Back to Journals » Infection and Drug Resistance » Volume 16
Clostridium paraputrificum Bacteremia in a Patient with Human Immunodeficiency Virus Infection: A Case Report and Literature Review
Authors Hosin N, Abu-Ali BM ![]() , Al Rashed AS
, Al Rashed AS ![]() , Al-Warthan SM, Diab AE
, Al-Warthan SM, Diab AE
Received 16 December 2022
Accepted for publication 6 March 2023
Published 14 March 2023 Volume 2023:16 Pages 1449—1454
DOI https://doi.org/10.2147/IDR.S400490
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Nehal Hosin,1,* Batool M Abu-Ali,2,* Abdullatif S Al Rashed,1,* Sara M Al-Warthan,3,* Asim E Diab1,*
1Department of Microbiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Department of Internal Medicine, Infectious Diseases Division, King Fahad Hospital, Hofuf, Saudi Arabia; 3Department of Internal Medicine, King Fahd Hospital of the University (Imam Abdulrahman Bin Faisal University), Al Khobar, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Abdullatif S Al Rashed, Department of Microbiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia, Tel +966555969048, Email [email protected]
Abstract: Clostridium paraputrificum (C. paraputrificum) is clinically important due to its association with underlying medical conditions. Infection with C. paraputrificum may worsen HIV prognosis, leading to acquired immunodeficiency syndrome. However, it is not frequently isolated and its susceptibility to antibiotics has not been well studied. Our report examines the case of a patient with human immunodeficiency virus (HIV) infection, who was diagnosed with Clostridium paraputrificum bacteremia. A 59-year-old male was admitted to hospital with a medical history of human immunodeficiency virus (HIV), hepatitis C virus (HCV), and neck pain. Following episodes of high fever, the patient received a full work up to test for sepsis. Blood culture revealed bacterial growth, and MALDI-TOF mass spectrometry confirmed the diagnosis of Clostridium paraputrificum bacteremia. The patient received treatment with meropenem and vancomycin antibiotics, which cleared the infection after 48 hours; however, inflammatory markers remained high. To date, a limited number of reported cases of C. paraputrificum exist; thus, this case report contributes valuable information to the literature to improve our understanding of its action and resistance profiles and aid future bacteremia management.
Keywords: clostridia, gram-positive bacteria, anaerobe, pathogen, hepatitis C, hepatitis B
Background
Clostridium species (spp.) are obligatory, anaerobic, gram-positive bacteria responsible for a wide range of invasive infections in humans, including bacteremia.1 The genus is large and diverse, composed of >164 species, such as Clostridium perfringens, Clostridium botulinum, Clostridium tetani, and Clostridium difficile, which can cause clinical syndromes in humans. Clostridium can be difficult to treat due to its capacity to produce antibiotic-resistant endospores.2 Blood infections with this bacteria have been frequently reported in patients with underlying medical diseases, such as colon cancer, acquired immunodeficiency syndrome (AIDS), hemodialysis, inflammatory enteropathy, septic arthritis, and sickle cell disease.3–6 The mortality rate of clinically relevant clostridial bacteremia ranges from 29% to 35%, and the risk factors for mortality are liver disease and older age.7
Despite the numerous complications associated with Clostridium spp. infections, C. paraputrificum is not well described. The aim of this article was to present a case report of a patient with HIV infected with C. paraputrificum bacteremia and provide a brief overview of relevant literature. Our findings will further our understanding of the impacts of anaerobic pathogens on human health and help inform the development of more effective treatment management of Clostridium spp.; particularly, patients with underlying medical conditions.
Case
Initial Presentation & Past History
The patient was a 59-year-old male from Dammam, Saudi Arabia with a history of HIV for 15 years, who was non-compliant to HIV treatment for five years. The patient last visited the HIV clinic in December 2020 and blood tests showed a viral load of 9340 copies per mL. Furthermore, this person had a history of HBV (immune to hepatitis B due to natural immunity), chronic non-treated HCV, diabetes mellitus type II for three years, hypertension (HTN), smoking and active drug abuse for heroin and alcohol, chronic kidney disease stage III, and a previously treated cervical spine abscess with internal fixation surgery. The patient was prescribed tenofovir and emtricitabine; no antiretroviral resistance screening test was performed, and we could not obtain lymphocyte subset results. Prior to emergency department (ER) admittance, the patient had three months history of progressive neck pain, and sudden weakness in the upper and lower limbs the day before presenting to the ER; however, they experienced no numbness, loss of sphincter control, fever, night sweats, or weight loss. The results of the patient’s physical examination, blood pressure and other vital signs were normal, and neuromuscular examination results were unremarkable. However, laboratory blood test results revealed a high white blood cell (WBC) count, decreased hemoglobin level (Hgb), and high platelet count (Plt). The patient’s serum creatinine level was 2.54 mg/dL and blood urea nitrogen was 45 mg/dL. Notably, there were elevated levels of inflammatory markers, such as procalcitonin and C-reactive protein, and erythrocyte sedimentation rate. A brain computed tomography (CT) revealed chronic small vessel disease, with a number of lytic lesions on the patient’s first cervical vertebra.
Present History
Seven days post admission, the patient experienced fever (38.8°C), in addition to persistent and uncontrolled high blood pressure; however, a physical examination showed no evidence of limited movement or mobility. Prior to receiving blood culture results for sepsis testing, vancomycin and meropenem antibiotics were empirically prescribed. The patient received a complete work-up, and was tested for complete blood count (CBC), C-reactive protein (CRP), procalcitonin, and blood and urine cultures.
Laboratory Investigation
The septic workup results showed a high WBC count and high levels of inflammatory markers, including CRP and procalcitonin (Table 1).
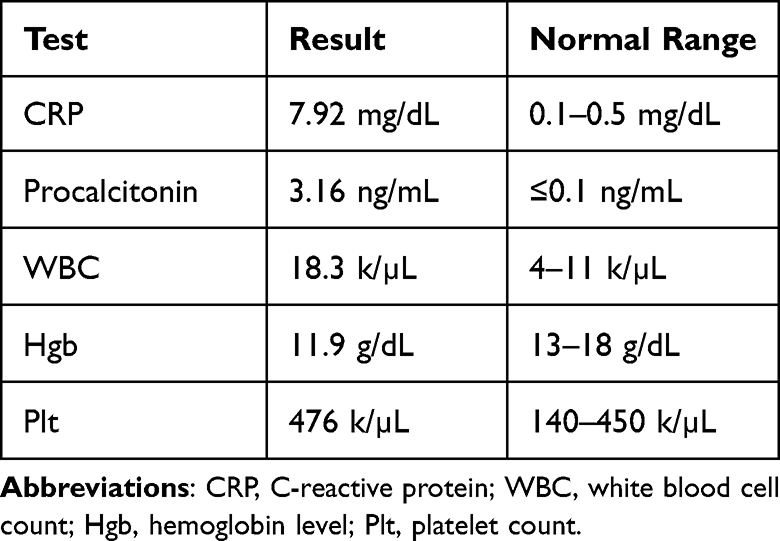 |
Table 1 Laboratory Results for the Patient After Developing Fever |
Microbiology Investigation
We incubated one set of blood culture vials in a BacT/Alert Virtuo system (BioMérieux, France) for 5 days, according to the internal policies and procedures of the microbiology laboratory at King Fahd Hospital of the University. After 72 hours of incubation, one of the two blood culture vials flagged positive, and direct Gram staining showed Gram-positive bacilli. Subsequently, the blood culture vials were sub-cultured on sheep blood, MacConkey, chocolate, and anaerobic Brucella agars.
After 48 hours incubation at 37°C, there was no growth present on sheep blood, MacConkey’s, and chocolate agars. However, there was bacterial growth on anaerobic Brucella agar (Figure 1). We used Matrix-assisted laser desorption/ionization-time of flight-mass spectrometry (MALDI-TOF-MS) (VITEK MS; bioMérieux) and the Knowledge Base database (version 3.0) with a confidence value of 99.9% to identify Clostridium paraputrificum. Antibiotics-susceptibility tests for anaerobic organisms were not available in our routine diagnostic laboratory; therefore, we depended on 2022 Clinical and Laboratory Standards Institute (CLSI) cumulative data, which showed that Clostridium was sensitive to imipenem, meropenem, and metronidazole antibiotics. Urine analysis results were normal, and the urine culture showed no growth.
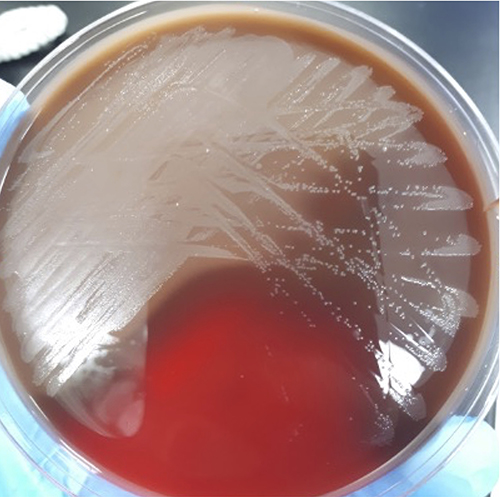 |
Figure 1 Nonhemolytic, translucent pinpoint colonies grew on anaerobic Brucella Agar. Abbreviations: HIV, human immunodeficiency virus; C. paraputrificum, Clostridium paraputrificum, Clostridium spp., Clostridium species; HCV, Hepatitis C virus; MALDI-TOF, Matrix-assisted laser desorption/ionization-time of flight; HBV, hepatitis B virus; HTN, hypertension; ER, emergency department; WBC, white blood cell count; Hgb, hemoglobin level; Plt, platelet count; CT, computed tomography; CBC, complete blood count; CRP, C-reactive protein; CLSI, Clinical Laboratory Standards Institute. |
Treatment Plan and Outcome
Forty-eight hours following treatment with vancomycin and meropenem antibiotics, the patient clinically improved, the fever subsided, and blood cultures showed no growth. All subsequent cultures were negative, but inflammatory markers remained high. On day 12 of admission, the patient experienced sudden cardiac arrest due to reflex arrhythmia caused by atlantoaxial subluxation and passed away.
Discussion
Clostridium spp. are widespread in nature owing to their ability to form resistant endospores.8 Infection with Clostridium species occurs at an annual rate of 1.8/100,000 persons,1 and a mortality rate ranging from 29% to 35% from clinically relevant clostridial bacteremia. Risk factors for mortality include liver disease and older age;7 Clostridium paraputrificum is a rare isolate, comprising only ~1% of all Clostridium cases.1
Clostridia are opportunistic bacteria, generally encountered in wounds, exudates, blood, and other normally sterile body fluids. Infection with Clostridium spp. may not develop into serious or progressive disease, unless conditions in the host are favorable. Owing to the inherent difficulty of performing susceptibility assays for anaerobes, new methods using phenotypic and molecular techniques are in development.21 Drugs lacking antimicrobial activity against various Clostridia include trimethoprim-sulfamethoxazole, ampicillin, and clindamycin. Notably, clostridia are not resistant to ampicillin-sulbactam, piperacillin-tazobactam, imipenem, metronidazole, and vancomycin. According to the reported cases in the literature, the most used therapy is a combination beta-lactam/metronidazole (Table 2).
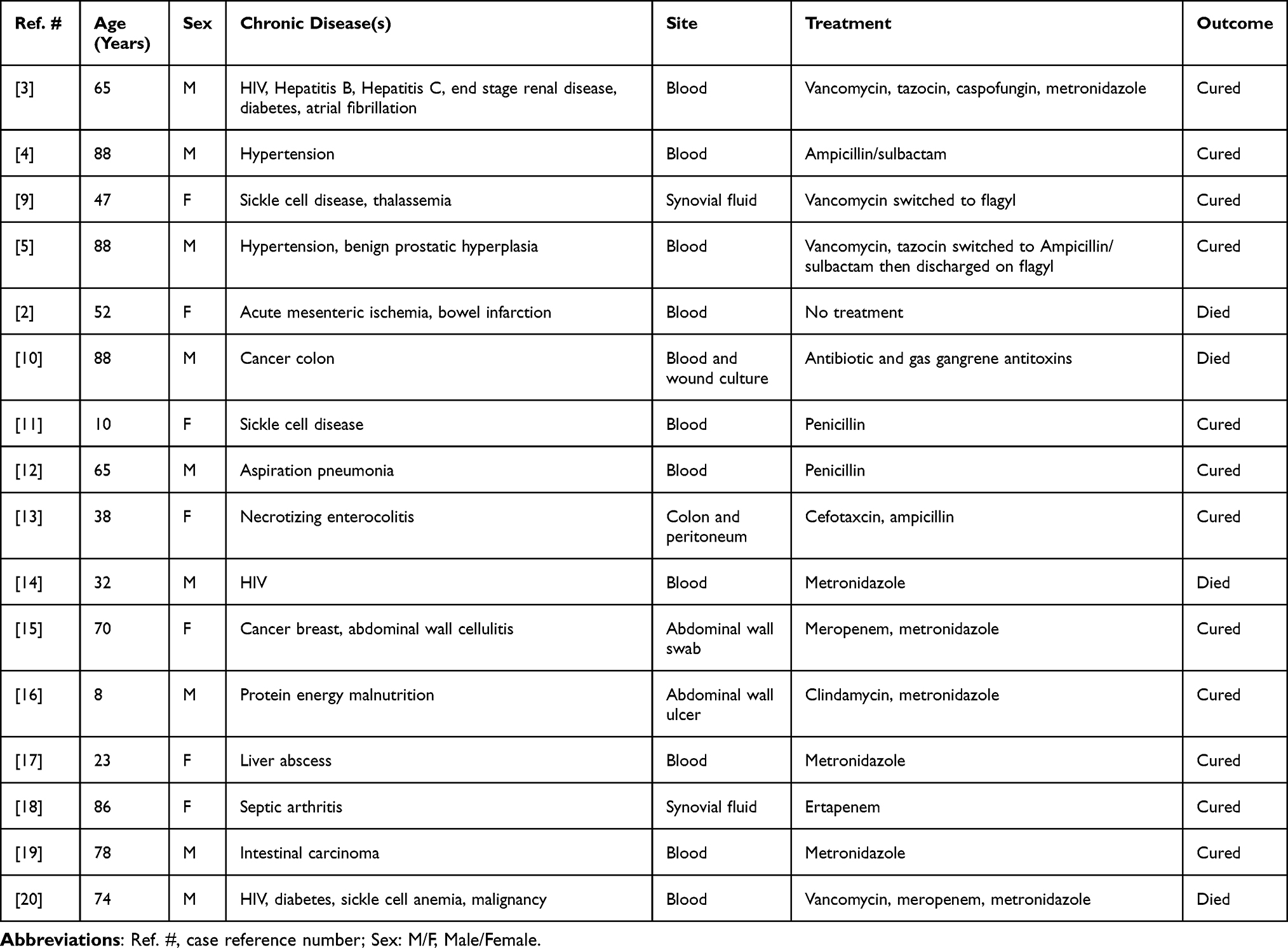 |
Table 2 Summary of the Reported Cases of Clostridium paraputrificum Infections |
Conclusion
Clostridium spp. are one of the most commonly isolated anaerobic pathogens. However, C. paraputrificum is rarely isolated. We presented a case study of a patient with multiple comorbidities and associated predisposing factors, such as hepatitis B, hepatitis C, and HIV with C. paraputrificum bacteremia. Further studies are needed to determine the associated risk factors and pathogenesis of C. paraputrificum.
Ethics Approval and Consent to Participate
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the consent document is available for review upon request from the Editor-in-Chief of this journal.
Consent for Publication
Consent for publication was not required for this case report in accordance with the legislation and the institutional requirement at Imam Abdulrahman Bin Faisal University.
Acknowledgments
The authors would like to thank Ms Bashayer Aldossary (Microbiology Lab, King Fahd Hospital of The University, Al Khobar, Saudi Arabia) for her contribution to our work during sample processing.
Funding
No funding was received from any public, commercial or non-profit organization for this research.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Leal J, Gregson DB, Ross T, Church DL, Laupland KB. Epidemiology of Clostridium species bacteremia in Calgary, Canada, 2000–2006. J Infect. 2008;57:198–203. doi:10.1016/j.jinf.2008.06.018
2. Wiot JF, Felson B. Gas in the portal venous system. Am J Roentgenol Radium Ther Nucl Med. 1961;86:920–929. PMID: 14040292.
3. Shinha T, Hadi C. Clostridium paraputrificum bacteremia Associated with Colonic Necrosis in a patient with AIDS. Case Rep Infect Dis. 2015;2015:312919. doi:10.1155/2015/312919
4. Fukui M, Iwai S, Sakamoto R, Takahashi H, Hayashi T, Kenzaka T. Clostridium paraputrificum bacteremia in an older patient with no predisposing medical condition. Intern Med. 2017;56(24):3395–3397. doi:10.2169/internalmedicine.8164-16
5. Mostel Z, Hernandez A, Tatem L. Clostridium paraputrificum bacteremia in a patient with presumptive complicated appendicitis: a case report. ID Cases. 2021;27:e01361. doi:10.1016/j.idcr.2021.e01361
6. Kuijper EJ, Coignard B, Brazier JS, et al. Update of Clostridium difficile-associated disease due to PCR ribotype 027 in Europe. Euro Surveill. 2007;12(6):E1–2. doi:10.2807/esm.12.06.00714-en
7. Wilson JR, Limaye AP. Risk factors for mortality in patients with anaerobic bacteremia. Eur J Clin Microbiol Infect Dis. 2004;23(4):310–316. doi:10.1007/s10096-004-1111-y
8. Smith LDS, Williams BL. The Pathogenic Anaerobic Bacteria.
9. Ciuro J, Little T, Hiner E, Vakhariya C. Clostridium paraputrificum: an atypical and rare case of septic arthritis mimicking an acute sickle cell crisis. ID Cases. 2020;23:e01031. doi:10.1016/j.idcr.2020.e01031
10. Babenco GO, Joffe N, Tischler AS, Kasdon E. Gas-forming clostridial mycotic aneurysm of the abdominal aorta. A case report. Angiology. 1976;27(10):602–609. doi:10.1177/000331977602701007
11. Brook I, Gluck RS. Clostridium paraputrificum sepsis in sickle cell anemia. South Med J. 1980;73(12):1644–1645. doi:10.1097/00007611-198012000-00033
12. Nachamkin I, DeBlois GE, Dalton HP. Clostridium paraputrificum bacteremia associated with aspiration pneumonia. South Med J. 1982;75(8):1023–1024. doi:10.1097/00007611-198208000-00030
13. Shandera WX, Humphrey RL, Stratton LB. Necrotizing enterocolitis associated with Clostridium paraputrificum septicemia. South Med J. 1988;81(2):283–284. doi:10.1097/00007611-198802000-00037
14. Nerad JL, Pulvirenti JJ. Clostridium paraputrificum bacteremia in a patient with AIDS and Duodenal Kaposi’s sarcoma. Clin Infect Dis. 1996;23(5):1183–1184. doi:10.1093/clinids/23.5.1183
15. Lindenmann J, Fink-Neuboeck N, Leitner E, Grisold A, Kohek P, Smolle-Juettner FM. Clostridium paraputrificum as rare causative of life-threatening spontaneous necrotizing cellulitis of the abdominal wall. J Microbiol Infect. 2016;2:1. doi:10.7243/2052-6180-4-3
16. Ghosh P, Biswas T, Chakraborty B, Saha S, Ghosh P. Clostridium paraputrificum–an extraordinary agent of necrotising subcutaneous ulcers in a child with protein-energy malnutrition. IOSR J Dent Med Sci. 2018;17(1):67–68. doi:10.9790/0853-1701166768
17. Kwon YK, Cheema FA, Maneckshana BT, Rochon C, Sheiner PA. Clostridium paraputrificum septicemia and liver abscess. World J Hepatol. 2018;10(3):388–395. doi:10.4254/wjh.v10.i3.388
18. Vijayvargiya P, Garrigos ZE, Rodino KG, Razonable RR, Abu Saleh OM. Clostridium paraputrificum septic arthritis and osteomyelitis of shoulder: a case report and review of literature. Anaerobe. 2020;62:102105. doi:10.1016/j.anaerobe.2019.102105
19. Intra J, Milano A, Sarto C, Brambilla P. A rare case of Clostridium paraputrificum bacteremia in a 78-year-old Caucasian man diagnosed with an intestinal neoplasm. Anaerobe. 2020;66:102292. doi:10.1016/j.anaerobe.2020.102292
20. Haider A, Alavi F, Siddiqa A, Abbas H, Patel H. Fulminant Pseudomembranous Colitis leading to Clostridium paraputrificum bacteremia. Cureus. 2021;13(3):e13763. doi:10.7759/cureus.13763
21. Jenkins SG, Schuetz AN. Current concepts in laboratory testing to guide antimicrobial therapy. Mayo Clin Proc. 2012;87(3):290–308. doi:10.1016/j.mayocp.2012.01.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.