Back to Journals » Patient Preference and Adherence » Volume 20
Cognitive and Behavioral Transformation in Type 2 Diabetes Through a Self-Efficacy-Focused Structured Education Program: A Descriptive Qualitative Study
Authors Jiang X, Jiang H ![]() , Tang R, Li M
, Tang R, Li M
Received 12 November 2025
Accepted for publication 5 February 2026
Published 17 February 2026 Volume 2026:20 581035
DOI https://doi.org/10.2147/PPA.S581035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Xinjun Jiang,1 Hua Jiang,2 Rongsong Tang,3 Mingzi Li2
1School of Nursing, Hainan Medical University, Haikou, Hainan, People’s Republic of China; 2School of Nursing, Peking University, Beijing, People’s Republic of China; 3Department of Endocrinology, Peking University Third Hospital, Beijing, People’s Republic of China
Correspondence: Mingzi Li, School of Nursing, Peking University, 38 Xueyuan Road, Haidian District, Beijing, 100191, People’s Republic of China, Email [email protected]
Purpose: To explore how adults with type 2 diabetes perceived and sustained self-management 12 months after completing a Self-Efficacy-Focused Structured Education Program (SSEP).
Methods: A descriptive qualitative design was employed. Seventeen participants from a multicenter randomized controlled trial in China completed in-depth, semi-structured interviews. Data were analyzed using Braun and Clarke’s reflexive thematic analysis with NVivo 11.
Results: Five researcher-constructed themes were identified: (1) restructuring of diabetes cognition, (2) enhancement of self-efficacy, (3) reshaping of mindset through learning, (4) reconstruction and internalization of behaviors, and (5) factors influencing behavioral persistence. Participants experienced a cognitive-behavioral transformation in which reflective learning facilitated sustained behavioral change.
Conclusion: The findings reveal a dual-process mechanism: reflective System 2 learning evolved into automatic System 1 habits supported by heuristic tools. Integrating contextual cues, visual prompts, and mobile-based nudges into future SSEP delivery may enhance habit formation and long-term adherence. Combining reflective training with ongoing family and community support could further strengthen diabetes self-management behaviors sustainability.
Keywords: type 2 diabetes mellitus, self-efficacy-focused structured education, self-management behaviors, cognitive restructuring, dual-process perspective, qualitative research
Background
Diabetes mellitus has become a major global public health challenge, with an estimated worldwide prevalence of approximately 11.1%.1 In China, the prevalence stands at 11.9%,2 ranking the country first worldwide in the number of affected individuals. Among these, 90–95% are diagnosed with type 2 diabetes mellitus (T2DM),2 which imposes a substantial and growing disease burden. T2DM carries serious health risks, especially when glycemic control is suboptimal.
Diabetes self-management education (DSME) is widely recognized as a cornerstone of effective diabetes care, enabling patients to acquire essential knowledge, skills, and confidence for daily self-management. Extensive evidence confirms that DSME can enhance diabetes self-management behaviors, improve glycemic control, and reduce complications.3–7 However, despite numerous studies demonstrating DSME’s efficacy, limited attention has been paid to how patients interpret and integrate these educational experiences into their everyday lives once formal programs conclude. Understanding this post-intervention experience is vital for translating educational benefits into sustained behavioral change.
Most previous DSME research has been dominated by quantitative evaluations focusing on metabolic or psychosocial outcomes.5,6 Qualitative inquiries have largely examined practical barriers to diabetes care,8–10 patients’ preferences for DSME content and delivery,11,12 or challenges encountered during participation and implementation.13–15 While informative, these studies have seldom explored patients’ lived experiences after completing DSME—specifically how they internalize, reinterpret, and apply learned strategies in daily self-management.
To address this gap, a broader theoretical lens is needed. Behavior change is not solely a deliberate, reflective process but also involves the gradual formation of automatic, habitual responses—corresponding to reflective, deliberative System 2 and automatic, intuitive System 1 processes in dual-process theory. Integrating this systems perspective provides a conceptual framework for understanding how DSME initially engages reflective cognitive processes (System 2) and, through practice and reinforcement, evolves into automatic self-regulatory patterns (System 1).16,17
The research team previously developed a DSME program—a self-efficacy-focused structured education program (SSEP) grounded in self-efficacy theory, general systems theory, and prior structural equation modeling18 (Figure 1). This program was evaluated in a multicenter randomized controlled trial across four hospitals in China, demonstrating significant improvements in metabolic and psychosocial outcomes.3,4,19,20 While quantitative results confirmed the program’s effectiveness, no qualitative study has yet examined how participants perceived and experienced SSEP after long-term follow-up.
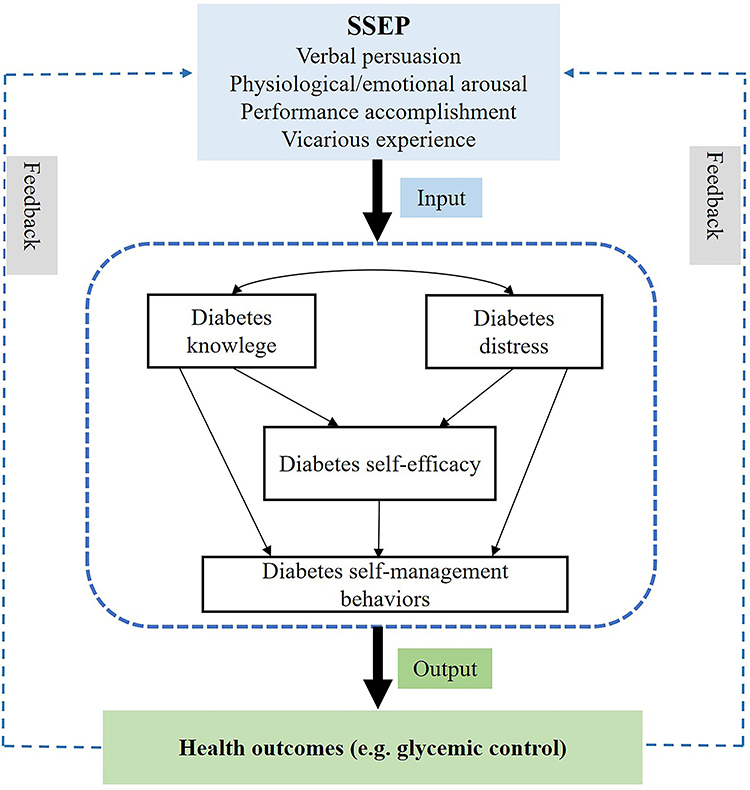 |
Figure 1 Conceptual framework of the self-efficacy-focused structured education program (SSEP). Notes: SSEP draws on the four core sources of self-efficacy: verbal persuasion, physiological/emotional arousal, performance accomplishment, and vicarious experience. Solid arrows indicate hypothesized directional relationships between key constructs. The dashed box represents the core self-management process, including diabetes knowledge, diabetes distress, diabetes self-efficacy, and diabetes self-management behaviors. Dashed arrows labeled as feedback indicate iterative feedback loops between health outcomes and the intervention process. Input refers to the delivery of the SSEP, and Output represents health outcomes, such as glycemic control. |
Therefore, this study aimed to explore how individuals with T2DM perceived, interpreted, and applied the SSEP 12 months after participation. Guided by a systems and dual-process perspective, the study sought to elucidate how reflective learning and enhanced self-efficacy translate into automatic, sustained diabetes self-management behaviors—providing theoretical and practical insights for refining future DSME programs.
Methods
Design
We adopted a descriptive qualitative design to explore participants’ perceptions and experiences after receiving the SSEP. This approach facilitated the generation of rich, detailed, and contextually grounded accounts while retaining flexibility, allowing participants to articulate their thoughts, feelings, and experiences in their own words. One-to-one, in-depth semi-structured interviews were conducted with adults with type 2 diabetes at the 12-month follow-up after completing the SSEP to gain a comprehensive understanding of their post-intervention experiences. The study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist.21
Study Setting
The study was conducted across four hospitals in China that had completed a 12-month randomized controlled trial3,19 (Chinese Clinical Trial Registry (ChiCTR): ChiCTR-IOR-17011007; registered on 30 March 2017). These included primary, secondary, and tertiary hospitals located in Beijing Municipality, Jiangxi Province, and Fujian Province, providing heterogeneity in service level and context. This variation supported a more diverse and analytically informative range of participant experiences.
Participants
Participants were purposively sampled from the randomized controlled trial that evaluated the effectiveness of the SSEP across four hospitals. Purposive sampling was undertaken to ensure variation in key sociodemographic characteristics, including age, gender, occupational status, and educational background, in order to capture a broad range of participant experiences. Interviewees were required to meet the following inclusion criteria: (1) receipt of the SSEP during the trial; (2) completion of 12-month follow-up assessments; (3) ability to communicate in Mandarin; and (4) willingness to participate in semi-structured interviews.
In qualitative research, sample adequacy is guided by the richness and sufficiency of the data in relation to the study aims rather than a priori numbers. Data collection proceeded until the dataset was judged sufficiently rich, detailed, and varied to support meaningful theme development and interpretation. A total of 17 participants were interviewed, providing a rich and diverse dataset consistent with descriptive qualitative principles.22
To further contextualize the qualitative sample within the parent trial, baseline characteristics of interviewees were compared with those of the entire SSEP intervention group. No statistically significant differences were observed between the 17 interviewees and the overall intervention cohort (Table 1). Although the qualitative findings are not intended to be statistically generalizable, this comparability supports the transferability of the findings to patients with similar characteristics and experiences within comparable clinical contexts.
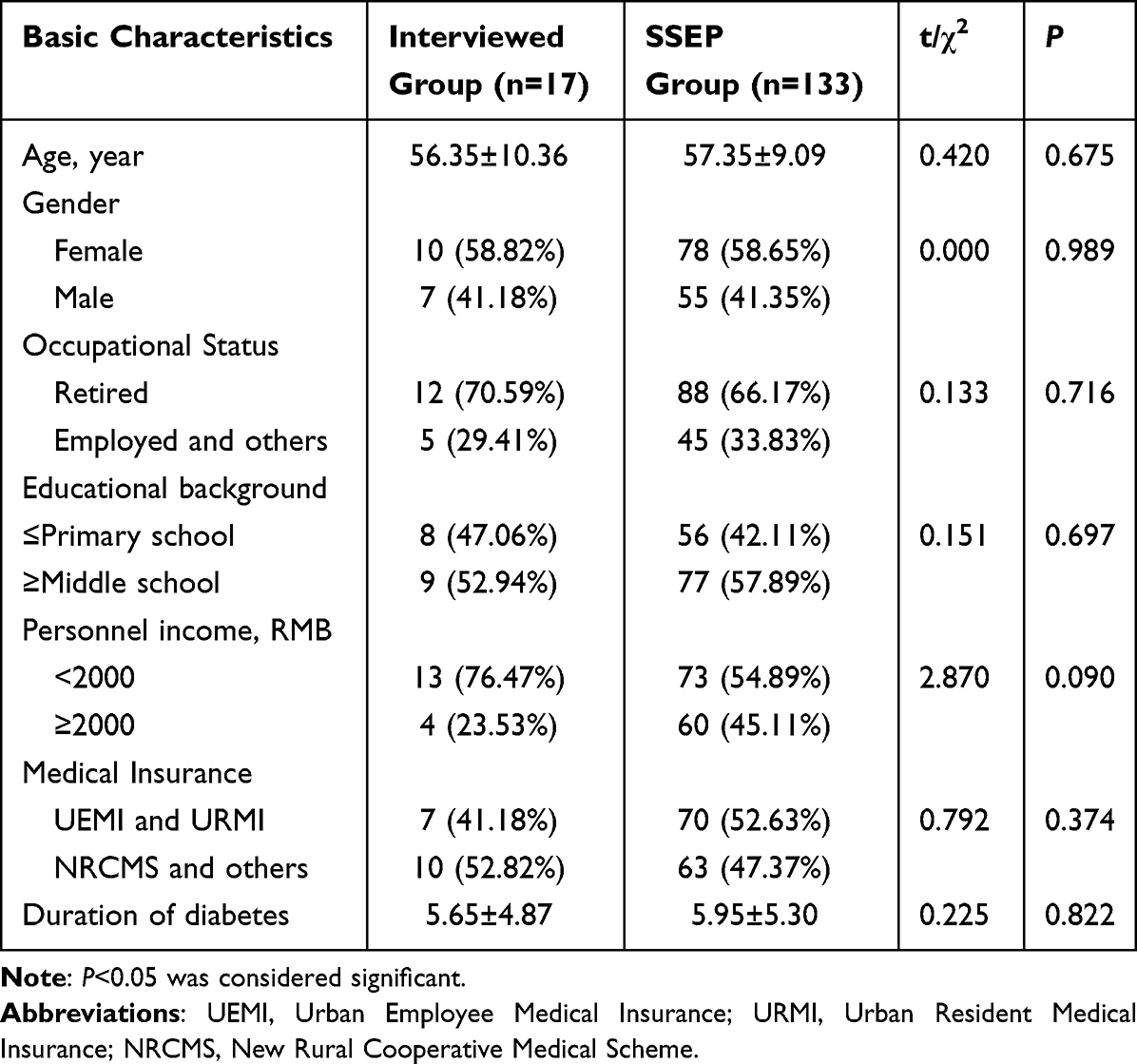 |
Table 1 Comparison of Baseline Characteristics Between the Interviewed Group and the SSEP Group |
Research Team
Interviews were conducted and audio-recorded by Xinjun Jiang (female), assisted by two nurses (female) from hospitals in Jiangxi and Fujian who clarified content when local dialects were used. Although Xinjun Jiang was involved in delivering the SSEP at one study site during the parent randomized controlled trial, she had no role in intervention delivery at the other three study sites. The other members of the research team—Hua Jiang, Rongsong Tang, and Mingzi Li (all female)—were not involved in delivering the intervention at any study site.
Xinjun Jiang is a teacher and PhD candidate with approximately three years of qualitative interviewing experience, a 10-year academic background in nursing, and formal training in qualitative and mixed-methods research (eg, Nursing Research Methods; Mixed Methods Research Design). Other team members also received training in qualitative methods. During data collection, interviews were conducted in accordance with a predefined semi-structured interview guide, and other research team members or nurses were present to assist with participant coordination and provide oversight of the interview process, thereby helping to manage potential expectations or preconceptions. Prior to this study, Xinjun Jiang co-authored a publication on a culturally sensitive nurse-led structured education programme for patients with type 2 diabetes.23
As interviewees were recruited from different research centers by research nurses, the interviewer had no clinical role or supervisory relationship with participants, and no prior contact occurred before recruitment. Before data collection, participants were informed that the study sought to gain deeper insight into their experiences and how they integrated the SSEP into everyday practice. Participation was voluntary and confidential. To ensure descriptive accuracy and minimize interpretive influence, the interviewer used open-ended, participant-led prompts and maintained reflexive notes during data collection to remain attentive to participants’ own expressions. Regular discussions within the research team supported transparency and consistency in data interpretation. The interviewer’s motivation was to gain an in-depth understanding of participants’ perceptions following the SSEP.
Data Collection
Interviews were conducted by Xinjun Jiang between August and October 2018 at each research center. A research nurse at each site screened and telephone-approached potential participants using the inclusion criteria and considered variation in age, gender, education, occupation, economic circumstances, and disease duration. Following enrolment, one-to-one, face-to-face semi-structured interviews were held in a quiet private room at each hospital with assistance from research nurses. Before each interview, the study aim and procedures were explained, and written informed consent was obtained. Research nurses assisted with participant coordination and translated dialects into Mandarin when necessary. The interviewer maintained a reflexive stance to privilege participants’ accounts. Materials prepared included a voice recorder, laptop, notebook, pen, and the interview guide.
The interview guide focused on perceptions and experiences after the SSEP, including diabetes cognition, confidence, emotions, and diabetes self-management behaviors. It was developed and refined through literature review, pilot interviews, and expert feedback. Open-ended questions were used, and the interviewer employed repetition, probing, clarifying questions, summarizing, and responsive listening to elicit detailed narratives, while noting salient non-verbal cues. Each participant completed a single interview lasting 20–30 minutes, and all sessions were audio-recorded with consent.
Ethical Considerations
All study procedures involving human participants were reviewed and approved by the Peking University Institutional Review Board (IRB00001052-17031) and were conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment, including consent for the publication of anonymized data and anonymized direct quotes where applicable.
Data Analysis
This study presents a secondary, theoretically informed reanalysis of qualitative data originally collected in 2018 as part of a multicenter randomized controlled trial evaluating the SSEP. The reanalysis was conducted in 2025 to reinterpret participants’ experiences through contemporary theoretical perspectives integrating self-efficacy theory and dual-process frameworks of behavior change. This approach aimed to generate new conceptual insights into how SSEP fosters long-term cognitive and behavioral transformation.
The data analysis proceeded in two stages. The first stage comprised a collaborative analysis conducted with Rongsong Tang during the researcher’s doctoral studies. The second stage involved an independent, reflexive reanalysis undertaken after the researcher had further studied theories relevant to behavioral economics.
The first stage of qualitative data analysis began concurrently with the interviews. Audio recordings were transcribed verbatim into Microsoft Word immediately after each session. Transcripts were cross-checked by two researchers, and all data were anonymized during transcription, analysis, and reporting. The qualitative software NVivo Pro 11 was used to manage and organize the data. Non-verbal cues observed during the interviews were recorded in analytic memos within NVivo.
Reflexive thematic analysis was conducted following Braun and Clarke’s six-step method.24–26 This involved (1) familiarization with the data; (2) generating initial codes; (3) constructing initial themes; (4) reviewing and refining themes; (5) defining and naming themes; and (6) producing the final analytic narrative. Two researchers independently engaged with the data to enhance interpretive depth; discrepancies were discussed to enrich understanding rather than to seek consensus or calculate inter-rater reliability.
Because the interviews and analyses were conducted in Mandarin Chinese, all transcripts were analyzed in the original language to preserve linguistic and cultural nuances. For publication, representative participant quotations were translated into English through a forward–backward translation process by two bilingual researchers. A third bilingual expert compared the translated quotations with the original transcripts to ensure semantic, conceptual, and cultural equivalence. Any discrepancies were resolved through discussion and consensus.
Member checking was undertaken by telephone after transcription and preliminary analysis. Participants were invited to confirm that their statements accurately reflected their intended meanings and to comment on our interpretations and theme summaries. Their feedback was documented in analytic memos and incorporated into the refinement of the final themes.
The second stage of analysis, conducted between March and August 2025, was guided by the researcher’s reflexive recognition that earlier interpretations had remained primarily descriptive. In this reanalysis, the data were revisited with an explicitly theoretical lens, integrating the dual-process and self-efficacy perspectives to reconstruct deeper meanings underlying participants’ cognitive and behavioral changes. Analytic reflections were recorded throughout the process to ensure transparency and to enhance interpretive rigor.
During data analysis, reflexive awareness was maintained through regular team discussions, documentation of analytic memos, and iterative comparison between emerging interpretations and the original interview data. Analytic decisions were critically examined within the research team to ensure that interpretations remained grounded in participants’ accounts rather than researchers’ prior assumptions.
Results
Characteristics of Interviewees
A total of 17 participants were interviewed, ranging in age from 39 to 75 years (mean = 56.35 ± 10.36 years). The duration of diabetes ranged from 1 to 20 years, with a mean of 5.65 ± 4.87 years. Among the participants, 7 (41.18%) were male and 10 (58.82%) were female; 12 (70.59%) were retired, and 5 (29.41%) were employed. Regarding educational background, 1 (5.88%) participant was illiterate, 7 (41.18%) had completed primary school, and 9 (52.94%) had completed middle school.
With respect to income, 3 (17.65%) participants had no personal income, 10 (58.82%) reported a monthly income below 2000 RMB, and 4 (23.53%) reported an income between 2000 and 5000 RMB. In terms of medical insurance coverage, 4 (23.53%) were covered by urban employee medical insurance, 3 (17.65%) by urban resident medical insurance, and 10 (58.82%) by the New Rural Cooperative Medical Scheme (Table 1, Table 2).
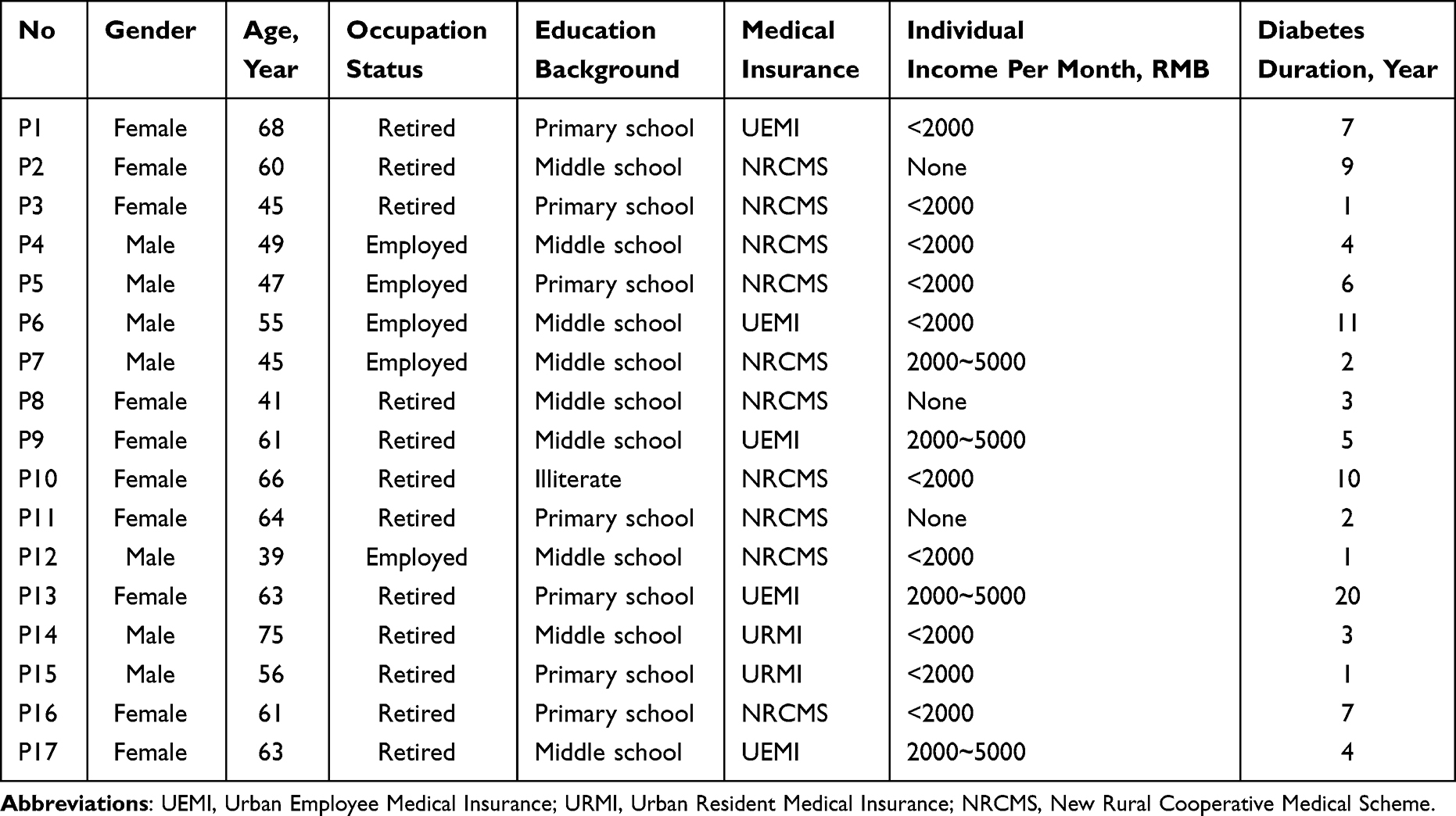 |
Table 2 Characteristics of Interviewees |
Thematic Findings
Five major themes were constructed from the data analysis: (1) restructuring of diabetes cognition, (2) enhancement of self-efficacy in diabetes management, (3) reshaping of mindset empowered by diabetes knowledge, (4) reconstruction and internalization of diabetes self-management behaviors, and (5) factors influencing behavioral persistence. These themes collectively capture the multidimensional cognitive and behavioral changes experienced by participants after completing the SSEP.
Theme 1: Restructuring of Diabetes Cognition
We found that participation in the SSEP prompted a process of cognitive restructuring regarding diabetes. It helped correct misconceptions and reduced participants’ susceptibility to misinformation through cognitive debiasing, while enhanced diabetes knowledge was actively applied to daily health decisions. This transformation was supported by visual tools and concrete heuristics, reflecting a deeper restructuring of patients’ cognitive frameworks.
Cognitive Debiasing and Restructuring
Participants expressed that after engaging in the SSEP, they gained a more accurate understanding of diabetes, corrected previous misconceptions, and became less vulnerable to misleading information. Their perception of the disease shifted from viewing it as a catastrophic and uncontrollable threat to understanding it as a manageable chronic condition.
When I returned to the room, I felt weak and trembling all over. At that time, I thought I had some kind of disease. At first, I didn’t know; I thought that diabetes was like cancer—some people said that, right? After learning a bit, I realized that diabetes is not scary; it’s the complications that are scary. (P4)
Participants, particularly those from rural areas, also reported being less likely to trust misleading health advertisements after the SSEP.
I wouldn’t resort to desperate measures when I was ill, and I wouldn’t listen to television advertisements. (P1)
Deep-Structure Cognitive Restructuring
Participants noted that their knowledge about diet, hypoglycemia, foot care, and exercise improved substantially after attending the SSEP. They were able to translate this knowledge into practical decision-making, a process facilitated by the program’s visual materials and concrete heuristics.
For example, the color-coded diet cards, designed to match actual food sizes, helped participants categorize foods more effectively and make healthier dietary choices:
Those pictures showed what can and cannot be eaten—things we didn’t know before, we know now after seeing them. When I eat, I think of the diet pictures, and then I know which to choose. (P13)
Like those drinks, those sweet things, beer—those things cannot be eaten. (P12)
After the class, I knew what could be eaten and what could not. Eat less fat, and chicken skin cannot be eaten. (P8)
Theme 2: Enhancement of Self-Efficacy in Diabetes Management
We found that participation in the SSEP strengthened participants’ self-efficacy and perceived ability to manage their diabetes effectively. The program enabled them to sustain engagement and self-management efforts despite external challenges, further reinforcing their sense of self-efficacy.
Strengthening Self-Efficacy Through Knowledge and Understanding
After attending the SSEP, participants described a marked increase in self-efficacy (participants’ perceived confidence in managing diabetes) in managing diabetes, which they attributed to the structured acquisition of knowledge and a clearer scientific understanding of the disease.
We are very confident, full of confidence. The teacher said as long as blood sugar can be controlled well, we can also live a healthy life like normal people. That has increased my confidence. (P1)
It gives me a hundredfold confidence. Now I am not afraid anymore. I used to be afraid of not living long, being so young. (P8)
Overcoming Barriers as a Reinforcement of Self-Efficacy
As self-efficacy increased, patients reframed external barriers (such as heavy rain) as situations that could be overcome, and by engaging in the act of attending. They validated the belief “I can do it”, thereby further reinforcing their sense of efficacy.
Even in heavy rain, I will come to attend the class. Once, it was pouring rain, but I still came. (P1)
Theme 3: Reshaping of Mindset Empowered by Diabetes Knowledge
Before participating in the SSEP, many patients reported experiencing negative emotional states due to limited disease awareness and difficulties in glycemic control. These challenges often manifested as feelings of frustration, helplessness, and emotional instability following diagnosis, as well as a sense of inferiority when blood glucose levels were elevated.
When I was first diagnosed, I felt so depressed and conflicted, I would get angry. My blood sugar level is high, so I must be inferior, and I feel very sad. (P8)
After completing the SSEP, participants developed a more systematic understanding of diabetes and a rational, science-based perspective on the condition, which fostered a positive shift in mindset. By internalizing the concept that “diabetes is manageable”, they reported reduced fear and greater emotional stability.
After learning, I feel much more psychologically relaxed. Sometimes if my blood sugar level is a bit high, I’m not afraid anymore. I’ll just control it better next time. I’m not afraid anymore. (P8)
At the same time, participants described improvements in emotion regulation and a greater sense of psychological balance.
My mood is happier. We know that diabetes is just a process, so we can relax our minds. (P13)
Ultimately, participants described a form of psychological restructuring, characterized by a transition from fear and anxiety to acceptance and confidence.
It’s not as terrifying, not as scary anymore. My mood has also improved a lot. (P16)
Theme 4: Reconstruction and Internalization of Diabetes Self-Management Behaviors
After participating in the SSEP, participants’ diabetes self-management behaviors underwent systematic reconstruction through knowledge translation and the gradual internalization of skills. The performance across each behavioral domain was as follows:
Diet, Blood Glucose Monitoring, and Medication: From Empirical Intuition to Guided Adherence
Prior to the SSEP, patients typically relied on personal experience when making dietary choices. After the intervention, they reported adhering more closely to educator-led guidance, adopting healthier and more structured dietary routines.
If I didn’t take this class, I would definitely be more blind and confused. I would just eat however I wanted without paying attention. Through this program, Dr. Wu (the education nurse) taught me how to eat, and my blood sugar levels improved. (P9)
Regarding self-monitoring of blood glucose and medication management, participants shifted from irregular, experience-based practices to regular, evidence-based routines guided by the educator.
Prior to having a blood glucose monitor, I wouldn’t test my blood sugar at all. After buying the monitor, I was only testing it roughly once a month or every two weeks. Now I test it almost every two to three days. (P7)
Before taking the SSEP, if we had high blood sugar levels, we would blindly increase the medication dosage, lowering it too much—even to the point of causing hypoglycemia. Now we know what hypoglycemia is, that medication should be taken at regular times and in fixed amounts, and that if hypoglycemia occurs, we should inform the instructors. (P1)
Physical Activity and Foot Care: Gradual Development of Habitual Practices
Participants reported learning to select suitable forms of exercise—such as walking, calisthenics, or square dancing—and establishing consistent exercise routines, indicating habit formation.
I usually take walks, like 3000 steps or 6000 steps. (P1)
At night I do calisthenics, that is, square dancing; I simply dance in the square. (P2)
I walk or run every day; I strengthen my exercise routine every day. I walk for about half an hour in the morning and half an hour in the evening. (P5)
Similarly, after learning about foot care, some participants developed long-term, proactive maintenance behaviors.
When I get up in the morning, I do foot exercises for a few minutes. (P7)
Managing Hypoglycemia: Upgrading from Reactive Response to Proactive Prevention
Participants demonstrated improved capabilities in recognizing hypoglycemia symptoms, initiating timely self-intervention, and implementing preventive measures. They described being able to plan ahead and carry snacks or water to manage hypoglycemia independently.
Every time I ride my bike, I always have something in my bag, like water or snacks. If my body starts shaking, I quickly stop and eat something—anything will do, even just drinking some water helps. (P4)
Theme 5: Factors Influencing Behavioral Persistence
After completing the SSEP, participants reflected on the challenges they encountered when attempting to sustain and integrate newly acquired diabetes self-management behaviors into daily life. Their narratives revealed that multiple interrelated factors at both individual and environmental levels created dynamic constraints that collectively undermined the continuity and persistence of these behaviors.
The Compounded Strain of Personal Health Limitations and Family Responsibilities
Personal health conditions—such as coexisting chronic illnesses—often restricted participants’ ability to maintain physical activity.
I have other chronic diseases; I can’t exercise vigorously. I still try to persist in exercising, but just a little less. (P16)
In addition, family caregiving responsibilities further consumed the limited time and energy available for self-management.
There are a lot of chores in our family, doing this, doing that—seven or eight people, a lot of chores at home. (P17)
Together, these dual pressures of personal health conditions and family responsibilities produced a sense of “insufficient capacity and scarce time”, causing diabetes self-management behaviors to shift from “less frequent” to “difficult to sustain”.
The Reinforcing Interplay of Insufficient Family Support and Personal Inertia
A lack of family support weakened external motivation to engage in ongoing behavioral practice.
I feel like doing foot exercises, but sitting there alone doing it—I can’t persist. (P16)
At the same time, personal inertia diminished internal drive, reducing the likelihood of initiating or maintaining behaviors.
Sometimes I’m just lazier and don’t want to exercise. I’m a very lazy person. (P17)
This interaction between weak external motivation and low internal drive created a vacuum of “no internal drive and no external prompting”, making behaviors that required consistent practice—such as foot exercises or blood glucose monitoring—especially vulnerable to discontinuation.
After learning the foot exercises at that time, I would also forget them. (P15)
Sometimes I would secretly play and then wouldn’t bother to test my blood sugar. (P17)
The Dual Constraint of Economic Pressure and Livelihood Demands
Economic pressure and demanding work schedules often led to physical fatigue and limited time for disease management, reducing adherence to prescribed exercise and medication routines.
I engaged in physical work until five or six o’clock every day, worked until late at night. When I come home, I just take a shower and go to sleep. How could I still exercise? I’m too tired. (P4)
I was so busy at that time because of my tea plantation. I often forgot to take my medicine. (P15)
Furthermore, manual labor created high caloric needs that conflicted with dietary management, forcing compromises between survival demands and health maintenance.
The pressure is always like this: you have to work, and you have to eat. I know I should eat less, but when there’s meat, I can’t stop myself. I must eat. If I’m not full, I can’t work. (P4)
Discussion
The findings of this qualitative study offer interpretive insights into how participants experienced the SSEP and how they made sense of cognitive and behavioral changes over a 12-month period. Participants described multiple positive shifts—including restructured diabetes cognition, enhanced self-efficacy, reshaped mindsets, and reconstructed diabetes self-management behaviors. However, several individual and contextual factors also perceived by participants as constraining the persistence of these behavioral gains.
Interviewees described improvements in cognitive understanding, self-efficacy, and perceived behavioral capability, which are consistent with prior quantitative evidence on the psychosocial effects of the SSEP.3,19 Importantly, this qualitative inquiry deepens understanding by illustrating how participants narrated and interpreted these changes, extending interpretive depth beyond statistical outcomes. Most participants came from grassroots communities with limited education and financial resources, yet their narratives revealed a process of reinterpretation and re-empowerment: reframing diabetes from an uncontrollable burden into a manageable condition and rebuilding self-efficacy through mastery. From an interpretive perspective, enhanced self-efficacy co-occur with cognitive restructuring, while improved understanding was described by participants as provided the psychological foundation for sustained self-management. These patterns can be interpreted through the lens of self-efficacy theory and the previously established conceptual framework18,27–29 which offers a conceptual perspective for understanding participants experiences, rather than implying a direct causal relationship between knowledge acquisition, self-efficacy enhancement, and behavioral change.
This study further contributes to theory by situating participants’ accounts of self-efficacy within a broader cognitive–behavioral systems perspective. Self-efficacy was not described by participants as operating in isolation; rather, it interacted dynamically with knowledge, emotion, and environmental reinforcement to sustain change. Repeated practice and feedback fostered habit formation, which participants experienced as a gradual shift from deliberate, effortful regulation into more automatic self-management routines. This experiential shift can be interpreted using dual-process theory as reflecting movement between reflective (System 2) and intuitive (System 1) processes in diabetes self-management behaviors, rather than as evidence of a definitive or universal mechanistic transition.
Within this interpretive framework, cognitive restructuring was described by participants as enabling more deliberate, goal-directed decisions consistent with reflective System 2 processing.16 Through repetition and reinforcement, these decisions were often experienced as becoming increasingly automatic, guided by familiarity and accumulated experience. The SSEP’s visual dietary tools and heuristic cues were perceived by participants as cognitive bridges between conscious reasoning and everyday intuitive decision-making. Consequently, sustained diabetes management may be understood not only as a function of improved knowledge and motivation, but also as arising from the perceived integration of reflective learning with environmental design that supports automatic healthy choices.17
Beyond these transformative processes, Theme 5 illuminated participants’ post-program reflections as they sought to maintain newly acquired behaviors after completing the 12-month SSEP. Although barriers such as family responsibilities, financial strain, or comorbidities pre-existed, participants reframed these challenges in terms of how they impeded self-management once structured support ended. Their accounts reflected a transition from externally guided to self-regulated practice, highlighting the lived difficulties of sustaining learned behaviors in real-world contexts.
Four interrelated barriers—personal limitations, motivational decline, caregiving burdens, and economic hardship—were consistently described by participants as undermining long-term adherence. In contrast to studies of patients without DSME,8,10,15 these persistent barriers highlight that post-program decline may be perceived as stemming less from informational deficits than from enduring contextual and motivational pressures. Accordingly, education alone may not be sufficient for long-term maintenance. Continuous family engagement, community-based reinforcement, and supportive workplace or policy environments can be viewed as potentially important contextual supports, helping to bridge individual capability and environmental constraints and supporting the continuity of diabetes self-management behaviors beyond the program period.
Strength and Limitations
This is the first qualitative study conducted across multiple research centers and one of the few to explore participants’ perceptions and experiences after completing the SSEP over a 12-month follow-up. The study demonstrates how participants changed following the intervention and identifies both individual and environmental barriers that influenced this process. These qualitative insights, which could not be captured through quantitative methods alone, enrich the previously proposed conceptual framework and enhance understanding of the mechanisms underlying self-management improvement.
However, a limitation should be acknowledged: interviews were conducted only at the 12-month follow-up, without earlier or intermediate data points, restricting the ability to capture dynamic trajectories of participants’ perceptions and behavioral adaptation over time. Nevertheless, this study represents a theoretically informed reanalysis of qualitative data originally collected in 2018. By reinterpreting participants’ experiences through contemporary frameworks of self-efficacy and dual-process theory, and employing an updated reflexive thematic analysis approach, the study extends the explanatory depth of the original dataset and offers novel conceptual insights into the mechanisms of sustained diabetes self-management behaviors. Future longitudinal qualitative work could map temporal shifts in cognition, emotion, and habit formation to further refine this explanatory model.
Conclusions
This study advances theoretical and practical understanding of how the self-efficacy-focused structured education program (SSEP) facilitates cognitive and behavioral transformation in individuals with type 2 diabetes mellitus. Enhanced knowledge and self-efficacy jointly fostered cognitive restructuring, emotional adaptation, and the internalization of diabetes self-management behaviors into enduring habits.
By integrating self-efficacy theory with the dual-process perspective, this study elucidates the mechanism of behavioral consolidation—showing how reflective, goal-directed learning (System 2) progressively transitions into automatic, intuitive routines (System 1) through repetition and reinforcement. The SSEP’s visual tools and heuristic aids functioned as cognitive bridges that linked deliberate reasoning with intuitive daily choices, supporting this reflective-to-automatic shift.
Practically, these insights underscore that sustainable diabetes self-management behaviors arises from the synergy between reflective education and ecological behavioral design. Future SSEP iterations should embed System 1-oriented strategies—including contextual prompts, visual or environmental cues, and mobile-based nudges—to strengthen habit formation and real-world transfer. Continuous family engagement, community reinforcement, and enabling policy environments are also essential to maintain long-term behavioral persistence beyond structured programs.
Acknowledgment
The authors thank the nurses who assisted with the interviews and all interviewees who took part in this study. This work was supported by the China Scholarship Council (Grant No. 202408460019) and the Hainan Provincial Natural Science Foundation of China (Grant No. 825RC766).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. International Diabetes Federation. Idf diabetes atlas 2025; [cited June 23, 2025]. Available from: https://diabetesatlas.org/resources/idf-diabetes-atlas-2025/.
2. Chinese Diabetes Society. Chinese diabetes prevention and treatment guidelines (2024 edition). Chin J Diab. 2025;17(1):16–13. 10.13406/j.cnki.cyxb.003749.
3. Jiang X, Jiang H, Chen Y, et al. The effectiveness of a self-efficacy-focused structured education program (ssep) in improving metabolic control and psychological outcomes of type 2 diabetes patients: a 12-month follow-up of a multicenter randomized controlled trial. Diab Metab Syndr Obes. 2021;14:305–313. doi:10.2147/DMSO.S290029
4. Jiang X, Jiang H, Tao L, Li M. The cost-effectiveness analysis of self-efficacy-focused structured education program for patients with type 2 diabetes mellitus in mainland China setting. Front Public Health. 2021;9(9):767123. doi:10.3389/fpubh.2021.767123
5. Versluis A, Boels AM, Huijden MCG, Mijnsbergen MD, Rutten GEHM, Vos RC. Diabetes self-management education and support delivered by mobile health (mhealth) interventions for adults with type 2 diabetes-a systematic review and meta-analysis. Diabet Med. 2025;e70002. doi:10.1111/dme.70002
6. Romadlon DS, Tu Y, Chen Y, Hasan F, Kurniawan R, Chiu H. Comparative effects of diabetes self-management programs on type 2 diabetes clinical outcomes: a systematic review and network meta-analysis. Diab Metab Res Rev. 2024;40(6):e3840. doi:10.1002/dmrr.3840
7. Kiçaj E, Saliaj A, Çerçizaj R, Prifti V, Qirko S, Rogozea L. Navigating diabetes: enhancing self-management through education among diabetic people at the early stages of the disease-a systematic review. Int J Environ Res Public Health. 2024;21(5). doi:10.3390/ijerph21050522
8. Tuobenyiere J, Mensah GP, Korsah KA. Patient perspective on barriers in type 2 diabetes self-management: a qualitative study. Nurs Open. 2023;10(10):7003–7013. doi:10.1002/nop2.1956
9. Othman MM, Al-Wattary NA, Khudadad H, et al. Perspectives of persons with type 2 diabetes toward diabetes self-management: a qualitative study. Health Educ Behav. 2022;49(4):680–688. doi:10.1177/10901981221098373
10. Li H, Li Y, Wang J, Zhang Y, Ben S. Enablers and barriers to medication self-management in patients with type 2 diabetes: a qualitative study using the com-b model. Patient Prefer Adherence. 2025;19:485–501. doi:10.2147/PPA.S503350
11. Sim RRJ, Soon W, Smith HE, Griva K, Wong SKW. Understanding the preferences of young adults with type 2 diabetes mellitus with regard to diabetes self-management education: a qualitative study. BMJ Open. 2024;14(7):e86133. doi:10.1136/bmjopen-2024-086133
12. Robertson M, Paré GC, Costa I, Alvarado B, Duhn L, Plazas PC. “I could have stood a little more education rather than just: ‘hey, you’re diabetic man, make the best out of it’”: revisioning diabetes self-management education for older adults. Res Aging. 2023;45(7–8):563–573. doi:10.1177/01640275221138968
13. Bamuya C, Correia JC, Brady EM, et al. Use of the socio-ecological model to explore factors that influence the implementation of a diabetes structured education programme (extend project) inlilongwe, Malawi and Maputo, Mozambique: a qualitative study. Bmc Public Health. 2021;21(1):1355. doi:10.1186/s12889-021-11338-y
14. Coningsby I, Ainsworth B, Dack C. A qualitative study exploring the barriers to attending structured education programmes among adults with type 2 diabetes. Bmc Health Serv Res. 2022;22(1):584. doi:10.1186/s12913-022-07980-w
15. Allory E, Lucas H, Maury A, et al. Perspectives of deprived patients on diabetes self-management programmes delivered by the local primary care team: a qualitative study on facilitators and barriers for participation, in France. Bmc Health Serv Res. 2020;20(1):855. doi:10.1186/s12913-020-05715-3
16. Kahneman D. Thinking Fast and Slow. New York: Farrar, Straus and Giroux; 2011.
17. Marteau TM. Changing minds about changing behaviour. Lancet. 2018;391(10116):116–117. doi:10.1016/S0140-6736(17)33324-X
18. Jiang XJ. The Clinical Effectiveness, Behavior Change Mechanism and Economic Evaluation of Structured Education in Patients with Type 2 Diabetes. Beijing: Peking University; 2019.
19. Jiang X, Jiang H, Lu Y, et al. The effectiveness of a self-efficacy-focused structured education programme on adults with type 2 diabetes: a multicentre randomised controlled trial. J Clin Nurs. 2019;28(17–18):3299–3309. doi:10.1111/jocn.14908
20. Ye C, Zhou Q, Yang W, Tao L, Jiang X. Health economic evaluation of structured education programs for patients with diabetes: a systematic review. Front Public Health. 2024;12:1467178.
21. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (coreq): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
22. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523.
23. Liu Y, Jiang X, Jiang H, Lin K, Li M, Ji L. A culturally sensitive nurse-led structured education programme in patients with type 2 diabetes. Int J Nurs Pract. 2019;25(5):e12757. doi:10.1111/ijn.12757
24. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
25. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–597. doi:10.1080/2159676X.2019.1628806
26. Braun V, Clarke V. Toward good practice in thematic analysis: avoiding common problems and be(com)ing a knowing researcher. Int J Transgend Health. 2023;24(1):1–06. doi:10.1080/26895269.2022.2129597
27. Bandura A. Toward a psychology of human agency. Perspect Psychol Sci. 2006;1(2):164–180. doi:10.1111/j.1745-6916.2006.00011.x
28. Jiang X, Jiang H, Li M, Lu Y, Liu K, Sun X. The mediating role of self‐efficacy in shaping self‐management behaviors among adults with type 2 diabetes. Worldviews Evid Based Nurs. 2019;16(2):151–160.
29. Jiang X, Jiang H, Li M. The role of self-efficacy enhancement in improving self-management behavior for type 2 diabetes mellitus patients. Diab Metab Syndr Obes. 2024;17:3131–3138.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Role of Psychological Distress in the Assessment of Chronic Illness Care and Self-Management Behaviors of Elderly Patients with T2DM Chronic Complications
Sun X, Wang X, Zhou R, Deng W, Jiang J, Shi Y
Diabetes, Metabolic Syndrome and Obesity 2025, 18:185-196
Published Date: 22 January 2025
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025