")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Clinician Perceptions of the Negative Impact of Telehealth Services in the Management of Drug-Induced Movement Disorders and Opportunities for Quality Improvement: A 2021 Internet-Based Survey
Authors Bera R, Bron M , Benning B , Cicero S, Calara H, Darling D, Franey E, Martello K, Yonan C
Received 18 August 2022
Accepted for publication 10 December 2022
Published 19 December 2022 Volume 2022:18 Pages 2945—2955
DOI https://doi.org/10.2147/NDT.S385960
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Rimal Bera,1 Morgan Bron,2 Betsy Benning,3 Samantha Cicero,4 Heintje Calara,2 Diane Darling,2 Ericha Franey,2 Kendra Martello,5 Charles Yonan2
1Irvine Medical Center, University of California, Orange, CA, USA; 2Health Economics and Outcomes Research, Neurocrine Biosciences, Inc., San Diego, CA, USA; 3Emerging Biopharma, IQVIA Inc., Danbury, CT, USA; 4Field Medical Affairs, Neurocrine Biosciences, Inc., San Diego, CA, USA; 5Public Policy, Neurocrine Biosciences, Inc., San Diego, CA, USA
Correspondence: Rimal Bera, Irvine Medical Center, University of California, 101 City Drive, Orange, CA, 92618, USA, Tel +1-714-456-6898, Fax +1-714-456-5112, Email [email protected]
Purpose: Tardive dyskinesia (TD) is a drug-induced movement disorder (DIMD) seen in patients taking dopamine-receptor blocking agents (DRBAs). Clinicians should regularly monitor patients with or at risk of developing DIMDs; however, telehealth visits during the COVID-19 pandemic presented several significant challenges related to screening and care of these patients. In this observational survey study, respondents compared in-person with video/telephone visits to determine the impact on the evaluation, diagnosis, and monitoring of patients with DIMDs.
Methods: The online survey was conducted (May 14–June 21, 2021) with qualified clinicians who prescribed a vesicular monoamine transporter 2 inhibitor or benztropine for DIMDs in the past 6 months, spent ≤ 70% of their professional time in the clinic, and conducted telehealth visits with ≥ 15% of their patients between December 2020 and January 2021. The questionnaire probed clinicians about their ability to evaluate, diagnose and monitor (hereinafter referred to as manage) patients with DIMDs via telehealth.
Results: Survey respondents included 277 clinicians from psychiatry (n = 168) and neurology (n = 109) practices. Certain signs and symptoms (visual cues) used for diagnosis of DIMDs were not observable through telehealth and evaluation was comparatively more difficult with phone visits than video visits. Patients without caregivers and lower-functioning patients were at higher risk of missed diagnosis of DIMDs and were also difficult to monitor via telehealth. Limited access to computers or telephones and patients living alone were among the top socioeconomic barriers limiting clinicians’ ability to diagnose DIMDs. Patients without a regular caregiver were also more difficult for clinicians to evaluate and monitor adequately. Further, most clinicians received no training related to evaluation of DIMDs via telehealth or engaging caregivers as health care partners.
Conclusion: Our study highlights specific limitations and challenges and provides considerations to help clinicians better manage DIMDs in the context of telehealth services.
Keywords: telemental health, telemedicine, psychiatry, caregiver, neurology, training
Introduction
Drug-induced movement disorders (DIMDs) are often underrecognized, underreported, and inadequately managed.1,2 Tardive dyskinesia (TD) is a DIMD commonly associated with dopamine-receptor blocking agents (DRBAs; antipsychotics) that are prescribed to treat psychiatric conditions such as schizophrenia, major depressive disorder, and bipolar disorder. TD is characterized by involuntary, abnormal, and repetitive movements of the face, torso, and other body parts, which can persist even after discontinuing the causative drug.3–5 As many as 30% of patients taking first-generation antipsychotics develop TD, and many patients experience impairment in their physical, functional, and social activities, face social stigma, and suffer embarrassment as a consequence of TD symptoms.6 Furthermore, as the indications for the use of DRBAs (indicated and off-label) have expanded to include depressive disorders,7,8 it is expected that TD prevalence will also increase, and it is therefore important to evaluate and diagnose patients with TD regularly to initiate timely treatment. It is recommended that a brief clinical assessment of patients taking antipsychotics be carried out routinely.9
The COVID-19 pandemic led to global disruptions in health care services and telehealth services were widely adopted in provider practices and across specialties in the US and around the world10,11 In the US, waivers granted flexibilities to allow expanded use of telehealth, including removing barriers that limited the use of telehealth services to only specific patients and circumstances.12,13 This led to a rapid shift from in-person visits to virtual visits despite disparities in access to health care.14 In psychiatry and neurology, clinicians executed patient visits via videoconference platforms and/or telephone calls in lieu of face-to-face consultations. However, when using these platforms, they found challenges with remotely assessing motor functions and monitoring the patient’s ability to perform normal daily activities.15 Challenges due to telehealth may have impacted physicians differentially based on their clinical set up and individual perceptions.16
Telehealth visits via videoconferencing can help providers assess, diagnose, and treat patients with hyperkinetic movement disorders in remote, underserviced areas.17 Even prior to the pandemic, the American Psychiatric Association (APA) and American Telemedicine Association (ATA) developed guidelines for safe and effective delivery of telehealth services.18 Recommendations were made to develop practice-level protocols and procedures for regular DIMD evaluation of all patients taking antipsychotic medication.17 Further, guidance for implementing videoconferencing protocols to examine DIMDs in an asynchronous mode or to deploy software to monitor changes in facial expression over time were developed.19 After the Abnormal Involuntary Movement Scale (AIMS) was validated for telehealth services, it became possible to monitor DIMDs and remotely measure the severity of abnormal movements in TD.20
Although in-person visits are preferred, telehealth is often perceived as a way to increase patient access to care, reduce appointment no-shows, and cut patient travel and wait times.21–23 However, the impact of telehealth on overall health care utilization and quality outcomes needs to be established.24 Further, privacy concerns, issues surrounding reimbursement, legal and regulatory issues, limited access to audio-video technologies, and lack of training were identified as key limitations for telehealth services.10,21,25 Despite improving access to a wide range of routine and specialized medical services,26 the effectiveness of telehealth and increased access to care provided by the availability of telehealth for patients with DIMDs still remains to be established. More insights are needed into the telehealth methods clinicians use in the outpatient setting to evaluate, diagnose and monitor DIMDs, specifically TD. To further understand important barriers and hurdles from the provider’s perspective, the present physician perception observational study, Real-World Tele-Health Evaluation of Tardive Dyskinesia Symptoms Communication/Observation Procedure Evaluation in Outpatient Clinical Settings (TeleSCOPE) study, compared telehealth visits with in-person visits to determine their impact on the detection and management of DIMDs. This study may enable clinicians to better evaluate and manage patients with DIMDs using telehealth services.
Objective
The objective of this study was to create an inventory of methods clinicians use (in telehealth visits) to assess possible DIMDs, such as TD, as well as to understand clinicians’ ability or barriers to monitor and detect the movements over phone calls or videoconferences compared to in-person visits.
Materials and Methods
Study Design
This was an internet-based, double-blind, quantitative, physician perception-based observational survey. The survey instrument was jointly developed by IQVIA and Neurocrine Biosciences, Inc., and was administered by IQVIA. Clinicians in the United States were asked to provide insights on the use of telehealth to evaluate, diagnose and monitor (hereinafter referred to as manage) TD. The WCG Institutional Review Board (formerly, Western IRB) granted approval for IQVIA to conduct this study.
Data from all variables of interest collected from respondents were characterized with descriptive statistics. This includes proportions for categorical variables (n, %) and the mean, median, standard deviation, minimum, and maximum number for continuous variables, collectively providing an interpretation of the distributional characteristics of the data. Group differences between psychiatry and neurology practices were analyzed via t-test and z-tests. Statistical significance was set at p < 0.05.
Study Population
Target respondents were clinicians (physicians [psychiatrists and neurologists], nurse practitioners [NPs], or physician assistants [PAs]) who worked in psychiatry or neurology practices with prescribing authorization in the US, per state regulations. Participants in the survey included clinicians who prescribed a vesicular monoamine transporter 2 inhibitor and/or benztropine for DIMDs at least once in the past 6 months, clinicians with 3 to 30 years of practice, those who spent at least 70% of their professional time in the clinic, clinicians with more than 80% adult patients in practice, and clinicians who conducted telehealth visits with ≥15% of their patients between December 2020 and January 2021.
Survey Method
The online survey was conducted (May 14, 2021–June 21, 2021) with qualified clinicians and consisted of a questionnaire comprised of 35 items that took approximately 20 minutes to complete. The data collected were validated and analyzed for significant differences at 95% confidence interval (CI) between clinicians in psychiatry and neurology settings.
Results
Respondents to this physician perception-based survey included 277 clinicians (psychiatry: n = 168 [100 physicians, 68 NP/PAs]; neurology: n =109 [101 physicians, 8 NP/PAs]) (Table 1). On average, psychiatry clinicians spent 31% of their time in community mental health clinics.
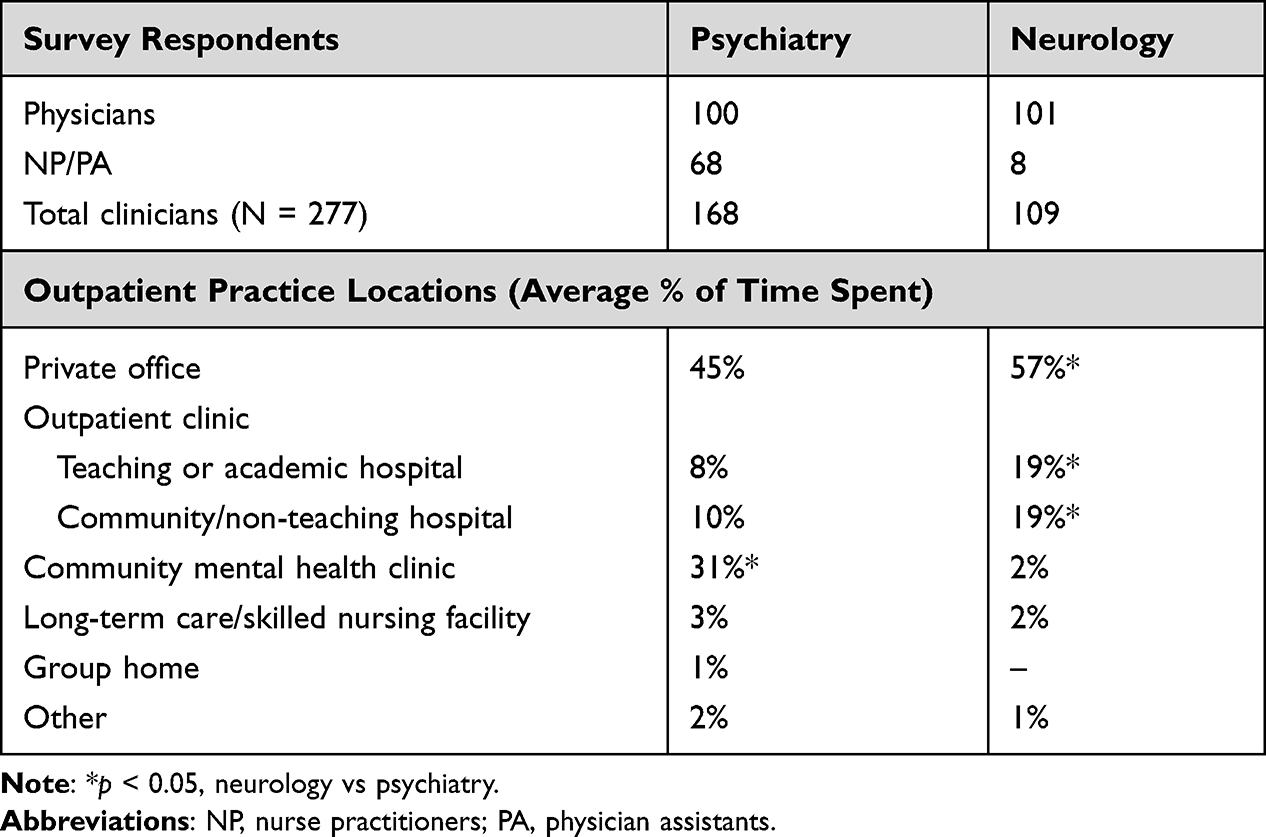 |
Table 1 Characteristics of Respondents |
Impact of Telehealth Visits on DIMD Patient Evaluation and Diagnosis
The COVID-19 pandemic led to a rapid shift from in-person visits to telehealth visits (Supplementary Data 1). However, telehealth led to fewer patients being evaluated and diagnosed for DIMDs. Neurology clinicians reported that 30% of patients treated with DRBAs were evaluated for DIMDs via video visits, and only 9% were evaluated via phone visits, whereas 72% of patients who were seen in person were evaluated (Figure 1). On the other hand, psychiatry clinicians seemed more comfortable than neurologists evaluating patients via telehealth. On average, 55% of their patients were evaluated for DIMDs via video visits, whereas only 24% of patients were evaluated via phone visits, and 56% were evaluated in person.
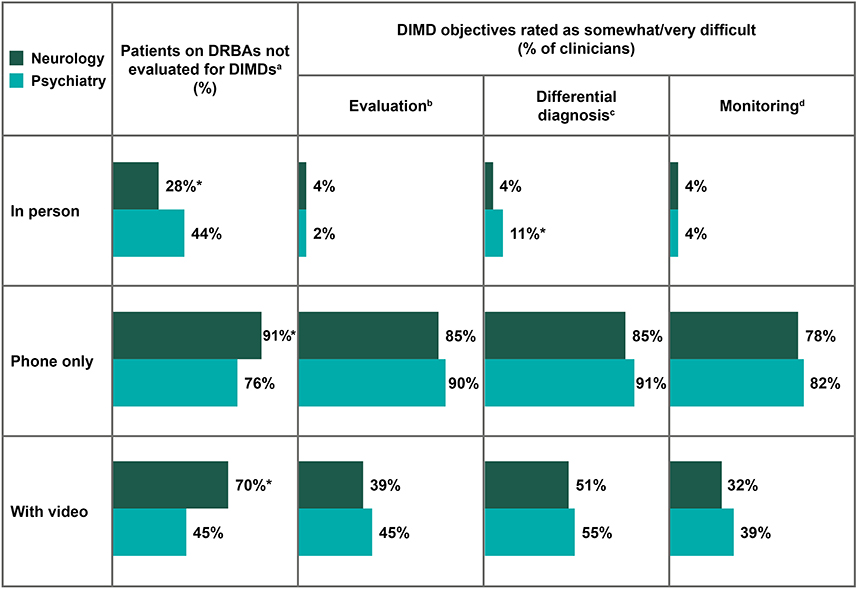 |
Figure 1 Difficulties in evaluating, diagnosing, and monitoring DIMDs via telehealth. Survey questions: aThinking about your patients on dopamine-receptor-blocking agents, what percentage do you evaluate (examine/test/interview) for drug-induced movement disorder (DIMD) in each treatment setting? bPlease rate the difficulty in evaluating patients on dopamine-receptor-blocking agents for DIMD in each setting, where 1 is “very easy” and 5 is “very difficult.” cPlease rate the difficulty of differential diagnosis of various DIMDs such as parkinsonism vs dystonia vs tardive dyskinesia in each setting using the scale below, where 1 is “very easy” and 5 is “very difficult.” dOn a scale of 1 to 5, please rate the difficulty in monitoring patients for DIMD (these are patients who are past the phase of treatment initiation and now considered to be stable) in each of the following treatment settings, where 1 is “very easy” and 5 is “very difficult.”. Abbreviations: DIMD, drug-induced movement disorders; DRBA, dopamine-receptor blocking agent. Note: *p < 0.05, neurology vs psychiatry. |
Managing patients with DIMDs is more difficult via phone visits compared to video visits. Clinicians were asked to assess the difficulty in evaluating, diagnosing, and monitoring patients with DIMDs via each type of interaction. Whereas 32–55% of clinicians found it difficult to manage patients with DIMDs via video visits, >75% of clinicians found it difficult to manage patients via phone visits (Figure 1).
Telehealth Challenges and Barriers for Evaluation, Diagnosis, and Monitoring of DIMDs
Clinicians reported difficulties in observing signs and symptoms via telehealth that would lead to DIMD evaluation. Signs and symptoms that lead clinicians from both specialties to further evaluate patients with DIMDs for TD most commonly include mention of symptoms (tics/movements) by family members (86% of clinicians); trouble with gait, falls, walking, or standing (82%); difficulty swallowing or eating (74%); difficulty writing, using the phone, or computer (71%); and difficulty speaking (70%) (Figure 2). Among the clinicians who report relying on observations of “trouble with gait, falls, walking, or standing”, more than half (55%) were unable to observe this sign via a phone call. Findings were somewhat better for patients seen via video visits; however, 28% of clinicians still reported challenges observing trouble with gait. Similar findings were observed for clinicians who rely on tics/movements mentioned by family members: 26% and 19% of clinicians reported it could not be evaluated over a phone visit or video visit, respectively (Figure 2).
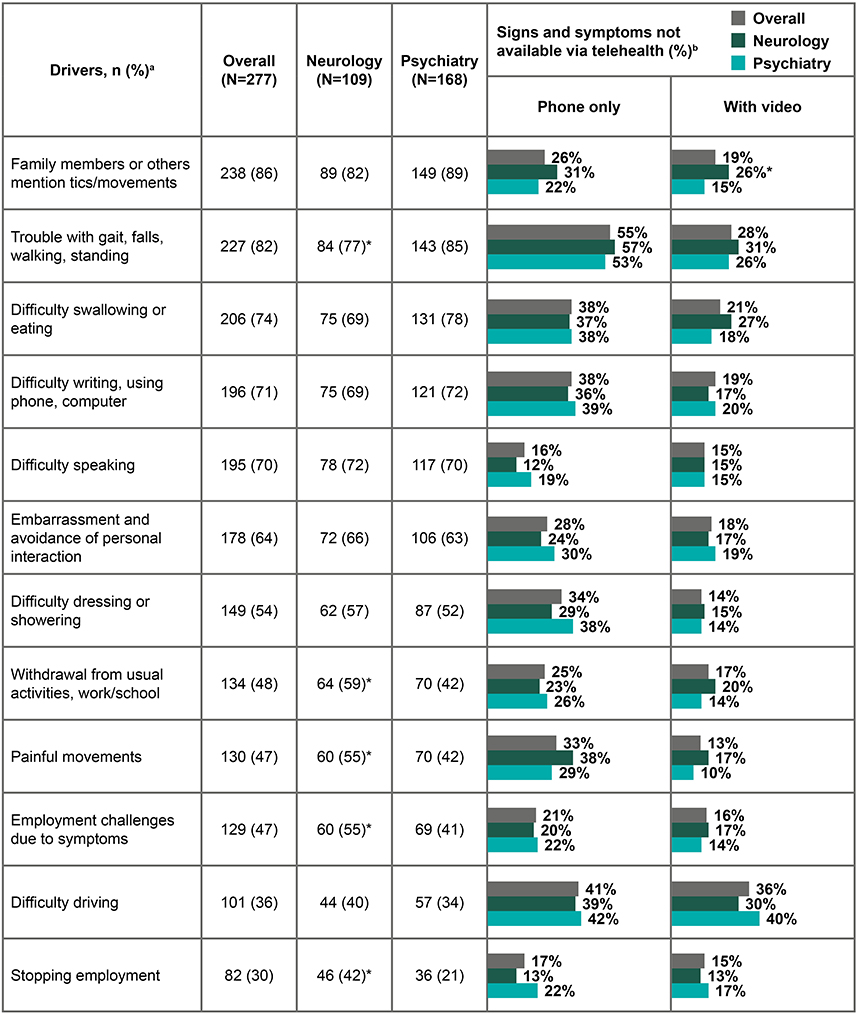 |
Figure 2 Difficulties in evaluating signs and symptoms of DIMDs via telehealth. Survey questions: aWhat observed patient signs and symptoms drive you to evaluate (examine/test/interview) patients with DIMD for possible tardive dyskinesia when you see patients in person? bAmong the patient signs and symptoms that drive you to evaluate (examine/test/interview) patients with DIMD for possible tardive dyskinesia in person, which of these are not available when you are evaluating the patient via telehealth (phone call or video conference)? Abbreviation: DIMD, drug-induced movement disorders. Note: *p < 0.05, neurology vs psychiatry. |
The study asked clinicians to assess patient types who are at the highest risk of missed diagnosis when seen via telehealth. Most clinicians in both specialties agreed that patients without a caregiver and lower-functioning patients are at risk of missed diagnosis (Table 2A). Beyond those two patient types, perceptions vary across the specialties. A significantly higher proportion of neurology clinicians compared to psychiatry clinicians reported patients residing in a group home were at higher risk of missed diagnosis (37% psychiatry vs 68% neurology, p < 0.05). Conversely, a significantly higher proportion of psychiatry clinicians compared to neurology clinicians reported patients in private residences were at higher risk for missed diagnosis (35% psychiatry vs 19% neurology, p < 0.05) (Table 2A).
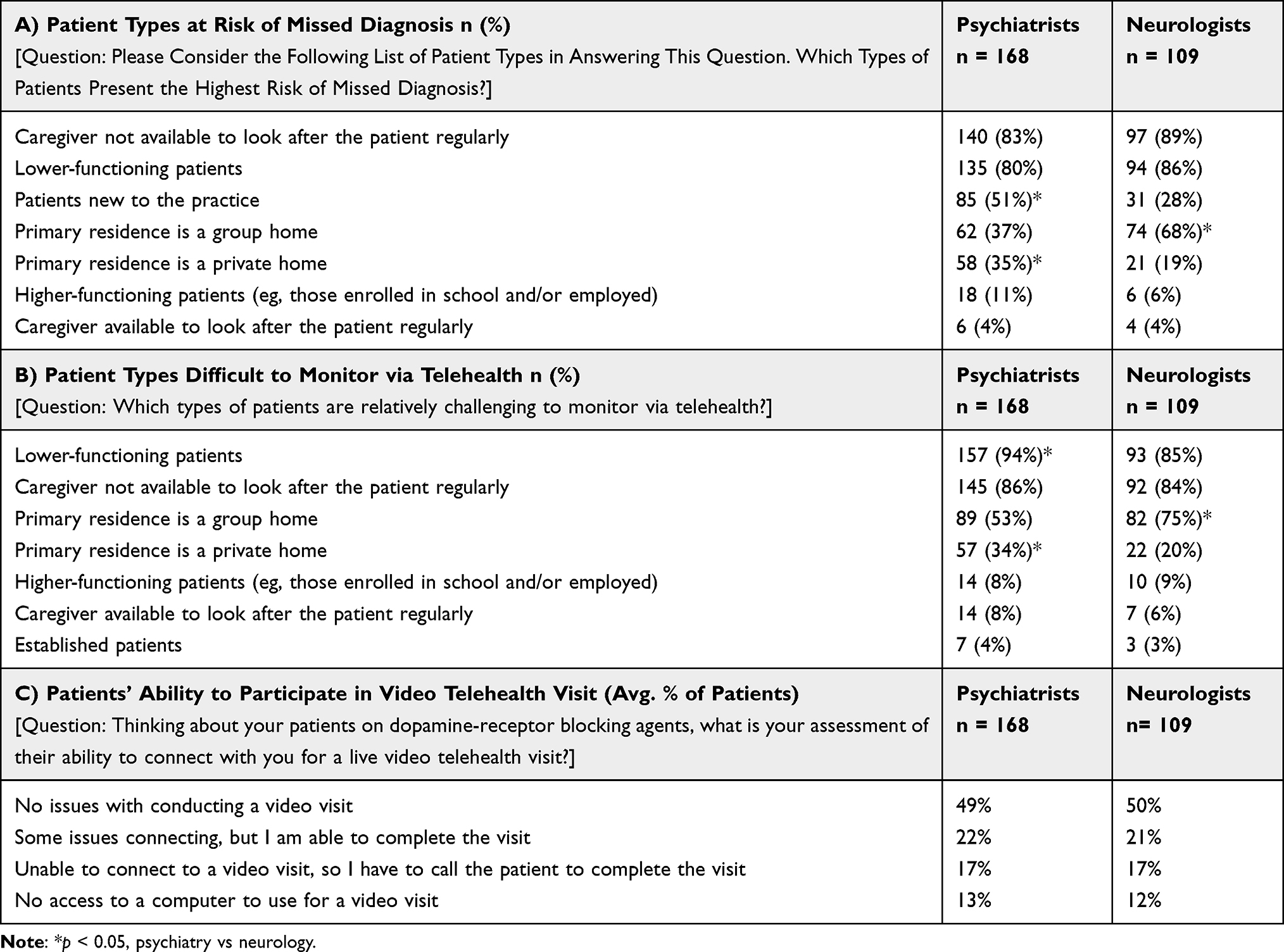 |
Table 2 Patient Characteristics |
Respondents were also asked to report the difficulty of monitoring patients via telehealth. Consistent with the findings related to patient types at risk of missed diagnosis, most clinicians reported that lower-functioning patients (94% psychiatry vs 85% neurology, p < 0.05) and those who live in group homes (53% psychiatry vs 75% neurology, p < 0.05) are difficult to monitor. They also find patients without caregivers (86% psychiatry vs 84% neurology) more difficult to monitor (Table 2B).
Additionally, technical barriers can limit clinicians’ ability to care for patients with DIMDs via telehealth. Clinicians across both specialties reported that on average only 50% of patients had no issues connecting for video visits. In fact, on average 30% of patients were either unable to connect successfully to a videoconference or did not have computer access, so the clinician either had to revert to a phone call or not provide care for the patient at all (Table 2C). The situation is even more challenging for patients seen in community mental health clinics where clinicians reported that on average approximately 40% of patients could not complete a video visit.
Socioeconomic and technical factors constrain access to telehealth for certain patient populations. Across both specialties, limited access to a computer was ranked as the most significant factor reducing clinicians’ ability to diagnose DIMDs via telehealth (Table 3). Clinicians in both psychiatry (83%) and neurology (73%) ranked this factor as one of their top three concerns. Other prominent factors included living alone (53% psychiatry vs 48% neurology), limited access to a telephone (48% psychiatry vs 43% neurology), and living in a group home (23% psychiatry vs 39% neurology) (Table 3).
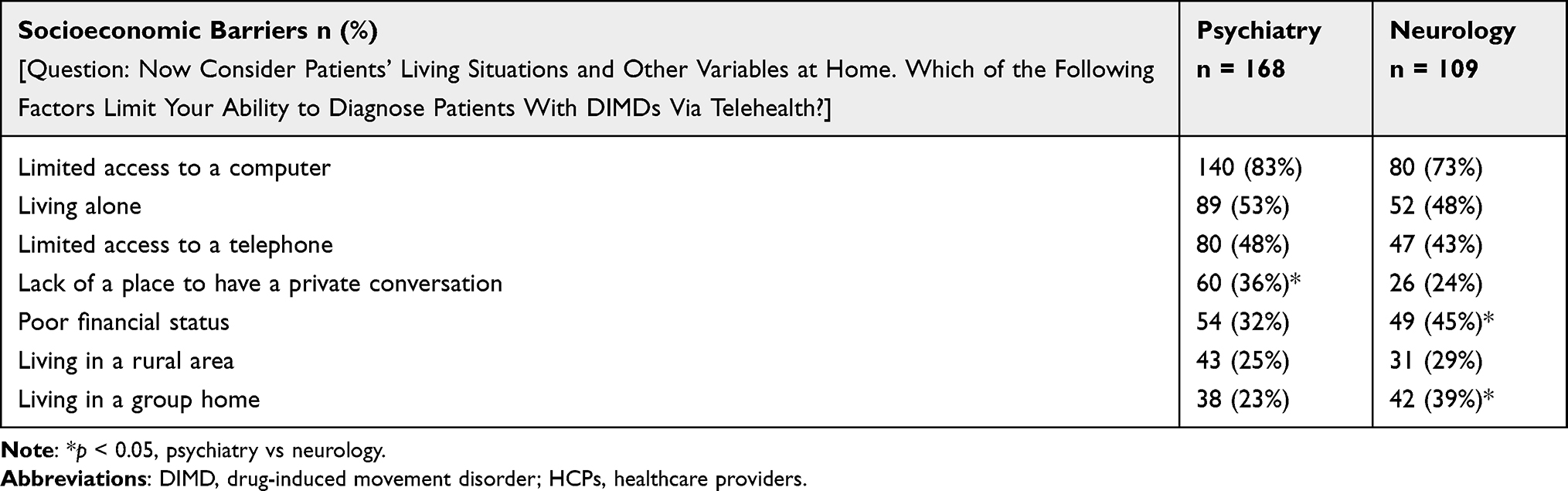 |
Table 3 Factors Limiting Ability of Clinicians to Diagnose DIMDs via Telehealth (% of HCPs) |
Caregiver Support and Training for Managing the Care of Patients with DIMDs
Caregiver participation improved clinicians’ ability to care for patients with DIMDs. Neurology clinicians reported that caregivers are present during an average of 64% of in-person visits compared to 51% of video visits and only 37% of phone visits. Of note, caregiver presence does seem to decrease the difficulty in evaluating patients via telehealth especially for phone visits. In general, 85% of neurology clinicians report difficulty in evaluating DIMDs via phone visits. However, that number drops to 69% when a caregiver is present (Figure 3). Similarly, 90% of psychiatry clinicians report difficulty in evaluating DIMDs via phone visits, but in the presence of a caregiver this drops to 69%. Furthermore, 83% of psychiatry clinicians and 89% of neurology clinicians were concerned about the risk of missed diagnosis during visits with patients without regular caregivers (Table 2A). Similarly, clinicians (86% psychiatry and 84% neurology) reported that patients without the presence of a regular caregiver were also very difficult to sufficiently monitor (Table 2B) Further, approximately half of the clinicians (53% in psychiatry and 48% in neurology) reported patients living alone were difficult to diagnose with DIMDs via telehealth (Table 3).
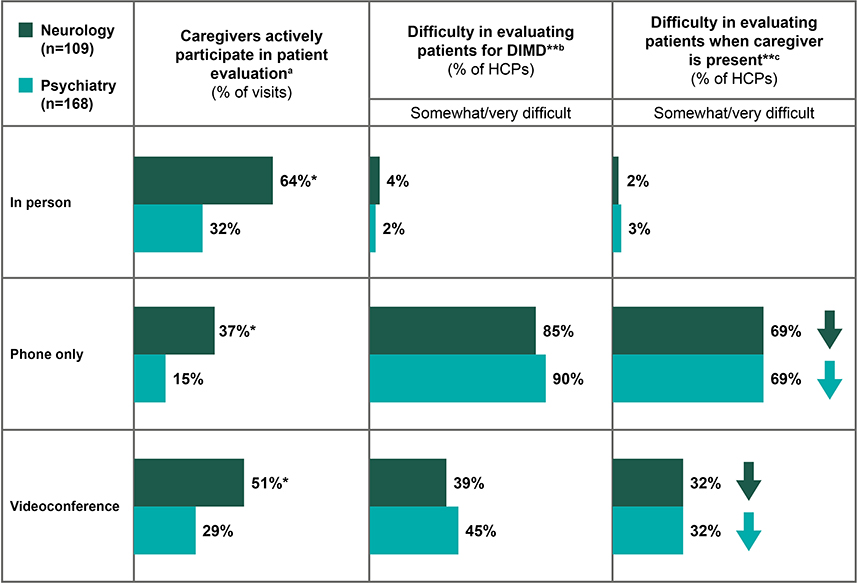 |
Figure 3 Impact of caregiver on the difficulty of evaluating patients with DIMDs. Survey questions: aWhen you evaluate patients on dopamine-receptor-blocking agents, what percentage of the time do their caregivers actively participate during the visit in each of the following treatment settings? bPlease rate the difficulty in evaluating patients on dopamine-receptor-blocking agents for DIMD in each setting, where 1 is “very easy” and 5 is “very difficult.” cHow would you rate the difficulty in evaluating patients on dopamine-receptor-blocking agents for DIMD when a caregiver is actively participating in the visit? Abbreviations: DIMD, drug-induced movement disorders; HCP, health care provider. Note: *p < 0.05, neurology vs psychiatry. **Rated on scale of 1–5 where, 1 is “very easy” and 5 is “very difficult”. |
Clinicians were asked to report their formal training on several topics related to telehealth. Most clinicians (58% psychiatry and 67% neurology) had no training on engaging caregivers as a health care partner despite the perceived positive impact of caregivers during telehealth visits. Approximately 50% of clinicians did not receive any training on topics such as general assessment and observation of patients, evaluation of patients with possible DIMDs, techniques for interviewing patients, and equipment for videoconferencing. Hence, providing clinicians with the necessary training to implement telehealth visits and engage caregivers can further facilitate effective management of patients with DIMDs.
Discussion
This real-world study outlines the challenges involved in detecting and monitoring patients with DIMDs via telehealth. This physician perception study consolidates limitations as reported by psychiatry and neurology clinicians and covers aspects of patient care while suggesting best practices for clinicians to improve their services via telehealth. Patients taking DRBAs should be evaluated regularly for DIMDs.27 A recent Delphi consensus recommends that a brief clinical assessment be performed at every clinical visit for patients taking DRBA.9 However, telehealth poses significant challenges for implementing these recommendations. The COVID-19 pandemic induced a surge in telehealth services14,28,29 (Supplementary Data 1, and Supplementary Figure 1), creating challenges in every facet of patient care in terms of evaluation, diagnosis, and monitoring. Fewer patients taking DRBAs were being evaluated for DIMDs in telehealth visits compared to in-person visits across both practice settings. Approximately 50% of clinicians in the study observed that physical symptoms of patients, such as trouble with gait, could not be evaluated via phone visits. Most clinicians found differential diagnosis and monitoring more difficult via phone visits compared to video visits. This study lists signs and symptoms related to patient social/emotional domains, physical activities, and activities of daily functioning that drive detailed evaluation of patients. The signs and symptoms within social and emotional domains include mention of tics/movements, embarrassment, avoidance of personal interactions, withdrawal from school/work, and challenges with employment. Physical signs and symptoms include trouble with gait, falls, walking, standing, difficulty in speaking, and painful movements. Signs and symptoms pertaining to activities of daily functioning include difficulty in swallowing or eating, showering and dressing, writing, using a phone or computer, and driving. Many of the above-mentioned top drivers or signs and symptoms that clinicians use to detect or monitor DIMDs in patients are difficult, if not impossible, to identify via phone and video visits. Overall, the study indicates that evaluation of DIMD symptoms is more challenging via phone visits and highlights the limitations clinicians face during evaluation of DIMD symptoms via telehealth.
Certain patient-related limitations that could impact proper diagnosis and monitoring of DIMDs were reported in the study. Specifically, patients without caregivers and lower-functioning patients were at higher risk of missed diagnosis and the same patient groups were also the most difficult to monitor. Also, patients from lower socioeconomic areas may have limited access to telehealth services despite the need for higher-care services.30 Lack of technical equipment and related resources can further hinder the effectiveness of telehealth visits.31 Hence, patient-associated factors, such as limited access to computers and/or telephones, and living alone, can also reduce the ability of clinicians to diagnose DIMDs. This suggests that a patient’s socioeconomic and technical limitations can impact diagnosis of DIMDs via telehealth, and prior awareness of these limitations can help clinicians plan more effective telehealth visits.
Challenges and difficulties clinicians experienced during the study can be resolved in several ways. On average, 30% of patients could not successfully complete a telehealth visit; caregiver support in such scenarios can alleviate difficulties associated with evaluation via telehealth. Accordingly, most clinicians in the study experienced less difficulty evaluating patients in the presence of a caregiver, especially during phone visits. Caregiver presence during telehealth visits can also reduce the risk of missed diagnosis. This was a major finding in the study as caregivers could be supportive in evaluating patients over a phone visit, and help clinicians monitor symptom progress over time. In this regard, training clinicians to engage caregivers can ease several limitations associated with DIMD care. Further training clinicians with the skills necessary for telehealth services will also enable them to improve the quality of their telehealth interactions. Developing a skilled workforce is the key requirement for long-term sustainability of telehealth services.25
Knowledge of patient-related limitations, such as lack of technical resources (computers and telephones)32 or absence of caregivers or family members, can help clinicians plan telehealth visits. As discussed earlier, approximately 30% of patients could not access telehealth successfully, and many had limited access to telephones. A physician’s pre-emptive knowledge of these patient-related factors can improve telehealth evaluation and facilitate symptom capture during a telehealth visit. We have summarized recommendations for improving clinician interactions via phone or video visits in Table 4. Based on the experiences from psychiatry and neurology practices, suitable probing questions for detection and monitoring DIMDs via telehealth visits were tabulated. Clinicians can pre-emptively identify those patients difficult to evaluate and monitor, at high risk of missed diagnosis, or having technical limitations. This information will enable them to optimally plan their assessment of signs and symptoms during the visit, which could then be confirmed by the caregiver or family member.
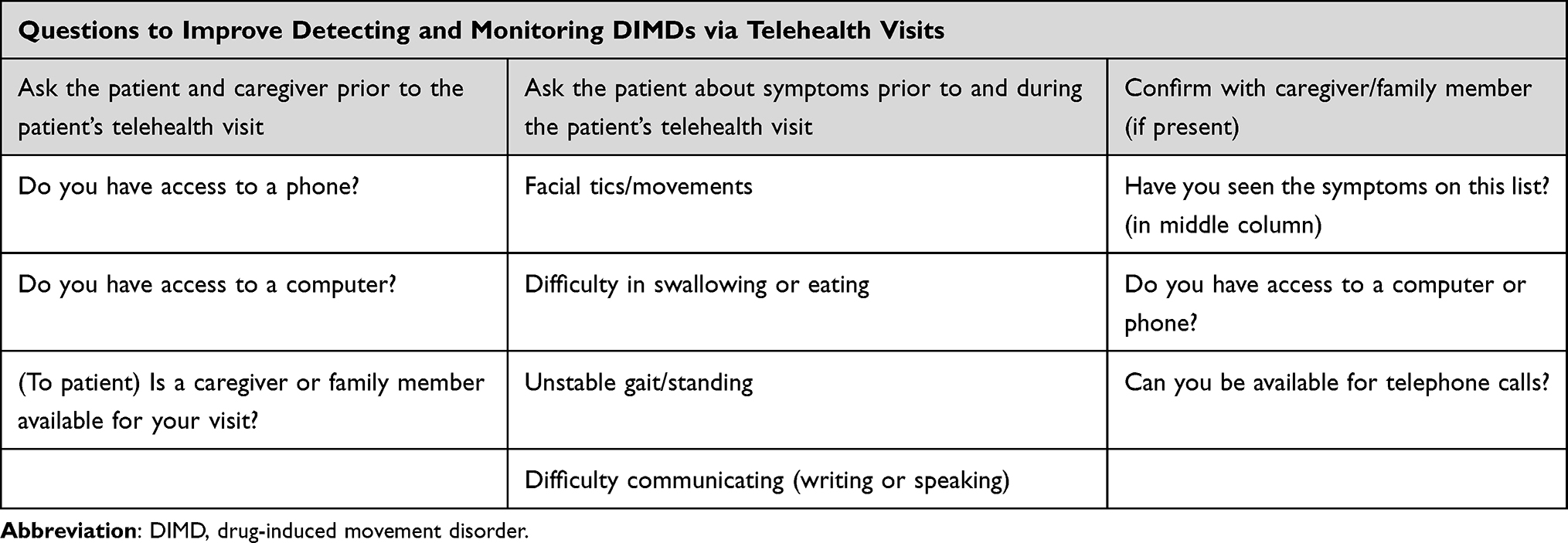 |
Table 4 Recommended Prompts for Improving Telehealth Queries |
Currently it is not clear if telehealth services alone, without periodic in-person care, will lead to improved DIMD health outcomes (Supplementary Data 2 and Supplementary Table 1). With the availability of validated instruments, telehealth can be used to help regularly monitor symptoms remotely.20 The convenience of telehealth services has been noted in previous studies in other clinical areas.26 Our study indicates that clinicians who treat mental health conditions and DIMDs perceived telehealth to be a convenient method to access health care. This suggests that telehealth services will be used beyond the COVID-19 public health emergency. In this regard, psychiatrists seem to be more open to telehealth services compared to neurologists (Supplementary Figure 2). However, telehealth has multifactorial limitations for evaluation of DIMDs, as seen in this study. Additional implementation and experience with telehealth by clinicians will provide more data to evaluate the quality of telehealth services and to gauge the impact of these services on health outcomes of patients with DIMDs.
The study had several limitations. It was restricted to those clinicians who conducted telehealth visits with >15% of their patients to ensure responding clinicians had some experience with telehealth and could provide a perspective on its impact on patient care. However, this may have limited feedback from clinicians who experienced more difficulties or had other reasons to not use telehealth. Also, the short timeframe during which clinicians joined the survey (~1 month) was due to the limited available quota for clinicians (100 for neurologists, 100 for psychiatrists, and 75 for NPPAs). With regard to the survey instrument, more questions should be developed probing training and education aspects of patients, family members, caregivers, and care staff. Also, options available for clinicians in our survey were constrained to only three modes of patient communication (in-person, telephone call, and video call) either in the presence or absence of a caregiver. The survey could have collected information about using asynchronous forms of communication like pre-recorded videos from family members or relatives, or other health care providers. Other important telehealth aspects related to equity of access, clinician perceptions about patient outcomes and impact of socioeconomic factors on outcomes were also beyond the scope of the study. The limited scope of our study allowed us to ask clinicians only about their experiences and their perceptions about managing patients with DIMD via telehealth. Despite these limitations, we believe the best telehealth practices discussed in the study may offer clinicians an opportunity to diagnose patients with a frequently debilitating condition. In this direction, future research can focus on various ways one can quantify clinician perception of improvement in the quality of telehealth visits.
Conclusion
The COVID-19 pandemic led to a surge in telehealth visits in both psychiatry and neurology practices, with the unfavorable consequence of considerably reducing clinicians’ ability to evaluate and monitor DIMDs. The physician perception survey results highlight limitations and risks faced by clinicians in diagnosing DIMDs and offers opportunities for improvement. Although in-person evaluation has been the gold standard for detecting and monitoring DIMDs, telehealth services will play a greater role in providing clinical care even after the pandemic wanes. Appropriate training for detection and monitoring in a telehealth setting, improving access to resources (computers and/or smart phones), engaging caregivers as health care partners, and developing in-between visit (patient-focused) tools can positively impact attitudes of clinicians toward incorporating telehealth services into their routine practices. This study highlights specific limitations and challenges and provides considerations to help clinicians better assess and manage DIMDs in the context of telehealth services.
Abbreviations
AIMS, Abnormal Involuntary Movement Scale; APA, American Psychiatric Association; ATA, American Telemedicine Association; CI, confidence interval; DIMD, drug-induced movement disorder; DRBA, dopamine-receptor blocking agent; IRB, Institutional Review Board; NP, nurse practitioner; PA, physician assistant; TD, tardive dyskinesia.
Ethics
The study was exempted under Common Rule 45 CFR § 46.104 (d)(2) from the Institutional Review Board (IRB), because the study did not include any interventions or patient interactions. Survey participant interactions were limited to survey and interview procedures, and there were adequate provisions to maintain patient privacy and confidentiality. Despite the study being exempted from IRB oversight, good research practices as per the Declaration of Helsinki were followed. Informed consent was obtained from participating clinicians at the beginning of the survey. Consenting clinicians were also informed about how survey responses and associated data will be used and publicly released. The WCG IRB (formerly Western IRB) granted approval for IQVIA to conduct this study.
Acknowledgments
We would like to acknowledge Prachi Deshpande from IQVIA for contributing to the study and reviewing the manuscript. We would like to thank Lakshman Puli, Laura Huber, and Jay Patel from IQVIA for their medical writing and editing support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Neurocrine Biosciences Inc., San Diego, CA.
Disclosure
RB has received research funding from Neurocrine Biosciences, Inc. EF, MB, SC, KM, DD, HC, and CY are employees and shareholders of Neurocrine Biosciences, Inc. BB is an employee of Emerging BioPharma, IQVIA Inc. The authors report no other conflicts of interest in this work.
References
1. Duma SR, Fung VS. Drug-induced movement disorders. Aust Prescr. 2019;42(2):56–61. doi:10.18773/austprescr.2019.014
2. Factor SA, Burkhard PR, Caroff S, et al. Recent developments in drug-induced movement disorders: a mixed picture. Lancet Neurol. 2019;18(9):880–890. doi:10.1016/s1474-4422(19)30152-8
3. Soares-Weiser K, Rathbone J, Ogawa Y, Shinohara K, Bergman H. Miscellaneous treatments for antipsychotic-induced tardive dyskinesia. Cochrane Database Syst Rev. 2018;3:CD000208. doi:10.1002/14651858.CD000208.pub2
4. Caroff SN. Overcoming barriers to effective management of tardive dyskinesia. Neuropsychiatr Dis Treat. 2019;15:785–794. doi:10.2147/ndt.S196541
5. Correll CU, Kane JM, Citrome LL. Epidemiology, prevention, and assessment of tardive dyskinesia and advances in treatment. J Clin Psychiatry. 2017;78(8):1136–1147. doi:10.4088/JCP.tv17016ah4c
6. Caroff SN, Aggarwal S, Yonan C. Treatment of tardive dyskinesia with tetrabenazine or valbenazine: a systematic review. J Comp Eff Res. 2018;7(2):135–148. doi:10.2217/cer-2017-0065
7. Carton L, Cottencin O, Lapeyre-Mestre M, et al. Off-label prescribing of antipsychotics in adults, children and elderly individuals: a systematic review of recent prescription trends. Curr Pharm Des. 2015;21(23):3280–3297. doi:10.2174/1381612821666150619092903
8. O’Brien PL, Cummings N, Mark TL. Off-label prescribing of psychotropic medication, 2005–2013: an examination of potential influences. Psychiatr Serv. 2017;68(6):549–558. doi:10.1176/appi.ps.201500482
9. Caroff SN, Citrome L, Meyer J, et al. A modified delphi consensus study of the screening, diagnosis, and treatment of tardive dyskinesia. J Clin Psychiatry. 2020;81(2). doi:10.4088/JCP.19cs12983
10. Hassan A, Mari Z, Gatto EM, et al. Global survey on telemedicine utilization for movement disorders during the COVID-19 pandemic. Mov Disord. 2020;35(10):1701–1711. doi:10.1002/mds.28284
11. Smith AC, Thomas E, Snoswell CL, et al. Telehealth for global emergencies: implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020;26(5):309–313. doi:10.1177/1357633X20916567
12. Suran M. Increased use of medicare telehealth during the pandemic. JAMA. 2022;327(4):313. doi:10.1001/jama.2021.23332
13. Kuehn BM. Despite improvements, COVID-19’s health care disruptions persist. JAMA. 2021;325(23):2335. doi:10.1001/jama.2021.9134
14. Esper CD, Scorr L, Papazian S, Bartholomew D, Esper GJ, Factor SA. Telemedicine in an academic movement disorders center during COVID-19. J Mov Disord. 2021;14(2):119–125. doi:10.14802/jmd.20099
15. Perez DL, Biffi A, Camprodon JA, et al. Telemedicine in behavioral neurology-neuropsychiatry: opportunities and challenges catalyzed by COVID-19. Cogn Behav Neurol. 2020;33(3):226–229. doi:10.1097/wnn.0000000000000239
16. Hu PJ-H, Chau PYK, Sheng ORL. Adoption of telemedicine technology by health care organizations: an exploratory study. J Organ Comput Electron Commer. 2002;12(3):197–221. doi:10.1207/S15327744JOCE1203_01
17. Srinivasan R, Ben-Pazi H, Dekker M, et al. Telemedicine for hyperkinetic movement disorders. Tremor Other Hyperkinet Mov. 2020;10. doi:10.7916/tohm.v0.698
18. Shore JH, Yellowlees P, Caudill R, et al. Best practices in videoconferencing-based telemental health April 2018. Telemed J E Health. 2018;24(11):827–832. doi:10.1089/tmj.2018.0237
19. Shore J, Vo A, Yellowlees P, et al. Antipsychotic-induced movement disorder: screening via telemental health. Telemed J E Health. 2015;21(12):1027–1029. doi:10.1089/tmj.2014.0242
20. Amarendran V, George A, Gersappe V, Krishnaswamy S, Warren C. The reliability of telepsychiatry for a neuropsychiatric assessment. Telemed J E Health. 2011;17(3):223–225. doi:10.1089/tmj.2010.0144
21. Gajarawala SN, Pelkowski JN. Telehealth Benefits and Barriers. J Nurse Pract. 2021;17(2):218–221. doi:10.1016/j.nurpra.2020.09.013
22. Snoswell CL, Chelberg G, De Guzman KR, et al. The clinical effectiveness of telehealth: a systematic review of meta-analyses from 2010 to 2019. J Telemed Telecare. 2021:1357633x211022907. doi:10.1177/1357633x211022907
23. Snoswell CL, Stringer H, Taylor ML, Caffery LJ, Smith AC. An overview of the effect of telehealth on mortality: a systematic review of meta-analyses. J Telemed Telecare. 2021;1357633X211023700. doi:10.1177/1357633X211023700
24. Chu C, Cram P, Pang A, Stamenova V, Tadrous M, Bhatia RS. Rural telemedicine use before and during the COVID-19 pandemic: repeated cross-sectional study. J Med Internet Res. 2021;23(4):e26960. doi:10.2196/26960
25. Thomas EE, Haydon HM, Mehrotra A, et al. Building on the momentum: sustaining telehealth beyond COVID-19. J Telemed Telecare. 2020;28(4):301–308. doi:10.1177/1357633X20960638
26. Barbosa W, Zhou K, Waddell E, Myers T, Dorsey ER. Improving access to care: telemedicine across medical domains. Annu Rev Public Health. 2021;42(1):463–481. doi:10.1146/annurev-publhealth-090519-093711
27. American Psychiatric Association. The American Psychiatric Association practice guideline for the treatment of patients with schizophrenia 3rd ed; 2021.
28. Cantor JH, McBain RK, Pera MF, Bravata DM, Whaley CM. Who is (and is not) receiving telemedicine care during the COVID-19 Pandemic. Am J Prev Med. 2021;61(3):434–438. doi:10.1016/j.amepre.2021.01.030
29. Svistova J, Harris C, Fogarty B, Kulp C, Lee A. Use of telehealth amid the COVID-19 pandemic: experiences of mental health providers serving rural youth and elderly in Pennsylvania. Adm Policy Ment Health. 2021;1–9. doi:10.1007/s10488-021-01181-z
30. Gallegos-Rejas VM, Thomas EE, Kelly JT, Smith AC. A multi-stakeholder approach is needed to reduce the digital divide and encourage equitable access to telehealth. J Telemed Telecare. 2022;1357633X221107995. doi:10.1177/1357633X221107995
31. Clare CA. Telehealth and the digital divide as a social determinant of health during the COVID-19 pandemic. Netw Model Anal Health Inform Bioinform. 2021;10(1):26. doi:10.1007/s13721-021-00300-y
32. Sanders C, Rogers A, Bowen R, et al. Exploring barriers to participation and adoption of telehealth and telecare within the whole system demonstrator trial: a qualitative study. BMC Health Serv Res. 2012;12:220. doi:10.1186/1472-6963-12-220
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.