")
Back to Journals » Journal of Inflammation Research » Volume 16
Coincidence of Systemic Lupus Erythematosus and ANCA-Associated Vasculitis: A Case Report with Perforation of Nasal Septum and Palate
Authors Liu Y , Yu S , Ma S, Yu J, Zuo D, Zhao W , Wang J, Wang J
Received 9 August 2023
Accepted for publication 21 November 2023
Published 6 December 2023 Volume 2023:16 Pages 5949—5957
DOI https://doi.org/10.2147/JIR.S434178
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yurun Liu,1,* Shengnan Yu,2,* Sha Ma,2 Juan Yu,2 Dachen Zuo,2 Weiqing Zhao,2 Juan Wang,2 Jing Wang2
1Department of Rheumatology and Immunology, The Affiliated Hospital of Kunming University of Science and Technology, The First People’s Hospital of Yunnan Province, Kunming, Yunnan, People’s Republic of China; 2Department of Rheumatology and Immunology, The First People’s Hospital of Yunnan Province, The Affiliated Hospital of Kunming University of Science and Technology, Kunming, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Wang, Department of Rheumatology and Immunology, The First People’s Hospital of Yunnan Province, The Affiliated Hospital of Kunming University of Science and Technology, Kunming, Yunnan, People’s Republic of China, Email [email protected]
Background: An overlap of systemic lupus erythematosus (SLE) and antineutrophil cytoplasmic antibodies- (ANCA-) associated vasculitis (AAV) is extremely uncommon and no clear definition has been proposed. The SLE/AAV overlap syndrome mainly affects kidney, blood count, nervous system and lung. However, few previous cases reported nasal septal and palatal perforation in this disorder.
Case Presentation: We presented a case of a 16-year-old female with a 6-month history of SLE, developed perforation of the nasal septum and palate. She was diagnosed with SLE due to facial malar rash, oral ulcer, increased erythrocyte sedimentation rate (ESR), low complement levels, and positive anti-Smith antibody. Approximately 6 months later, she had a perforation of the nasal septum and palate with positive anti-proteinase 3 antibody (anti-PR3-ANCA). A nasal endoscopic biopsy revealed an inflammatory polyp with chronic suppurative inflammation and inflammatory granulomatous hyperplasia. In this case, the clinical, biological, radiological, and histological findings substantiated the diagnosis of AAV. Infections, drug abuse, malignancies, IgG4-related disease (IgG4-RD) and trauma were excluded. So we diagnosed her with SLE/AAV overlap syndrome.
Conclusion: When a patient’s symptoms cannot be explained by one disease, we need to consider the overlapping of two diseases, especially in patients with autoimmune diseases.
Keywords: perforation of palate, systemic lupus erythematosus, ANCA-associated vasculitis, SLE/AAV overlap syndrome
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease with multisystemic involvement, ranging from mild cutaneous involvement to severe organ damage, such as kidney failure, pulmonary hypertension, and cardiac failure.1,2 The most frequent coexisting autoimmune diseases in SLE patients are autoimmune thyroid disease (18%), antiphospholipid syndrome (APS) (14%), and Sjogren’s Syndrome (SS) (14%),3 but the overlap syndrome between SLE and AAV is rare originally described in 2008.4
SLE/AAV overlap syndrome is an inflammatory disease characterized by clinical features of both SLE and AAV.5 According to recent literature, any organ may be affected in the SLE/AAV overlap syndrome. It is to be noted that kidney is most commonly involved, with rapidly progressive glomerulonephritis as the most common clinical manifestation.5,6 Other systemic involvement of the SLE/AAV overlap syndrome include cerebral ischemia, central nervous system vasculitis, subarachnoid hemorrhage, lupus granulomatous pneumonitis, pulmonary hemorrhage, arthritis, serositis, cytopenia, rhinosinusitis, and thrombopenia.5–7 As we have known so far, few previous cases have reported nasal and palatal perforation in this disorder. Here, we present a SLE/AAV overlap syndrome patient with perforation of the nasal septum and palate.
Case Report
A 16-year-old female patient was admitted to the emergency room with severe epistaxis and increased bleeding for 5 days. The patient was diagnosed with SLE 6 months ago due to facial malar rash, oral ulcer, increased erythrocyte sedimentation rate (ESR), low complement levels and positive anti-Smith antibody. The laboratory test results revealed blood count, urinalysis, immunology and biochemistry (Table 1). SLE disease activity index 2000 (SLEDAI-2K) of the patient was 6.8 She had not taken hydralazine, thioridazine or propylthiouracil, known to induce SLE and/or AAV. The patient was initially given intravenous methylprednisolone 80 mg per day for 3 times. After leaving the hospital, she was treated with prednisone 40 mg daily with subsequent dose tapering, hydroxychloroquine (HCQ) 0.2 g twice daily, and intravenous cyclophosphamide (CYC) 0.4 g half a month until remission was achieved and maintained. However, she stopped taking the medicine when prednisone was tapered to 20 mg.
 |
Table 1 Laboratory Results of First Admission |
The intraoral examination identified a 1*2 cm ulcer on the hard palate. Laboratory assessments revealed (Table 2) severe pancytopenia, elevated ESR and serum ferritin, decreased serum levels of complement C3 and C4, proteinuria and hepatic insufficiency. Compared to the last hospitalization, anti-Smith antibody turned negative, anti-U1-RNP, anti-SS-A, anti-SS-B and anti-ribosomal P protein (anti-P) antibodies were still positive by line-immunoassay (LIA). Meanwhile, our patient had c-ANCA positivity with a titer of 1:100 (<1:10) by indirect immunofluorescence (IIF). P-ANCA was negative. The titer of anti-PR3-ANCA antibody was >400.00 RU/mL (NR <20 RU/mL) by magnetic particle based chemiluminescent immunoassay (MPCLIA). Anti-MPO-ANCA antibody was <2.00 RU/mL (NR <20 RU/mL). We excluded pancytopenia caused by hematological diseases by performing bone marrow puncture. Cranial computed tomography (CT) scan showed soft tissue densities in paranasal sinuses and nasal cavities, and no bone destruction was found in the maxillary area and oral cavity. Chest CT scan revealed no evidence of numerous pulmonary nodules. SLEDAI-2K was 18.8
 |
Table 2 Laboratory Results of Second Admission |
Based on the above manifestations and examinations, we considered that the patient had recurrence of lupus. We gave methylprednisolone pulse therapy, intravenous immunoglobulin, together with immunosuppressor. The patient’s rash, blood count, liver enzymes, serum levels of complement C3 and C4, and ESR improved, but the palatal ulcer worsened, resulting in perforation of the hard palate (Figure 1). CT showed the palatal perforation (Figure 2). A nasal endoscopic biopsy was performed and histopathology showed an inflammatory polyp with chronic suppurative inflammation and inflammatory granulomatous hyperplasia (Figure 3). The cells within these lesions consist of fibroblasts, epithelioid cells, giant cells, surrounding scattered infiltrates of lymphocytes, monocytes, macrophages, plasma cells and neutrophils. Palatal perforation, a rare condition, can be seen in infections (eg syphilis, tuberculosis), autoimmune diseases (eg IgG4-RD, GPA), drug abuse (eg cocaine), malignancies (eg oral cavity squamous cell carcinoma, extranodal natural killer/T-cell lymphoma), and trauma.6,9–11 First, the syphilis antibodies and t-spot detection results for the patient were both negative, we ruled out syphilis and tuberculosis. Second, our patient had no previous history of drug abuse and trauma. Third, pathologists did not detect greater than 50 IgG4-positive plasma cells under high-power microscopy in the nasal histopathology. Furthermore, squamous cell carcinoma was not found in the nasal histopathology. Extranodal natural killer/T-cell lymphoma confirmatory histopathological and immunohistochemical tests with features of CD2+, cytoplasmic CD3+, CD56+, and EBV-encoded small RNA (EBER) positivity in situ.10 So we performed immunohistochemical tests of CD3, CD56, CD2, CD4, CD5, CD7, CD79a, CD8, CD19, CD20, PAX5, TIA-1, Ki-67, EBER, and Granzyme B were negative (Figure 4). According to Chapel Hill Consensus Conference definitions and 2022 ACR/EULAR classification criteria, the clinical, biological, radiological, and histological findings of our patient substantiated the diagnosis of GPA. At follow-up visits, the patient’s anti-PR3-ANCA antibody turned negative and the palatal perforation did not continue to enlarge. The patient was given low-dose maintenance steroid treatment and then referred to the Department of Otolaryngology for the evaluation of surgical repair of palatal perforation.
 |
Figure 1 Perforation of the hard palate, and the nasal cavity could be peered through the perforation. |
 |
Figure 2 CT showed the palatal perforation (red arrow). |
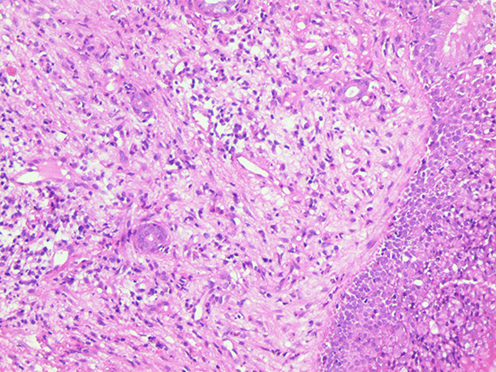 |
Figure 3 The nasal endoscopic biopsy section indicates inflammatory polyp with chronic suppurative inflammation and inflammatory granulomatous hyperplasia. (Hematoxylin-eosin stain). |
 |
Figure 4 Immunohistochemical tests of nasal biopsy were negative. (A) EBER. (B) Ki-67. (C) CD19. (D) CD20. (E) TIA-1. (F) CD8. (G) CD3. (H) CD2. (I) CD56. (J) CD79a. (K) CD7. (L) CD4. (M) Granzyme B. (N) Pax-5. |
Discussion
In conclusion, SLE patients with positive ANCAs can be characterized into two categories. One group of patients only present with positive ANCAs (in which more than 96% present with positive MPO),9 but with no clinical manifestations and pathological features of AAV. Another group of patients fulfill the classification criteria of both SLE and AAV, which can be defined as an overlap between SLE and AAV. The coexistence of SLE and AAV as an overlapping syndrome is not common, the patient that we discussed here had specific clinical manifestations and pathological features of GPA. Therefore, SLE/AAV overlap syndrome was established as the final diagnosis. This case suggests that there are several causes for nasal septal perforation, such as syphilis, tuberculosis, drug abuse, GPA, IgG4-RD and malignancies.
We searched and summarized the characteristics of SLE/AAV overlap syndrome in previous literature (Table 3). Of all cases, 18 patients were female, and the average age of diagnosis was 42. The patients mainly presented with multisystem involvement, of which nondestructive polyarthritis was the most common clinical presentation, and all patients were MPO positive. The case we reported was a young female with epistaxis onset, and then gradually developed nasal septal and palatal perforation, accompanied with hematological involvement and positive PR3-ANCAs, negative MPO-ANCAs. Positive PR3-ANCAs was also consistent with the clinical features of the patient, who presented with epistaxis, nasal septal perforation, and palatal perforation.
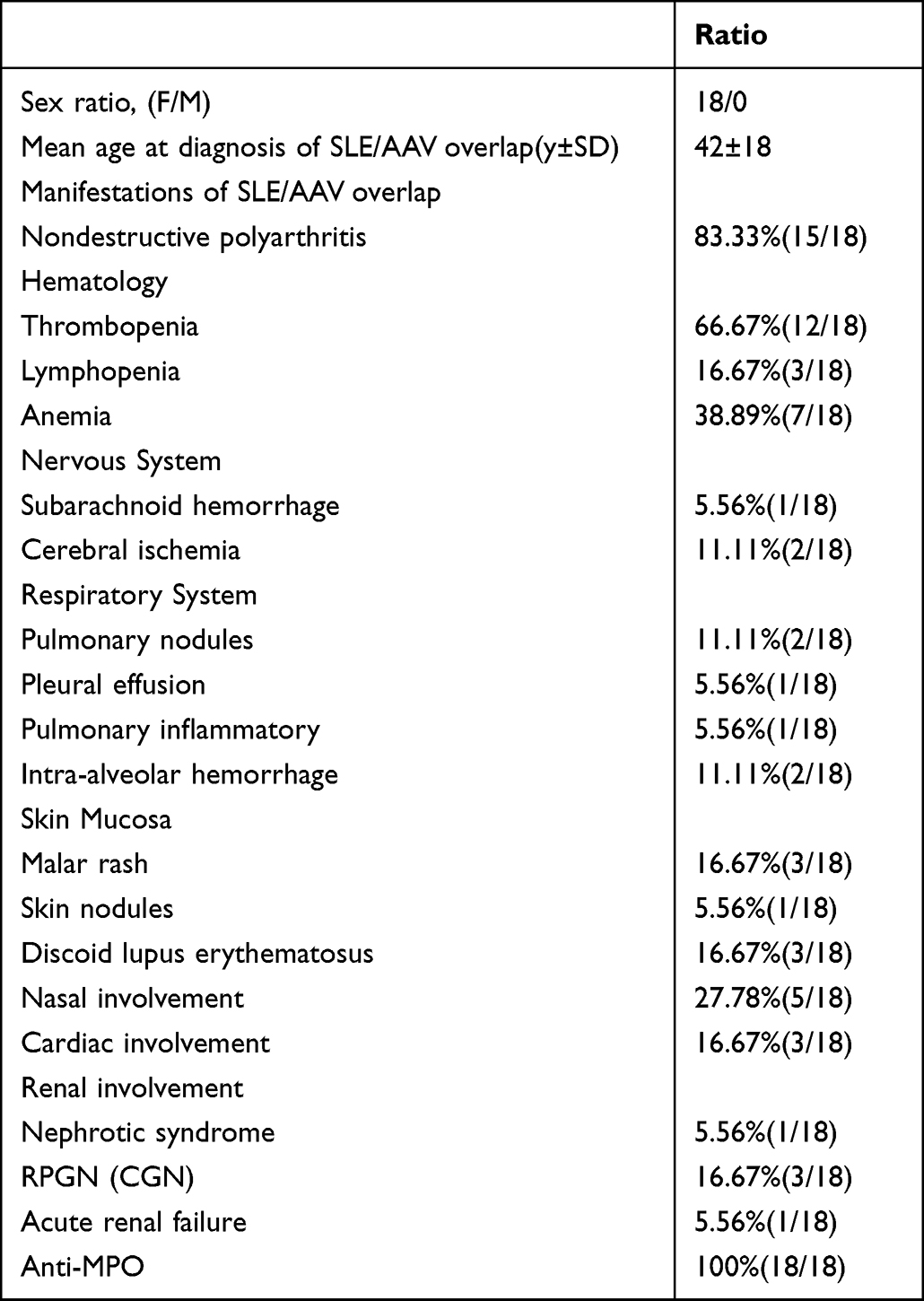 |
Table 3 Summary of Patients with the SLE/AAV Syndrome from Previous Reports in the Literature |
The concept of Shared Autoimmunity posits that overlap syndromes may be explained by a combination of common environmental factors and predisposing genes.12 During analysis of AAV genetic risk factors, it was found that SLE is associated with susceptibility genes for AAV (eg CD40, HLA-DRB1, IL-10, IL2RA, PTPN22, FCGR3B).13 The association indicates that is possible the presence of a common mechanism shared by SLE and AAV. No specific genetic studies were tested in this patient, but given these relations there is likely a common underlying genetic susceptibility.
SLE/AAV overlap syndrome is less common compared to SLE overlapping with SS or APS. The analysis of gene expression has revealed a robust neutrophil signature in SLE, while the activation of neutrophils is recognized as a characteristic feature of AAV.14 It indicates that the mechanism of SLE/AAV overlap is perhaps associated with neutrophils. Recently, it has been proposed that neutrophil extracellular traps (NETs) play a significant role in a variety of autoimmune diseases, such as SLE and AAV.15 NETs are extracellular networks of DNA scaffolds decorated with granular components, histones and cytoplasmic proteins which protrude from the membrane of activated neutrophils.16,17 Impaired degradation of NETs was observed in the serum of SLE patients, which was due to the presence of DNase-1 inhibitors and anti-NET antibodies that prevented access of DNase-1 to NETs.18 Meanwhile, SLE immune complexes can drive NETs formation.19 In AAV, ANCAs stimulate polymorphonuclear leukocytes (PMNs), monocytes, and endothelial cells to produce IL-8, which in turn cause NETs formation. Following that, NETs formation activates autoreactive B cells to produce more ANCAs.16 Impaired NETs clearance generates the accumulation of active-NETs at inflammatory sites, resulting in greater inflammation and the persistence of NETs autoantigens for a longer period of time. Reduced serum DNase1 activity was observed in both AAV and SLE.18,20 The imbalance between the creation and destruction of NETs during the NETosis process may be linked to the etiology of autoimmune diseases.16 NETs can interrupt self-tolerance by being a source of autoantigens for autoantibodies, such as anti-citrullinated protein antibodies (ACPAs) in RA, anti-dsDNA in SLE, and MPO-ANCA and PR3-ANCA in AAV.21 In the light of the above, we propose a hypothesis for the SLE/AAV overlap syndrome: regardless of whether the patient was first diagnosed with SLE or AAV, the excessive production and impaired degradation of NETs may cause the production of the autoimmune antibodies for another autoimmune disease, which in turn leads to overlap syndrome.
Conclusion
Not all SLE could be associated with AAV, it’s a small probability event. Since similar clinical features exist in both SLE and AAV, the symptoms should be first identified as caused by which disease before considering the diagnosis of SLE/AAV overlap syndrome. When a patient develops new symptoms that cannot be explained by the original disease, consideration should be given to whether the patient has overlapping syndrome, especially autoimmune diseases that are more likely to overlap with other autoimmune diseases. Characteristic histopathologic manifestations play an important role in the diagnosis of SLE/AAV overlap syndrome. More researches are needed to study the mechanisms of SLE/AAV overlap syndrome in order to better guide future treatments.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Jing Wang) upon request.
Ethical Approval and Consent to Participate
Written informed consent was obtained from the patient and the patient’s parents for the publication of all the images and data included in this article. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). Ethical review and approval were not required to publish the case details in accordance with the institutional requirements.
Consent to Publish
The patient provided informed consent to publish their case details and any accompanying images.
Acknowledgments
All of us thank the patient and the patient’s parents for consent to the publication of the case.
Author Contributions
Jing Wang serves as the corresponding author for this paper. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tsokos GC. Systemic lupus erythematosus. N Engl J Med. 2011;365(22):2110–2121. doi:10.1056/NEJMra1100359
2. Ameer MA, Chaudhry H, Mushtaq J, et al. An overview of Systemic Lupus Erythematosus (SLE) pathogenesis, classification, and management. Cureus. 2022;14(10):e30330. doi:10.7759/cureus.30330
3. Matusiewicz A, Stróżyńska-Byrska J, Olesińska M. Polyautoimmunity in rheumatological conditions. Int J Rheum Dis. 2019;22(3):386–391. doi:10.1111/1756-185X.13454
4. Gharwan H, Yarlagadda L, Duffy A. Acrometastasis as the initial presentation of a KRAS-positive colon cancer. Case Rep Oncol. 2012;5(2):404–408. doi:10.1159/000340011
5. Khorolsky C, Castellano A, Comstock D, Brinster NK, See SY, Garner BF. Systemic lupus erythematosus and antineutrophilic cytoplasmic antibody-associated vasculitis overlap syndrome complicated by subarachnoid hemorrhage: case-based review. Rheumatol Int. 2018;38(12):2329–2335. doi:10.1007/s00296-018-4169-z
6. Curtiss P, Liebman T, Khorolsky C, Brinster N, Beasley J, Lo Sicco K. Systemic lupus erythematosus and antineutrophil cytoplasmic antibody-associated vasculitis: an emerging overlap syndrome with cutaneous manifestations. JAAD Case Rep. 2018;4(5):493–496. doi:10.1016/j.jdcr.2018.01.021
7. Botero BJD, Bernal-Macías S, Celis PCA, et al. Systemic lupus erythematosus/ANCA-associated vasculitis overlap: an explanation for atypical lupus manifestation. Lupus. 2022;31(4):495–499. doi:10.1177/09612033221084519
8. Gladman DD, Ibañez D, Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. 2002;29(2):288–291.
9. Hervier B, Hamidou M, Haroche J, Durant C, Mathian A, Amoura Z. Systemic lupus erythematosus associated with ANCA-associated vasculitis: an overlapping syndrome? Rheumatol Int. 2012;32(10):3285–3290. doi:10.1007/s00296-011-2055-z
10. Chang SW, Kim JH. Extranodal nasal-type natural killer/T-cell lymphoma with nasal septal perforation. Ear Nose Throat J. 2022;1455613221092206. doi:10.1177/01455613221092206
11. Bains MK, Hosseini-Ardehali M. Palatal perforations: past and present. Two case reports and a literature review. Br Dent J. 2005;199(5):267–269. doi:10.1038/sj.bdj.4812650
12. Rodríguez-Reyna TS, Alarcón-Segovia D. Overlap syndromes in the context of shared autoimmunity. Autoimmunity. 2005;38(3):219–223. doi:10.1080/08916930500050145
13. Reesor E, Bhavsar SV. Overlapping systemic lupus erythematosus, seropositive erosive rheumatoid arthritis, and ANCA-associated vasculitis, a case report and literature review. 2023 Oct 7. Mod Rheumatol Case Rep. 2023;rxad056. doi:10.1093/mrcr/rxad056
14. Jarrot PA, Chiche L, Hervier B, et al. Systemic lupus erythematosus and antineutrophil cytoplasmic antibody-associated vasculitis overlap syndrome in patients with biopsy-proven glomerulonephritis. Medicine. 2016;95(22):e3748. doi:10.1097/MD.0000000000003748
15. Senda A, Sasai R, Kato K, et al. Involvement of neutrophil extracellular traps in the pathogenesis of glomerulonephritis in a case of systemic lupus erythematosus and antineutrophil cytoplasmic antibody-associated vasculitis overlap syndrome. CEN Case Rep. 2022;11(3):339–346. doi:10.1007/s13730-021-00682-y
16. Lee KH, Kronbichler A, Park DD, et al. Neutrophil extracellular traps (NETs) in autoimmune diseases: a comprehensive review. Autoimmun Rev. 2017;16(11):1160–1173. doi:10.1016/j.autrev.2017.09.012
17. Frangou E, Vassilopoulos D, Boletis J, Boumpas DT. An emerging role of neutrophils and NETosis in chronic inflammation and fibrosis in systemic lupus erythematosus (SLE) and ANCA-associated vasculitides (AAV): implications for the pathogenesis and treatment. Autoimmun Rev. 2019;18(8):751–760. doi:10.1016/j.autrev.2019.06.011
18. Hakkim A, Fürnrohr BG, Amann K, et al. Impairment of neutrophil extracellular trap degradation is associated with lupus nephritis. Proc Natl Acad Sci U S A. 2010;107(21):9813–9818. doi:10.1073/pnas.0909927107
19. van Dam LS, Kraaij T, Kamerling SWA, et al. Intrinsically distinct role of neutrophil extracellular trap formation in antineutrophil cytoplasmic antibody-associated vasculitis compared to systemic lupus erythematosus. Arthritis Rheumatol. 2019;71(12):2047–2058. doi:10.1002/art.41047
20. Nakazawa D, Shida H, Tomaru U, et al. Enhanced formation and disordered regulation of NETs in myeloperoxidase-ANCA-associated microscopic polyangiitis. J Am Soc Nephrol. 2014;25(5):990–997. doi:10.1681/ASN.2013060606
21. Fousert E, Toes R, Desai J. Neutrophil extracellular traps (NETs) take the central stage in driving autoimmune responses. Cells. 2020;9(4):915. doi:10.3390/cells9040915
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.