Back to Journals » Advances in Medical Education and Practice » Volume 13
Clinician-Scientist Faculty Mentoring Program (FAME) – A New Inclusive Training Model at Penn State Increases Scholarly Productivity and Extramural Grant Funding
Authors Dovat S, Gowda C, Mailman RB, Parent LJ ![]() , Huang X
, Huang X
Received 24 March 2022
Accepted for publication 17 August 2022
Published 12 September 2022 Volume 2022:13 Pages 1039—1050
DOI https://doi.org/10.2147/AMEP.S365953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
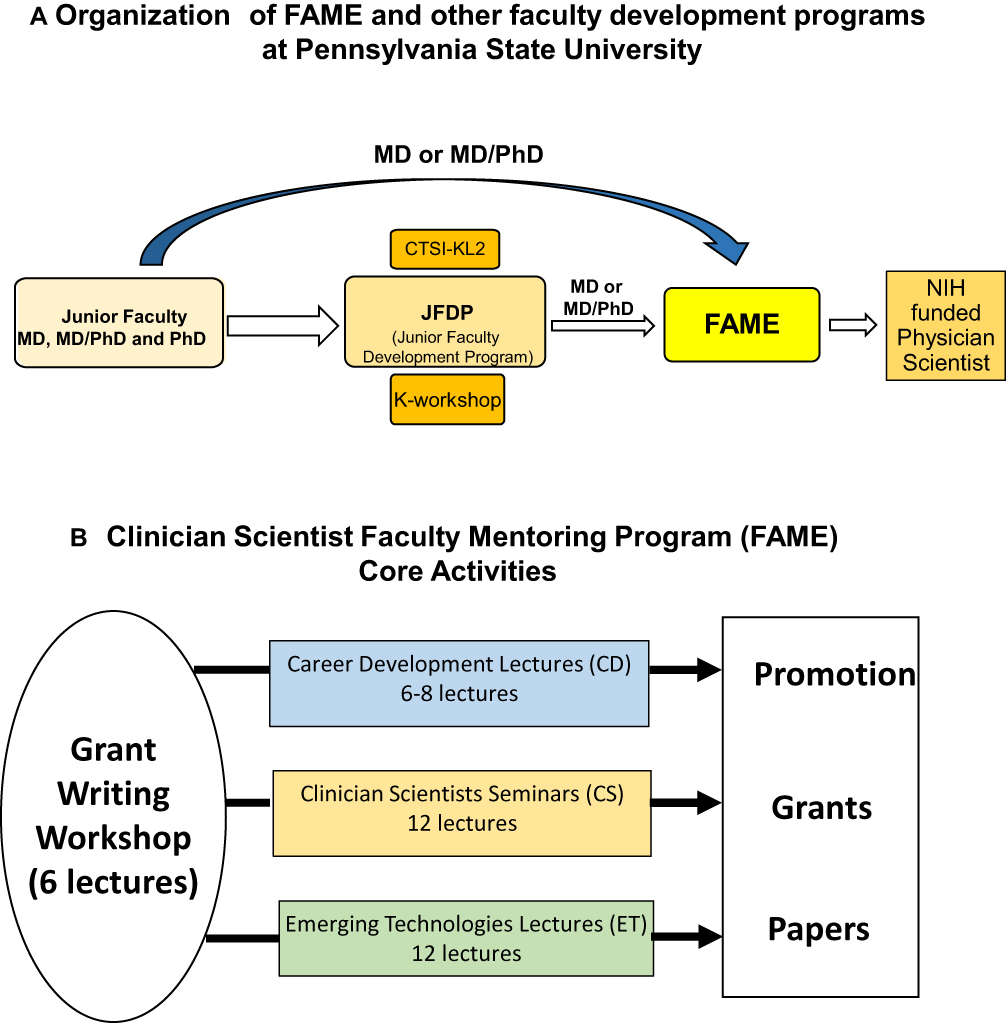
Sinisa Dovat,1 Chandrika Gowda,1 Richard B Mailman,2,3 Leslie J Parent,4 Xuemei Huang2,3 Over the last 30 years, there has been a decline in the number of clinician-scientists in the US, largely due to a high attrition rate.1–5 The major period of loss in the clinician-scientist pool occurs at the junior faculty level, prior to someone achieving an independent position.6–8 At the Penn State College of Medicine, and other institutions, educational programs have been designed for junior faculty and are attended by both basic and clinician-scientists.9–11 These efforts, however, have not reversed the trend of the high attrition rate of clinician-scientists either nationally or at Penn State. In mid-sized colleges of medicine, such as ours, two additional problems that contribute to the high attrition rate of clinician-scientists were identified: small clinician-scientist community due to the overall low number of clinician-scientists12–14 and minimal collaboration between clinician-scientists and clinicians with predominantly clinical duties.12,13,15–21 This lack of collaboration especially limits the ability of clinician-scientists to conduct translational, patient-oriented team science. It also exacerbates a sense of isolation, causing clinician-scientists, to miss opportunities to make advances in medicine, decreasing their scholarly activity and their academic advancement of clinicians.20,22–27 To address this issue, we created a novel educational program entitled the Clinician-Scientist Faculty Mentoring program (FAME). This program was specifically developed for junior faculty clinician-scientists, and we formulated a unique, inclusive approach to provide training and integrate the research of lab-based clinician-scientists with clinical investigators with predominantly clinical duties. For our purposes, we define “junior faculty” as clinicians with an initial full-time academic appointment as instructor or assistant professor and early-stage investigator status (ie, yet to obtain NIH-R01 or R01 equivalent funding award). The design of the program is based on the two hypotheses: 1) during the junior faculty stage, clinician-scientists would benefit professionally from an additional educational program designed specifically to address their unique needs and 2) providing a training program for both “traditional” lab-based clinician-scientists (“clinician-scientists”, as defined by McKinney2) and “non-traditional” clinician-scientists (“clinical researchers”, as defined by McKinney2), will increase the scholarly output of both groups and enhance the sense of community and collaboration. Here, we present the approach and organization of the FAME curriculum, with an emphasis on the novel aspects of the program and an assessment of the early analysis of outcomes as it relates to the original goals. Penn State College of Medicine had developed several scholarly programs to assist in scientific development, including the Junior Faculty Development Program (JFDP), Grants Academy, K-workshop series and the Clinical and Translational Science Institute (CTSI) sponsored KL2 program (Figure 1A). The FAME program was a directed supplement/complement to these and other existing educational, career development, and mentoring resources for clinician-scientists at Penn State College of Medicine (Figure 1A).9 For the purposes of the FAME program, a clinician-scientist is defined as a medical doctor (MD or DO) or other health professional (eg, nurse practitioner, clinical psychologist, etc.), who is working to advance medical knowledge through clinical, translational, or basic research. The program was aimed at being inclusive and involving all health care professionals who have either a substantial portion of their effort allocated for research or have expressed a strong desire to advance their research skills and take part in collaborative research at the Penn State College of Medicine. Defining “protected research time” as the amount of “full time equivalent” (FTE) allocated and supported by institution/employer to a faculty to perform research activities free of clinical, teaching or administrative responsibilities,28 the FAME program requires a minimum of 0.1 FTE “protected research time” during the two-years of the FAME program. The FAME scholars have been selected based on their background in research, personal statement that expressed a strong commitment toward advancing their career in research, and strong support from their respective department chairs. The prior research experience of the selected scholars was diverse: six had a formal research training (ie, MD/PhD degrees or equivalent), whereas the research training of others was limited to that from their clinical fellowships and/or attending the other mentoring programs noted above. Figure 1 Clinician-scientist Faculty Mentoring Program (FAME) – curriculum and role in faculty development programs at Penn State College of Medicine. (A) Faculty development programs at Penn State College of Medicine. (B) Clinician-scientist Faculty Mentoring Program (FAME) Core Curriculum. Abbreviations: CTSI, Clinical and Translational Science Institute; NIH, National Institute of Health. The leadership of the FAME training program consisted of a program director and approximately 20 instructors/mentors who were all clinician-scientists and/or basic scientists with substantial track records of NIH funding and service on NIH study sections. FAME instructors/mentors gave individual lectures and actively participated in interactive sessions that are detailed below. The duration of FAME training was two academic years and consisted of 36 interactive two-hour lectures given biweekly. The lectures alternated with weekly scholarly advancement time (2 hours), which involved self-learning scholarly activities during which FAME scholars reviewed the didactic sessions from the previous week and engaged in additional reading related to the selected topic. The FAME program core curriculum consists of 4 types of seminars and core activities (Figure 1B and Supplemental Table S1–S3):
The Emerging Technology Seminars and Clinician-scientist Mentored Work-in-Progress Research Seminars are novel educational tools incorporated into the FAME program curriculum. These presentations are highly interactive sessions, during which FAME instructors, mentors, and other FAME scholars ask questions and provide advice and suggestions to the presenter regarding his/her project and plans for future grant submission. Mentored Work-in-Progress Research Seminars complement mentoring by a primary mentor with feedback from other mentors in the FAME program. In addition, the FAME scholars learn how to provide constructive feedback to the presenters, with the goal of developing their grant reviewing skills. During the two-year duration of the FAME program, scholars give a total of 12 two-hour work-in progress seminars (total 24 presentations), which allows each FAME scholar to present their data and grant plans at least once (most of them twice) and obtain valuable feedback from FAME instructors, mentors, and other scholars. In addition, FAME scholars participated in our Institutional Mock Review of Grants (MoRe) sessions to receive feedback on their Specific Aims page from senior faculty members with NIH study section experience. Their participation in MoRe was in three different roles: 1) as an observer; 2) as an applicant, but witnessing an NIH style review processed internally (but prior to submission of their application); and 3) as a reviewer, where the FAME scholars serve as one of the secondary or tertiary reviewers of proposals submitted by other junior investigators and FAME scholars (the primary and at least one secondary reviewer are all seasoned investigators). The purpose of the FAME scholars’ participation in MoRe is to demystify the NIH review process and to provide FAME scholars with different perspectives of how to analyze grant proposals, both as an applicant and as a reviewer. The effectiveness of the FAME program was assessed in several ways:
Data regarding scholarly productivity (manuscript submissions, publications, and funded awards) were collected and analyzed using both self-reporting and objective methods. These include:
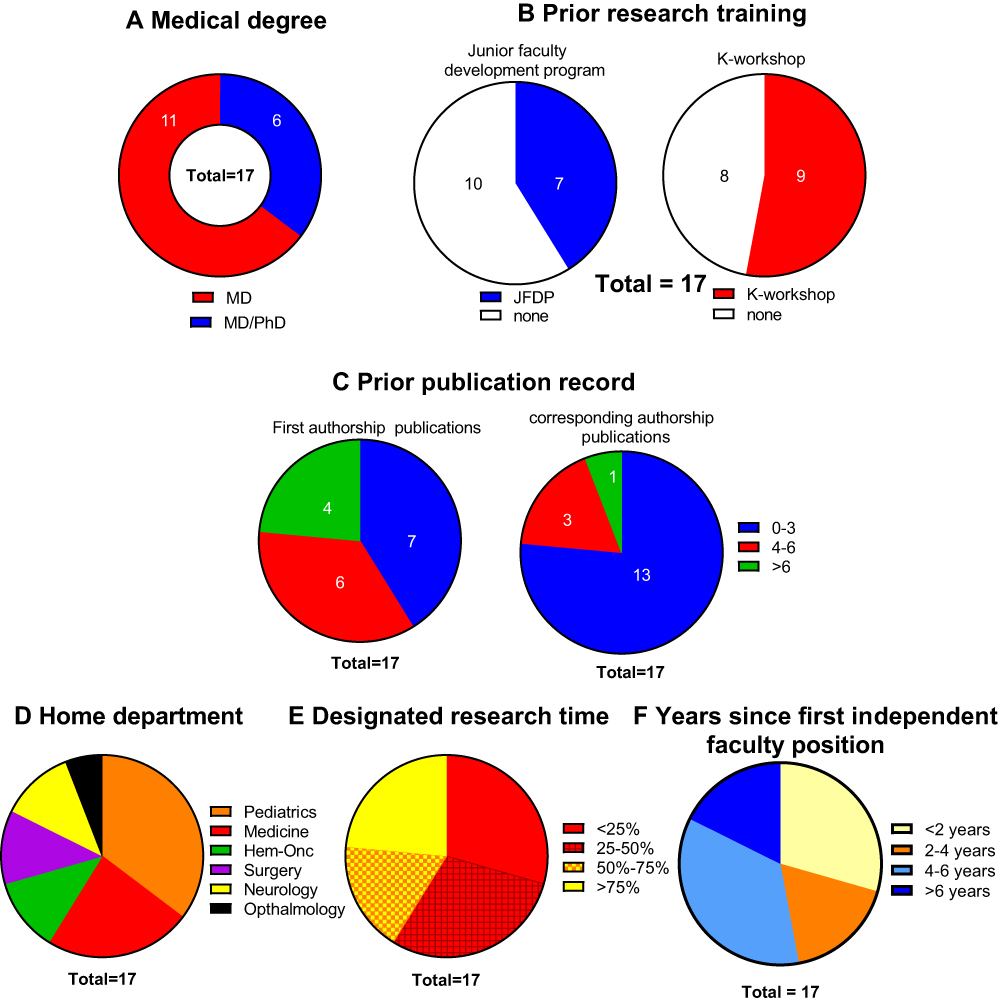
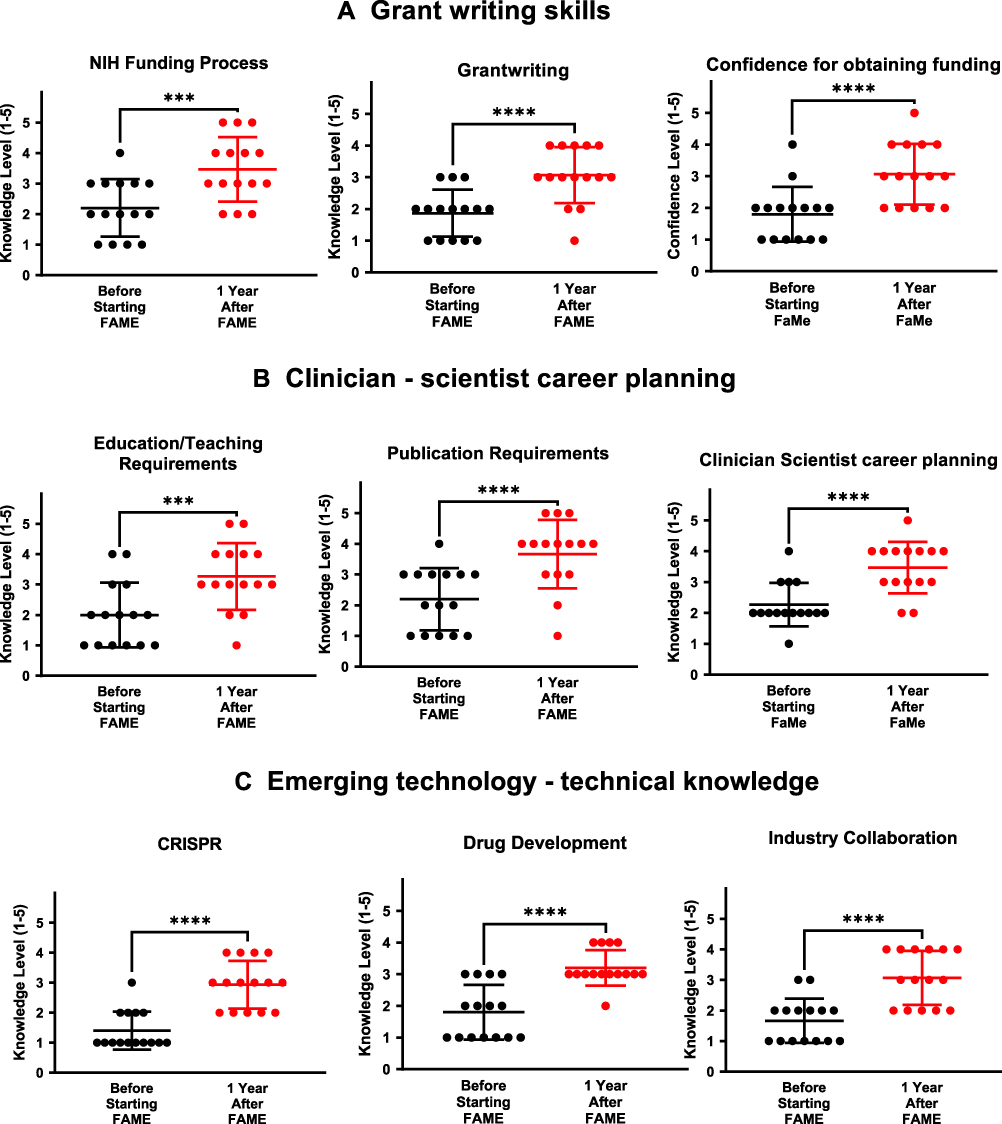
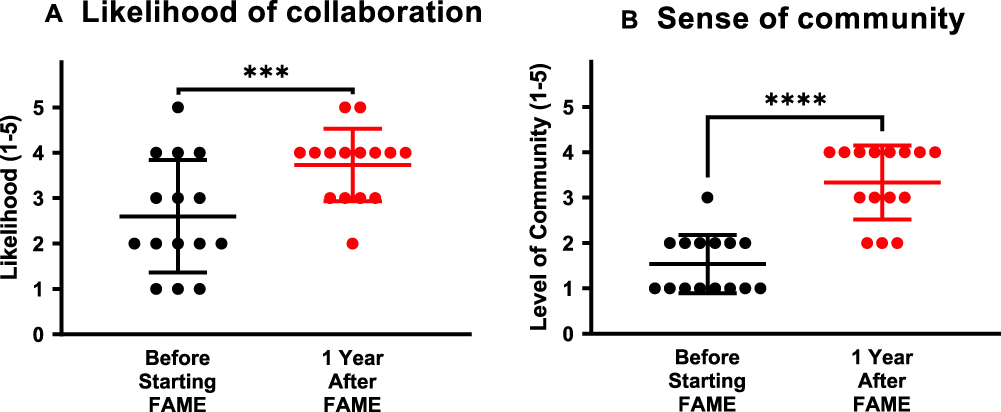
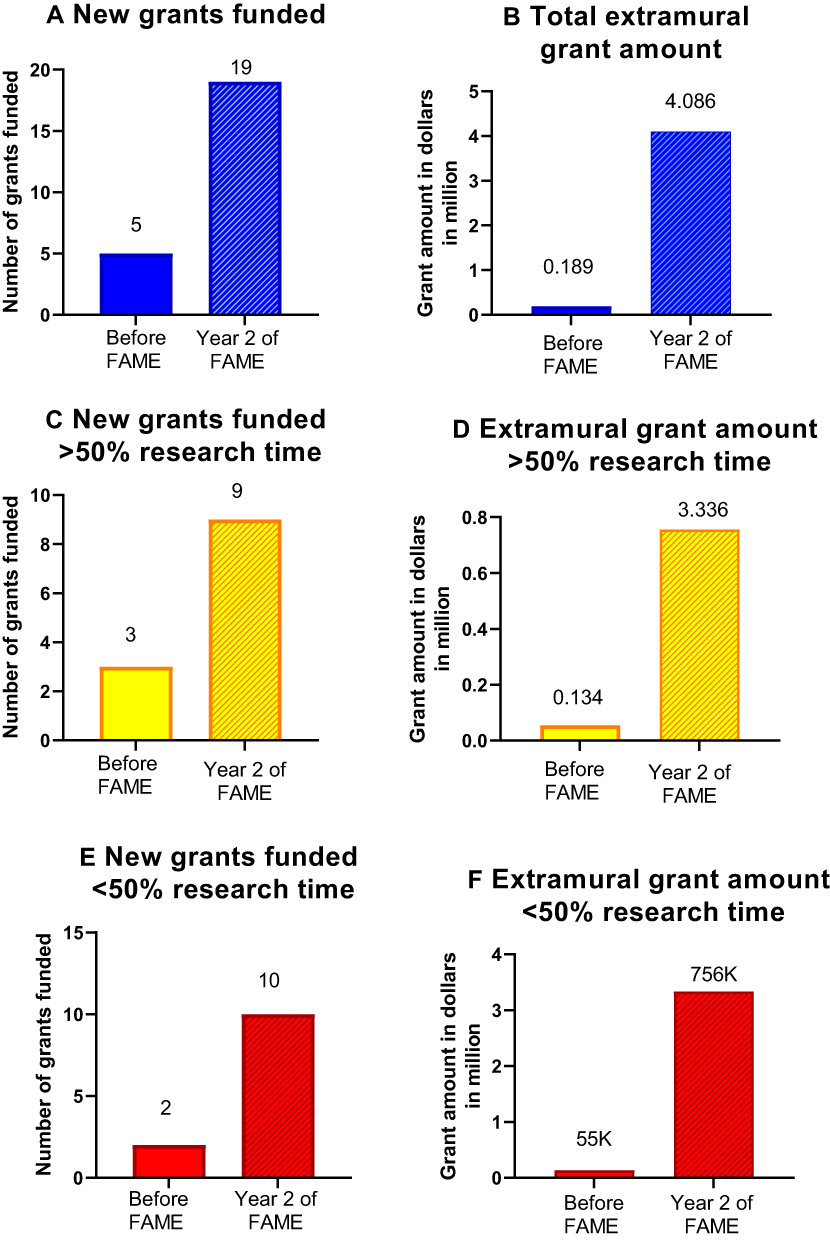
The first FAME cohort enrolled 17 clinician-scientists (scholars) with a diverse formal research training (PhD and/or formal research training at Penn State) and research experience (based on the number of 1st and corresponding authorship papers) (Figure 2A–C), from 6 different departments (Figure 2D). The class was heterogeneous regarding designated protected research time (Figure 2E), as well as research and clinical career stage (Figure 2F). High diversity of the FAME scholars was designed purposefully to fulfill the goals of the program. Figure 2 Diverse background of clinician-scientists enrolled into FAME program. (A) Medical and research background of Clinician-scientists – FAME scholars; (B) completion of formal scholarly and/or research training programs at Penn State College of Medicine before enrollment to the FAME program; (C) number of first and corresponding authorship papers before enrollment to the FAME program; (D) specialty background of FAME scholars; (E) designated research time of FAME scholars; (F) stage of clinical/research career of FAME scholars. The research training of FAME scholars focused on three areas: 1) Improvement of grant writing skills; 2) Development of strategy for a successful career as a clinician-scientist; and 3) acquisition of knowledge of cutting-edge and emerging technologies that could be used in their research projects. We evaluated the efficacy of the research training using a self-assessment survey of FAME scholars focusing on the above three areas (Figure 3A–C). Results showed that FAME scholars showed significant improvements in knowledge of the NIH funding process and grant writing skills, as well as increased confidence in their ability to obtain funding (Figure 3A). The FAME scholars showed a significantly enhanced understanding of the role of publications and educational activities in career advancement and the ability to plan their career as a clinician-scientist (Figure 3B). The efficacy of the seminar that focused on the emerging technologies in clinical research was analyzed by a self-assessment survey of three lectures that focused on basic science (CRISPR-gene editing) and translational (drug development) technologies, as well as their clinical applications (collaboration with industry). The analysis showed that FAME scholars significantly improved their knowledge and applicability of emerging technologies (Figure 3C), as well as their familiarity with resources available at Penn State (Supplemental Figure S1). Figure 3 Results of the outcome self-assessment survey of FAME scholars. Results of outcome self-assessment survey showed a strong improvement in (A) grant writing skills; (B) clinician-scientist career preparation; and (C) emerging technology knowledge.***p<0.001, ****p<0.0001. Overall, before starting FAME, the scholars perceived to have a knowledge deficit in all of the areas covered by research training included in the FAME program curriculum, as evidenced by a low score (<2) of knowledge level. Following a one-year attendance in FAME, the knowledge level of all areas, as well as their confidence in obtaining extramural funding, significantly improved. Important goals of the FAME program were to establish new collaborations between lab-based clinician-scientists and clinical investigators, as well as to establish a sense of community among all types of clinician-scientists. At the self-assessment survey, FAME scholars reported that the likelihood of establishing novel collaborations was highly increased (Figure 4A) and that a sense of community of FAME scholars was strongly enhanced after one year of attending FAME (Figure 4B). It is important to note that the initial sense of community of FAME scholars was at an extremely low level and showed marked improvement after one year of attending the program. Figure 4 The effect of FAME program on sense of community among participating clinician-scientists. Likelihood of collaboration (A) and increased sense of community (B) of FAME scholars following completion of the program.***p<0.001, ****p<0.0001. The results presented in Figures 3 and 4 demonstrate that FAME scholars identified all of the areas covered in the FAME program curriculum as “perceived deficits”, which was defined as a score less than 2 (on scale 1 to 5). Following 12 months attendance of the FAME program, the scholars reported “perceived growth”, which was defined as a positive change in scores from baseline to 12 months of FAME attendance in specific areas. The “perceived growth” was evident both in acquiring research knowledge and in the improvement in the sense of community and collaboration. Following the completion of the 2-year program, a large number of FAME scholars reported high scholarly productivity, as evidenced by an increased number of submitted manuscripts and accepted manuscripts (65.9% increase, Supplemental Figure S2A and 30.9% increase, Supplemental Figure S2B, respectively). These data showed that attending the FAME program was associated with increased productivity of FAME scholars. The total number of newly-funded grants following the completion of the FAME program increased almost 5-fold compared to the year prior to starting the FAME program (5 vs 19; Figure 5A). In the year prior to entering the FAME program, the amount of new extramural funding, was quite low (less than $200,000). However, in the year following the completion of FAME program, scholars were awarded a total of $4,096,000 by NIH or national philanthropic foundations (Figure 5B). Nine FAME scholars were awarded an extramural grant greater than $50,000 in the year following the completion of FAME program, as compared to two in the year prior to starting the program (Supplemental Figure S3). Stratification of FAME scholars by the amount of protected research time showed that the “traditional” clinician-scientists with >50% research time received an increased number of newly funded grants by 3-fold (3 vs 9; Figure 5C), and extramural grant funding by almost 25-fold ($0.134 vs $3.336 million; Figure 5D). The “non-traditional” clinician-scientists, with ≤50% research time increased the number of new funded grants by 5-fold (2 vs 10; Figure 5E), and funding from new extramural grants by over 13-fold ($55,000 compared with $756,000; Figure 5F). Figure 5 The effect of FAME program on ability of FAME scholars to obtain new extramural grant funding. The total number of new grants (A) and total grant amount (B) of all FAME scholars after completion of FAME program vs the year before entering FAME; The number of new grants (C) and funding amount from the new grants (D) of FAME scholars – “traditional” (>50% research time) clinician-scientists after completion of FAME program vs the year before entering FAME; The number of new grants (E) and funding from the new grants (F) of FAME scholars – “non-traditional” clinician-scientists (<50% research time) after completion of FAME program vs the year before entering FAME. The results of our qualitative and quantitative review of the outcome of the FAME program were strongly positive in enhancing the career development of clinician-scientists. Participation in the FAME program had the strongest positive effect on the ability of FAME scholars to obtain new extramural grant funding. This outcome suggests that the predominant impact of the FAME program was on the competence of clinician-scientists to transform results of their research into successful grant submissions. The unique approach of the FAME program is the inclusion of lab-based (“traditional”) clinician-scientists together with clinical investigators, with predominantly clinical duties (“non-traditional” clinician-scientists) in the same program. The significant increase of new extramural grant funding, along with an increase of scholarly activity by both groups of clinician-scientists, appears to validate the structure of the program. New extramural funding was markedly increased among both “traditional” (>20-fold) and “non-traditional” (>25-fold) clinician-scientists. Clinician-researchers with predominantly clinical duties often struggle to find the time for scholarly activity, resulting in difficulty in achieving academic promotion as well as a sense of isolation from the rest of the academic community.2,3,20,26,27 All of these factors can contribute to physician burnout, one of the main problems in academic medicine today.30 There are several limitations to our study. First, this study involves only a single institution. Although we believe it has broader applicability, this will have to be tested by implementing elsewhere. This also provides a unique opportunity if different institutions exchange their ideas and findings that can help make this approach more mature and effective. Second, because this was only one site and only one class of scholars, the number of scholars included (17) is limited. When data from our second and subsequent FAME cohorts are available, the findings will be more reliable. Indeed, if our data can be combined with that of other institutions, the true value of the approach will be much clearer. Another important issue is whether the significant short-term benefits we have found will translate into long-term effects on the academic careers of the FAME scholars; this is the most critical outcome parameter. A related issue is that while one strength of the FAME program to date has been the high diversity of the scholars, this can also be a confound. Evaluation of scholarly performance of the FAME scholars in subsequent classes will help to identify additional opportunities to tailor the curriculum toward specific needs of the specific groups. These are some of the future directions we plan to use to validate our findings and use them to improve the program. If this can be a collaborative effort with other sites, the benefit to the field as a whole may be markedly magnified. The analysis of the outcome measures of the FAME program suggests that implementing additional training tailored to clinician-scientists leads to increased scholarly activity regardless of the scholar’s previous experience in research. The newly-developed educational tools used in FAME appear to be useful in the training of clinician-scientists. The second FAME cohort has been enrolled (18 clinician-scientists), and they also will use this curriculum as a foundation for their career development program. We recognize the importance of ascertaining whether the substantial effect seen in the first cohort also occurs in this second, as well as subsequent years. It is also important to determine whether the effects of completing FAME training are durable and keep these faculty members engaged in research careers over the long term. Our plan is to perform an annual follow-up to evaluate their scholarly maturation and extramural funding. Our results suggest that clinician-scientists with predominantly clinical duties and limited research-protected time (“non-traditional” clinician-scientists) have strong, unrecognized potential that can be fulfilled with optimal extra training. The amount of funding in new grants obtained by “non-traditional” clinician-scientists was significantly lower than that of “traditional” clinician-scientists. This is because the majority of grants of the former are smaller in size, nonetheless they could represent a bridge toward large grants. We have several new ideas for the creation of additional training programs for “non-traditional clinician-scientists” to help them secure larger extramural grants. We propose that the structure and organization of the FAME program would have the most impact on the scholarly activity in small-to-medium sized institutions, such as Penn State College of Medicine, where the relatively small cadre of clinician-scientists is more pronounced than in larger institutions. However, we further postulate that in larger academic centers, the FAME program could be tailored to individual specialties (eg oncologists, cardiologists, etc.) to have a more focused impact in each area. We also would hope to see a program such as FAME implemented nationally via national professional organizations (American Association for Cancer Research (AACR), American Thoracic Society (ATS) etc.). Our results suggest that a training and mentoring tailored to clinician-scientists leads to increased scholarly activity regardless of research background. The newly developed educational tools were well received, and the results suggested they enhance the productivity of early-stage clinician scientists. The data also suggest that clinician scientists with limited research-protected time have unrecognized potential that can be elicited by an environment that is supportive and provides optimal training. Both the lack of a sense of community and the low collaboration between lab-based clinician-scientists and clinician-scientists with predominantly clinical duties can be addressed by an inclusive program that targets both populations. Preliminary outcome data supports the use of this model of clinician-scientist junior faculty training program in small-to-medium sized academic health institutions, and it may well have a broader impact for other academic environments. This study was exempt from the Penn State College of Medicine Institutional Review Board (PSCOM IRB) review since no identifiable results were presented. This work is supported by funding from Penn State University College of Medicine. The authors report no conflicts of interest in this work. 1. Jain MK, Cheung VG, Utz PJ, Kobilka BK, Yamada T, Lefkowitz R. Saving the endangered physician-scientist - a plan for accelerating medical breakthroughs. N Engl J Med. 2019;381(5):399–402. doi:10.1056/NEJMp1904482 2. McKinney RE 3. Wyngaarden JB. The clinical investigator as an endangered species. N Engl J Med. 1979;301(23):1254–1259. doi:10.1056/NEJM197912063012303 4. Andriole DA, Wolfson RK. The physician-investigator workforce: looking ahead. Acad Med. 2021;96:486–489. doi:10.1097/ACM.0000000000003944 5. Hall AK, Mills SL, Lund PK. Clinician-investigator training and the need to pilot new approaches to recruiting and retaining this workforce. Acad Med. 2017;92(10):1382–1389. doi:10.1097/ACM.0000000000001859 6. Daye D, Patel CB, Ahn J, Nguyen FT. Challenges and opportunities for reinvigorating the physician-scientist pipeline. J Clin Invest. 2015;125(3):883–887. doi:10.1172/JCI80933 7. Murillo H, Reece EA, Snyderman R, Sung NS. Meeting the challenges facing clinical research: solutions proposed by leaders of medical specialty and clinical research societies. Acad Med. 2006;81(2):107–112. doi:10.1097/00001888-200602000-00002 8. Furuya H, Brenner D, Rosser CJ. On the brink of extinction: the future of translational physician-scientists in the United States. J Transl Med. 2017;15(1):88. doi:10.1186/s12967-017-1188-6 9. Huang X, Dovat S, Mailman R, Thiboutot D, Berini D, Parent LJ. Building a system to engage and sustain research careers for physicians. Acad Med. 2020;96:490–494. 10. Flores G, Mendoza F, Brimacombe MB, Frazier W 11. Brownson RC, Jacob RR, Carothers BJ, et al. Building the next generation of researchers: mentored training in dissemination and implementation science. Acad Med. 2021;96(1):86–92. doi:10.1097/ACM.0000000000003750 12. Somekh I, Somekh E, Pettoello-Mantovani M, Somech R. The clinician scientist, a distinct and disappearing entity. J Pediatr. 2019;212:252–253 e252. doi:10.1016/j.jpeds.2019.06.063 13. Weggemans MM, Friesen F, Kluijtmans M, et al. Critical gaps in understanding the clinician-scientist workforce: results of an international expert meeting. Acad Med. 2019;94(10):1448–1454. doi:10.1097/ACM.0000000000002802 14. Neul JL. Interested in a career as a clinician-scientist? Dis Model Mech. 2010;3(3–4):125–130. doi:10.1242/dmm.005462 15. Bensken WP, Nath A, Heiss JD, Khan OI. Future directions of training physician-scientists: reimagining and remeasuring the workforce. Acad Med. 2019;94(5):659–663. doi:10.1097/ACM.0000000000002581 16. Schafer AI. The vanishing physician-scientist? Transl Res. 2010;155(1):1–2. doi:10.1016/j.trsl.2009.09.006 17. Blevins D, Farmer MS, Edlund C, Sullivan G, Kirchner JE. Collaborative research between clinicians and researchers: a multiple case study of implementation. Implement Sci. 2010;5:76. doi:10.1186/1748-5908-5-76 18. Schwartz DA. Physician-scientists: the bridge between medicine and science. Am J Respir Crit Care Med. 2012;185(6):595–596. doi:10.1164/rccm.201110-1806ED 19. Restifo LL, Phelan GR. The cultural divide: exploring communication barriers between scientists and clinicians. Dis Model Mech. 2011;4(4):423–426. doi:10.1242/dmm.008177 20. Warner ET, Carapinha R, Weber GM, Hill EV, Reede JY. Faculty promotion and attrition: the importance of coauthor network reach at an academic medical center. J Gen Intern Med. 2016;31(1):60–67. doi:10.1007/s11606-015-3463-7 21. Berger A, Matloubian M, Shah NP, Wachter RM, DeRisi JL, Anderson M. The molecular medicine investigation unit: linking patient care and scientific inquiry in physician-scientist training. J Grad Med Educ. 2020;12(1):92–97. doi:10.4300/JGME-D-19-00507.1 22. Jagsi R, Griffith KA, Jones RD, Stewart A, Ubel PA. Factors associated with success of clinician-researchers receiving career development awards from the national institutes of health: a longitudinal cohort study. Acad Med. 2017;92(10):1429–1439. doi:10.1097/ACM.0000000000001728 23. Little MM, St Hill CA, Ware KB, et al. Team science as interprofessional collaborative research practice: a systematic review of the science of team science literature. J Investig Med. 2017;65(1):15–22. doi:10.1136/jim-2016-000216 24. Steer CJ, Jackson PR, Hornbeak H, McKay CK, Sriramarao P, Murtaugh MP. Team science and the physician-scientist in the age of grand health challenges. Ann N Y Acad Sci. 2017;1404(1):3–16. doi:10.1111/nyas.13498 25. Roberts SF, Fischhoff MA, Sakowski SA, Feldman EL. Perspective: transforming science into medicine: how clinician-scientists can build bridges across research’s “valley of death”. Acad Med. 2012;87(3):266–270. doi:10.1097/ACM.0b013e3182446fa3 26. Chaiyachati KH, Liao JM, Weissman GE, Morgan AU, Shea JA, Armstrong KA. The association between mentor-mentee network features and publication productivity among early career academic generalists. J Gen Intern Med. 2019;34(3):346–348. doi:10.1007/s11606-018-4702-5 27. Braxton MM, Infante Linares JL, Tumin D, Campbell KM. Scholarly productivity of faculty in primary care roles related to tenure versus non-tenure tracks. BMC Med Educ. 2020;20(1):174. doi:10.1186/s12909-020-02085-6 28. Barnard JA. Protected time: a vital ingredient for research career development. J Pediatr Gastroenterol Nutr. 2015;60(3):292–293. doi:10.1097/MPG.0000000000000693 29. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010 30. Perumalswami CR, Griffith KA, Jones RD, Stewart A, Ubel PA, Jagsi R. Patterns of work-related burnout in physician-scientists receiving career development awards from the national institutes of health. JAMA Intern Med. 2019;180:150–153.
1Department of Pediatrics, Penn State Milton S. Hershey Medical Center and College of Medicine, Hershey, PA, USA; 2Department of Pharmacology, Penn State Milton S. Hershey Medical Center and College of Medicine, Hershey, PA, USA; 3Department of Neurology, Penn State Milton S. Hershey Medical Center and College of Medicine, Hershey, PA, USA; 4Department of Medicine and Microbiology and Immunology, Penn State Milton S. Hershey Medical Center and College of Medicine, Hershey, PA, USA
Correspondence: Sinisa Dovat, Tel +1 7175316012, Fax +1 7175314789, Email [email protected]
Purpose: Clinician-scientists have a high attrition rate at the junior-faculty level, before they gain independent funding. We identified the lack of skill set, clinician-scientist community and collaboration between clinician-scientists and clinicians with predominantly clinical duties, as key problems in our medium-size college of medicine.
Methods: We designed a novel two-year educational program, the Clinician-scientist Faculty Mentoring program (FAME) specifically to target junior clinician-scientists. The program enrollment included both lab-based, “traditional” and “non-traditional” clinician-scientists, with predominantly clinical duties and limited time for research. The curriculum included the novel educational tools: Emerging technology seminars and mentored work-in-progress research seminars, integrated with mock grant review.
Results: The first class enrolled 17 clinician-scientists with diverse clinical subspecialty, previous research training, and protected research time. After two years in the program, the self-assessment of FAME scholars demonstrated strong improvement in grantsmanship skills, career development, emerging technologies, and the sense of community and collaboration. Compared to the period before initiating FAME, scholars increased annual scholarly output by 65% and new extramural funding by > 20-fold (Introduction
Specific Goals and Objectives of FAME Program
Organization and Content of FAME Program
Curriculum
Methods
Program Assessments
Results
Diverse Background of FAME Program Participants
FAME Scholars’ Self-Assessment Survey of Competency
FAME Scholars’ Outcome Self-Assessment Survey of the Sense of Community and Collaboration
Objective Assessment of Scholars’ Career Advancement, Scholarship Publication and New Extramural Grant Funding
Discussion
Limitation of the Study and Confounding Factors
Validation of the FAME Program in Subsequent Classes
Long-Term Follow-Up of Former Trainees
Design of Additional Training Programs for “Non-Traditional” Clinician-Scientists
Expand the FAME Program Nationally
Conclusion
Ethical Approval
Acknowledgment
Disclosure
References
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.