Back to Journals » Infection and Drug Resistance » Volume 19
Co-Infection of Chlamydia psittaci and Methicillin-Resistant Staphylococcus aureus in Community-Acquired Pneumonia - A Case Report
Authors Zhu SL, Pan LJ, Cheng WB, Zheng XF, Chen Y, Li M
Received 23 February 2026
Accepted for publication 10 June 2026
Published 19 June 2026 Volume 2026:19 603306
DOI https://doi.org/10.2147/IDR.S603306
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Shuang-Li Zhu, Li-Jie Pan, Wen-Bin Cheng, Xiao-Fen Zheng, Ye Chen, Minjing Li
Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Minjing Li, Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Abstract: This study presents a rare case of community-acquired pneumonia (CAP) caused by a co-infection of Chlamydia psittaci and Methicillin-resistant Staphylococcus aureus (MRSA), confirmed by targeted next-generation sequencing (tNGS). The patient had a history of diabetes mellitus and hypertension. He developed fever, fatigue, myalgia and poor appetite two days before admission. He had watched someone slaughter a chicken two days prior to the onset of symptoms. The chest CT revealed consolidative changes. We suspected that the patient might have Chlamydia psittaci infection. Given the low sensitivity and time-consuming nature of conventional microbial culture, tNGS was utilized in this case to improve diagnostic accuracy and reduce detection time. Targeted next-generation sequencing (tNGS) identified a co-infection with Chlamydia psittaci and methicillin-resistant Staphylococcus aureus (MRSA). Recovery was achieved after treatment with omadacycline and linezolid. The Chlamydia psittaci was likely transmitted from the chicken, and the patient’s diabetes mellitus increased susceptibility to MRSA. This case highlights the risk of polymicrobial infections in diabetic individuals and the diagnostic value of tNGS.
Keywords: pneumonia, Chlamydia psittaci, methicillin-resistant Staphylococcus aureus, co-infection, targeted next-generation sequencing
Introduction
Psittacosis is a zoonotic disease caused by Chlamydia psittaci, primarily transmitted through inhalation of aerosols containing secretions or dried excreta from infected birds. Methicillin-resistant Staphylococcus aureus is an uncommon but highly lethal cause of CAP. Co-infection with both agents is extremely rare, difficult to recognize clinically, and prone to misdiagnosis or delayed treatment. We report an elderly male patient with multiple comorbidities who was ultimately diagnosed with Chlamydia psittaci pneumonia complicated by MRSA. The patient, who had type 2 diabetes mellitus, had observed the slaughtering of a chicken before symptom onset. The main clinical manifestations were fever and fatigue. Pathogens were identified by targeted next-generation sequencing of bronchoalveolar lavage fluid (BALF), and the patient recovered after receiving combination therapy with omadacycline and linezolid.
Case Presentation
The patient, a 71-year-old male farmer, had a history of diabetes mellitus for more than 10 years, currently taking metformin and reporting good glycemic control, and a history of hypertension for more than 10 years without medication. He developed fever and fatigue two days before admission. Although his temperature was not measured, he also experienced myalgia and poor appetite, with no cough or sputum. The patient was not concerned about these symptoms. On the morning of admission, he experienced weakness and syncope with transient loss of consciousness. He recovered after oral glucose administration but remained fatigued and subsequently came to our emergency department.
In the emergency department, the temperature of the patient was 38.6 °C. Blood tests showed a white blood cell count of 11.2 × 109/L, neutrophil count of 83.1%, lymphocyte count of 10.8%, hemoglobin of 156 g/L, and platelet count of 131 × 109/L. C-reactive protein was 88.93 mg/L and procalcitonin was 0.2 ng/mL. Glycated hemoglobin (HbA1c) was 5.6%. Serum chemistry panel revealed glucose 9.05 mmol/L, alanine aminotransferase (ALT) 17 U/L, aspartate aminotransferase (AST) 17 U/L, and creatine kinase (CK) 40 U/L (see Table 1). Tumor markers, including carcinoembryonic antigen (CEA), neuron-specific enolase (NSE), cytokeratin 19 fragment (CYFRA21-1), and squamous cell carcinoma (SCC) antigen, were negative. Arterial blood gas (ABG) analysis showed pH 7.461, partial pressure of oxygen (pO2) 107 mmHg, partial pressure of carbon dioxide (pCO2) 36.4 mmHg, bicarbonate (HCO3−) 25.1 mmol/L, and a P/F ratio of 324. Head computed tomography (CT) revealed mild periventricular ischemic changes and age-related brain atrophy. Chest CT demonstrated left lower lobe pneumonia, bilateral scattered fibrotic and proliferative foci, and right pleural thickening.
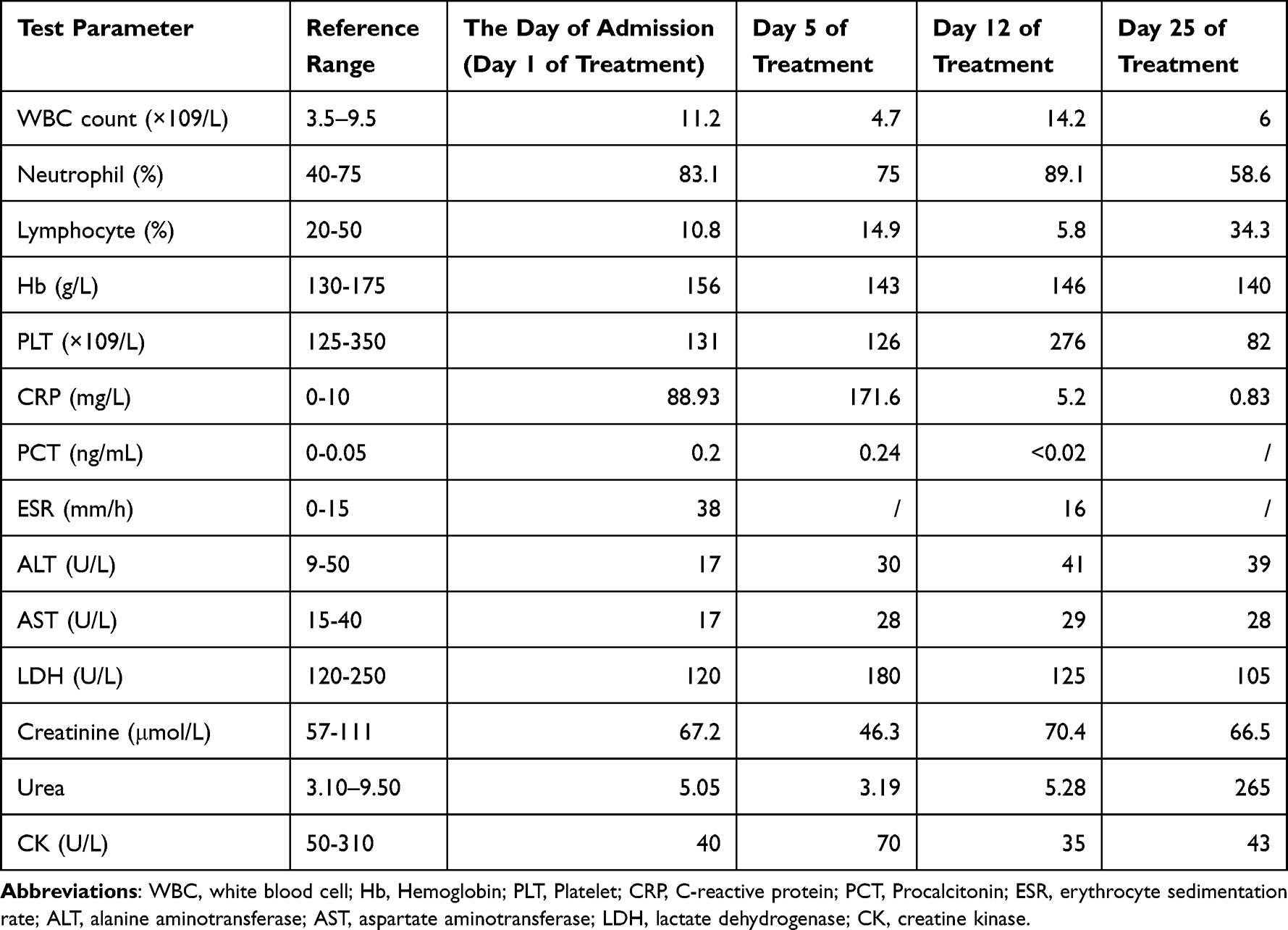 |
Table 1 Laboratory Test Results of the Patient |
He was diagnosed with community-acquired pneumonia and admitted to our department for hospitalization that evening. The patient denied keeping birds and poultry. On Day 1, empirical treatment with nemonoxacin (0.5g daily) intravenously was initiated, and further workup such as sputum culture and blood culture were performed. On day 2, the patient remained febrile (temperature 39.6°C). By nasopharyngeal swab PCR, the RNA of Influenza A/B, Respiratory Syncytial Virus, COVID-19, and Rhinovirus, as well as the DNA of Adenovirus and Mycoplasma pneumoniae, were all detected as negative. Holter monitoring showed frequent atrial and ventricular premature beats. We reviewed the chest CT, which revealed consolidative changes. We suspected that the patient might have Chlamydia psittaci infection. We re-questioned the patient ‘s history of domestic poultry exposure. The patient reported having watched someone slaughter a chicken at a vegetable market two days prior to the onset of symptoms. This strengthened our suspicion of Chlamydia psittaci infection. Considering the poor efficacy of quinolones against Chlamydia psittaci, the treatment regimen was adjusted. Nemonoxacin was discontinued, and the antibacterial agent was switched to omadacycline injection (0.1g once daily, with the first dose doubled). Additionally, ambroxol was administered intravenously to resolve phlegm, metoprolol sustained-release tablets to control heart rate, and symptomatic treatments such as gastric protection, hypoglycemic therapy, hypotensive therapy, potassium supplementation, and fluid replacement were provided.
On day 3, to identify the pathogen, the patient underwent bronchoscopy, and bronchoalveolar lavage was performed on the lateral posterior basal segment of the left lower lobe, with 30 mL of lavage fluid recovered. On this day, the patient’s maximum body temperature was 39.3°C, and on day 4, it decreased to 38.1°C with relief of fatigue symptoms. On day 4, sputum culture grew only normal flora. Results of the bronchoalveolar lavage fluid were reported: cytological examination showed a predominance of neutrophils; acid-fast bacilli were negative; tNGS based on the MGI high-throughput sequencing platform detected Chlamydia psittaci (25 sequences fragments), mecA-gene-positive Staphylococcus aureus (838,341 sequences fragments) and common microflora. The detection of the mecA gene in Staphylococcus aureus indicated that it was Methicillin-resistant Staphylococcus aureus (MRSA). Theoretically, omadacycline was effective against MRSA, but the patient remained febrile with worsening coughing. Therefore, on day 4, linezolid injection (0.6g every 12 hours) was added for anti-infective treatment. On day 5, the body temperature decreased to 37.8°C. On day 6, the bronchoalveolar lavage fluid culture results indicated a positive finding for MRSA and the body temperature returned to normal. The patient was discharged on day 13 and continued oral anti-infective treatment after discharge: doxycycline enteric-coated capsules (0.1g every 12 hours for a total of 9 days) and linezolid tablets (0.6g every 12 hours for a total of 13 days). The patient’s temperature changes and use of antibacterial agents was shown in Figure 1.
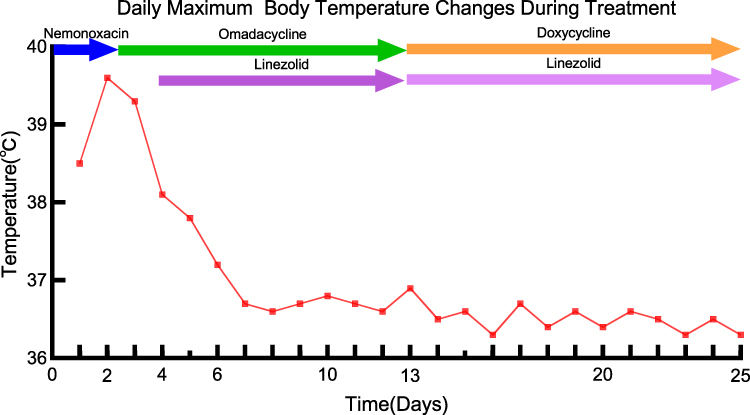 |
Figure 1 The patient’s temperature changes and use of antibacterial agents. |
We rechecked complete blood cell count, CRP, and biochemistry on day 5, day 12, and day 25 of treatment (see Table 1). After antibacterial therapy, the patient’s inflammatory indicators such as white blood cell count, CRP, and PCT decreased. Chest CT reexaminations were performed on day 11 and day 25: the chest CT on day 11 (Figure 2, v–viii) showed slight progression of lesions compared with previous images, while the chest CT on day 25 (Figure 2, ix–xii) indicated significant absorption of lesions.
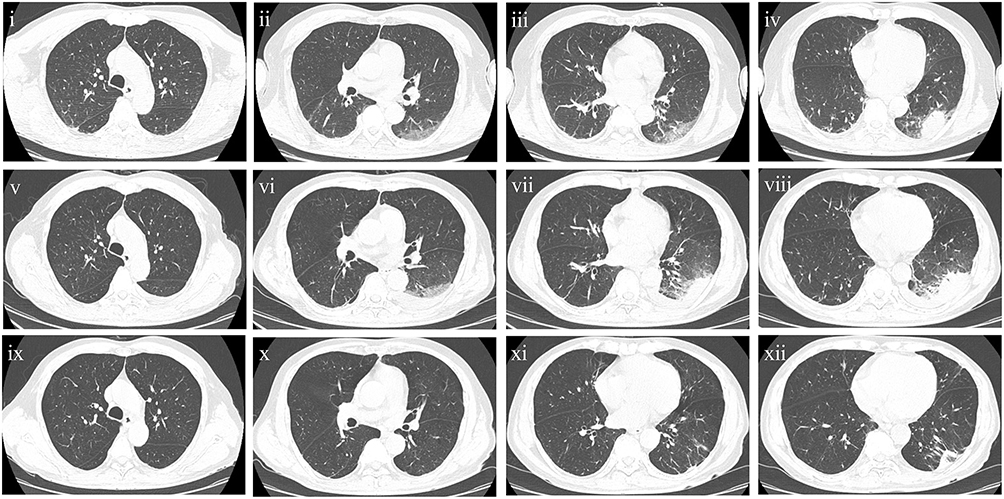 |
Figure 2 Chest computed tomography (CT) images of the patient. Chest CT on admission showed pneumonia (i–iv). Chest CT on day 11 of treatment showed slight progression of the pneumonia (v–viii); Chest CT on day 25 of treatment showed resolution of the pneumonia (ix–xii). |
Discussion
Chlamydia psittaci is an obligate intracellular gram-negative pathogen commonly found in birds and poultry. Humans can be infected through direct inhalation or indirect exposure to infected bird secretions, aerosols of dry feces, or feather dust.1 Community-acquired pneumonia caused by Chlamydia psittaci accounts for 1.03% of all CAP in adults.2 CAP secondary to methicillin-resistant Staphylococcus aureus is a rare occurrence and the prevalence rate is unknown.3 Inpatients, elderly patients and those with comorbidities have a higher risk of MRSA infection.4 We found an article reporting a case of pneumonia caused by co-infection with Chlamydia psittaci and methicillin-sensitive Staphylococcus aureus (MSSA) in a 28-year-old female patient.5 Her initial symptoms included sore throat, dry cough, and high fever. After two days of treatment with moxifloxacin, her symptoms did not improve significantly, and her headache worsened. She was then treated with omadacycline for three days, after which her symptoms improved. To our knowledge, no case report of psittacosis combined with MRSA has been found to date. In our case report, the patient had a history of exposure to poultry, which was the source of Chlamydia psittaci infection. He is a 71-year-old male with diabetes mellitus and hypertension, which increase the risk of MRSA infection.
The mechanism underlying this co-infection remains unclear. It may involve either sequential or simultaneous invasion, both of which are facilitated by compromised host immunity, such as in cases of diabetes mellitus or advanced age. We speculate that the patient was initially infected with MRSA (methicillin-resistant Staphylococcus aureus). Its virulence factors, such as hemolysins and leukocidins, impair the function of immune cells. These impairments in immune cell function may increase susceptibility to Chlamydia psittaci infection.
Patients with Chlamydia psittaci infection do not necessarily have a history of keeping birds or poultry. Moreover, their clinical manifestations are non-specific. Routine diagnostic methods, such as serological testing and sputum culture, have limitations in the diagnosis of psittacosis,6 making the diagnosis quite challenging. The imaging manifestations of Chlamydia psittaci pneumonia can provide us with some valuable clues. It typically presents with exudative and consolidative changes on chest computed tomography, including lung consolidation, bronchial air trapping, pleural effusion, and ground-glass opacities.7 In this case, the patient exhibited atypical symptoms of pulmonary infection and the chest CT findings resembled typical imaging findings of psittacosis, we suspected the possibility of Chlamydia psittaci. The patient was ultimately diagnosed with psittacosis complicated by MRSA infection through tNGS testing of bronchoalveolar lavage fluid. Targeted next-generation sequencing, an emerging etiological diagnostic method, can directly extract microbial DNA or RNA from clinical specimens without the need for culture and can also detect antimicrobial resistance genes in pathogens. Clinical reports have confirmed the important value of tNGS in the early diagnosis of psittacosis,8 especially its significant advantages in detecting mixed pathogen infections.9 In this case, the diagnosis of a co-infection involving Chlamydia psittaci and mecA-gene-positive Staphylococcus aureus was established by tNGS of bronchoalveolar lavage fluid, providing a direct basis for clinical management. Notably, tNGS provide rapid results several days earlier than the subsequent sputum culture. Therefore, for patients presenting with atypical symptoms of pulmonary infection, negative routine pathogen detection results, but pulmonary imaging suggesting lobar consolidation or ground-glass opacity, the possibility of rare pathogen infection should be considered in the differential diagnosis. Bronchoalveolar lavage should be performed in a timely manner along with tNGS detection.
Chlamydia psittaci belongs to the family Chlamydiaceae. Antibacterial agents that interfere with DNA/protein synthesis are optional, including tetracyclines, macrolides, and quinolones.10 Tetracyclines are the first choice, mainly omadacycline and doxycycline; macrolides are the second choice, followed by fluoroquinolones. Omadacycline has been proven to possess excellent antibacterial activity against Chlamydia psittaci. For the treatment of MRSA pneumonia, linezolid is the standard medication.11 Omadacycline exhibits high antibacterial activity against MRSA in vitro, with a susceptibility rate of 93%-98%.12,13 The clinical effective rate of omadacycline for Staphylococcus aureus pneumonia is 73%.14 No large observational experience is currently available on the use of omadacycline for the treatment of MRSA pneumonia and the clinical efficacy of omacycline in the treatment of MRSA remains unclear. In this case, omacycline was ineffective for the treatment of MRSA pneumonia and we selected omadacycline combined with linezolid for treatment. After discharge, the patient was switched to sequential therapy with doxycycline enteric-coated tablets and linezolid tablets and achieved a good therapeutic effect.
The severity of the Chlamydia psittaci pneumonia vary. In previous literature, most patients with Chlamydia psittaci pneumonia have relatively mild conditions, while some experience rapid disease progression—such as elderly patients or those with concurrent infections.15 These patients can develop severe pneumonia and respiratory failure in a short period, requiring ventilator-assisted ventilation and even extracorporeal membrane oxygenation (ECMO) therapy.16 Community-acquired pneumonia caused by MRSA may also lead to severe pneumonia.17 In this case report, the patient was a 71-year-old elderly male with a history of hypertension and diabetes mellitus, who was infected with Chlamydia psittaci combined with MRSA. These factors may increase his risk of developing severe pneumonia. Chlamydia psittaci can impair the function of macrophages. It can inhibit the host immune response by suppressing humoral immunity and altering the Th1/Th2 cell balance, leading to increased mortality.18 Virulence factors of MRSA affect the function of immune cells, resulting in severe pneumonia. Based on these research findings, we speculate that co-infection with Chlamydia psittaci and MRSA may exacerbate the severity of the disease, leading to increased tissue damage and higher mortality. If not treated promptly, the co-infection of Chlamydia psittaci and MRSA can progress to severe pneumonia and may lead to multiple organ dysfunction, so early diagnosis and timely treatment are even more important. In this case, the patient underwent bronchoscopy in a timely manner. The collected BALF was sent for targeted next-generation sequencing analysis. Through early diagnosis and treatment, the patient recovered well.
Conclusion
Pneumonia caused by the co-infection of Chlamydia psittaci and MRSA is extremely rare. It has no specific clinical manifestations, but the imaging features of Chlamydia psittaci pneumonia can provide valuable clues. Targeted next-generation sequencing is an important tool for achieving accurate diagnosis. Early diagnosis combined with treatment of tetracyclines and linezolid can improve patient prognosis with favorable outcomes.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
The samples analyzed in this study were collected following standard procedures of the hospital laboratory. Our research strictly adhered to the principles outlined in the Declaration of Helsinki and received ethical approval from the Ethics Committee of the second affiliated Hospital of Zhejiang Chinese Medical University. Publishing case details did not require institutional approval. The patient provided consent for the publication of the research results. Written informed consent was obtained for the publication of the case details and any accompanying images.
Acknowledgments
The authors thank the patient for his cooperation during the diagnostic process.
Funding
This study was supported by Zhejiang Provincial Natural Science Foundation Project (Grant No. LY23H270003) and Zhejiang Traditional Chinese Medicine Science and Technology Project (Grant No. 2026ZL0383).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Hocking JS, Geisler WM, Kong FYS. Update on the epidemiology, screening, and management of chlamydia trachomatis infection. Infect Dis Clin North Am. 2023;37(2):267–6. doi:10.1016/j.idc.2023.02.007
2. Hogerwerf L, De Gier B, Baan B, Van Der Hoek W. Chlamydia psittaci (psittacosis) as a cause of community-acquired pneumonia: a systematic review and meta-analysis. Epidemiol Infect. 2017;145(15):3096–3105. doi:10.1017/S0950268817002060
3. Mahapatra S, Reddy S, Duggal S, et al. Community-acquired methicillin-resistant Staphylococcus aureus pneumonia. Cureus. 2024;16(10):e72166. doi:10.7759/cureus.72166
4. Gu F, Zhang Y, Sun J, Guo W, Han L. The characteristics of methicillin-resistant Staphylococcus aureus co-infection in COVID-19 pneumonia. Front Cell Infect Microbiol. 2025;15:1560688. doi:10.3389/fcimb.2025.1560688
5. Zhou GQ, Liu JL, Zhang M. Omadacycline for pulmonary coinfection with Chlamydia psittaci and Staphylococcus aureus: a case report. Infect Inflam Repair. 2025;26(3):207–209. doi:10.3969/j.issn.1672-8521.2025.03.013
6. Huang W, Wang F, Cai Q, et al. Epidemiological and clinical characteristics of psittacosis among cases with complicated or atypical pulmonary infection using metagenomic next-generation sequencing: a multi-center observational study in China. Ann Clin Microbiol Antimicrob. 2023;22(1):80. doi:10.1186/s12941-023-00631-w
7. Ni Y, Zhong H, Gu Y, et al. Clinical features, treatment, and outcome of psittacosis pneumonia: a multicenter study. Open Forum Infect Dis. 2023;10(2):ofac518. doi:10.1093/ofid/ofac518
8. Yan X, Fu H, Deng W, Zhang Z, Wang D. Early and rapid diagnosis of Chlamydia psittaci pneumonia by tNGS in six patients: a case series. Front Med Lausanne. 2024;11:1491838. doi:10.3389/fmed.2024.1491838
9. Liang A, Wu X, Zhu Y, et al. Targeted next-generation sequencing (tNGS): an upcoming application for pathogen identification in clinical diagnosis. J Infect Public Health. 2025;18(10):102936. doi:10.1016/j.jiph.2025.102936
10. Balsamo G, Maxted AM, Midla JW, et al. Compendium of measures to control Chlamydia psittaci infection among humans (psittacosis) and pet birds (avian chlamydiosis), 2017. J Avian Med Surg. 2017;31(3):262–282. doi:10.1647/217-265
11. Wunderink RG. How important is methicillin-resistant Staphylococcus aureus as a cause of community-acquired pneumonia and what is best antimicrobial therapy? Infect Dis Clin North Am. 2013;27(1):177–188. doi:10.1016/j.idc.2012.11.006
12. File TM, Ramirez JA, Wilde AM. New perspectives on antimicrobial agents: omadacycline for community-acquired pneumonia, skin and soft tissue infections, and nontuberculous mycobacteria (focus on M. abscessus). Antimicrob Agents Chemother. 2025;69(2):e0108724. doi:10.1128/aac.01087-24
13. Huband MD, Fedler KA, Mendes RE, et al. Surveillance of omadacycline against 35,000 bacterial clinical isolates from the United States (2019-2023). Diagn Microbiol Infect Dis. 2025;111(3):116711. PMID: 39892370. doi:10.1016/j.diagmicrobio.2025.116711
14. Stets R, Popescu M, Gonong JR, et al. Omadacycline for community-acquired bacterial pneumonia. N Engl J Med. 2019;380(6):517–527. doi:10.1056/NEJMoa1800201
15. Wang DX, Xiao LX, Deng XY, Deng W. Omadacycline for the treatment of severe pneumonia caused by Chlamydia psittaci complicated with acute respiratory distress syndrome during the COVID-19 pandemic. Front Med Lausanne. 2024;10:1207534. doi:10.3389/fmed.2023.1207534
16. Wang L, Shi Z, Chen W, Du X, Zhan L. Extracorporeal membrane oxygenation in severe acute respiratory distress syndrome caused by Chlamydia psittaci: a case report and review of the literature. Front Med Lausanne. 2021;8:731047. doi:10.3389/fmed.2021.731047
17. He H, Wunderink RG. Staphylococcus aureus pneumonia in the community. Semin Respir Crit Care Med. 2020;41(4):470–479. doi:10.1055/s-0040-1709992
18. Chu J, Zhang Q, Zhang T, et al. Chlamydia psittaci infection increases mortality of avian influenza virus H9N2 by suppressing host immune response. Sci Rep. 2016;6(1):29421. doi:10.1038/srep29421
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Omadacycline for the Treatment of Severe Chlamydia psittaci Pneumonia Complicated with Multiple Organ Failure: A Case Report
Fang C, Xu L, Tan J, Tan H, Lin J, Zhao Z
Infection and Drug Resistance 2022, 15:5831-5838
Published Date: 4 October 2022
Chlamydia Psittaci Pneumonia-Induced Myocarditis: A Case Report
Yang X, Liu Z, Liu X, Li Q, Huang H, Li R, He M
Infection and Drug Resistance 2023, 16:4259-4264
Published Date: 29 June 2023
A Rare Fatal Case of COVID-19 Co-Infection with Community-Acquired Methicillin-Resistant Staphylococcus Aureus in a Diabetic Patient
Meng Z, Wuxiuer R, Zhao F, Yang Q
Infection and Drug Resistance 2025, 18:1935-1939
Published Date: 17 April 2025
Liver Function Abnormalities in Patients with Chlamydia psittaci Pneumonia: A Multicenter Retrospective Study
Fang C, Xu L, Lu J, Li Y, Zhao Z
Infection and Drug Resistance 2025, 18:3207-3217
Published Date: 28 June 2025
Pneumonia with BALF Detection of Tropheryma whipplei and Chlamydia psittaci by Targeted Next-Generation Sequencing: A Case Report
Li X, Feng Q
Infection and Drug Resistance 2026, 19:609565
Published Date: 12 June 2026