosa. The band size was 232 bp. Samples 5–8 were positive, whereas 3 and 4 were negative clinical samples. |
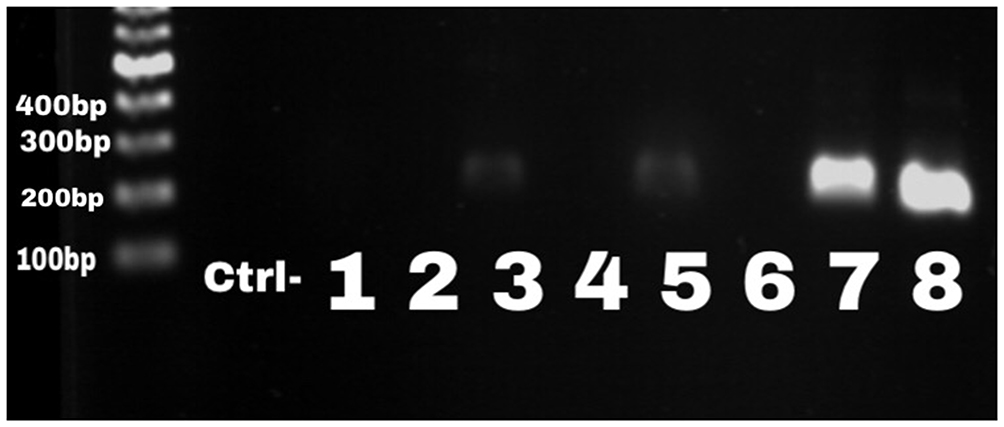 |
Figure 2 Gel electrophoresis for nuc gene to determine the prevalence of S. aureus. The band size was 279 bp; sample 8 was the positive control. Samples 3, 5, and 7 were considered as positive clinical samples. |
The incidence of the three microorganisms among the three investigated gastroduodenal diseases with positivity for H. pylori is presented in Table 3. Here, all patients were divided into three groups according to their pathology reports and clinical diagnoses established by a clinician: 62 had gastritis, 18 duodenal ulcer, and 20 gastric ulcer. We found a significant difference between subjects without H. pylori or with H. pylori who were also colonized with P. aeruginosa (P = 0.03). Similarly, colonization with S. aureus was significantly different between patients with or without H. pylori infection (P = 0.04).
 |
Table 3 Incidence of the Three Microorganisms Among Patients with the Three Digestive Conditions |
We calculated the incidence of each microorganism among the three groups of patients. We found that patients with gastritis were colonized significantly more with P. aeruginosa regardless of being coinfected with H. pylori (P < 0.001). Interestingly, colonization of P. aeruginosa in patients without H. pylori was more prevalent than in those with H. pylori, that is 38/49 (77%) versus 26/51 (50%), respectively (Table 2).
Discussion
Historically, the low gastric pH has been thought to be a physiological barrier against colonization by microorganisms.28,29 Moreover, colonization by Gram-negative bacteria in the upper gastrointestinal tract has reportedly been uncommon.30–32 To assess the prevalence and likely clinical relevance of the three microorganisms—P. aeruginosa, S. aureus, and S. epidermidis—in the context of gastritis, gastric ulcer, and duodenal ulcer, we studied 100 Iranian patients with or without H. pylori infection. The patients were diagnosed according to pathological and endoscopic findings. We found that colonization by P. aeruginosa in the antral biopsies of patients with or without H. pylori was high, 74% and 91.8%, respectively. Because the incidence of P. aeruginosa in patients without H. pylori was higher 38/49 (77%) than that in patients with H. pylori, we speculated that this higher incidence may be associated with pylori-negative gastritis patients. As presented in Table 3, patients with gastritis were more significantly colonized with P. aeruginosa (P < 0.001) than patients with S. epidermidis or S. aureus (P > 0.05). As far as we know, such a finding has not been reported previously. Present literature mostly reports on the microbial communities in the gastrointestinal tract of pediatric patients,33–36 whereas our subjects were older adults. The population studied here represent those of a particular socioeconomic status and a different ethnical group and genetic pool. Several studies have shown that patients with or without H. pylori infection are colonized with discrepant Enterobacteriaceae populations.37–41 As we found, subjects without H. pylori infection were colonized more significantly with the three investigated microorganisms compared to those with H. pylori co-infection (P < 0.05; Table 2). Our findings do not agree with that by Benavides et al, reporting a significant link between colonization by Prevotella, Clostridium, and the presence of H. pylori infection.42
Association of gastritis with H. pylori infection has been well documented.43–45 However, gastritis due to non-pylori bacteria and its prognosis to develop into severe gastroduodenal disorders are not well studied.46 We, thus, present that the roles of P. aeruginosa or S. aureus in initiating local acute mucosal gastritis will be an interesting future area of gastroenterology research. Our study was limited by the small population size, hampering the conclusions on the impact of H. pylori on other potential gastric co-infections. A longitudinal study with a larger population size is necessary to elucidate various aspects of the implications of our study.
Non-Pylori Gastritis: Unknown Clinical Relevance
Presently, the predominant clinical understanding of H. pylori is that this microorganism majorly causes gastritis, and that successful eradication of H. pylori leads to the elimination of problematic gastroduodenal diseases and their complications.47 Haber et al reported that up to 90% of non-pylori gastritis may be explained by colonization with other microbiological agents;48 for example, autoimmune gastritis and long-term administration of proton-pump inhibitors (PPIs).49 In our study, we documented whether patients had a history of PPI medication and excluded those with any PPI treatment done 2 months before the endoscopy. We tend to conclude that easy access to PPI treatment in Iran and other developing countries should be an acceptable factor for non-pylori gastritis cases. We did not have any history of autoimmune gastritis for patients who participated in our study. To date, the infectious cause of non-pylori gastritis has been underestimated as evidenced by the lack of relevant studies. Our findings showed that high incidence of P. aeruginosa among the non-pylori gastritis cases (77.5%) should be a starting point for future studies. Importantly, our findings also highlight that the clinical prognoses of non-pylori gastritis are unknown. For instance, can the patients progress to develop pan-gastritis or gastric cancer later in life? Is there a risk of peptic ulcer in such patients? We hope that molecular and future long-term clinical studies will resolve such questions for patients with non-pylori gastritis.
Conclusion
We found a relatively high incidence of S. epidermidis, P. aeruginosa, and S. aureus in non-pylori gastritis patients, a previously unexpected observation. The novelty of our findings reflects the significant colonization of P. aeruginosa among patients suffering from gastritis. An initial endoscopy without positive RUT results or positive microbiological or genetic H. pylori results should trigger the search for other causative agents. We conclude that clinicians should consider eradication of this multidrug-resistant Gram-negative bacterium (P. aeruginosa) before prescribing antibiotics against H. pylori.
Acknowledgment
The authors would thank the research deputy of Tarbiat Modares University, Iran for financially supporting this project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khalifa MM, Sharaf RR, Aziz RK. Helicobacter pylori: a poor man’s gut pathogen? Gut Pathog. 2010;2(1):2. doi:10.1186/1757-4749-2-2
2. Venneman K, Huybrechts I, Gunter MJ, Vandendaele L, Herrero R, Van Herck K. The epidemiology of Helicobacter pylori infection in Europe and the impact of lifestyle on its natural evolution toward stomach cancer after infection: a systematic review. Helicobacter. 2018;23(3):e12483. doi:10.1111/hel.12483
3. Dicksved J, Lindberg M, Rosenquist M, Enroth H, Jansson JK, Engstrand L. Molecular characterization of the stomach microbiota in patients with gastric cancer and in controls. J Med Microbiol. 2009;58(4):509–516. doi:10.1099/jmm.0.007302-0
4. Khosravi Y, Dieye Y, Poh BH, et al. Culturable bacterial microbiota of the stomach of Helicobacter pylori positive and negative gastric disease patients. ScientificWorldJournal. 2014;2014:610421. doi:10.1155/2014/610421
5. Chen X, Xia C, Li Q, Jin L, Zheng L, Wu Z. Comparisons between bacterial communities in mucosa in patients with gastric antrum ulcer and a duodenal ulcer. Front Cell Infect Microbiol. 2018;8:126. doi:10.3389/fcimb.2018.00126
6. Di Pilato V, Freschi G, Ringressi MN, Pallecchi L, Rossolini GM, Bechi P. The esophageal microbiota in health and disease. Ann NY Acad Sci. 2016;1381(1):21–33. doi:10.1111/nyas.13127
7. Khosravi Y, Loke MF, Goh KL, Vadivelu J. Proteomics analysis revealed that crosstalk between Helicobacter pylori and Streptococcus mitis may enhance bacterial survival and reduces carcinogenesis. Front Microbiol. 2016;7:1462. doi:10.3389/fmicb.2016.01462
8. Beasley DE, Koltz AM, Lambert JE, Fierer N, Dunn RR. The evolution of stomach acidity and its relevance to the human microbiome. PLoS One. 2015;10(7):e0134116. doi:10.1371/journal.pone.0134116
9. Hansson LE, Nyren O, Hsing AW, et al. The risk of stomach cancer in patients with gastric or duodenal ulcer disease. N Engl J Med. 1996;335(4):242–249. doi:10.1056/NEJM199607253350404
10. Kim N, Choi YJ. Change of acid secretions, ghrelin and leptin. In: H. Pylori. In: Helicobacter Pylori. Springer; 2016:53–76.
11. Andersson AF, Lindberg M, Jakobsson H, Backhed F, Nyren P, Engstrand L. Comparative analysis of human gut microbiota by barcoded pyrosequencing. PLoS One. 2008;3(7):e2836. doi:10.1371/journal.pone.0002836
12. Ronaghi M, Uhlen M, Nyren P. A sequencing method based on real-time pyrophosphate. Science. 1998;281(5375):363, 365. doi:10.1126/science.281.5375.363
13. Llorca L, Perez-Perez G, Urruzuno P, et al. Characterization of the gastric microbiota in a pediatric population according to Helicobacter pylori status. Pediatr Infect Dis J. 2017;36(2):173–178. doi:10.1097/INF.0000000000001383
14. Schulz C, Schutte K, Koch N, et al. The active bacterial assemblages of the upper GI tract in individuals with and without Helicobacter infection. Gut. 2018;67(2):216–225. doi:10.1136/gutjnl-2016-312904
15. Aviles-Jimenez F, Vazquez-Jimenez F, Medrano-Guzman R, Mantilla A, Torres J. Stomach microbiota composition varies between patients with non-atrophic gastritis and patients with intestinal type of gastric cancer. Sci Rep. 2014;4(1):4202. doi:10.1038/srep04202
16. Baker JL, Bor B, Agnello M, Shi W, He X. Ecology of the oral microbiome: beyond bacteria. Trends Microbiol. 2017;25(5):362–374. doi:10.1016/j.tim.2016.12.012
17. Fan X, Alekseyenko AV, Wu J, et al. Human oral microbiome and prospective risk for pancreatic cancer: a population-based nested case-control study. Gut. 2018;67(1):120–127. doi:10.1136/gutjnl-2016-312580
18. Koren O, Spor A, Felin J, et al. Human oral, gut, and plaque microbiota in patients with atherosclerosis. Proc Natl Acad Sci USA. 2011;108(Suppl 1):4592–4598. doi:10.1073/pnas.1011383107
19. Dominguez-Bello MG, Reyes N, Teppa-Garran A, Romero R, Interference of Pseudomonas strains in the identification of Helicobacter pylori. J Clin Microbiol. 2000;38(2):937. doi:10.1128/JCM.38.2.937-937.2000
20. Hu Y, He LH, Xiao D, et al. Bacterial flora concurrent with Helicobacter pylori in the stomach of patients with upper gastrointestinal diseases. World J Gastroenterol. 2012;18(11):1257–1261. doi:10.3748/wjg.v18.i11.1257
21. Pereira V, Abraham P, Nallapeta S, Shetty A. Gastric bacterial flora in patients harbouring Helicobacter pylori with or without chronic dyspepsia: analysis with matrix-assisted laser desorption ionization time-of-flight mass spectroscopy. BMC Gastroenterol. 2018;18(1):20. doi:10.1186/s12876-018-0744-8
22. Maleki I, Mohammadpour M, Zarrinpour N, Khabazi M, Mohammadpour RA. Prevalence of Helicobacter pylori infection in Sari Northern Iran; a population based study. Gastroenterol Hepatol Bed Bench. 2019;12(1):31–37.
23. Niknam R, Fattahi MR, Sepehrimanesh M, Safarpour A. Prevalence of Helicobacter pylori in southern part of Iran. Jundishapur J Microb. 2018;11(6). doi:10.5812/jjm.62379
24. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
25. Lu JJ, Perng CL, Shyu RY, et al. Comparison of five PCR methods for detection of Helicobacter pylori DNA in gastric tissues. J Clin Microbiol. 1999;37(3):772–774.
26. Choi HJ, Kim MH, Cho MS, et al. Improved PCR for identification of Pseudomonas aeruginosa. Appl Microbiol Biotechnol. 2013;97(8):3643–3651. doi:10.1007/s00253-013-4709-0
27. Wang T, Cai H, Sasazuki S, et al. Fruit and vegetable consumption, Helicobacter pylori antibodies, and gastric cancer risk: a pooled analysis of prospective studies in China, Japan, and Korea. Int J Cancer. 2017;140(3):591–599. doi:10.1002/ijc.30477
28. Martinsen TC, Bergh K, Waldum HL. Gastric juice: a barrier against infectious diseases. Basic Clin Pharmacol Toxicol. 2005;96(2):94–102. doi:10.1111/j.1742-7843.2005.pto960202.x
29. Tennant SM, Hartland EL, Phumoonna T, et al. Influence of gastric acid on susceptibility to infection with ingested bacterial pathogens. Infect Immun. 2008;76(2):639–645. doi:10.1128/IAI.01138-07
30. Brummer RJ, Stockbrugger RW. Effect of nizatidine 300 mg at night and omeprazole 20 mg in the morning on 24-hour intragastric pH and bacterial overgrowth in patients with acute duodenal ulcer. Digest Dis Sci. 1996;41(10):2048–2054. doi:10.1007/bf02093609
31. Gall A, Fero J, McCoy C, et al. Bacterial composition of the human upper gastrointestinal tract microbiome is dynamic and associated with genomic instability in a Barrett’s Esophagus Cohort. PLoS One. 2015;10(6):e0129055. doi:10.1371/journal.pone.0129055
32. Overby A, Murayama SY, Michimae H, et al. Prevalence of gastric non-Helicobacter pylori-Helicobacters in Japanese patients with gastric disease. Digestion. 2017;95(1):61–66. doi:10.1159/000452400
33. Collins BS, Lin HC. Chronic abdominal pain in children is associated with high prevalence of abnormal microbial fermentation. Digest Dis Sci. 2010;55(1):124–130. doi:10.1007/s10620-009-1026-7
34. Rosen R, Amirault J, Liu H, et al. Changes in gastric and lung microflora with acid suppression: acid suppression and bacterial growth. JAMA Pediatr. 2014;168(10):932–937. doi:10.1001/jamapediatrics.2014.696
35. Saulnier DM, Riehle K, Mistretta TA, et al. Gastrointestinal microbiome signatures of pediatric patients with irritable bowel syndrome. Gastroenterology. 2011;141(5):1782–1791. doi:10.1053/j.gastro.2011.06.072
36. Michail S, Lin M, Frey MR, et al. Altered gut microbial energy and metabolism in children with non-alcoholic fatty liver disease. FEMS Microbiol Ecol. 2015;91(2):1–9. doi:10.1093/femsec/fiu002
37. Brandi G, Biavati B, Calabrese C, et al. Urease-positive bacteria other than Helicobacter pylori in human gastric juice and mucosa. Am J Gastroenterol. 2006;101(8):1756–1761. doi:10.1111/j.1572-0241.2006.00698.x
38. Delgado S, Cabrera-Rubio R, Mira A, Suarez A, Mayo B. Microbiological survey of the human gastric ecosystem using culturing and pyrosequencing methods. Microb Ecol. 2013;65(3):763–772. doi:10.1007/s00248-013-0192-5
39. Lertpiriyapong K, Whary MT, Muthupalani S, et al. Gastric colonisation with a restricted commensal microbiota replicates the promotion of neoplastic lesions by diverse intestinal microbiota in the Helicobacter pylori INS-GAS mouse model of gastric carcinogenesis. Gut. 2014;63(1):54–63. doi:10.1136/gutjnl-2013-305178
40. Monstein HJ, Tiveljung A, Kraft CH, Borch K, Jonasson J. Profiling of bacterial flora in gastric biopsies from patients with Helicobacter pylori-associated gastritis and histologically normal control individuals by temperature gradient gel electrophoresis and 16S rDNA sequence analysis. J Med Microbiol. 2000;49(9):817–822. doi:10.1099/0022-1317-49-9-817
41. Pantoflickova D, Corthesy-Theulaz I, Dorta G, et al. Favourable effect of regular intake of fermented milk containing Lactobacillus johnsonii on Helicobacter pylori associated gastritis. Aliment Pharmacol Ther. 2003;18(8):805–813. doi:10.1046/j.1365-2036.2003.01675.x
42. Benavides-Ward A, Vasquez-Achaya F, Silva-Caso W, et al. Helicobacter pylori and its relationship with variations of gut microbiota in asymptomatic children between 6 and 12 years. BMC Res Notes. 2018;11:468. doi:10.1186/s13104-018-3565-5
43. Kuipers EJ, Uyterlinde AM, Pena AS, et al. Long-term sequelae of Helicobacter pylori gastritis. Lancet. 1995;345(8964):1525–1528. doi:10.1016/s0140-6736(95)91084-0
44. Shiota S, Thrift AP, Green L, et al. Clinical manifestations of Helicobacter pylori-negative gastritis. Clin Gastroenterol Hepatol. 2017;15(7):1037–1046e1033. doi:10.1016/j.cgh.2017.01.006
45. Sugano K, Tack J, Kuipers EJ, et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut. 2015;64(9):1353–1367. doi:10.1136/gutjnl-2015-309252
46. Nordenstedt H, Graham DY, Kramer JR, et al. Helicobacter pylori-negative gastritis: prevalence and risk factors. Am J Gastroenterol. 2013;108(1):65–71. doi:10.1038/ajg.2012.372
47. Ohkusa T, Fujiki K, Takashimizu I, et al. Improvement in atrophic gastritis and intestinal metaplasia in patients in whom Helicobacter pylori was eradicated. Ann Intern Med. 2006;101(5):380–386. doi:10.1111/j.1572-0241.2006.00698.x
48. Haber MM, Hunt B, Freston JW, et al. Changes of gastric histology in patients with erosive oesophagitis receiving long-term lansoprazole maintenance therapy. Aliment Pharmacol Ther. 2010;32(1):83–96. doi:10.1111/j.1365-2036.2010.04310.x
49. Zavros Y, Rieder G, Ferguson A, Samuelson LC, Merchant JL. Genetic or chemical hypochlorhydria is associated with inflammation that modulates parietal and G-cell populations in mice. Gastroenterology. 2002;122(1):119–133. doi:10.1053/gast.2002.30298
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.