Back to Journals » Patient Preference and Adherence » Volume 17
Cognitive and Emotional Motivation to Explain Infection-Prevention Behaviors with Social Support as a Mediator During the COVID-19 Pandemic: A Nationwide Cross-Sectional Study in Korea
Authors Park M ![]() , Oh K, Kim H, Fan X, Giap TTT, Song R
, Oh K, Kim H, Fan X, Giap TTT, Song R ![]()
Received 24 January 2023
Accepted for publication 6 April 2023
Published 18 April 2023 Volume 2023:17 Pages 1063—1073
DOI https://doi.org/10.2147/PPA.S404310
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Myonghwa Park,1 Keunyeob Oh,2 Hyungjun Kim,3 Xing Fan,1,4 Thi-Thanh-Thnh Giap,1,5 Rhayun Song1
1College of Nursing, Chungnam National University, Daejeon, South Korea; 2College of Economics and Management, Chungnam National University, Daejeon, South Korea; 3School of Business, Chungnam National University, Daejeon, South Korea; 4College of Medicine, Lishui University, Lishui, People’s Republic of China; 5College of Health Sciences, VinUniversity, Hanoi, Vietnam
Correspondence: Rhayun Song, College of Nursing, Chungnam National University, Munwha-ro 266, Jung-Gu, Daejeon, 35015, South Korea, Tel +82-42-580-8331, Fax +82-42-580-8309, Email [email protected] Xing Fan, College of Nursing, Chungnam National University, Munwha-ro 266, Jung-Gu, Daejeon, 35015, South Korea, Tel +82-42-580-8331, Fax +82-42-580-8309, Email [email protected]
Purpose: To predict the performance of infection-prevention behaviors among adults in Korea based on the health belief model, using social support as a mediator.
Patients and Methods: A nationwide cross-sectional survey of 700 participants from the local community was conducted using both online and offline methods from 8 metropolitan cities and 9 provinces in Korea from November 2021 to March 2022. The questionnaire was composed of 4 sections: demographic information, motivational factors for behavior change, social support, and infection-prevention behaviors. Data were analyzed using structural equation modeling with the AMOS program. The general least-squares method was applied to assess the fit of the model and the bootstrapping method was tested for indirect effect and the total effect.
Results: Motivation factors that directly affected infection-prevention behaviors were self-efficacy (γ=0.58, p< 0.001), perceived barriers (γ=– .08, p=0.004), perceived benefits (γ=0.10, p=0.002), perceived threats (γ=0.08, p=0.009), and social support (γ=0.13, p< 0.001), after controlling for related demographic variables. Cognitive and emotional motivation factors together explained 59% of the variance in infection-prevention behaviors. Social support exerted significant mediating effects between each cognitive and emotional motivation variable and infection-prevention behaviors, along with a significant direct effect on infection-prevention behaviors (γ=0.12, p< 0.001).
Conclusion: The engagement of prevention behaviors among community-dwelling adults was influenced by their self-efficacy, perceived barriers, perceived benefits, and perceived threats with social support as a mediator. Prevention policy approaches could include providing specific information to improve self-efficacy and build awareness of the severity of the disease while establishing a supportive social environment for promoting health behaviors during the COVID-19 pandemic.
Keywords: COVID-19, health belief model, prevention behavior, motivation factor, social support
Introduction
After the World Health Organization officially announced the start of the Coronavirus disease 2019 (COVID-19) pandemic in March 2020, most countries enacted strict universal control and social-distancing policies to stop the spread of COVID-19, leading to restraints of individual economic, social, and cultural activities.1 Since effective treatments for COVID-19 became available only recently, it was essential for each individual to engage in infection-prevention behaviors, such as physical distancing, personal hygiene, wearing masks, and getting a vaccination in order to protect themselves as well as other society members.2
Previous studies of the SARS (severe acute respiratory syndrome) outbreak suggested that psychosocial factors, including self-efficacy, age, perceived susceptibility, and attitudes toward preventive measures, affect the motivation of individuals to engage in infection-prevention behaviors.3 Anxiety also influences the protective behaviors of members, while the presence of symptoms leads to greater use of health services.4 Chuang et al confirmed that during an influenza pandemic, government trust and interpersonal networks played crucial roles in adopting health-protective behaviors.5 Similar results have been obtained in recent studies since the beginning of the COVID-19 pandemic,6–9 all supporting that the awareness of risk is the strongest predictor for engaging in infection-prevention behaviors (eg, getting a COVID-19 vaccination), while Wise et al considered that people often underestimate their risk of infection.8 Moreover, Jørgensen et al reported that self-efficacy was the key to engaging in infection-prevention behaviors.6 This conclusion was confirmed by the results of a systematic review, while further supporting the perceived benefits as the strongest predictor for infection-prevention behavior, followed by self-efficacy.9
Recent studies have also analyzed various theoretical models to identify the factors affecting infection-prevention behaviors, among which the health belief model (HBM) proposed by Rosenstock is useful for explaining the motivation of health behaviors.9,10 Later, the extended health belief model was introduced when self-efficacy was incorporated into the model.11 The threat perceptions of individuals and evaluations of health behaviors to cope with such threats have been analyzed using the extended HBM,12 with four components being considered: (1) perceived threats which, combined with perceived susceptibility and severity, refer to a feeling of real danger and to having a serious condition; (2) perceived benefits, referring to the perception of effectiveness and benefits of taking actions; (3) perceived barriers, referring to the perception of negative outcomes preventing them from taking actions; and (4) self-efficacy, referring to the confidence in the ability to take actions. Individuals believe that when they are affected by a condition whose consequences are sufficiently serious, they would evaluate the potential benefits of intervention behaviors and their costs and barriers and will be more likely to follow health behaviors when they consider that there are more positive benefits, fewer barriers and that they are sufficiently capable of performing them. Meanwhile, self-efficacy, perceived benefits, and perceived barriers are presented as cognitive motivating factors for explaining an individual’s behavior, and the perceived threat of a specific health risk is explained as an emotional motivator to affect behavioral changes.13
In addition, some cues, such as the internal personal perception of symptoms or external social-influence triggers, can activate health behaviors.14,15 In previous studies, social support has been introduced as a potential reason for individuals to choose to perform health behaviors.16,17 Social support in this context refers to the degree to which individuals seek and receive appraisal support from others in a specific situation (ie, social distancing due to COVID-19).18 The supportive relationship can provide encouragement and feedback regarding health behaviors and health information to cope with stressful and threat situations.16 The previous studies supported the role of social support as a mediator between HBM determinants and infection-prevention behaviors.16,19,20
Considering the importance of following prevention policies during the COVID-19 pandemic, the present study utilized motivation factors based on the extended HBM with social support as a mediator to predict the performance of infection-prevention behaviors among adults in Korea (Figure 1).
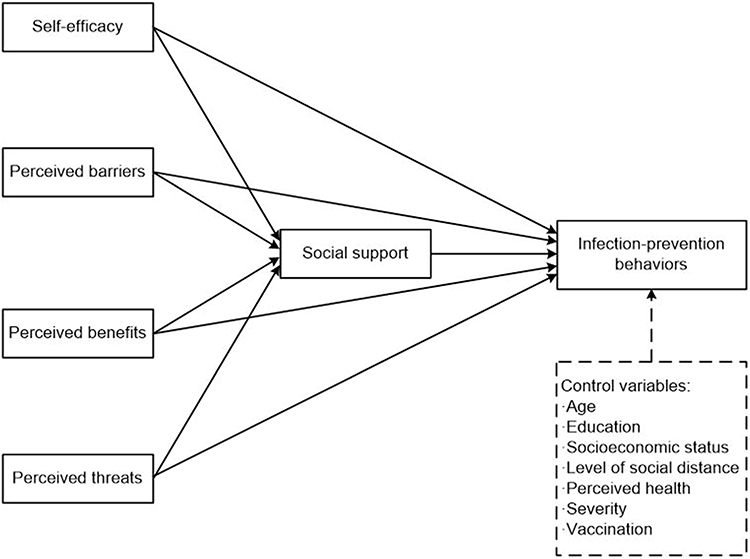 |
Figure 1 Conceptual framework of the study. |
Materials and Methods
Design
A nationwide cross-sectional survey was conducted among 700 adults living in the local community from 8 metropolitan cities and 9 provinces in Korea while considering their age, gender, and regional distributions.
Participants
The inclusion criteria for this study were living in the community (including metropolitan cities, small or medium-sized cities, and urban and rural areas), both genders, and aged from 18 to 80 years. Those who were hospitalized in hospitals or nursing homes, restricted in performing their daily activities independently due to physical or situational circumstances, or who refused to respond to the questionnaire were excluded.
The required number of subjects when using the maximum-likelihood method in a structural model was applied in this study (200 or more), and a sample size of 700 was chosen to represent the nationwide cohort.
Data Collection Procedure
The study was conducted following the Declaration of Helsinki. After obtaining IRB approval (approval number 202109-SB-191-01) from Chungnam National University where the researchers are affiliated, a nationwide cross-sectional survey was conducted from 8 metropolitan cities and 9 provinces in Korea, using both online (70%) and offline (30%) methods from November 2021 to March 2022, with approximately 40% of response rates. The online survey was used for the young and middle-aged, including some in their 50s, which took about 20 minutes. In order to secure responses from those in their late 50s or older, a team of trained interviewers was dispatched to each region to recruit participants at apartment complexes, senior citizen centers, shopping malls, and bus terminals in the area. The face-to-face interview took 30–40 minutes to complete and strictly followed the recommended social isolation policy by the Korean Centers for Disease Control and Prevention (KCDC). Structured questionnaires were used to recruit 700 participants from the general population living in the local community while considering their gender, age, and regional distributions as a representative of the Korean adult population.
All study participants provided informed consent. The data collected through online and face-to-face surveys were entered into Excel without personal-identifiable information and transferred to SPSS and AMOS software for the data analysis.
Measurements
Motivational Factors for Behavior Change
The motivation scale for health behaviors was developed based on social cognitive theory and Ford’s emotional motivation theory, and validated in Korean population.13 After receiving approval from the authors, the items were modified to specify infection-prevention behaviors as target behaviors (Supplement A). The content validity of the modified scale was confirmed by a medical professor, two professors who specialize in research surveys, and two nursing professors. The motivation scale for infection-prevention behaviors consists of four subdomains of cognitive and emotional motivation: self-efficacy (six items), perceived benefit (six items), perceived barriers (six items), and perceived threats (six items). This 24-item scale was measured on a five-point Likert scale from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating higher levels of self-efficacy, perceived benefits, and perceived threats, and less perceived barriers. At the time of development of the motivation scale, its Cronbach’s ⍺ was 0.84,13 and 0.87 (range of 0.80–0.92) for the modified scale used in the present study.
Social Support
Social support was assessed using the 4-item social support scale selected as appraisal support from the interpersonal support evaluation list developed by Cohen et al.21 The items of appraisal social support are related to the feedback given to individuals to assist them in self-evaluation or appraising a situation.22 The items were modified to reflect the perceived availability of social support in performing infection-prevention behaviors (Supplement B). The scale was rated on a five-point Likert scale from 1 (definitely false) to 5 (definitely true). The higher scores indicated a higher level of perceived social support. The reliability of the 4-item social support scale was Cronbach’s alpha of 0.86 for this study.
Infection-Prevention Behaviors
The scale for assessing infection-prevention behaviors was developed for this study based on the Korean version of the National Code of Conduct for COVID-19 Prevention Manual distributed by the Korea Centers for Disease Control and Prevention (KCDC) in March 6, 2020. A 25-item Infection Prevention Behavior Performance Scale (IPBP-25) consisted of social distancing (3 items), symptom management (5 items), environmental management (3 items), stress management (4 items), healthy living (2 items), and guidelines (2 items). The IPBP-25 measured the frequency of performance on a four-point Likert scale from 1 (never) to 4 (always), with a higher score indicating the better performance of infection-prevention behaviors. The content validity of IPBP-25 was confirmed by an expert panel in preventive medicine, nursing, and social research. The Cronbach’s alpha was 0.92 for this study (Supplement C).
Data Analysis
The collected data were analyzed using the IBM SPSS (version 26.0) and AMOS (version 26.0) software, and the statistical significance cutoff in two-sided tests was 0.05. The general characteristics and main variables of subjects were analyzed using descriptive statistics, and skewness and kurtosis were checked for sample normality. Differences in infection-prevention behaviors according to the general characteristics of subjects were tested using the independent t-test and one-way ANOVA, and the Scheffe test was performed as a post-hoc test. The correlations between measurement variables were quantified using Pearson’s correlation coefficients. The direct and indirect effects of the variables on infection-prevention behaviors were analyzed by path analysis. The general least-squares method was applied to assess the fit of the model. The fitness of the model was tested using χ2, χ2/df, GFI (goodness-of-fit index), SRMR (standardized root-mean-square residual), CFI (comparative fit index), TLI (Tucker-Lewis index), and RMSEA (root-mean-square error of approximation). The statistical significance of the indirect effect and the total effect was tested using the bootstrapping method.
Results
General Characteristics and Infection-Prevention Behaviors of the Subjects
Table 1 presents the differences in infection-prevention behaviors according to the general characteristics of the subjects. The mean age of the subjects was 48.13 years, with an age range from 18 to 80 years, and the distribution of all age groups was similar. The distributions of the men and women were similar. Most (n=443, 63.3%) of the subjects had graduated from university and reported their socioeconomic status as moderate (N=414, 59.2%). Regarding the social-distancing stage, 187 people (26.7%) were in the third stage, 173 (24.6%) were in the second stage, and 188 (26.9%) were not aware of the social-distancing stage in their residence area.
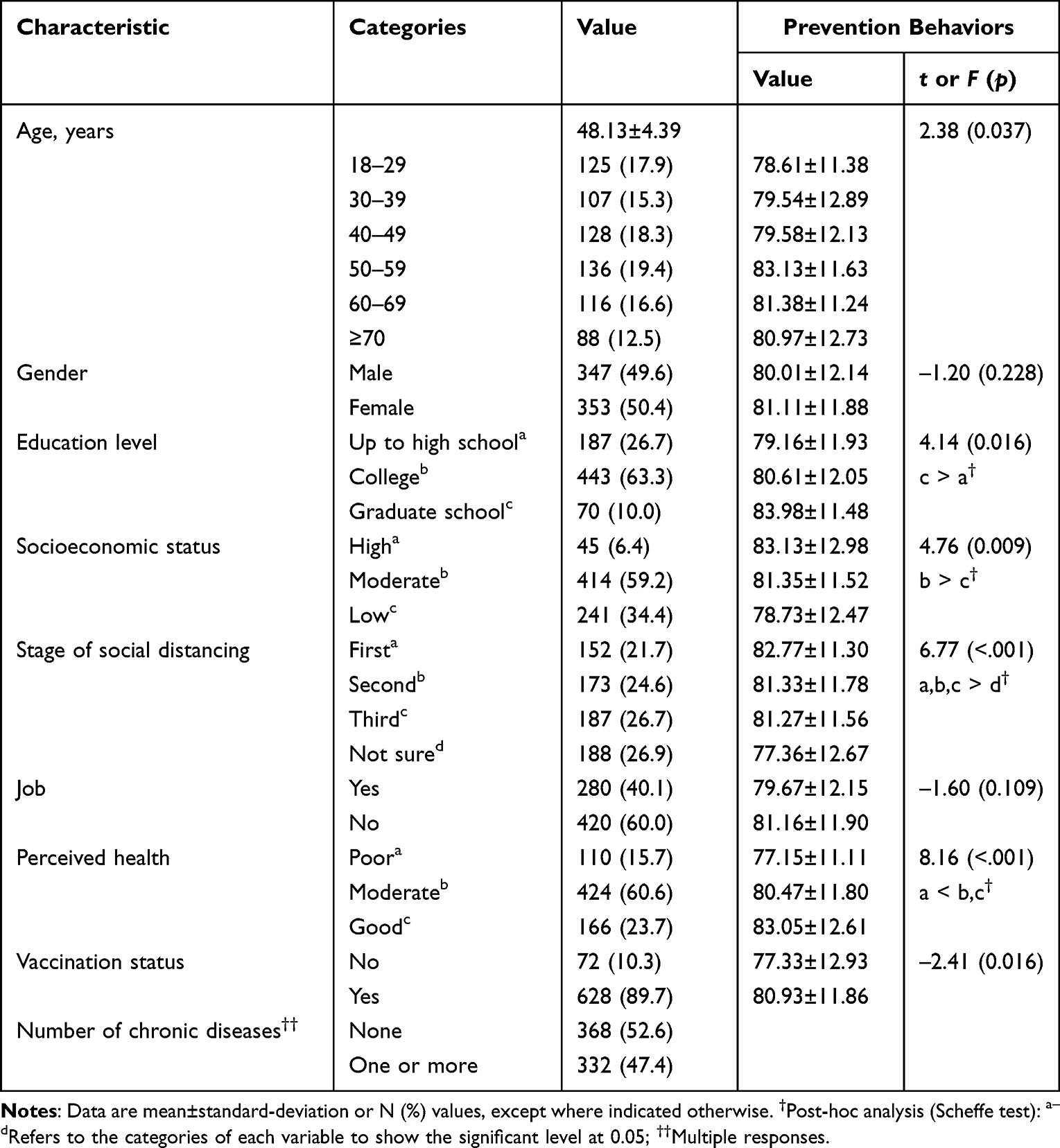 |
Table 1 Characteristics of the Participants and Infection-Prevention Behaviors (N=700) |
There were significant differences in the performance of infection-prevention behaviors according to age, education level, socioeconomic status, social-distancing level, perceived health status, and vaccination status. Those aged 50–59 years (F=2.38, p=0.037) who were more educated (F=4.14, p=0.016), had a higher income (F=4.76, p=0.009), were more aware of the social-distancing stage (F=6.77, p<0.001), had better perceived health (F=8.16, p<0.001), and were vaccinated (t=–2.41, p=0.016) performed better infection-prevention behaviors than those in the other corresponding categories.
Descriptive Statistics of Study Variables
The motivational variables and infection-prevention behaviors are presented in Table 2. The mean item score for performing infection-prevention behaviors among participants was 3.22, indicating individuals performed prevention behaviors between “often” and “always.” The self-efficacy score was 4.25±0.62 (mean±standard deviation) on the five-point scale, showing strong confidence in complying with prevention behaviors, followed by perceived benefits (mean=3.99). The social-support score was 3.94±0.76, also indicating a high level of social support perceived by individuals. The skewness and kurtosis of the measured variables met the assumption of a univariate normal distribution based on their absolute values, but the multivariate kurtosis index was 21.25, which did not satisfy the assumption of multivariate normality at the significance cutoff of 0.05; in this case, the generalized least-squares method was used.
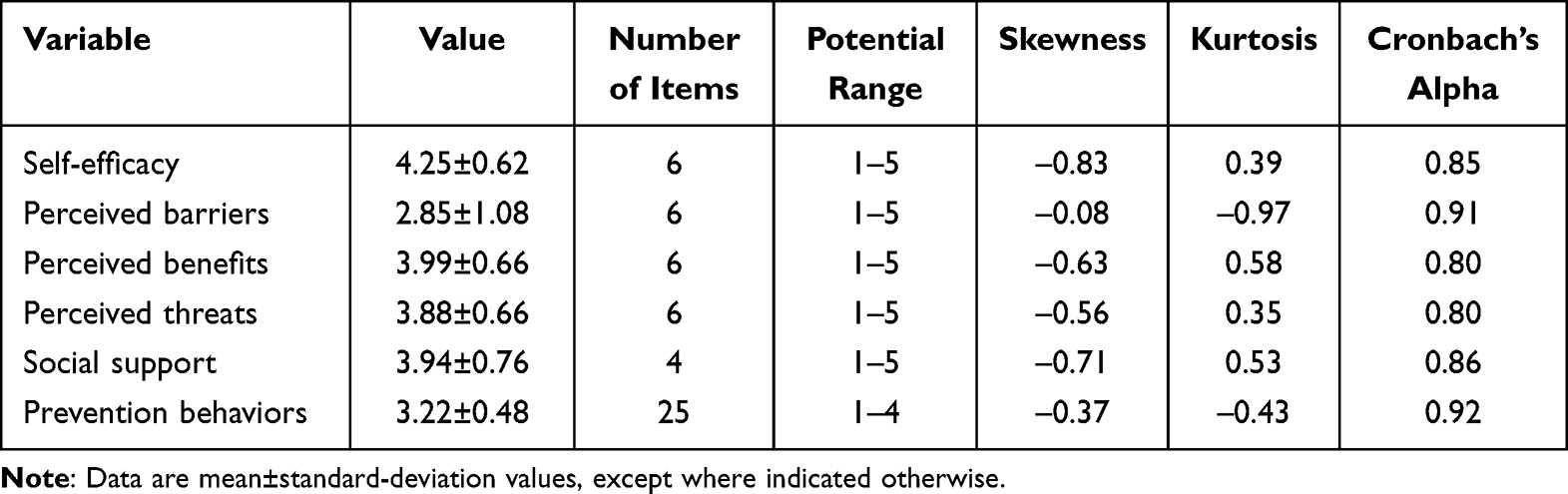 |
Table 2 Descriptive Statistics of Observed Variables (N=700) |
Correlations Among Motivation Factors and Infection-Prevention Behaviors
Infection-prevention behaviors were significantly correlated with self-efficacy (r=0.73, p<0.001), perceived benefits (r=0.57, p<0.001), perceived threats (r=0.40, p<0.001), and social support (r=0.52, p<0.001). Perceived threats showed moderate correlations with other cognitive motivation variables, with coefficients ranging from 0.32 to 0.41 (p<0.001). Social support as the mediating variable was moderately correlated with infection-prevention behavior (r=0.52, p<0.001), also with self-efficacy (r=0.50, p<0.001), perceived benefits (r=0.53, p<0.001), and perceived threats (r=0.39, p<0.001). The absolute values of the coefficients for the correlations between the measured variables were 0.01 to 0.73, the tolerance limits were 0.52 to 0.84 (ie, >0.10), and the variance expansion index ranged from 1.18 to 1.91 (ie, <10), indicating no multicollinearity issue between variables (Table 3).
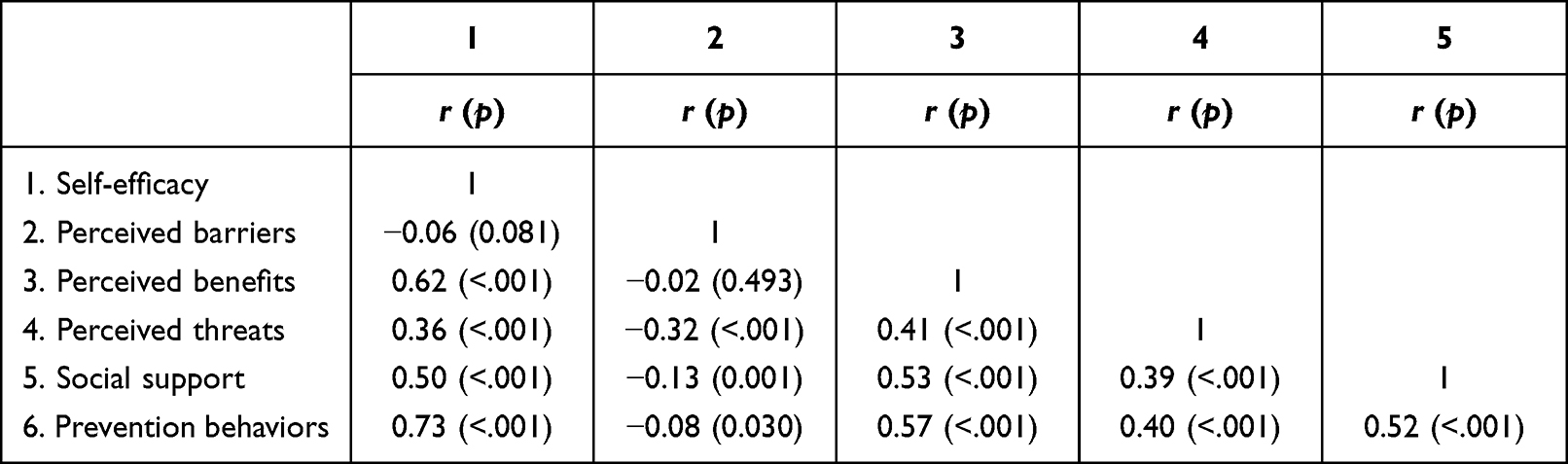 |
Table 3 Correlation Matrix of Observed Variables (N=700) |
Hypothesis Model Testing
Testing the fit of the hypothesis model in this study yielded values of χ2=0.47 (p=0.492), χ2/df=0.47, GFI=1.00, and RMSEA=0.00 (90% confidence interval=0.00–0.08). With SRMR=0.01, TLI=1.00, and CFI=1.00, all indices met the recommended level for a good fit. All nine pathways established in the hypothetical model of this study were found to be significant even after controlling for demographic variables, including age, education level, socioeconomic status, social-distancing level, perceived health, and vaccination status (Figure 2). Table 4 presents the results of analyzing the direct, indirect, and total effects of the hypothetical model on endogenous variables. The variables that directly affected social support were self-efficacy (γ=0.26, p<0.001), perceived barriers (γ=–.08, p=0.012), perceived benefits (γ=0.28, p<0.001), and perceived threats (γ=0.15, p<0.001), with perceived benefits being the most-influential variable. The cognitive and emotional motivation variables together explained 36.6% of the variance in social support.
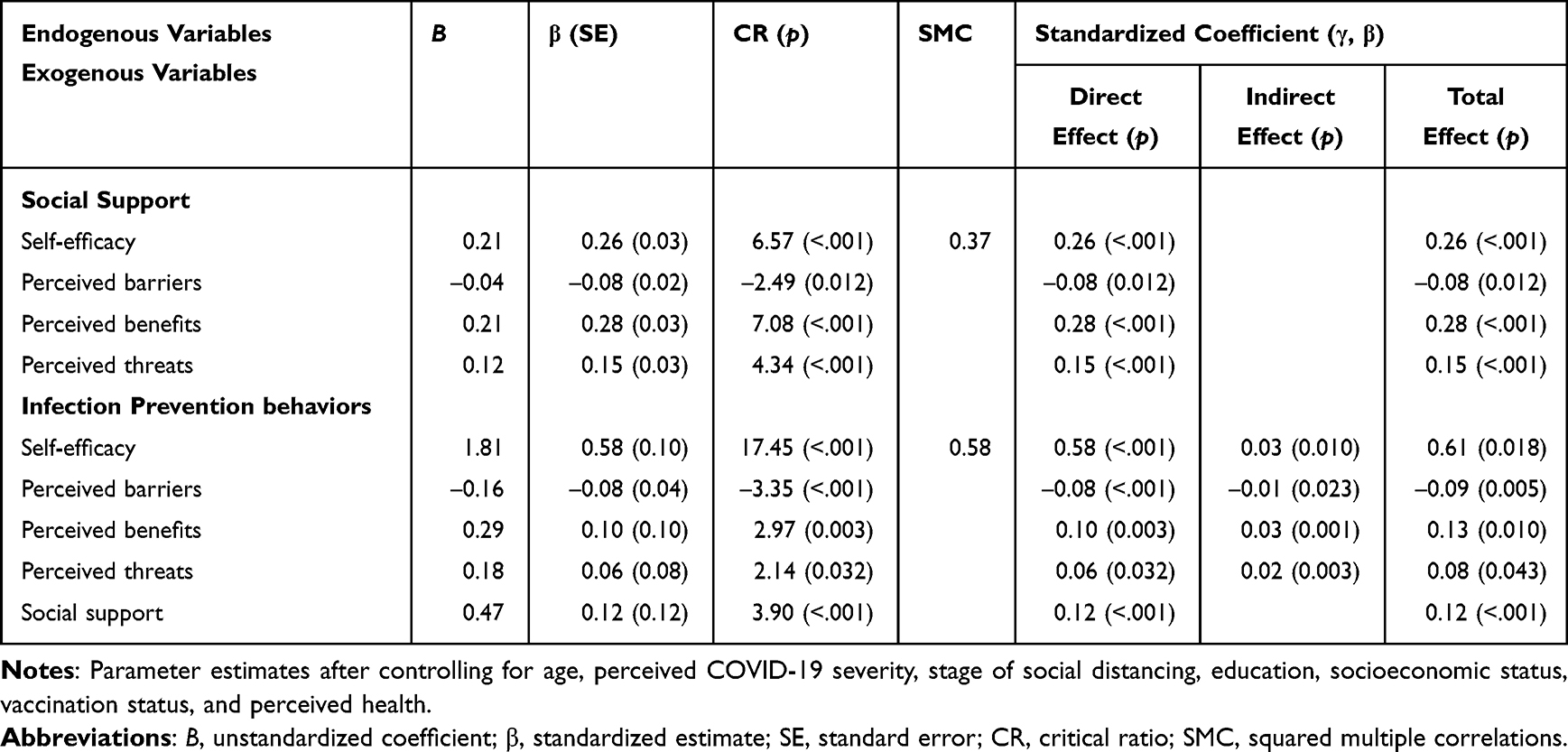 |
Table 4 Parameter Estimates for the Hypothetical Model and Standardized Direct, Indirect, and Total Effects After Controlling for Demographic Characteristics (N=700) |
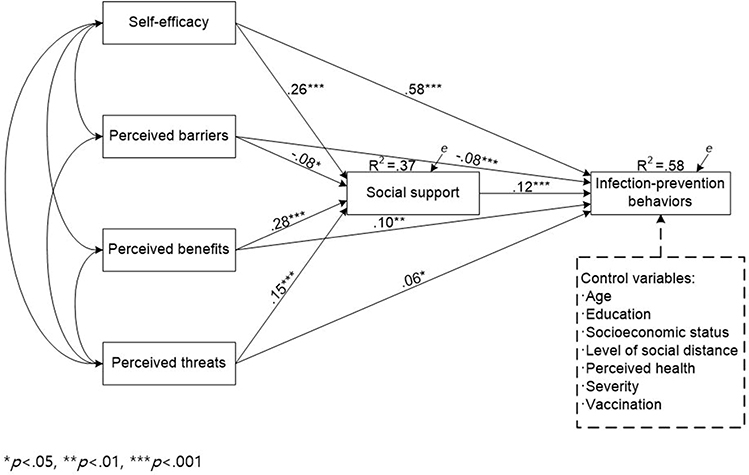 |
Figure 2 Path diagram for the hypothetical model. *p<0.05, ** p<0.01, *** p<0.001. |
Motivation factors that directly affected infection-prevention behaviors were self-efficacy (γ=0.58, p<0.001), perceived barriers (γ=–.08, p=0.004), perceived benefits (γ=0.10, p=0.003), perceived threats (γ=0.06, p=0.032), and social support (γ=0.12, p<0.001), with self-efficacy being the most-influential variable. The motivation variables and social support together explained 58% of the variance in infection-prevention behaviors. Social support exerted significant mediating effects (γ= –0.01 to 0.03) between motivation variables and infection-prevention behaviors, along with a significant direct effect on infection-prevention behaviors (γ=0.13, p<0.001).
Discussion
The extended HBM with social support as a mediator was the conceptual framework used in this study, and it has been confirmed as having an appropriate explanatory power for infection-prevention behaviors.23 The current national survey revealed that engagement in infection-prevention behaviors by Korean adults living in the community were explained by self-efficacy, perceived barriers, perceived benefits, and perceived threats, and mediated by social support. This hypothetical model was found significant after controlling for the general characteristics of age, education level, income, vaccination status, and perceived health.
Among all the constructs of the extended HBM, self-efficacy was the most-significant factor to explain the prevention behaviors. Self-efficacy has been described as the confidence in successfully carrying out behaviors,24 and people with high self-efficacy would consider themselves competent to overcome the perceived barriers, and then succeed in complying with health behaviors.14 Consistent with our findings, a recent systematic review found that self-efficacy was able to predict COVID-19-related behaviors in 87.5% of studies.9 Moreover, Mortada et al25 and Lahiri et al26 both identified self-efficacy as the most-significant factor in practicing COVID-19 protective behaviors. Therefore, education programs for enhancing self-efficacy by identifying preventive strategies or setting progressive goals could be effective when people are facing the pandemic.
The present study found that perceived benefits were another variable affecting infection-prevention behaviors. It is believed that individuals’ beliefs about effectiveness and availability would determine what actions they take.15 The perceived benefits of prevention behaviors such as distancing from others, washing hands, wearing masks, and ventilating frequently to avoid COVID-19 were supported by several empirical studies.27–29 A systematic review23 also found that perceived benefits were the most-frequent significant predictor of behaviors related to COVID-19.
Perceived barriers were one of the cognitive motivation factors that inversely affected infection-prevention behaviors: perceiving more barriers resulted in more discouragement from engaging in prevention behaviors, which was supported by previous studies.27,30 The present study found that the participants still perceived that they lacked information about COVID-19 prevention measures, which combined with the complexity of the quarantine guidelines, made it difficult for them to comply and caused them feelings of anxiety. These perceived barriers influenced their adherence to prevention behaviors, as supported by previous studies.31,32
Similar to previous findings,5,32,33 our results indicated that the construct of perceived threats (combining perceived susceptibility and perceived severity) significantly predicted the prevention behaviors for COVID-19. When people experienced the risk of COVID-19 and believed they were vulnerable to infection, they would be more willing to adopt preventive measures. However, previous studies identified that the ability to perceive threats was the least predictive for prevention behaviors.23,34 Wise et al8 argued that perceptions of the individual risk from the COVID-19 pandemic shifted from over-optimism to a less-optimistic bias, with this shift also predicting more engagement in prevention behaviors. This implies that pandemic prevention strategies need to be tailored to different populations over time and in accordance with virus mutations by considering the public’s perceived threat level in order to effectively promote prevention behaviors.
The most notable finding in this study was that social support mediated the relationship between motivational factors and prevention behaviors, indicating that those motivated people would seek and receive more social support, leading to better prevention behaviors. Consistent with this result, other studies have shown that interactions with family, friends, and neighbors during the COVID-19 pandemic supported the acquisition of information.32,35,36 Meanwhile, getting help and support from others helps to reduce anxiety and loneliness and improve well-being, thus promoting compliance with various prevention behaviors31,37–39 such as increasing the frequency of handwashing and the likelihood of vaccination,40,41 or reducing the likelihood of violating home quarantine guidelines.42 The HBM provides insight into how and why people actively seek or forgo social support when facing disease. If people were in a supportive environment during the COVID-19 pandemic, they would be more likely to acknowledge their own risks40 and perceive themselves as having greater confidence and resilience in coping with this adversity.40,43,44 Moreover, social support might also explain the relationships between motivational factors and health behaviors in other health-related situations. Zhao et al45 believed that information and emotional support would greatly contribute to the benefits perceived by patients with chronic diseases, thus positively affecting their health-information-seeking behaviors.
There were some limitations in this study. Firstly, a cross-sectional design was applied in the survey to represent the associations between motivational factors and prevention behaviors for the given social-distancing policy, rather than exploring the changes therein over time. Given the evolving level of COVID-19 transmission since 2020 to date and the ongoing adjustments to national policies, future studies with multiple longitudinal time points would be helpful for capturing the changes in motivation factors and prevention behaviors as government policies evolve. Secondly, to obtain more-representative samples, this survey adopted both online and offline data collection methods. However, the presence of uneven age and education-level distributions also implied the presence of sampling bias, reflecting the underrepresentation of the sample for older adults and those with a low education level. At the same time, the utilization of self-report measurements might have resulted in social-desirability response bias,46 namely that individuals tend to respond according to prevailing values during the COVID-19 pandemic. Finally, we used the theoretical framework of the extended HBM and social support to explain the prevention behaviors of individuals during the pandemic. While we included both cognitive and emotional factors as individual factors to explain prevention behaviors, we do not examine the influence of government policies. Since participation in prevention behaviors may also be influenced by the family context,42 government social media,47 national policies, and other factors, future studies should also include those interactive factors at the family, social, and political levels in this context.
Implications
Over the past few years, countries worldwide have made tremendous efforts to contain the spread of COVID-19, among which implementing active preventive measures is one of the crucial interventions; the present findings have some important implications for formulating such preventive measures. Firstly, vaccination status and the level of infection-prevention behaviors varied according to the characteristics of the population demographics, which should be taken into account when implementing prevention policy to define the vulnerable population during the pandemic crisis.
Secondly, to enhance the capacity to cope with COVID-19, focus could be placed on improving the self-efficacy of individuals, building their awareness of the severity of disease and the benefits of taking actions, and removing related barriers.
Finally, policies could be designed around promoting social support, to strengthen supportive relationships between families and friends and increase interactions within the community. Future research could explore non-face-to-face interaction patterns that can provide information, advice, and emotional support at a safe social distance to induce behavioral awareness among individuals.
Conclusion
This study employed the framework of the extended HBM and social support to reveal that, during the COVID-19 pandemic, the engagement of prevention behaviors among community-dwelling adults was influenced by their self-efficacy, perceived barriers, perceived benefits, and perceived threats with social support as a mediator. Prevention policy approaches could include providing specific information to improve self-efficacy and build awareness of the severity of the disease while establishing a supportive social environment for promoting health behaviors during the COVID-19 pandemic.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of Chungnam National University (202109-SB-191-01) and was conducted according to the guidelines of the Declaration of Helsinki. Informed consent was obtained from all study subjects.
Funding
This study was supported by the National Research Foundation of Korea Grant funded by the Korean Government (MOE).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO director-general’s opening remarks at the media briefing on COVID-19. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-The-media-briefing-on-covid-19---11-march-2020.
2. Lee SH, Kim JM. Coronavirus disease 2019 (COVID-19): pandemic and the challenge of public health. Korean J Fam Pract. 2020;10(2):9. doi:10.21215/kjfp.2020.10.2.87
3. Tang CSK, Wong CY. An outbreak of the severe acute respiratory syndrome: predictors of health behaviors and effect of community prevention measures in Hong Kong, China. Am J Public Health. 2003;93(11):1887–1888. doi:10.2105/ajph.93.11.1887
4. Leung GM, Ho LM, Chan SK, et al. Longitudinal assessment of community psychobehavioral responses during and after the 2003 outbreak of severe acute respiratory syndrome in Hong Kong. Clin Infect Dis. 2005;40(12):1713–1720. doi:10.1086/429923
5. Chuang YC, Huang YL, Tseng KC, Yen CH, Yang LH. Social capital and health-protective behavior intentions in an influenza pandemic. PLoS One. 2015;10(4):e0122970. doi:10.1371/journal.pone.0122970
6. Jørgensen F, Bor A, Petersen MB. Compliance without fear: individual-level protective behaviour during the first wave of the COVID-19 pandemic. Br J Health Psychol. 2021;26(2):679–696. doi:10.1111/bjhp.12519
7. Wang P-W, Ahorsu DK, Lin C-Y, et al. Motivation to have COVID-19 vaccination explained using an extended protection motivation theory among university students in China: the role of information sources. Vaccines. 2021;9(4):380. doi:10.3390/vaccines9040380
8. Wise T, Zbozinek TD, Michelini G, Hagan CC, Mobbs D. Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States. R Soc Open Sci. 2020;7(9):200742. doi:10.1098/rsos.200742
9. Zewdie A, Mose A, Sahle T, et al. The health belief model’s ability to predict COVID-19 preventive behavior: a systematic review. SAGE Open Med. 2022;10:1–10. doi:10.1177/20503121221113668
10. Rosenstock IM. The health belief model and preventive health behavior. Health Educ Monogr. 1974;2(4):354–386. doi:10.1177/109019817400200405
11. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the Health Belief Model. Health Educ Q. 1988;15(2):175–183. doi:10.1177/109019818801500203
12. Conner M, Norman P. Predicting and Changing Health Behaviour: Research and Practice with Social Cognition Models.
13. Song R, Park M. Motivation factors for stages of behavioral change among individuals with metabolic syndrome. Korean J Adult Nurs. 2018;30(1):60–69. doi:10.7475/KJAN.2018.30.1.60
14. Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice. John Wiley & Sons; 2008.
15. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
16. Akey JE, Rintamaki LS, Kane TL. Health Belief Model deterrents of social support seeking among people coping with eating disorders. J Affect Disord. 2013;145(2):246–252. doi:10.1016/j.jad.2012.04.045
17. Padchasuwan N, Kaewpitoon SJ, Rujirakul R, et al. Modifying health behavior for liver fluke and cholangiocarcinoma prevention with the health belief model and social support theory. Asian Pac J Cancer Prev. 2016;17(8):3721–3725.
18. Ashida S, Wilkinson AV, Koehly LM. Social influence and motivation to change health behaviors among Mexican-origin adults: implications for diet and physical activity. Am J Health Promot. 2012;26(3):176–179. doi:10.4278/ajhp.100107-QUAN-2
19. Fisher MH, Sung C, Kammes RR, Okyere C, Park J. Social support as a mediator of stress and life satisfaction for people with intellectual or developmental disabilities during the COVID-19 pandemic. J Appl Res Intellect Disabil. 2022;35(1):243–251. doi:10.1111/jar.12943
20. Pearlman RL, Patel V, Davis RE, et al. Effects of health beliefs, social support, and self-efficacy on sun protection behaviors among medical students: testing of an extended health belief model. Arch Dermatol Res. 2021;313(6):445–452. doi:10.1007/s00403-020-02123-9
21. Cohen LH, McGowan J, Fooskas S, Rose S. Positive life events and social support and the relationship between life stress and psychological disorder. Am J Community Psychol. 1984;12(5):567–587. doi:10.1007/BF00897213
22. Cohen S, Mermelstein R, Kamarck T, Hoberman HM. Interpersonal Support Evaluation List. Social Support: Theory, Research, and Application. Martinus Niijhoff; 1985.
23. Zewdie A, Mose A, Sahle T, et al. The health belief model’s ability to predict COVID-19 preventive behavior: a systematic review. SAGE Open Med. 2022;10:20503121221113668. doi:10.1177/20503121221113668
24. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Social Foundations of Thought and Action: A Social Cognitive Theory. Prentice-Hall, Inc; 1986:xiii, 617–xiii, 617.
25. Mortada E, Abdel-Azeem A, Al Showair A, Zalat MM. Preventive behaviors towards covid-19 pandemic among healthcare providers in Saudi Arabia using the protection motivation theory. Risk Manag Healthc Policy. 2021;14:685–694. doi:10.2147/rmhp.S289837
26. Lahiri A, Jha SS, Chakraborty A, Dobe M, Dey A. Role of threat and coping appraisal in protection motivation for adoption of preventive behavior during COVID-19 pandemic. Front Public Health. 2021;9:678566. doi:10.3389/fpubh.2021.678566
27. Shahnazi H, Ahmadi-Livani M, Pahlavanzadeh B, Rajabi A, Hamrah MS, Charkazi A. Assessing preventive health behaviors from COVID-19: a cross sectional study with health belief model in Golestan Province, Northern of Iran. Infect Dis Poverty. 2020;9(1):157. doi:10.1186/s40249-020-00776-2
28. Mahindarathne PP. Assessing COVID-19 preventive behaviours using the health belief model: a Sri Lankan study. J Taibah Univ Med Sci. 2021;16(6):914–919. doi:10.1016/j.jtumed.2021.07.006
29. Shah GH, Faraz AA, Khan H, Waterfield KC. Perceived benefits matter the most in COVID-19 preventive behaviors: empirical evidence from Okara District, Pakistan. Int J Environ Res Public Health. 2021;18(13). doi:10.3390/ijerph18136772
30. Arceo E, Jurado JE, Cortez LA, et al. Understanding COVID-19 preventive behavior: an application of the health belief model in the Philippine setting. J Educ Health Promot. 2021;10:228. doi:10.4103/jehp.jehp_1441_20
31. Pouresmali A, Dargahi S, Alizadehgoradel J, Kamran A, Fathi D, Molaei B. Self-care behavior prevention of COVID-19 in the general population based on Pender Health Promotion Model: a cross-sectional study. Health Sci Rep. 2022;5(6):e894. doi:10.1002/hsr2.894
32. Kim S, Kim S. Analysis of the impact of health beliefs and resource factors on preventive behaviors against the COVID-19 Pandemic. Int J Environ Res Public Health. 2020;17(22). doi:10.3390/ijerph17228666
33. Li J-B, Yang A, Dou K, Wang L-X, Zhang M-C, Lin X-Q. Chinese public’s knowledge, perceived severity, and perceived controllability of COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: a national survey. BMC Public Health. 2020;20(1):1589. doi:10.1186/s12889-020-09695-1
34. Acar D, Kıcali Ü. An integrated approach to COVID-19 preventive behaviour intentions: protection motivation theory, information acquisition, and trust. Soc Work Public Health. 2022;37(5):419–434. doi:10.1080/19371918.2021.2018082
35. Kimura M, Ide K, Kimura K, Ojima T. Predictors of happiness during the COVID-19 pandemic in mothers of infants and/or preschoolers: a pre-COVID-19 comparative study in Japan. Environ Health Prev Med. 2022;27(1):14. doi:10.1265/ehpm.22-00008
36. Steijvers LCJ, Brinkhues S, Hoebe C, et al. Social networks and infectious diseases prevention behavior: a cross-sectional study in people aged 40 years and older. PLoS One. 2021;16(5):e0251862. doi:10.1371/journal.pone.0251862
37. Fontes A, Pereira CR, Menezes S, et al. Predictors of health-protective and helping behaviors during the covid-19 pandemic: the role of social support and resilience. Psychol Rep. 2022:332941221123777. doi:10.1177/00332941221123777
38. Mahdizadeh SM, Sany SBT, Sarpooshi DR, Jafari A, Mahdizadeh M. Predictors of preventive behavior of nosocomial infections in nursing staff: a structural equation model based on the social cognitive theory. BMC Health Serv Res. 2021;21(1):1187. doi:10.1186/s12913-021-07205-6
39. Yodmai K, Pechrapa K, Kittipichai W, Charupoonpol P, Suksatan W. Factors associated with good COVID-19 preventive behaviors among older adults in Urban Communities in Thailand. J Prim Care Community Health. 2021;12:21501327211036251. doi:10.1177/21501327211036251
40. Jaspal R, Breakwell GM. Social support, perceived risk and the likelihood of COVID-19 testing and vaccination: cross-sectional data from the United Kingdom. Curr Psychol. 2022;41(1):492–504. doi:10.1007/s12144-021-01681-z
41. Bukchin-Peles S, Ronen T. The role of adolescents’ personal and social resources in achieving desired emotional and behavioral outcomes during an anxiety-provoking pandemic outbreak. Int J Environ Res Public Health. 2021;18(12). doi:10.3390/ijerph18126280
42. Shushtari ZJ, Salimi Y, Ahmadi S, et al. Social determinants of adherence to COVID-19 preventive guidelines: a comprehensive review. Osong Public Health Res Perspect. 2021;12(6):346–360. doi:10.24171/j.phrp.2021.0180
43. Hou T, Zhang T, Cai W, et al. Social support and mental health among health care workers during Coronavirus Disease 2019 outbreak: a moderated mediation model. PLoS One. 2020;15(5):e0233831. doi:10.1371/journal.pone.0233831
44. Lim XY, Yap AC, Mahendran R, Yu J. The interplay between anxiety, fear, protective behaviors, compassion, and resilience among older adults during a COVID-19 lockdown: a structural equation modeling study. Transl Behav Med. 2021;11(5):1172–1178. doi:10.1093/tbm/ibaa143
45. Zhao YC, Zhao M, Song S. Online health information seeking among patients with chronic conditions: integrating the health belief model and social support theory. J Med Internet Res. 2022;24(11):e42447. doi:10.2196/42447
46. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice.
47. Tang Z, Miller AS, Zhou Z, Warkentin M. Does government social media promote users’ information security behavior towards COVID-19 scams? Cultivation effects and protective motivations. Gov Inf Q. 2021;38(2):101572. doi:10.1016/j.giq.2021.101572
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.