")
Back to Journals » International Journal of General Medicine » Volume 17
Clinical Presentation and 6-Month Outcomes of Patients with Peripartum Cardiomyopathy in Indonesia
Authors Prameswari HS , Dewi TI, Hasan M, Martanto E, Astuti A , Saboe A , Cool CJ
Received 30 October 2023
Accepted for publication 28 February 2024
Published 21 March 2024 Volume 2024:17 Pages 1073—1083
DOI https://doi.org/10.2147/IJGM.S447214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Hawani Sasmaya Prameswari, Triwedya Indra Dewi, Melawati Hasan, Erwan Martanto ,† Astri Astuti, Aninka Saboe, Charlotte Johanna Cool
Department of Cardiology and Vascular Medicine, Faculty of Medicine, Padjadjaran University, Bandung, West Java, Indonesia
†Erwan Martanto passed away on 17 August 2023
Correspondence: Hawani Sasmaya Prameswari, Department of Cardiology and Vascular Medicine, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia, Email [email protected]
Background: Due to the rarity of peripartum cardiomyopathy (PPCM) globally, baseline characteristic data for PPCM patients are still scarce. Therefore, this study aims to determine the baseline characteristics and 6-month outcomes of PPCM patients in Indonesia.
Methods: From January 2014 to December 2021, all PPCM patients aged ≥ 18 years who were admitted to Dr. Hasan Sadikin General Hospital in Bandung, Indonesia, participated in this single-center, prospective cohort study. All patients were re-evaluated within 6 months of PPCM diagnosis.
Results: A total of 138 patients with PPCM were admitted to Dr. Hasan Sadikin General Hospital in Bandung. The mean age of all patients was 30.4 ± 6.4 years old. Approximately 60% patients were multipara and had preeclampsia. All guideline-directed medical therapy for heart failure was received by most patients, excluding mineralocorticoid receptor antagonists (25.2%) and bromocriptine (14.1%). The neonatal mortality rate was 5.1%. Among those who survived, 61.2% had normal weight, 31.8% had low birth weight, and 7% had very low birth weight. At the 6-month follow-up, 6.7% of the patients died, 63.3% recovered, and 1.9% were rehospitalized.
Conclusion: The present study found a high incidence of PPCM in Indonesia. Our patients frequently had preeclampsia, which contributed to the higher rate of miscarriage and low birth weight. Our liberal use of beta-blockers and ACEi/ARB may have contributed to the higher 6-month recovery rate than that in other countries.
Keywords: peripartum cardiomyopathy, preeclampsia, PPCM, recovery, registry
Introduction
Peripartum cardiomyopathy (PPCM) is an uncommon form of heart failure (HF) defined by left ventricular (LV) systolic dysfunction and left ventricular ejection fraction (LVEF) less than 45% in women during pregnancy or within months following parturition.1,2 The global prevalence of this condition is estimated to be 144 events per 100,000 births.3 It varies markedly across regions, with the highest incidence in Nigeria (1 in 102 births)4 and the lowest prevalence in Japan (1 in 15.533 births).5
Although rare, and the diagnosis is primarily made by exclusion, PPCM is an important entity that cannot be easily overlooked as PPCM was considered highly fatal and accounted for 4% and 14% of maternal deaths in both developed and developing countries, respectively, according to a recent meta-analysis.6 Not to mention the devastating long-term consequences it had on previously healthy women, as the European Society of Cardiology (ESC) revealed that 54% of these patients had not fully recovered and 6% deceased after six months of follow-up.7
In 2020, the European Society of Cardiology (ESC) developed the largest PPCM registry, which recruited 739 patients with PPCM from several regions, including Europe, Asia-Pacific, Middle East, and Africa.7 However, owing to its rarity, PPCM data in most other countries, including China and Indonesia, are still scarce. As we completed the first full 6-month follow-up of patients with PPCM in Indonesia, which was initiated at Hasan Sadikin General Hospital, a tertiary referral hospital in the largest province in Indonesia, this study aimed to demonstrate the baseline characteristics and 6-month outcomes of patients with PPCM in Indonesia.
Methods
Study Design and Patient Selection
From January 2014 to December 2021, all PPCM patients aged ≥18 years who were admitted to Dr. Hasan Sadikin General Hospital in Bandung, Indonesia, participated in this single-center, prospective cohort study. All patients included in this study provided informed consent at the beginning of the study, and those who did not provide informed consent were excluded. This study was approved by the Medical Research Ethics Committee of Dr. Hasan Sadikin General Hospital, Bandung, Indonesia, in accordance with the principles outlined in the Declaration of Helsinki. Our exclusion criteria were as follows: (1) patients diagnosed with other causes of heart failure, (2) LVEF > 50%, and (3) patients who were lost to follow-up at the conclusion of the follow-up period.
Definition of Variables and Outcome
The diagnosis of PPCM was confirmed if the following criteria were fulfilled:2 (1) experienced congestive heart failure symptoms during the prepartum period or within several months after delivery, (2) no other possible etiologies of HF discovered by clinical examination and several auxiliary tests performed prior to the last month of pregnancy, and (3) LVEF <45%.
The baseline characteristics of consecutive patients were recorded when PPCM was initially diagnosed at the beginning of the study, including age, comorbidities (chronic hypertension, gestational hypertension, preeclampsia, and obesity), obstetric status (multiparity, twin pregnancy, and history of pregnancy resulting in fetal death), breastfeeding history, PPCM onset, clinical examination upon admission (body mass index (BMI) (calculated by body weight in kilograms divided by the square of the height in meters), New York Heart Association (NYHA) functional class, tachycardia (refers to a heart rate of more than 100 beats per minute), heart rate, and blood pressure), electrocardiographic (ECG) markers (left ventricular hypertrophy (LVH), corrected and prolonged QT (QTc) interval, echocardiographic parameters (left ventricular end-diastolic diameter (LVEDD), left ventricular end-systolic diameter (LVESD), interventricular septal end diastole (IVSD), left atrium diameter, mitral regurgitation, and reduced right ventricular (RV) function), and medication history (beta-blocker (BB), alpha-blocker, angiotensin-converting enzyme inhibitor (ACEi), angiotensin receptor blocker (ARB), mineralocorticoid receptor antagonist (MRA), diuretic, and bromocriptine).
The International Society for the Study of Hypertension in Pregnancy (ISSHP) guidelines were employed to establish the diagnosis of hypertensive disorders in pregnancy.8 Chronic hypertension was diagnosed if the patient had a history of hypertension prior to 20 weeks of pregnancy. Gestational hypertension was defined as hypertension that developed spontaneously during ≥20 weeks of pregnancy in the absence of proteinuria (urine albumin/creatinine ratio <30 mg/mmol) and haematological abnormalities. Preeclampsia was classified as gestational hypertension with proteinuria and/or evidence of haematological abnormalities including acute kidney injury (AKI), liver dysfunction, hemolysis, or thrombocytopenia. Obesity was defined as a body mass index of ≥30 kg/m2. Tachycardia was defined as a heart rate >100 beats per minute (bpm).
The severity of heart failure symptoms in patients with PPCM was classified according to the New York Heart Association (NYHA) functional classification (FC): Class I, asymptomatic diseases; Class II, mild symptoms with intense physical exercise; Class III, symptoms with daily activity; and Class IV, symptoms at rest.
A 12-lead electrocardiogram (ECG) was utilized to determine the QTc interval and left ventricular hypertrophy (LVH). The ECG employed Sokolow-Lyon criteria to detect LVH. The corrected QT was obtained by adjusting the interval using Bazett’s method. A prolonged QTc interval was characterized as having a duration ≥460 ms.
All echocardiographic variables were defined and calculated according to the American Society of Echocardiography guidelines.9,10 The LVEF was primarily measured using the Simpson Biplane. Teicholz was employed as an alternative approach to calculate LVEF in the presence of suboptimal images. Tricuspid annular plane systolic excursion (TAPSE), LVESD, LVEDD, and IVSD were assessed using M-mode echocardiography. Right ventricular function was categorized as normal if TAPSE ≥ 18 mm. Moderate and severe mitral regurgitation were categorized as significant mitral regurgitation.
All patients were re-evaluated within 6 months of PPCM diagnosis. Echocardiography was performed to calculate the LVEF, and LVEF ≥50% was regarded as the LV function recovery group.7
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to evaluate the data distribution. Categorical variables were presented as numbers and percentages. If the data distribution was normal according to the statistical analysis, numerical variables were expressed as mean ± SD, otherwise as median (interquartile range).
Results
Baseline Characteristics
The main results of this study are depicted in Figure 1. A total of 138 patients with PPCM were admitted to Dr. Hasan Sadikin General Hospital Bandung and were enrolled in this study. The mean age of all patients was 30.4 ± 6.4 years old. The majority of patients (68.1%) were multipara, with only 2.9% having a history of PPCM. Of the patients, 60.9% had preeclampsia. ECG of LVH was present in 34.1% of the patients. The mean hemoglobin level in our patients was 7.28 ± 1.14. Echocardiography characteristics showed mean LVEF of 32.6% ± 7.5%, LVEDd of 55.2 ± 7.4 mm, atrial size of 38.6 ± 6.5 mm, at least mild mitral regurgitation in 63.8%, at least mild pulmonary hypertension in 63.5%, reduced RV systolic function in 27.9% of the patients. Most patients presented prepartum (52.9%). Most patients received beta blockers (89.4%), ACEi/ARBs (99.2%), and diuretics (95.1%). Approximately a quarter of patients received mineralocorticoid receptor antagonists (25.2%), and fewer patients received bromocriptine (14.1%) (Table 1).
 |
Table 1 Baseline Characteristics of Patients with Peripartum Cardiomyopathy in Indonesia |
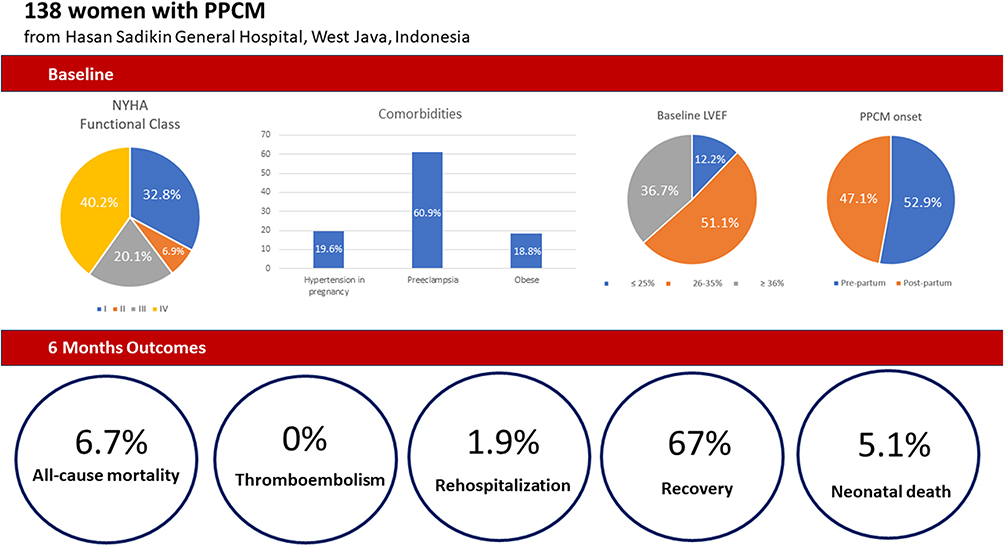 |
Figure 1 The main results of PPCM registry of Hasan Sadikin General Hospital, West Java, Indonesia. |
Of total participants, 47.1% of the patients underwent caesarean delivery. The neonatal mortality was 5.1%. Among those who survived, 61.2% had normal weight, 31.8% had low birth weight, and 7% had very low birth weight. The mean APGAR Score at 1 and 5 minutes was 6.5 ± 1.6 and 8.5 ± 1.7, respectively (Table 2).
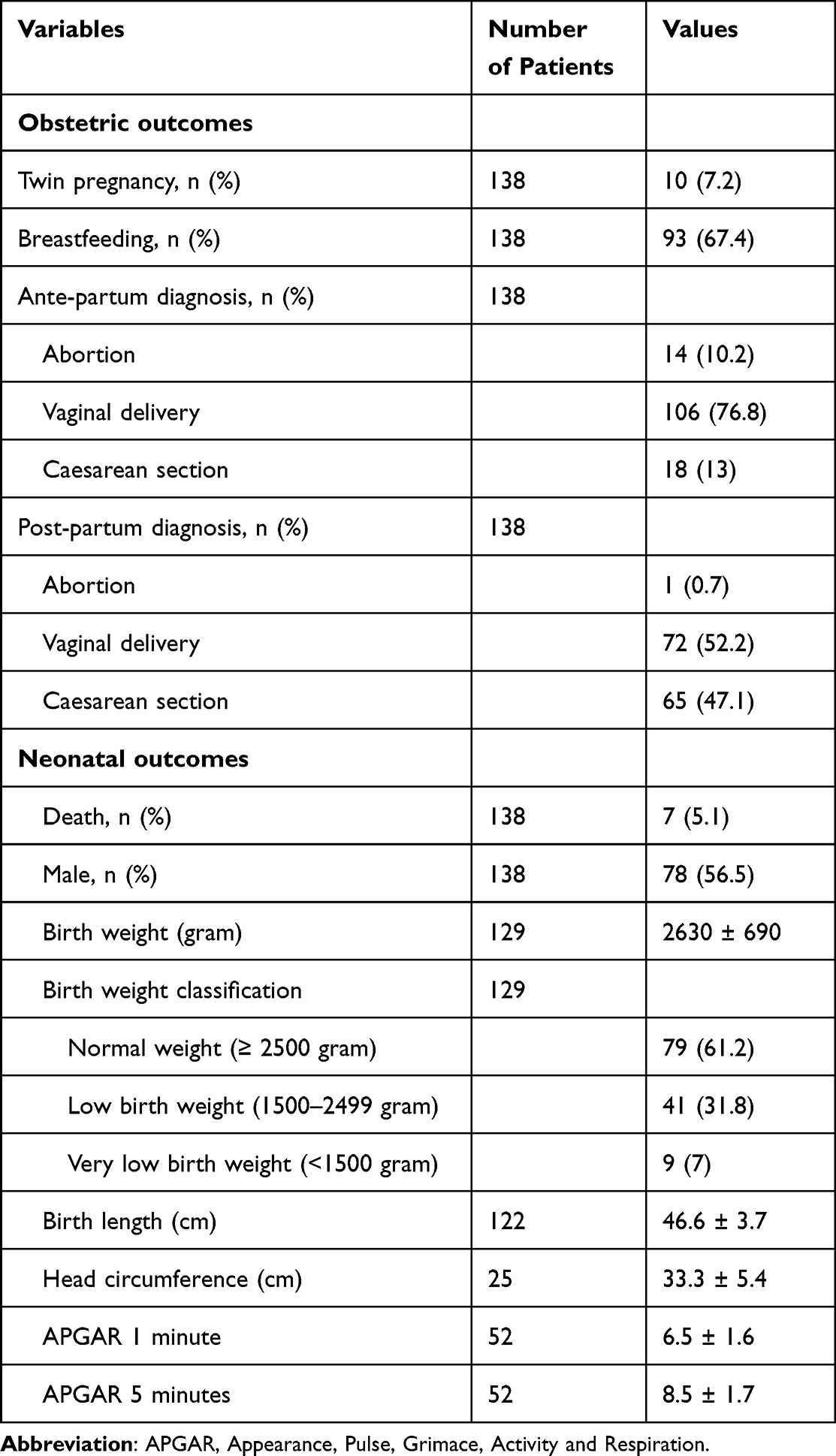 |
Table 2 Obstetric and Neonatal Outcomes of Patients with Peripartum Cardiomyopathy in Indonesia |
At 6-month follow-up, the mean LVEF and LVEDD (mm) were 52.6 ± 11.2 and 51.7 ± 6.3, respectively. About 6.7% of the patients died and 67% recovered, and 1.9% were rehospitalized. NYHA functional class I was in 78.3% of the patients (Table 3).
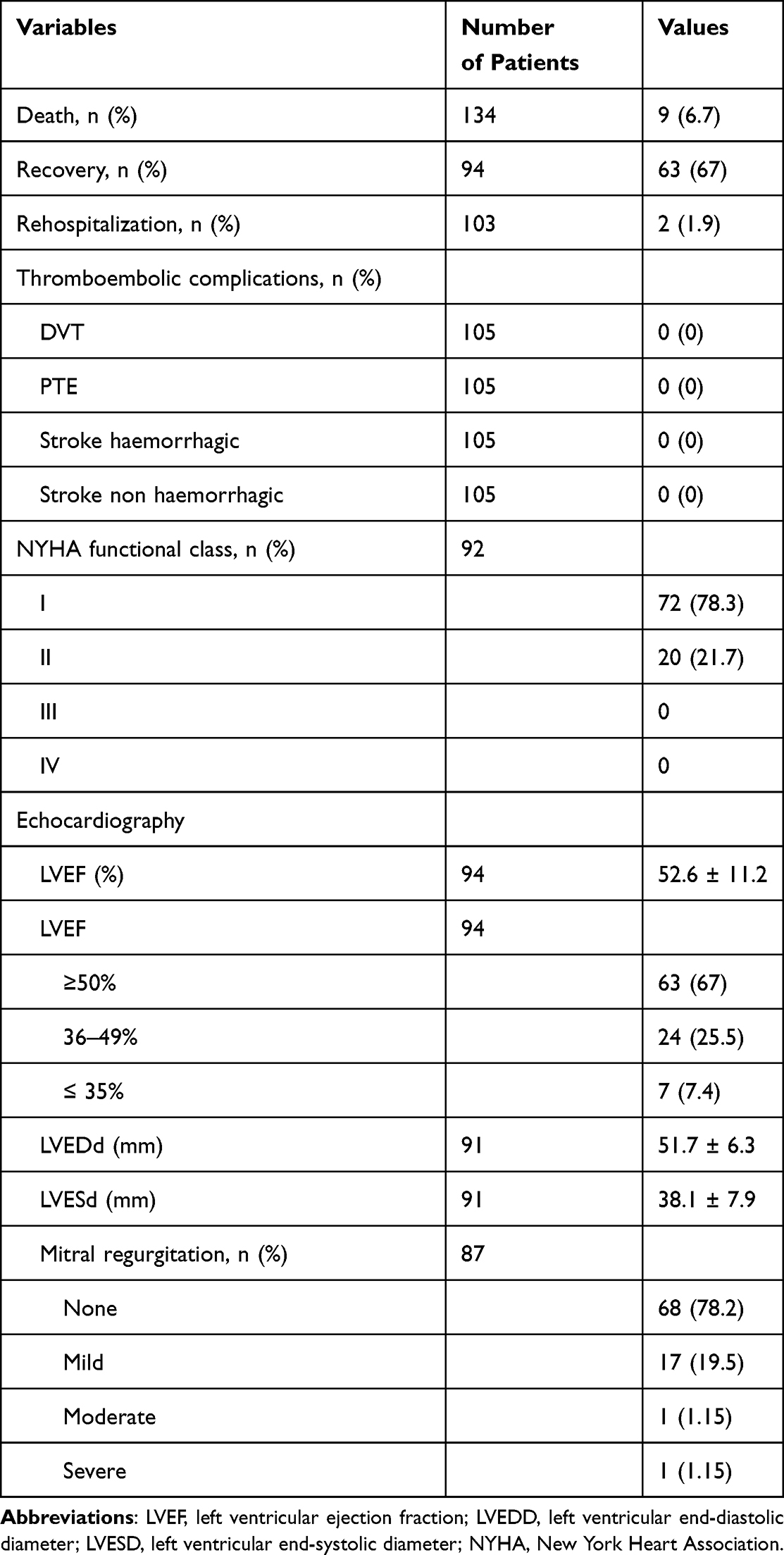 |
Table 3 6-Month Outcomes of Patients with Peripartum Cardiomyopathy in Indonesia |
Discussion
This is the first prospective study to report the characteristics and 6-month outcome of patients with PPCM in Indonesia. PPCM is a rare disease; however, the high birth rate in Indonesia contributes to the high number of caseloads. Although the data are only single-center data from a referral hospital in West Java, the number of patients was 138, which is approximately one-fifth of the size of ESC EORP PPCM data, which involved >100 national and affiliated member cardiac societies of the European Society of Cardiology over a similar period.7
The neonatal mortality rate was 5% in the ESC registry, similar to our data; however, 38.8% of the neonates in our registry had birth weights <2500 g compared to 28% in the ESC registry (25% in European Countries). In the antepartum PPCM diagnosis group, the rate of miscarriage was 10.2%, which is higher than that in the ESC EORP registry (5%) and Asia registry (2.3%).7,11 This may be explained by the higher number of patients with preeclampsia, and our data showed that 60.9% of PPCM patients had preeclampsia in the current pregnancy, which is present in only 25% and 18.4% of the EORP registry and Asian registry, respectively.7,11 Preeclampsia may contribute to intrauterine fetal growth retardation and intrauterine fetal death, thus contributing to low birth weight and miscarriage. Impact of preeclampsia on birth weight was also reflected in another study using data from ESC EORP PPCM registry.12 On the contrary, preeclampsia was proposed to have favorable outcome in terms of increasing the risk of recovery rate in PPCM patients. Patients with PPCM and hypertensive disorder had better baseline cardiac function, which may increase the possibility of recovery. The renin-aldosterone-angiotensin system (RAAS) has been shown to function differently in hypertensive disorders, especially preeclampsia, with increased angiotensin type II (AT II) receptor sensitivity and angiotensin type I (AT1) receptor overaction, which may increase the efficacy of RAAS inhibitor drugs. Thus, preeclampsia may contribute to a better outcome in terms of LV function recovery, but over a longer period, it may increase the risk of CV disease later in life.12
We observed a higher percentage of PPCM recovery at six months (67% vs 46%) than in the EORP registry. Our findings showed a similar number of deaths compared to EORP and Asian registries (6.7% vs 6% vs 6.9%).7,11 A systematic review of 47 studies (4875 patients from 60 countries) has an overall recovery rate of 44.4% at 6 months; thus, the recovery rate at our center was higher than the average.13 Regarding the use of medications, we prescribed beta-blockers (89.4 vs 81%) and ACEi/ARB (99.2 vs 85%) more often but prescribed MRA (25.2 vs 45%) less often and prescribed bromocriptine (14.1 vs 15%) at a similar rate. A study showed that patients with preeclampsia have a higher rate of PPCM recovery (57.5 vs 48.5), which is hypothesized that women with PPCM and concomitant hypertensive disorders have higher blood pressure, which may allow more aggressive optimization of heart failure therapies.12 Additionally, there may be two pathophysiological processes involved in the development of PPCM – the first is vascular, which is associated with higher recovery rate, and the second one is genetic, which is associated with persistent, dilated cardiomyopathy.12,14,15
This study has several limitations. First, since this was a single-center study, despite being conducted at a referral center for PPCM patients in West Java, Indonesia, it still cannot explain the disparities in racial outcomes, which are likely to be multifactorial, including potential genetic, environmental, and possible healthcare system differences. Second, because of the limited availability of these biomarkers in our facility, this study did not include cardiac biomarkers that have been recognized as parameters of LV function recovery in patients with PPCM, including B-type natriuretic peptide (BNP) and N-terminal (NT)-pro BNP (NT-pro BNP).16,17 We acknowledge that the disproportionate and small number of non-recovery cases might restrict the statistical power of this study.
In conclusion, this study demonstrates a high incidence of PPCM in Indonesia. Our patients frequently had preeclampsia, which contributed to the higher rate of miscarriage and low birth weight. Our liberal use of beta-blockers and ACEi/ARB, in which aggressive therapy may be due to concomitant preeclampsia, may have contributed to the higher 6-month recovery rate than that in other countries.
Ethical Approval
This study was approved by the Medical Research Ethics Committee of Dr. Hasan Sadikin General Hospital, West Java, Indonesia.
Acknowledgment
A portion of the participants enrolled in this study is part of the European Society of Cardiology EURObservational Research Programme PPCM Registry (ESC EORP PPCM Registry). We express our gratitude to Prof. Karen Sliwa and Prof. Johann Bauersachs as Chairs of the Executive Committee ESC EORP PPCM Registry. We acknowledge the late Erwan Martanto, MD, for his faithful generosity and insights shared with us within the process of writing this manuscript. We also would like to acknowledge Raymond Pranata, MD, and Iwan Cahyo Santosa Putra, MD, for their assistance in the writing and submission of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ricke-Hoch M, Pfeffer TJ, Hilfiker-Kleiner D. Peripartum cardiomyopathy: basic mechanisms and hope for new therapies. Cardiovas Res. 2020;116:520–531. doi:10.1093/cvr/cvz252
2. Bauersachs J, König T, van der Meer P, et al. Pathophysiology, diagnosis and management of peripartum cardiomyopathy: a position statement from the heart failure association of the European society of cardiology study group on peripartum cardiomyopathy. Europ J Heart Fail. 2019;21:827–843. doi:10.1002/ejhf.1493
3. Isogai T, Kamiya CA. Worldwide incidence of peripartum cardiomyopathy and overall maternal mortality. Int Heart J. 2019;60:503–511. doi:10.1536/ihj.18-729
4. Cenac A, Djibo A. Postpartum cardiac failure in Sudanese-Sahelian Africa: clinical prevalence in western Niger. Am J Trop Med Hyg. 1998;58:319–323. doi:10.4269/ajtmh.1998.58.319
5. Kamiya CA, Kitakaze M, Ishibashi-Ueda H, et al. Different characteristics of peripartum cardiomyopathy between patients complicated with and without hypertensive disorders. -Results from the Japanese Nationwide survey of peripartum cardiomyopathy-. Circ J. 2011;75:1975–1981. doi:10.1253/circj.CJ-10-1214
6. Kerpen K, Koutrolou-Sotiropoulou P, Zhu C, et al. Disparities in death rates in women with peripartum cardiomyopathy between advanced and developing countries: a systematic review and meta-analysis. Arch Cardiov Dis. 2019;112:187–198. doi:10.1016/j.acvd.2018.10.002
7. Sliwa K, Petrie MC, Van Der Meer P, et al. Clinical presentation, management, and 6-month outcomes in women with peripartum cardiomyopathy: an ESC EORP registry. Eur Heart J. 2020;41:3787–3797. doi:10.1093/eurheartj/ehaa455
8. Brown MA, Magee LA, Kenny LC, et al. Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension. 2018;72:24–43. doi:10.1161/HYPERTENSIONAHA.117.10803
9. Lang RM, Badano LP, Victor MA, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiog. 2015;28:1–39.e14. doi:10.1016/j.echo.2014.10.003
10. Zoghbi WA, Adams D, Bonow RO, et al. Recommendations for noninvasive evaluation of native valvular regurgitation: a report from the American society of echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. J Am Soc Echocardiog. 2017;30:303–371. doi:10.1016/j.echo.2017.01.007
11. Wu VC, Chen TH, Yeh JK, et al. Clinical outcomes of peripartum cardiomyopathy: a 15-year nationwide population-based study in Asia. Medicine. 2017;96:e8374. doi:10.1097/MD.0000000000008374
12. Jackson AM, Petrie MC, Frogoudaki A, et al. Hypertensive disorders in women with peripartum cardiomyopathy: insights from the <scp>ESC</scp> EORP PPCM Registry. Europ J Heart Fail. 2021;23:2058–2069. doi:10.1002/ejhf.2264
13. Hoevelmann J, Engel ME, Muller E, et al. Global prevalence of mortality and LV recovery in women with PPCM – a systematic review and meta-analysis. Eur Heart J. 2022;2022:43.
14. Davis MB, Arany Z, McNamara DM, Goland S, Elkayam U. Peripartum cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75:207–221. doi:10.1016/j.jacc.2019.11.014
15. Arany Z, Elkayam U. Peripartum cardiomyopathy. Circulation. 2016;133:1397–1409. doi:10.1161/CIRCULATIONAHA.115.020491
16. Hoevelmann J, Muller E, Azibani F, et al. Prognostic value of NT-proBNP for myocardial recovery in peripartum cardiomyopathy (PPCM). Clin Res Cardiol. 2021;110:1259–1269. doi:10.1007/s00392-021-01808-z
17. Biteker M, Özlek B, Özlek E, et al. Predictors of early and delayed recovery in peripartum cardiomyopathy: a prospective study of 52 Patients. J Matern Fetal Neonatal Med. 2020;33:390–397. doi:10.1080/14767058.2018.1494146
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.