")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Clozapine Use in Patients with Early-Stage Schizophrenia in a Chinese Psychiatric Hospital
Authors Yi W, She S, Zhang J, Wu H, Zheng Y, Ning Y
Received 20 June 2020
Accepted for publication 9 November 2020
Published 24 November 2020 Volume 2020:16 Pages 2827—2836
DOI https://doi.org/10.2147/NDT.S261503
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jun Chen
Wenying Yi,1,2 Shenglin She,2 Jie Zhang,2 Haibo Wu,2 Yingjun Zheng,2 Yuping Ning1,2
1The First School of Clinical Medicine, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Psychiatry, The Affiliated Brain Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China
Correspondence: Yuping Ning
Department of Psychiatry, The Affiliated Brain Hospital of Guangzhou Medical University, No. 36 Mingxin Road, Liwan District, Guangzhou, People’s Republic of China
Tel +86-18922165368
Fax +86-020-82068107
Email [email protected]
Objective: Previous studies suggest that clozapine is commonly underutilized and that its initiation is delayed in patients with first-episode schizophrenia. Knowledge regarding clozapine use among Chinese patients with early-stage schizophrenia is limited. The aim of the present study was to investigate the point prevalence of and patterns and factors associated with clozapine use in patients with early-stage schizophrenia discharged from a psychiatric hospital in China.
Methods: A retrospective study was conducted to analyze the prescriptions of 867 consecutive patients with early-stage schizophrenia who were admitted to the Affiliated Brain Hospital of Guangzhou Medical University between Jan 1, 2011 and Dec 31, 2016.
Results: At discharge from the hospital, 114 (13.1%) patients were prescribed clozapine. Among the patients taking clozapine, 93 patients (81.6%) were prescribed clozapine polypharmacy, and only 21 patients (18.4%) were prescribed clozapine monotherapy. None of the patients were prescribed an overdose of clozapine. The mean daily dosage of clozapine was 160.97 mg, 149.05 mg and 213.69 mg among all patients taking clozapine, patients taking clozapine polypharmacy and patients taking clozapine monotherapy, respectively. The antipsychotic most frequently combined with clozapine was risperidone. Logistic regression suggested that the length of hospital stay, high school education, lower benzodiazepine use and antipsychotic polypharmacy were independently and significantly associated with clozapine use (P< 0.05).
Conclusion: Although clozapine has been commonly used in China in recent years, the present study found that clozapine was not commonly used in patients with early-stage schizophrenia. An underutilization and delayed initiation of clozapine may exist in a portion of patients with early-stage schizophrenia. Given the unfavorable outcomes of underutilized and delayed clozapine use, future studies may be needed to assess and increase clozapine use in this population.
Keywords: clozapine, early-stage, schizophrenia, China
Introduction
Treatment-resistant schizophrenia (TRS) has been reported to be associated with a higher risk of smoking, substance abuse, suicide ideation, severe adverse effects to antipsychotics, a poor quality of life and substantial economic burden and has annual costs that are 3–11 times higher than those of non-TRS.1 TRS is conservatively estimated to increase direct medical costs by more than $34 billion per year in the United States.1 Many studies and meta-analyses have confirmed the superiority of clozapine in treating patients with schizophrenia and TRS.2–5 For example, compared to other antipsychotics, clozapine could significantly improve the overall and positive symptoms,2 decrease the long-term all-cause mortality rate,3 reduce suicidal behaviors4 and shorten the length of hospital stay in treating schizophrenia.5 Even in treating elderly patients with chronic resistant schizophrenia, clozapine is efficacious and well tolerated.6 Compared with other antipsychotics, clozapine could significantly decrease mortality and rehospitalization over a five-year period in these elderly patients.6
However, clozapine has been found to be commonly underutilized in patients with schizophrenia in many countries and territories.7 For example, approximately 0.5–0.7% of the population worldwide suffers from schizophrenia, and approximately one-third of patients with schizophrenia show treatment resistance to antipsychotics; Bachmann et al estimated that the optimal prevalence of clozapine use should be 0.2% (200/100,000) in the adult population, but these authors found that the highest and lowest overall prevalence of clozapine use was 189.2/100,000 in Finland and 0.6/100,000 in Japan, respectively.7 That study suggested that the prevalence of clozapine use has increased in most counties/territories in recent years but that clozapine is still underutilized in many counties/territories.7 Patients with early-stage schizophrenia usually respond well to antipsychotics. However, a portion of patients with schizophrenia manifest treatment resistance to antipsychotics at the onset of schizophrenia, and the reported prevalence of TRS in patients with first-episode schizophrenia widely varies from 8.4% to 34%.8–12 However, clozapine was commonly underutilized, and its initiation was delayed among patients with first-episode schizophrenia.12–15 Approximately 0.7%-26.6% of patients with first-episode schizophrenia received clozapine treatment.12–18 The average time of the clozapine trial was 19.3 weeks and ranged from 7.6 to 45.0 weeks in patients with first-episode psychosis in Singapore.14 Another study conducted in Ireland reported that the average time to initiate clozapine among patients with first-episode psychosis was 6.7 years.15
Several reasons may explain the underutilization and delayed initiation of clozapine use. First, clozapine has been associated with several serious adverse effects, such as neutropenia,19 metabolic disturbance,20 sialorrhea,21 constipation,22 myocarditis and cardiomyopathy,23 suggesting that clozapine is not recommended as a first-line antipsychotic in the treatment of schizophrenia.24 In Chinese schizophrenia treatment guidelines, clozapine was recommended for the patients with TRS and should be trialed only after two antipsychotics have been considered ineffective following 6–8 weeks of treatment.24 The patients with schizophrenia receiving clozapine should receive mandatory blood monitoring weekly or biweekly during the first 6 months and biweekly of monthly thereafter.24 Previous studies have reported that clozapine has a low risk of agranulocytosis, but agranulocytosis leads to death,25 and such adverse effects hinder clozapine use and increase the cost and burden of blood monitoring.25,26 Regarding metabolic syndrome, a systematic review and meta-analysis suggested that the pooled metabolic syndrome prevalence in patients taking clozapine was 47.2%; patients taking clozapine had a significantly higher prevalence of metabolic syndrome than patients receiving other antipsychotics.20 Constipation was another common adverse effect of clozapine that could be fatal in a portion of patients.22 According to a systematic review and meta-analysis of 32 studies, the overall rate of clozapine-associated constipation was 31.2%, and treatment with clozapine was associated with an approximately threefold increased risk of constipation.22 In an Icelandic study involving 188 patients taking clozapine, 4 patients developed ileus, resulting in hospital admission, and 2 of these 4 patients required a permanent stoma because of the ileus.27 Second, prescriber inexperience could affect the choice of clozapine use. For example, Nielsen et al investigated the attitudes and knowledge of clozapine treatment among 100 psychiatrists and found that approximately 50% of psychiatrists prescribed clozapine to fewer than 5 patients.28 Most psychiatrists may prefer to use a high dosage of antipsychotics or antipsychotic polypharmacy than use clozapine to treat TRS.29 Furthermore, other barriers, such as difficulty in identifying patients with TRS, service fragmentation and lack of adherence by patients, lead to clozapine underutilization.25,26
However, a recent systematic review and meta-analysis of 34 articles involving 9386 patients with schizophrenia spectrum disorders suggested that the early use of clozapine could improve the outcome of patients with first-episode schizophrenia.30 Another systematic review demonstrated that delayed clozapine use was related to poor treatment outcomes among patients with TRS.31 Several studies suggested that clozapine should be attempted at the earliest phase of TRS.32–34 For example, a study comparing the safety of clozapine between first-episode patients with TRS and multiple-episode patients with TRS suggested that the rate of response to clozapine was negatively associated with age.32 Across patients with TRS taking clozapine, a study showed that the best predictive cut-off value for delaying the initiation of clozapine use for response was 2.8 years.33 In that study, the rate of response to clozapine among patients with a delay in initiating clozapine ≤2.8 years was 81.6%, but the rate of response to clozapine declined to 30.8% in patients taking clozapine for longer than 2.8 years.33 Joffe el al. showed that clozapine could be safe and improve the symptoms of patients with early TRS whose duration of schizophrenia ranged from 0.8 to 3.8 years.34 Moreover, these patients were likely to respond to a relatively low clozapine dose, with a mean dosage of 192.5 to 225.0 mg/day.34
Clozapine has been widely and commonly used to treat schizophrenia in China in recent years.35,36 For example, three Chinese national surveys concerning the use of antipsychotics in 2002–2012 suggested that 32.9% of 14,013 patients with schizophrenia were prescribed clozapine.35 However, knowledge regarding clozapine use in Chinese patients with early-stage schizophrenia is limited. Zhai et al reported that the prevalence of clozapine use in Chinese patients with first-episode schizophrenia was 2.7%.18 However, that study did not investigate the prescription patterns of and factors associated with clozapine use.18 Very limited studies explored the current clozapine use in early-stage schizophrenia in China; however, investigating the real-world use of clozapine in patients with early-stage schizophrenia is important to provide supporting evidence for future clinical decisions. Therefore, we conducted this study to investigate the point prevalence of and patterns and factors associated with clozapine use in consecutive patients with early-stage schizophrenia at the time of discharge from a psychiatric hospital in China.
Methods
This cross-sectional retrospective study was carried out at the Affiliated Brain Hospital of Guangzhou Medical University, which is one of the largest psychiatric hospitals in China, with 1920 beds for patients with mental disorders. This hospital was also the first psychiatric hospital in China and was established in 1898. According to a review, the most commonly criteria for define early-stage schizophrenia included experience of the first episode of schizophrenia or the duration of schizophrenia less than 1, 2 or 5 years.37 In the present study, A duration of schizophrenia no more than 2 years was defined as early-stage schizophrenia. Clozapine monotherapy was defined as the concurrent prescription of clozapine without another antipsychotics. Clozapine polypharmacy was defined as the concurrent prescription of clozapine with other antipsychotic medicine at the time of discharge from the hospital.
We screened the hospital’s electronic database and recorded the demographic, clinical and prescriptions data of all consecutive inpatients with early-stage schizophrenia who were admitted to the hospital between January 1, 2011, and December 31, 2016. If a patient was hospitalized multiple times during this period, only the data for the first hospitalization were included in the analysis. All included patients met the following criteria: (1) met the criteria of ICD10 for schizophrenia and were diagnosed by two experienced psychiatrists; (2) a schizophrenia duration ≤ 2 years; (3) age between 14 and 45 years; (4) Han Chinese ethnicity; (5) no mental retardation or serious physical diseases; and (6) no drug abuse or pregnancy.
The present study was approved by the Ethics Committee of the Affiliated Brain Hospital of Guangzhou Medical University (approval number: 2020014), and all principles outlined in the Declaration of Helsinki were followed. This study will not disclose the patient’s personal information and other private content. Because of the retrospective data, the present study met the following conditions for the waiver of informed consent: 1.The purpose of the present study was important. 2. The risk of the study to the patients was not greater than the minimum risk. 3.The waiver of informed consent would not badly affect the rights and health of the patients. 4. The privacy and personal identity information of the patients were protected. 5. If informed consent was required, the study would not be conducted. 6. Whenever possible, the researchers would provide the patients with appropriate information at an appropriate time after the present study. 7. If after the researchers reviewed the patient’s medical records and found that the patients and the guardians refused to use their medical records for future studies, the study would not use the data of the patients.
Statistical Analysis
A t-test (for the continuous variables) and chi-squared test (for the categorical variables) were used to compare the demographic and clinical variables between the patients taking clozapine and the patients not taking clozapine. A binary logistic regression analysis was used to identify the factors associated with clozapine use. The statistical analyses were performed with SPSS 19.0.
Results
Table 1 Shows the Sociodemographic and Clinical Characteristics of the Patients Taking Clozapine and the Patients Not Taking Clozapine
As shown in Table 1, in total, 867 consecutive patients with early-stage schizophrenia were included in the present study, including 520 males and 347 females. The average age was 26.7 years, and the mean duration of schizophrenia was 1.1 years in all patients. In total, 114 (13.1%) patients were prescribed clozapine, and 753 (86.9%) patients were not prescribed clozapine. There were no significant differences in gender, family history of psychosis and insurance status between the patients taking clozapine and the patients not taking clozapine (P>0.05). The patients taking clozapine were significantly younger, had a significantly longer duration of schizophrenia and had a significantly longer length of hospital stay than the patients not taking clozapine (P<0.05). There were significant differences in the marital status, education level, benzodiazepine use and antipsychotic polypharmacy between the patients taking clozapine and the patients not taking clozapine (P<0.05).
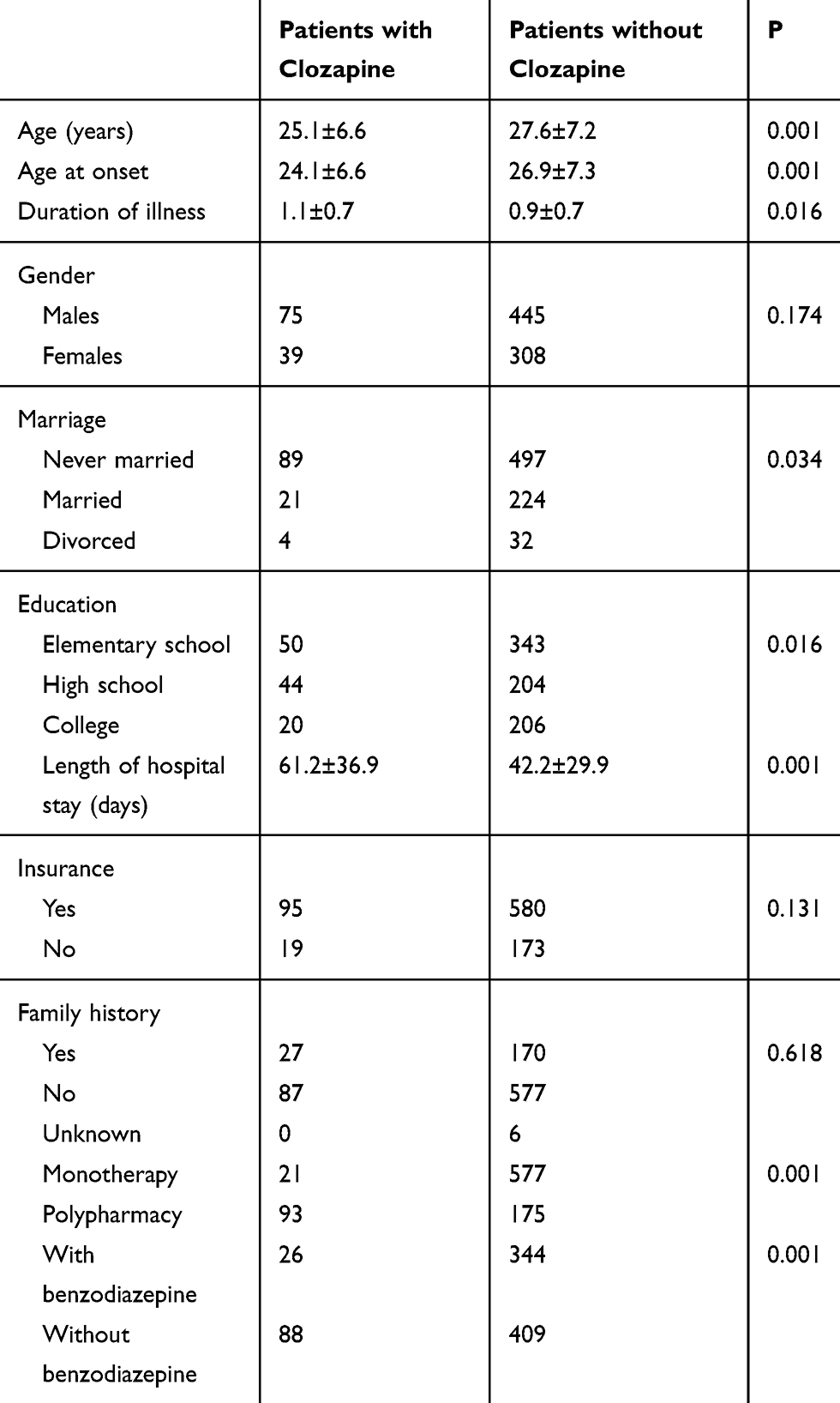 |
Table 1 Comparison of Demographics and Characteristics Between Patients with Clozapine and Patients Without Clozapine |
Table 2 Shows the Dosage of Clozapine in the Patients Taking Clozapine
Among the patients taking clozapine, 21 patients (18.4%) were prescribed clozapine monotherapy, and 93 patients (81.6%) were prescribed clozapine polypharmacy. The mean dosage of clozapine was 160.97 mg/d, 213.69 mg/d and 149.05 mg/d among all patients taking clozapine, the patients taking clozapine monotherapy and the patients taking clozapine polypharmacy, respectively. The mean dosage of clozapine in the patients taking clozapine monotherapy was significantly higher than that in the patients taking clozapine polypharmacy (P<0.05).
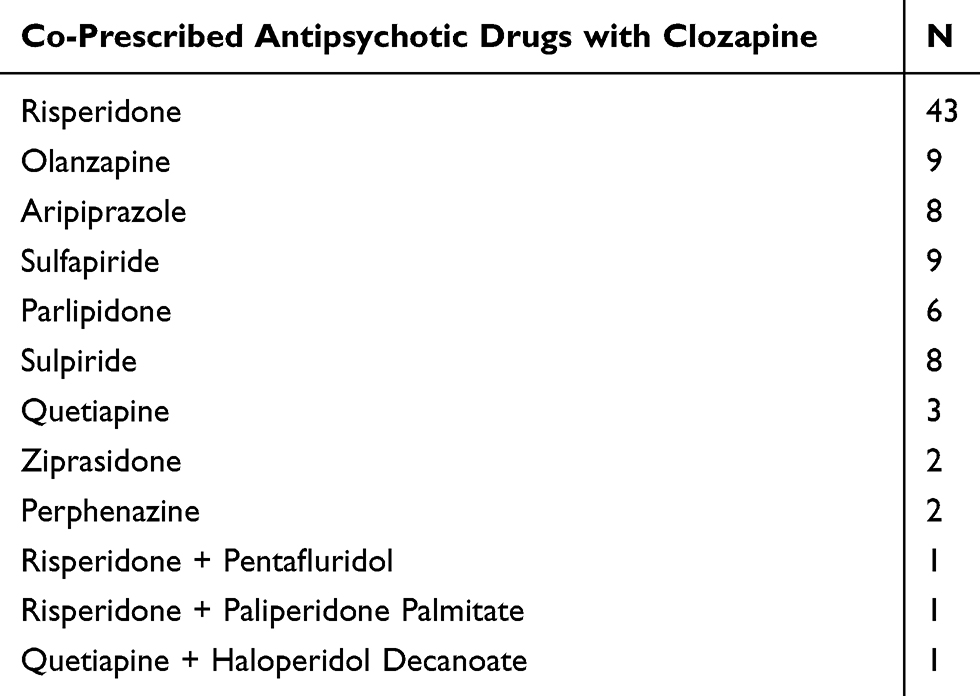 |
Table 2 Co-Prescribed Antipsychotic Drugs with Clozapine |
Table 3 Shows the Antipsychotic Combinations with Clozapine
Among the 93 patients receiving clozapine polypharmacy, 90 patients were prescribed clozapine combined with one antipsychotic, 3 patients were prescribed clozapine combined with two antipsychotics, 10 patients were prescribed clozapine combined with a typical antipsychotic, 80 patients were prescribed clozapine combined with an atypical antipsychotic, 2 patients were prescribed clozapine combined with a typical antipsychotic and an atypical antipsychotic, and 1 patient was prescribed two atypical antipsychotics.
 |
Table 3 Factors Associated with Clozapine Use |
There were 12 types of prescription patterns with clozapine. The antipsychotics most frequently combined with clozapine were risperidone (45/93, 48.4%), olanzapine (9/93, 9.7%), amisulpride (9/93, 9.7%), aripiprazole (8/93, 8.6%), sulpiride (8/93, 8.6%), paliperidone (6/93, 6.5%), quetiapine (4/93, 4.3%), ziprasidone (2/93, 2.2%), perphenazine (2/93, 2.2%), penfluridol (1/93, 1.1%), paliperidone palmitate (1.1%), and haloperidol depot (1/93, 1.1%).
Table 3 Shows the Factors Associated with Clozapine Use in Patients with Early-Stage Schizophrenia
The logistic regression suggested that the length of hospital stay, high school education, the use of fewer benzodiazepines and antipsychotic polypharmacy were independently and significantly associated with clozapine use (P<0.05).
Discussion
To the best of our knowledge, this study is the first to investigate the use of clozapine in patients with early-stage schizophrenia in China. In the present study, the prevalence of clozapine use in the patients with early-stage schizophrenia was 13.1%. The prevalence of clozapine use in our study is significantly lower than that in Chinese patients with chronic schizophrenia (26.4%-39.7%) from 2002 to 2012,35 but similar to the figures in Asian countries and territories (14.5%-15.9%) from 2001 to 2009.38 The prevalence of clozapine use in the present study is lower than that in an Irish study reporting a prevalence of 16.3% in patients with first-episode schizophrenia15 but higher than that in America (0.7%),16 Spain (2.4%),39 Singapore (4.3%)14 and UK (9.7%).9 Several reasons may account for the higher prevalence of clozapine use in the present study. First, clozapine is among the least expensive antipsychotics in China, as a 400 mg clozapine dose costs less than 1 dollar. Previously, clozapine was among the most commonly used antipsychotics in China.35,36 Chinese psychiatrists have vast experience with clozapine use. Second, the present study sample included only inpatients, who usually have more serious symptoms than outpatients or patients living in the community, and a relatively higher proportion of patients may show resistance to antipsychotics, leading to the need for a higher prevalence of clozapine use. Third, the present study enrolled patients with early-stage schizophrenia rather than only patients with first-episode schizophrenia, and a portion of the patients received antipsychotic treatment at the outpatient department. In addition, a portion of the patients may have multiple episodes of schizophrenia before being admitted to the hospital. Furthermore, clozapine could be used as a second-line antipsychotic for acute schizophrenia when patients do not respond to prior antipsychotic treatment according to the Chinese schizophrenia treatment guidelines.24
The prevalence of clozapine use in the present study is lower than most reported prevalence rates of TRS in patients with first-episode schizophrenia.8–12 Several reasons may lead to the relatively low prevalence of clozapine use. First, a portion of patients may refuse to take clozapine because of the adverse effects of clozapine or the regular blood monitoring required in our study.25,26 The lack of agreement of the patients may lead to the low prevalence of clozapine use reported in this study.25,26 Second, a portion of patients with TRS may have received psychotherapy or electroconvulsive therapy (ECT) in the present study. A 25-year systematic review and exploratory meta-analysis of 42 articles suggested that psychotherapy, especially cognitive behavioral therapy (CBT), could be beneficial for improving general psychopathology and positive symptoms among patients with TRS.40 ECT also plays an important role in treating schizophrenia. ECT has been proven to be effective and safe in patients with first-episode schizophrenia and chronic schizophrenia, especially in TRS.41 Psychotherapy and ECT are commonly conducted to treat schizophrenia in our hospital. A portion of patients may have received psychotherapy or ECT, leading to a lower clozapine prescription rate in the present study. Third, according to the schizophrenia treatment guidelines in China, clozapine should be used only after two different antipsychotics were ineffective following 6–8 weeks of treatment.24 The mean length of hospital stay was 58 days in the present study, and the length of hospital stay did not meet the criteria to prescribe clozapine. A portion of patients may be prescribed clozapine after they are discharged from the hospital. Fourth, a portion of patients were supposed to be treated with clozapine, but these patients may be prescribed antipsychotic polypharmacy. Psychiatrists usually do not prefer to prescribe clozapine, and clozapine was the fifth preference for treating TRS in the US.29 Fifth, although clozapine is widely used in China, the prescription of clozapine for schizophrenia has gradually decreased in recent years.35,36 Moreover, the data from the first discharge may underestimate the use of clozapine in the present study.
Compared with a previous study reporting that the prevalence of clozapine use was 2.9% among patients with first-episode schizophrenia in China,18 clozapine use was significantly higher in our study. The difference in the study populations may account for this gap. Clozapine is not recommended as the first choice for treating patients with first-episode schizophrenia in China;24 thus, only 2.9% of patients with first-episode schizophrenia were prescribed clozapine in that study. However, the present study enrolled patients with early-stage schizophrenia, and a portion of these patients had multiepisode schizophrenia in the present study, leading to a higher prevalence of clozapine use.
In China, the schizophrenia treatment guidelines recommend a dosage of clozapine within 300–800 mg/d for the treatment of acute patients with multiepisode schizophrenia.24 No patients were prescribed an excessive dosage of clozapine in the present study. The average clozapine dosage in clozapine monotherapy was significantly higher than that in clozapine polypharmacy. This finding likely reflects that the patients with clozapine polypharmacy may have switched to clozapine from a prior antipsychotic, as slow titration and cross switching antipsychotics are often used to decrease the adverse effects of antipsychotics in clinic practice. The mean dosage of clozapine in the present study was lower than that in Western studies of first-episode schizophrenia.15,16,39 Ethnic differences may account for the difference in the clozapine dosage. For example, Chong et al reported that the mean daily clozapine dosage was 408 mg/day and 169 mg/day among Canadian subjects and an Asian sample, respectively.42 Furthermore, a recent review demonstrated that Asians usually need lower clozapine doses than Caucasians, and the mean clozapine dosage was usually lower than 300 mg/day in Asian countries, while Caucasians need a mean clozapine dosage of 300 to 600 mg/day to achieve a therapeutic effect.43 Interestingly, Ballon et al suggested that slow titration with clozapine could achieve a sustained response at a low maintenance dose of 81 mg/d in patients with a duration of psychosis no longer than 1 year.44 Future trials may need to verify the low dosage of clozapine use in Chinese patients with early-stage schizophrenia.
Risperidone was the antipsychotic most frequently prescribed in combination with clozapine in the present study, which is consistent with the findings reported in the three national surveys concerning the use of antipsychotics in China.35 Risperidone is also among the least expensive antipsychotics and costs less than 1 dollar for 4 mg in China.35 Risperidone has a good effect, is safe and is commonly used to treat schizophrenia in China. In the present study, risperidone was the most frequently used antipsychotic in antipsychotic monotherapy and antipsychotic polypharmacy. An Australian study also noted that risperidone was the most commonly used antipsychotic medication for the first trial in patients with early psychosis.12 One possible explanation may be that a portion of patients did not respond to risperidone; thus, these patients may have switched to clozapine from risperidone at the time of discharge from the hospital. The findings of a recent review and meta-analysis suggest that 81.3% of patients with first-episode schizophrenia could respond to antipsychotics with a 20% PANSS/BPRS reduction from baseline, while 51.9% of patients with first-episode schizophrenia could respond to antipsychotics with a 50% PANSS/BPRS reduction from baseline.45 According to that study, 19.7–38.1% of patients with first-episode schizophrenia need to switch to another antipsychotic. The schizophrenia treatment guidelines in China recommend that patients should receive a sufficient dosage of an antipsychotic for 4–6 weeks before they switch to another.24 Given that several studies reported that an early response to antipsychotics could predict the outcome, there is no need to wait for 4–6 weeks to switch antipsychotics. However, a short hospital stay may lead to the sustained use of two antipsychotics. Consequently, a case report and review demonstrated that the combination of clozapine and risperidone was well tolerated and effective in treating patients with clozapine-resistant schizophrenia.46 Psychiatrists may have added clozapine to treat a portion of patients who did not respond well to risperidone in the present study.
Benzodiazepine use was significantly negatively associated with clozapine use in the present study. The prevalence of benzodiazepine use among patients with clozapine was 22.8% in the present study. A lower prevalence of benzodiazepine use among patients with clozapine use, ie, 7%, was reported in a previous study.47
One possible explanation is the fact that benzodiazepines combined with clozapine are not recommended for treating schizophrenia in China.24 Thus, several studies suggest that clozapine combined with benzodiazepines did not lead to improvement in TRS but increased the risk of adverse effects.48,49 A large population-based cohort study demonstrated that the combined use of clozapine and benzodiazepines was significantly associated with a risk of pneumonia in patients with schizophrenia.50 Furthermore, clozapine is often associated with sedation.51,52 In total, 49.6–64.7% of patients taking clozapine experienced sedation associated with clozapine.51,52 The effect of sedation induced by clozapine could decrease benzodiazepine use, which may be used for insomnia and the agitated behavior of patients with schizophrenia. A previous study also reported that benzodiazepine use declined in a group of outpatients with schizophrenia after initiating clozapine.53
Our study found that clozapine use was significantly associated with antipsychotic polypharmacy, which is consistent with previous studies.35,47,54,55 For example, Pai et al suggested that 72% of patients using clozapine were prescribed another antipsychotic.47 The findings in three public hospitals in Sydney showed that 32.1% of 451 registered clozapine clinic attenders were prescribed another antipsychotic.54 In Iceland, 65.6% of patients taking clozapine received at least one other antipsychotic.55 In total, 48.9% of patients taking clozapine were prescribed another antipsychotic in the three national surveys concerning antipsychotics among schizophrenic patients in China.35 According to a systematic review and meta-analysis, only 40% of patients with TRS respond to clozapine, and it was estimated that 12% to 20% of patients with schizophrenia could be ultraresistant.56 For these patients who do not respond to clozapine, other antipsychotics may be used to augmentation strategies, but no high-quality studies verified the efficacy of clozapine augmentation strategies.56 Another possible explanation may be that a portion of patients was switched to clozapine from a prior antipsychotic at the time of discharge from the hospital. Because of the slow titration and cross titration, there may not have been sufficient time to discontinue the prior antipsychotic during hospitalization.
According to previous studies, a higher educational level is positively correlated with the clinical response and functional outcome.57,58 A primary education level was found to be significantly associated with TRS in Denmark.57 A university education was significantly related to a better functional outcome in treatment-resistant psychotic patients taking clozapine.58 The present study found that a high school education was significantly related to clozapine use, suggesting that patients with a relatively lower education level may be at a higher risk when receiving clozapine treatment.
Clozapine use was independently and significantly associated with the length of hospital stay in the present study. Clozapine could significantly shorten the length of hospital stay,5 but it is difficult to identify TRS in early-stage schizophrenia, especially in patients who are first admitted to the hospital because of schizophrenia. A longer length of hospital stay is usually associated with more serious symptoms and treatment resistance. A population-based cohort study in Denmark reported that a length of hospital stay longer than 30 bed-days in a psychiatric hospital in previous years was significantly associated with TRS.57 Although our study did not investigate the time when clozapine was initiated, the findings may reflect that a portion of the patients show resistance to antipsychotics after being hospitalized for a long period. Thus, patients taking clozapine usually have an insufficient response to prior antipsychotics, which may lead to the need for a longer time to achieve clinical remission.
There were several limitations in our study. First, the present study was conducted in only one psychiatric hospital in China and only enrolled inpatients with early-stage schizophrenia, while outpatients with early-stage schizophrenia were not included. It is well known that there are regional differences in clozapine use in China.36 The sample in the present study cannot represent all patients with early-stage schizophrenia in China. However, the present study examined clozapine use over a relatively long period of 6 years, and our hospital is the first and one of the largest psychiatric hospital in China, with 1920 beds.
Second, because of the retrospective study design, the present study did not assess the severity of symptoms before and after clozapine use, the prevalence of TRS, the reason for clozapine use and the duration of clozapine use. Hence, we could not determine the efficacy of clozapine, whether clozapine was used to treat patients with TRS or whether the use of clozapine was rational. Third, our study only assessed the point prevalence of clozapine use at the time of discharge from the hospital. A portion of patients may have discontinued clozapine before discharge from the hospital because of several serious adverse effects or for other reasons. Moreover, ECT and CBT, which can improve the symptoms of schizophrenia, were commonly conducted in our hospital and may have decreased clozapine use in the present study. However, the present study did not examine the use of ECT and CBT. The actual prevalence of clozapine use may be affected by these factors. Fourth, our study did not document the time of clozapine initiation and the antipsychotics used before clozapine; thus, the results cannot reflect the delayed time of clozapine use in patients with early-stage schizophrenia. Furthermore, the data from the first discharge also may underestimate the use of clozapine. However, the present study is the first to investigate clozapine use in a relatively large sample of 867 patients with early-stage schizophrenia over a relatively long period of 6 years. This study could partially reflect clozapine use in the real world in China.
In conclusion, although clozapine has been commonly used to treat schizophrenia in recent years in China, it was not commonly used in early-stage schizophrenia in the present study. According to the reported prevalence of TRS in early-stage schizophrenia, clozapine may be underused, and its initiation may be delayed in a portion of patients in the present study. Delayed clozapine use was usually associated with unfavorable outcomes. Future studies may be needed to assess and increase clozapine use in patients with early-stage schizophrenia.
Funding
The present study was funded by Science and Technology Plan Project of Guangdong Province (No. 2019B030316001), Planed science and technology Projects of Guangzhou (No. 201904010267).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kennedy JL, Altar C, Taylor DL, et al. The social and economic burden of treatment-resistant schizophrenia: a systematic literature review. Int Clin Psychopharmacol. 2014;29(2):63–76. doi:10.1097/YIC.0b013e32836508e6
2. Siskind D, Mccartney L, Goldschlager R, et al. Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis. Br J Psychiatry. 2016;209(5):385–392. doi:10.1192/bjp.bp.115.177261
3. Vermeulen JM, Van Rooijen G, De Kerkhof MV, et al. Clozapine and Long-Term Mortality Risk in Patients With Schizophrenia: A Systematic Review and Meta-analysis of Studies Lasting 1.1–12.5 Years. Schizophr Bull. 2019;45(2):315–329. doi:10.1093/schbul/sby052
4. Hennen J, Baldessarini RJ. Suicidal risk during treatment with clozapine: a meta-analysis. Schizophr Res. 2005;73(2):139–145. doi:10.1016/j.schres.2004.05.015
5. Land R, Siskind D, Mcardle P, et al. The impact of clozapine on hospital use: a systematic review and meta-analysis. Acta Psychiatr Scand. 2017;135(4):296–309. doi:10.1111/acps.12700
6. Pridan S, Swartz M, Baruch Y, et al. Effectiveness and safety of clozapine in elderly patients with chronic resistant schizophrenia. Int Psychogeriatr. 2015;27(1):131–134. doi:10.1017/S1041610214001756
7. Bachmann C, Aagaard L, Bernardo M, et al. International trends in clozapine use: a study in 17 countries. Acta Psychiatr Scand. 2017;136(1):37–51. doi:10.1111/acps.12742
8. Yoshimura B, Sato K, Takaki M, et al. Algorithm-based pharmacotherapy for first-episode schizophrenia involuntarily hospitalized: A retrospective analysis of real-world practice. Early Interv Psychiatry. 2019;13(1):39–46. doi:10.1111/eip.12442
9. Tungaraza TE, Ahmed W, Chira C, et al. Prescribing pattern of clozapine and other antipsychotics for patients with first-episode psychosis: a cross-sectional survey of early intervention teams. Ther Adv Psychopharmacol. 2017;7(3):103–111. doi:10.1177/2045125316683151
10. Lally J, Ajnakina O, Forti MD, et al. Two distinct patterns of treatment resistance: clinical predictors of treatment resistance in first-episode schizophrenia spectrum psychoses. Psychol Med. 2016;46(15):3231–3240. doi:10.1017/S0033291716002014
11. Demjaha A, Lappin J, Stahl D, et al. Antipsychotic treatment resistance in first-episode psychosis: prevalence, subtypes and predictors. Psychol Med. 2017;47(11):1981–1989. doi:10.1017/S0033291717000435
12. Thien K, Bowtell M, Eaton S, et al. Clozapine use in early psychosis. Schizophr Res. 2018;199:374–379. doi:10.1016/j.schres
13. Üçok A, Çıkrıkçılı U, Ergül C. Correlates of Clozapine Use after a First Episode of Schizophrenia: results From a Long-term Prospective Study. CNS Drugs. 2016;30(10):997–1006. doi:10.1007/s40263-016-0358-z
14. Tang C, Subramaniam M, B T N, et al. Clozapine Use in First-Episode Psychosis: the Singapore Early Psychosis Intervention Programme (EPIP) Perspective. J Clin Psychiatry. 2016;77(11):1447–1453. doi:10.4088/JCP.15m10063
15. Doyle R, Behan C, O’keeffe D, et al. Clozapine Use in a Cohort of First-Episode Psychosis. J Clin Psychopharmacol. 2017;37(5):512–517. doi:10.1097/JCP.0000000000000734
16. Robinson DG, Schooler NR, John M, et al. Prescription Practices in the Treatment of First-Episode Schizophrenia Spectrum Disorders: data From the National RAISE-ETP Study. Am J Psychiatry. 2015;172(3):237–248. doi:10.1176/appi.ajp.2014.13101355
17. Kreyenbuhl JA, Medoff DR, Mcevoy JP, et al. The RAISE Connection Program: psychopharmacological Treatment of People With a First Episode of Schizophrenia. Psychiatr Serv. 2016;67(12):1300–1306. doi:10.1176/appi.ps.201500438
18. Zhai D, Cui T, Xu Y, et al. Cardiometabolic risk in first-episode schizophrenia (FES) patients with the earliest stages of both illness and antipsychotic treatment. Schizophr Res. 2017;179:41–49. doi:10.1016/j.schres.2016.09.001
19. Myles N, Myles H, Xia S, et al. Meta‐analysis examining the epidemiology of clozapine‐associated neutropenia. Acta Psychiatr Scand. 2018;138(2):101–109. doi:10.1111/acps.12898
20. Vancampfort D, Stubbs B, Mitchell AJ, et al. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: a systematic review and meta-analysis. World Psychiatry. 2015;14(3):339–347. doi:10.1002/wps.20252
21. Tessier P. Antonello C. Clozapine and Sialorrhea: update. Psychiatry Neurosci. 2001;26(3):253.
22. Shirazi A, Stubbs B, Gomez L, et al. Prevalence and predictors of clozapine-associated constipation: a systematic review and meta-analysis. Int J Mol Sci. 2016;17(6):863. doi:10.3390/ijms17060863
23. Siskind D, Sidhu A, Cross J, et al. Systematic review and meta-analysis of rates of clozapine-associated myocarditis and cardiomyopathy. Aust N Z J Psychiatry. 2020;54(5):467–481. doi:10.1177/0004867419898760
24. Shu L, Ed.. Guidelines for Prevention and Treatment of Schizophrenia. Peking University Medical Press; 2007.
25. Sharma A, Grover S. Delay in starting clozapine and treatment guidelines. Br J Psychiatry. 2013;202(2):154–155. doi:10.1192/bjp.202.2.154b
26. Farooq S, Choudry A, Cohen D, et al. Barriers to using clozapine in treatment-resistant schizophrenia: systematic review. BJPsych Bull. 2019;43(1):8–16. doi:10.1192/bjb.2018.67
27. Ingimarsson O, Maccabe JH, Sigurdsson E. Constipation, ileus and medication use during clozapine treatment in patients with schizophrenia in Iceland. Nord J Psychiatry. 2018;72(7):497–500. doi:10.1080/08039488.2018.1517189
28. Nielsen J, Dahm M, Lublin H, et al. Psychiatrists’ attitude towards and knowledge of clozapine treatment. J Psychopharmacol. 2010;24(7):965–971. doi:10.1177/0269881108100320
29. Correll CU, Brevig T, Brain C, et al. Patient characteristics, burden and pharmacotherapy of treatment-resistant schizophrenia: results from a survey of 204 US psychiatrists. BMC Psychiatry. 2019;19(1):362. doi:10.1186/s12888-019-2318-x
30. Okhuijsenpfeifer C, A Y S, I M H, et al. Demographic and clinical features as predictors of clozapine response in patients with schizophrenia spectrum disorders: A systematic review and meta-analysis. Neurosci Biobehav Rev. 2020;111:246–252. doi:10.1016/j.neubiorev.2020.01.017
31. Shah P, Iwata Y, Plitman E, et al. The impact of delay in clozapine initiation on treatment outcomes in patients with treatment-resistant schizophrenia: A systematic review. Psychiatry Res. 2018;268:114–122. doi:10.1016/j.psychres.2018.06.070
32. Hofer A, Hummer M, Kemmler G, et al. The safety of clozapine in the treatment of first- and multiple-episode patients with treatment-resistant schizophrenia. Int J Neuropsychopharmacol. 2003;6(3):201–206. doi:10.1017/S1461145703003456
33. Yoshimura B, Yada Y, So R, et al. The critical treatment window of clozapine in treatment-resistant schizophrenia: secondary analysis of an observational study. Psychiatry Res. 2017;250:65–70. doi:10.1016/j.psychres
34. Joffe G, Rybak J, Burkin M, et al. Clozapine response in early treatment-resistant schizophrenia. Int J Psychiatry Clin Pract. 1997;1(4):261–268. doi:10.3109/13651509709024737
35. Li Q, Xiang Y, Su Y, et al. Clozapine in schizophrenia and its association with treatment satisfaction and quality of life: findings of the three national surveys on use of psychotropic medications in China (2002-2012). Schizophr Res. 2015;168(1–2):523–529. doi:10.1016/j.schres.2015.07.048
36. T M S, Y S Z, Shu L, et al. Use of clozapine for the treatment of schizophrenia: findings of the 2006 research on the China Psychotropic Prescription Studies. Clin Psychopharmacol Neurosci. 2012;10(2):99–104. doi:10.9758/cpn.2012.10.2.99
37. Newton R, Rouleau A, Nylander AG, et al. Diverse Definitions of the Early Course of Schizophrenia-A Targeted Literature Review. NPJ Schizophr. 2018;4(1):21. doi:10.1038/s41537-018-0063-7
38. Xiang Y, Wang C, Si T, et al. Clozapine use in schizophrenia: findings of the research on Asia Psychotropic Prescription (REAP) Studies from 2001 to 2009. Aust N Z J Psychiatry. 2011;45(11):968–975. doi:10.3109/00048674.2011.607426
39. Bioque M, Llerena A, Cabrera B, et al. A pharmacovigilance study in first episode of psychosis: psychopharmacological interventions and safety profiles in the PEPs Project. Int J Neuropsychopharmacol. 2016;19(4):pyv121. doi:10.1093/ijnp/pyv121
40. Polese D, Fornaro M, Palermo M, et al. Treatment-resistant to antipsychotics: a resistance to everything? Psychotherapy in treatment-resistant schizophrenia and nonaffective psychosis: a 25-year systematic review and exploratory meta-analysis. Front Psychiatry. 2019;10:210. doi:10.3389/fpsyt.2019.00210
41. Grover S, Sahoo S, Rabha A, et al. ECT in schizophrenia: a review of the evidence. Acta Neuropsychiatr. 2019;31(3):115–127. doi:10.1017/neu.2018.32
42. S A C, G J R, Lee N, et al. Contrasting clozapine prescribing patterns in the east and west? Ann Acad Med Singapore. 2000;29(1):75–78.
43. De Leon J, A P R, A R K, et al. Do asian patients require only half of the clozapine dose prescribed for caucasians? A critical overview. Indian J Psychol Med. 2020;42(1):4–10. doi:10.4103/IJPSYM.IJPSYM_379_19
44. J S B, Ashfaq H, Noordsy DL. Clozapine titration for people in early psychosis: A chart review and treatment guideline. J Clin Psychopharmacol. 2018;38(3):234–238. doi:10.1097/JCP.0000000000000860
45. Zhu Y, Li C, Huhn M, et al. How well do patients with a first episode of schizophrenia respond to antipsychotics: A systematic review and meta-analysis. Eur Neuropsychopharmacol. 2017;27(9):835–844. doi:10.1016/j.euroneuro.2017.06.011
46. Lerma-Carrillo I, J D M, Cuevas-Durán T, et al. Adjunctive treatment with risperidone in clozapine-resistant schizophrenia: a case report and review. Clin Neuropharmacol. 2007;30(2):114–121. doi:10.1097/01.wnf.0000240947.51994.96
47. N B P, Laidlaw M, Vella S-C. Augmentation of clozapine with another pharmacological agent: treatment for refractory schizophrenia in the ‘real world’. Acta Psychiatr Scand. 2012;126(1):40–46. doi:10.1111/j.1600-0447.2012.01854.x
48. S A C, Clozapine Augmentation: RG. Safety and Efficacy. Schizophr Bull. 2000;26(2):421–440. doi:10.1093/oxfordjournals.schbul.a033463
49. Meltzer HY. Treatment-resistant schizophrenia–the role of clozapine. Curr Med Res Opin. 1997;14(1):1–20. doi:10.1185/03007999709113338
50. C S W. Estimating the risk of pneumonia in patients with schizophrenia newly receiving clozapine: a nationwide cohort study. J Clin Psychopharmacol. 2019;39(4):297–304. doi:10.1097/JCP.0000000000001052
51. S R P, R S Q, Mane A, et al. An observational study of clozapine induced sedation and its pharmacological management. Eur Neuropsychopharmacol. 2016;26(1):156–161. doi:10.1016/j.euroneuro
52. Delgado A, Velosa J, Zhang J, et al. Clozapine in bipolar disorder: A systematic review and meta-analysis. J Psychiatr Res. 2020;125:21–27. doi:10.1016/j.jpsychires.2020.02.026
53. S A C, G J R, Bezchlibnyk-Butler KZ. Effect of clozapine on polypharmacy. Psychiatr Serv. 2000;51(2):250–252. doi:10.1176/appi.ps.51.2.250
54. J M L, Wijaya M, Watkins A, et al. Cardio-metabolic risk and its management in a cohort of clozapine-treated outpatients. Schizophr Res. 2018;199:367–373. doi:10.1016/j.schres.2018.02.035
55. Ingimarsson O, J H M, Haraldsson M, et al. Clozapine treatment and discontinuation in Iceland: A national longitudinal study using electronic patient records. Nord J Psychiatry. 2016;70(6):450–455. doi:10.3109/08039488.2016.1155234
56. Wagner E, Lohrs L, Siskind D, et al. Clozapine augmentation strategies – a systematic meta-review of available evidence. Treatment options for clozapine resistance. J Psychopharmacol. 2019;33(4):423–435. doi:10.1177/0269881118822171
57. Wimberley T, Støvring H, Sørensen HJ, et al. Predictors of treatment resistance in patients with schizophrenia: a population-based cohort study. Lancet Psychiatry. 2016;3(4):358–366. doi:10.1016/S2215-0366(15)00575-1
58. Ciapparelli A, Ducci F, Carmassi C, et al. Predictors of response in a sample of treatment-resistant psychotic patients on clozapine. Eur Arch Psychiatry Clin Neurosci. 2004;254(5):343–346. doi:10.1007/s00406-004-0511-4
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.