Back to Journals » Infection and Drug Resistance » Volume 19
Clinical Utility of a Droplet Digital PCR-Based Assay for Quantitative Detection of Pneumocystis jirovecii in Suspected Fungal Pneumonia
Authors Jiang Z, Zhou Y, Huang H, Yuan Y, Tang Q, He C
Received 31 October 2025
Accepted for publication 13 February 2026
Published 27 February 2026 Volume 2026:19 573471
DOI https://doi.org/10.2147/IDR.S573471
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Ziyang Jiang,1,* Yi Zhou,1,* Hengjian Huang,2 Yu Yuan,1 Qiuping Tang,1 Chao He1
1Department of Laboratory Medicine/Clinical Laboratory Medicine Research Center/Sichuan Clinical Research Center for Laboratory Medicine, West China Hospital of Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China; 2West China Precision Medicine Industrial Technology Institute, West China Hospital of Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao He, Department of Laboratory Medicine/Clinical Laboratory Medicine Research Center/Sichuan Clinical Research Center for Laboratory Medicine, West China Hospital of Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China, Tel +86-13880719269, Email [email protected]
Purpose: Pneumocystis jirovecii typically causes life-threatening Pneumocystis pneumonia (PCP), calling for accurate detection of P. jirovecii in clinical samples to facilitate PCP management.
Patients and Methods: An observational cohort of 193 patients with suspected fungal pneumonia was enrolled. The cell-free DNA (cfDNA) in bronchoalveolar lavage fluid (BALF) and serum samples was prepared and quantitated via a ddPCR assay targeting the mitochondrial large subunit rRNA gene of P. jirovecii. The correlations between ddPCR results and medical data were analyzed.
Results: The cases with complete data were classified into a PCP group (N=30) and a non-PCP group (N=139). This ddPCR assay demonstrated a sensitivity of 91.3% and a specificity of 96.8% for BALF, in contrast to a sensitivity of 57.1% and a specificity of 100% for serum. The area under the curve of 0.896 for diagnosis was obtained via ddPCR assay, compared with 0.627 via G-test (P< 0.0001). The cfDNA copies were positively correlated with antifungal agents usage, certain clinical characteristics, lactate dehydrogenase levels, and G-test results (all P< 0.05). Moreover, higher cfDNA copies were associated with increased in-hospital mortality (aHR> 1, P< 0.05).
Conclusion: The ddPCR assay exhibited robust diagnostic performance for PCP in BALF samples and cfDNA copies may serve as an indicator for improving the management of patients.
Keywords: cell-free DNA, droplet digital PCR, Pneumocystis jirovecii, pneumonia, diagnosis, quantitative detection
Introduction
Pneumocystis jirovecii is a common opportunistic fungal pathogen that frequently causes life-threatening Pneumocystis pneumonia (PCP).1 Clinical manifestations of PCP, including fever, dry or productive cough, hemoptysis, progressive dyspnea, and even acute respiratory failure, are often nonspecific and can mimic other pulmonary infections or conditions.2 Owing to the rapid disease progression, the in-hospital mortality of the patients with PCP was estimated to be 67.0%.3 Daily delay of effective treatment was associated with an increased mortality risk of 11.1%.4 Therefore, there is an urgent need for rapid and accurate detection of P. jirovecii from clinical samples to facilitate timely diagnosis and targeted treatment of the patients with PCP.5
Conventionally, it is extremely challenging to recover P. jirovecii from clinical samples. Subsequently, direct microscopic detection of cystic or trophic forms in lower respiratory tract specimens or lung biopsies can be conducted; however this method is labor-intensive, lacks sensitivity, and is highly dependent on the experience of laboratory technologists.6,7 Immunofluorescence assays targeting the antigens of P. jirovecii provide good sensitivity but are limited by low specificity and dependence on specimen quality and type.6,7 The (1,3)-beta-D glucan test (G-test) is commonly used for PCP diagnosis but exhibits suboptimal diagnostic performance, with a sensitivity of 53.5% and a specificity of 78.4%.8 Additionally, negative G-test results were observed in 12.0%~27.2% of PCP patients without human immunodeficiency virus infection, indicating that the diagnostic accuracy of the G-test may vary across different populations.9 Moreover, its clinical utility is limited by the false positivity from non-fungal factors, for example, cellulose membrane hemodialysis, intravenous immunoglobulin or specific antibiotics, and blood product transfusions.10–12
Furthermore, nucleic acid-based methods have been developed for rapid identification of P. jirovecii from clinical samples. For example, polymerase chain reaction (PCR) achieved a sensitivity of 87.9% and a specificity of 67.2% in bronchoalveolar lavage fluid (BALF) or sputum.13 Quantitative PCR (qPCR) demonstrated sensitivities ranging from 83.3% to 100% and specificities ranging from 91.8% to 100% in various types of respiratory tract samples.14 However, this method exhibits notable limitations, eg unstable amplification efficiency, limited dynamic range, operator variability, and sensitivity to PCR suppressors. Metagenomic next-generation sequencing showed sensitivities ranging from 82.1% to 92.3% and specificities ranging from 68.8% to 87.4% in lower respiratory tract specimens.15,16 Nonetheless, this technique has some disadvantages in clinical application, such as the need for expensive instruments and reagents, complicated operating procedures, and difficulty of interpreting the results.17 This calls for the development of simple and innovative techniques for rapid detection of P. jirovecii in clinical samples, as well as revealing the fungal burden as an important reference for the precise management of patients.
Recently, digital droplet PCR (ddPCR), a new generation PCR technique based on the partitioning of the oil-water emulsion droplet, was characterized by absolute quantification of nucleic acids without the need for standard curves.18 It demonstrated superior analytical performance and increased tolerance to PCR inhibitors,19 and it also showed promising potential in infectious diseases caused by various pathogens.20 In our previous study, a ddPCR assay specifically designed for Aspergillus spp. exhibited good performance for diagnosing invasive pulmonary aspergillosis.21 This technique needs to be applied to various infectious diseases. Several studies have applied ddPCR assays for PCP diagnosis, but the application was limited to immunocompromised patients and BALF samples.22–26 Therefore, in this study, the diagnostic performance of a ddPCR-based assay targeting P. jirovecii in a cohort with suspected fungal pneumonia was investigated, and the correlations between ddPCR results and other clinical data were also explored to verify the clinical utility of this technique in various clinical settings.
Materials and Methods
Study Design and Sample Collection
This was an observational study involving a total of 193 patients with suspected fungal pneumonia admitted between January 2021 and December 2021. Both immunocompromised and immunocompetent patients were enrolled. According to the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium (EORTC/MSGERC) guidelines, suspected fungal pneumonia was defined as the presence of at least one host factor, a clinical feature, and with or without mycological evidence.27 For each patient, BALF or serum samples, as requested by the attending for G-test, were also collected for ddPCR assays. The medical records for each patient were retrieved from the hospital information system. The flowchart of study design is shown in Figure 1A.
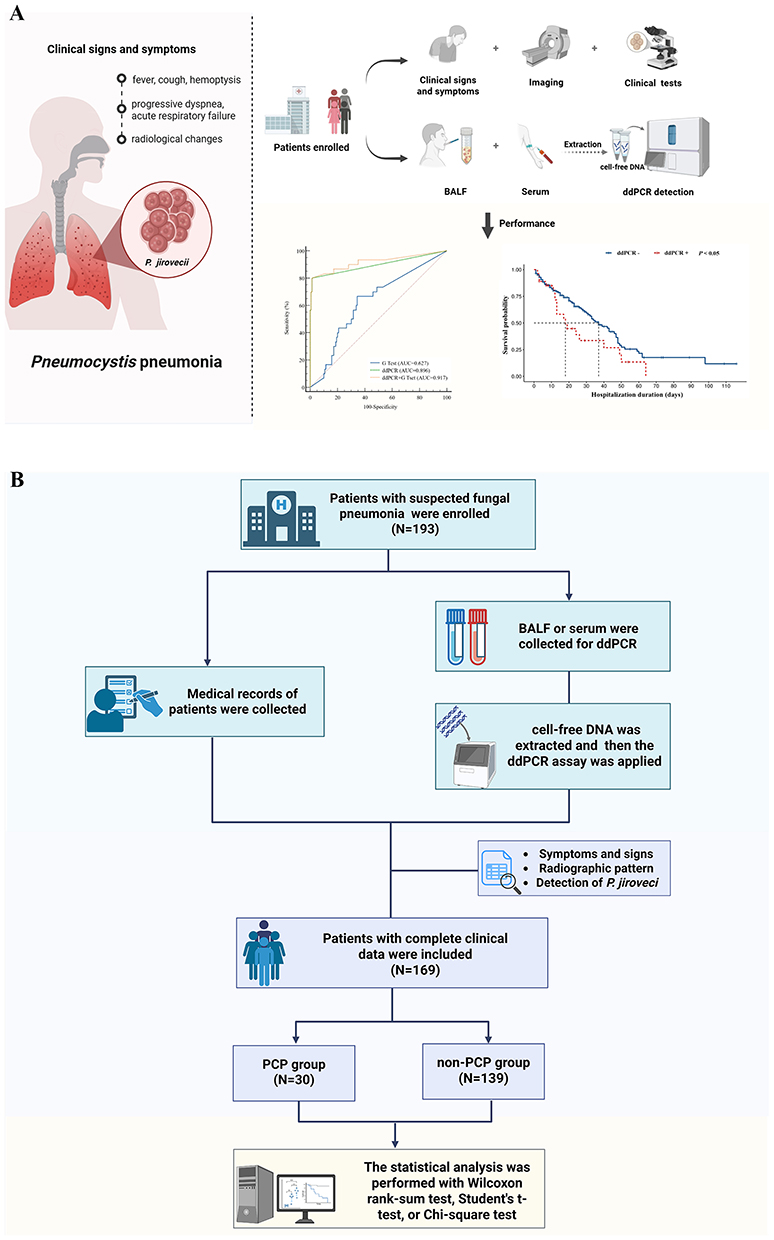 |
Figure 1 Design of this study. (A) Flowchart of the study. (B) Patient enrollment and statistical analysis. Abbreviations: P. jirovecii, Pneumocystis jirovecii; BALF, bronchoalveolar lavage fluid; ddPCR, digital droplet polymerase chain reaction. |
The consensus established by the EORTC/MSGERC was used to develop the diagnostic criteria for PCP as follows:28 (1) symptoms and signs included fever, progressive dyspnea, nonproductive cough, chest pain, circulatory failure, pneumothorax, and hemoptysis; (2) radiographic patterns included the presence of bilateral, diffuse ground-glass opacity (GGO) with interstitial infiltrates; (3) detection of P. jirovecii in tissue or respiratory tract specimens under microscopy; (4) detection of P. jirovecii using molecular methods in respiratory tract specimens and/or detection of (1,3)-beta-D-glucan in serum, with exclusion of results involving the presence of other invasive fungal diseases or false-positivity. In this study, the diagnostic criteria for PCP were defined when the above criteria (1), (2), and either (3) or (4) were met. Patients with incomplete medical records or under the age of 18 years were excluded. After the application of eligibility criteria, 169 cases included were categorized into a PCP group (N=30) and a non-PCP group (N=139). Next, the data from both groups were statistically analyzed (Figure 1B).
Cell-Free DNA (cfDNA) Preparation and ddPCR Assay
Briefly, cfDNA was extracted from each sample using the commercial nucleic acid extraction kit C1016 (Concert Biotechnology, Xiamen, China) on an automated HF24/48 extraction system, following the manufacturer’s protocols. Each 5 μL cfDNA was mixed with 10 μL ddPCR premix (Bio-Rad Laboratories, CA, USA) and loaded into a pre-sterilized disposable plastic microchip. Droplet generation was performed using an AD16 droplet generator (PilotGene Tech., Hangzhou, China), producing approximately 20,000 nanoliter-sized water-in-oil droplets.
Referring to a previous report,29 the mitochondrial large subunit rRNA of P. jirovecii was targeted using the forward primer (5′-CTGTTTCCCTTTCGACTATCTACCTT-3′), the reverse primer (5′-CACTGAATATCTCGAGGGAGTATGAA-3′), and the probe (5′-FAM-TCGCACATAGTCTGATTAT-NFQ-MGB-3′). Subsequently, the target gene was amplified via a ddPCR thermal cycler (PilotGene Tech., Hangzhou, China) under the following conditions: initial denaturation at 95°C for 5 min, followed by 40 cycles of 95°C for 15s and 60°C for 60s. Positive fluorescence signals were analyzed using GenePMS v2.0.1.2001. A detection threshold of 0.5 copies/μL was employed to define a positive result following the manufacturer’s instructions and the method described by Armbruster and Pry.30
Statistical Analysis
Continuous variables were expressed as median and interquartile range (IQR) or as mean with a 95% confidence interval (CI). Non-normally distributed data were analyzed using the Wilcoxon rank-sum test, while parametric tests were performed using Student’s t-test. Categorical variables were presented as frequencies and analyzed using the chi-square test. Logistic regression analysis was used to identify the risk factors, while Spearman’s rank correlation was applied to assess the associations between ddPCR results and other indicators. The Cox proportional hazards model adjusted for age and sex was used to identify the factors associated with in-hospital mortality.31,32 Statistical analyses were conducted with SPSS 27.0 software. A P-value of <0.05 was considered statistically significant.
Results
Clinical Characteristics of Enrolled Patients
The characteristics with statistically significant differences between the PCP and non-PCP groups were demonstrated in Table 1 in bold text (P<0.05). Uni-variate logistic regression analysis revealed that the PCP group had more severe underlying conditions (P<0.05). Multivariate logistic regression analysis identified immunodeficiency status as an independent risk factor (P<0.05) (Figure 2).
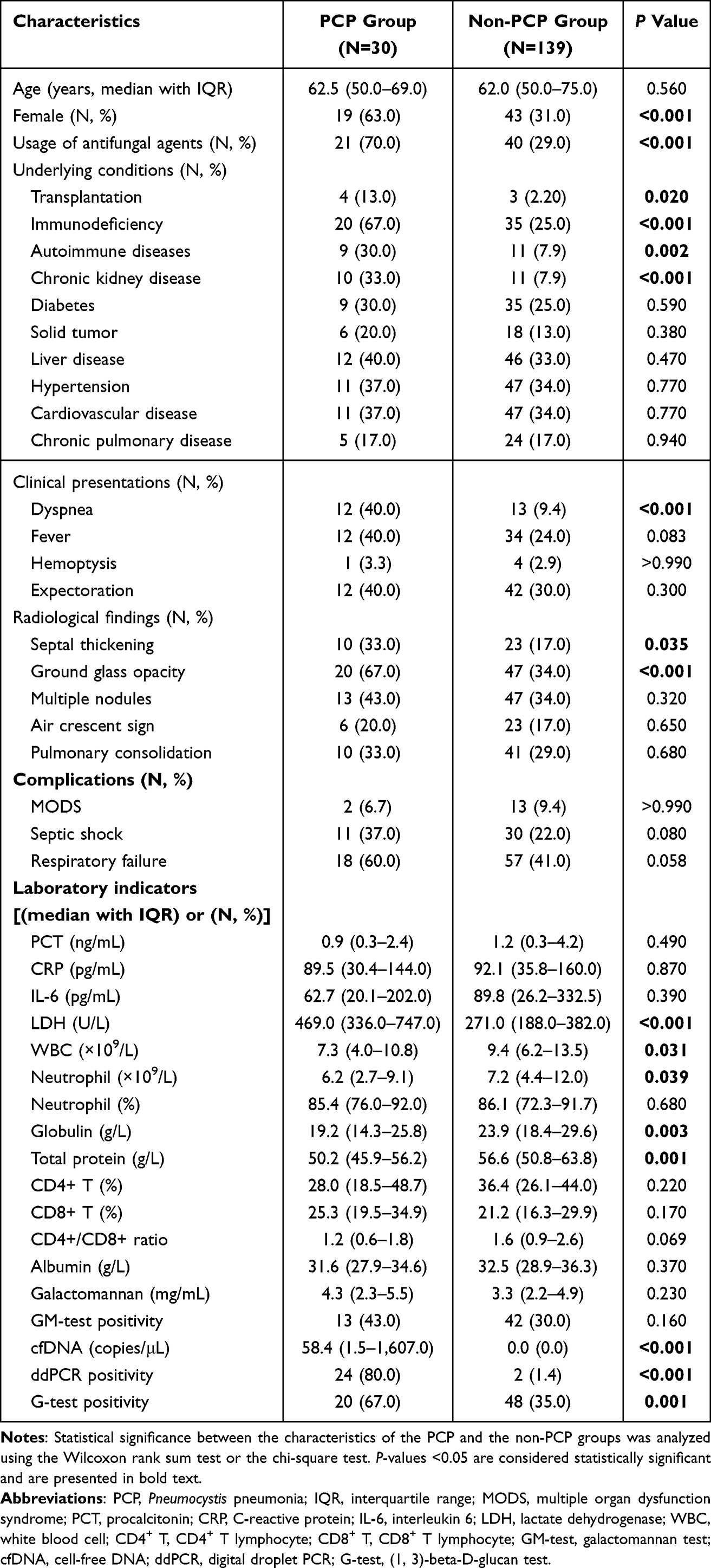 |
Table 1 Clinical Characteristics for the Cases Included |
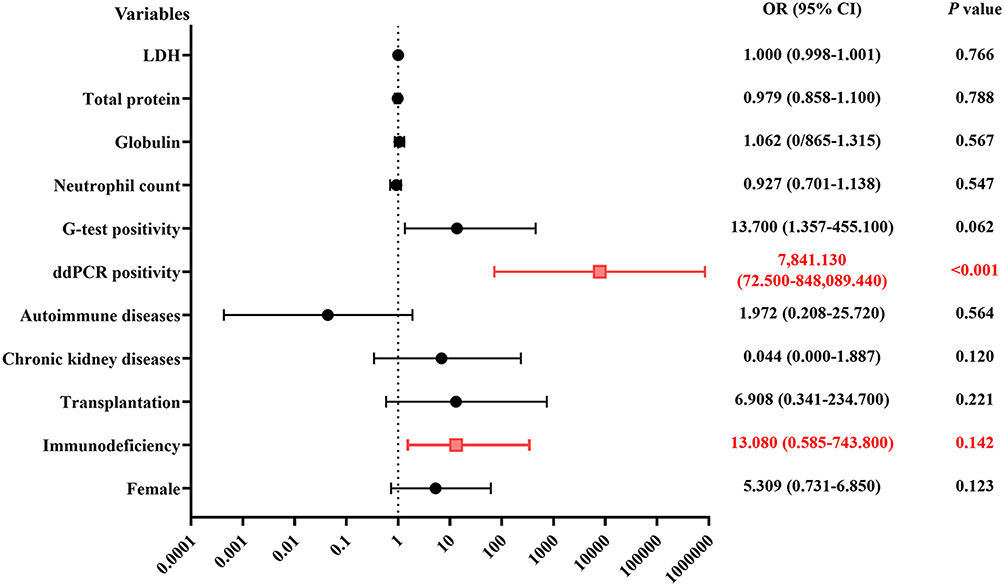 |
Figure 2 Multivariable logistic regression analysis of the risk factors for PCP. The forest plot illustrates OR with 95% CI for variables independently associated with PCP. Multivariable analysis was performed on the clinical variables and laboratory indicators. Statistically significant independent predictors, along with their corresponding ORs (95% CIs) and P values, are marked in red (Wald test, P< 0.05). The vertical dashed line indicates the null effect (OR=1). Abbreviations: PCP, Pneumocystis pneumonia; OR, odds ratio; 95% CI, 95% confidence interval; LDH, lactate dehydrogenase; G-test, (1, 3)-beta-D-glucan test; ddPCR, droplet digital PCR. |
Performance of the ddPCR Assay for PCP Diagnosis
The cfDNA in both BALF and serum samples was detected using the ddPCR assay (Figure 3A). This ddPCR assay showed a sensitivity of 91.3% and a specificity of 96.8% for BALF samples, while a sensitivity of 57.1% and a specificity of 100% were obtained for serum samples (Table 2). As shown in Figure 3B, the area under the curves (AUCs) of the ddPCR assay and G-test were 0.896 and 0.627 (P<0.0001), respectively. The approach combining ddPCR assay and G-test increased the AUC to 0.917, but no significant difference was observed compared with ddPCR assay alone (P=0.396).
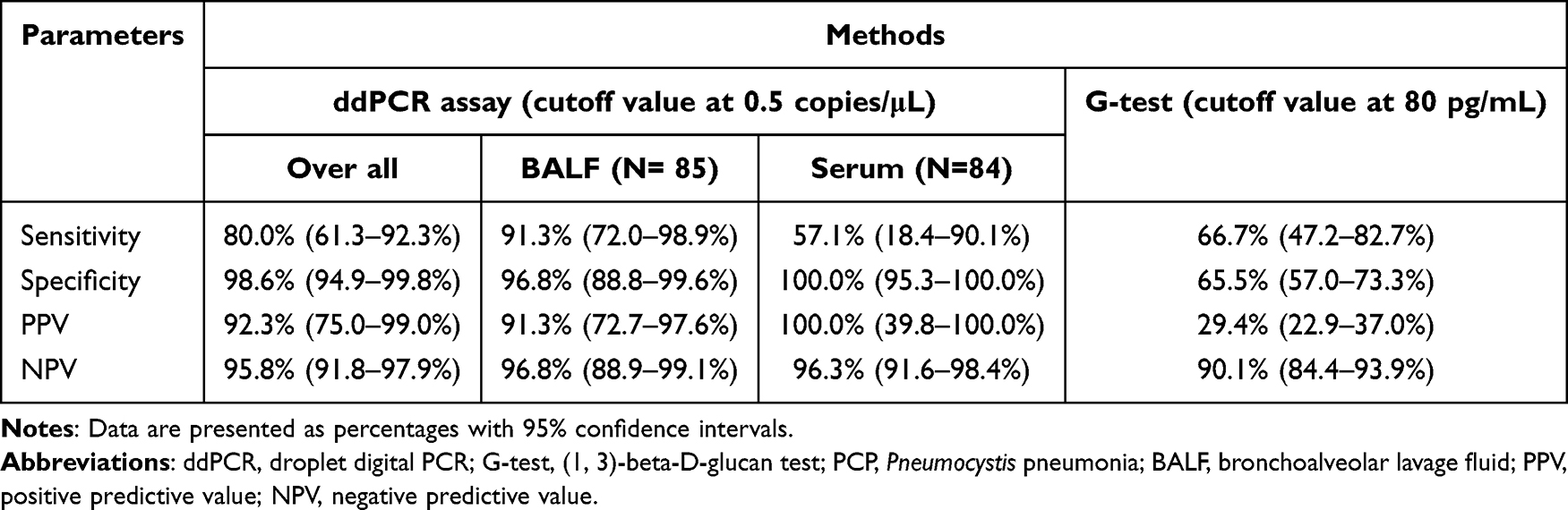 |
Table 2 Diagnostic Performance of the ddPCR Assay and G-Test for PCP |
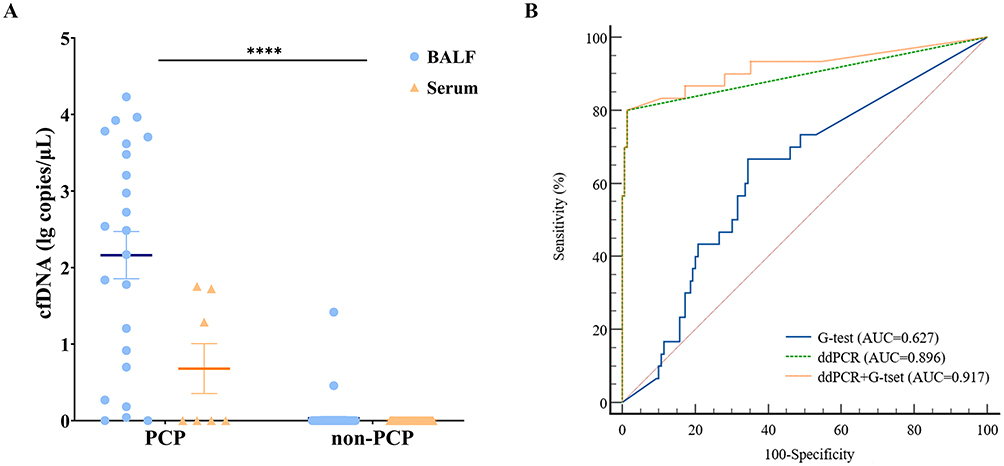 |
Figure 3 Quantitative results and diagnostic performance of the ddPCR assay. (A) cfDNA copies in the groups. Normalization of cfDNA copies determined using ddPCR involved transformation using log10. ****, P<0.001. (B) Receiver operating characteristic curve (ROC) analysis of ddPCR and G-test in PCP diagnosis. Abbreviations: cfDNA, cell-free DNA; PCP, Pneumocystis pneumonia; ddPCR, droplet digital PCR; BALF, bronchoalveolar lavage fluid; G-test, (1, 3)-beta-D-glucan test. |
Correlation Between cfDNA Copies and Other Clinical Data
As indicated in Figure 4A–C, cfDNA copies were positively correlated with the frequency of antifungal agents usage, the presence of specific characteristics (including immunodeficiency, ground-glass opacity on imaging, chronic kidney disease, autoimmune diseases, septic shock, dyspnea), the levels of lactate dehydrogenase (LDH), and G-test results (all P<0.05).
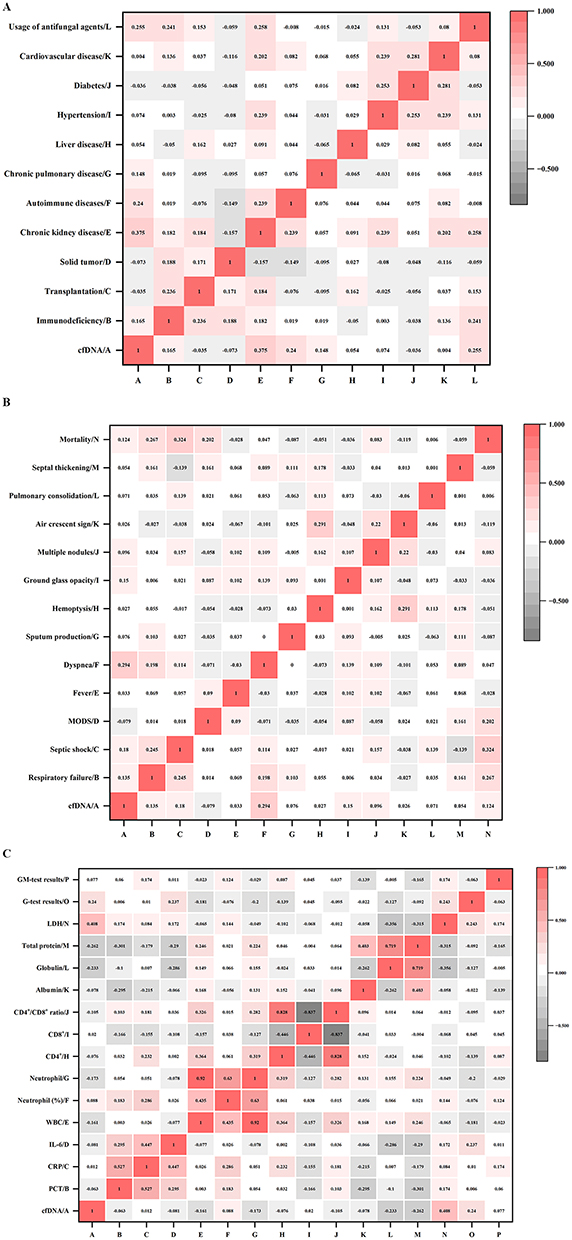 |
Figure 4 Correlation analysis of cfDNA copies with other clinical data of the cases included. The heatmap depicts Spearman’s rank correlation coefficients between cfDNA copies and (A) baseline characteristics, (B) clinical presentations, and (C) laboratory indicators. The figure in the box represents the Spearman correlation coefficient (r). Red boxes represent positive correlations, and grey boxes represent negative associations. Abbreviations: cfDNA, cell-free DNA; MODS, multiple organ dysfunction syndrome; LDH, lactate dehydrogenase; PCT, procalcitonin; CRP, C-reactive protein; IL-6, interleukin 6; WBC, white blood cell; CD4+ T, CD4+ T lymphocyte; CD8+ T, CD8+ T lymphocyte; G-test, (1, 3)-beta-D-glucan test; GM-test, galactomannan test. |
Survival Analysis of the Cases During Hospitalization
Among all patient enrolled, the ddPCR-positive ones had higher mortality (63.3%) compared to 51.7% of ddPCR-negative ones, but the difference was not statistically significant (P=0.100). Whereas, survival analysis based on hospitalization duration revealed that the ddPCR results were correlated with the prognosis of the patients at the discharge (P<0.05, Figure 5A).
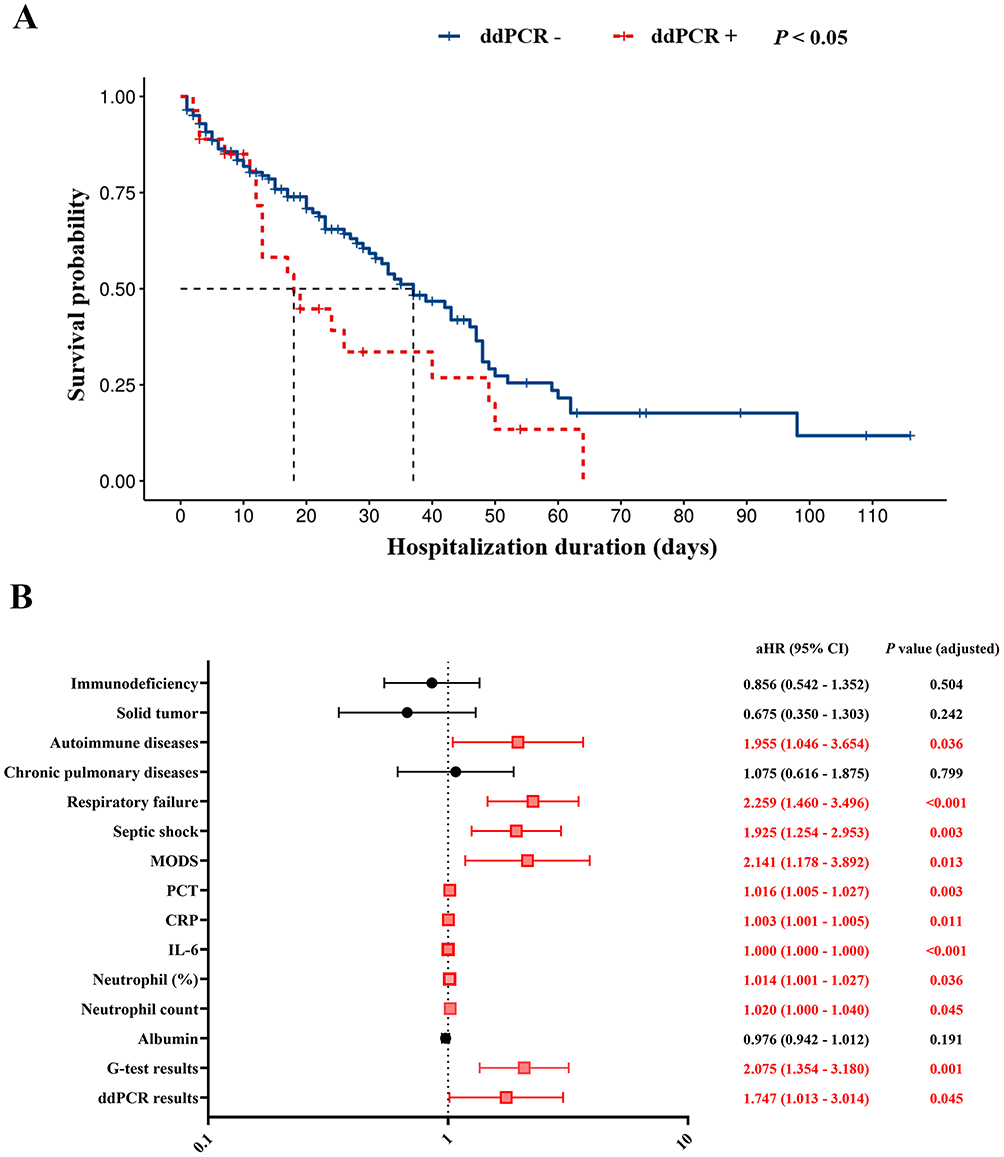 |
Figure 5 Mortality and its risk factors among the included patients during hospitalization. (A) Kaplan–Meier curves stratified using the ddPCR results demonstrate significantly reduced survival probability in ddPCR-positive patients (Log rank test, P<0.05). (B) Forest plot of multivariable Cox regression analysis identifying independent predictors of mortality. Adjusted hazard ratios (aHRs) with 95% confidence intervals are shown for clinical variables and laboratory indicators. Symbols marked in red represent statistically independent predictors, along with the corresponding aHRs (95% CIs) and P values (Wald test, P<0.05). The vertical dashed line indicates the null effect (aHR=1). Abbreviations: aHR, adjusted hazard ratios; MODS, multiple organ dysfunction syndrome; CRP, C-reactive protein; PCT, procalcitonin; IL-6, interleukin 6; ddPCR, droplet digital PCR; G-test, (1, 3)-beta-D-glucan test. |
The clinical characteristics of the survival and non-survival cases were shown in supplemental Table S1. Using the Cox proportional hazards model with age and sex as adjusting covariates, the presence of autoimmune diseases, severe complications, and higher fungal burdens (higher cfDNA copies and (1,3)-beta-D glucan levels) were associated with increased in-hospital mortality (adjusted hazard ratio [aHR]>1, P<0.05) (Figure 5B).
Discussion
Studies have reported that PCP affected approximately 505,000 individuals across 120 countries worldwide between 2010 and 2023, with a mortality rate of 42.4%.33 Traditional detection methods for P. jirovecii in clinical laboratories show limited diagnostic performance for PCP, necessitating the development of accurate innovative techniques with enhanced sensitivity and specificity for quantitative detection of this pathogen in clinical samples.
Recently, ddPCR was developed for the detection of P. jirovecii in clinical samples, and the multicopy major surface glycoprotein (MSG) gene or mitochondrial large subunit (mtLSU) rRNA gene was used as the target.34,35 MSG-targeted detection using the QX200 ddPCR system in BALF samples from 54 immunocompromised patients demonstrated a sensitivity of 91.7% and a specificity of 88.1%, with AUC values of 0.800 and 0.990 in HIV-infected and non-HIV patients.22 Using a TargetingOne digital PCR system to detect mtLSU rRNA in 98 non-HIV immunocompromised patients, the positive rates of P. jirovecii in BALF and in sputum were 43.9% and 62.2% respectively.24 Subsequent application via the same system yielded a sensitivity of 98.0%, a specificity of 85.7%, and an AUC of 0.973 in BALF samples from 89 immunocompromised patients.25 Elsewhere, a study comprising 170 patients reported that the Pilot Gene Tech ddPCR system achieved a sensitivity of 100%, a specificity of 97.9%, and an AUC of 0.975 in BALF.23 These studies demonstrate that the ddPCR assays achieves good performance for PCP diagnosis. However, this assay was only applied to immunocompromised patients and BALF samples. Therefore, the clinical utility of ddPCR across various clinical settings needs to be further explored.
In our study, the 121 bp fragment of the mtLSU rRNA gene was targeted, referring to the previous study.29 The results revealed a sensitivity of 91.3% and a specificity of 96.8% in BALF samples. Though the high specificity of 100% was detected in serum samples, the low sensitivity (57.1%) may be related to the pathogenesis of P. jirovecii.36,37 This revealed that BALF was the optimal sample type for PCP diagnosis using the ddPCR assay. Additionally, we observed that the diagnostic approach combining ddPCR and G-test improved the AUC value, although no significant difference was detected compared with ddPCR assay alone. A retrospective study reported that sensitivity of qPCR for PCP was increased from 85.7% to 96.9% when combined with the G-test.38 More studies are needed to evaluate whether combining the ddPCR results with other indicators could improve the diagnostic performance for PCP.
Moreover, considering that ddPCR can quantify the copies of nucleic acids in an absolute manner, we further analyzed the correlation between the cfDNA copies and clinical data. A significant positive correlation was found between the cfDNA copies and LDH levels. LDH, as a biomarker of lung tissue injury, was generally increased in proportion to the severity of PCP.39,40 Also, the cfDNA copies exhibited positive correlations with the severity of the underlying conditions and clinical manifestations, as demonstrated by the positive correlations between the cfDNA copies and other indicators, including reduced oxygenation index and increased levels of inflammatory indicators.25,26 These findings indicates that the cfDNA copies might be used to assess the severity of PCP and fungal burdens.
In addition, the association of ddPCR results with clinical outcomes of the patients was analyzed in our study, and poorer prognosis at discharge was observed in ddPCR-positive patients compared with ddPCR-negative patients. A significant positive correlation was detected between the higher cfDNA copies and higher in-hospital mortality (aHR>1, P<0.05). Previous studies have reported that continued PCR positivity was significantly associated with in-hospital mortality (P=0.003), and rapid declines in P. jirovecii cfDNA burden were observed after effective therapy.41,42 The potential of ddPCR to guide antibiotic treatment by dynamic monitoring of pathogen burden was demonstrated.43 Collectively, ddPCR may be useful for monitoring and managing PCP, and cfDNA thresholds might be established to guide treatment.
This study has several limitations that need to be acknowledged. Firstly, the sample size was small, which reduces the statistical power. Secondly, the relationship between ddPCR results and the effects of anti-infective treatment could not be evaluated in this observational study.
Conclusion
The ddPCR-based assay showed robust diagnostic performance for PCP in BALF samples. Analysis of the relationship between ddPCR results and other medical data indicated that cfDNA may serve as an indicator for the management of PCP patients.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Ethics Approval
This study received ethical approval from the Institutional Review Board of West China Hospital of Sichuan University (Approval No. 2020–954) and was conducted in strict compliance with the principles of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all individual patients included in the study.
Author Contributions
Ziyang Jiang and Yi Zhou share first authorship. Authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Department of Sichuan Province [Grant No. 2021YFS0183, 2024YFFK0225].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weyant RB, Kabbani D, Doucette K, Lau C, Cervera C. Pneumocystis jirovecii: a review with a focus on prevention and treatment. Expert Opin Pharmacother. 2021;22(12):1579–12. doi:10.1080/14656566.2021.1915989
2. Azoulay E, Russell L, Van de Louw A, et al. Diagnosis of severe respiratory infections in immunocompromised patients. Intensive Care Med. 2020;46(2):298–314. doi:10.1007/s00134-019-05906-5
3. Giacobbe DR, Dettori S, Di Pilato V, et al. Pneumocystis jirovecii pneumonia in intensive care units: a multicenter study by ESGCIP and EFISG. Crit Care. 2023;27(1):323. doi:10.1186/s13054-023-04608-1
4. Roux A, Canet E, Valade S, et al. Pneumocystis jirovecii Pneumonia in Patients with or without AIDS, France. Emerg Infect Dis. 2014;20(9):1490–1497. doi:10.3201/eid2009.131668
5. Hänsel L, Schumacher J, Denis B, Hamane S, Cornely OA, Koehler P. How to diagnose and treat a patient without human immunodeficiency virus infection having Pneumocystis jirovecii pneumonia? Clin Microbiol Infect. 2023;29(8):1015–1023. doi:10.1016/j.cmi.2023.04.015
6. Bateman M, Oladele R, Kolls JK. Diagnosing Pneumocystis jirovecii pneumonia: a review of current methods and novel approaches. Med Mycol. 2020;58(8):1015–1028. doi:10.1093/mmy/myaa024
7. Jaramillo Cartagena A, Asowata OE, Ng D, Babady NE, Humphries RM. An overview of the laboratory diagnosis of Pneumocystis jirovecii pneumonia. J Clin Microbiol. 2025;63(3):e0036124. doi:10.1128/jcm.00361-24
8. Szvalb AD, Malek AE, Jiang Y, Bhatti MM, Wurster S, Kontoyiannis DP. Serum (1,3)-Beta-d-Glucan has suboptimal performance for the diagnosis of Pneumocystis jirovecii pneumonia in cancer patients and correlates poorly with respiratory burden as measured by quantitative PCR. J Infect. 2020;81(3):443–451. doi:10.1016/j.jinf.2020.07.003
9. Ishihara M, Tanzawa S, Honda T, Ichikawa Y, Watanabe K, Seki N. Clinical Features of Pneumocystis Pneumonia in Non-Human Immunodeficiency Virus-Infected Patients: a Systemic Review and Meta-Analysis. J Clin Question. 2024;1(2):12–23. doi:10.69854/jcq.2024.0003
10. Prattes J, Schilcher G, Krause R. Reliability of serum 1,3-beta- d -glucan assay in patients undergoing renal replacement therapy: a review of the literature. Mycoses. 2015;58(1):4–9. doi:10.1111/myc.12267
11. Tschopp J, Brunel AS, Spertini O, Croxatto A, Lamoth F, Bochud PY. High False-Positive Rate of (1,3)-β-D-Glucan in Onco-Hematological Patients Receiving Immunoglobulins and Therapeutic Antibodies. Clin Infect Dis. 2022;75(2):330–333. doi:10.1093/cid/ciab1028
12. Liss B, Cornely OA, Hoffmann D, Dimitriou V, Wisplinghoff H. 1,3-ß-D-glucan concentrations in blood products predict false positive post-transfusion results. Mycoses. 2016;59(1):39–42. doi:10.1111/myc.12432
13. Li Y, Liu H, Lv Q, Long J. Diagnosis model of early Pneumocystis jirovecii pneumonia based on convolutional neural network: a comparison with traditional PCR diagnostic method. BMC Pulm Med. 2024;24(1):205. doi:10.1186/s12890-024-02987-x
14. Veintimilla C, Álvarez-Uría A, Martín-Rabadán P, et al. Pneumocystis jirovecii Pneumonia Diagnostic Approach: real-Life Experience in a Tertiary Centre. J Fungi. 2023;9(4):414. doi:10.3390/jof9040414
15. Liu Y, Wang X, Xu J, Yang Q, Zhu H, Yang J. Diagnostic value of metagenomic next-generation sequencing of lower respiratory tract specimen for the diagnosis of suspected Pneumocystis jirovecii pneumonia. Annals of Medicine. 2023;55(1):2232358. doi:10.1080/07853890.2023.2232358
16. Xing F, Deng C, Luo Z, et al. Rapid Diagnosis of Pneumocystis jirovecii Pneumonia and Respiratory Tract Colonization by Next-Generation Sequencing. Mycopathologia. 2024;189(3):38. doi:10.1007/s11046-024-00849-y
17. Zhang Z, Liu T, Ming M, et al. Metagenomic next-generation sequencing promotes diagnosis and treatment of Pneumocystis jirovecii pneumonia in non-HIV infected children: a retrospective study. BMC Pulm Med. 2024;24(1):338. doi:10.1186/s12890-024-03135-1
18. Kojabad AA, Farzanehpour M, Galeh HEG, et al. Droplet digital PCR of viral DNA/RNA, current progress, challenges, and future perspectives. J Med Virol. 2021;93(7):4182–4197. doi:10.1002/jmv.26846
19. Gaňová M, Zhang H, Zhu H, Korabečná M, Neužil P. Multiplexed digital polymerase chain reaction as a powerful diagnostic tool. Biosens. Bioelectron. 2021;181:113155. doi:10.1016/j.bios.2021.113155
20. Yang X, Yu F, Yan C, et al. Global trends in the application of droplet digital PCR technology in the field of infectious disease pathogen diagnosis: a bibliometric analysis from 2012 to 2023. Diagn Microbiol Infect Dis. 2025;111(3):116623. doi:10.1016/j.diagmicrobio.2024.116623
21. Liu Y, Tang Q, Tang S, et al. Clinical evaluation of droplet digital PCR in suspected invasive pulmonary aspergillosis. Int J Clin Chem. 2025;569:120153. doi:10.1016/j.cca.2025.120153
22. Jitmuang A, Nititammaluk A, Boonsong T, Sarasombath PT, Sompradeekul S, Chayakulkeeree M. A novel droplet digital polymerase chain reaction for diagnosis of Pneumocystis pneumonia (PCP)-a clinical performance study and survey of sulfamethoxazole-trimethoprim resistant mutations. J Infect. 2021;83(6):701–708. doi:10.1016/j.jinf.2021.09.014
23. Guo J, Tian W, Lin H, et al. Analytical and clinical validation of multiplex droplet digital PCR assay for detecting pathogenic fungal infection in lungs. Mycology. 2024;15(1):110–119. doi:10.1080/21501203.2023.2296941
24. Yi J, Wang N, Wu J, et al. Development of a Droplet Digital Polymerase Chain Reaction for Sensitive Detection of Pneumocystis jirovecii in Respiratory Tract Specimens. Front Med. 2021;8:761788. doi:10.3389/fmed.2021.761788
25. Bian W, Shang Y, Zhao L, et al. Clinical performance of BALF droplet digital PCR for differential diagnosis of Pneumocystis jirovecii pneumonia and Pneumocystis jirovecii colonization. Diagn Microbiol Infect Dis. 2024;108(3):116168. doi:10.1016/j.diagmicrobio.2023.116168
26. Bian W, Xie Y, Shang Y, et al. Relationship between clinical features and droplet digital PCR copy number in non-HIV patients with pneumocystis pneumonia. BMC Infect Dis. 2023;23(1):833. doi:10.1186/s12879-023-08580-7
27. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
28. Lagrou K, Chen S, Masur H, et al. Pneumocystis jirovecii Disease: basis for the Revised EORTC/MSGERC Invasive Fungal Disease Definitions in Individuals Without Human Immunodeficiency Virus. Clin Infect Dis. 2021;72(Suppl _2):S114–s120. doi:10.1093/cid/ciaa1805
29. Alanio A, Desoubeaux G, Sarfati C, et al. Real-time PCR assay-based strategy for differentiation between active Pneumocystis jirovecii pneumonia and colonization in immunocompromised patients. Clin Infect Dis. 2011;17(10):1531–1537. doi:10.1111/j.1469-0691.2010.03400.x
30. Armbruster DA, Pry T. Limit of blank, limit of detection and limit of quantitation. Clin Biochem Rev. 2008;29(Suppl 1):S49–52.
31. Yu Z, Zhao Z, Ding C, et al. The association between sarcopenia and cardiovascular disease: an investigative analysis from the NHANES. Nutr Metab Cardiovasc Dis. 2025;35(7):103864. doi:10.1016/j.numecd.2025.103864
32. Pompermaier L, Steinvall I, Elmasry M, et al. Long-term mortality after self-inflicted burns. Burns. 2024;50(1):252–261. doi:10.1016/j.burns.2023.09.015
33. Denning DW. Global incidence and mortality of severe fungal disease. Lancet Infect Dis. 2024;24(7):e428–e438. doi:10.1016/S1473-3099(23)00692-8
34. Meenakshi K, Gowtham RR, Usha K. Pneumocystis jirovecii Pneumonia: a Revisit to the Old Malady. J Clin Diagn Res. 2019;13(11).
35. Matouri R, Aboutalebian S, Nasri E, et al. Molecular and microscopy detection of Pneumocystis jirovecii in hospitalized patients during the COVID-19 pandemic. Front Med. 2023;10:1148320. doi:10.3389/fmed.2023.1148320
36. Apostolopoulou A, Fishman JA. The Pathogenesis and Diagnosis of Pneumocystis jiroveci Pneumonia. J Fungi. 2022;8(11):1167. doi:10.3390/jof8111167
37. Heung LJ, Wiesner DL, Wang K, Rivera A, Hohl TM. Immunity to fungi in the lung. Semin Immunopathol. 2023;66:101728. doi:10.1016/j.smim.2023.101728
38. Price JS, Fallon M, Posso R, Backx M, White PL. An Evaluation of the OLM PneumID Real-Time Polymerase Chain Reaction to Aid in the Diagnosis of Pneumocystis Pneumonia. J Fungi. 2023;9(11):1106. doi:10.3390/jof9111106
39. Sun R, Lv D, Xiao M, et al. Diagnostic accuracy of the 1,3-beta-D-glucan test and lactate dehydrogenase for pneumocystis pneumonia in non-HIV patients. Sci Rep. 2021;11(1):9226. doi:10.1038/s41598-021-88729-z
40. Sun J, Su J, Xie Y, et al. Plasma IL-6/IL-10 Ratio and IL-8, LDH, and HBDH Level Predict the Severity and the Risk of Death in AIDS Patients with Pneumocystis Pneumonia. J Immunol Res. 2016;2016:1583951. doi:10.1155/2016/1583951
41. Moreno A, Epstein D, Budvytiene I, Banaei N. Accuracy of Pneumocystis jirovecii Plasma Cell-Free DNA PCR for Noninvasive Diagnosis of Pneumocystis Pneumonia. J Clin Microbiol. 2022;60(5):e0010122. doi:10.1128/jcm.00101-22
42. Choi JS, Lee SH, Leem AY, et al. Pneumocystis jirovecii pneumonia (PCP) PCR-negative conversion predicts prognosis of HIV-negative patients with PCP and acute respiratory failure. PLoS One. 2018;13(10):e0206231. doi:10.1371/journal.pone.0206231
43. Jiang S, Zhao D, Wang C, et al. Clinical evaluation of droplet digital PCR in the early identification of suspected sepsis patients in the emergency department: a prospective observational study. Front Cell Infect Microbiol. 2024;14:1358801. doi:10.3389/fcimb.2024.1358801
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Application of Droplet Digital PCR in Sputum Samples in Myasthenia Gravis Patients with Pneumonia
Su M, Luo Y, Huan X, Xi C, Yang L, Zhong H, Liu F, Zhang Q, Liu Q, Wang X, Cao Y, Wang M, Ta F, Wang B, Ai J, Zhao C, Zheng J, Luo S
Infection and Drug Resistance 2026, 19:588779
Published Date: 4 March 2026