Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Value of Sampling Time of Metagenomic Next-Generation Sequencing in Patients with Severe Pneumonia
Authors Li S, Zhou P, Yang L, Tang T, Qin J, Qian J, Bo S ![]() , Yu S
, Yu S
Received 21 June 2023
Accepted for publication 10 August 2023
Published 14 August 2023 Volume 2023:16 Pages 5263—5274
DOI https://doi.org/10.2147/IDR.S424185
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Shixiao Li,1 Peng Zhou,2 Lihong Yang,1 Tianbin Tang,1 Jiajia Qin,1 Jiao Qian,1 Shen Bo,1 Sufei Yu1
1Department of Clinical Microbiology Laboratory, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Taizhou, Zhejiang, People’s Republic of China; 2Department of Pharmacy, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Sufei Yu, Email [email protected]
Objective: Severe pneumonia is a common infectious disease with high morbidity and mortality. Early etiological diagnosis is crucial for improving the prognosis. The aim of this study is to evaluate the clinical value of sampling time of mNGS in patients with severe pneumonia.
Methods: This retrospective study enrolled 105 patients with severe pneumonia. mNGS was performed on bronchoalveolar lavage fluid (BALF). Patients were divided into the sampling time ≤ 72h vs sampling time > 72h groups and survivors vs non-survivors groups according to their sampling time and prognosis. Clinical characteristics, the adjustment of antibiotics and clinical prognostic value were evaluated.
Results: Our study showed that, early sampling of mNGS can significantly shorten the mechanical ventilation time (p = 0.007) and hospitalization time (p = 0.004). In the non-survivors group, CURB-65, SOFA, and APACHE II scores were higher. Age (OR: 1.051, 95% CI: 1.004– 1.100, p = 0.034), chronic respiratory diseases (OR: 4.639, 95% CI: 1.260– 17.082, p = 0.021), immunosuppression (OR: 5.008, 95% CI: 1.617– 15.510, p = 0.005) and SOFA score on the day of mNGS sampling (OR: 1.492, 95% CI: 1.212– 1.837, p < 0.001) were independent risk factors of in-hospital mortality. The most common pathogens were Klebsiella pneumoniae and Human gammaherpesvirus 4. The proportion of appropriate and targeted antibiotics adjusted was significantly higher than that in the sampling time > 72h group, and the proportion of antifungal and antiviral agents adjusted was lower. In the early sampling group, it was significantly decreased in the CRP, PCT level and NEU% at discharge.
Conclusion: This study demonstrated that early sampling of mNGS could shorten the time of mechanical ventilation and hospitalization of patients with severe pneumonia. Patients with higher SOFA score on the day of sampling had a poorer prognosis. It emphasizes that early sampling of mNGS has a positive value.
Keywords: metagenomic next generation sequencing, severe pneumonia, sampling time, mortality
Introduction
Severe pneumonia is associated with high morbidity and mortality, especially in the ICU, and is one of the global burdens of infectious diseases.1,2 For patients with severe pneumonia, rapid identification of pathogens and timely initiation of appropriate anti-infective therapy are the most critical determinants of prognosis. Furthermore, pathogen diagnosis is a key step in anti-infective treatment. Enteric Gram-negative bacilli, Staphylococcus aureus and non-fermentative bacteria accounted for most isolates from lower respiratory tract specimens. Atypical infections (2%) were uncommon.3 Viruses, except the influenza virus, respiratory viruses accounted for approximately 13.5–56.2% of community-acquired pneumonia (CAP).4
Conventional microbial culture methods, serological antigen and/or antibody testing and polymerase chain reaction (PCR) have limitations for pathogens detection, only using specific primers or probes, and only targeting a limited number of pathogens. As high-throughput and unbiased sequencing-based pathogens detection technology, mNGS characterizes all DNA or RNA existing in various clinical samples, providing new diagnostic evidence, which can be used to guide treatment planning and improve antibiotic management.5–7 In this study, we performed microbial mNGS assays on respiratory tract specimens of patients with severe pneumonia. However, reports on evaluating the impact of mNGS sampling time on patients with severe pneumonia remain scarce. The purpose of this study was to evaluate the correlation between the different sampling time of mNGS with the prognosis of patients with severe pneumonia, and to evaluate the benefits of early detection, which may be helpful to make more accurate clinical decisions.
Materials and Methods
Study Population
Patients hospitalized for suspected pneumonia from January 2019 to November 2022 were recruited from Taizhou Hospital of Zhejiang Province. All patients met the American Thoracic Society/ the Infectious Disease Society of America (ATS/IDSA 2019) criteria for predicting severe pneumonia.8 Inclusion criteria were (1) clinical suspicion of severe pneumonia; (2) could tolerate bronchoscopy. The exclusion criteria were as follow: (1) <18 years old; (2) missing data; (3) inter-hospital transfer; (4) having a history of hospitalization within 14 days before illness onset (Figure 1). Depending on the sampling time of mNGS after admission and clinical outcome that differentiate the sampling time ≤ 72h vs sampling time >72h groups or survivors vs non-survivors groups. In the sampling time ≤ 72h group (n=61), there were 36 survivors and 25 non-survivors. Among the patients whose sampling time was more than 72 h (n=44), 19 patients survived and 25 patients died. All patients signed informed consent forms before mNGS testing. This study was approved by the Institutional Medical Ethics Committee of Taizhou Hospital of Zhejiang Province.
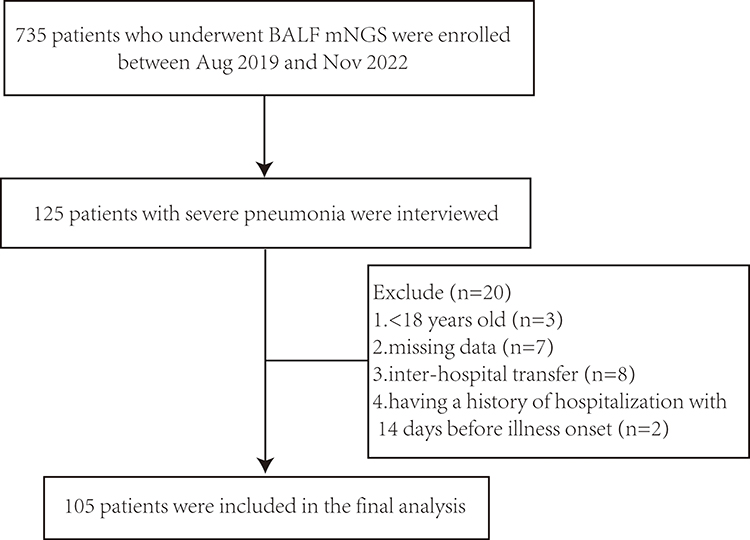 |
Figure 1 The flowchart of patient enrollment. |
Clinical Data Collection
Clinical information was collected from electronic medical records, including age, gender, smoking, underlying disease, first symptoms, blood laboratory tests on the day of mNGS sampling, usage of antimicrobial agents, invasive procedures, complications, clinical outcomes and changes in routine blood and inflammatory indicators (C-reactive protein, procalcitonin). Disease severity was determined based on confusion of new onset, blood urea nitrogen, respiratory rate, blood pressure and age 65 years or older (CURB65), sequential organ failure (SOFA) and acute physiology and chronic health evaluation II (APACHE II) scores.
mNGS Procedure for BALF Samples
BALF was collected from patients according to standard operating procedures. mNGS sequencing and analysis were performed by the methods reported in previous literature.9 The process of mNGS included experimental operation and bioinformatics analysis. (1) Sample processing and nucleic acid extraction: DNA was extracted according to the manufacturer’s recommendation. (2) Library construction and sequencing included DNA fragmentation, end repair, adapter ligation, PCR amplification and sequenced. For each batch, we used positive and negative controls for quality control and to minimize contamination. (3) Bioinformatics analysis included the following steps: data quality control, human sequence removal and microbial species comparison annotation. Interpretation criteria referred to previous research.9
Statistical Analysis
All data in the study were statistically analyzed by SPSS 23.0 (SPSS Inc., Chicago, IL, USA) and plotted using GraphPad Prism 7 software (GraphPad Software, Inc., La Jolla, CA, USA). Normally distributed data were presented as mean ± standard deviation (SD) and were compared between the two groups by t-test. Non-normally distributed data were presented as median and interquartile range (IQR) and were compared by Mann–Whitney U-test. The categorical variables were described by percentage and compared using the chi-square test. The factors screened in univariate analysis (variable p<0.2) were selected and multivariate analysis was conducted by binary logistic regression. The p<0.05 was considered to be statistically significant.
Results
A total of 105 critically ill patients were eligible for the study. Their baseline characteristics are shown in Table 1, 72.4% (76/105) of them were men. In-hospital mortality was 47.6%. Smoking and drinking histories of patients in different groups were similar. According to different sampling times, the mechanical ventilation time and hospitalization time in the sampling time ≤ 72h group were significantly shorter. Compared with the survivors group, patients in the non-survivors groups were older. There were significant differences in the following symptoms in the non-survivors group compared to the survivors group: fever (38.0% vs 60.0%, p = 0.024) and obnubilation (14.0% vs 1.8%, p = 0.026). In terms of underlying disease, the non-survivors group had a significantly higher proportion of cardiovascular diseases, chronic respiratory diseases and immunosuppression. Based on disease severity on the day of sampling, CURB-65, SOFA and APACHE II scores were higher in the non-survivors group.
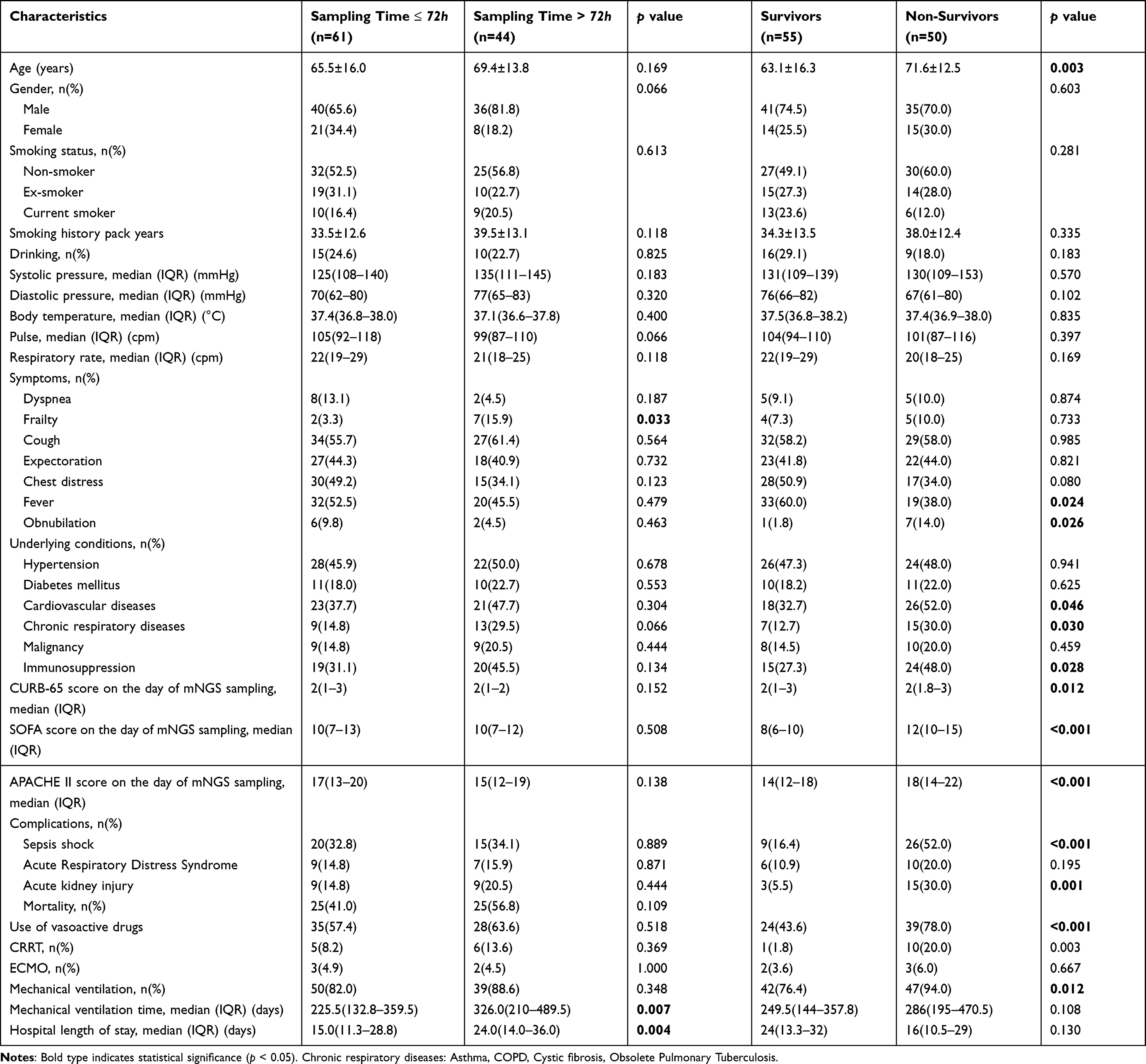 |
Table 1 Demographics, Clinical Characteristics and Outcome of Patients of Patients with Severe Pneumonia |
Laboratory findings recorded on the day of mNGS sampling were presented in Table 2. There was no specificity in routine laboratory findings among different groups. In the sampling time ≤ 72h group, PCT was significantly higher than that in the sampling time > 72h group, and the levels of ALP were significantly lower (p = 0.001). Compared with the survivors group, PLT was lower in non-survivor patients.
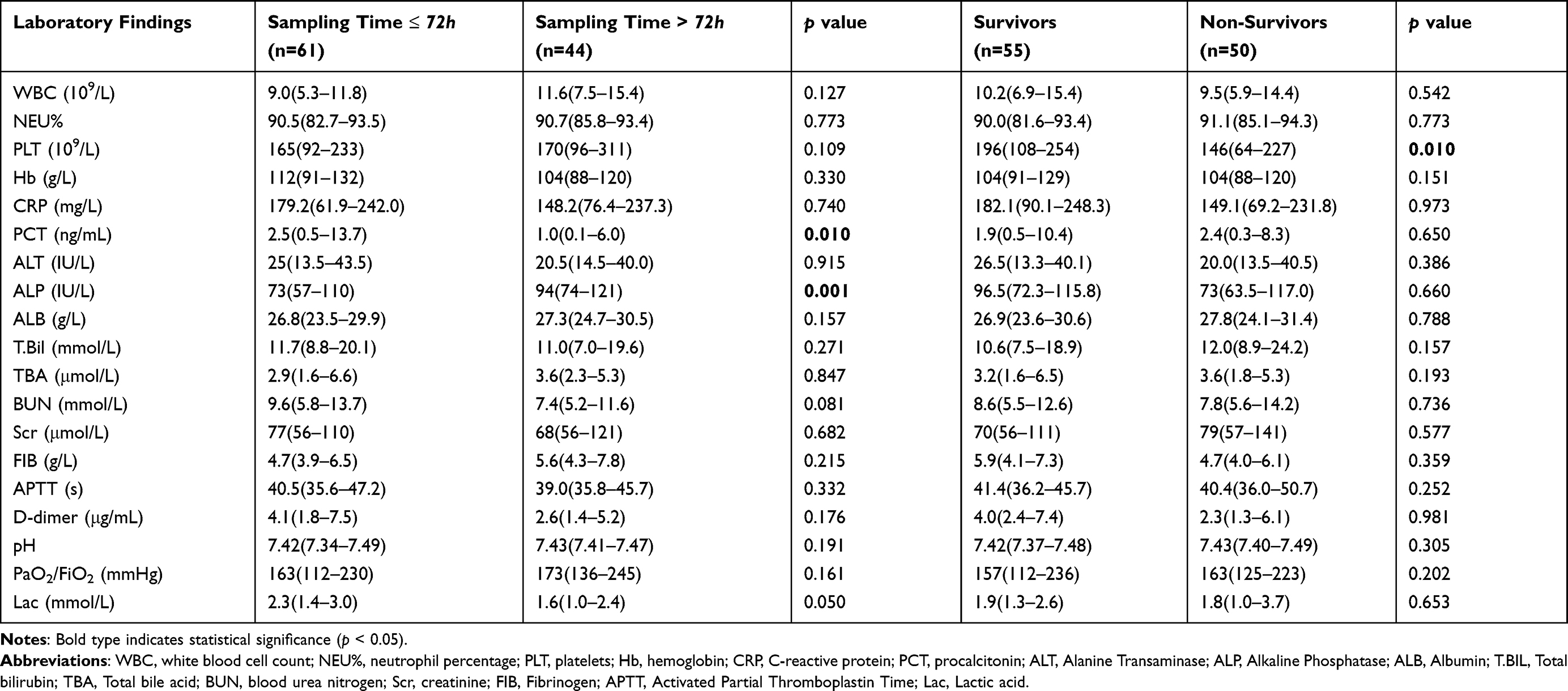 |
Table 2 Laboratory Findings of Patients with Severe Pneumonia on the Day of mNGS Sampling |
Further binary logistic regression analysis of p<0.2 above indicated that the independent variables related to in-hospital mortality included age (OR: 1.051, 95% CI: 1.004–1.100, p = 0.034), chronic respiratory diseases (OR: 4.639, 95% CI: 1.260–17.082, p = 0.021), immunosuppression (OR: 5.008, 95% CI: 1.617–15.510, p = 0.005) and SOFA score on the day of mNGS sampling (OR: 1.492, 95% CI: 1.212–1.837, p < 0.001) (Table 3).
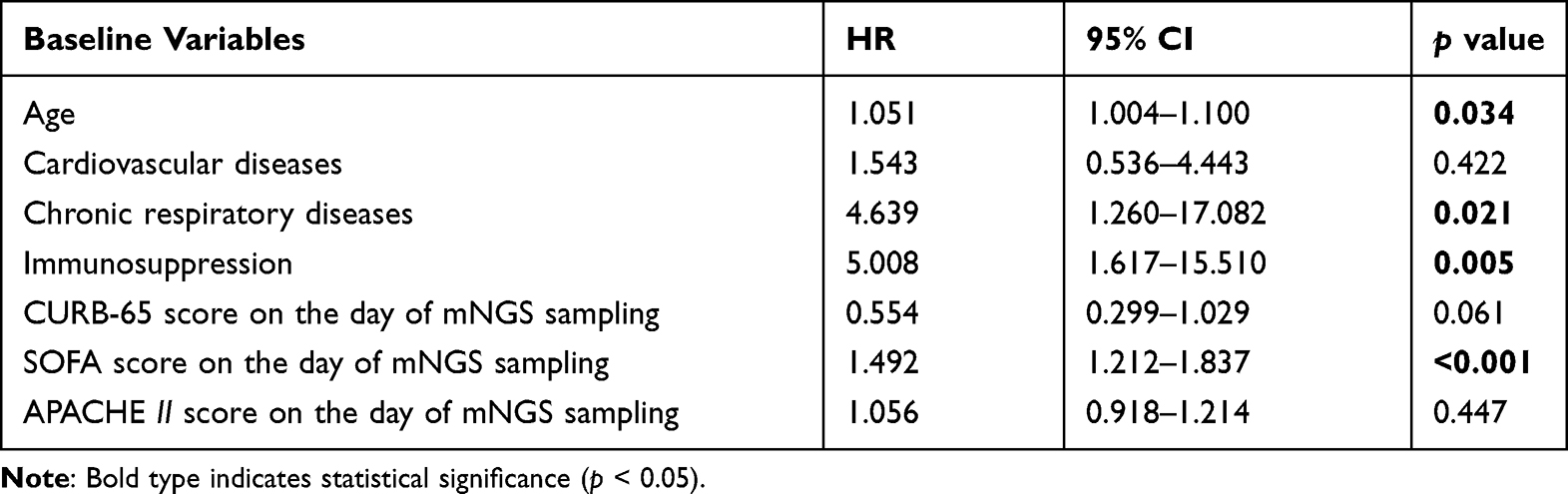 |
Table 3 Multivariable Analyses for Mortality with the Logistic Regression Model |
Of 105 cases, 5 cases were negative for mNGS analysis, single microorganism was detected in 27 cases, and multiple microorganisms were detected in 78 cases. The most frequently detected pathogen was Klebsiella pneumoniae (31 cases), followed by Human gammaherpesvirus 4 (25 cases), Candida albicans (23 cases) and Pseudomonas aeruginosa (23 cases) (Figure 2). 5 cases were positive for Chlamydia psittaci and 1 case was positive for Leptospira interrogans.
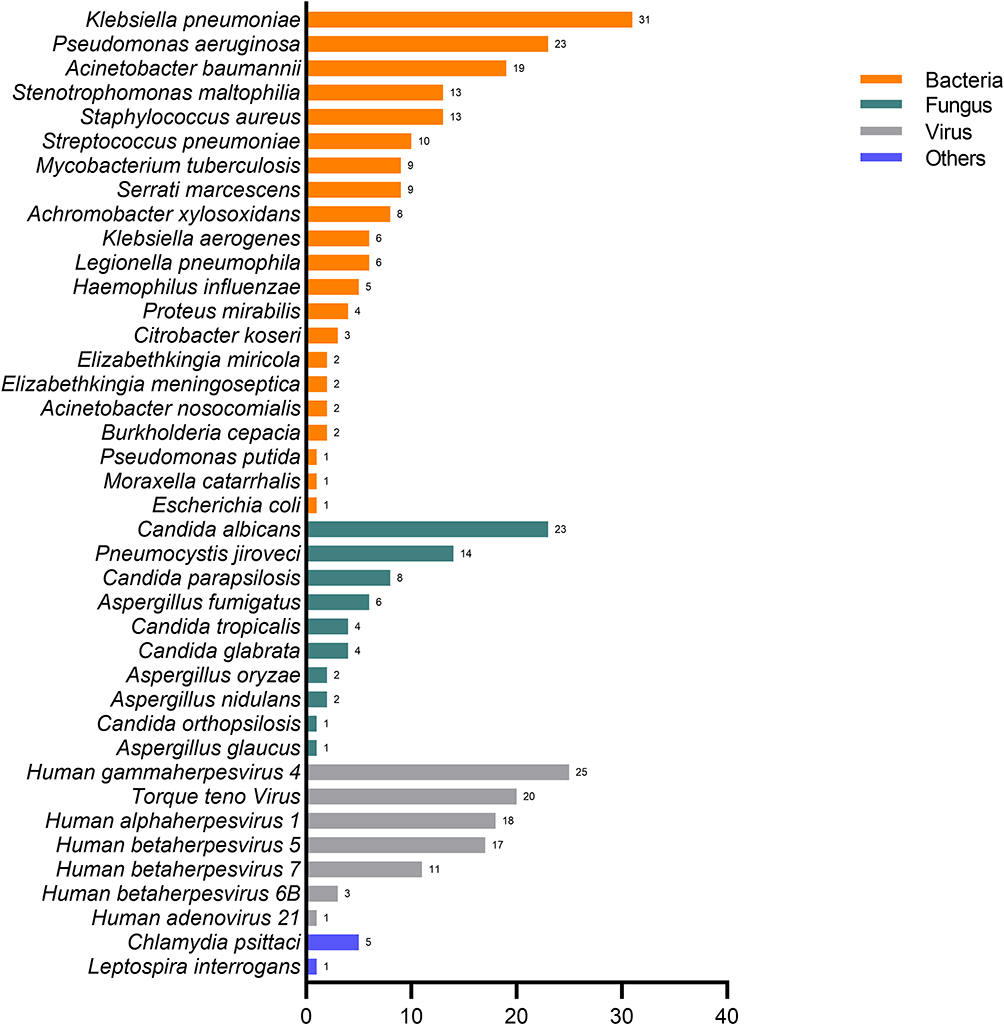 |
Figure 2 Different pathogenic organisms (in numbers) in mNGS. |
In clinical samples, the positive rates of various pathogenic microorganisms in different groups were compared (Figure 3). The most frequently detected pathogens in the sampling time ≤ 72h group were Klebsiella pneumoniae (32.8%), Pseudomonas aeruginosa (34.4%), Acinetobacter baumannii (21.3%), Staphylococcus aureus (18.0%), Streptococcus pneumoniae (13.1%), Candida albicans (36.1%) and Chlamydia psittaci (8.2%). While in the sampling time > 72h group, Stenotrophomonas maltophilia (15.9%), Pneumocystis jiroveci (22.7%), Aspergillus fumigatus (9.1%), Human alphaherpesvirus 1 (25.0%) and Human gammaherpesvirus 4 (31.8%). Staphylococcus aureus (16.4%), Mycobacterium tuberculosis (10.9%), Chlamydia psittaci (9.1%), Human gammaherpesvirus 4 (30.9%) had higher positive rate in the survivors group. Pseudomonas aeruginosa (30.0%), Acinetobacter baumannii (24.0%), Legionella pneumophila (10.0%), Aspergillus fumigatus (8.0%) and Human betaherpesvirus 5 (24.0%) had higher positive rate in the non-survivors group.
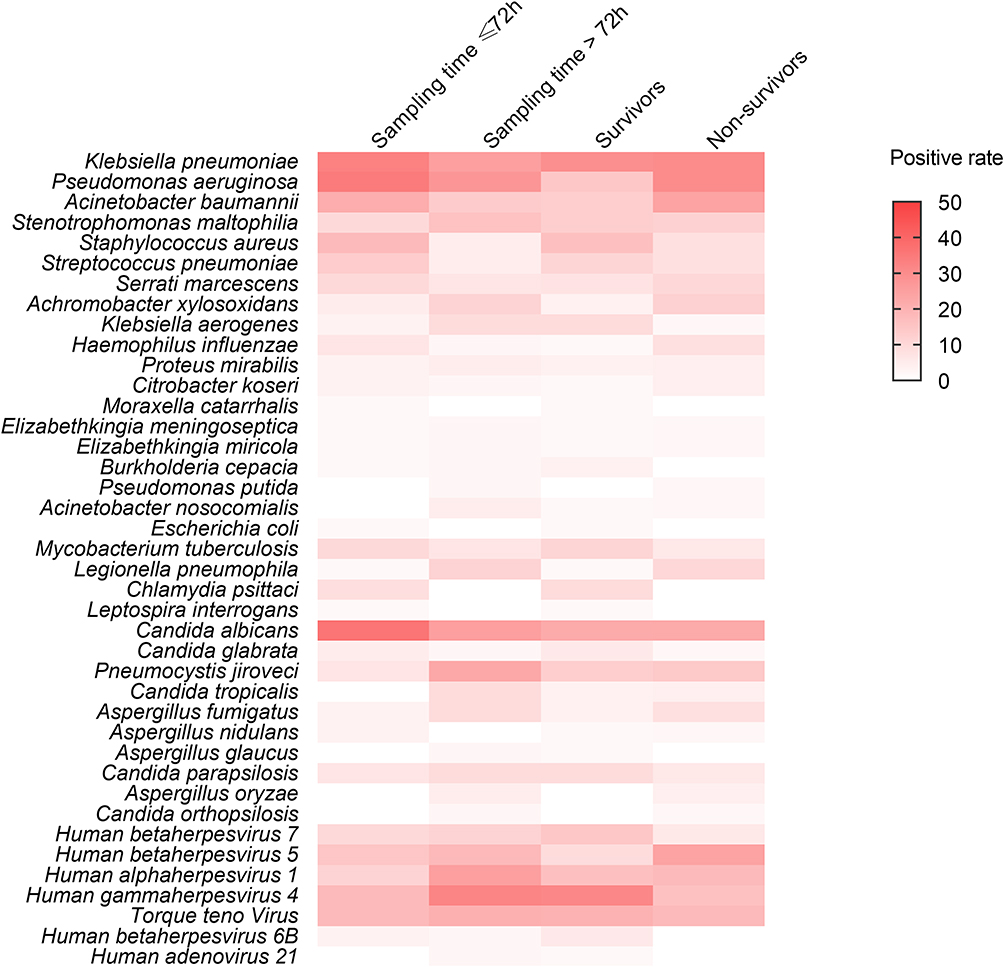 |
Figure 3 Positive rate of different pathogens in different groups. |
All 105 patients were treated with antibiotics during their hospitalization. According to the mNGS results, 22 cases had appropriate and targeted treatment in the sampling time ≤ 72h group, and the proportion of appropriate antibiotics adjusted was significantly higher than that in the sampling time > 72h group. While, the proportion of antifungal and antiviral agents adjusted in the sampling time > 72h group was higher than that in the sampling time ≤ 72h group (Figure 4).
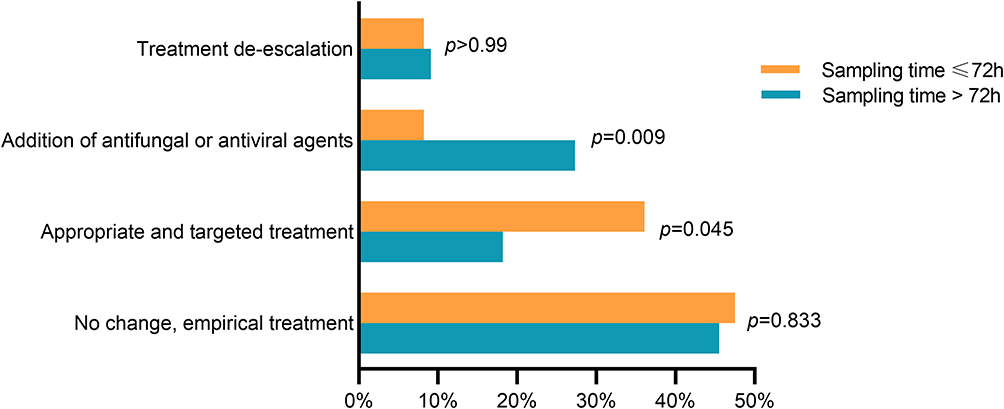 |
Figure 4 Clinical impact of different mNGS sampling time on antimicrobial adjustment. |
Most of the patients had obvious changes in inflammatory indicators from mNGS sampling to discharge. In the sampling time ≤ 72h group, it was significantly decreased in the CRP, PCT level and NEU%. In the sampling time > 72h group, CRP significantly decreased at discharge, while other inflammatory indicators had no significant difference (Figure 5).
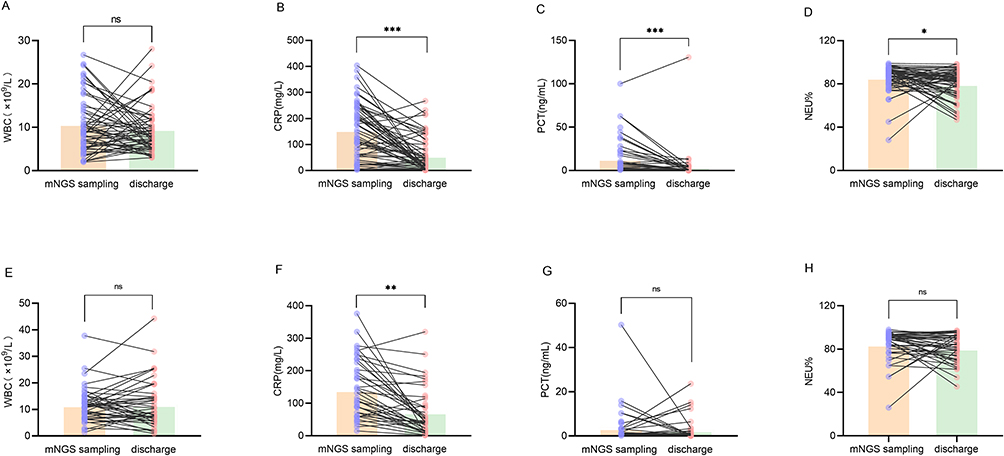 |
Figure 5 Comparison of inflammatory indicators at the time of mNGS sampling and discharge. (A–D) Sampling time ≤ 72h group, (E–H) Sampling time > 72h group. Abbreviation: ns, no significance. Notes: *p<0.05, **p<0.01, ***p<0.001. |
Discussion
The high mortality of severe pneumonia was related to unclear diagnosis and untimely treatment,10 and we speculated that the sampling time of mNGS was related to its clinical outcome. This retrospective study described the clinical utilization of mNGS in the diagnosis of infectious pathogens with BALF in patients with severe pneumonia. We compared the complications, mechanical ventilation and hospitalization time between the early sampling and non-early sampling, as well as the survivors and the non- survivors groups. We found that early sampling could reduce the time of mechanical ventilation and hospitalization, and the SOFA score of mNGS sampling was closely related to the hospital mortality. Our findings have important implications for choosing the appropriate sampling time for mNGS.
At present, there is no uniform and accurate suggestion on the best time for patients with severe pneumonia to use mNGS. Our data suggested that early sampling was significantly associated with decreased mechanical ventilation time and reduced hospital stays. Some studies showed that compared with non-NGS group, NGS had a tendency to reduce the mortality and shorten the mechanical ventilation time of patients with severe pneumonia.11,12 mNGS survey could reduce the 28-day mortality of ICU patients with mechanical ventilation, which may be associated with a better prognosis.13 Previous studies have proved that mechanical ventilation has become an important means to treat critically ill patients.14 Early anti-infection treatment is conducive to shortening the mechanical ventilation time and reducing the mortality. All these findings demonstrated that early sampling could provide patients with greater opportunities for treatment. However, in the end, it failed to improve the mortality of patients. There was no significant difference in hospitalization mortality between the two groups. Most of the patients had serious complications, and they might die of other complications, such as embolism and gastrointestinal bleeding, or more serious pneumonia (such as higher SOFA and APACHE II scores).
In addition, this study explored the severity of the patient at the time of mNGS sampling associated with in-hospital mortality, which may be crucial for clinical application. Consistent with a previous study, He et al reported that SOFA score on the day of mNGS sampling was an independent risk factor of the 28-day mortality in patients with sepsis (OR, 1.204; 95% CI, 1.038–1.397; p = 0.014).15 Sun et al showed that patients with high APACHE II score were more likely to obtain positive mNGS results, and the mNGS could help screen the pathogenic microorganisms when it was obtained within 24 hours.16 These indicated that it was necessary to have the timely use of mNGS when individuals with severe conditions.
This study showed that the lower respiratory tract samples of patients with severe pneumonia contained a variety of bacteria, fungi, viruses and atypical pathogens. The positive rate of mNGS was 95.2%. Previous studies indicated that compared to conventional methods, it had a wider pathogen spectrum and higher detection sensitivity.17 A prospective study showed that in immunocompromised adults, mNGS technology had an advantage in the diagnosis of mixed pathogens infection.18 In this study, 37.1% (39/105) patients were immunocompromised. Among them, multiple pathogens were detected in 27 patients. As shown in our results, in the sampling time ≤ 72h group, bacteria were more commonly detected because of shorter antibiotic exposure. While in the sampling time > 72h group, the proportion of Pneumocystis jiroveci, Aspergillus fumigatus, Human alphaherpesvirus 1 and Human gamma herpesvirus 4 was higher. In the non-survivors group, the proportion of Human betaherpesvirus 5 was higher. In addition, our results showed that the proportion of anti-fungal and anti-virus agents was higher than those in the sampling time > 72h group. It indicated that late sampling of mNGS had an advantage in the detection of opportunistic pathogens (ie, Pneumocystis jirovecii and Aspergillus) and viruses. As previously reported, patients with severe pneumonia in ICU were usually accompanied by the reactivation of cytomegalovirus (CMV), herpes simplex virus (HSV) and Epstein-Barr virus (EBV) in the process of disease treatment.19 Huang et al showed that CMV, HSV-1 and EBV reactivation were common and associated with an increased risk of mortality.20 The severity of the illness might increase the risk for viral reactivation and detection of fungi with a long incubation period.
The present study has several limitations. First, current results came from a single-center retrospective study. The limited number of cases might lead to biased conclusions, and further validation with a larger sample size is necessary. Second, we only included in-hospital mortality, some patients might die after hospital discharge and we could not obtain the leading cause of death. Third, due to the limitation of economic cost, we only conducted mNGS on DNA to detect bacteria, fungi and DNA viruses, while RNA viruses were not detected.
Conclusion
In conclusion, mNGS with different sampling times was valuable for the diagnosis, treatment and prognosis of severe pneumonia. This study emphasized that early sampling of mNGS could shorten the time of mechanical ventilation and hospitalization. Patients with higher SOFA score on the day of sampling had a poorer prognosis.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
The Institutional Medical Ethics Committee of Taizhou Hospital of Zhejiang Province granted approval for this retrospective study. Written informed consent was obtained from each patient before performing bronchoscopy, and identifying information was removed.
Acknowledgments
This study was conducted at Taizhou Hospital of Zhejiang Province affiliated to Wenzhou Medical University. We would like to thank all the staff and participants for their important contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from Taizhou Technology Project, Zhejiang Province (22ywa04) and Medical Science and Technology Project of Zhejiang Province (2023KY397).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stafylaki D, Maraki S, Vaporidi K, et al. Impact of molecular syndromic diagnosis of severe pneumonia in the management of critically Ill patients. Microbiol Spectr. 2022;10(5):e0161622. doi:10.1128/spectrum.01616-22
2. Nolley EP, Sahetya SK, Hochberg CH, et al. Outcomes among mechanically ventilated patients with severe pneumonia and acute hypoxemic respiratory failure from SARS-CoV-2 and other etiologies. JAMA Netw Open. 2023;6(1):e2250401. doi:10.1001/jamanetworkopen.2022.50401
3. El-Solh AA, Aquilina AT, Dhillon RS, Ramadan F, Nowak P, Davies J. Impact of invasive strategy on management of antimicrobial treatment failure in institutionalized older people with severe pneumonia. Am J Respir Crit Care Med. 2002;166(8):1038–1043. doi:10.1164/rccm.200202-123OC
4. Choi SH, Hong SB, Ko GB, et al. Viral infection in patients with severe pneumonia requiring intensive care unit admission. Am J Respir Crit Care Med. 2012;186(4):325–332. doi:10.1164/rccm.201112-2240OC
5. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341–355. doi:10.1038/s41576-019-0113-7
6. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 2019;14:319–338. doi:10.1146/annurev-pathmechdis-012418-012751
7. Han DS, Li ZY, Li R, Tan P, Zhang R, Li JM. mNGS in clinical microbiology laboratories: on the road to maturity. Crit Rev Microbiol. 2019;45:668–685. doi:10.1080/1040841X.2019.1681933
8. Metlay J, Waterer G, Long A, et al. Diagnosis and treatment of adults with community-acquired pneumonia. an official clinical practice guideline of the American thoracic society and infectious diseases society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
9. Li SX, Qin JJ, Zhou P, et al. The clinical significance of in-house metagenomic next-generation sequencing for bronchoalveolar lavage fluid diagnostics in patients with lower respiratory tract infections. Front Cell Infect Microbiol. 2022;12:961746. doi:10.3389/fcimb.2022.961746
10. Azoulay E, Mokart D, Kouatchet A, Demoule A, Lemiale V. Acute respiratory failure in immunocompromised adults. Lancet Respir Med. 2019;7(2):173–186. doi:10.1016/S2213-2600(18)30345-X
11. Liu Y, Zhang R, Yao B, et al. Metagenomics next-generation sequencing provides insights into the causative pathogens from critically ill patients with pneumonia and improves treatment strategies. Front Cell Infect Microbiol. 2022;12:1094518. doi:10.3389/fcimb.2022.1094518
12. Zhang P, Chen Y, Li SY, et al. Metagenomic next-generation sequencing for the clinical diagnosis and prognosis of acute respiratory distress syndrome caused by severe pneumonia: a retrospective study. PeerJ. 2020;8:e9623. doi:10.7717/peerj.9623
13. Xi Y, Zhou J, Lin ZM, et al. Patients with infectious diseases undergoing mechanical ventilation in the intensive care unit have better prognosis after receiving metagenomic next-generation sequencing assay. Int J Infect Dis. 2022;122:959–969. doi:10.1016/j.ijid.2022.07.062
14. John K, John T, Taljaard J, et al. The outcome of severe varicella pneumonia with respiratory failure admitted to the intensive care unit for mechanical ventilation. Eur Respir J. 2018;52(1):1800407. doi:10.1183/13993003.00407-2018
15. He DH, Liu M, Chen QM, et al. Clinical characteristics and the effect of timing for metagenomic next-generation sequencing in critically ill patients with sepsis. Infect Drug Resist. 2022;15:7377–7387. doi:10.2147/IDR.S390256
16. Sun LM, Zhang SG, Yang ZY, et al. Clinical application and influencing factor analysis of metagenomic next-generation sequencing (mNGS) in ICU patients with sepsis. Front Cell Infect Microbiol. 2022;12:905132. doi:10.3389/fcimb.2022.905132
17. Weng P, Wu LJ, Li Y, et al. Metagenomic next-generation sequencing for the detection of pathogenic microorganisms in patients with pulmonary infection. Am J Transl Res. 2022;14(9):6282–6288.
18. Parize P, Muth E, Richaud C, et al. Untargeted next-generation sequencing-based first-line diagnosis of infection in immunocompromised adults: a multicentre, blinded, prospective study. Clin Microbiol Infect. 2017;23(8):574 e571–574 e576. doi:10.1016/j.cmi.2017.02.006
19. Imlay H, Dasgupta S, Boeckh M, et al. Risk factors for cytomegalovirus reactivation and association with outcomes in critically ill adults with sepsis: a pooled analysis of prospective studies. J Infect Dis. 2021;223(12):2108–2112. doi:10.1093/infdis/jiaa697
20. Huang LT, Zhang X, Pang LS, et al. Viral reactivation in the lungs of patients with severe pneumonia is associated with increased mortality, a multicenter, retrospective study. J Med Virol. 2023;95(1):e28337. doi:10.1002/jmv.28337
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Endotracheal Intubation Timing on Clinical Outcomes in Patients with Severe Pneumonia: A Single-Center Retrospective Cohort Study
Bai WH, Cheng L
Infection and Drug Resistance 2026, 19:595644
Published Date: 27 March 2026