")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Cognitive impairment in depression: recent advances and novel treatments
Authors Perini G, Cotta Ramusino M, Sinforiani E, Bernini S, Petrachi R, Costa A
Received 28 December 2018
Accepted for publication 14 March 2019
Published 10 May 2019 Volume 2019:15 Pages 1249—1258
DOI https://doi.org/10.2147/NDT.S199746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Giulia Perini,1,2 Matteo Cotta Ramusino,1,2 Elena Sinforiani,1 Sara Bernini,1 Roberto Petrachi,3 Alfredo Costa1,2
1Center of Cognitive and Behavioral Disorders, IRCCS Fondazione Mondino, National Institute of Neurology, Pavia, Italy; 2Department of Brain and Behavior, University of Pavia, Pavia, Italy; 3Unit of Mood Disorders, Psychiatry Service, ASST, Acqui Terme, Alessandria, Italy
Abstract: In the past, little or no attention was paid to cognitive disorders associated with depression (a condition sometimes termed pseudodementia). However, recent years have seen a growing interest in these changes, not only because of their high frequency in acute-stage depression, but also because they have been found to persist, as residual symptoms (in addition to affective and psychomotor ones), in many patients who respond well to antidepressant treatment. These cognitive symptoms seem to impact significantly not only on patients’ functioning and quality of life, but also on the risk of recurrence of depression. Therefore, over the past decade, pharmacological research in this field has focused on the development of new agents able to counteract not only depressive symptoms, but also cognitive and functional ones. In this context, novel antidepressants with multimodal activity have emerged. This review considers the different issues, in terms of disease evolution, raised by the presence of cognitive disorders associated with depression and considers, particularly from the neurologist’s perspective, the ways in which the clinical approach to cognitive symptoms, and their interpretation to diagnostic and therapeutic ends, have changed in recent years. Finally, after outlining the pharmacodynamics and pharmacokinetics of the first multimodal antidepressant, vortioxetine, it reports the main results obtained with the drug in depressed patients, also in consideration of the ever-increasing evidence on its different mechanisms of action in animal models.
Keywords: depression, major depressive disorder, pseudodementia, antidepressant drugs, vortioxetine, SSRIs
Introduction
Depressive disorders, due to their prevalence, functional burden and complications, are conditions that have a substantial social impact; they also carry a considerable risk of becoming chronic. Despite this, relatively few innovative medications for the condition have been developed in recent years. It was recently reported that depression is estimated to affect more than 300 million people worldwide, with the number of cases increasing by 18% between 2005 and 2015.1 In Italy, approximately 10% of the population has had at least one episode of depression in their lifetime,2 and major depressive disorder (MDD) and dysthymic disorder have estimated prevalence rates of 10.1% and 3.4%, respectively.3 In Europe, the prevalence of depression in the elderly population (≥65 years) has been found to stand at around 10–15%,4,5 rising to 20–25% among elderly nursing home residents.6
Furthermore, with today’s widespread use of antidepressant drugs, the risk of recurrence of depressive episodes is very high, with chronic forms of depression reportedly developed by around 20% of patients affected by MDD, especially those who present residual depressive symptoms during remissions.1,7 There has also been a steady increase in antidepressant use in elderly people, especially in the “older old”.8 Selective serotonin reuptake inhibitors (SSRIs) are currently the most commonly used antidepressants, often emerging as the first-choice treatment on the basis of their efficacy and tolerability profile and ease of use. Sleep disorders and poor appetite are often the first symptoms to improve in response to pharmacological treatment, although this may apply more for tricyclic antidepressants than SSRIs. Agitation, anxiety and depressed mood are manifestations that generally improve later. Other symptoms, including asthenia, poor concentration, lack of initiative and reduced libido, tend to be less responsive to pharmacological treatment.
Among the symptoms most frequently reported, by patients and their relatives, special mention should be made of cognitive disorders, which include deficits in various domains: attention, executive functions, memory and processing speed.9,10 These disorders often tend to persist even during remission of depressive symptoms: in prevalence terms, cognitive problems in individuals affected by MDD have been reported to be “present 85–94% of the time during depressive episodes and 39–44% of the time during remissions”.7
Major depression is often associated with cognitive problems, but in some cases, this loss of higher mental function dominates the clinical picture and has a significant impact on the overall functioning of the individual concerned, giving rise to the controversial condition for decades labeled pseudodementia.
Cognitive symptoms of depression and the concept of pseudodementia
The term pseudodementia was coined by Kiloh in 1961.11 Since then, it has been used, rather loosely, to describe cognitive deficits occurring in depression, especially in the elderly, and no meaningful attempt has been made to set its characteristics within a nosographic framework. Indeed, over time, the condition has continued to be poorly characterized neuropsychologically, and it has never been properly integrated into the currently used dementia classification systems.12 In the 1980s, it was included among the reversible or treatable “subcortical” forms of dementia, together with, for example, normotensive hydrocephalus and metabolic dementia.13 Subsequently, various attempts were made to redefine the condition; according to one of these, pseudodementia is cognitive impairment of the dementia type that correlates positively with unipolar affective (mood) disorders, previous mood disorders and favorable outcomes, and negatively with non-depressive conditions and confusion disorders.14
In the 1990s, however, it became more apparent that a depressive state associated with cognitive impairment can be the prodromal stage of dementia that is actually irreversible.15 In this regard, a more recent meta-analysis study found depression to be associated with a twofold increased risk of developing dementia.16 Along the same lines, an observational study found that over a period of at least five years, more than 70% of elderly patients initially presenting with pseudodementia converted to overt dementia, as opposed to 18% of subjects initially defined cognitively intact. These findings indicate that cognitive impairment in elderly individuals with moderate-to-severe depression is a strong predictor of dementia.17 Over the years, there has been increasing criticism of the term pseudodementia from authors who, on the basis of their clinical experience, consider it to be redundant and misleading, given that a complete history and thorough clinical examination of the patient are usually sufficient to establish a diagnosis.18 More recently, some authors have even stated that, among the “very old”, the presence of cognitive disorders in patients with depression, including those with a lifetime history of mood disorders, almost always indicates an incipient dementia process and should prompt the specialist to start an appropriate diagnostic and therapeutic workup for dementia.19 Furthermore, the DSM-V20 identifies cognitive disorders as core symptoms of depression and includes several (difficulty thinking and concentrating and/or making decisions) among the diagnostic criteria for MDD. Although the DSM-V acknowledges, in its commentary, that disorders of the cognitive sphere—particularly those involving memory—can persist following improvement or remission of depressive symptoms, and therefore be interpreted as the initial presentation of dementia, a definition of “reversible dementia caused by psychiatric illness” is not yet contemplated as a formal diagnostic category, contrary to what some authors recommend.21 On the other hand, it should always be remembered that, in depressed patients, reversible cognitive deficits can sometimes coexist with irreversible ones, and thus with true dementia.22
It is now recognized, on the basis of observations and scientific evidence, that cognitive disorders are a core feature of the clinical picture of depression and should not be considered merely secondary to it; moreover, they are among the main causes of functional impairment in depressed patients. Cognitive symptoms should therefore be regarded as a partially independent dimension of MDD, and an important target of any treatment that is initiated.23
Differential diagnosis: the neurologist’s perspective
In clinical practice, it is extremely difficult to distinguish, early on, between cognitive impairment (degenerative or vascular) that is destined to advance and depression-related cognitive impairment that can be reversed. Although various features have been identified to help support this differential diagnostic process (Table 1), on their own they are insufficient. Nevertheless, in recent years, there have been several interesting developments in this field. For example, it has been observed that on certain neuropsychological tests (the clock-drawing test, Stroop test, the Boston Naming Test and above all facial recognition tests, like the Benton Facial Recognition Test), the performances of patients with Alzheimer’s disease (AD) differ significantly from those of patients with pseudodementia, who, moreover, do not show the reduced left hippocampal volume that instead characterizes patients with AD.24 However, it is widely felt that the use of neuropsychological tests alone (the traditional ones at least) does not allow good diagnostic definition,25 and indeed neurologists now have at their disposal other tools (in addition to neuropsychological tests) that can be applied at increasingly early stages to assist in the diagnostic workup of dementia (degenerative forms at least), namely biological disease markers.
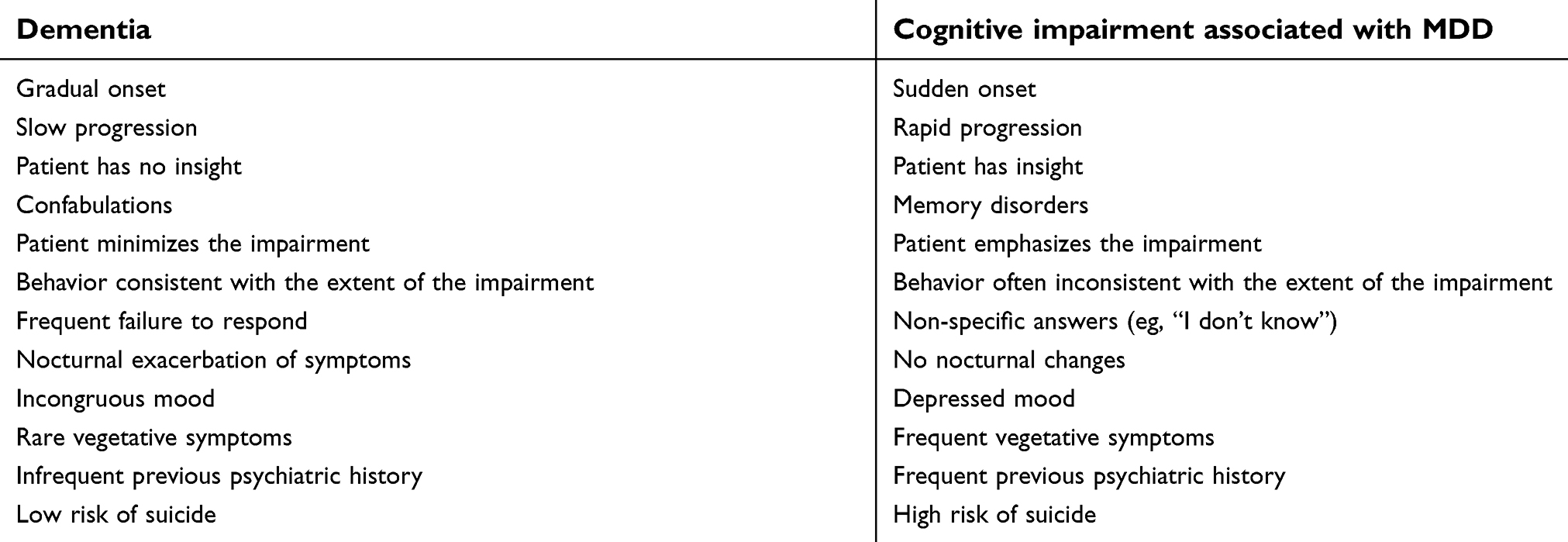 | Table 1 Anamnestic and clinical features distinguishing dementia from cognitive impairment associated with major depressive disorder (MDD) (“pseudodementia”) |
A diagnosis of dementia based on the DSM-V criteria still requires the presence of a deficit in one or more cognitive domains, severe enough to interfere with social functioning, work functioning or activities of daily living.26 Developed on the basis of a probabilistic approach, the NINCDS-ADRDA diagnostic criteria,27 the first to be developed for AD, distinguished between three clinical forms of AD: probable, possible and definite. Probable AD was defined by the presence of a progressive worsening both of memory and of another cognitive function, onset between 40 and 90 years of age (most commonly after the age of 65), and the absence of consciousness and other systemic or cerebral disorders that might account for the decline. Patients showing atypical features in the natural history of the disease (its onset, clinical presentation or course), or disorders that can give rise to dementia, could only be assigned a diagnosis of possible AD. Finally, only histopathological examination, confirming the presence of the characteristic brain lesions, could provide diagnostic certainty and thus allow a diagnosis of definite AD. Over time, this clinical-neuropathological approach, together with the absence of clinical and biological criteria allowing the identification of other forms of dementia, resulted in low diagnostic specificity for AD (23–88%).27 In fact, the NINCDS-ADRDA criteria can also be met by patients affected by various other forms of cognitive decline, such as frontotemporal dementia, corticobasal degeneration, diffuse Lewy Body disease and vascular dementia. However, in more recent years, thanks to the development of more precise histopathological definitions, a growing understanding of the pathophysiological processes underlying the disease, and the availability of in vivo biomarkers of disease, the foundations were laid for the formulation of new diagnostic criteria, which marked the transition from the old (clinical-neuropathological) approach to a new (clinical-biological) one. Indeed, according to the revised criteria developed by the International Working Group (IWG) in 2007,28 AD can be identified in vivo, regardless of the degree of cognitive impairment, by the presence of a typical phenotype (a progressive disorder of episodic memory referred to as amnestic syndrome of the hippocampal type, ie, characterized mainly by recall deficits not normalized by cueing) together with at least one disease biomarker (medial temporal lobe atrophy on MRI, changes in the levels of Aβ or tau protein in the CSF, amyloid-positive PET scan or metabolic changes on FDG-PET). This new vision of the disease had two important effects: (1) it eliminated the concept of possible AD, which is incompatible with the new, highly specific, criteria for AD, and (2) it extended the diagnosis to include the prodromal stage, understood as the presence of amnestic mild cognitive impairment supported by neurobiological markers.
The real advantage of these criteria seems to lie in their applicability to all the stages along the disease continuum. However, they also have limitations, such as their failure to take into account atypical AD and mixed AD, and the fact that all the biomarkers are assigned equal weight. A revised version of the IWG criteria29 suggests that only the pathophysiological biomarkers (and not the topographical ones) should be used in the diagnostic workup. Table 2 shows these diagnostic criteria: notably, they state that typical AD can only be diagnosed if major depression has been excluded.
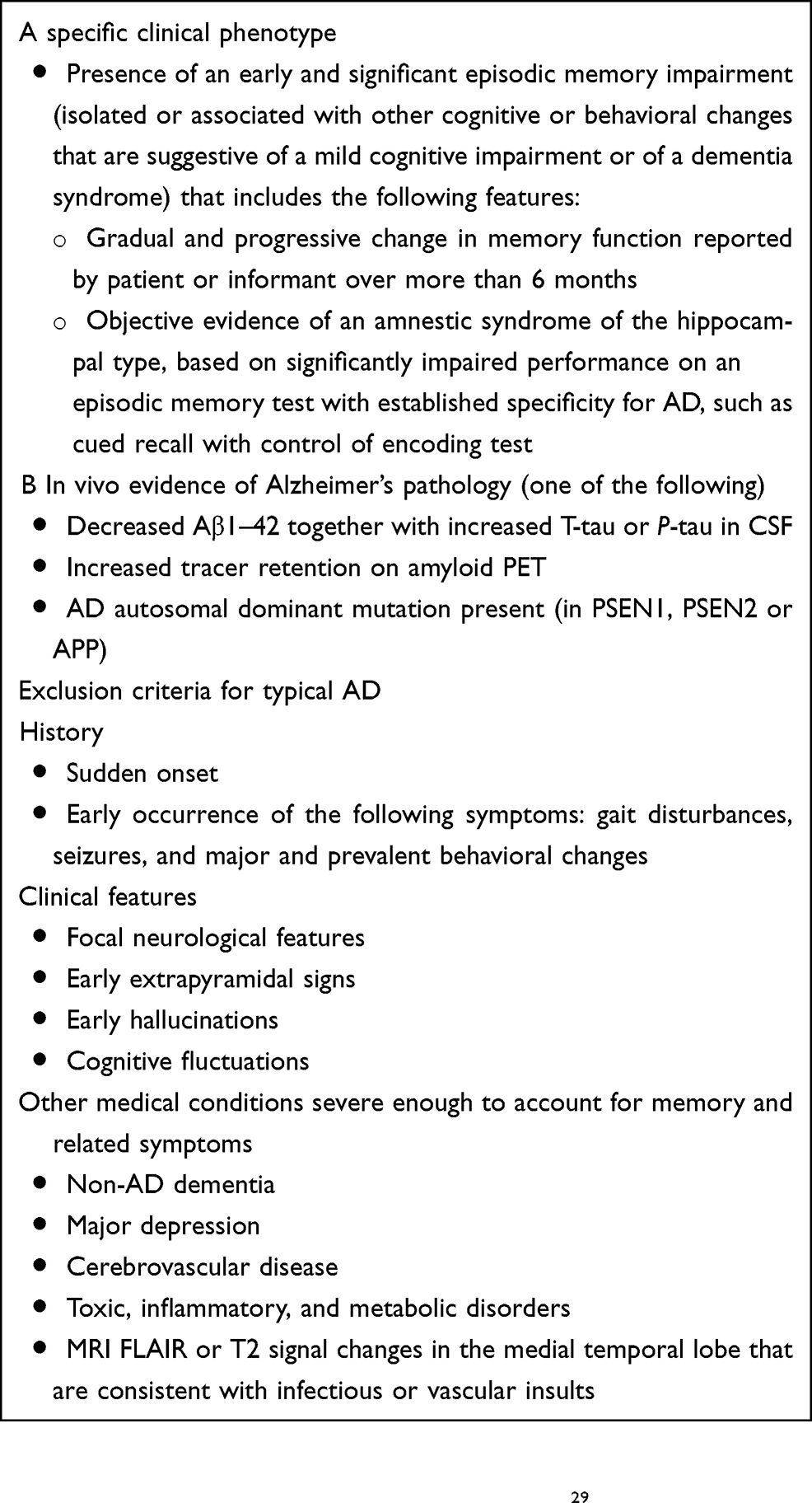 | Table 2 IWG-2 criteria for typical Alzheimer’s disease (AD) (A plus B at any stage) |
The above considerations show that the most complex cases of association between cognitive disorders and depression can already be addressed using methods that allow early differential diagnosis between reversible forms of cognitive impairment and degenerative dementias. Conversely, despite significant advances in neuroscience, no widely accepted biomarkers are available to help diagnostics or identify preferred treatments for individuals with MDD. Neuroimaging has substantially contributed to understanding the putative neuronal mechanisms involved in depression as well as cognitive impairments in depressed individuals. Morphological, functional and molecular approaches have been used. Voxel-based morphometry and diffusion tensor imaging DTI studies have shown alterations in the anterior cingulate cortex, frontal cortex, insula, thalamus, hippocampus and in the prefrontal white matter, right solitary fasciculus, corpus callosum, inferior fronto-occipital fasciculus and left superior longitudinal fasciculus.30 fMRI has shown aberrant functional connectivity in the salience network (predominantly consisting of the anterior insular cortex and dorsal anterior cingulate cortex) and in the cognitive control network (dorsolateral prefrontal cortex and pregenual anterior cingulate cortex), as well as hyperactivity in the default mode network (posterior cingulate cortex, medial prefrontal cortex, precuneus and temporo-parietal cortices) and in the affective network (amygdala and the subgenual and pregenual cingulate).30 However, little evidence is available on an association of regional changes in brain function and cognitive deficits in MDD. Serotonergic system involved in MDD can be investigated with novel molecular tracers. Depressed individuals show an increased uptake on 11C-WAY-100635 (a 5-HT1A autoinhibitory receptor antagonist) PET, an indirect evidence of low 5-HT release and a decreased uptake on 4-[18F]-ADAM (a highly selective radiotracer for assessing SERT availability) PET.31 Recently, both fMRI and molecular neuroimaging have been used to evaluate the therapeutic effect of a panoply of treatments in MDD, as will be further pointed out.
New pharmacological approaches: vortioxetine
Evidence has emerged in recent years that the underlying cause of depression lies in dysfunctions not only of the known aminergic neurotransmitter systems, but also of other circuits, such as the glutamatergic ones; similarly, the role of other pathogenetic mechanisms, such as loss of synaptic plasticity in areas involved in regulation of emotion and affect, has increasingly been clarified as well.32 This has led to a growing interest in new molecules able to interfere with these systems and mechanisms, known to be involved in cognitive processes. However, the currently available antidepressant drugs have never been shown to have any efficacy on cognitive disorders.33 In recent years, vortioxetine has emerged as an agent capable of acting on the serotonergic system through a peculiar mechanism of action, completely different to those characterizing the previously available therapeutic options. Having being shown, both in various animal models and in clinical trials, to improve cognitive performance, in 2013, this drug, which has a distinctive pharmacological profile, was approved in the European Union and in the USA for the treatment of MDD in adults. In 2015, the European Medicines Agency updated its data on the clinical efficacy of vortioxetine, stating that its effects include effects on cognitive and global functioning (to date, it remains the only antidepressant to which this applies).
Pharmacodynamic features
Most psychotropic drugs have a single mechanism of action, ie, they act on multiple targets but in the same way. For example, some of the more recent antidepressants block more than one transporter. Conversely, there are few drugs that act on different targets through more than one mechanism of action. Vortioxetine is an example of this latter category of molecules, termed “multimodal”: indeed, as well as inhibiting serotonin (5-HT) reuptake mediated by the serotonin reuptake transporter (SERT) protein, it also modulates the activity of other serotonin (5-HT) receptors.34 Figure 1 shows three of its mechanisms of action:
- inhibition of a transporter (in this case, SERT);
- various actions on different G protein-coupled receptors (ie, an agonist action on 5-HT1A receptors, a partial agonist action on 5-HT1B receptors, an antagonist action on 5-HT1D and 5-HT7 receptors);
- an antagonist action on a ligand-dependent ion channel (ie, the 5-HT3 receptor).
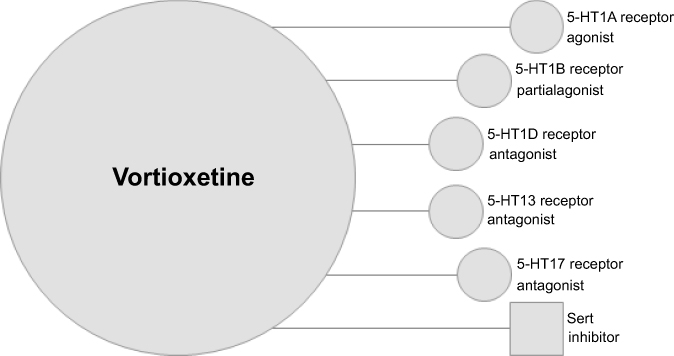 | Figure 1 Multimodal mechanism of action of vortioxetine. |
The 5-HT1A, 5-HT1B and 5-HT1D receptors are located at presynaptic sites, while only the 5-HT7 receptor is located postsynaptically. Serotonergic neurons are well known to self-regulate their activity through the 5-HT transporters at presynaptic nerve terminals; inhibition of these transporters is the mode of action of SSRIs. When SERT proteins are inhibited, the amount of 5-HT in the synaptic cleft increases. However, the quantity of 5-HT released is regulated in an inhibitory manner by negative feedback mechanisms, mediated predominantly by presynaptic 5-HT1A receptors. This mechanism is thought to underlie the long-term desensitization of SSRIs and the restriction of their capacity to increase the amount of 5-HT they release.35 Preclinical studies suggest that simultaneous stimulation of 5-HT1A autoreceptors and inhibition of SERT proteins accelerates the desensitization of 5-HT1A receptors and increases the release of 5HT.36 There exist various rationales supporting the procognitive potential of vortioexitine. For example, 5-HT3 receptor antagonists, such as ondansetron, can counteract deficits in the retrieval of spatial (episodic) and fear-related memory in animal models of depression and cognitive dysfunction.37
Pharmacokinetic aspects
Studies have shown that vortioxetine possesses a linear pharmacokinetic profile.38 Administered orally, it has a bioavailability of approximately 75%, irrespective of food intake. It shows high (98%) plasma protein binding, which does not seem to differ between healthy individuals and those with hepatic or renal insufficiency. Its plasma concentration peaks at between 7 and 11 hrs after oral administration, and it has a plasma half-life ranging from 57 to 66 hrs. Its apparent distribution volume is approximately 2,600 L, indicating that it is a lipophilic compound that shows extensive extravascular distribution. The pharmacological activity of vortioxetine is due to the unmodified molecule. The drug is largely metabolized in the liver. Various cytochrome p450 isozymes (CYP2D6, CYP3A4/5, CYP2C19, CYP2C9, CYP2A6, CYP2C8 and CYP2B6) are involved in its metabolism. CYP2D6 is the primary enzyme responsible for converting the drug into its inactive metabolite. Slow CYP2D6 metabolizers have been found to show vortioxetine levels twofold greater than those of rapid metabolizers.39 Around 59% of inactive metabolites are excreted in urine and 26% in feces. Only negligible amounts of active vortioxetine are excreted in feces.
Animal studies
Vortioxetine, due to its effects on serotonin receptors, has been reported to prevent learning and memory deficits induced by central serotonin depletion and stress in rats,40,41 and to have positive effects on the modulation of circadian rhythms and episodic memory in rodents.42 But the effects of the drug should not be viewed only in the context of “microcircuits” (or synapses) between presynaptic serotonergic neurons and postsynaptic sites; however, these neurons are also part of “macrocircuits” within a neural network (connectome) that links together huge numbers of cells. The activity inside this connectome explains the drug’s indirect effects on other neurotransmitter systems. It is particularly interesting to note that prolonged administration of vortioxetine results in increased extracellular levels of noradrenaline in the medial prefrontal cortex and hippocampus, whereas its acute administration facilitates dopamine, histamine and acetylcholine release in different brain areas.43 Moreover, it should be underlined that although vortioxetine induces increased dopamine levels in the brain areas involved in higher cognitive functions, it does not induce changes associated with abuse potential, given that it does not increase dopamine levels or the firing frequency of dopaminergic neurons in the nucleus accumbens.44 Vortioxetine’s 5-HT3 receptor antagonism is also thought to inhibit the activity of GABAergic interneurons (per se inhibitors) on pyramidal neurons and thus to trigger increased release of glutamate by the latter.45,46
With reference to what has already been said about the new mechanisms suggested to be involved in the pathogenesis of depression, several studies have reported that vortioxetine can play a significant role in neuronal plasticity, through the development of dendritic spines and the formation of new synaptic contacts.47,48 Indeed, the drug has been shown, in adult rats, to stimulate neurogenesis and thus hippocampal plasticity49 and, through these mechanisms, to improve context discrimination (CD) in a laboratory mouse model.50 However, a similar effect of vortioxetine in CD could involve mechanisms unrelated to neurogenesis.51 A role could also be played by increased release of the brain-derived neurotrophic factor in the hippocampus, a phenomenon that vortioxetine appeared to induce in an experimental model of depression (chronic unpredictable mild stress in rats).52
Studies in humans
In 2013, vortioxetine was approved for the treatment of MDD in adults, at doses of between 5 and 20 mg/day (recommended starting dose, 10 mg/day for the under-65s and 5 mg/day for patients aged over 65 years). This is currently its only approved indication. The effectiveness (both short- and long-term) of vortioxetine has been demonstrated in numerous double-blind randomized controlled clinical trials, subsequently supported by meta-analyses. In 2017, a Cochrane systematic review53 showed vortioxetine to be more effective than placebo in terms of response and clinical remission. However, it was pointed out that, in the absence of a comparison with SSRIs, the clinical significance of these effects remains uncertain. On the other hand, indirect comparison with serotonin-noradrenaline reuptake inhibitors (SNRIs) failed to show any advantage of vortioxetine, other than a lower number of side effects. In both these studies, vortioxetine was found to improve cognitive performances.54 In three large randomized controlled studies in adults with recurrent MDD, short-term treatment with vortioxetine was associated with improved performances on the Digit Symbol Substitution Test and the Rey Auditory Verbal Learning Test, two objective assessment tools that cover a wide range of cognitive domains, including executive function, attention, processing speed, learning and memory.55–57 The improvements observed on these measures were, in most cases, largely independent of the improvements shown in depressive symptoms. Furthermore, in another study, conducted in perimenopausal and early postmenopausal women, vortioxetine was found to improve depression as well as other symptoms, including cognitive ones, associated with this stage in female reproductive life.58 More recently, vortioxetine 10–20 mg per day was found to be effective and well tolerated; the treatment was associated with improved performances on the Perceived Deficits Questionnaire, but not the Cognitive and Physical Functioning Questionnaire—these are two subjective measures of cognitive function—and it produced a significant and clinically meaningful improvement in performance on the University of California San Diego Performance-Based Skills Assessment, an objective measure of functional capacity.59 Finally, in humans, two PET studies have been conducted using 5-HT transporter ligands (11C-MADAM or 11C-DASB) to quantify the 5-HT transporter occupancy in the brain across different dose levels. The mean 5-HT transporter occupancy in the raphe nuclei was approximately 50% at 5 mg/day and 65% at 10 mg/day and increased to above 80% at 20 mg/day.60,61
Safety and tolerability
Overall, the current literature shows vortioxetine to have a good safety and tolerability profile.62,63 Adverse events are reported by approximately 5% of patients in short- and long-term clinical trials. Nausea is the most frequent adverse event; generally of mild-to-moderate severity, it is commonly observed within one week of starting the treatment. This is an interesting finding in view of the drug’s 5-HT3 antagonist activity. Dizziness, insomnia and nausea are more frequently reported at higher doses. Sexual dysfunction is reported in between 1% and 1.8% of cases. Among severe adverse events, suicide-related events are reported in 0.4% of cases (similarly to placebo). Vortioxetine is not associated with any clinically relevant changes in laboratory test results, even though elderly patients, and patients taking diuretics are at risk of developing hyponatremia during treatment. Similarly, the drug has not been found to significantly affect weight, blood pressure, heart rate or ECG variables.64 While the efficacy of vortioxetine is comparable to that of other antidepressents (duloxetine, escitalopram, levomilnacipran, sertraline, venlafaxine, vilazodone), its tolerability, evaluated on the basis of discontinuation of the treatment because of an adverse event, is different; indeed, vortioxetine treatment is five times more likely than placebo treatment to be associated with a clinical response rather than discontinuation due to an adverse event.65
Conclusions and future perspectives
Cognitive disorders are now widely acknowledged to be a transnosological category represented in many developmental mental disorders (ADHD, schizophrenia, and also MDD). To date, however, studies on antidepressants have almost always treated cognitive impairment as a secondary end point. Instead, cognitive function should be a critical target of therapy in patients with MDD; in fact, a large European longitudinal study involving 1,159 patients (PERFORM) showed that mental health-related quality of life in MDD is significantly low due to the severity of the depressive symptoms, but also of the cognitive impairment displayed by these patients.66 We are thus seeing a change of emphasis in clinical research in this field, with future clinical trials necessarily including cognitive improvements among the primary end points. Future studies will need to involve observation of larger patient populations, over longer periods of time. Indeed, as mentioned, many patients whose MDD is in remission continue to show residual cognitive deficits, which can have a major impact on their functional outcome.
Overall, as shown by the currently available literature (specifically, ad hoc designed studies with cognitive outcome as the primary end point), vortioxetine is the first antidepressant drug with proven efficacy in improving cognitive symptoms of depression. Furthermore, it is the only antidepressant agent, among those to date evaluated, showing relatively strong evidence of a positive effect on multiple cognitive domains; for others (SSRIs, SNRIs and bupropione), on the other hand, the available evidence is still relatively weak.67
Furthermore, with regard to the methodological approach adopted in studies on vortioxetine and any new drugs with a similar profile, it will be important to identify a more suitable battery of tests for depressed patients, in order to minimize the possible discrepancies between studies. Indeed, the currently used neuropsychological tests do not seem to lend themselves adequately to these patients25,68 for a series of reasons, such as their inability to detect under ecological conditions the true effect of cognitive impairment in patients’ daily lives, and the fact that they are often self-administered measures, and thus poorly overlap with objective cognitive assessment tools.
It is nevertheless comforting to note the findings of a recent survey, which showed that Italian psychiatrists regard cognitive impairment as an important dimension of MDD and that cognitive symptoms were the most frequently cited symptoms when evaluating patients’ possible return to work and risk of recurrent depression.69 It should be noted, however, that although 70% of specialists claim that the presence of cognitive symptoms influences their subsequent therapeutic decisions, this is not always objectively confirmed in clinical practice.
From the neurologist’s perspective, since the efficacy of vortioxetine may extend beyond patients with depression, it would clearly be worth exploring its procognitive action—this implies excluding a pseudospecific effect of the drug—in those clinical models that are currently at the center of clinical research, ie, patients in the very early stages of cognitive impairment, and who are biologically well-defined, thanks to the use of degenerative dementia biomarkers.
Acknowledgment
Payments of only open access publication fees for this paper were sustained by Lundbeck, Italy.
Disclosure
The authors report no conflicts of interest in this work.
References
1.
2. Battaglia A, Dubini A, Mannheimer R, Pancheri P. Depression in the Italian community: epidemiology and socio-economic implications. Int Clin Psychopharmacol. 2004;19:135–142.
3. de Girolamo G, Polidori G, Morosini P, et al. Prevalence of common mental disorders in Italy, risk factors, health status, and utilization of health services: the ESEMeD-WMH project. Epidemiol Psichiatr Soc. 2005;14:1–100.
4. Castro-Costa E, Dewey M, Stewart R, et al. Prevalence of depressive symptoms and syndromes in later life in ten European countries: the SHARE study. Br J Psychiatry. 2007;191:393–401. doi:10.1192/bjp.bp.107.036772
5. Copeland JR, Beekman AT, Dewey ME, et al. Depression in Europe. Geographical distribution among older people. Br J Psychiatry. 1999;174:312–321.
6. Rovner BW, German PS, Brant LJ, Clark R, Burton L, Folstein MF. Depression and mortality in nursing homes. JAMA. 1991;265(8):993–996.
7. Conradi HJ, Ormel J, de Jonge P. Presence of individual (residual) symptoms during depressive episodes and periods of remission: a 3-year prospective study. Psychol Med. 2011;41(6):1165–1174. doi:10.1017/S0033291710001911
8. Sonnenberg CM, Deeg DJ, Comijs HC, van Tilburg W, Beekman ATF. Trends in antidepressant use in the older population: results from the LASA-study over a period of 10 years. J Affect Disord. 2008;111(2–3):299–305. doi:10.1016/j.jad.2008.03.009
9. McIntyre RS, Xiao HX, Syeda K, et al. The prevalence, measurement, and treatment of the cognitive dimension/domain in major depressive disorder. CNS Drugs. 2015;29(7):577–589. doi:10.1007/s40263-015-0263-x
10. Millan MJ, Agid Y, Brüne M, et al. Cognitive dysfunction in psychiatric disorders: characteristics, causes and the quest for improved therapy. Nat Rev Drug Discov. 2012;11(2):141–168. doi:10.1038/nrd3628
11. Kiloh LG. Pseudo-dementia. Acta Psychiatr Scand. 1961;37:336–351. doi:10.1111/acp.1961.37.issue-4
12. Kang H, Zhao F, You L, et al. Pseudo-dementia: a neuropsychological review. Ann Indian Acad Neurol. 2014;17(2):147–154. doi:10.4103/0972-2327.132613
13. Mahendra B. Depression and dementia: the multi-faceted relationship. Psychol Med. 1985;15:227–236. doi:10.1017/S0033291700023503
14. Bulbena A, Berrios GE. Pseudodementia: facts and figures. Br J Psychiatry. 1986;148:87–94. doi:10.1192/bjp.148.1.87
15. Alexopoulos GS, Meyers BS, Young RC, et al. The course of geriatric depression with “reversible dementia”: a controlled study. Am J Psychiatry. 1993;150(11):1693–1699. doi:10.1176/ajp.150.11.1693
16. Ownby RL, Crocco E, Acevedo A, John V, Loewenstein D. Depression and risk for Alzheimer disease: systematic review, meta-analysis, and metaregression analysis. Arch Gen Psychiatry. 2006;63(5):530–538. doi:10.1001/archpsyc.63.5.530
17. Sáez-Fonseca JA, Lee L, Walker Z. Long-term outcome of depressive pseudodementia in the elderly. J Affect Disord. 2007;101:123–129. doi:10.1016/j.jad.2006.11.004
18. Lovestone S. Alzheimer’ s disease and other dementias (including pseudodementias). In: David AS, Fleminger S, Kopelman MD, Lovestone S, Mellers JDC, editors. Lishman’s Organic Psychiatry: A Textbook of Neuropsychiatry.
19. Heser K, Bleckwenn M, Wiese B, et al. Late-life depressive symptoms and lifetime history of major depression: cognitive deficits are largely due to incipient dementia rather than depression. J Alzheimers Dis. 2016;54(1):185–199. doi:10.3233/JAD-160209
20.
21. Rabins PV, Lyketsos CG. A commentary on the proposed DSM revision regarding the classification of cognitive disorders. Am J Geriatr Psychiatry. 2011;19:201–204. doi:10.1097/JGP.0b013e3182051ac7
22. McAllister TW, Price TR. Severe depressive pseudodementia with and without dementia. Am J Psychiatry. 1982;139:626–629. doi:10.1176/ajp.139.5.626
23. Miskowiak KW, Ott CV, Petersen JZ, Kessing LV. Systematic review of randomized controlled trials of candidate treatments for cognitive impairment in depression and methodological challenges in the field. Eur Neuropsychopharmacol. 2016;26(12):1845–1867. doi:10.1016/j.euroneuro.2016.09.641
24. Sahin S, Okluoglu Önal T, Cinar N, Bozdemir M, Çubuk R, Karsidag S. Distinguishing depressive pseudodementia from Alzheimer disease: a comparative study of hippocampal volumetry and cognitive tests. Dement Geriatr Cogn Dis Extra. 2017;7(2):230–239. doi:10.1159/000477759
25. McIntyre RS, Cha DS, Soczynska JK, et al. Cognitive deficits and functional outcomes in major depressive disorder: determinants, substrates, and treatment interventions. Depress Anxiety. 2013;30:515–527. doi:10.1002/da.22063
26. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939–944.
27. Varma AR, Snowden JS, Lloyd JJ, Talbot PR, Mann DM, Neary D. Evaluation of the NINCDS-ADRDA criteria in the differentiation of Alzheimer’s disease and frontotemporal dementia. J Neurol Neurosurg Psychiatry. 1999;66(2):184–188.
28. Dubois B, Feldman HH, Jacova C, et al. Research criteria for the diagnosis of Alzheimer’s disease: revising the NINCDS-ADRDA criteria. Lancet Neurol. 2007;6(8):734–746. doi:10.1016/S1474-4422(07)70178-3
29. Dubois B, Feldman HH, Jacova C, et al. Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. Lancet Neurol. 2014;13(6):614–629. doi:10.1016/S1474-4422(14)70090-0
30. Zhang K, Zhu Y, Zhu Y, et al. Molecular, functional, and structural imaging of major depressive disorder. Neurosci Bull. 2016;32(3):273–285. doi:10.1007/s12264-016-0030-0
31. Huang M, Lu S, Yu L, et al. Altered fractional amplitude of low frequency fluctuation associated with cognitive dysfunction in first-episode drug-naïve major depressive disorder patients. BMC Psychiatry. 2017;17(1):11. doi:10.1186/s12888-017-1489-6
32. Kavalali ET, Monteggia LM. Synaptic mechanisms underlying rapid antidepressant action of ketamine. Am J Psychiatry. 2012;169(11):1150–1156. doi:10.1176/appi.ajp.2012.12040531
33. McIntyre RS. Using measurement strategies to identify and monitor residual symptoms. J Clin Psychiatry. 2013;74(Suppl. 2):14–18. doi:10.4088/JCP.12084su1c.03
34. Bang-Andersen B, Ruhland T, Jørgensen M, et al. Discovery of 1-[2-(2,4-dimethylphenylsulfanyl)phenyl]piperazine (Lu AA21004): a novel multimodal compound for the treatment of major depressive disorder. J Med Chem. 2011;54(9):3206–3221. doi:10.1021/jm101459g
35. Stahl SM. Modes and nodes explain the mechanism of action of vortioxetine, a multimodal agent (MMA): enhancing serotonin release by combining serotonin (5HT) transporter inhibition with actions at 5HT receptors (5HT1A, 5HT1B, 5HT1D, 5HT7 receptors). CNS Spectr. 2015;20(2):93–97. doi:10.1017/S1092852915000139
36. Assié M-B, Lomenech H, Ravailhe V, Faucillon V, Newman-Tancredi A. Rapid desensitization of somatodendritic 5-HT1A receptors by chronic administration of the high-efficacy 5-HT1A agonist, F13714: a microdialysis study in the rat. Br J Pharmacol. 2006;149(2):170–178. doi:10.1038/sj.bjp.0706859
37. Roychoudhury M, Kulkarni SK. Effects of ondansetron on short-term memory retrieval in mice. Methods Find Exp Clin Pharmacol. 1997;19(1):43–46.
38. Areberg J, Søgaard B, Højer A-M. The clinical pharmacokinetics of Lu AA21004 and its major metabolite in healthy young volunteers. Basic Clin Pharmacol Toxicol. 2012;111(3):198–205. doi:10.1111/j.1742-7843.2012.00886.x
39. Hvenegaard MG, Bang-Andersen B, Pedersen H, Jørgensen M, Püschl A, Dalgaard L. Identification of the cytochrome P450 and other enzymes involved in the in vitro oxidative metabolism of a novel antidepressant, Lu AA21004. Drug Metab Dispos. 2012;40(7):1357–1365. doi:10.1124/dmd.112.044610
40. Jensen JB, Du Jardin KG, Song D, et al. Vortioxetine, but not escitalopram or duloxetine, reverses memory impairment induced by central 5-HT depletion in rats: evidence for direct 5-HT receptor modulation. Eur Neuropsychopharmacol. 2014;24(1):148–159. doi:10.1016/j.euroneuro.2013.10.011
41. Wallace A, Pehrson AL, Sánchez C, Morilak DA. Vortioxetine restores reversal learning impaired by 5-HT depletion or chronic intermittent cold stress in rats. Int J Neuropsychopharmacol. 2014;17(10):1695–1706. doi:10.1017/S1461145714000571
42. Westrich L, Haddjeri N, Dkhissi-Benyahya O, Sánchez C. Involvement of 5-HT₇ receptors in vortioxetine‘s modulation of circadian rhythms and episodic memory in rodents. Neuropharmacology. 2015;89:382–390. doi:10.1016/j.neuropharm.2014.10.015
43. de Bartolomeis A, Fagiolini A, Maina G. Vortioxetine in the treatment of major depression. Riv Psichiatr. 2016;51(6):215–230. doi:10.1708/2596.26720
44. Pehrson AL, Cremers T, Bétry C, et al. Lu AA21004, a novel multimodal antidepressant, produces regionally selective increases of multiple neurotransmitters – a rat microdialysis and electrophysiology study. Eur Neuropsychopharmacol. 2013;23(2):133–145. doi:10.1016/j.euroneuro.2012.04.006
45. Sanchez C, Asin KE, Artigas F. Vortioxetine, a novel antidepressant with multimodal activity: review of preclinical and clinical data. Pharmacol Ther. 2015;145:43–57. doi:10.1016/j.pharmthera.2014.07.001
46. Bétry C, Pehrson AL, Etiévant A, Ebert B, Sánchez C, Haddjeri N. The rapid recovery of 5-HT cell firing induced by the antidepressant vortioxetine involves 5-HT(3) receptor antagonism. Int J Neuropsychopharmacol. 2013;16(5):1115–1127. doi:10.1017/S1461145712001058
47. Chen F, du Jardin KG, Waller JA, Sanchez C, Nyengaard JR, Wegener G. Vortioxetine promotes early changes in dendritic morphology compared to fluoxetine in rat hippocampus. Eur Neuropsychopharmacol. 2016;26(2):234–245. doi:10.1016/j.euroneuro.2015.12.018
48. Waller JA, Chen F, Sánchez C. Vortioxetine promotes maturation of dendritic spines in vitro: a comparative study in hippocampal cultures. Neuropharmacology. 2016;103:143–154. doi:10.1016/j.neuropharm.2015.12.012
49. Bétry C, Etiévant A, Pehrson A, Sánchez C, Haddjeri N. Effect of the multimodal acting antidepressant vortioxetine on rat hippocampal plasticity and recognition memory. Prog Neuropsychopharmacol Biol Psychiatry. 2015;58:38–46. doi:10.1016/j.pnpbp.2014.12.002
50. Guilloux J-P, Mendez-David I, Pehrson A, et al. Antidepressant and anxiolytic potential of the multimodal antidepressant vortioxetine (Lu AA21004) assessed by behavioural and neurogenesis outcomes in mice. Neuropharmacology. 2013;73:147–159. doi:10.1016/j.neuropharm.2013.05.014
51. Felice D, Guilloux J-P, Pehrson A, et al. Vortioxetine improves context discrimination in mice through a neurogenesis independent mechanism. Front Pharmacol. 2018;9:204. doi:10.3389/fphar.2018.00204
52. Lu Y, Ho CS, McIntyre RS, Wang W, Ho RC. Effects of vortioxetine and fluoxetine on the level of brain derived neurotrophic factors (BDNF) in the hippocampus of chronic unpredictable mild stress-induced depressive rats. Brain Res Bull. 2018;142:1–7. doi:10.1016/j.brainresbull.2018.06.007
53. Koesters M, Ostuzzi G, Guaiana G, et al. Vortioxetine for depression in adults. Cochrane Database Syst Rev. 2017;7:CD011520. doi:10.1002/14651858.CD003881.pub4
54. Frampton JE. Vortioxetine: a review in cognitive dysfunction in depression. Drugs. 2016;76(17):1675–1682. doi:10.1007/s40265-016-0655-3
55. McIntyre RS, Lophaven S, Olsen CK. A randomized, double-blind, placebo-controlled study of vortioxetine on cognitive function in depressed adults. Int J Neuropsychopharmacol. 2014;17(10):1557–1567. doi:10.1017/S1461145714000546
56. Mahableshwarkar AR, Zajecka J, Jacobson W, Chen Y, Keefe RS. A randomized, placebo-controlled, active-reference, double-blind, flexible-dose study of the efficacy of vortioxetine on cognitive function in major depressive disorder. Neuropsychopharmacology. 2016;41(12):2961. doi:10.1038/npp.2016.181
57. Katona C, Hansen T, Olsen CK. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Int Clin Psychopharmacol. 2012;27(4):215–223. doi:10.1097/YIC.0b013e3283542457
58. Freeman MP, Cheng LJ, Moustafa D, et al. Vortioxetine for major depressive disorder, vasomotor, and cognitive symptoms associated with the menopausal transition. Ann Clin Psychiatry. 2017;29(4):249–257.
59. Mahableshwarkar AR, Zajecka J, Jacobson W, Chen Y, Keefe RS. A randomized, placebo-controlled, active-reference, double-blind, flexible-dose study of the efficacy of vortioxetine on cognitive function in major depressive disorder. Neuropsychopharmacology. 2015;40(8):2025–2037. doi:10.1038/npp.2015.52
60. Areberg J, Luntang-Jensen M, Søgaard B, Nilausen DØ. Occupancy of the serotonin transporter after administration of Lu AA21004 and its relation to plasma concentration in healthy subjects. Basic Clin Pharmacol Toxicol. 2012;110(4):401–404. doi:10.1111/j.1742-7843.2011.00810.x
61. Stenkrona P, Halldin C, Lundberg J. 5-HTT and 5-HT(1A) receptor occupancy of the novel substance vortioxetine (Lu AA21004). A PET study in control subjects. Eur Neuropsychopharmacol. 2013;23(10):1190–1198. doi:10.1016/j.euroneuro.2013.01.002
62. Alvarez E, Perez V, Artigas F. Pharmacology and clinical potential of vortioxetine in the treatment of major depressive disorder. Neuropsychiatr Dis Treat. 2014;10:1297–1307. doi:10.2147/NDT.S41387
63. Baldwin DS, Chrones L, Florea I, et al. The safety and tolerability of vortioxetine: analysis of data from randomized placebo-controlled trials and open-label extension studies. J Psychopharmacol. 2016;30(3):242–252. doi:10.1177/0269881116628440
64. Pearce EF, Murphy JA. Vortioxetine for the treatment of depression. Ann Pharmacother. 2014;48(6):758–765. doi:10.1177/1060028014528305
65. Citrome L. Vortioxetine for major depressive disorder: an indirect comparison with duloxetine, escitalopram, levomilnacipran, sertraline, venlafaxine, and vilazodone, using number needed to treat, number needed to harm, and likelihood to be helped or harmed. J Affect Disord. 2016;196:225–233. doi:10.1016/j.jad.2016.02.042
66. Saragoussi D, Christensen MC, Hammer-Helmich L, Rive B, Touya M, Haro JM. Long-term follow-up on health-related quality of life in major depressive disorder: a 2-year European cohort study. Neuropsychiatr Dis Treat. 2018;14:1339–1350. doi:10.2147/NDT.S159276
67. Rosenblat JD, Kakar R, McIntyre RS. The cognitive effects of antidepressants in major depressive disorder: a systematic review and meta-analysis of randomized clinical trials. Int J Neuropsychopharmacol. 2015;19(2). pii:pyv082. doi:10.1093/ijnp/pyv082.
68. McIntyre RS, Lee Y. Cognition in major depressive disorder: a ‘Systemically Important Functional Index‘ (SIFI). Curr Opin Psychiatry. 2016;29(1):48–55. doi:10.1097/YCO.0000000000000221
69. Albert U, Brugnoli R, Caraci F, et al. Italian psychiatrists‘ perception on cognitive symptoms in major depressive disorder. Int J Psychiatry Clin Pract. 2016;20(1):2–9. doi:10.3109/13651501.2015.1093147
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.