Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Co-Administration Treatment in Drug-Naïve Major Depression: Exploratory Real-World Patterns and Predictors in China
Authors Wu J, Zou Y ![]() , Zhou J, Meng F, Xiao L
, Zhou J, Meng F, Xiao L ![]()
Received 28 November 2025
Accepted for publication 27 February 2026
Published 13 March 2026 Volume 2026:22 579440
DOI https://doi.org/10.2147/NDT.S579440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Jiamiao Wu,* Yuchuan Zou,* Jia Zhou, Fanchao Meng, Le Xiao
Beijing Key Laboratory of Intelligent Drug Research and Development for Mental Disorders; National Clinical Research Center for Mental Disorders; National Center for Mental Disorders; Beijing Anding Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Le Xiao, Beijing Key Laboratory of Intelligent Drug Research and Development for Mental Disorders; National Clinical Research Center for Mental Disorders; National Center for Mental Disorders; Beijing Anding Hospital, No.5 Ankang Lane, Xicheng District, Beijing, 100088, People’s Republic of China, Email [email protected]
Objective: Co-administration of psychotropic medications is common in major depressive disorder (MDD), yet its patterns and predictors remain underexplored in drug-naïve patients. This study aimed to characterize the prevalence and correlates of co-administration strategies at treatment initiation in China.
Methods: In this multicenter, real-world study, we enrolled 1330 drug-naïve adults experiencing a depressive episode. Sociodemographic, clinical, and treatment data were collected at baseline. Univariate and multivariable logistic regression analyses identified factors associated with co-administration.
Results: Co-administration was utilized in 27.14% of patients. Antipsychotic augmentation was the most common strategy (18.87%), surpassing the use of multiple antidepressants (7.89%), while mood stabilizers (lithium 3.76%; valproate 2.78%) were less frequent. Patients receiving co-administration were typically male, older, had lower education/income, and more severe depressive symptoms. The most prescribed adjunctive antidepressants were SNRIs, NaSSAs, bupropion, and trazodone; the most common antipsychotics were quetiapine, olanzapine, aripiprazole, and risperidone. Multivariable analyses identified sympathetic arousal (OR=1.64) and leaden paralysis (OR=1.30) as key independent predictors.
Conclusion: Co-administration, particularly with antipsychotics, is frequently employed at the first treatment encounter for MDD in China. This practice appears to be a symptom-driven approach, targeting specific features like sympathetic arousal and leaden paralysis, which may reflect a pragmatic adaptation to local clinical realities beyond standard guidelines. Due to exploratory nature of the study, these findings are just hypothesis-generating, warranting further validation through more robust, longitudinal studies.
Keywords: major depressive disorder, drug-naïve, antipsychotics, co-administration, real-world study, China
Introduction
Major depressive disorder (MDD) is a leading cause of global disability, with pharmacological treatment remaining a cornerstone of management.1–3 While antidepressant monotherapy is the recommended first-line treatment for MDD, real-world prescribing patterns often deviate from this approach. Studies indicate that 30–60% of patients receive co-administration therapy (concurrent use of ≥2 psychotropic drugs).4–6 However, this practice has been disproportionately studied in treatment-resistant or chronic populations rather than in drug-naïve individuals with unipolar MDD.
Co-administration strategy is increasingly common yet controversial in early-stage MDD.7,8 This evidence gap is particularly salient in the context of drug-naïve patients, who are presumed to require simpler initial regimens according to most guidelines.9–11 Emerging data suggest that clinicians frequently deviate from this paradigm. For instance, a European study found that 29.5% of MDD patients received antidepressant combinations regardless of treatment history.6 The drivers behind co-administration in drug-naïve patients are poorly understood but may include clinical factors such as greater illness severity and specific symptom profiles (eg, insomnia, agitation, or atypical features), as well as sociodemographic factors like socioeconomic status and educational level, which can influence help-seeking behaviors and treatment expectations.
This gap in knowledge is especially critical in China, where cultural perceptions of mental illness, uneven distribution of mental health resources, and healthcare system policies may uniquely shape prescribing patterns.12,13 To date, no large-scale study has specifically investigated the prevalence and correlates of co-administration in drug-naïve MDD patients within the Chinese healthcare setting. Here, we present the first large-scale, multicenter analyses to address this gap. Using real-world data from drug-naïve Chinese adults with unipolar MDD, this study aims to:
- Quantify the prevalence of co-administration and describe the specific types of psychotropic medications (eg, antipsychotics, mood stabilizers, multiple antidepressants) used in this population.
- Identify the key sociodemographic (eg, age, gender, education, income) and symptom-specific (assessed via the Inventory of Depressive Symptomatology, Self-Report [IDS-SR30]) predictors associated with the use of co-administration strategies at treatment initiation.
Materials and Methods
Study Design
Data was derived from a multicenter cohort study (National key research and development program of China – Clinical Cohort Platform for Mental Disorders, study ID: 2017YFC1311101) from August 2020 to November 2021. A total of 23 tertiary and secondary psychiatric hospitals and psychiatric departments in general hospitals across China participated in the study. Drug-naïve MDD patients were consecutively enrolled.
Ethical Approval and Informed Consent
This multicenter, non-interventional, observational study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol, which served as a data collection platform for patients with Major Depressive Disorder, was reviewed and approved by the Ethics Committee of the lead center, Beijing Anding Hospital (Approval No. 2019–90). Written informed consent was obtained from all individual participants included in the study prior to any data collection, in line with the requirements of the lead center’s ethics approval and the respective local Institutional Review Boards (IRBs) of all participating hospitals.
Participants
The inclusion criteria were as follows: (1) Outpatient or inpatient aged 18–65; (2) Met diagnostic criteria of ICD-10 for depressive episode/recurrent depressive disorder after thorough evaluation by a qualified psychiatrist; (3) The total score of The Inventory of Depressive Symptomatology, Self-Report (IDS-SR30) was ≥14 during screening period; (4) Were drug-naïve, defined as having no lifetime history of any psychiatric medication use for any mental disorder prior to study enrollment. This criterion ensured that all patients, regardless of whether they were experiencing their first or a recurrent depressive episode, were initiating their first-ever pharmacological treatment for depression.; (5) Prescribed with antidepressants at their first visit at outpatients and inpatients.
The exclusion criteria were: (1) Diagnosis of bipolar disorder, schizoaffective disorder, or schizophrenia. (2) Utilization of herbal or traditional Chinese medicine that may affect the central nervous system (such as Shugan Jieyu Capsule, Morinda officinalis capsule, St. John’s Wort extract, Wuling capsule, Jiuwei Zhenxin granule, Tianmeng oral fluid, Shumian capsule, etc). (3) Use of flupentixol and melitracen. As a fixed-dose combination product, it is commonly used in China for mild to moderate depression and anxiety. It was excluded because it contains the typical antipsychotic flupentixol, and its use would confound the analyses of co-administration patterns involving antidepressants and adjunctive antipsychotics. (4) Participated in interventional clinical trials within 3 months. Patients with suicidal ideation were not excluded, as this study aimed to reflect the real-world clinical profile of drug-naïve MDD patients.
Data Collection
The collected information includes: (1) Sociodemographic data: age, gender, educational level, place of residence, occupational status, monthly income and insurance status; (2) Medical history: age of onset, number of depressive episodes, the course of current episode; family history of mental illness, and general medical condition; (3) Prescriptions have to written simultaneously at study entry.
Patients also self-rated Sheehan Disability Scale (SDS) and Quality of Life Enjoyment Satisfaction Questionnaire Short Form (Q-LES-Q-SF) under the guidance of a clinician. Depression severity was assessed using the 30-item Inventory of Depressive Symptomatology Self-Report (IDS-SR30), with scores categorized as mild (14–25), moderate (26–38), and severe (≥39).14,15
Statistical Analyses
Monotherapy was defined as treatment with a single antidepressant, without concomitant use of antipsychotics or mood stabilizers. Co-administration was defined as the use of more than one antidepressant, and/or an antidepressant augmented with an antipsychotic or a mood stabilizer (lithium or valproate). For the purpose of this analysis, benzodiazepines and other sleep aids (eg, zolpidem) were not considered part of the co-administration strategy. This distinction was made because these medications are typically used as adjunctive treatments for transient symptomatic relief (eg, insomnia, agitation) and do not constitute a core antidepressant or disease-modifying strategy. Their usage patterns are reported separately. The prevalence of co-administration treatment was calculated as the proportion of patients receiving such regimens relative to the total study sample, expressed as a percentage with the corresponding numerator and denominator.
Data distribution was evaluated by Kolmogorov–Smirnov test. Continuous data were expressed by median and interquartile range (IQR, statistical analyses: Wilcoxon rank-sum test), with categorical variables analyzed by Pearson Chi-squared or Fisher exact test. Binary logistic regression analysis was applied to find independent variables. All P-values were two-tailed, defined <0.05 as significant for every analysis. Data analyses were performed employing the Statistics Analysis System (SAS version 9.4). A stepwise multivariate logistic regression was performed to identify factors associated with co-administration treatment. While this approach allows for data-driven exploration of potential predictors, its inherent limitations in statistical inference are acknowledged and further discussed.
Results
A total of 1330 MDD patients were included in this analyses. Among them, 71.13% were female, 30.45% had recurrent depressive episodes, 15.26% had a family history of mental disorders, and 23.08% had general medical conditions. In terms of the severity of depression, 4.66% were classified as mild, 27.97% as moderate, and 67.37% as severe.
Prevalence and Types of Co-Administration Strategies
Co-administration therapy was employed in 27.14% (n=361) of the drug-naïve cohort. Among these patients, augmentation with antipsychotics was the most common strategy (18.87%, n=251), followed by the use of multiple antidepressants (7.89%, n=105). Mood stabilizers were less frequently prescribed, with lithium and valproate used in 3.76% (n=50) and 2.78% (n=37) of patients receiving combination therapy, respectively. Concomitant use of benzodiazepines or other sleep aids was common in the overall sample, observed in 47.74% (n=635) of patients.
Univariate Predictors of Co-Administration Treatment
Univariate analyses identified several factors associated with co-administration (Table 1). Patients receiving combination therapy were significantly more likely to be male, older, and to have lower educational attainment and monthly income. They also had a shorter duration of the current depressive episode. Clinically, this group demonstrated greater functional impairment, as evidenced by higher total scores on the Sheehan Disability Scale (SDS), particularly in the “work/school” and “family life/home responsibilities” domains. Moreover, they presented with more severe depressive symptoms, indicated by significantly higher total scores on the IDS-SR30 and elevated scores on specific items including mid-nocturnal insomnia, early morning insomnia, hypersomnia, mood variation, reactivity of mood, appetite and weight changes, suicidal ideation, anhedonia, and various somatic symptoms (see Table 1 for details). Bonferroni correction was not applied in this exploratory univariate analysis.
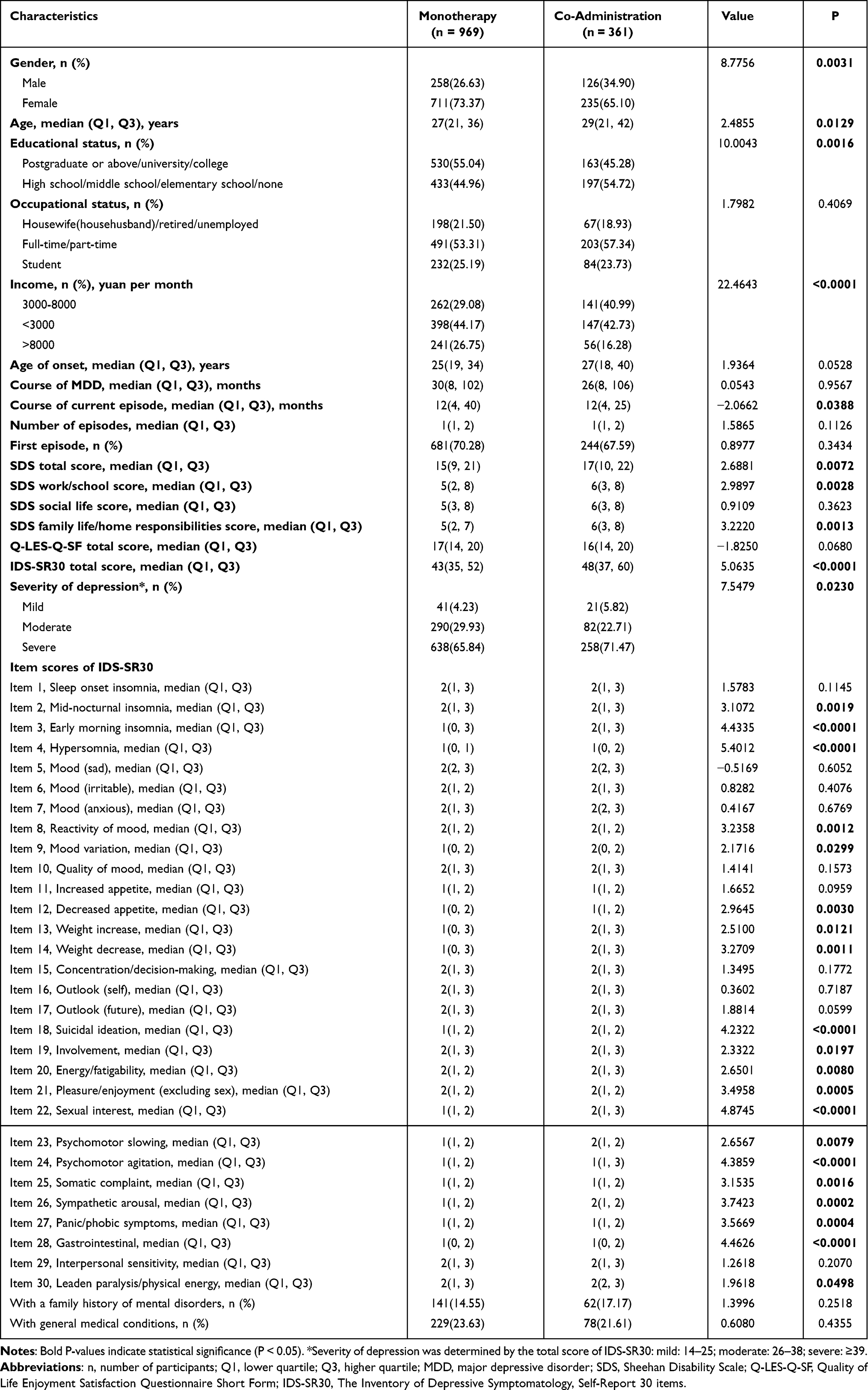 |
Table 1 Patients’ Sociodemographic and Clinical Characteristics |
Multivariate Analyses of Factors Associated with Co-Administration Treatment
The stepwise multivariate analyses revealed that lower scores on psychomotor slowing (OR=0.65, 95% CI=0.505–0.844) and somatic complaint (OR=0.721, 95% CI=0.563–0.923), and higher scores on sympathetic arousal (OR=1.636, 95% CI=1.307–2.049) and leaden paralysis/physical energy (OR=1.295, 95% CI=1.033–1.625) were significantly associated with co-administration treatment (Table 2).
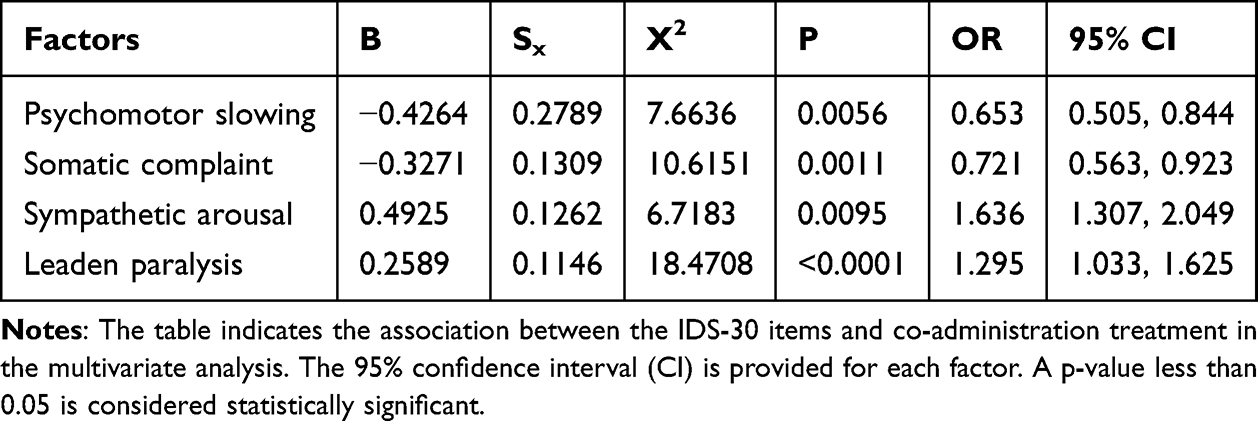 |
Table 2 Factors Associated with Co-Administration Treatment |
The Overall Usage of Antidepressants and Other Medications
The use of antidepressants by class was compared between monotherapy and co-administration treatment (Table 3). Significant differences were found in the use of SSRIs, NaSSAs, bupropion, and trazodone between the two groups (P values all < 0.01). Trazodone’s higher use in co-administration likely reflects its role in addressing insomnia—a frequent target in combination regimens. The overall use of benzodiazepines, sleep aids, and non-benzodiazepine anxiolytics is listed in Table 4. The proportion of antipsychotics in overall medication use is detailed in Supplemental Table 1, with the most frequently prescribed antipsychotic medications for quetiapine (53.29%), olanzapine (24.32%), aripiprazole (8.49%), and risperidone (4.25%).
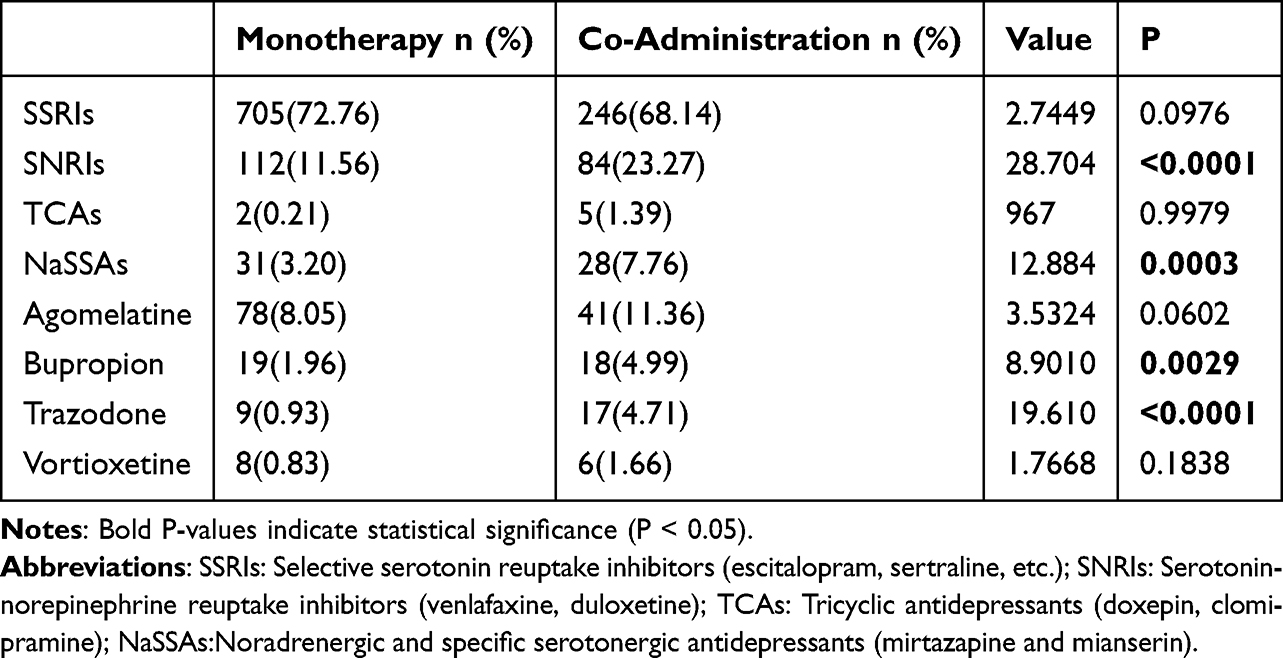 |
Table 3 Classes of Antidepressants in Monotherapy/Co-Administration Treatment |
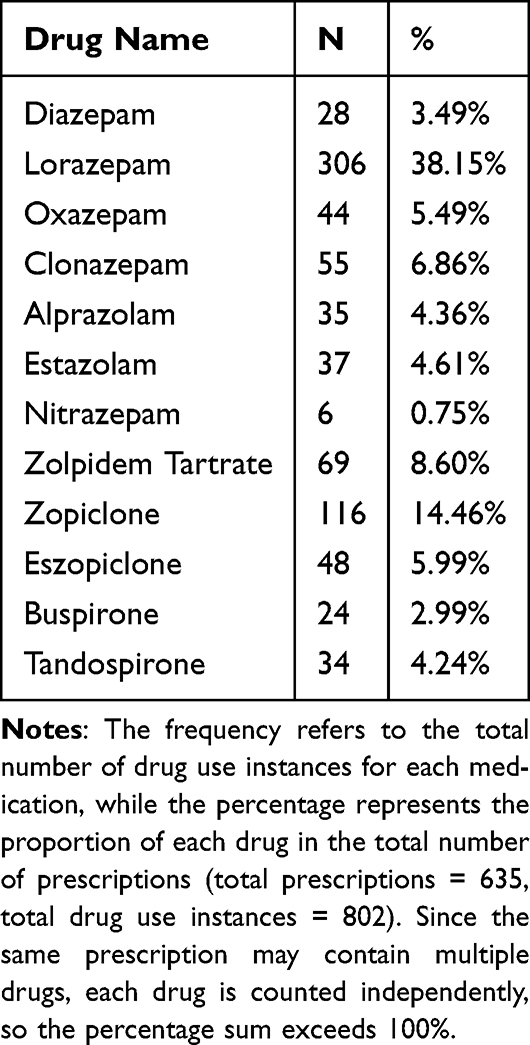 |
Table 4 Usage of Benzodiazepine and Non-Benzodiazepine Anxiolytics and Sleep Aids |
Discussion
In this real-world study of strictly drug-naïve MDD patients in China, 27.14% initiated treatment with a co-administration strategy. This prevalence provides a crucial benchmark for this understudied population. While this figure is lower than the 60.64% reported in a European study of predominantly non-naïve patients from tertiary centers,16 the comparison highlights a fundamental difference in study populations. Notably, 69.5% of our participants were in their first depressive episode, contrasting sharply with the 9% in the Dold et al cohort. Therefore, our findings uniquely characterize the initial treatment decisions for MDD in China. The relatively lower rate of antidepressant combinations may reflect a local tradition of monotherapy-first, whereas the substantial use of antipsychotics (18.87%) suggests that clinicians pragmatically prioritize rapid symptom control over strict guideline adherence in severe or complex presentations.
Our findings align with evidence suggesting that co-administration is prioritized for patients with severe depressive symptoms (Zhou et al, 2015). Specifically, higher IDS-SR30 scores were independently associated with co-administration, possibly reflecting clinicians’ preference for combination treatment in severely affected patients to achieve rapid symptom remission.17 We found that male gender, older age, lower educational status, lower monthly income, shorter episode duration, and higher depressive scores were positively associated with co-administration treatment, a finding not yet explored in prior research. Males and those with lower education and socioeconomic status may delay help-seeking, leading to more severe presentations and reduced engagement with psychotherapy.18–20 This may prompt clinicians to prioritize rapid symptom relief through combined treatment rather than relying on monotherapy alone. Older adults frequently exhibit complex clinical profiles, including comorbid medical conditions, cognitive decline, and sleep disturbances, necessitating co-administered intervention.21–24 Patients with shorter disease duration but more severe symptoms may also require aggressive intervention.11 In summary, the preference for drug co-administration in these subgroups likely reflects a combination of clinical complexity, patient-specific barriers to care, and the need for rapid and comprehensive symptom management. Further research is needed to disentangle these mediating factors and optimize treatment strategies for vulnerable populations.
The analyses of each item of IDS-SR30 showed that co-administration treatment was more often used in patients with mid-nocturnal insomnia, early morning insomnia, hypersomnia, mood variation, reactivity of mood, appetite decrease, weight change, suicidal ideation, involvement, fatigability, anhedonia, psychomotor slowing or agitation, somatic complaint, sympathetic arousal, panic/phobic, gastrointestinal symptoms and leaden paralysis/physical energy. Furthermore, the multivariate analyses identified four independent symptom predictors. The analyses revealed a differential association pattern: higher scores on sympathetic arousal (OR=1.636) and leaden paralysis (OR=1.295) were positive predictors for co-administration, whereas higher scores on psychomotor slowing (OR=0.65) and somatic complaints (OR=0.721) were inversely associated with combination therapy. This pattern may reflect distinct clinical decision-making. Sympathetic arousal, a feature of somatic anxiety linked to excessive activation of the norepinephrine system, may drive clinicians to add sedating agents (eg, trazodone) or anxiolytics to achieve rapid symptom control. Similarly, leaden paralysis, as a core feature of atypical depression characterized by a physical sensation of being weighed down, is historically associated with a better response to combination therapies. Additionally, higher rates of leaden paralysis and sympathetic arousal have been linked to severe medical comorbidities,25 which might also prompt a more aggressive treatment approach.26 Conversely, the inverse association with psychomotor slowing and somatic complaints could indicate that in drug-naïve patients, clinicians might initially opt for monotherapy and observe the response for these more “retarded” or non-specific somatic manifestations, reserving combination strategies for cases with prominent agitation or atypical features. Of course, these inverse associations could also be influenced by unmeasured confounding variables and require verification in future prospective studies.
Our findings that specific symptom profiles—particularly sympathetic arousal and leaden paralysis—predict co-administration provide a potential roadmap for personalizing initial treatment strategies in drug-naïve MDD. This observed symptom-driven prescribing pattern suggests that clinicians intuitively select more aggressive regimens for patients presenting with specific, high-burden symptom clusters. This framework powerfully elucidates China’s distinct prescribing pattern, which prioritized SGAs (18.87%) over antidepressant combinations (7.89%).
The efficacy of SGAs for MDD is well-established in meta-analyses,5 and their use in our cohort appears to be a pragmatic application of this evidence, strategically aligned with the symptom predictors we identified. For instance, sympathetic arousal, a marker of hyperarousal and agitation, likely drives the preference for sedating SGAs like quetiapine and olanzapine (together accounting for over 77% of SGA prescriptions) to address insomnia and anxiety. Conversely, for patients with leaden paralysis—a core atypical feature characterized by profound fatigue—clinicians may opt for activating agents like aripiprazole to counter energy deficits, while risperidone might be chosen for its efficacy against co-occurring paranoid symptoms. This symptom-targeted approach may reflect a cultural and clinical adaptation to rapidly address the most salient patient complaints.
Furthermore, this prescribing pattern is likely reinforced by non-clinical factors. Within China’s centralized procurement system, generic formulations of quetiapine and olanzapine are widely available at reduced prices, enhancing their accessibility compared to newer antipsychotics. This cost-containment policy, coupled with the clinical urgency to manage severe symptoms like agitation and insomnia, creates a pragmatic environment where SGA augmentation becomes a frequently utilized first-line strategy, even as guidelines like NICE and BAP primarily endorse them for treatment-resistant depression.
Beyond SGAs, other augmentation agents were used with lower frequency, which may also reflect a targeting of specific clinical subpopulations. Lithium was also proven to be effective as an adjunctive agent in the treatment of MDD patients,27,28 though it was less frequently used in our study (3.76%). Factors predicting a good outcome of lithium augmentation therapy include a history of three or more depressive episodes, severe depressive symptoms, psychomotor retardation, significant weight loss, and first-degree family history of major depressive disorder (MDD) or bipolar disorder (BD). The prescription of lithium may have been limited by its slow onset and the need for constant plasma level monitoring. Thirty-seven patients (2.78%) used valproate as an adjunctive agent in our study. Current guidelines do not recommend its use for unipolar depression in general.11,29 However, it is recommended for MDD patients exhibiting mixed features (simultaneous depressive and hypomanic symptoms) and those at higher risk for suicide, either as monotherapy or in combination with antidepressants.10 Its mood-stabilizing properties may help mitigate the severity of mood fluctuations and suicidal ideation.30 Although we lacked data on psychosis/mixed features, the high antipsychotic use may reflect off-label management of subthreshold psychotic symptoms or agitation—a common challenge in Asian MDD patients.
In contrast to the relatively high use of antipsychotics, only 7.89% of patients received more than one antidepressant, a much lower figure than in some previous studies. This indicates that antidepressant combination is approached with greater caution in Chinese practice. Previous studies have shown that antidepressant combinations often do not demonstrate superior efficacy and may lead to additional side effects.8,31 While some studies suggest that combination therapy can be more effective and tolerable for acute depression than monotherapy,32,33 it is typically recommended as a second- or third-line option in current guidelines due to the lack of robust evidence.11 Nevertheless, the specific antidepressant classes commonly used in combination in our study—SNRIs, NaSSAs, bupropion, and trazodone—align with a symptom-driven approach. The preferential use of SNRIs (eg, venlafaxine for comorbid anxiety) and NaSSAs (eg, mirtazapine for insomnia) in co-administration aligns with their complementary mechanisms.33 Bupropion was likely prescribed for patients with fatigue and energy deficits, and trazodone for insomnia and anxiety, despite its side effects. Overall, our results suggest that across all medication types, the choice of co-administration strategy is frequently guided by the specific symptom profile of the patient.
This study contributes valuable epidemiological data on co-administration treatment in drug-naïve MDD patients in China, highlighting region-specific treatment patterns. Given the current healthcare structure where patients typically seek first psychiatric care in public secondary and tertiary hospitals rather than primary or community hospitals in China, the data from 23 such hospitals provides a representative sample.
Our study’s findings warrant cautious interpretation, given the methodological limitation. The present work constitutes an exploratory analyses, relying on univariate analysis without Bonferroni correction and the use of stepwise regression. While such approaches can be valuable for generating hypotheses and exploring potential associations, they are inherently prone to inflated Type I error rates, overestimation of effect sizes, and underestimated p-values. These statistical properties collectively compromise the robustness and reproducibility of the results, thereby limiting their causal interpretability. Furthermore, additional limitations beyond the statistical methodology are acknowledged. The lack of data on psychosis or mixed features prevented us from comprehensively evaluating their potential influence on antidepressant prescribing patterns. Moreover, the cross-sectional design of our study inherently precludes the assessment of treatment outcomes. Consequently, we could not definitively determine whether the symptom-driven prescribing patterns observed actually lead to superior patient outcomes.
In light of these limitations, the current study’s findings are best considered exploratory and hypothesis-generating, with potentially limited reproducibility. The associations identified between the four symptoms (psychomotor slowing, somatic complaint, sympathetic arousal, leaden paralysis) and co-administration treatment offer valuable preliminary insights into current prescribing practices. However, these considerations underscore the critical need for future longitudinal research. Such studies should incorporate more robust and theory-driven statistical approaches and follow patients over time. This approach is essential to verify the effectiveness of the observed prescribing patterns and to advance toward a more personalized, predictive model for initial treatment selection in Major Depressive Disorder (MDD).
Conclusion
In summary, our findings reveal that co-administration treatment is common in Chinese drug-naïve MDD patients, particularly antipsychotic augmentation with quetiapine and olanzapine being most frequently prescribed. This pattern, though not guideline-recommended as first-line, appears to reflect a symptom-driven approach targeting specific clinical presentations (eg, sympathetic arousal, leaden paralysis) in real-world practice. Given China’s limited mental health resources, such pragmatic prescribing strategies may represent clinicians’ attempt to balance rapid symptom control against potential side effects, highlighting the need for tailored treatment algorithms that consider both clinical and healthcare system factors.12
Data Sharing Statement
The datasets used and analyzed during the current study are not publicly available due to privacy or ethical restriction.
Ethics Approval and Consent to Participant
The study was approved by the ethics committee of every participating hospital and all participants provided written informed consent. All participants provided written informed consent before participation in the study. The study was conducted in accordance with the Declaration of Helsinki and adhered to all ethical guidelines regarding patient confidentiality and privacy.
Consent for Publication
Written informed consent for publication was obtained from all participants involved in this study. The consent procedure explicitly covered the publication of their anonymized data in scientific articles, both in print and online. Furthermore, participants were assured that all personal identifiers have been removed to safeguard their anonymity. The authors affirm that they are prepared to provide signed consent documentation to the journal editorial office if requested.
Acknowledgments
We would like to express our sincere gratitude to Professor Gang Wang for his valuable consultation, and funding support throughout this research. Thanks to all clinicians and researchers from all 23 hospitals and psychiatric departments for helping us completing the study.
Funding
This work was supported by High-Level Public Health Technical Talent Development Program, Beijing Municipal Health Commission (Main Participant-0308) and National Key Research & Development Program of China (2017YFC1311101).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bromet E, Andrade LH, Hwang I, et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011;9:90. doi:10.1186/1741-7015-9-90
2. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095–10. doi:10.1001/jama.289.23.3095
3. Kovess-Masfety V, Alonso J, Angermeyer M, et al. Irritable mood in adult major depressive disorder: results from the world mental health surveys. Depress Anxiety. 2013;30(4):395–406. doi:10.1002/da.22033
4. Zhou X, Keitner GI, Qin B, et al. Atypical antipsychotic augmentation for treatment-resistant depression: a systematic review and network meta-analysis. Int J Neuropsychopharmacol. 2015;18(11):pyv060. doi:10.1093/ijnp/pyv060
5. Nelson JC, Papakostas GI. Atypical antipsychotic augmentation in major depressive disorder: a meta-analysis of placebo-controlled randomized trials. Am J Psychiatry. 2009;166(9):980–991. doi:10.1176/appi.ajp.2009.09030312
6. Dold M, Bartova L, Mendlewicz J, et al. Clinical correlates of augmentation/combination treatment strategies in major depressive disorder. Acta Psychiatr Scand. 2018;137(5):401–412. doi:10.1111/acps.12870
7. Demyttenaere K, Stahl SM. Co-administration in the treatment of depression: deconstructing the tower of Babel? Eur Neuropsychopharmacol. 2023;72:1–3. doi:10.1016/j.euroneuro.2023.03.002
8. Rush AJ, Trivedi MH, Stewart JW, et al. Combining medications to enhance depression outcomes (CO-MED): acute and long-term outcomes of a single-blind randomized study. Am J Psychiatry. 2011;168(7):689–701. doi:10.1176/appi.ajp.2011.10111645
9. NICE. Depression in adults: treatment and management. London: National Institute for Health and Care Excellence Available from: https://www.ncbi.nlm.nih.gov/books/NBK583074/.
10. Stahl SM, Morrissette DA, Faedda G, et al. Guidelines for the recognition and management of mixed depression. CNS Spectr. 2017;22(2):203–219. doi:10.1017/s1092852917000165
11. Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. pharmacological treatments. Can J Psychiatry. 2016;61(9):540–560. doi:10.1177/0706743716659417
12. Xia L, Jiang F, Rakofsky J, et al. Resources and workforce in top-tier psychiatric hospitals in China: a nationwide survey. Front Psych. 2021;12:573333.
13. Liu S, Yang L, Zhang C, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7(4):e17–e18. doi:10.1016/s2215-0366(20)30077-8
14. Wu D, Yin H, Xu S, Carmody T, Morris DW. Psychometric properties of the Chinese version of Inventory for Depressive Symptomatology (IDS): preliminary findings. Asian J Psychiatr. 2010;3(3):126–129. doi:10.1016/j.ajp.2010.08.003
15. Corruble E, Legrand JM, Duret C, Charles G, Guelfi JD. IDS-C and IDS-sr: psychometric properties in depressed in-patients. J Affect Disord. 1999;56(2–3):95–101. doi:10.1016/s0165-0327(99)00055-5
16. Dold M, Kautzky A, Bartova L, et al. Pharmacological treatment strategies in unipolar depression in European tertiary psychiatric treatment centers - A pharmacoepidemiological cross-sectional multicenter study. Eur Neuropsychopharmacol. 2016;26(12):1960–1971. doi:10.1016/j.euroneuro.2016.10.005
17. Dunlop BW. Evidence-Based applications of combination psychotherapy and pharmacotherapy for depression. Focus. 2016;14(2):156–173. doi:10.1176/appi.focus.20150042
18. Mokhwelepa LW, Sumbane GO. Men’s mental health matters: the impact of traditional masculinity norms on men’s willingness to seek mental health support; a systematic review of literature. Am J Mens Health. 2025;19(3):15579883251321670. doi:10.1177/15579883251321670
19. Andrade LH, Alonso J, Mneimneh Z, et al. Barriers to mental health treatment: results from the WHO World Mental Health surveys. Psychol Med. 2014;44(6):1303–1317. doi:10.1017/s0033291713001943
20. Wang PS, Berglund P, Olfson M, Pincus HA, Wells KB, Kessler RC. Failure and delay in initial treatment contact after first onset of mental disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):603–613. doi:10.1001/archpsyc.62.6.603
21. Scott KM, Bruffaerts R, Tsang A, et al. Depression-anxiety relationships with chronic physical conditions: results from the World Mental Health Surveys. J Affect Disord. 2007;103(1–3):113–120. doi:10.1016/j.jad.2007.01.015
22. Alexopoulos GS. Depression in the elderly. Lancet. 2005;365(9475):1961–1970. doi:10.1016/s0140-6736(05)66665-2
23. Riemann D, Krone LB, Wulff K, Nissen C. Sleep, insomnia, and depression. Neuropsychopharmacology. 2020;45(1):74–89. doi:10.1038/s41386-019-0411-y
24. Kok RM, Reynolds CF, 3rd. Management of depression in older adults: a review. JAMA. 2017;317(20):2114–2122. doi:10.1001/jama.2017.5706
25. Yates WR, Mitchell J, John Rush A, et al. Clinical features of depression in outpatients with and without co-occurring general medical conditions in STAR*D: confirmatory analysis. Prim Care Companion J Clin Psychiatry. 2007;9(1):7–15. doi:10.4088/pcc.v09n0102
26. McIntyre RS, Rosenblat JD, Nemeroff CB, et al. Synthesizing the evidence for ketamine and esketamine in treatment-resistant depression: an international expert opinion on the available evidence and implementation. Am J Psychiatry. 2021;178(5):383–399. doi:10.1176/appi.ajp.2020.20081251
27. Bauer M, Adli M, Ricken R, Severus E, Pilhatsch M. Role of lithium augmentation in the management of major depressive disorder. CNS Drugs. 2014;28(4):331–342. doi:10.1007/s40263-014-0152-8
28. Nelson JC, Baumann P, Delucchi K, Joffe R, Katona C. A systematic review and meta-analysis of lithium augmentation of tricyclic and second generation antidepressants in major depression. J Affect Disord. 2014;168:269–275. doi:10.1016/j.jad.2014.05.053
29. Bauer M, Pfennig A, Severus E, Whybrow PC, Angst J, Möller HJ. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of unipolar depressive disorders, part 1: update 2013 on the acute and continuation treatment of unipolar depressive disorders. World J Biol Psychiatry. 2013;14(5):334–385. doi:10.3109/15622975.2013.804195
30. Fava M, Rush AJ. Current status of augmentation and combination treatments for major depressive disorder: a literature review and a proposal for a novel approach to improve practice. Psychother Psychosomat. 2006;75(3):139–153. doi:10.1159/000091771
31. Galling B, Calsina Ferrer A, Abi Zeid Daou M, Sangroula D, Hagi K, Correll CU. Safety and tolerability of antidepressant co-treatment in acute major depressive disorder: results from a systematic review and exploratory meta-analysis. Expert Opin Drug Saf. 2015;14(10):1587–1608. doi:10.1517/14740338.2015.1085970
32. Henssler J, Bschor T, Baethge C. Combining antidepressants in acute treatment of depression: a meta-analysis of 38 studies including 4511 patients. Can J Psychiatry. 2016;61(1):29–43. doi:10.1177/0706743715620411
33. Henssler J, Alexander D, Schwarzer G, Bschor T, Baethge C. Combining antidepressants vs antidepressant monotherapy for treatment of patients with acute depression: a systematic review and meta-analysis. JAMA Psychiatry. 2022;79(4):300–312. doi:10.1001/jamapsychiatry.2021.4313
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.