")
Back to Journals » International Journal of General Medicine » Volume 16
Clinical Value of Hospital-Community-Family Integrated Nursing Model in the Treatment of Patients with Hyperlipidemia Pancreatitis
Authors Wu JL, Liu JH, Zhang L, Shu Y, Guo XL, Gao AP
Received 19 May 2023
Accepted for publication 18 July 2023
Published 31 July 2023 Volume 2023:16 Pages 3219—3227
DOI https://doi.org/10.2147/IJGM.S421160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jin-Lan Wu,1,* Jin-Huan Liu,2,* Li Zhang,2 Yan Shu,1 Xiao-Li Guo,3 Ai-Ping Gao4
1Department of Respiratory and Critical Care Medicine, The People’s Hospital of Suzhou New District, Suzhou, Jiangsu, People’s Republic of China; 2Nursing Department, The People’s Hospital of Suzhou New District, Suzhou, Jiangsu, People’s Republic of China; 3Department of Gastroenterology, The People’s Hospital of Suzhou New District, Suzhou, Jiangsu, People’s Republic of China; 4Special Needs Clinic, The People’s Hospital of Suzhou New District, Suzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ai-Ping Gao, Email [email protected]
Objective: This study aimed to observe the impact of the hospital-community-family integrated nursing paradigm on the compliance, psychological state, and blood lipid levels in patients with hyperlipidemia pancreatitis (HLP).
Methods: Totally 66 HLP patients treated in our institution between June 2018 and June 2021 were randomized to Exp group and Con group. The Exp group received the hospital-community-family integrated nursing mode, whereas Con group adopted conventional nursing. Outcome measures included patient compliance, mental state, and blood cholesterol levels.
Results: Patients with integrated nursing exhibited markedly higher compliance than those with conventional nursing, as evinced by higher scores of compliance behavior, compliance awareness, medication attitude, and treatment attitude (P < 0.05). Integrated nursing offered more potent mitigation of negative emotions of patients than conventional nursing (P < 0.05). Integrated nursing resulted in better enhanced quality of life of patients versus conventional nursing (P < 0.05). Superior blood lipid amelioration was observed in patients after integration nursing versus those after conventional nursing, demonstrated by a higher serum high-density lipoprotein (HDL) level, and lower levels of triglycerides (TG), cholesterol (TC), and low-density lipoprotein (LDL) (P < 0.05). Patients were more satisfied with integrated nursing (96.97%) than conventional nursing (72.73%), suggesting a high patient acceptance of the nursing mode (P < 0.05).
Conclusion: The hospital-community-family integrated nursing model provides a viable alternative to enhance HLP patients’ compliance and optimize their psychological state and blood lipid levels, demonstrating good potential for clinical promotion.
Keywords: hospital-community-family, nursing model, hyperlipidemia pancreatitis, compliance, blood lipid level
Introduction
Hyperlipidaemic pancreatitis (HLP) features local inflammation of the pancreas, frequently accompanied by acute and persistent abdominal pain, and its prevalence has exhibited a rising trend with the changes in lifestyles and dietary habits.1 The onset of cute HLP is usually associated with existing diabetes, obesity, and hypertriglyceridaemia, while 15–20% of patients develop hypertriglyceridaemia in response to medication or dietary factors independently of diabetes, alcohol, or obesity.2,3 The pathophysiology is linked to increased synthesis of free fatty acids from the breakdown of high triglycerides, which exerts toxic effects on the pancreas and pathologically leads to reduced pancreatic microcirculation and calcium overload.4
The main clinical features of HLP are identical to those of non-hyperlipidemic acute pancreatitis, with upper abdominal pain, abdominal distension, nausea and vomiting as the main features.5 Nonetheless, abdominal pain and signs of peritonitis are not invariably observed, and early symptoms may only be reduced to abdominal distension, nausea and fever.6 In severe cases, toxic shock, severe metabolic disorders, fulminant pancreatitis, and even sepsis may arise, involving multiple organs such as the gastrointestinal tract, lungs, and kidneys, posing significant threats to patients’ lives.7 The key to treatment lies in triglyceride control, lifestyle modifications, and weight loss to prevent recurrence.8,9 If patients do not take their own lipid levels seriously, they are highly prone to disease recurrence due to excessively high blood lipid levels, causing secondary harm and resulting in poor prognosis. Clinical research has found that implementing effective nursing care during clinical treatment can control the disease progression and ensure the physical health of patients with acute pancreatitis complicated by hyperlipidemia.
HLP is considered a serious threat to human life given its rapid onset, severe conditions, and functional alterations in other organs,10 for which long-term nursing is required to facilitate functional rehabilitation of the joint. Conventionally, routine care and discharge instructions are adopted to improve patients’ outcomes.11,12 However, long-term medication, loss of treatment confidence, a negative psychological state, and low treatment compliance at home care are associated with poor treatment outcomes and reduced QoL.13,14 In this context, the hospital-community-family nursing model has emerged. The hospital-community-family linkage continuum of nursing care is an intervention model that effectively combines nursing at hospital, community and family, which extends the specialized care services from the hospital to the family, provides continuous and systematic care services, multi-level psychological, technical and professional information and care measures.15,16
The model has shown promising results of home care after percutaneous coronary intervention for coronary heart disease.17 Here, this study employed 66 HLP patients treated at our hospital between 2018 and June 2021 to investigate the effects of the hospital-community-home care model on treatment adherence, psychological state, and cholesterol levels in HLP patients.
Materials and Methods
Grouping
We adopted the random approach to assign 66 HLP patients admitted to our hospital between June 2018 and June 2021 into two groups based on different management strategies. The randomization was carried out using an online web-based randomization tool (freely available at http://www.randomizer.org/). For the concealment of allocation, the randomization procedure and assignment were managed by an independent research assistant who was not involved in the screening or evaluation of the participants. The original sample size calculation estimated that 30 patients in each group would be needed to detect a 3-point difference between groups in a 2-sided significance test with a power of 0.8 and an alpha error level of 0.05.
Prior to enrolment, informed consent was obtained from patients and signed by them for the study. The study protocol was approved by the ethics committee of the people’s hospital of Suzhou New District. Ethical review: SD-SE20180606. All processes were conducted in accordance with the Declaration of Helsinki Ethical Guidelines for clinical research.
Inclusion Criteria
(1) Patients who met the clinical diagnostic criteria in the Guidelines for the Diagnosis and Treatment of Acute Pancreatitis.18 (2) Patients aged ≥25 years old. (3) Patients with complete clinical medical records. (4) This study was conducted with approval from the ethics committee of our hospital and the consent of the patients and their families was obtained.
Exclusion Criteria
(1) Patients were complicated with severe cardiovascular, cerebrovascular, hepatic, renal and haematopoietic systems and psychiatric disorders. (2) Patients who had participated in similar research. (3) Patients who had mental or cognitive impairment or were reluctant to cooperate with the study. (4) Patients who rescinded their consent due to uncontrollable factors. (5) Patients with other causes such as bile duct stones, obstruction, trauma, and surgery. (6) Patients with altered consciousness, shock or acute respiratory distress syndrome on admission. (7) Patients who have not been treated in accordance with the prescribed requirements and whose efficacy cannot be judged, or whose results cannot be judged because of incomplete information.
Methods
Both groups received standardized treatment, including instructions on medication, diet, and blood lipid monitoring. The Con group received conventional care and discharge instructions, and the Exp group adopted the hospital-community-family integrated care mode. The Con group was given routine care and discharge instructions, including medication administration and health education in accordance with routine nursing procedures, and patients were informed of post-discharge matters and followed up regularly.
The Exp group received a hospital-community-family integrated nursing model, and the specific interventions were as follows: 1) A three-tier linkage care team consisting of 2 specialist doctors from the hospital, 2 head nurses, 2 nurses, 1 community doctor, and 2 community nurses and family members was set up, and regular training was provided to the team members, including knowledge of HLP, care methods and precautions, and clarification of job responsibilities. 2) Internet information platform was established, including modules for general data, medical records, specialist consultation records, disease knowledge and doctor-patient communication, and staff was assigned for management and maintenance. 3) Hospital-level nursing. Medical staff collected all the data of inpatients and combined the actual conditions of the patients to formulate a ternary linkage nursing home care plan. The specific contents include the use of Internet system, data query, informing patients of the nearest community hospital, regularly sending HLP disease information, first aid knowledge, medication guidance, diet guidance through the official WeChat account, answering questions raised by patients online, and video visits to understand patients’ disease status and offer suggestions. 4) Community-level nursing. Community nurses were arranged to carry out regular home visits to keep track of the patients’ recovery status, answer questions raised by the patients one by one, formulate a reasonable diet and exercise plan, and upload the actual situation of the patients after the return visits to the online platform.
- Family-level nursing. Families were educated about triple-linked care to understand the disease and related nursing skills and improve their disease awareness and nursing skills through the online platform. The families of the patients were allowed to consult the medical staff in the WeChat group about issues encountered in the nursing process. Their families were encouraged to communicate with the patients to understand their thoughts, relieve adverse psychological emotions, and improve their confidence in treatment. Both groups received continuous care for 3 months.
Observation Indicators
Baseline Data
The baseline data such as sex, age, course of disease and other data of patients were compared.
Treatment Compliance
The Champion Health Belief Model Scale (CHBMS) was used to evaluate the compliance of patients before and after intervention from the four dimensions of perception, application, diet, and medication, with a score of 4, 3, 2, and 1 point(s), respectively.19 A higher score indicates a better compliance.
Compliance Behaviors
It was scored from the three dimensions of compliance awareness, medication attitude, and treatment attitude, using our hospital’s self-made compliance behavior assessment scale (total score: 100 points). A higher score implies a higher the degree of coordination and compliance.
Post-Intervention Psychological State
The anxiety and depression were evaluated using self-rating anxiety scale (SAS)/self-rating depression scale (SDS) compiled by Zung.20 The scores for the 20 items were added to give a gross score and then multiplied by 1.25 to give a whole number fraction as the standard score. Based on the results, the cutoff value of SAS and SDS was 50 points, with 50–59 points for mild anxiety and depression, 60–69 for moderate, 70 or more for severe.
Quality of Life
The SF-36 scale was used to evaluate emotional function, social function, physiological function, and mental health of patients. Each dimension was scored from 0 to 100, and a higher score indicates a better QoL.21
Blood Lipid Levels
Fasting venous blood (3mL) was collected from the patients before the intervention and on the next morning after the intervention, and an automatic biochemical instrument was used to determine the high-density lipoprotein (HDL), triglycerides (TG), low-density lipoprotein (LDL), and cholesterol (TC). The normal value was as follows: HDL-C: 0.9–2.19 mmol/L (35–85mg/dI); TG: 0.22–1.21 mmol/L (20–110mg/dl); TC: 2.86–5.98 mmol/L (110–230mg/dl); LDL-C: <3.12 mmol/L (120 mg/dl).
Nursing Satisfaction
The satisfaction was evaluated using a self-made satisfaction survey questionnaire to monitor the satisfaction of the whole nursing process, including extremely satisfied, satisfied, and dissatisfied. The overall satisfaction = (very satisfied + satisfied)/number of cases × 100%.
Statistical Analyses
All data were analyzed using SPSS20.0 software. The count data were expressed as [n (%)], and the comparison was conducted by x2 test; Normally distributed measurement data were expressed as ( ), and compared by t-test. P < 0.05 indicates a notable difference.
), and compared by t-test. P < 0.05 indicates a notable difference.
Results
General Data
The age, BMI, disease, HLP severity, marriage status, education-related information were collected and compared. The results showed that the two groups were similar in age, BMI, course of disease, gender, etc. (P > 0.05) (Table 1).
 |
Table 1 Comparison of the General Information |
Comparison of the Compliance
The Con group exhibited the compliance score of (15.18±5.23) and (13.56±3.76) before and after the intervention, respectively, whereas the Exp group had the compliance scores of (15.21±5.12) and (18.52±3.65) before and after the intervention, respectively. No significant difference in compliance was observed between Con group and Exp group before intervention. After intervention, the compliance score of Exp group was increased and higher than Con group (all P < 0.05) (Figure 1).
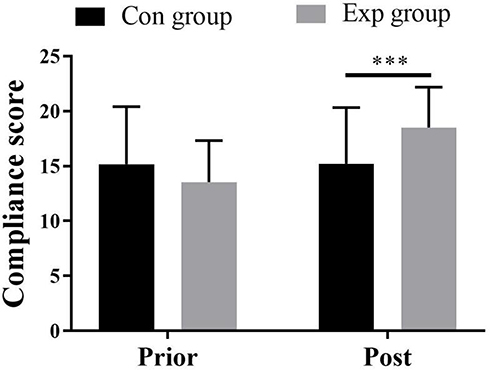 |
Figure 1 Comparison of compliance, ***Indicated P < 0.001. |
Inter-Comparison of the Behavior Following Doctor’s Instruction
Patients with integrated nursing exhibited markedly higher compliance than those with conventional nursing, as evinced by higher scores of compliance behavior, compliance awareness, medication attitude, and treatment attitude (P < 0.05) (Table 2).
 |
Table 2 Comparison of Behaviors Following Doctor Instructions ( |

Inter-Comparison of the Mental State
Before intervention, SAS and SDS score of the Exp group was (61.25±8.58) and (66.25±11.26), whereas the Con group was (63.25±8.29) and (63.84±9.26), respectively. After intervention, SAS and SDS score of the Exp group was (42.25±3.12) and (45.36±2.45), whereas the Con group was (51.36±3.68) and (49.74±2.86), respectively. Prior intervention, there was no significant difference between the SAS and SDS scores between the two groups, and the above scores decreased significantly post intervention, and the Exp group was significantly lower than that of the Con group. Integrated nursing offer more potent mitigation in negative emotions of patients than conventional nursing (P < 0.05) (Figure 2A and B).
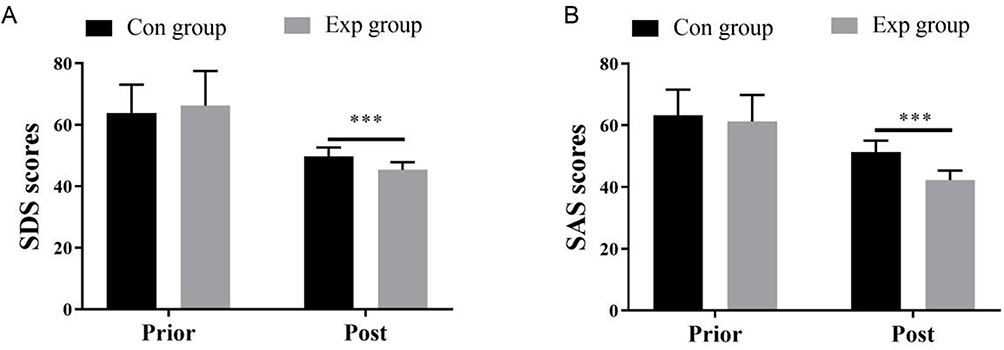 |
Figure 2 Comparison of the psychological state. (A) SDS score. (B) SAS score. ***Indicated P < 0.001. |
Inter-Comparison of the QoL
Prior to intervention, there was no discernible difference in QoL between the two groups (P > 0.05). Integrated nursing resulted in better enhanced quality of life of patients versus conventional nursing (P < 0.05) (Table 3).
 |

Inter-Comparison of the Blood Lipid Levels
Prior to intervention, no significant difference was presented in blood lipid levels between the two groups (P > 0.05). Superior blood lipid amelioration was observed in patients after integration nursing versus those after conventional nursing, demonstrated by a higher serum HDL level and lower levels of TG, TC, and LDL (P < 0.05) (Table 4).
 |

Comparison of the Satisfaction
The total number of satisfied cases in the Exp and Con groups was 32 and 24. Patients were more satisfied with integrated nursing (96.97%) than conventional nursing (72.73%), suggesting a high patient acceptance of the nursing mode (P < 0.05) (P < 0.05). For one unsatisfied patient in Exp group, he felt that there was too much contact with people and information in nursing and that it consumed a lot of time which was unnecessary (Table 5).
 |
Table 5 Comparison of the Satisfaction [n (%)] |
Discussion
HLP is a contributing factor to pancreatitis, whose etiology has been hypothesized to be associated with foods containing large amounts of fats, cholesterol and alcohol, which causes abnormally high serum triglycerides, leading to increased pressure on the pancreas and eventually the rupture of the alveoli and the development of pancreatitis.22,23 Thus, dietary avoidance of foods high in cholesterol and fat, appropriate exercise to prevent hyperlipidemia, and the use of lipid-lowering medications, such as simvastatin might reduce the risk of HLP.24,25 Of critical importance in the treatment of HLP is the control of lipid levels, which can be challenging to cure due to the long course of the disease.26 Therefore, long-term medication is required to control disease progression, and ineffective blood lipids control may cause disease exacerbation and compromise the patient’s health and life. In patients with atrial fibrillation, chronic heart failure, and hypertension, the application of hospital-community-family integrated nursing can vertically integrate medical resources and establish a truly effective hierarchical treatment model. Hospital-community-family integrated nursing can improve patient compliance with treatment, enhance patients’ self-management ability and confidence, and improve the management efficiency of medical staff.27
Non-pharmacological therapies such as healthy dietary management, exercise therapy, positive stress reduction therapy, and continuity of care play a key role in the management of chronic disease.28 The extended care, a new model of care, has proven its effectiveness in the rehabilitation of chronic diseases. The application of the triadic linkage extended care model to the care of patients with chronic diseases has achieved positive results. This care model integrates hospital, community, and family provides targeted care for patients through the formation of ternary care teams, and develops an internet-based platform to improve communication among doctors, nurses, patients, and their families.29 In addition, this model enables more humane care and improves patients’ compliance, which avoids poor adherence behaviour, alleviates negative psychological states, and enhances lipid control.30
This study confirmed a higher compliance score of the Exp group than the Con group after intervention. In detail, higher scores of compliance awareness, medication attitude, and treatment attitude of the Exp group than the Con group indicate that integrated nursing can improve patients’ compliance, and boost the patient’s behavior following doctor instruction. The reason for this is that in the hospital-community-family continuum of care, the hospital organizes and designs the nursing program, uses the online platform to strengthen communication with the community and the patient’s family, and promotes the linkage between the hospital and the community, thus ensuring easy access to continuum of care services for patients. The responsibility of the community mainly consists of providing home visit and question resolving, offering health advice and rehabilitation guidance, and correcting patients’ unreasonable rehabilitation measures in a timely manner. Thus, patients were instructed to better follow medical advice during home care.31,32
Moreover, the Exp group experienced a better psychological state after intervention, which was in line with the results of Chen et al, suggesting that the negative mental state of patients can be relieved by this nursing mode.33 Also, the current study demonstrated that the Exp group had a high HDL after intervention, but a lower level of TG, TC and LDL than the Con group. The total satisfaction rate of the Exp group was higher than that of the Con group. The hospital-community-family integrated nursing mode could control the blood lipids, stabilize the condition, and improve the satisfaction of patients. The hospital-community-home continuum of care allows family caregivers to access the knowledge according to their specific needs, which increases their disease awareness and improves their nursing skills, thus ensuring continuous professional guidance and care during out-of-hospital rehabilitation.34,35
In hospital medicine, the population of patients with chronic conditions who require maintenance treatment after discharge from a stable HLP condition is much larger than the inpatient population. A significant proportion of chronic disease patients return to the community or to their families as a continuation of their inpatient treatment to understand the effects of their hospitalisation.36 The lack of awareness of and adherence to maintenance treatment in this group of patients resulted in treatment difficulty and recurrence, as well as noncompliance and low adherence to medication in others, which may compromise the treatment outcomes and quality of survival and lower patient satisfaction.37 There are no mature follow-up health services after discharge from hospital in China, and the lack of appropriate and effective care may easily cause physical and mental dysfunction or lead to readmission to hospital. The Hospital-Community-Family Interactive Care organically combines the technical strengths of hospitals with the strength of nursing experts to form an interaction among doctors, nurses and patients, allowing the extension of hospital nursing services to the community and even to the family.
Conclusion
The hospital-community-family integrated nursing model provides a viable alternative to enhance HLP patients’ compliance and optimize their psychological state and blood lipid levels, demonstrating good potential for clinical promotion.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu Y, Sun Y, Xue BH, et al. Negative regulation of SIRT1 by IRF9 involved in hyperlipidemia acute pancreatitis associated with kidney injury. Dig Dis Sci. 2021;66(4):1063–1071. doi:10.1007/s10620-020-06331-1
2. Wu Z, Wang X, Jiang X. Study on the mechanism of probucol nanosuspension on hyperlipidemic pancreatitis and regulation of blood lipid function. J Nanosci Nanotechnol. 2021;21(2):1286–1292. doi:10.1166/jnn.2021.18663
3. Renated L, Iversen T, Mogensen PR, et al. Effect of fish oil supplementation on hyperlipidemia during childhood acute lymphoblastic leukemia treatment – a pilot study. Nutr Cancer. 2021;73(9):1816–1820. doi:10.1080/01635581.2020.1803934
4. Liu Y, Sun Y, Xue BH, et al. Negative regulation of SIRT1 by IRF9 involved in hyperlipidemia acute pancreatitis associated with kidney injury. Dig Dis Sci. 2020;66(4):1063–1071.
5. Li X, Li L, Liu L, et al. Risk factors of multidrug resistant pathogens induced infection in severe acute pancreatitis. Shock. 2020;53(3):293–298. doi:10.1097/SHK.0000000000001371
6. Li M, Xing XK, Zhi-Hua L, et al. Comparison of scoring systems in predicting severity and prognosis of hypertriglyceridemia-induced acute pancreatitis. Dig Dis Sci. 2020;65(4):1206–1211. doi:10.1007/s10620-019-05827-9
7. Shan Y, Kong W, Zhu A, Zhang J, Ying R, Zhu W. Increased levels of miR-372 correlate with disease progression in patients with hyperlipidemic acute pancreatitis. Exp Ther Med. 2020;19(6):3845–3850. doi:10.3892/etm.2020.8609
8. Yan Z, Zang B, Gong X, et al. MiR-214-3p exacerbates kidney damages and inflammation induced by hyperlipidemic pancreatitis complicated with acute renal injury. Life Sci. 2020;241:117118.
9. Sardana O, Kumari P, Singh R, Chopra H, Emran TB. Health-related quality of life among acute pancreatitis patients correlates with metabolic variables and associated factors. Ann Med Surg. 2022;82:104504. doi:10.1016/j.amsu.2022.104504
10. Tenner S, Baillie J, DeWitt J, Vege SS. American College of Gastroenterology guideline: management of acute pancreatitis. Off J Am Coll Gastroenterol. 2013;108(9):1400–1415. doi:10.1038/ajg.2013.218
11. Ippisch HM, Alfaro-Cruz L, Fei L, Zou Y, Thompson T, Abu-El-Haija M. Hypertriglyceridemia induced pancreatitis inpatient management at a single pediatric institution. Pancreas. 2020;49(3):429–434. doi:10.1097/MPA.0000000000001505
12. Zhang H, Liu F. Predictive nursing versus routine nursing on health status, cancer-related fatigue and psychological state of patients with pancreatic cancer undergoing chemotherapy. J Mod Nurs Pract Res. 2023;3(1):3. doi:10.53964/jmnpr.2023003
13. Zheng Q, Cao L, Ma H, et al. Evidence-based care can improve treatment compliance and quality of life of patients with acute pancreatitis. J Healthc Eng. 2022;2022:1–8. doi:10.1155/2022/7621658
14. Yang W, Ren S, Liang J. Application and effect of high-quality nursing combined with enteral nutrition support in patients with acute pancreatitis. J Mod Nurs Pract Res. 2021;1(1):1. doi:10.53964/jmnpr.2021001
15. Dongying T, Meifeng W, Ling W. Application of nursing collaboration model in nursing of a patient with severe hyperlipidemia pancreatitis. Chin J Nurs. 2018;53(7):3.
16. Wang S, Wu M. Effects of multidisciplinary specialized nursing care on the short and long-term postoperative quality of life in patients with pancreatic cancer: a randomized controlled trial. J Mod Nurs Pract Res. 2023;3(1):2. doi:10.53964/jmnpr.2023002
17. Zhang L, Zhang L, Wang J, Ding F, Zhang S. Community health service center-based cardiac rehabilitation in patients with coronary heart disease: a prospective study. BMC Health Serv Res. 2017;17(1):1–8. doi:10.1186/s12913-017-2036-3
18. Li J, Chen J, Tang W. The consensus of integrative diagnosis and treatment of acute pancreatitis‐2017. J Evid Based Med. 2019;12(1):76–88. doi:10.1111/jebm.12342
19. Gabriel EH, Hoch MC, Cramer RJ. Health belief model scale and theory of planned behavior scale to assess attitudes and perceptions of injury prevention program participation: an exploratory factor analysis. J Sci Med Sport. 2019;22(5):544–549. doi:10.1016/j.jsams.2018.11.004
20. Yue T, Li Q, Wang R, et al. Comparison of Hospital Anxiety and Depression Scale (Hads) and Zung self-rating anxiety/depression scale (SAS/SDS) in evaluating anxiety and depression in patients with psoriatic arthritis. Dermatology. 2020;236(2):170–178. doi:10.1159/000498848
21. Selim A, Rogers W, Qian S, Rothendler JA, Kent EE, Kazis LE. A new algorithm to build bridges between two patient-reported health outcome instruments: the MOS SF-36® and the VR-12 Health Survey. Qual Life Res. 2018;27(8):2195–2206. doi:10.1007/s11136-018-1850-3
22. Sun Y, Liu Y, Xue B, Wang X, Yu W. Upregulated IRF9 promotes cell apoptosis of hyperlipidemia acute pancreatitis with heart injury by regulating SIRT1. Biocell. 2021;45(1):129. doi:10.32604/biocell.2021.013275
23. Shirolkar A, Yadav A, Mandal TK, Dabur R. Intervention of Ayurvedic drug Tinospora cordifolia attenuates the metabolic alterations in hypertriglyceridemia: a pilot clinical trial. J Diabetes Metab Disord. 2020;19(2):1367–1379. doi:10.1007/s40200-020-00657-3
24. Huang JH, He D, Chen L, et al. GC-MS based metabolomics strategy to distinguish three types of acute pancreatitis. Pancreatology. 2019;19(5):630–637. doi:10.1016/j.pan.2019.05.456
25. Shih HJ, Tsai PS, Wen YC, Kao MC, Fan YC, Huang CJ. Hyperlipidemia patients with long-term statin treatment are associated with a reduced risk of progression of benign prostatic enlargement. Aging Male. 2018;23(5):354–361. doi:10.1080/13685538.2018.1487392
26. Parhofer KG, Laufs U. The diagnosis and treatment of hypertriglyceridemia. Dtsch Arztebl Int. 2019;116(49):825. doi:10.3238/arztebl.2019.0825
27. Fletcher GS. Clinical Epidemiology: The Essentials. Lippincott Williams & Wilkins; 2019.
28. Dong X, Tsang CC, Zhao S, et al. Effects of the Medicare Part D comprehensive medication review on medication adherence among patients with Alzheimer’s disease. Curr Med Res Opin. 2021;37(9):1581–1588. doi:10.1080/03007995.2021.1935224
29. Cong T. Application Research of Internet + “Three-Element Linkage” Management Model of Chronic Hypertension in Hypertension; 2019. Nanjing University of Traditional Chinese Medicine.
30. Pang J, Sullivan DR, Brett T, Kostner KM, Hare DL, Watts GF. Familial hypercholesterolaemia in 2020: a leading tier 1 genomic application. Heart Lung Circ. 2020;29(4):619–633. doi:10.1016/j.hlc.2019.12.002
31. Zhihong Y, Mengjuan L, Yanyan C. Effect of hospital-community-family ternary nursing model combined with continuous nursing on the treatment of patients with coronary heart disease with isosorbide mononitrate. Clin Res. 2021;29(09):165–167.
32. Wei W, Xin Z, Yue L, et al. Application of hospital-community-family ternary nursing model in home care of patients with pressure injury. Chin J Mod Nurs. 2022;28(04):442–446.
33. Chen J, Xiao H, Chen Y, Sun H, Chen S, Zheng J. Effect of reminiscence therapy based on positive psychology theory (RTBPPT) on the positive feelings of the spousal caregivers of elderly patients with advanced cancer in China. Eur J Cancer Care. 2020;29(6):e13324. doi:10.1111/ecc.13324
34. Honghong H, Biyu W, Lanlan C. Development and application analysis of hospital-community-family ternary nursing platform. China Health Stand Manage. 2021;12(16):134–136.
35. Qinghua H, Aiying H. Analysis of the application effect of hospital-community-family ternary linkage nursing model in elderly patients with type 2 diabetes. General Nurs. 2021;19(21):2909–2911.
36. Hestevik CH, Molin M, Debesay J, Bergland A, Bye A. Older persons’ experiences of adapting to daily life at home after hospital discharge: a qualitative metasummary. BMC Health Serv Res. 2019;19(1):1–3. doi:10.1186/s12913-019-4035-z
37. Chan AH, Horne R, Hankins M, Chisari C. The medication adherence report scale: a measurement tool for eliciting patients’ reports of nonadherence. Br J Clin Pharmacol. 2020;86(7):1281–1288. doi:10.1111/bcp.14193
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.