")
Back to Journals » International Journal of Women's Health » Volume 15
Clinical Significance of Application of Chromosomal Karyotyping of Villus Tissues
Authors Zhang S, Wu L, Li X , Yang L, Shen S, Shen H, Zhao D, Qi L
Received 6 June 2023
Accepted for publication 7 October 2023
Published 7 November 2023 Volume 2023:15 Pages 1705—1710
DOI https://doi.org/10.2147/IJWH.S424665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Shuyun Zhang,1,* Lijuan Wu,1,* Xue Li,1 Li Yang,1 Sujuan Shen,1 Hong Shen,1 Dan Zhao,2 Lin Qi2,3
1Center of Reproductive Medicine, The Second Affiliated Hospital of Soochow University, Su Zhou, People’s Republic of China; 2Precision Medicine Center, The Second Affiliated Hospital of Soochow University, Su Zhou, People’s Republic of China; 3State Key Laboratory of Radiation Medicine and Protection, School of Radiation Medicine and Protection, Soochow University, Suzhou, 215000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lin Qi, Precision Medicine Center, The Second Affiliated Hospital of Soochow University, Su Zhou, People’s Republic of China, Tel +86-13962187070, Email [email protected]
Purpose: Karyotype analysis of villus chromosomes in spontaneous abortion by high-throughput ligation-dependent probe amplification (HLPA) was performed to explore relationship between spontaneous abortion and chromosomal abnormalities in spontaneous abortion tissues.
Patients and Methods: The karyotypes of chromosomes of villus tissues from 516 patients with spontaneous abortion who were admitted to our hospital between 2014 and 2019 were analyzed. The data were grouped by the age (ie, ≤ 29, 30– 35, and ≥ 36 years old) in which embryonic chromosomal abnormality rate, and abnormal distribution of chromosome number in abortion tissue of 294 patients.
Results: The examination of 516 samples of spontaneous abortion tissues showed that the chromosomes of 294 samples were abnormal, and the abnormality rate was 60.97%. Among 294 samples with chromosomal abnormalities, 136 (89.47%) samples had numerical chromosomal abnormalities, 15 (9.87%) samples had structural chromosomal abnormalities, and 1 (0.07%) sample had uniparental disomy. A total of 308 couples voluntarily underwent peripheral blood chromosome analysis. The results showed that 56 couples had abnormality in one or both spouses, and rate of embryonic chromosomal abnormality in these 26 cases with chromosomal abnormalities was 100%.
Conclusion: Numerical and structural chromosomal abnormalities are among the important causes of embryonic arrest, while the increase in age could also be a high-risk factor for embryonic chromosomal abnormality. Therefore, examination of the karyotypes of embryo chorionic villus may help understand the reasons of embryonic arrest, which could provide important guidance for more genetic counseling for patients with early spontaneous abortion, as well as improving the preconception preparation.
Keywords: spontaneous abortion, villus tissue, HLPA test, chromosomal abnormality
Introduction
Spontaneous abortion is one of the most common reproductive diseases in clinical practice, referring to the natural termination of pregnancy before a gestational age of 28 weeks and fetal weight of less than 1000 g, severely influencing women’s physical and mental health.1 Spontaneous abortion accounts for approximately 10–20% of all clinical pregnancies, and 80% of which are early trimester spontaneous abortion.2,3 Previous clinical studies have shown that factors causing spontaneous abortion include embryonic factors, maternal factors, immune dysfunction, and environmental factors, of which embryonic chromosomal abnormalities account for over 50%.1,4 It was suggested that genetic factors and chromosomal abnormalities are the main factors causing spontaneous abortion.5 In clinical practice, a noticeable attention has been paid to karyotype analysis of early trimester spontaneous abortion tissues. Therefore, chromosome examination of villi of early trimester spontaneous abortion tissues is of great clinical significance.
High-throughput ligation-dependent probe amplification (HLPA) is a method modified from traditional multiplex ligation-dependent probe amplification (MAPA) for multiple fluorescence PCR amplification of ligation products, which is mainly used for the detection of copy number changes in nucleotide sequences.5,6 HLPA possesses the advantages of high throughput, remarkable accuracy, high resolution, great repeatability, and high-speed detection.6,7 Compared with chromosomal microarray analysis, HLPA can rapidly and accurately spot chromosomal abnormalities at a comparable performance while at a lower cost. Therefore, HLPA provides an accurate, rapid, and inexpensive method for chromosome analysis of miscarriage in clinical practice.8,9
In the present study, HLPA was used to analyze the copy numbers in 265 spontaneous abortion tissues, in order to explore the relationship between spontaneous abortion and embryonic chromosomal abnormalities. The findings could provide important guidance for genetic counseling and improving preconception preparation for couples with spontaneous abortion.
Patients and Methods
Study Design and Subjects
A total of 516 pregnant women who were diagnosed with embryonic arrest by ultrasound and required embryonic chromosomal examination of abortion tissues in the Reproductive Center of the Second Affiliated Hospital of Soochow University between May 2014 and July 2018 were included in this study. All patients signed informed consent forms prior to examination. The study was approved by the Ethics Committee of the Second Affiliated Hospital of Soochow University (Suzhou, China). Pregnant women’s age was 30±3.68 (range, 23–42) years old, and the mean gestational age was 8.72±2.39 (range, 6–25) weeks at the abortion. The age was ≤29, 30–35, and ≥36 years old in 252, 209, and 55 patients, respectively.
Methods
For patients who were diagnosed with embryonic arrest by ultrasound, the disease conditions were explained, and then, patients signed informed consent forms. Afterwards, a uterine cavity evacuation was performed, and 50–200 mg embryonic villus tissues were obtained, which were immediately rinsed with sterile normal saline until the villus tissues became clear. Samples were placed in a sterile centrifuge tube (1 mL), containing 75 mL preservation solution (2% alcohol), which were then labeled and put into the sample box and sent for testing immediately.
Chromosomal Examination of the Villus of Abortion Tissues and Detection of Maternal Blood Contamination
Chromosomal examination of the villus of abortion tissues and detection of maternal blood contamination were performed by Suzhou Tianhao Medical Examination Laboratory (Suzhou, China).
Statistic Analysis
SPSS 19.0 software (IBM, Armonk, NY, USA) was used for the statistical analysis. Qualitative data were described in terms of frequency (percentage), and a chi-square test was used to make a comparison between two groups. Quantitative data were presented as mean ± standard deviation (SD), and an independent t-test was utilized to make a comparison between two groups. P<0.05 was considered statistically significant.
Ethical Consideration
Our study adheres to the principles of the Helsinki Declaration and the rules of the ethical requirements of the Second Affiliated Hospital of Soochow University.
Results
Data of 516 Villus Samples of Patients with Spontaneous Abortion
The examination of 516 samples of spontaneous abortion tissues showed that the chromosomes of 222 samples were normal, while the chromosomes of 294 samples were abnormal, and the abnormality rate was 60.97%. Among 294 samples with chromosomal abnormalities, 136 (89.47%) samples had numerical chromosomal abnormalities, 15 (9.87%) samples had structural chromosomal abnormalities, and 1 (0.07%) sample had uniparental disomy (Figure 1).
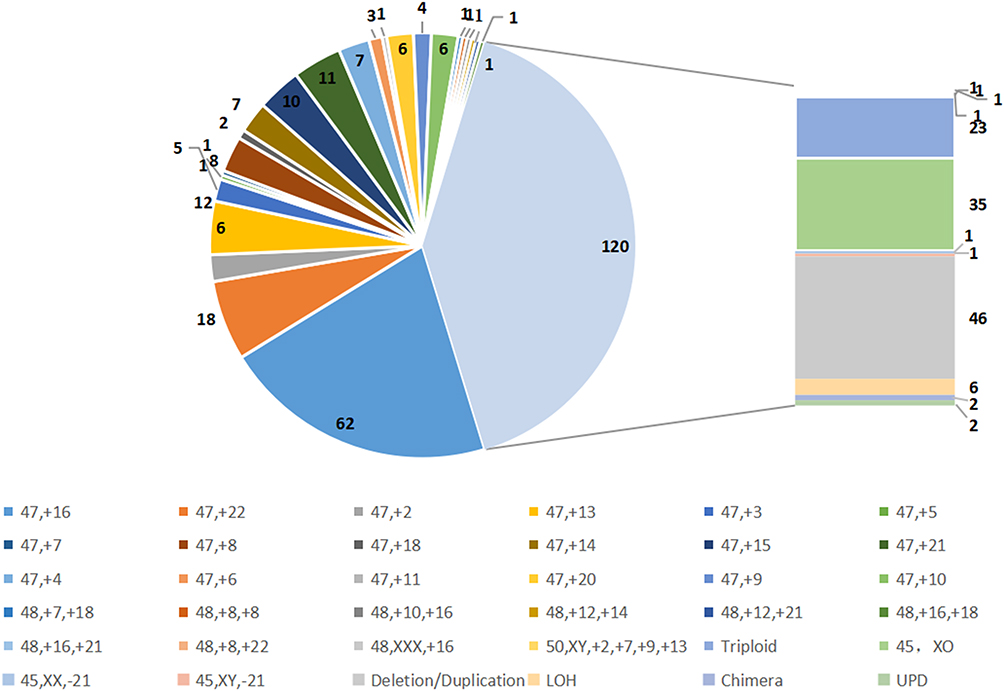 |
Figure 1 Analysis of the abnormal number of villus chromosomes detected in 294 patients. Abnormal distribution of chromosome number in abortion tissue of 294 patients, including 47, +16 (62 cases); 47, +22 (18 cases); 47, +13 (12 cases);47, +15 (10 cases);47, +21 (11 cases); Triploid (23 cases); 45, XO (35 cases); Deletion/Duplication(46 cases), and so on. |
Association Between Different Age Groups and Embryonic Karyotypes
The proportions of abnormal karyotypes were compared among different age groups (≤29, 30–35, and ≥36 years old) (Table 1).
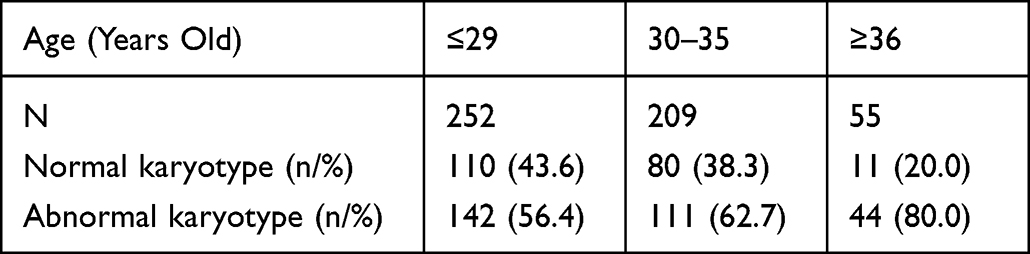 |
Table 1 Comparison of Proportions of Abnormal Karyotypes Among Different Age Groups |
Incidence of Chromosomal Abnormalities in Both Husband and Wife, and the Association with Embryonic Chromosomal Abnormalities
Of the 516 couples with spontaneous abortion, 308 couples voluntarily underwent peripheral blood chromosome analysis. The results showed that 56 couples had abnormality in one or both spouses, and the abnormality rate was 18.0%. Specifically, 16 couples were found with abnormalities in wife, 10 couples were found with abnormalities in husband, and 1 couple was found with abnormalities in both husband and wife. The rate of embryonic chromosomal abnormality in these 26 cases with chromosomal abnormalities was 100% (Table 2).
 |
Table 2 Chromosomal Abnormalities in Couples and Abnormal Embryonic Karyotypes |
Discussion
The etiology of spontaneous abortion is complex, while embryonic chromosomal abnormality is one of the main causes. Embryonic chromosomal abnormalities account for about 50–70% of all first trimester spontaneous abortions, of which numerical chromosomal abnormality (chromosomal aneuploidy) is the most important cause, including triploid, polyploidy, X monomer, etc.10
In the present study, HLPA test was performed for the villus tissues of embryos from 516 patients with spontaneous abortion who were treated in our hospital, of whom 294 cases had abnormal karyotypes, and the abnormality rate increased significantly. Specifically, the proportion of numerical chromosomal abnormality in abnormal karyotypes increased significantly, which mainly include triploid, 45, XO (turner syndrome), and so on, which was consistent with previously reported findings.11,12 Of the autosomal abnormalities, 16-trisomy was the most common abnormality, which had a relatively high lethality to embryonic development.13 Previous studies have shown that triploidy was mainly caused by random mutations, rather than pregnancy environment or inadequate prevention.14 45, XO, ie the sex chromosome contains only one X chromosome, is associated with turner syndrome (monosomy X), and it is also known as congenital ovarian hypoplasia.15 Moreover, 99% of patients with Turner syndrome experience spontaneous abortion during embryonic period, accounting for about 15% of first trimester spontaneous abortion cases. Turner syndrome is caused by non-separation of sex chromosomes during meiosis, and about 70% of nondisjunction occurs in the father. As most of these chromosomal abnormalities are new-onset random mutations, the risk of recurrence is very low.16 In the present study, structural chromosomal abnormalities were found in 44 patients, of whom 7 cases had duplication, deletion, translocation, and inversion in the chromosome of the father or mother. In addition, the abnormality of the chorionic villus chromosome of the embryos indicated that the embryonic chromosomal abnormality was inherited from the mother or father.
In the present study, patients were divided into three groups according to their age (ie, ≤29, 30–35, and ≥36 years old). The results showed that the rate of embryonic chromosomal abnormality was 56.4%, 62.7%, and 80.0% in the three groups, respectively. Therefore, the risk of aneuploidy was higher in pregnant women with older age, which could be one of the high-risk factors for embryonic chromosomal abnormalities.
Of the 516 couples with spontaneous abortion, 308 couples voluntarily participated in peripheral blood chromosome analysis, of whom 56 cases had abnormalities in one or both spouses, and the abnormality rate was 18.0%. The findings revealed that the presence of chromosomal abnormality in one or both parents could be one of the risk factors for the occurrence of embryonic chromosomal abnormalities. Several studies have confirmed that peripheral blood chromosomal abnormalities in one or both spouses could cause embryonic chromosomal abnormalities. However, such vertical inheritance was not the major cause of chromosomal abnormalities, while abnormalities in gametes of one or both parents, and chromosomal mutations during embryonic formation and development, were the main causes.17 Chromosomal mutations may be related to the age of maternal, paternal, environmental, and other factors.18,19
Conclusions
In conclusion, findings of the present study and previous studies suggested that embryonic chromosomal abnormalities were the major cause of first trimester spontaneous abortion. Therefore, it is of great significance to examine the chromosomes of the villus tissues of the abortion tissues when exploring the causes of spontaneous abortion, especially in couples with more than 2 spontaneous abortions. Therefore, examination of the karyotypes of the embryo chorionic villus may help understand the reasons of embryonic arrest, which could provide important guidance for more genetic counseling, particularly for patients with early spontaneous abortion, as well as improving the preconception preparation.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Youth Research Fund of the Second Affiliated Hospital of Soochow University (Grant No. SDFEYQN 1709) and The Open project of the State Key Laboratory of Radiation Medicine and Radiation Protection (Grant No. GZK1202108).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Griebel CP, Halvorsen J, Golemon TB, Day AA. Management of spontaneous abortion. Am Fam Physician. 2005;72(7):1243–1250.
2. Farquharson RG, Jauniaux E, Exalto N. Updated and revised nomenclature for description of early pregnancy events. Hum Reprod. 2005;20(11):3008–3011. doi:10.1093/humrep/dei167
3. Chen S, Liu D, Zhang J, et al. A copy number variation genotyping method for aneuploidy detection in spontaneous abortion specimens. Prenat Diagn. 2017;37(2):176–183. doi:10.1002/pd.4986
4. Yuan SM, Liao C, Li DZ, et al. Chorionic villus cell culture and karyotype analysis in 1 983 cases of spontaneous miscarriage. Zhonghua Fu Chan Ke Za Zhi. 2017;52(7):461–466. doi:10.3760/cma.j.issn.0529-567X.2017.07.006
5. Sugiura-Ogasawara M, Ozaki Y, Katano K, et al. Abnormal embryonic karyotype is the most frequent cause of recurrent miscarriage. Hum Reprod. 2012;27(8):2297–2303. doi:10.1093/humrep/des179
6. Xu C, Wang T, Liu C, et al. Noninvasive prenatal screening of fetal aneuploidy without massively parallel sequencing. Clin Chem. 2017;63(4):861–869. doi:10.1373/clinchem.2016.266247
7. Mao J, Wang H, Li H, et al. Genetic analysis of products of conception using a HLPA/SNP-array strategy. Mol Cytogenet. 2019;12:40. doi:10.1186/s13039-019-0452-2
8. Mccombie WR, Mcpherson JD, Mardis ER. Next-generation sequencing technologies. Cold Spring Harb Perspect Med. 2018;9(11):a036798. doi:10.1101/cshperspect.a036798
9. Wang Y, Zhou R, Jiang L, et al. Identification of chromosomal abnormalities in early pregnancy loss using a high-throughput ligation-dependent probe amplification-based assay. J Mol Diagn. 2021;23(1):38–45. doi:10.1016/j.jmoldx.2020.10.002
10. Du Y, Chen L, Lin J, et al. Chromosomal karyotype in chorionic villi of recurrent spontaneous abortion patients. Biosci Trends. 2018;12(1):32–39. doi:10.5582/bst.2017.01296
11. Soler A, Morales C, Mademont-Soler I, et al. Overview of chromosome abnormalities in first trimester miscarriages: a series of 1011 consecutive chorionic villi sample karyotypes. Cytogenet Genome Res. 2017;152(2):81–89. doi:10.1159/000477707
12. Zhang R, Chen X, Wang D, et al. Prevalence of chromosomal abnormalities identified by copy number variation sequencing in high-risk pregnancies, spontaneous abortions, and suspected genetic disorders. J Int Med Res. 2019;47(3):1169–1178. doi:10.1177/0300060518818020
13. Ohno M, Maeda T, Matsunobu A. A cytogenetic study of spontaneous abortions with direct analysis of chorionic villi. Obstet Gynecol. 1991;77(3):394–398.
14. Warburton D, Kline J, Stein Z, et al. Does the karyotype of a spontaneous abortion predict the karyotype of a subsequent abortion? Evidence from 273 women with two karyotyped spontaneous abortions. Am J Hum Genet. 1987;41(3):465–483.
15. Álvarez-Nava F, Lanes R. Epigenetics in turner syndrome. Clin Epigenetics. 2018;10:45. doi:10.1186/s13148-018-0477-0
16. Ogata T, Wakui K, Muroya K, et al. Microphthalmia with linear skin defects syndrome in a mosaic female infant with monosomy for the Xp22 region: molecular analysis of the Xp22 breakpoint and the X-inactivation pattern. Hum Genet. 1998;103(1):51–56. doi:10.1007/s004390050782
17. Yang L, Tao T, Zhao X, et al. Association between fetal chromosomal abnormalities and the frequency of spontaneous abortions. Exp Ther Med. 2020;19(4):2505–2510. doi:10.3892/etm.2020.8524
18. Yun Y, Lee S, So C, et al. Oocyte development and quality in young and old mice following exposure to atrazine. Environ Health Perspect. 2022;130(11):117007. doi:10.1289/EHP11343
19. du Fossé NA, van der Hoorn MP, van Lith JMM, le Cessie S, Lashley E. Advanced paternal age is associated with an increased risk of spontaneous miscarriage: a systematic review and meta-analysis. Hum Reprod Update. 2020;26(5):650–669. doi:10.1093/humupd/dmaa010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.