Back to Journals » Psychology Research and Behavior Management » Volume 16
Coffee Consumption Behavior in Young Adults: Exploring Motivations, Frequencies, and Reporting Adverse Effects and Withdrawal Symptoms
Authors Lone A ![]() , Alnawah AK, Hadadi AS
, Alnawah AK, Hadadi AS ![]() , Alturkie FM
, Alturkie FM ![]() , Aldreweesh YA, Alhedhod AT
, Aldreweesh YA, Alhedhod AT
Received 6 August 2023
Accepted for publication 14 September 2023
Published 21 September 2023 Volume 2023:16 Pages 3925—3937
DOI https://doi.org/10.2147/PRBM.S427867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Ayoob Lone,1 Ahmed Khalid Alnawah,2 Abdulaziz S Hadadi,2 Fahad Mohammed Alturkie,2 Yousef Abdullah Aldreweesh,2 Azam Tarek Alhedhod2
1Department of Clinical Neuroscience, College of Medicine, King Faisal University, Alhasa, 31982, Saudi Arabia; 2College of Medicine, King Faisal University, Alhasa, 31982, Saudi Arabia
Correspondence: Ayoob Lone, Tel +966553039056, Email [email protected]
Background: Coffee consumption by young people has increased dramatically over the last decades as there are substantial evidence of the physiological, cognitive, and emotional effects of coffee consumption. To reduce the risk of consuming related harm, it is necessary to understand the consumer’s motivation for its use.
Objective: This study aimed to investigate coffee consumption behavior in young adults, assess the type of coffee consumption, explore motivation, document adverse effects and withdrawal symptoms of coffee intake.
Methods: A sample of 923 young adults were recruited voluntarily to complete a set of measures examining motivations, adverse effects, and withdrawal symptoms of coffee intake. Logistic regression analysis was performed to determine the association between coffee consumption and all independent variables. A p-value of 0.005 was considered as statistically significant.
Results: The results indicate that more than half of the participants consumed coffee. Coffee consumers were more like to be male, young adults, unmarried, poor sleep pattern (3– 5 hours), and smokers. Main motivations of coffee intake were those related to reinforcing effects. The prevalence of dripper coffee consumption (85.59%) was observed to be highest with 20.1% participants consuming coffee in 2– 3 times per day. Participants experienced restlessness, shaky, excited, difficulty in falling sleep, and fast heart beat as adverse effects of coffee consumption. Withdrawal symptoms such as headache, mood change, and tiredness were also noticed after consuming a high amount of coffee. Gender (p < 0.005), age (p < 0.003), family income (p < 0.004), BMI (p < 0.002) and sleeping pattern (p < 0.005) were found important variables associated with coffee intake.
Conclusion: The association reported in this study may allow for the implementation of appropriate strategies to address behaviors towards excessive coffee consumption and its link to an increased risk of poor health.
Keywords: coffee, motivation, adverse effects, withdrawal symptoms, young adults, Saudi Arabia
Introduction
Coffee is one of the most consumed beverages throughout the world,1,2 it offers delightful taste and fragrance, along with its ability to act as an antioxidant and potential physiological effect.3 Approximately 166.63 million 60 kilogram bags of coffee were consumed globally in 2020–2021, showing an increase over the previous year’s 164 million bags.4 Saudi Arabia is among the top 10 countries in terms of coffee consumption. According to the Saudi Press Agency (SPA) report, Saudi Arabia imports around 70,000–90,000 tons of every year and Saudi spends more than SR1 billion on coffee.5 Caffeinated beverages are tremendously consumed by young people as life styles have become more westernized. According to the current trends in food and beverage consumption, coffee is the most preferred food rather than a functional food containing caffeine. The majority of consumers, however, are unaware of the health risks associated with caffeine or the amount of it in their caffeinated beverages.6
Previous research indicated that caffeine has a variety of positive and negative effects on health, with a potentially positive effect when consumed normally and a negative impact when consumed excessively, but also the impact of caffeine depends on age, physiological state, and individual’s caffeine sensitivity and tolerance.1,2,7,8 Moreover, caffeine has well-known short-term effects on health, including central nervous system stimulation and its impact on psychomotor and cognitive functions.1,9,10 By triggering the central nervous system, among others, it affects the processes of sleep and wakefulness, enhances concentration, and lessens the feeling of being sleepy. If taken later in the day, higher doses may negatively affect sleep in a dose-dependent manner.2,7,11 Furthermore, caffeine activates the motor zone of the cerebral cortex, which may cause psychomotor agitation, irritability, anxiety, and insomnia. It may also increase urine production and exacerbate dyspeptic symptoms.2,9,10,12,13
There are more controversies surrounding caffeine’s potential long-term effects.14,15 Previous findings reported that caffeine improves the level of cholesterol and homocysteine in the blood.16 Moreover, consumption of caffeine products increases arterial wall stiffness, which leads to hypertension and increases the risk of ischemic heart disease.8,14,16 On the other hand, moderate caffeine consumption on a regular basis has positive health effects, including a decreased risk of cancer, coronary heart disease, metabolic disorders, and possibly a reduction in the risk of cognitive impairment.1,8 According to a recent study, the recommended daily intake of caffeine is between 300 and 400 mg/day or about 4–5 cups per day, for positive and safe health effects.8
Research has shown that several factors influence the consumption of food and beverages17 including those containing caffeine, such as expected outcome, hedonic, environmental and sociocultural influences. In addition, motivation for consumption may vary depends on the caffeine source and consumer demography. The Planned behavior theory18 explains why consumer motivation and expected outcome are likely to predict as well as describing particular caffeine intake behaviours. The proclaimed benefits of caffeine include improve alertness, endurance and combating fatigue.19 These positive effects are likely to encourage additional or continuous caffeine consumption, whereas negative effects, such as anxiety, nervousness and sleep disturbances are likely to discourage additional or continual caffeine consumption.20,21 Additionally, since genetics may determine whether an individual reacts favorably to caffeine, there will also be a genetic influence on the quantity of caffeine that a person consumes.22
Despite the popularity and prevalence of consumption, many studies are conducted on the consumption of caffeine and caffeinated energy drinks in Saudi Arabia.23–26 With growing concerns about excessive use of coffee consumption, it is important to investigate the prevalence of coffee consumed in Saudi Arabia’s young population. It is crucial to understand the type of coffee consumed and the motivation that lead to this consumption. In the present study, we further intend to identify the adverse effects and withdrawal symptoms of coffee intake.
Materials and Methods
Study Design
In this descriptive cross-sectional study, the participants were recruited from Alhasa Governorate of Saudi Arabia from December 2022 to April 2023. This study was conducted in accordance with the Helsinki Declaration for the research with human participants and received the required ethical approval from the Deanship of Scientific Research, King Faisal University, AlHasa, Saudi Arabia (KFU-REC-2022-DEC-ETHICS410). The purpose and demand of the study was explained to all study participants and the survey proceeded after all respondents provided written consent.
Participants
We recruited participants from Alhasa Governorate of Saudi Arabia through a convenient sampling method. A total of 986 young adults were recruited to participate in this study voluntarily, and 923 participants aged between 16 and 40 years (mean age = 26.88 ± 7.85 years) finally completed the questionnaire with a 93.61% response rate. The other 63 participants were excluded because of missing or incomplete answers of the survey items. The sample size for this study was calculated using Slovin’s formula, with a population size of 930 participants from a recently published study by Alfawaz et al25 with a confidence interval (CI) of 0.90, and margin of error of 5%. The inclusion criteria were the absence of any health problem impeding caffeine consumption, Saudi citizens, aged >16 years’ old, and signed informal consent. Participants who have one or more following reasons were excluded: <16 years’ old, non-Saudi, and history of physical and mental illness.
Data Collection
The following data were collected from the participants in five subsections to examine the motivations for coffee consumption, daily intake, adverse effects, withdrawal symptoms, and association of lifestyle factors, such as smoking habits and sleep duration.
Motivations for Coffee Consumption
An Arabic version of the previously validated Caffeine Motives Questionnaire27 was used to examine the motivations for coffee consumption among the study samples. This 21-item questionnaire comprises of four dimensions for the motivations of coffee consumption, ie, cognitive enhancement (6 items: alert, concentration, drowsiness, attention, energy, stay awake), negative affect relief (3 items: stress, anxiety, depression), reinforcement effect (9 items: headache relief, taste convenience, relax, social, crave, reward, cued craving, mood) and weight control (3 items: ingredient in diet pills, powerful diuretics, lose or control weight). Responses are obtained on a 5-point Likert scale ranging from 1 (Never) to 5 (Always). Total score is produced by adding each subscale score together that ranges from 21 to 105. In the present study, internal consistency reliability (Cronbach's alpha) of different subscales of Caffeine Motives Questionnaire were 0.89 (cognitive enhancement), 0.83 (negative affect relief), 0.86 (reinforcement effect), 0.79 (weight control). Internal consistency reliability of the scale for total score was 0.90.
Coffee Intake
A previously designed self-reported questionnaire was used to measure daily coffee intake.11 The frequency intake of common products containing caffeine was ascertained using the question ‘how often do you consume? The optons was “2–3 times daily”, “once in day”, 100“2–3 times in week”, “once in week”, “2–3 times in month”, “once in month”. Products included in the questionnaire were coffee preparation, including instant coffee, Arabic coffee, expresso, ice coffee, coffee dripper, plunger/dip coffee, and decaffeinated coffee. Coffee consumption was estimated from the intake of each coffee preparation contained in the questionnaire.
Coffee Consumption Trend
Participants answered yes/no questions about their coffee consumption behavior. This section also addressed withdrawal symptoms. Symptoms of caffeine withdrawal was measured by using self-reported questionnaire, which included headache, mood changes, marked tiredness, difficulty in concentration, and drowsiness. Moreover, some questions about adverse effects of coffee consumption were also included.
Demographic data including age, gender, area of residence, educational qualification, marital status, family type, and employment status. In addition, self-reported body weight and height were recorded. BMI was calculated as mass (kg) divided by the square of height (meters). BMI values used to classify the participants as follows: normal (<25kg/m2), overweight (25–29.9kg/ m2), and obese (≥30kg/m2). Participants were asked if they smoked (Yes/No) regarding cigarette use and then participants were classified as smokers and non-smokers. Sleep duration was also assessed by the amount of sleep per night.
Procedure
The process of translation and validation of the study tools was 3-step process. First, the questionnaire was translated to Arabic language by two bilingual professors (both fluent in English and Arabic), and the Arabic version was translated again in English by the other two bilingual professors. Second, feedback and suggestions from the experts were incorporated in the final questionnaire. Third, the final Arabic version was tested by 25 healthy volunteers recruited from the locality for a pilot study in order to confirm the reliability and validity of the questionnaire. Finally, these specialists approved the final version and the final version of the questionnaire was administered through personal contact. The participants were briefed about the estimated time needed to complete the survey and the study purpose. Moreover, the participants were informed about the confidentiality and anonymity policy.
Statistical Analysis
Statistical analysis was performed by using IBM, SPSS Statistics version 25.0 software (IBM, SPSS, Chicago, IL, USA). To maintain the homogeneous number of respondents throughout the study and in all analyses, only participants who provided all relevant information were included in the statistical analysis (N= 923). All categorical variables were presented as frequencies and percentages and their associations were estimated using Chi-square test. Mean and standard deviation (SD) were reported for the quantitative variables. An independent t-test was used to examine gender differences for coffee consumption. Logistic regression analysis was performed to determine the association between coffee consumption (Yes/No) and all independent variables. A p-value of 0.005 was considered as statistically significant.
Result
Demographic and Coffee Consumption Characteristics
Table 1 presents the demographic characteristics of the respondents. Nine hundred and twenty-three completed the questionnaire. The percentage of participants consuming coffee was higher (N= 492, 53.30%) than non-consumers (N= 431, 46.70%). The frequency of coffee consumption was significantly higher (p = 0.003) in male than female participants. The respondents whose age ranges from 19 years to 30 years were consuming significantly more coffee (p = 0.001) compared to other age groups. Results also demonstrated that a significant higher frequency of coffee consumption was observed in the unmarried sample than married participants (p = 0.002). In addition, the frequency of coffee consumption was significantly higher (p = 0.001) in participants who slept 3–5 hours daily. Increased coffee intake (p = 0.002) was observed among smokers compared to non-smokers. Significant difference was not found between coffee consumers and non-coffee consumers in terms of qualification, monthly income, employment status, area of residence, family type, and body mass index.
 |
Table 1 General Characteristics of the Participants in this Study |
Motivation for Coffee Consumption
The motivations for coffee consumption were compared according to gender. Independent t-test clearly showed (Table 2) a significant difference in motivations for the reinforcing effect. Mean scores of motivations for coffee consumption of male and female participants clearly indicate that female participant’s consuming coffee for reinforcing effect (M = 29.85, SD = 8.82) compared to their male counterparts (M = 26.80, SD = 8.72). However, no significant differences between males and females were found for cognitive enhancement, negative affect relief, weight control, and global CMQ scores.
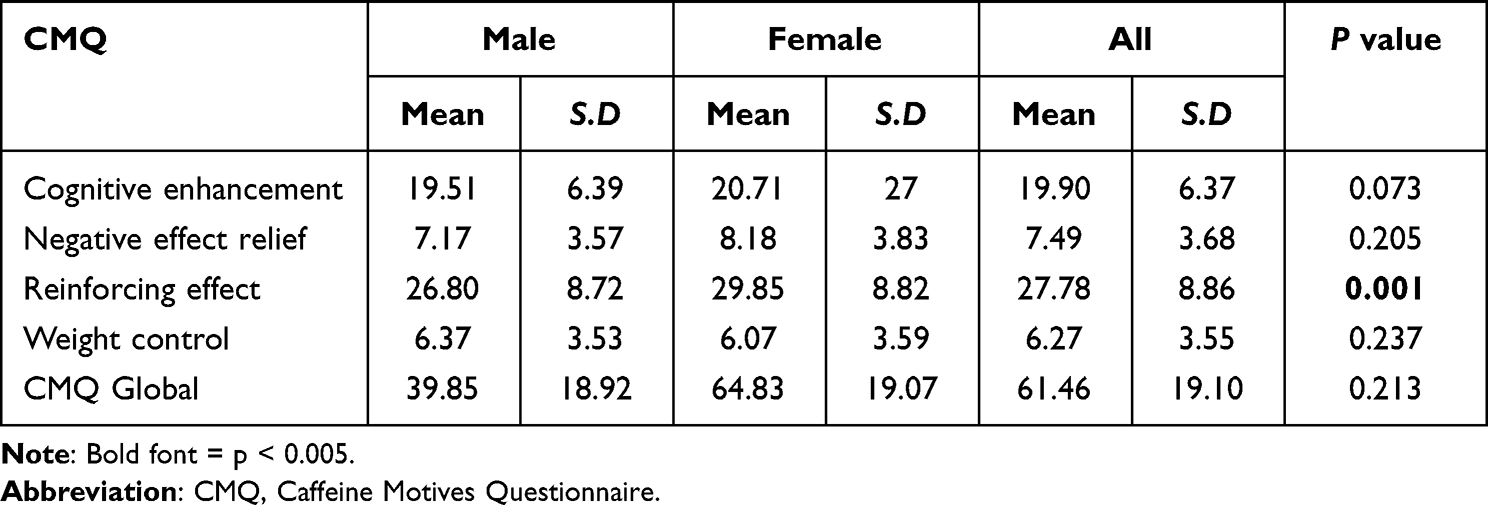 |
Table 2 Result of Coffee Consumption Motivations Among Male and Female Participants |
Coffee Consumption Trend
Among the different types of coffee consumed, the prevalence of dripper coffee consumption (N=790 (85.59%)) was observed (Table 3) to be the highest with 20.15% participant consumed coffee in 2–3 times per day, followed by Arabic coffee consumption (N=779, (84.40%)). The prevalence of ice coffee, instant coffee, small express, plunger coffee, and large expresso consumption was about 70.31%, 61.87%, 55.03%, 44.74%. 44.09%, respectively. The prevalence of decaffeinated coffee was the least consumed type of coffee (N=288, (31.20%)).
 |
Table 3 Frequency of Coffee Consumption by Type |
Coffee Adverse Effects and Withdrawal Symptoms
Table 4 shows the adverse effects and withdrawal symptoms experienced by the study participants after consuming coffee. Participants of the present study complaint of many adverse effects after consuming coffee, such as restlessness, shaky, excited, difficult falling, sleep, and fast heartbeat. Percentage of consuming coffee in male and female participants regarding adverse effects clearly indicated that male participants reported more adverse effects in terms of restlessness (71.42%), excited (65.11%), and difficulty of sleep (59.40%) compared to female counterparts (28.57%, 34.88%, 40.59% respectively). While female participants experienced shaky (52.42%) and fast heart beats (53.76%) in comparison to their counterpart male participants (47.57%, 46.23% respectively). However, significant differences between adverse effects of coffee consumption of male and female participants were not found for lack of energy, hot/red face, need to pee a lot, stomach upset, sudden leak, useful to comfort and difficulty in concentration.
 |
Table 4 Coffee Adverse Effects and Withdrawal Symptoms |
Regarding the withdrawal symptoms experienced by the study participants, the results clearly showed (Table 4) that withdrawal symptoms, such as headache (53.95%), mood change (58.50%), and tiredness (64.93%) were mostly experienced by male participants compared to female participants (46.04%, 41.49%, 35.06% respectively). However, no significant difference was found between male and female subjects for nausea and drowsiness.
Determinants of Coffee Consumption
Results of logistic regression analysis presented in Table 5 revealed gender (OR = 1.48, p value =0.005), age (OR = 1.01, p value =0.003), monthly income (OR = 0.59, p value =0.004), body mass index (OR = 3.49, p value =0.002), and smoking habits (OR = 1.30, p value =0.005), were significantly associated with coffee consumption. Analysis shows that coffee consumption was approximately one and half times more likely in male participants and about one time more likely in participants aged between 19 and 30 years old. The probability of coffee consumption was highest in participants with high family income levels. Moreover, coffee consumption was approximately three and a half times more likely in obese participants than in those with normal BMI. Moreover, coffee consumption was observed more in smokers than non-smokers. However, there was no statistically significant relationship between coffee consumption and participant’s qualification, employment status, marital status, area of residence, family type, and sleeping hours.
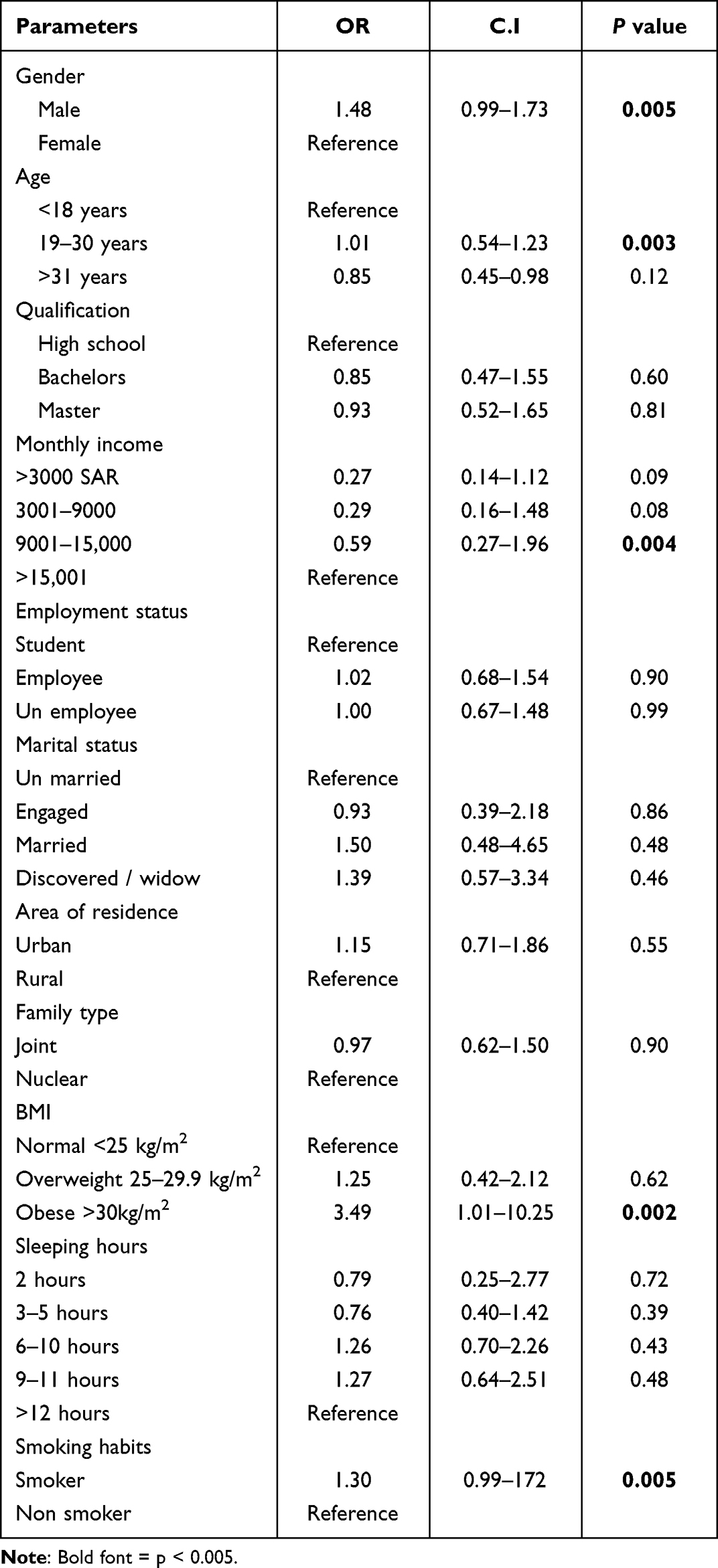 |
Table 5 Logistic Regression Model Determining Independent Predictors of Coffee Consumption |
Discussion
The present study was conducted to investigate the coffee consumption behavior, motivations, trend, adverse effects, and withdrawal symptoms in young adults. The results of the study reported a prevalence of more than half of the total (53.30%) study sample consumed coffee. This value is very similar to a study conducted in the general population in eastern Saudi Arabia.28 The data showed that male participants reported higher consumption of coffee compared to the female counterparts and these findings are in line with other studies.29,30 However, some studies did not find results in line with our research, although their subjects had a much lower average age than in the present study.11,31,32 Moreover, it is notable that females experienced more negative effects of caffeine consumption than males, which may condition the percentage of consumption to be higher in males.
The intake of caffeine depends on age and, therefore, the main dietary caffeine source vary as age advances.33 National Health and Nutrition Examination Surveys (NHANES) reported a positive correlation between age and total caffeine consumption until 45–65 years of age.34 Approximately 70% children and adolescents in the United States consume some form of caffeine on any given day, and around 89% of adults consume caffeinated beverages on a daily basis.35,36 Our results showed that participants whose age was 19–30 years consumed more coffee than other age groups, which is in agreement with previous studies.29,30 Pinhao et al37 reported that the age group between 30 and 40 years old was the one that consumed more caffeine, and in the second, people from 30 to 39 years old consumed caffeine similar to individuals more than 40 years of age.29,30 The consumption of coffee in older age may be higher because of rage and dependency.
The association between coffee consumption and marital status is still inconsistent. For instance, Deshmukh-Taskar and colleagues reported that married women consume caffeinated drinks nearly twice as frequently as unmarried women.38 However, a study conducted in Zayed University, United Arab Emirates, demonstrated that unmarried females consumed more coffee than married females,39 which is parallel to the present study. Furthermore, it was postulated that marital status and having children could bring changes in dietary habits and other lifestyle behaviors. Previous findings suggested that married people have a healthier dietary lifestyle compared to unmarried people, and this could be the main reason of less intake of coffee consumption among married people.40,41
Increased consumption of coffee has been also associated with poorer subjective sleep quality in university students.42,43 In agreement with these findings, in the present study, coffee intake was found to be related to poor sleep patterns. Effective sleep homeostasis has been linked to the effects of high adenosine concentrations during time awake and their dissipation during the sleep episode.44 Due to caffeine’s ability to block adenosine receptors,45 this mechanism may be disrupted, resulting in poorer sleep quality. Additionally, it has been suggested that caffeine may prevent the release of adenosine from melatonin.46 In humans, the regulation of the sleep-wake cycle is considered largely regulated by the neurohormone melatonin, whose levels begin to rise two hours before the usual bedtime.47 Therefore, caffeine consumption may alter melatonin’s common circadian rhythm, leading to sleep deprivation. In addition to the abovementioned factors, there may be other reasons that affect the sleep patterns such as stress, excessive usage of electronic gadgets before sleep, physical activities, and consumption of junk food.42
The present study demonstrated higher coffee intake among smokes than non-smokers. These results are similar to previous studies showing that smokers consume more coffee.31,42 Physiological, cognitive, and environmental factors may all contribute to the relationship between smoking and caffeine consumption.31 Smoking may increase the rate of caffeine metabolism,47 as a result, smokers must consume caffeine more frequently than non-smokers in order to maintain a similar effect. There are other factors such as stress, which could have similar effect on the use of both caffeine and nicotine leading to increased use of both.48 Previous studies reported that about 50% of the participants consumed more caffeine when experience stress.49
It is necessary to understand the motivations for coffee consumption and its misconceptions regarding its use. Previous studies demonstrated that college students believed that caffeine could use to enhance some aspects of mood, improve academic performance, feel more awake and alert, and to enjoy taste as well as to improve concentration.11,50,51 A study from Korea reported that the motivation for caffeine consumption was due to many reasons, such as social factors, alertness, health, mood, daily habits, and sensory effects.42 Since we observed that young adults consume coffee for reinforcing effects (eg, taste, convenience, relaxation, social craving, reward, and improving mood). Therefore, it is important to improve the consumer’s knowledge about the real effects of coffee consumption.
Among the different types of coffee consumed in the present study, the prevalence of dripper coffee consumption was observed to be highest with 2–3 times per day. The intake percentage of different types of coffee consumption ranges from 70.31% (ice coffee) to 44.09% (large expresso). However, a study conducted at King Saud University, Riyadh, Saudi Arabia, demonstrated a higher consumption of Arabic coffee,25 which is similar to our results. In Saudi Arabian culture, the use of Arabic coffee or “qahwa” is a regular practice during special occasions.52
Previous researches reported that caffeine consumption may have many side effects,2,9,10,14,53,54 including psychomotor agitation, irritability, restlessness and anxiety, and an increase in blood pressure and arrhythmias. Difficulty in falling sleep, or insomnia may also occur. The potential harmful effects may depend not only on the consumed dose, but also on individual sensitivity as well as the limited and lower ability to metabolize caffeine in the liver. The risk of adverse health effects increases in a particularly sensitive individuals, ie, those with slow caffeine metabolism.1,2 In agreement with these observations, the results of our study showed that participants reported restlessness, shaky, excited, difficult falling, sleep, and fast heartbeat. These adverse effects may only have occurred after taking the exceeded dose of coffee. There is strong evidence to suggest that caffeine withdrawal occurs when regular consumption is deprived. The participants of the present study reported various symptoms associated with their high coffee consumption, such as headache, mood change, and tiredness. However, it is not easy to link these withdrawal symptoms to the high amount of coffee consumption, many researches have shown a strong association between such symptoms and coffee consumption.42,55–57
Coffee consumption has been strongly associated with several demographic and lifestyle variables. Previous researches have not examined such an extensive series of demographic factors and controlled for their effects in multiple regression analyses. It is usually reported that males consume more coffee than females, as observed in this study, these results are parallel to the studies conducted in different contexts.29,30,37 Coffee consumption has been positively associated with age in several studies. In the present study, age was also associated with coffee consumption. Because of the culture and tradition of consuming coffee in Saudi Arabia, young adults consume coffee excessively.24 In this study, those aged 19 to 30 years consumed substantially more coffee than other age groups. Nevertheless, given the growing popularity of these products, continued monitoring of coffee by the young populations is warranted. Previous studies have also revealed a similar association of coffee intake with age.36,58
Coffee intake was also related to an individual’s socioeconomic status. The participants belong to a moderate range of family income (9001–15,000 SAR) consuming more coffee. Previous studies suggested a direct association between high household income levels and the prevalence of coffee consumption.38,59,60 Furthermore, adults with low socioeconomic status reported less consumption of caffeine than higher income adults.34 The association of coffee intake with body mass index (BMI) is still inconsistent with mixed data. Numerous biologically active substances found in coffee have positive effects on obesity and other related abnormalities. Studies have shown that coffee consumption and obesity have a direct,61 inverse62 and neutral relationship.63 The inconsistent impact of coffee on health can be attributed primarily to variations in coffee composition and intake trend (such as coffee type and intake amount). Various studies conducted in Saudi Arabia demonstrated a positive and significant association between coffee consumption and BMI among female students.60,64 The present study supports the above findings showing a direct relationship between coffee intake and BMI in young adults. The association between coffee consumption and poor sleep quality is still controversial. Many studies concluded that caffeine use disrupts the sleep patterns among adults,65–67 which is similar to the findings of our present study. In contrast, a study conducted in three European nations reported that caffeine did not cause difficulty in sleep after controlling for some demographics.68 There are other factors that affect sleep quality, such as electronic device usage, life style, and fast-food consumption.
One of the important strengths of the present study is that the motivations, adverse effects, and withdrawal symptoms of coffee consumption were examined first time in Saudi Arabia’s young adults. The second strength of this study is that a relatively close personal relationship between researchers and the study participants enable the authors to receive reliable and valid data. Because the researchers and the participants of this study belonged to Saudi Arabia, they shared language, religion, culture, and other attributes, which facilitated data acquisition and helped to get reliable and in-depth information. The researchers collected data in a congenial atmosphere, and with respect and understanding of their cultural background. This increased the likelihood of obtaining valid and reliable data.
Despite the strengths of the present study, this study presents some limitations that should be acknowledged. First, the present study confronts with the selection bias because the sample was taken from only one region of Saudi Arabia. Moreover, convenience sampling method was used to collect the sample was oblivious limitation. Therefore, the generalizability of our study should be carefully discussed. Second, due to its cross-sectional nature, no plausible causation can be obtained from our study. Third limitation of the study was sex disparity; our sample is mostly male, which made it impossible to general the results. Fourth, the majority of the participants were young adults, which represents an oblivious limitation in this study due to poor sample representativeness across all sociodemographic variables. Finally, this study did not measure the amount of coffee intake. Rather, it focused on the frequency of consumption of coffee. The caffeine content of products depends on the methods of preparation, brand, and serving size; hence variation exists.69 Measuring the amount of caffeine in products would not be accurate in self-reported studies; therefore, this study did not assess the actual caffeine amount. Future experimental studies to examine the retail caffeinated beverage products available in Saudi Arabia may be needed.
Conclusions
In the present study, more than half of this convenience sample consumes coffee, with the primary reason of consuming coffee for reinforcing effect. Moreover, the prevalence of dripper coffee consumption was observed to be the highest type of coffee consumed. Respondents experienced restlessness, shaky, excited, difficult falling sleep, and fast heartbeat as adverse effects of coffee consumption. Withdrawal symptoms such as headache, mood change, and tiredness were also reported after consuming a high amount of coffee. Gender, age, monthly income, BMI, and smoking habits are particularly important variables associated with coffee intake. Associations reported in the present study could allow implementing appropriate strategies to address behaviors towards excessive coffee consumption and its link to increased risk of poor health. This information from this study contributes to understanding the motivation behind coffee consumption in the young population of Saudi Arabia and provides knowledge on which to develop strategies to reduce the excess coffee consumption in this group. Considering the findings of this research as a baseline and adding more information such as the motives and profile of coffee, further research will be needed to continue monitoring the consumption, adverse effects and withdrawal symptoms of coffee among young adults in Saudi Arabia.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Deanship of Scientific Research, King Faisal University, Saudi Arabia.
Data Sharing Statement
The data that support our findings can be found through directly asking the corresponding author.
Informed Consent Statement
Informed consent was obtained from all participants, except for participants <18 years of age, the written consent was taken from their parents and elder brothers.
Author Contributions
All authors made a significant contribution to the work reported whether that is in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article, gave final approval of the version to be published; have agreed on the journal to the article has been submitted and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Deanship of Scientific Research, King Faisal University, Alhasa, Saudi Arabia (Grant No. GRANT4148).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Barrea L, Pugliese G, Frias-Toral E, et al. Coffee consumption, health benefits and side effects: a narrative review and update for dietitians and nutritionists. Crit Rev Food Sci Nutr. 2023;63(9):1238–1261.
2. dePaula J, Farah A. Caffeine consumption through coffee: content in the beverage, metabolism, health benefits and risks. Beverages. 2019;5(2):37. doi:10.3390/beverages5020037
3. Vignoli JA, Viegas MC, Bassoli DG, Benassi MDT. Roasting process affects differently the bioactive compounds and the antioxidant activity of Arabica and Robusta coffees. Food Res Int. 2014;61:279–285. doi:10.1016/j.foodres.2013.06.006
4. Global coffee consumption 2020/21. Statista. Available from: https://www.statista.com/statistics/292595/global-coffee-consumption/.
5. Saudi coffee industry to join top table of global producers. Arab News. Available from: https://www.arabnews.com/node/2277846/amp.
6. Mitchell DC, Knight CA, Hockenberry J, Teplansky R, Hartman TJ. Beverage Caffeine Intakes in the US. Food Chem Toxicol. 2014;63:136–142. doi:10.1016/j.fct.2013.10.042
7. Booth N, Saxton J, Rodda SN. Estimates of caffeine use disorder, caffeine withdrawal, harm and help-seeking in New Zealand: a cross-sectional survey. Addict Behav. 2020;109:106470. doi:10.1016/j.addbeh.2020.106470
8. Grosso G, Godos J, Galvano F, Giovannucci EL. Coffee, caffeine, and health outcomes: an umbrella review. Annu Rev Nutr. 2017;37(1):131–156. doi:10.1146/annurev-nutr-071816-064941
9. Temple JL, Bernard C, Lipshultz SE, Czachor JD, Westphal JA, Mestre MA. The safety of ingested caffeine: a comprehensive review. Front Psychiatry. 2017;8:80. doi:10.3389/fpsyt.2017.00080
10. Wikoff D, Welsh BT, Henderson R, et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem Toxicol. 2017;109(1):585–648.
11. Riera-Sampol A, Rodas L, Martínez S, Moir HJ, Tauler P. Caffeine intake among undergraduate students: sex differences, sources, motivations, and associations with smoking status and self-reported sleep quality. Nutr. 2022;14(8):1661.
12. Paz-Graniel I, Kose J, Babio N, et al. Caffeine intake and its sex-specific association with general anxiety: a cross-sectional analysis among general population adults. Nutr. 2022;14(6):1242.
13. Poole R, Kennedy OJ, Roderick P, Fallowfield JA, Hayes PC, Parkes J. Coffee consumption and health: umbrella review of meta-analyses of multiple health outcomes. BMJ. 2017;22(359):5024. doi:10.1136/bmj.j5024
14. Ding M, Bhupathiraju SN, Satija A, van Dam RM, Hu FB. Long-term coffee consumption and risk of cardiovascular disease: a systematic review and a dose-response meta-analysis of prospective cohort studies. Circulation. 2014;129(6):643–659. doi:10.1161/CIRCULATIONAHA.113.005925
15. Gökcen BB, Şanlier N. Coffee consumption and disease correlations. Crit Rev Food Sci Nutr. 2019;59(2):336–348. doi:10.1080/10408398.2017.1369391
16. Jee SH, He J, Appel LJ, Whelton PK, Suh I, Klag MJ. Coffee consumption and serum lipids: a meta-analysis of randomized controlled clinical trials. Am J Epidemiol. 2001;153(4):353–362. doi:10.1093/aje/153.4.353
17. Baranowski T, Cullen KW, Baranowski J. Psychosocial correlates of dietary intake: advancing dietary intervention. Annu Rev Nutr. 1999;19(1):17–40. doi:10.1146/annurev.nutr.19.1.17
18. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
19. Puckeridge M, Fulcher BD, Phillips AJK, Robinson PA. Incorporation of caffeine into a quantitative model of fatigue and sleep. J Theor Biol. 2011;273(1):44–54. doi:10.1016/j.jtbi.2010.12.018
20. Lorist MM, Tops M. Caffeine, fatigue, and cognition. Brain Cogn. 2003;53(1):82–94. doi:10.1016/S0278-2626(03)00206-9
21. Smith AP. Caffeine at work. Hum Psychopharmacol. 2005;20(6):441–445. doi:10.1002/hup.705
22. Cornelis MC, El-Sohemy A, Campos H. Genetic polymorphism of the adenosine A (2A) receptor is associated with habitual caffeine consumption. Am J Clin Nutr. 2007;86(1):240–244. doi:10.1093/ajcn/86.1.240
23. Almalki AA, Alqarni MA, Homsi AM, Feda YAA, Aljabri MK. Caffeine consumption among dental students in Umm Al-Qura University. Int Dent J Stud Res. 2016;3(4):170–173.
24. Faris MA. Patterns of caffeinated energy drinks consumption among adolescents and adults in Hail, Saudi Arabia. Food Nutr Sci. 2014;5(2):158–168.
25. Alfawaz HA, Khan N, Yakout SM, et al. Prevalence, predictors, and awareness of coffee consumption and its trend among Saudi female students. Int J Environ Res Public Health. 2020;17(19):7020. doi:10.3390/ijerph17197020
26. Al Shoshan A. Predictors of caffeine consumption among young women. Pak J Nutr. 2007;6(6):597–602. doi:10.3923/pjn.2007.597.602
27. Irons J, Heinz A, Bassett D, et al. Development and initial validation of the caffeine motives questionnaire. J Caffeine Res. 2014;4:49–55. doi:10.1089/jcr.2014.0002
28. Alawadh RA, Abid N, Alsaad AS, Aljohar HI, Alharbi MM, Alhussain FK. Arabic coffee consumption and its correlation to obesity among the general population in the Eastern Province, Kingdom of Saudi Arabia. Cureus. 2022;14(10):e30848. doi:10.7759/cureus.30848
29. Knapik JJ, Steelman RA, Trone DW, Farina EK, Lieberman HR. Prevalence of caffeine consumers, daily caffeine consumption, and factors associated with caffeine use among active duty United States military personnel. Nutr J. 2022;21(1):22. doi:10.1186/s12937-022-00774-0
30. Batista P, Peixoto J, Oliveira-Silva P. An exploratory study about the characterization of caffeine consumption in a Portuguese sample. Behav Sci. 2022;12(10):386. doi:10.3390/bs12100386
31. Mahoney CR, Giles GE, Marriott BP, et al. Intake of caffeine from all sources and reasons for use by college students. Clin Nutr Edinb Scotl. 2019;38(2):668–675. doi:10.1016/j.clnu.2018.04.004
32. Kharaba Z, Sammani N, Ashour S, et al. Caffeine consumption among various university students in the UAE, exploring the frequencies, different sources and reporting adverse effects and withdrawal symptoms. J Nutr Metab. 2022;2022:5762299. doi:10.1155/2022/5762299
33. Ahluwalia N, Herrick K, Moshfegh A, Rybak M. Caffeine intake among children in the United States and 10-year trends: 2001–2010. Am J Clin Nutr. 2014;100(4):1124–1132. doi:10.3945/ajcn.113.082172
34. Tran NL, Barraj LM, Bi X, Jack MM. Trends and patterns of caffeine consumption among US teenagers and young adults, NHANES 2003–2012. Food Chem Toxicol. 2016;94:227–242. doi:10.1016/j.fct.2016.06.007
35. Branum AM, Rossen LM, Schoendorf KC. Trends in caffeine intake among US children and adolescents. Pediatrics. 2014;133(3):386–393. doi:10.1542/peds.2013-2877
36. Fulgoni VL, Keast DR, Lieberman HR. Trends in intake and sources of caffeine in the diets of US adults: 2001–2010. Am J Clin Nutr. 2015;101(5):1081–1087. doi:10.3945/ajcn.113.080077
37. Pinhão S, Poínhos R, Franchini B, et al. Avaliação Da Ingestão Energética e Em Macronutrientes Da População Adulta Portuguesa [Evaluation of energetic and macronutrients intake in the adult Portuguese population]. Rev Port Saúde Pública. 2016;34(3):220–235. doi:10.1016/j.rpsp.2016.06.004
38. Deshmukh-Taskar P, Nicklas TA, Yang SJ, Berenson GS. Does food group consumption vary by differences in socioeconomic, demographic, and lifestyle factors in young adults? The Bogalusa Heart Study. J Am Diet Assoc. 2007;107(2):223–234. doi:10.1016/j.jada.2006.11.004
39. Ghali RMA, Shaibi HA, Majed HA, Haroun D. Caffeine consumption among Zayed University Students in Dubai, United Arab Emirates: a cross-sectional study. Arab J Nutr Exerc. 2016;131–141. doi:10.18502/ajne.v1i3.1230
40. Heo M, Kim RS, Wylie-Rosett J, Allison DB, Heymsfield SB, Faith MS. Inverse association between fruit and vegetable intake and BMI even after controlling for demographic, socioeconomic and lifestyle factors. Obes Facts. 2011;4(6):449–455. doi:10.1159/000335279
41. Conklin AI, Forouhi NG, Surtees P, Khaw KT, Wareham NJ, Monsivais P. Social relationships and healthful dietary behaviour: evidence from over-50s in the EPIC cohort, UK. Soc Sci Med. 2014;100(100):167–175. doi:10.1016/j.socscimed.2013.08.018
42. Choi J. Motivations influencing caffeine consumption behaviors among college students in Korea: associations with sleep quality. Nutrients. 2020;12(4):953. doi:10.3390/nu12040953
43. Brick CA, Seely DL, Palermo TM. Association between sleep hygiene and sleep quality in medical students. Behav Sleep Med. 2010;8(2):113–121. doi:10.1080/15402001003622925
44. Landolt HP. Sleep homeostasis: a role for adenosine in humans? Biochem Pharmacol. 2008;75(11):2070–2079. doi:10.1016/j.bcp.2008.02.024
45. Fredholm BB, Bättig K, Holmén J, Nehlig A, Zvartau EE. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol Rev. 1999;51(1):83–133.
46. Shilo L, Sabbah H, Hadari R, et al. The effects of coffee consumption on sleep and melatonin secretion. Sleep Med. 2002;3(3):271–273. doi:10.1016/S1389-9457(02)00015-1
47. Carrillo JA, Benítez J. Caffeine metabolism in a healthy Spanish population: n-acetylator phenotype and oxidation pathways. Clin Pharmacol Ther. 1994;55(3):293–304. doi:10.1038/clpt.1994.30
48. Swanson JA, Lee JW, Hopp JW. Caffeine and nicotine: a review of their joint use and possible interactive effects in tobacco withdrawal. Addict Behav. 1994;19(3):229–256. doi:10.1016/0306-4603(94)90027-2
49. Ratliff-Crain J, Kane J. Predictors for altering caffeine consumption during stress. Addict Behav. 1995;20(4):509–516. doi:10.1016/0306-4603(95)00012-2
50. Brice CF, Smith AP. Effects of caffeine on mood and performance: a study of realistic consumption. Psychopharmacology. 2002;164(2):188–192. doi:10.1007/s00213-002-1175-2
51. Ágoston C, Urbán R, Király O, Griffiths MD, Rogers PJ, Demetrovics Z. Why do you drink caffeine? The development of the Motives for Caffeine Consumption Questionnaire (MCCQ) and its relationship with gender, age and the types of caffeinated beverages. Int J Ment Health Addict. 2018;16(4):981–999. doi:10.1007/s11469-017-9822-3
52. Al-Othman A, Al-Musharaf S, Al-Daghri NM, et al. Tea and coffee consumption in relation to vitamin D and calcium levels in Saudi adolescents. Nutr J. 2012;11(1):56. doi:10.1186/1475-2891-11-56
53. Cornelis MC. The impact of caffeine and coffee on human health. Nutrients. 2019;11(2):416. doi:10.3390/nu11020416
54. Willson C. The clinical toxicology of caffeine: a review and case study. Toxicol Rep. 2018;5:1140–1152. doi:10.1016/j.toxrep.2018.11.002
55. Comer SD, Haney M, Foltin RW, Fischman MW. Effects of caffeine withdrawal on humans living in a residential laboratory. Exp Clin Psychopharmacol. 1997;5(4):399–403. doi:10.1037/1064-1297.5.4.399
56. Juliano LM, Griffiths RR. A critical review of caffeine withdrawal: empirical validation of symptoms and signs, incidence, severity, and associated features. Psychopharmacology. 2004;176(1):1–29. doi:10.1007/s00213-004-2000-x
57. Amer SA, AlAmri FA, AlRadini FA, et al. Caffeine addiction and determinants of caffeine consumption among health care providers: a descriptive national study. Eur Rev Med Pharmacol Sci. 2023;27(8):3230–3242. doi:10.26355/eurrev_202304_32093
58. Rybak ME, Sternberg MR, Pao CI, Ahluwalia N, Pfeiffer CM. Urine excretion of caffeine and select caffeine metabolites is common in the US population and associated with caffeine intake. J Nutr. 2015;145(4):766–774. doi:10.3945/jn.114.205476
59. Drewnowski A, Rehm CD. Sources of caffeine in diets of US children and adults: trends by beverage type and purchase location. Nutr. 2016;8(3):154.
60. Je Y, Jeong S, Park T. Coffee consumption patterns in Korean adults: the Korean National Health and Nutrition Examination Survey (2001–2011). Asia Pac J Clin Nutr. 2014;23(4):691–702. doi:10.6133/apjcn.2014.23.4.11
61. Lee J, Kim HY, Kim J. Coffee consumption and the risk of obesity in Korean women. Nutrients. 2017;9(12):1340. doi:10.3390/nu9121340
62. Maki C, Funakoshi-Tago M, Aoyagi R, et al. Coffee extract inhibits adipogenesis in 3T3-L1 preadipocyes by interrupting insulin signaling through the downregulation of IRS1. PLoS One. 2017;12(3):e0173264. doi:10.1371/journal.pone.0173264
63. Larsen SC, Mikkelsen ML, Frederiksen P, Heitmann BL. Habitual coffee consumption and changes in measures of adiposity: a comprehensive study of longitudinal associations. Int J Obes. 2018;42(4):880–886. doi:10.1038/ijo.2017.310
64. Jalloun RA, Alhathlool MH. Arabic coffee consumption and the risk of obesity among Saudi’s female population. J Food Sci. 2020;13(1):59–67.
65. O’Callaghan F, Muurlink O, Reid N. Effects of caffeine on sleep quality and daytime functioning. Risk Manag Healthc Policy. 2018;11:263–271. doi:10.2147/RMHP.S156404
66. Ramakrishnan S, Wesensten NJ, Kamimori GH, Moon JE, Balkin TJ, Reifman J. A unified model of performance for predicting the effects of sleep and caffeine. Sleep. 2016;39(10):1827–1841. doi:10.5665/sleep.6164
67. Park S, Lee Y, Lee JH. Association between energy drink intake, sleep, stress, and suicidality in Korean adolescents: energy drink use in isolation or in combination with junk food consumption. Nutr J. 2016;15(1):87. doi:10.1186/s12937-016-0204-7
68. Janson C, Gislason T, De Backer W, et al. Prevalence of sleep disturbances among young adults in three European countries. Sleep. 1995;18(7):589–597.
69. Nawrot P, Jordan S, Eastwood J, Rotstein J, Hugenholtz A, Feeley M. Effects of caffeine on human health. Food Addit Contam. 2003;20(1):1–30. doi:10.1080/0265203021000007840
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Job Motivation and Satisfaction Among Female Pharmacists Working in Private Pharmacy Professional Sectors in Saudi Arabia
Al-Omar HA, Khurshid F, Sayed SK, Alotaibi WH, Almutairi RM, Arafah AM, Mansy W, Alshathry S
Risk Management and Healthcare Policy 2022, 15:1383-1394
Published Date: 21 July 2022