Back to Journals » International Journal of General Medicine » Volume 16
Coagulation Parameters in Post-Covid-19 Condition in Relation to Various Titers of Anti-SARS-CoV-2 IgG in Blood Plasma
Authors Strubchevska K ![]() , Rachkovska A
, Rachkovska A ![]() , Krenytska D, Karbovskyy V, Kozyk M, Secor B, Raksha N, Vovk T, Savchuk O
, Krenytska D, Karbovskyy V, Kozyk M, Secor B, Raksha N, Vovk T, Savchuk O ![]() , Falalyeyeva T
, Falalyeyeva T ![]() , Kaminsky R, Ostapchenko L
, Kaminsky R, Ostapchenko L
Received 12 June 2023
Accepted for publication 30 November 2023
Published 27 December 2023 Volume 2023:16 Pages 6127—6135
DOI https://doi.org/10.2147/IJGM.S425496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Kateryna Strubchevska,1 Antonina Rachkovska,2 Daryna Krenytska,2 Vitalii Karbovskyy,3 Marko Kozyk,1 Benjamin Secor,4 Nataliia Raksha,2 Tetiana Vovk,2 Olexii Savchuk,2 Tetyana Falalyeyeva,2 Rostyslav Kaminsky,5 Liudmyla Ostapchenko2
1Department of Internal Medicine, Corewell Health William Beaumont University Hospital, Royal Oak, MI, USA; 2Department of Internal Medicine, Taras Shevchenko National University of Kyiv, Kyiv, Ukraine; 3Department of Internal Medicine, LLS Biopharma-Plasa, Kyiv, Ukraine; 4Department of Internal Medicine, Oakland University William Beaumont School of Medicine, Auburn Hills, MI, USA; 5Department Educational-Scientific Center ”Institute of Biology and Medicine”, Taras Shevchenko National University of Kyiv, Kyiv, Ukraine
Correspondence: Marko Kozyk, 3601 W 13 Mile Road, Royal Oak, MI, 48073, Tel +1-305-773-5089, Email [email protected]
Background and Objectives: Post-COVID-19 condition is thought to affect 10– 20% of people at least 3 months after a diagnosis of COVID-19 and two months of symptoms. Post-COVID-19 condition presents itself with many clinical effects with varying degrees of severity ranging from a mild cough to a life-threatening coagulopathy. Our study aimed to identify a relationship between the titers of anti-SARS-CoV-2 IgG and anticoagulation parameters: antithrombin III (ATIII), protein C (PC) and thrombomodulin (TM).
Materials and Methods: Blood plasma was collected from healthy donors aged 25– 45 who had recovered from COVID-19 3– 6 months ago and their titers of anti-SARS-CoV-2 IgG and ATIII, PC, and TM were measured.
Results: We found that concentrations and activities of key anticoagulation parameters (ATIII, PC, and TM) measured in donor plasma during the post-COVID-19 varied in relation to the titers of anti-SARS-CoV-2 IgG.
Conclusion: While we identified a dysfunction of anticoagulation parameters in patients with post-COVID-19, we aim to explore the subpopulation antibody IgG fraction directly using in vivo and in vitro experiments with the possibility to contribute to the development of treatment options for post-COVID-19 conditions.
Keywords: long-COVID, antithrombin III, thrombomodulin, protein C
Introduction
Post-COVID-19 condition (long COVID-19, post-acute COVID-19, long-term effects of COVID-19) is an emerging health problem in people that had an active COVID-19 infection within the past 4–6 months. There is an array of presenting clinical symptoms in post-COVID-19 condition including, but not limited to, fatigue, muscle weakness, difficulty concentrating, depression/anxiety, diarrhea, cough, chest pain, and shortness of breath.1 These symptoms can last for weeks to years and even progress to severe multiple organ dysfunction, such as liver failure, lung failure, and acute kidney injury.2 The causative agent, SARS-CoV-2, is a virus that belongs to the coronavirus family which has led to the global pandemic known as COVID-19. The coronavirus family is a large group of viruses known for causing respiratory disease ranging from a common cold to respiratory failure. The primary mode of transmission is through respiratory droplets and contact via fomites, while there is growing data suggesting airborne transmission may also be a major contributing factor.3
Scientists have a focus on studying hemostasis damage after COVID-19 because coagulation disorders can often result in serious injury or death. For cases in clinical practice regarding continued hypercoagulation status after COVID-19, there is not enough information today. The mechanisms underlying the development of chronic coagulation pathology are being studied to identify factors that cause an imbalance in the regulation of the coagulation and anticoagulation systems. Several studies have established the presence of large anomalous amyloid and fibrinogen deposits in blood after COVID-19.4 Accordingly, coagulation potential increases due to acute inflammatory processes persists after recovery from COVID-19. Thus, the study of dysfunction of the anticoagulation system has become more of an urgent issue indicating that research on post-COVID-19 condition should focus on the assessment of both coagulation and anticoagulation statuses in patients.
The physiological anticoagulation mechanism is the basic component of fibrin clot formation stability and its cleavage into degradation products. Activation of the anticoagulation cascade leads to a reduction in thrombin generation and, consequently, prevents insoluble fibrin accumulation. There are three key anticoagulation proteins: antithrombin III (ATIII), thrombomodulin (TM) and protein C (PC).5 ATIII is the most powerful serine protease inhibitor among anticoagulation proteins, which has a binding domain to thrombin, factor Xa, and IXa for direct inactivation.6 PC participates in the inactivation of tenase and prothrombinase complex formation, which consist of FVIIIa with FIXa and FVa with FXa, respectively. This is the basis for the inhibition of the common pathway of blood coagulation, similar to that of ATIII. Remarkably, only the interaction between thrombin and TM is capable of activating PC. Therefore, PC and TM are interdependent anticoagulant proteins.7
Currently, patients are often recommended anticoagulant agents from the early to late stages of SARS-CoV-2 infection and after discharge in the post-COVID-19 period.8 Our study aimed to estimate the anticoagulation parameters, such as ATIII, PC and TM, based on the titers of anti-SARS-CoV-2 IgG.
Materials and Methods
Blood plasma was collected from donors who had recovered from COVID-19 3–6 months ago. Participants ranged in age from 25 to 45 years old. The blood plasma of donors was given to us with determined anti-SARS-CoV-2 IgG titers for scientific research.
The titers of anti-SARS-CoV-2 IgG in the blood plasma were determined using a chemiluminescent microparticle immunoassay (Abbott Laboratories, USA) according to the manufacturer’s instructions. All donors were selected based on their anti-SARS-CoV-2 IgG titers. We had donor groups with anti-SARS-CoV-2 IgG titers: 0 (n = 20), 10 ± 3 (n=20), 55 ± 5 (n=20), 65 ± 5 (n=20), 75 ± 5 (n=20), 85 ± 5 (n=20), 95 ± 5 (n=20), 125 ± 5 (n=20) and 175 ± 5 (n=20) Index (S/C). People with severe cardiovascular and cerebrovascular diseases, vitamin K deficiency, traumatic coagulation disorders; people taking anticoagulant therapy; and people with other disorders that can affect hemostasis system were excluded from the study.
All donors voluntarily agreed to participate in the study and provided written informed consent. Determination of APTT, TT. APTT and TT were measured by coagulation analyzer Sysmex CS-2000i using Dade Actin and Test Trombin reagents (Siemens, Germany), respectively. The detection was performed according to the manufacturer’s instructions.
Determination of activity of ATIII started with plasma diluted 1:30 by 0.05 M Tris-HCl buffer (pH 7.4). Thrombin with heparin was added at a final concentration 0.2 IU. Thrombin residue was measured using chromogenic substrate S2238 at a final concentration of 3 mM. Using reagents were lyophilized commercial preparations (RENAU, Ukraine). Optical density of samples was measured at a wavelength of 405 nm on the microplate spectrophotometer BioTek Instruments, Inc. The activity of ATIII was calculated according to the amount of released para-nitroaniline, which was inversely proportional to the activity of ATIII in the plasma sample.
Isolation of ATIII from blood plasma began with the fraction of ATIII was received by affinity chromatography using a BioLogic DuoFlow chromatography, (Bio-Rad, USA) on a heparin-Sepharose column. The column equilibration and sample application were performed with 0.1 M Tris-HCl buffer, 0.01 M sodium citrate buffer (pH 7.4), containing 0.225 M NaCl, then the column was washed with 0.1 M Tris-HCl, 0.01 M sodium citrate buffer (pH 7.4), containing 0.33 M NaCl. The elution step was performed with 0.1 M Tris-HCl, 0.01 M sodium citrate buffer (pH 7.4), containing 2 M NaCl. The stable flow rate was 3 mL/min. The concentration of the ATIII was determined using the Bradford method.9
Protein C activator was added, 50 µL, to samples according to the manufacturer’s instructions. The chromogenic substrate S2366 was added to the mixture at a final concentration of 3 mM. Using reagents were lyophilized commercial preparations (RENAU, Ukraine). Optical density of samples was measured at a wavelength of 405 nm on the microplate spectrophotometer BioTek Instruments, Inc. The activity of protein C was calculated according to the amount of released para-nitroaniline, which was directly proportional to the activity of protein C in the plasma sample.10
The levels of PC or TM were determined using enzyme-linked immunosorbent assay (ELISA).11,12 ELISA plates were coated with a sample of donor plasma diluted 1:100 with 0.05 M Tris-HCl buffer (pH 7.4) and incubated at 37°C for 1 hour. The plates were washed with 0.05 M Tris-HCl buffer (pH 7.4) containing 0.1% Tween-20, then coated with 3% nonfat dry milk to block any free binding sites and incubated overnight. The plates were washed again. The microplates were coated with mouse polyclonal antibodies (Sigma-Aldrich, USA) against the targeted antigens and incubated at 37°C for 1 hour. The microplates were washed and incubated with the appropriate secondary antibodies (Sigma-Aldrich, USA), which were conjugated to horseradish peroxidase at 37°C for 1 hour. The reaction was visualized using horseradish peroxidase substrate (o-phenylenediamine and hydrogen peroxide). The reaction was stopped by 2.5 M H2SO4. Changes in optical absorption were measured using a microplate spectrophotometer (µQuant BioTek Instruments, BioTek, USA) at a wavelength of 492 nm.
Statistical analysis of the results was performed using the computer program STATISTICA. The arithmetic mean and mean squared error indicators were calculated. The hypothesis of normal distribution was checked using the Shapiro–Wilk and Kolmogorov–Smirnov tests. All donor groups showed a normal distribution. Therefore, the differences between the samples were determined using one-way analysis of variance (ANOVA) with Tukey’s criterion. Differences were statistically significant when p-value was less than 0.05.
Results
We recorded serum changes in the analyzed parameters of APTT, TT, ATIII, PC, and TM in reference to the donor groups categorized by the titers of anti-SARS-CoV-2 IgG. We selected the minimum and maximum values of diagnostic parameters among the donor groups with titers of anti-SARS-CoV-2 IgG ≥ 10 ± 3 Index (S/C). The donor group with a titer of anti-SARS-CoV-2 IgG - 0 Index (S/C) was chosen as the reference point.
Our investigation began with an assessment of the status of intrinsic and common coagulation pathways. For this purpose, we measured the APTT and TT in the blood plasma of donors. Figure 1 shows that donor groups with titers of anti-SARS-CoV-2 IgG - 75 ± 5 and 85 ± 5 Index (S/C) had maximum and minimum values of APTT, respectively. Although the APTT in donors with IgG - 75 ± 5 Index (S/C) was higher by 35.35% than that in donors with IgG - 0 Index (S/C), a statistically significant difference was not observed between groups with IgG - 0 and 85 ± 5 Index (S/C), p > 0.05. In addition, the maximum APTT increased by 35.02% compared with the minimum APTT. Figure 2 shows that TT values were maximum and minimum in donors with titers of anti-SARS-CoV-2 IgG - 10 ± 3 and 65 ± 5 Index (S/C). At the same time, the group with IgG - 10 ± 3 Index (S/C) had higher TT values by 17.47% and 16.12%, than those in donors with IgG - 0 and 65 ± 5 Index (S/C), respectively. There were no statistically significant differences between the groups with IgG - 0 and 65 ± 5 Index (S/C), p > 0.05.
 |
Figure 1 The activated partial thromboplastin time in donor groups with titer of anti-SARS-CoV-2 IgG in blood plasma, Index (S/C): 1–0; 2–75 ± 5; 3–85 ± 5. *p < 0.05; **p > 0.05. |
 |
Figure 2 The thrombin time in donor groups with titer of anti-SARS-CoV-2 IgG in blood plasma, Index (S/C): 1–0; 2–10 ± 3; 3–65 ± 5. *p < 0.05; **p > 0.05. |
Based on the evaluation of the coagulation pathway status, we decided to analyze anticoagulation parameters in the donor plasma. Thus, the activity and quantitative composition of proteins, such as ATIII, PC and TM, were determined.
ATIII is a key anticoagulation factor that participates in 80% of coagulation inhibition. The maximum and minimum activity of ATIII was detected in the donor group with titers of anti-SARS-CoV-2 IgG - 65 ± 5 and 75 ± 5 Index (S/C), respectively, among all donor groups with titers of anti-SARS-CoV-2 IgG ≥ 10 ± 3 Index (S/C). In particular, donors with titer of anti-SARS-CoV-2 IgG - 65 ± 5 Index (S/C) had a higher activity of ATIII by 209.55% than that donors with IgG - 0 Index (S/C). Then, the activity of ATIII was lower by 74.40% in donors with titer of anti-SARS-CoV-2 IgG - 75 ± 5 Index (S/C) than in donors with IgG - 0 Index (S/C), Figure 3.
 |
Figure 3 The activity of ATIII in donor groups with titer of anti-SARS-CoV-2 IgG, Index (S/C): 1–0; 2–65 ± 5; 3–75 ± 5. *p < 0.05. |
A quantitative analysis was performed using the Bradford method to measure the concentration of ATIII. We determined that the maximum concentration of ATIII was characterized in the donor group with titer of anti-SARS-CoV-2 IgG - 175 ± 5 Index (S/C), and the minimum in donors with IgG - 75 ± 5 Index (S/C) among donor groups with titers of anti-SARS-CoV-2 IgG ≥ 10 ± 3 Index (S/C). According to the results, in the group with IgG - 175 ± 5 Index (S/C) the concentration of ATIII was higher by 92.27% and 356.22% than that in donors with IgG - 0 and 75 ± 5 Index(S/C), respectively. Donors with titer of anti-SARS-CoV-2 IgG - 75 ± 5 Index (S/C) had a lower concentration of ATIII by 58.06% compared to the group with IgG - 0 Index (S/C), Figure 4.
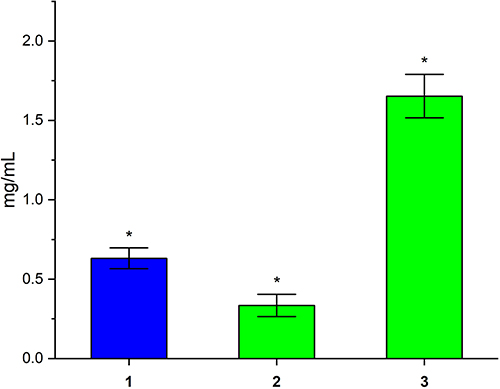 |
Figure 4 The concentration of ATIII in donor groups with titer of anti-SARS-CoV-2 IgG, Index (S/C): 1–0; 2–75 ± 5; 3–175 ± 5. *p < 0.05. |
At the same time, we established the activity of PC among all donor groups. Figure 5 shows that the maximum activity of PC was determined in donors with titer of anti-SARS-CoV-2 IgG - 55 ± 5 Index (S/C) among donors with titers of anti-SARS-CoV-2 IgG ≥ 10 ± 3 Index (S/C). It was higher by 44.06% than that in donors with IgG - 0 Index (S/C). The minimum activity of PC was detected in donors with titer of anti-SARS-CoV-2 IgG - 95 ± 5 Index (S/C). It was lower by 77.19% and 84.17% than that in donors with IgG - 0 and 55 ± 5 Index (S/C), respectively.
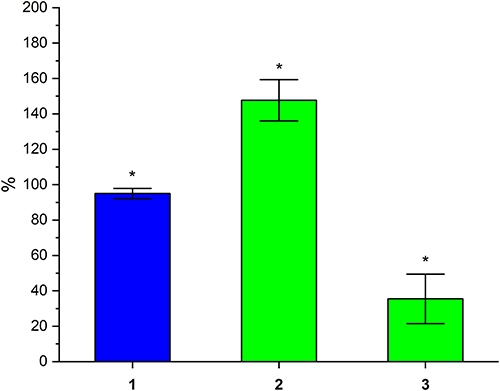 |
Figure 5 The PC activity in donor groups with titer of anti-SARS-CoV-2 IgG, Index (S/C): 1–0; 2–55 ± 5; 3–95 ± 5. *p < 0.05. |
Using ELISA, we analyzed the levels of PC in the blood plasma of the donors. It was determined that the maximum level of PC was in donors with titer of anti-SARS-CoV-2 IgG - 10 ± 3 Index (S/C), and the minimum IgG - 85 ± 5 Index (S/C) among all donor groups with titers of anti-SARS-CoV-2 IgG ≥ 10 ± 3 Index (S/C). We found that the level of PC in donors with titer of anti-SARS-CoV-2 IgG - 10 ± 3 Index (S/C) was higher by 34.01% and 82.32% than that in the donor groups with IgG - 0 and 85 ± 5 Index (S/C), respectively. The donor group with titer of anti-SARS-CoV-2 IgG - 85 ± 5 Index (S/C) had a lower concentration of PC by 26.50% compared to donors with IgG - 0 Index (S/C), Figure 6.
 |
Figure 6 The concentration of PC in donor groups with titer of anti-SARS-CoV-2 IgG, Index (S/C): 1–0; 2–10 ± 3; 3–85 ± 5. *p < 0.05. |
Finally, the concentration of TM was estimated for all groups. We emphasized that the donor groups with titers of anti-SARS-CoV-2 IgG ≥ 10 ± 3 Index (S/C) had a lower concentration of TM than that donors with IgG - 0 Index (S/C). The maximum and minimum levels of TM were detected in donors with titers of anti-SARS-CoV-2 IgG - 10 ± 3 and 75 ± 5 Index (S/C), respectively. The levels of TM in donors with IgG - 75 ± 5 Index (S/C) were lower by 41.01% and 32.42% than those in donors with IgG - 0 and 10 ± 3 Index (S/C). Then, the concentration of TM in donors with IgG - 10 ± 3 Index (S/C) was lower by 12.70% compared to donors with IgG - 0 Index (S/C), Figure 7.
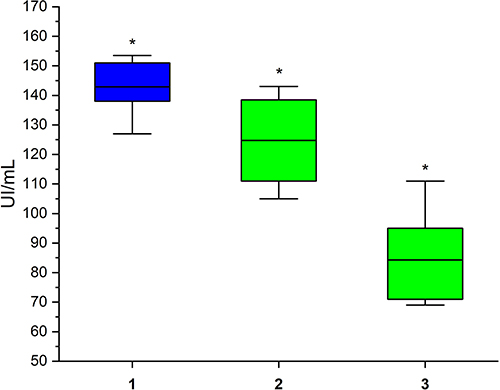 |
Figure 7 The concentration of thrombomodulin in donor groups with titer of anti-SARS-CoV-2 IgG, Index (S/C): 1–0; 2–10 ± 3; 3–75 ± 5. *p < 0.05. |
Discussion
The physiological balance between the coagulation and anticoagulation systems is tightly regulated. Inflammatory reactions against viral or bacterial diseases can cause a deviation in both systems that can lead to extremely intensive coagulation or bleeding. Patients are often prescribed anticoagulants and antithrombotic agents in the treatment protocols for COVID-19.13 However, coagulation deviations may persist after COVID-19 recovery, which is a potential risk factor for thrombosis. Clinical and scientific research is still insufficient to preclude the development of hemostasis complications in the post-COVID-19 period. This study provides information about the status of key anticoagulation parameters in donors who had suffered from COVID-19 and had different titers of anti-SARS-CoV-2 IgG.
Our previous research found that the post-COVID-19 period was associated with an increased risk of coagulation dysfunction in donor groups with various titers of anti-SARS-CoV-2 IgG.14 The current study investigated possible deviations in the anticoagulation system. We aimed to establish the presence or absence of changes in critical anticoagulation parameters, such as ATIII, PC, and TM, among the donor groups. We emphasize that the status of blood plasma from people without any infectious diseases or pathological processes was analyzed. As a result, the changes in the study parameters may depend on a single influencing factor, specifically the titer of anti-SARS-CoV-2 IgG.
Anticoagulant proteins inhibit the intrinsic and common coagulation pathways, directly or indirectly influencing coagulation factors. Using standard diagnostic tests, such as APTT and TT, we estimated the general status of the specified pathways to detect potential dysfunction of coagulation and anticoagulation balance. According to the results, donors tended to prolong APTT and TT in the post-COVID-19 period. The literature has selected some reasons for prolonged APTT, including defects in procoagulant factors, especially VIII and X.15 Moreover, APTT can decrease under conditions of shortage of ATIII and PC activity in some cases.16 APTT and TT were not lower among the donor groups with titers of anti-SARS-CoV-2 IgG ≥ 10 ± 3 Index (S/C) than at the reference point. We assume that changes in coagulation pathways may be caused by pro- and anticoagulation imbalances depending on the titers of anti-SARS-CoV-2 IgG. For this purpose, we decided to study the anticoagulant parameters among the donor groups in detail.
Literature reports that ATIII is a powerful inhibitor of thrombin and directly inactivates accumulated thrombin, preventing fibrin formation in blood vessels. Our study on ATIII consisted of two methods: measurement of activity in samples and quantitative analysis of purified proteins from blood plasma. Our results showed that the activity of ATIII varied in the donor groups, depending on the titers of anti-SARS-CoV-2 IgG. In summary, significant changes in the activity of ATIII were detected in donor groups with range of titers of anti-SARS-CoV-2 IgG from 65 ± 5 to 75 ±5 Index (S/C). Moreover, the maximum activity of ATIII among donor groups with titers of anti-SARS-CoV-2 ≥ 10 ±3 Index (S/C) was statistically higher than that in donors with IgG – 0 Index (S/C). Excessive activation of ATIII may indicate widespread thrombotic events in blood vessels, which influence the functional capacity of the anticoagulation cascade. The quantitative measurement results confirmed that the changes in ATIII concentration depended on the titers of anti-SARS-CoV-2 IgG in the donor groups. This may be associated with the formation of functionally incapable protein molecules, leading to the development of anticoagulation system pathology. A possible hypothesis is the presence of post-COVID-19 factors, such as abnormal degradation of coagulation molecules and/or antibody subpopulations, which can influence coagulation and anticoagulation disorders.
We emphasize that the quantitative analysis of PC was negatively correlated with the measurement of PC activity. An increase in the levels of PC was detected in the donor groups, which may indicate the destabilization of PC activities that are able to inhibit the functioning of anticoagulation proteins or the accumulation of unphysiological proteolytic molecules.
Given the above, the various values of the studied parameters depend on titer of anti-SARS-CoV-2 IgG. Early data have reported the influence of antibody subpopulations caused by infection and inflammation on the status of the hemostasis system. Currently, the development of coagulation disorders is a known consequence of diseases such as viral hepatitis, Epstein-Barr infection, systemic sclerosis, and ischemic stroke by accumulation of autoantibodies.17–20 A recent study has reported that autoantibodies can be detected in COVID-19 patients with three types being identified: antiphospholipids, anticytoplasmic neutrophils, and antinuclear antibodies.21 We determined the dependence of anticoagulation parameters and titers of anti-SARS-CoV-2 IgG in donors who had recovered from COVID-19. We assume that IgG subpopulations may lead to the development of a long post-COVID-19 period, which is accompanied by chronic violations of the hemostasis system. Consequently, the immune system can produce autoantibodies against coagulation factors.
Our study was limited by the number of participants included. Therefore, if more information about the status of anticoagulant parameters will be registered for people in the post-COVID-19 condition, we can reach specific conclusions regarding the influence of anti-SARS-CoV-2 IgG on dysfunctional coagulation processes.22
Conclusion
Post COVID-19 condition can affect multiple organ systems including the respiratory, gastrointestinal, neurological, or cardiovascular.23 We investigated the key anticoagulation parameters of donor plasma during the post-COVID-19 period and established that the changes in the concentration and activities of ATIII, PC, and TM depended on the titers of anti-SARS-CoV-2 IgG. This is a potential reason for prolonged thrombotic complications after recovery.
Titers of anti-SARS-CoV-2 IgG has been identified as a critical factor for possible coagulation disorders in the studied donor groups. Although we confirmed the dysfunction of anticoagulation parameters in the donor groups, we aim to explore the subpopulation of antibody IgG fraction directly using in vivo and in vitro experiments. Thus, we can begin to have a better understanding of post-COVID-19 hemostasis complications. This would significantly contribute to the development of post-treatment post-COVID-19 conditions. A detailed study of the anticoagulation parameters of healthy people with different titers of anti-SARS-CoV-2 IgG emphasizes the necessity for widespread clinical diagnostics in the post-COVID-19 period.
Data Sharing Statement
Data supporting the reported results are available on request by contacting the corresponder Marko Koyzk at 3601 W 13 Mile Rd, Royal Oak, MI, 48073, +1-305-773-5089, and email: [email protected].
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board at the ESC “Institute of Biology and Medicine” Taras Shevchenko National University of Kyiv, Kyiv, Ukraine (the protocol № 4, 25.05.2022).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–232. doi:10.1016/S0140-6736(20)32656-8
2. Mokhtari T, Hassani F, Ghaffari N, Ebrahimi B, Yarahmadi A, Hassanzadeh G. COVID-19 and multiorgan failure: a narrative review on potential mechanisms. J Mol Histol. 2020;51(6):613–628. doi:10.1007/s10735-020-09915-3
3. Priyanka COP, Singh I, Patra G, et al. Aerosol transmission of SARS-CoV-2: the unresolved paradox. Travel Med Infect Dis. 2020;37:101869. PMID: 32891726; PMCID: PMC7471761. doi:10.1016/j.tmaid.2020.101869
4. Pretorius E, Vlok M, Venter C, et al. Persistent clotting protein pathology in long COVID/post-acute sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol. 2021;20(1):172. doi:10.1186/s12933-021-01359-7
5. Adanma Ezihe-Ejiofor J, Hutchinson N. Anticlotting mechanisms 1: physiology and pathology. Cont Educ Anaesth Crit Care Pain. 2013;13(3):87–92. doi:10.1093/bjaceaccp/mks061
6. Perry DJ. Antithrombin and its inherited deficiencies. Blood Rev. 1994;8(1):37–55. doi:10.1016/0268-960x(94)90006-x
7. Griffin JH, Fernández JA, Gale AJ, Mosnier LO. Activated protein C. J Thromb Haemost. 2007;5(Suppl 1):73–80. doi:10.1111/j.1538-7836.2007.02491.x
8. Poh KC, Jia Tay VY, Lin SH, Chee HL, Thangavelautham S. A review of COVID-19-related thrombosis and anticoagulation strategies specific to the Asian population. Singapore Med J. 2022;63(7):350–361. doi:10.11622/smedj.2020174
9. Bradford MM. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal Biochem. 1976;72:248–254. doi:10.1006/abio.1976.9999
10. Kravchenko O, Melnyk V, Tsarenko T, et al. The blood coagulation tests from ischemic stroke patients with or without type 2 diabetes mellitus. Biomed Res. 2018;29(14):2938–2943. doi:10.4066/biomedicalresearch.29-18-332
11. Crowther JR. The ELISA guidebook. Methods Mol Biol. 2000;149:III–413. doi:10.1385/1592590497
12. Macarena FK. Antibody validation. Mater Methods. 2016;6:1.
13. Godino C, Scotti A, Maugeri N, et al. Antithrombotic therapy in patients with COVID-19? -rationale and evidence. Int J Cardiol. 2021;324:261–266. doi:10.1016/j.ijcard.2020.09.064
14. Rachkovska A, Krenytska D, Karbovskyy V, et al. Characteristics of products of fibrinogen origin in the presence of anti-SARS-CoV-2 IgG in the bloodstream. Rev Recent Clin Trials. 2022. doi:10.2174/1574887118666221219115856
15. Barbosa ACN, Montalvão SAL, Barbosa KGN, et al. Prolonged APTT of unknown etiology: a systematic evaluation of causes and laboratory resource use in an outpatient hemostasis academic unit. Res Pract Thromb Haemost. 2019;3(4):749–757. doi:10.1002/rth2.12252
16. Kim SY, Kim JE, Kim HK, Kim I, Yoon SS, Park S. Influence of coagulation and anticoagulant factors on global coagulation assays in healthy adults. Am J Clin Pathol. 2013;139(3):370–379. doi:10.1309/AJCPC5C4AGFRDKMX
17. Stratton R, Slapak G, Mahungu T, Kinloch-de Loes S. Autoimmunity and HIV. Curr Opin Infect Dis. 2009;22(1):49–56. doi:10.1097/QCO.0b013e3283210006
18. Houen G, Trier NH. Epstein-Barr virus and systemic autoimmune diseases. Front Immunol. 2021;11:587380. doi:10.3389/fimmu.2020.587380
19. Katrii T, Shandyuk V, Vovk T, et al. Effect of IgG from multiple sclerosis patients on amidolytic activity of coagulation and anticoagulation factors of hemostasis. Biomed Res Ther. 2017;4(08):1502–1512. doi:10.15419/bmrat.v4i08.205
20. Raksha N, Burlova-Vasylieva M, Torgalo E, Savchuk O. The appearance of molecules of prothrombin origin in blood upon development of atherothrombotic and cardioembolic ischemic stroke. Bull T Shevchenko Nat Univ Kyiv Ser Biol. 2014;68(3):57–60. doi:10.17721/1728_2748.2014.68.57-60
21. Darmarajan T, Paudel KR, Candasamy M, et al. Autoantibodies and autoimmune disorders in SARS-CoV-2 infection: pathogenicity and immune regulation. Environ Sci Pollut Res Int. 2022;29(36):54072–54087. doi:10.1007/s11356-022-20984-7
22. Falalyeyeva T, Komisarenko I, Yanchyshyn A, et al. Vitamin D in the prevention and treatment of type-2 diabetes and associated diseases: a critical view during COVID-19 time. Minerva Biotechnol Biomol Res. 2021;33(2):65–75. doi:10.23736/S2724-542X.21.02766-X
23. Kozyk M, Strubchevska K, Marynenko T, et al. Effect of peptides from plasma of patients with coronary artery disease on the vascular endothelial cells. Medicina. 2023;59(2):238. doi:10.3390/medicina59020238
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence of Inherited Thrombophilia in Women with Recurrent Pregnancy Loss During the First Trimester of Pregnancy
Yousif TYE
Journal of Blood Medicine 2023, 14:253-259
Published Date: 5 April 2023