")
Back to Journals » OncoTargets and Therapy » Volume 16
Clinical Utility of Mobocertinib in the Treatment of NSCLC – Patient Selection and Reported Outcomes
Received 24 March 2023
Accepted for publication 19 June 2023
Published 11 July 2023 Volume 2023:16 Pages 559—569
DOI https://doi.org/10.2147/OTT.S374489
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Abram Arnold,1 Apar Kishor Ganti2
1Department of Medicine, Veterans Affairs Nebraska-Western Iowa Health Care System, Omaha, NE, USA; 2Division of Oncology/Hematology, Department of Internal Medicine, Veterans Affairs Nebraska-Western Iowa Health Care System and University of Nebraska Medical Center, Omaha, NE, USA
Correspondence: Apar Kishor Ganti, 986840 Nebraska Medical Center, Omaha, NE, 68198, USA, Tel +1 402 559-5622, Email [email protected]
Abstract: Mobocertinib is an oral tyrosine kinase inhibitor (TKI) that selectively targets epidermal growth factor receptor exon 20 insertion (EGFRex20ins) mutations. It is a structural analog of the third-generation TKI osimertinib, which targets EGFR T790M mutant non-small cell lung cancer (NSCLC); however, mobocertinib gains selectivity for EGFRex20ins mutants over wild type (WT) by interacting with the C790 gatekeeper residue of EGFR. This is accomplished via a carboxylated isopropyl ester moiety at the C5-position of mobocertinib’s central pyrimidine core. In Phase 1/2 dose-escalation and dose-expansion studies, mobocertinib was found to have an investigator-confirmed overall response rate (ORR) of 56% (9/16; 95% CI: 30– 80%) and 25% (3/12; 95% CI: 5– 57%) in patients without and with baseline brain metastasis, respectively. Median investigator-assessed progression-free survival (mPFS) was 10.2 months (95% CI: 5.6 – not reached) and 3.7 months (95% CI: 1.8– 15.9) in patients without and with baseline brain metastasis, respectively. A third phase evaluated patients who had received pre-treatment with platinum-based chemotherapy (PPP) and included an extension cohort (EXCLAIM cohort) which evaluated patients treated previously with 1 or 2 lines of therapy. An Independent Review Committee (IRC) found both cohorts to have similar outcomes in terms of ORR, median time to response, mPFS, and disease progression or death. The treatment-emergent adverse events (TEAE) related to mobocertinib are similar to other EGFR inhibitors and are predominately gastrointestinal (eg diarrhea, nausea, vomiting) and cutaneous (eg rash). In September 2021, the FDA granted accelerated approval for mobocertinib in the treatment of patients with locally advanced or metastatic NSCLC with EGFRex20ins mutation whose disease progressed while on platinum-based chemotherapy. The present review describes data that led to the approval of mobocertinib.
Keywords: mobocertinib, exon 20 insertion of EGFR, NSCLC, TKI
Introduction
Non-small cell lung cancer (NSCLC) accounts for the vast majority of all lung cancers and can be further categorized by histologic subtype.1 These subtypes have recently been revised and include adenocarcinoma, squamous cell carcinoma, neuroendocrine tumors, adenosquamous carcinoma, large cell carcinoma, sarcomatoid carcinoma, and unclassified carcinoma.2 Of these subtypes, adenocarcinoma is the most common. Adenocarcinomas are further identified by driver mutations that result in neoplastic growth and may also serve as therapeutic targets. Kirsten rat sarcoma viral oncogene homolog (K-Ras) and epidermal growth factor receptor (EGFR) mutations are the most commonly identified driver mutations, with the latter occurring in 20% of patients diagnosed with lung adenocarcinoma.2
EGFR is an oncogenic transmembrane glycoprotein that, when activated, leads to intracellular tyrosine kinase activity defined by regulation of cellular proliferation, angiogenesis, and eventual apoptosis.3,4 The tyrosine kinase domain is made up of an N-terminal and a C-terminal lobe with an active site cleft in-between. The active site cleft is characterized by several key features including a “hinge” region (M793), a phosphate-binding loop (P-loop), a “gatekeeper” residue (T790), an activation loop (A-loop), a C-helix involved in kinase activation, and an exposed cysteine (C797).5 Under physiologic conditions, epidermal growth factor (EGF) binds to EGFR resulting in dimerization of the C-lobe of one monomer to the N-lobe of another.5
EGFR activating mutations are most prevalent within the first four exons (18–21) of the EGFR tyrosine kinase domain.6 Point mutations, such as the L858R substitution of exon 21, and in-frame deletion mutations in exon 19 account for up to 45% and up to 50%, respectively, of EGFR-activating mutations. These mutations are of particular interest as they lead to activation of the signaling pathway resulting in accelerated cell proliferation and angiogenesis while avoiding apoptosis and can be targeted using tyrosine kinase-inhibitors (TKI).6–9
Insertion mutations in exon 20 (EGFRex20ins) are driver mutations that are seen in up to 12% of EGFR-mutant NSCLCs.9 These mutations too result in the upregulation of EGFR kinase activity. Mutation-specific alterations in EGFR kinase domain’s “gatekeeper” residue confer resistance to first- and second-generation EGFR TKIs, including when used in combination.9–11 Structural modeling of EGFRex20ins mutants reveals considerable similarity to active WT EGFR resulting from in-frame insertion of amino acids at the C-terminal of the C-helix.6 Furthermore, the ATP-binding site of EGFRex20ins mutants is essentially unchanged from WT.5 This close resemblance creates a challenge in the development of TKIs that target mutant over WT.6
Clinical Implications of EGFR Exon 20 Insertion Mutations
Prior to the introduction of therapies that specifically target NSCLC with EGFRex20ins mutations, patients were treated with regimens intended for other EGFR mutations, albeit with varying results. First- and second-generation TKIs yielded ORR <30% and PFS of approximately 3 months. These parameters were slightly improved with the use of platinum-based chemotherapy.12
For long, platinum-based chemotherapy regimens have been utilized as first-line treatment for patients with EGFR exon 20 insertion mutations; however, the efficacy of these regimens is not optimal. Retrospective studies indicate an ORR between 19.0% and 19.2%, mPFS of 6.4–7.6 months, and mOS of 19.9 months.10 Monotherapy with docetaxel as a second-line agent following platinum failure provided little benefit (ORR 14%; mPFS 3.0 months) which was marginally improved when used in combination with the vascular endothelial receptor-2 antagonist, ramucirumab (ORR 23%; mPFS 4.5 months).12
With the less than favorable outcomes associated with use of first- and second-generation EGFR-TKIs and platinum-based chemotherapy regimens, further investigations into the efficacy of other therapies have been undertaken. The third-generation TKI poziotinib showed promising results during in vitro testing; however, ORR was only 15–19% with mPFS of 4–6 months. Osimertinib, a third-generation irreversible TKI approved for EGFR T790M-positive NSCLC, has demonstrated some activity against EGFRex20ins mutants and is associated with an improved ORR (25%) and mPFS (9.7 months) when used as second-line therapy at higher than approved doses (160mg).12 However, there remains a need for additional therapies that target NSCLC characterized by EGFRex20ins mutations.5 One such therapy is an oral TKI, mobocertinib (TAK-788), which was designed specifically to treat patients with EGFRexon20ins mutation positive NSCLC.6,10
Development of Mobocertinib
The development of a therapy that targets EGFRex20ins mutations required investigation into the structural properties inherent to these mutations. To this end, biochemical assays against double-mutant (T790M/L858R) and WT EGFR led to the identification of a pyrimidine ring as a key feature that allows selectivity for T790M over WT protein.5 These assays evaluated a variety of features from a library of compounds which included the position of the α,β-unsaturated acrylamide group and its importance in the modulation of thiol reactivity. Acrylamide, a reactive electrophile, ideally will have low thiol reactivity in order to initially form a reversible bond with the EGFR mutant target prior to covalent modification of the C797 residue. This low reactivity allows for proper orientation in binding and results in reduced off-target reactions with a resultant decrease in adverse events. These favorable properties were previously observed in osimertinib’s interaction with EGFR double mutants and the M793 hinge residue. From these assays, a structure was identified for its cellular potency in terms of half-maximal inhibitory concentration (IC50) and high selectivity against double mutant cells over WT. Furthermore, this molecule resulted in tumor growth suppression in mouse models.5
This molecule underwent further structural optimization to what would become mobocertinib. One modification, which was already utilized by osimertinib and identified to improve cellular potency, was the incorporation of N,N,N’-trimethylethylenediamine at the C4-position of the aniline ring. This modification improved flexibility and optimized interaction at the C797 binding site. Compared to osimertinib, mobocertinib differs by the presence of a carboxylated isopropyl ester moiety at the C5-position of the central pyrimidine core. Docking studies of the EGFRex20ins NPG mutant found that this modification facilitated an interaction with a selectivity pocket adjacent to T790 (gatekeeper residue) that was not occupied by osimertinib. This interaction accounts for the difference in affinity and selectivity of mobocertinib over osimertinib in EGFRex20ins mutants with and without T790M.5,6 Further assays were utilized to demonstrate the superior affinity of mobocertinib for mutant over WT.6
Mechanism of Action
Mobocertinib is an oral TKI that selectively targets EGFR and HER2 exon 20 insertion mutations. While the role of HER2 exon 20 insertion mutations in NSCLC is unclear, their presence accounts for a significant portion (90%) of HER2 mutation in NSCLC.13 For the purposes of this review, the focus will be on EGFR mutations.
Mobocertinib’s affinity for EGFRex20ins mutations is accomplished through a combination of interactions at the EGFR binding site. This includes the formation of an irreversible covalent bond with the cysteine 797 residue in EGFR.4,8,11 Additionally, the C5-carboxylate isopropyl ester moiety on mobocertinib’s middle pyrimidine ring interacts with the C790 gatekeeper residue in the ATP binding pocket of EGFR, therefore selectively targeting EGFRex20ins oncogenic variants.5,6,10
The result of mobocertinib’s affinity for EGFRex20ins portends significant inhibition against various mutants with IC50 values 1.5 to 8-fold less compared to WT (IC50 4.3 to 22.5nM vs 34.5nM, respectively).5 In preclinical studies, selectivity for potent inhibition of mutant over WT EGFR was found in all variants containing common activating mutations with or without T790M resistance mutations (D, L, DT, and LT), all uncommon activating mutations (G719A, G719S, S768I, L861Q, and L861R), and all variants containing EGFRex20ins mutations (FQEA, NPG, ASV, NPH, and SVD). Due to its highly selective nature, mobocertinib is postulated to reduce the risk for dose-limiting toxicities compared to other drugs which are less selective towards mutant EGFR.6
The activity of mobocertinib was evaluated in patient-derived cell lines, CUTO14 and LU0837 from lung adenocarcinoma containing EGFRex20ins ASV mutations and NPH mutations, respectively. Analysis indicated that mobocertinib inhibited phosphorylation, and therefore EGFR signaling in CUTO14 cells more effectively than osimertinib at similar concentrations of 100nm/L and 1000nmol/L (80 and 100% vs 38 and 63%, respectively). Additionally, mobocertinib greatly reduced the viability of CUTO14 cells relative to osimertinib, erlotinib, gefitinib, and afatinib. Furthermore, mobocertinib was found to be more effective than erlotinib, gefitinib, and osimertinib regarding inhibition of LU0387 cell viability.6
Pharmacokinetics
Mobocertinib when administered orally achieves peak concentration in plasma in 4 hours with a mean absolute bioavailability of 37% and a volume of distribution of 3509L.5 Metabolic activity of CYP3A4/5 results in oxidative N-demethylation and production of AP32914 and AP32960 which are active metabolites against EGFRex20ins mutants with IC50 of 2.4–14nM and 7.1–41nM, respectively. Finally, mobocertinib’s mean elimination half-life is 18 hours and is predominately eliminated in feces.5,6
Metabolization of mobocertinib by CYP3A4 presents a concern when used concurrently with moderate to strong CYP3A4 inhibitors and inducers. Concurrent use of inhibitors may increase mobocertinib concentration and subsequently possible toxicities. Conversely, concurrent use of inducers may decrease mobocertinib concentration and efficacy.13 Consequently, patients who had received moderate to strong CYP3A inhibitors or inducer within 10 days of enrollment were excluded from early phase clinical trials.14 Furthermore, a black box warning has been issued for concurrent use of mobocertinib in patients on moderate to strong CYP3A inhibitors or inducers.15
Early Clinical Trials
In June 2016, Riely et al initiated an open-label, multicenter, non-randomized phase 1/2 dose-escalation and expansion trial which assessed the efficacy and tolerability of mobocertinib in patients with metastatic NSCLC defined by a EGFRex20ins mutation. The escalation study concluded that mobocertinib has a maximum tolerated dose (MTD) of 160mg/day that was subsequently defined as the Recommended Phase 2 Dose (RP2D). The expansion phase enrolled 7 cohorts based on their histologic and molecular features for evaluation of efficacy at varying daily doses (5–40mg/day, 80mg/day, 120mg/day, and 160mg/day) and evaluation of safety at RP2D.12
The results of this phase 1/2 dose-escalation/expansion phase study are shown in Table 1. Mobocertinib demonstrated an ORR of 43% (12/28; 95% confidence interval [CI]: 24–63%), a median duration of response (mDOR) of 13.9 months (95% CI: 5.0 – not reached), and a mPFS of 7.3 months (95% CI: 4.4–15.6). Additionally, investigator-confirmed ORR was 56% (9/16; 95% CI: 30–80%) and 25% (3/12; 95% CI: 5–57%) in patient without and with baseline brain metastasis, respectively. Similarly, mDOR was assessed in confirmed responders without and with baseline brain metastasis and was found to be 13.8 months (95% CI: 5.0–16.6) and 5.5 months (95% CI: 3.0–1.42), respectively. Investigator-assessed mPFS was 10.2 months (95% CI: 5.6 – not reached) in patient without baseline brain metastasis and 3.7 months (95% CI: 1.8–15.9) in patient with baseline brain metastasis. Thus, mobocertinib demonstrated limited intracranial activity.12
 |
Table 1 Anti-Tumor Activity of Mobocertinib (160mg/Day) in EGFRex20ins Mutation Positive NSCLC Cohorts |
EXCLAIM Cohort
Following the encouraging results described by Riely et al, a single-arm extension cohort (EXCLAIM) included patients treated previously with 1 or 2 lines of therapy from 40 sites (Asia, North America, and Europe).14
Inclusion and exclusion criteria for the EXCLAIM cohort were similar to the phase 1/2-dose escalation/expansion study. Patients were still considered if they had previously received EGFR-TKI treatment unless they had an objective response followed by disease progression on TKI therapy. Patients with brain metastases were included in the EXCLAIM cohort if these were previously treated and had documented stability.14 In this cohort (n = 96), Independent Review Committee (IRC) ORR was 25% (95% CI 17–35%), the median time to response was 1.9 months (95% CI 1.8–3.6), while the mDOR was non-estimable. Median PFS was 7.3 months (95% CI 5.5–9.1) (Table 1). The brain was the first site of progression in 38% of cohort. Median OS was not achieved in this cohort at the time of reporting.14
In another analysis, 114 patients with EGFRex20ins mutation-positive NSCLC who had previously received platinum (platinum pre-treated patients [PPP]) were evaluated. This cohort included 6 patients from the dose-escalation cohort, 22 from the dose-expansion cohort, and 86 patients from the aforementioned EXCLAIM cohort.14 In the PPP cohort, the IRC ORR was 28% (95% CI: 20–37%), disease control rate (DCR) was 78% (95% CI: 69–85%), median time to response was 1.9 months (95% CI: 1.8–3.6), and mDOR was 17.5 months (95% CI: 7.4–20.3). The PPP cohort had a mPFS of 7.3 months (95% CI: 5.5–9.2), while the mOS was 24.0 months (95% CI: 14.6–28.8) (Table 1). Treatment was reportedly associated with improvement of symptoms related to underlying lung cancer (eg cough, dyspnea, shortness of breath) as well as stability in Global Health Status and quality of life (QOL) scores.14
Ongoing Clinical Trials
Currently, a Phase 3, open-label, multi-center (United States, Europe, and Asia) clinical trial (EXCLAIM-2) is enrolling patients with locally advance, recurrent, or metastatic EGFRex20ins-positive NSCLC who have not previously received treatment. This study compares mobocertinib with platinum-based chemotherapy regimens (intravenous pemetrexed/cisplatin or pemetrexed/carboplatin) as first-line therapy. The primary outcome measure of this trial is IRC assessed PFS (Table 2). 12,16
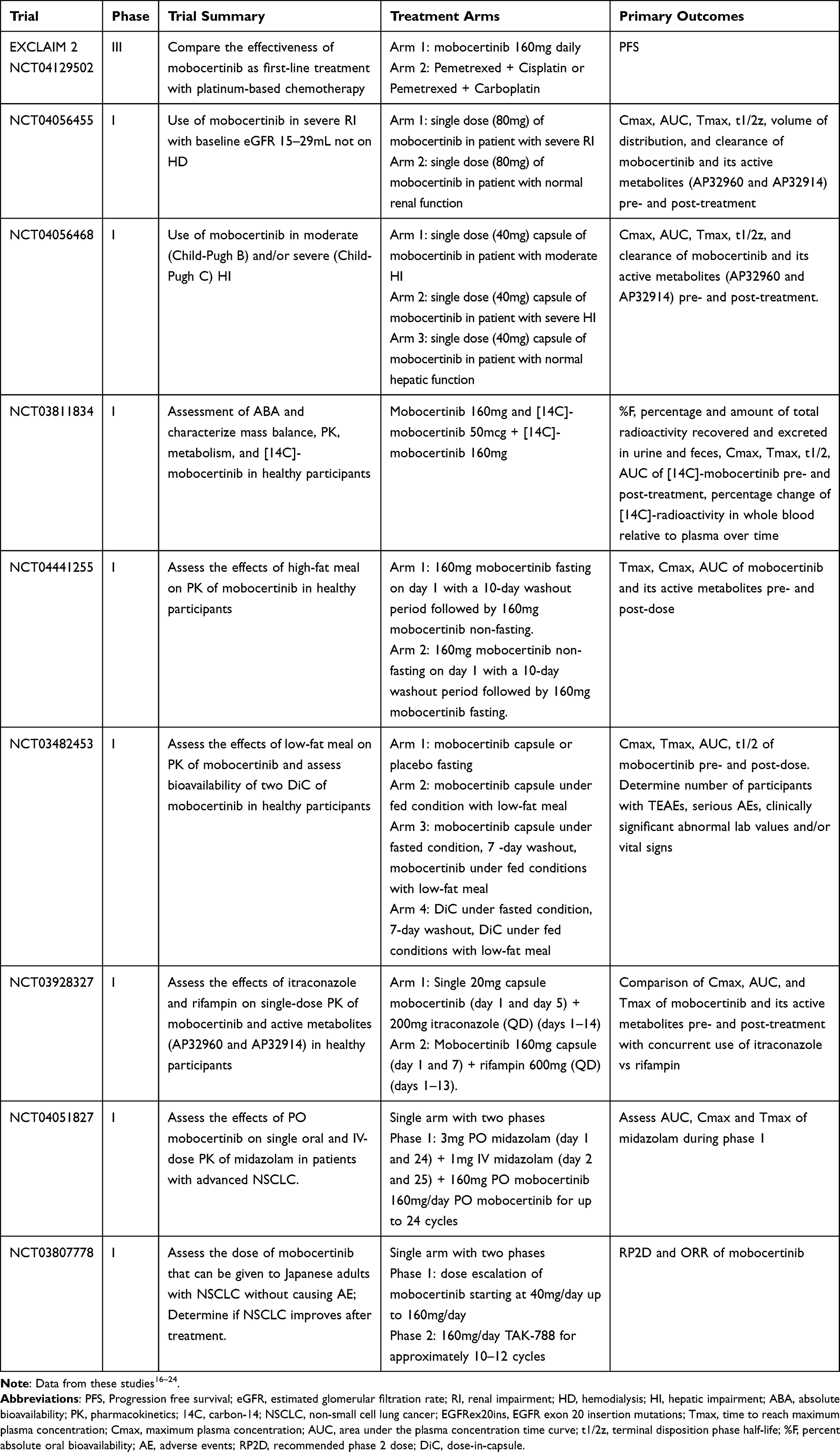 |
Table 2 Mobocertinib Prior and Ongoing Clinical Trials |
Notable Phase I clinical trials include those evaluating the pharmacokinetics of mobocertinib and its active metabolites in the setting of severe renal insufficiency (NCT04056455), moderate and/or severe hepatic impairment (NCT04056468), following high-fat (NCT04441255) or low-fat (NCT03482453) meal, and with concurrent use of itraconazole or rifampin (NCT03928327) or midazolam (NCT04051827) (Table 2).16–24
Indications for Mobocertinib
The US Food and Drug Administration (FDA) granted Breakthrough Therapy Designation for mobocertinib in April 2020 in light of the ORR and long-term benefits seen in the initial clinical trials.12 On September 15, 2021, the FDA granted accelerated approval of mobocertinib for treatment of patients with locally advanced or metastatic NSCLC with EGFRex20ins mutation that has progressed despite treatment with platinum-based chemotherapy.25
Safety of Mobocertinib
The safety of mobocertinib was addressed during the phase 1/2 trial.12 During the dose-escalation phase, no dose-limiting toxicities (DLT) occurred at doses between 5 and 40mg/day. The most common DLT described was pneumonitis. Grade 3 and 5 pneumonitis each occurred in 1 of 7 evaluable patients at a dose of 80mg/day and 120mg/day, respectively. Other DLTs included grade 3 mucositis occurring in 1 of 6 patients at a dose of 160mg/day, while grade 3 diarrhea was documented in 2 of 4 patients at a dose of 180mg/day and resulted in missing >25% of planned doses.12
In the dose-expansion phase, mobocertinib at RP2D resulted in treatment-emergent adverse events (TEAE) in 134 of 136 (99%) patients with 131 (96%) attributed directly to treatment with mobocertinib. The most prevalent TEAEs were diarrhea (113/136; 83%), nausea (58/136; 43%), vomiting (36/136; 26%), and rash (45/136; 33%). Other common TEAEs included decrease appetite (29/136; 21%), stomatitis (28/136; 21%), dry skin (30/136; 22%), fatigue (28/136; 21%), and paronychia (22/136; 16%). Grade ≥3 treatment-related TEAEs were documented in 54 of 136 (40%) patients with diarrhea being the most common (28/136; 21%). Treatment-related TEAEs resulting in dose-interruption occurred in 74 (54%) patients with 23 (17%) patients requiring dose-reduction, and 22 (22%) requiring complete discontinuation. Results were similar in patients with EGFRex20ins mutation NSCLC compared with all patients treated with mobocertinib at 160mg/day.12
In the EXCLAIM and PPP cohorts, the most common AEs were diarrhea (≈90%) and rash (45%). AEs leading to treatment discontinuation were seen in 19 of 114 (17%) and 10 of 96 (10%) of patients in the PPP and EXCLAIM cohort, respectively. Adverse events necessitating dose reduction occurred in 29 of 114 (25%) and 21 of 96 (22%) patients, respectively.14
Mobocertinib was also found to be less commonly associated with cardiac, pulmonary, and fetal-embryo toxicities. Specific cardiotoxicities included QTc prolongation that was found to be concentration dependent. At the RP2D (160mg/day), the mean increase of QTc above prior baseline was 23.0 msec. As a result, patients with prolonged QTc (males [≥450ms]; females [≥470ms]) were excluded from phase 1/2 studies. Additionally, QTc monitoring while on therapy was deemed necessary and a black box warning has been issued for QTc prolongation and increased risk of torsades de pointes.13–15 Additionally, heart failure was documented in 2.7% of evaluated patients, while pulmonary toxicities, including interstitial lung disease (ILD) or pneumonitis, occurred in 4.3% of evaluated patients.5,26
Real-World Efficacy and Safety
Furthering the results from the EXCLAIM study, Kian et al conducted a retrospective, non-interventional, multicentered study evaluating the efficacy and safety of mobocertinib in patients with locally advanced or metastatic EGFRex20ins mutation NSCLC (n = 16). The study population was similar to the PPP cohort of EXCLAIM study; however, it also included patients receiving mobocertinib as first-line treatment (5/16) as part of the compassionate use program (CUP) who were otherwise not suitable candidates for chemotherapy.4
Results from this retrospective study indicate similar efficacy in terms of ORR (25%) and DCR (75%) when compared to the PPP cohort of the EXCLAIM study. Progressive disease (PD) occurred in 4 of 16 patients who were non-responders, while stable disease (SD) was found in 8 of 16. The median duration of treatment (mDoT) was 5.6 months; however, it was longer (8.6 months) in responders. Of note, there was no difference in mDoT when mobocertinib was used as first-line (ie CUP) compared to second-line treatment. Additionally, treatment related adverse events (TRAEs) were similar to those in the PPP cohort of the EXCLAIM study.4
Comparison to Amivantamab
An alternative option for the treatment of patients with EGFRex20ins mutation-positive NSCLC is the bispecific human anti-MET proto-oncogene IgG antibody amivantamab (JNJ-61186372).5 Like mobocertinib, amivantamab demonstrates activity against exon 20 mutations as well as exon 19 and exon 21 mutations.13
Amivantamab received accelerated approval from the FDA in May 2021 for patients with EGFRex20ins positive NSCLC who had progressed on treatment with platinum-based chemotherapy. In the CHRYSALIS trial (Phase I/IB), an intravenous infusion of amivantamab was used in patients pre-treated with platinum-based chemotherapy with results indicating ORR of 40% (95% CI: 29, 51), mDOR of 11.1 months (95% CI: 6.9, not reached), and mPFS of 8.3 months (95% CI: 6.5, 10.9).27,28 The most common AEs documented in the CHRYSALIS trial were rash (86%), infusion reaction (66%), paronychia (45%), stomatitis (21%), pruritis (17%), and diarrhea (12%). Grade ≥3 AEs occurred in 35% of patients with treatment-related AE occurring in 16% of patients. The most commonly observed grade ≥3 AE was hypokalemia (5%), while rash, pulmonary embolism, diarrhea, and neutropenia were equally represented (4% each). Additionally, MET inhibition associated AEs included hypoalbuminemia (27%) and peripheral edema (21%).28
The CHRYSALIS trial evaluating amivantamab and phase 1/2 dose-escalation/expansion and subsequent extension trials of mobocertinib included patients with ECOG ≤1 with advanced or metastatic disease and absence of active brain lesions. All patients in the CHRYSALIS cohort had previously received treatment with platinum-based chemotherapy, while the mobocertinib trial was divided into two cohorts – the platinum pretreatment patient group (PPP) and the extension arm (EXCLAIM cohort). The latter had received prior treatment (eg platinum-based chemotherapy, immunotherapy, EGFR TKI) for EGFRex20ins mutation positive NSCLC, however not exclusively platinum-based chemotherapy. In the cohorts of both amivantamab and mobocertinib who had received prior platinum-based chemotherapy, patient demographics were similar (Table 3) in terms of median age (62 vs 60 years old respectively), proportion of female participants (59% vs 66% respectively), and history of previously treated and/or stable brain lesions (22% vs 35% respectively).13
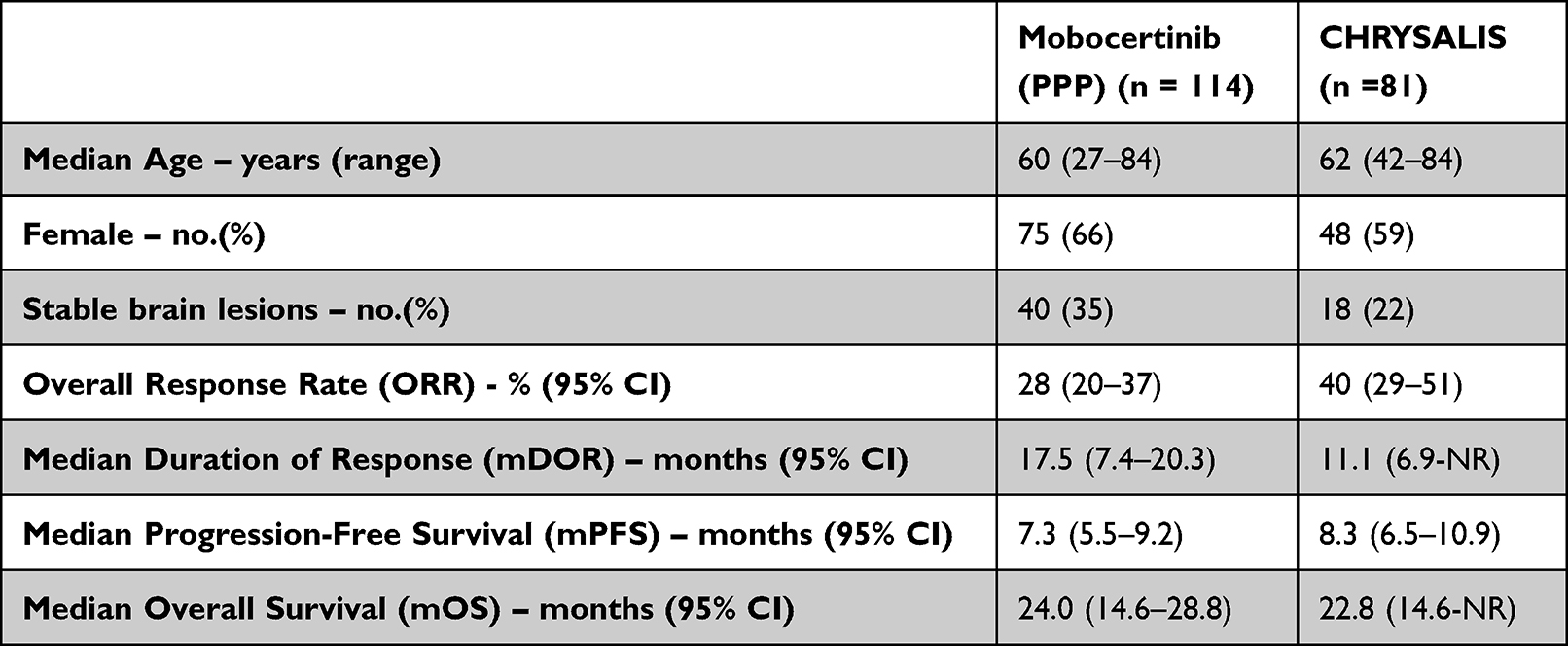 |
Table 3 Efficacy Data for Mobocertinib and Amivantamab Treatment of EGFRex20ins Mutation NSCLC Patients Previously Treated with Platinum-Based Chemotherapy |
The overall efficacy of amivantamab and mobocertinib in terms of ORR, mDOR, mPFS, and mOS is outlined in Table 3. Ultimately, there is no head-to-head study including amivantamab and mobocertinib; therefore, it is difficult to compare these two therapies.13
In terms of safety profiles of amivantamab and mobocertinib, they are qualitatively similar and related to the class effect of EGFR inhibition. However, rash seemed to be more common with amivantamab (86% vs 45% respectively), while diarrhea was less common (12% vs 91%). Additionally, amivantamab is administered intravenously and is associated with infusion reactions (chill, nausea, vomiting, hypotension, dyspnea).13
Both mobocertinib and amivantamab yield improved response rates in patients with EGFRex20ins mutant NSCLC who have previously received treatment with platinum-based chemotherapy.13 The decision to use one of these agents over the other will likely involve shared decision-making between patient and provider and be based on patient’s baseline characteristics and comorbidities, tolerability of AEs, and the preferred route of administration.
Comparison to Other Available Treatments
There are no head-to-head comparisons between mobocertinib and other available treatments for this patient cohort. Indirect comparison of other agents to mobocertinib was performed by Christopoulos et al, who evaluated patients with EGFRex20ins mutated NSCLC who received other available therapies including EGFR TKI, PD-(L)1 inhibitors, chemoimmunotherapy, and single-agent chemotherapy. Real-world data (RWD) regarding effectiveness of these therapies was obtained from a retrospective, observational study evaluating platinum-pretreated patients with advanced EGFRex20ins positive NSCLC.29,30 Patient selection for RWD cohort (n = 43) included those who met the inclusion criteria for the mobocertinib phase I/II study (n = 114) with inverse probability of treatment weighting (IPTW) utilized to further minimize differences in baseline characteristics.29
This indirect comparison found that the cohort treated with mobocertinib had better outcomes than those from the RWD cohort. Confirmed ORR in the mobocertinib cohort was 35.1% (95% CI, 26.4–44.6), while there was no confirmed response to index line of treatment in the RWD cohort (p < 0.0001). Similarly, mobocertinib prolonged mOS (20.2 vs 11.3 months; 95% CI, 0.32–0.76, p < 0.001), mPFS (7.3 vs 3.0 months; 95% CI, 0.22–0.51, p < 0.0001), and median time to death (mTTD) (7.4 vs 2.3 months; 95% CI, 0.23–0.53, p < 0.0001) compared to non-weighted RWD cohort, respectively. Following IPTW of RWD cohort, the mobocertinib cohort had persistently better outcomes with mOS (20.2 vs 9.8 months; 95% CI, 0.25–0.69, p = 0.0035), mPFS (7.3 vs 2.6 months; 95% CI, 0.18–0.44, p < 0.0001), and mTTD (7.4 vs 2.1 months; 95% CI, 0.18–0.65, p = 0.0004), respectively.29
Limitation and Future Direction of EGFR Exon-20 Inhibitors
Resistance and disease progression in patients treated with mobocertinib has been documented in the presence of C797S mutations (EGFR L858R/C797S and T790M/C797S) as well as triple mutants (L858R + T790M + C797S). The proposed mechanism for resistance is a mutation at the EGFR C797S binding site that results in loss of interaction between acrylamide group on mobocertinib at binding site.5,6,31
Conclusions
Mobocertinib is an oral TKI that targets EGFR exon 20 insertion mutations in NSCLC and has demonstrated promising results in phase 1 and 2 clinical trials evaluating patients previously treated with systemic therapy for locally advanced or metastatic disease (Figure 1). The efficacy of mobocertinib in EGFRex20ins positive NSCLC results from the C5-carboxylate isopropyl ester moiety on its middle pyrimidine ring which interacts with the C790 gatekeeper residue in the ATP binding pocket of mutant EGFR.
 |
Figure 1 Infographics depicting the key features of mobocertinib. |
Alternatively, the intravenous bispecific human anti-MET proto-oncogene IgG antibody amivantamab also targets EGFRex20ins mutant NSCLC. Although a head-to-head study comparing mobocertinib to amivantamab does not yet exist and is unlikely to be performed, these two agents have similar efficacy, but different pharmacokinetics and side effect profiles.
Finally, a Phase III clinical trial, EXCLAIM-2, is currently underway evaluating the use of mobocertinib in the treatment of patients with EGFRex20ins mutated NSCLC who have not received any prior therapy.
Disclosure
Abram Arnold – None
Apar Kishor Ganti – Consultant: Genentech, AstraZeneca, G1 Therapeutics, Jazz Pharmaceuticals, Flagship Biosciences, Sanofi-Genzyme, Regeneron; Research Support: Takeda; DSMC: Y-mAbs Therapeutics; Personal fees: Blueprint Medicines, Cardinal Health, Beigene Ltd, Mirati.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. doi:10.3322/caac.21763
2. Rodak O, Peris-Díaz MD, Olbromski M, Podhorska-Okołów M, Dzięgiel P. Current landscape of non-small cell lung cancer: epidemiology, histological classification, targeted therapies, and immunotherapy. Cancers. 2021;13(18):4705. doi:10.3390/cancers13184705
3. Herbst RS. Review of epidermal growth factor receptor biology. Int J Radiat Oncol Biol Phys. 2004;59(2 Suppl):S21–6. doi:10.1016/J.IJROBP.2003.11.041
4. Kian W, Christopoulos P, Remilah AA, et al. Real-world efficacy and safety of mobocertinib in EGFR exon 20 insertion-mutated lung cancer. Front Oncol. 2022;12:1010311. doi:10.3389/fonc.2022.1010311
5. Wang J, Lam D, Yang J, Hu L. Discovery of mobocertinib, a new irreversible tyrosine kinase inhibitor indicated for the treatment of non-small-cell lung cancer harboring EGFR exon 20 insertion mutations. Med Chem Res. 2022;31(10):1647–1662. doi:10.1007/s00044-022-02952-5
6. Gonzalvez F, Vincent S, Baker T, et al. Mobocertinib (TAK-788): a Targeted Inhibitor of EGFR Exon 20 Insertion Mutants in Non–Small Cell Lung Cancer. Cancer Discov. 2021;11(7):1672–1687. doi:10.1158/2159-8290.CD-20-1683
7. Sequist L, Bell D, Lynch T, Haber D. Molecular predictors of response to epidermal growth factor receptor antagonists in non–small-cell lung cancer. J Clin Oncol. 2007;25(5):587–595. doi:10.1200/JCO.2006.07.3585
8. Kuhri FR. Lung Cancer and Other Pulmonary Neoplasms. In: Goldman L, Schafer A, editors. Goldman-Cecil Medicine.
9. Riess JW, Gandara DR, Frampton GM, et al. Diverse EGFR Exon 20 Insertions and Co-Occurring Molecular Alterations Identified by Comprehensive Genomic Profiling of NSCLC. J Thorac Oncol. 2018;13(10):1560–1568. doi:10.1016/j.jtho.2018.06.019
10. Hou J, Li H, Ma S, et al. EGFR exon 20 insertion mutations in advanced non-small-cell lung cancer: current status and perspectives. Biomark Res. 2022;10(1):21. doi:10.1186/s40364-022-00372-6
11. Sharma S, Bell D, Settleman J, et al. Epidermal growth factor receptor mutations in lung cancer. Nat Rev Cancer. 2007;7(3):169–181. doi:10.1038/nrc2088
12. Riely GJ, Neal JW, Camidge DR, et al. Activity and Safety of Mobocertinib (TAK-788) in Previously Treated Non-Small Cell Lung Cancer with EGFR Exon 20 Insertion Mutations from a Phase I/II Trial. Cancer Discov. 2021;11(7):1688–1699. doi:10.1158/2159-8290.CD-20-1598
13. Russell MC, Garelli AM, Reeves DJ. Targeting EGFR Exon 20 Insertion Mutation in Non–small cell Lung Cancer: amivantamab and Mobocertinib. Ann Pharmacother. 2023;57(2):198–206. doi:10.1177/10600280221098398
14. Zhou C, Ramalingam SS, Kim TM, et al. Treatment Outcomes and Safety of Mobocertinib in Platinum-Pretreated Patients With EGFR Exon 20 Insertion-Positive Metastatic Non-Small Cell Lung Cancer: a Phase 1/2 Open-label Nonrandomized Clinical Trial. JAMA Oncol. 2021;7(12):e214761. doi:10.1001/jamaoncol.2021.4761
15. Takeda Pharmaceuticals America Inc. Exkivity (Mobocertinib) [Package Insert]. Lexington, MA: Takeda Pharmaceuticals America Inc; 2021.
16. TAK-788 as First-Line Treatment Versus Platinum-Based Chemotherapy for Non-Small Cell Lung Cancer (NSCLC) With EGFR Exon 20 Insertion Mutations. ClinicalTrials.gov identifier: NCT04129502. Available from: https://clinicaltrials.gov/ct2/show/NCT04129502?term=tak-788&draw=2&rank=8.
17. A Study of Mobocertinib Capsules in People With Severe Kidney Problems and People With Healthy Kidneys. ClinicalTrials.gov Identifier: NCT04056455. Available from: https://clinicaltrials.gov/ct2/show/NCT04056455?term=tak-788&draw=1&rank=10.
18. A Study to Evaluate Pharmacokinetics (PK) and Safety of Oral Mobocertinib in Participants With Moderate or Severe Hepatic Impairment (HI) and Normal Hepatic Function. ClinicalTrials.gov Identifier: NCT04056468. Available from: https://clinicaltrials.gov/ct2/show/NCT04056468?term=tak-788&draw=2&rank=11.
19. A Study to Assess Absolute Bioavailability (ABA) of Mobocertinib (TAK-788) and to Characterize Mass Balance, Pharmacokinetics (PK), Metabolism, and Excretion of Carbon-14 ([14C])-Mobocertinib in Male Healthy Participants. ClinicalTrials.gov Identifier: NCT03811834. Available from: https://clinicaltrials.gov/ct2/show/NCT03811834?term=tak-788&draw=2&rank=9.
20. A Study to Evaluate the Effect of High-Fat Meal on TAK-788 Pharmacokinetics (PK) in Healthy Adult Participants. ClinicalTrials.gov Identifier: NCT04441255. Available from: https://clinicaltrials.gov/ct2/show/NCT04441255?term=tak-788&draw=1&rank=2.
21. A Study to Evaluate the Pharmacokinetics (PK), Safety and Tolerability of TAK-788 Followed by Evaluation of the Effects of a Low-Fat Meal on TAK-788 PK and Evaluation of Relative Bioavailability of TAK-788 Capsules in Healthy Participants. ClinicalTrials.gov Identifier: NCT03482453. Available from: https://clinicaltrials.gov/ct2/show/NCT03482453?term=tak-788&draw=1&rank=6.
22. A Study to Evaluate Drug-Drug Interaction of TAK-788 With Itraconazole and Rifampin in Healthy Adult Participants. ClinicalTrials.gov Identifier: NCT03928327. Available from: https://clinicaltrials.gov/ct2/show/NCT03928327?term=tak-788&draw=1&rank=5.
23. Drug-Drug Interaction Study of TAK-788 and Midazolam in Participants With Advanced Non-small Cell Lung Cancer (NSCLC). ClinicalTrials.gov Identifier: NCT04051827. Available from: https://clinicaltrials.gov/ct2/show/NCT04051827?term=tak-788&draw=3&rank=4.
24. A Study of TAK-788 in Japanese Adults With Non-Small Cell Lung Cancer. ClinicalTrials.gov Identifier: NCT03807778. Available from: https://clinicaltrials.gov/ct2/show/NCT03807778?term=tak-788&draw=1&rank=1.
25. Duke E, Stapleford L, Drezner N, et al. FDA Approval Summary: mobocertinib for Metastatic Non–Small Cell Lung Cancer with EGFR Exon 20 Insertion Mutations. Clin Cancer Res. 2022;28:4173–4177. doi:10.1158/1078-0432.CCR-22-2072
26. Takeda Pharmaceuticals America Inc. Exkivity (Mobocertinib) [Prescribing Information]. Lexington, MA: Takeda Pharmaceuticals America Inc; 2021.
27. Petrini I, Giaccone G. Amivantamab in the Treatment of Metastatic NSCLC: patient Selection and Special Considerations. Onco Targets Ther. 2022;15:1197–1210. doi:10.2147/OTT.S329095
28. Park K, Haura EB, Leighl NB, et al. Amivantamab in EGFR Exon 20 Insertion-Mutated Non-Small-Cell Lung Cancer Progressing on Platinum Chemotherapy: initial Results From the CHRYSALIS Phase I Study. J Clin Oncol. 2021;39(30):3391–3402. doi:10.1200/JCO.21.00662
29. Christopoulos P, Prawitz T, Hong JL, et al. Indirect comparison of mobocertinib and real-world therapies for pre-treated non-small cell lung cancer with EGFR exon 20 insertion mutations. Lung Cancer. 2023;179:107191. doi:10.1016/j.lungcan.2023.107191
30. Christopoulos P, Kluck K, Kirchner M, et al. The impact of TP53 co-mutations and immunologic microenvironment on outcome of lung cancer with EGFR exon 20 insertions. Eur J Cancer. 2022;170:106–118. doi:10.1016/j.ejca.2022.04.020
31. Zhang W, Dong X. Positive progress for non-small cell lung cancer with epidermal growth factor receptor exon 20 insertion mutations: a novel targeted therapy option. J Oncol Pharm Practice. 2021;27(8):2007–2009. doi:10.1177/10781552211044980
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.