Back to Journals » Clinical Epidemiology » Volume 18
Clinical Prediction Model for Target Lesion Revascularization Within One Year After Drug-Eluting Stent Implantation: Nationwide Analysis Within the Netherlands Heart Registration
Authors Derks L, Wanten DS ![]() , Van Beek KA, Arkenbout K, Maessen JG, Van Veghel DH, Houterman S
, Van Beek KA, Arkenbout K, Maessen JG, Van Veghel DH, Houterman S
Received 5 February 2026
Accepted for publication 4 April 2026
Published 10 July 2026 Volume 2026:18 586896
DOI https://doi.org/10.2147/CLEP.S586896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Lineke Derks,1,2 Daphne S Wanten,1 Konrad AJ Van Beek,3 Karin Arkenbout,4 Jos G Maessen,1,2 Dennis HPA Van Veghel,1 Saskia Houterman1
1Netherlands Heart Registration, Utrecht, the Netherlands; 2Cardiovascular Research Institute Maastricht (CARIM), Maastricht University, Maastricht, the Netherlands; 3Heart Centre, Catharina Hospital, Eindhoven, the Netherlands; 4Department of Cardiology, Tergooi MC, Hilversum, the Netherlands
Correspondence: Lineke Derks, Netherlands Heart Registration, Moreelsepark 1, Utrecht, 3511 EP, the Netherlands, Tel +31 0 88 2200900, Email [email protected]
Purpose: This study aimed to develop and validate a clinical prediction model for target lesion revascularization (TLR) at one-year follow-up in patients undergoing percutaneous coronary intervention (PCI) with implantation of a drug-eluting stent (DES).
Patients and Methods: Using real-world data from the Netherlands Heart Registration, we included patients treated with at least one DES between 2019 and October 2022. The study cohort comprised 96,758 patients from 29 centers, while a sub-cohort of 11,789 patients from 11 centers had additional procedural data. Multivariable logistic regression with backward stepwise selection was used for model development. Final coefficients were pooled across 20 imputed datasets, and separate models were built for both cohorts.
Results: The study cohort model included age, sex, interaction between age and sex, diabetes mellitus, renal insufficiency, multivessel disease, out-of-hospital cardiac arrest (OHCA), cardiogenic shock, previous myocardial infarction, previous coronary intervention, access site, number of treated vessels, PCI in the left main, and PCI in arterial or venous grafts. The optimism-corrected area under the curve (AUC) was 0.645 (95% confidence interval (CI): 0.633– 0.657). The sub-cohort model incorporated total stent length in the left anterior descending artery, arterial or venous grafts, and left main, along with renal insufficiency, previous coronary intervention, and OHCA, yielding an AUC of 0.662 (95% CI: 0.631– 0.693).
Conclusion: The developed models provide a basis for predicting one-year TLR using routinely collected data. Despite strong calibration, their modest discrimination suggests a need for more detailed variables and advanced modelling approaches to improve performance.
Keywords: percutaneous coronary intervention, target lesion revascularization, drug-eluting stents, risk assessment
Introduction
Coronary artery disease (CAD) is still the most leading cause of mortality and morbidity worldwide.1 Patients with CAD can be treated by revascularization with percutaneous coronary intervention (PCI) using stents.2
In recent decades several developments have contributed to improved clinical outcomes following PCI, including the introduction of drug eluting stents (DES) and optimized antiplatelet therapy strategies. Nevertheless, adverse events such as in-stent restenosis (ISR) and stent thrombosis still occur at clinically relevant rates.3,4 Moreover, these adverse events are frequently followed by complications associated with increased morbidity, including myocardial infarction (MI) and in some cases sudden cardiac death.5 Importantly, the occurrence of recurrent adverse cardiac events has a significant impact on quality of life and healthcare costs.6
Target lesion revascularization (TLR) is a commonly used treatment in patients with adverse events like ISR and stent thrombosis. Therefore, identifying patients at high risk of TLR is crucial, as this may help clinicians optimize treatment strategies and thereby improve patient prognosis. Earlier studies revealed stent-related characteristics such as length and diameter, as well as patient-related factors such as diabetes mellitus as predictors of TLR7–10 Incorporating important predictive factors in a clinical prediction model may facilitate early recognition of patients at increased risk of TLR and tailor their post-PCI follow-up treatment.
The aim of this study was to develop and validate a clinical prediction model for the occurrence of TLR at one year follow-up for patients undergoing PCI with DES implantation. The model was developed using real-world data from the nationwide PCI registry of the Netherlands Heart Registration (NHR) and included only factors that are readily available in clinical practice.
Methods
Study Population
Patients who underwent PCI with at least one DES implantation between 2019 till October 2022 in the Netherlands were included in the analysis. The following patients were excluded: 1) those undergoing transcatheter aortic valve implantation (TAVI) on the same day as the PCI, 2) those with an elective PCI procedure performed within 90 days prior or post TAVI, 3) patients who died within one year without experiencing TLR, and 4) patients treated with a stent other than DES.
Study Endpoint and Potential Predictors
The primary outcome was TLR within one year, defined as any repeat PCI of the initially treated target lesion. Potential predictor variables were selected based on clinical relevance and availability in routine practice after the index procedure and insights from existing literature on TLR after PCI. The method of selection of relevant variables within the NHR is described in detail in the paper of Timmermans et al11 These included: demographics (age (continuous), sex), comorbidities (renal insufficiency (estimated glomerular filtration rate (eGFR) < 60 or ≥ 60), diabetes mellitus, multivessel disease, chronic total occlusion (CTO), admission with cardiogenic shock, or admission with out-of-hospital cardiac arrest (OHCA)), medical history (previous MI, previous PCI, previous coronary artery bypass grafting (CABG)), interventional characteristics (PCI indication, access site, treated vessels, number of stents (continuous), maximum stent diameter (mm, continuous), total stent length (mm, continuous), use of calcium modification therapy, and use of intravascular imaging). All potential predictors were binary coded unless specified.
Data Source
For the current retrospective observational cohort study prospectively collected data registered within the NHR were used. The study was approved by the institutional review board Medical research Ethics Committees United (MEC-U), which originated from a collaboration between ten hospitals and one university, and was conducted in agreement with the principles of the Declaration of Helsinki (W19.270). A waiver for informed consent for analysis with the data of the NHR registry was obtained, as this retrospective study uses existing data from patients who were already registered for another purpose (quality of care). Therefore, this research is not subject to the Medical Research Involving Human Subjects Act (in Dutch: WMO). All data handling complied with applicable data protection and privacy regulations, including the General Data Protection Regulation (GDPR). Detailed information on the process of data acquisition, completeness, data quality and analysis of the NHR has been published previously.11,12 In short, all 29 centers in the Netherlands performing PCI procedures submit information about patient- and procedural characteristics, as well as outcomes for each intervention. The data dictionary for the PCI registry is available online via https://www.nhr.nl/handboeken/. Mortality data were obtained by checking the regional municipal administration registration (Basisregistratie Personen (BRP)). Follow-up was complete up to one year after PCI. Since 2020, the PCI registry was expanded with additional procedural-related variables, namely number of stents, stent length, use of imaging, and use of calcium modification therapy. A total of 11 centers collected this additional variable set. This is defined as the sub-cohort.
Statistical Analysis
Categorical data is presented as number and percentage and compared by Chi-square test. Continuous variables were evaluated for normality and presented as mean ± standard deviation (SD) or as median with interquartile range (IQR), depending on normality.
Univariable logistic regression analysis was performed to identify predictors associated with TLR at a significance threshold P-value < 0.10. Interactions between sex and age and between sex and diabetes mellitus on the outcome were considered.
Missing data were addressed using multiple imputation with 20 imputations; outcomes were not imputed. Separate imputation models were built for the study cohort and sub-cohort; using variables identified from the univariable analyses, TLR and mortality at one year follow-up.
Model development was performed using multivariable logistic regression analysis with backward stepwise selection and adhering to a rule of at least 10 outcome events per predictor variable. Final model coefficients were estimated by pooling across the 20 imputed sets. Separate models were built for the study cohort and the sub-cohort. As a sensitivity analysis separate models were built for acute (ST-elevation myocardial infarction (STEMI) and non-STEMI) and elective patients using backwards selection within the study cohort.
Apparent performance of the models was assessed via Brier score, area under the receiver operating characteristics (ROC) curve (AUC), and Hosmer-Lemeshow goodness-of-fit test. These performance indicators were computed separately for each imputed set and pooled where applicable. To estimate optimism, 1000 bootstrap samples were drawn from the first imputed set.
All statistical analyses were performed using R Statistical Software (version 4.4.3 R Core Team 2025).
Results
We included 96,758 patients (study cohort), and for 11,789 patients additional procedural-related information was available (sub-cohort) (Figure 1). Missing data was <5% for potential predictors, except for imaging and preparation techniques (38.4%). Incidence of TLR within one year was 2.2% and 2.5%, respectively.
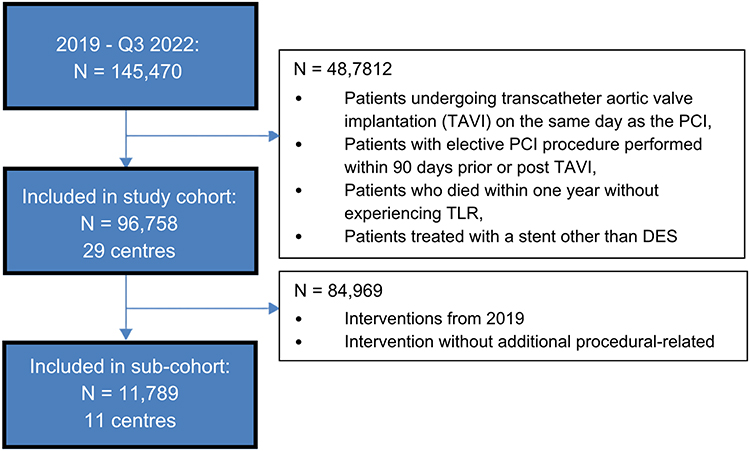 |
Figure 1 Flow-chart for selection of study cohort and sub-cohort of patients undergoing percutaneous coronary intervention (PCI) with drug-eluting stent implantation (DES). Abbreviation: TLR, target lesion revascularization. |
The characteristics of the study population are summarized in Table 1. The study cohort and sub-cohort were comparable on baseline characteristics. The sub-cohort showed, compared to the study cohort, a slightly higher prevalence of multivessel disease (52.1% vs. 51.1%) and a lower rate of renal insufficiency (eGFR < 60) (19.8% vs. 20.9%). Also, the procedural characteristics were comparable between the two cohorts, with some differences on access site, PCI indication, and incidence of treatment of the left main vessel.
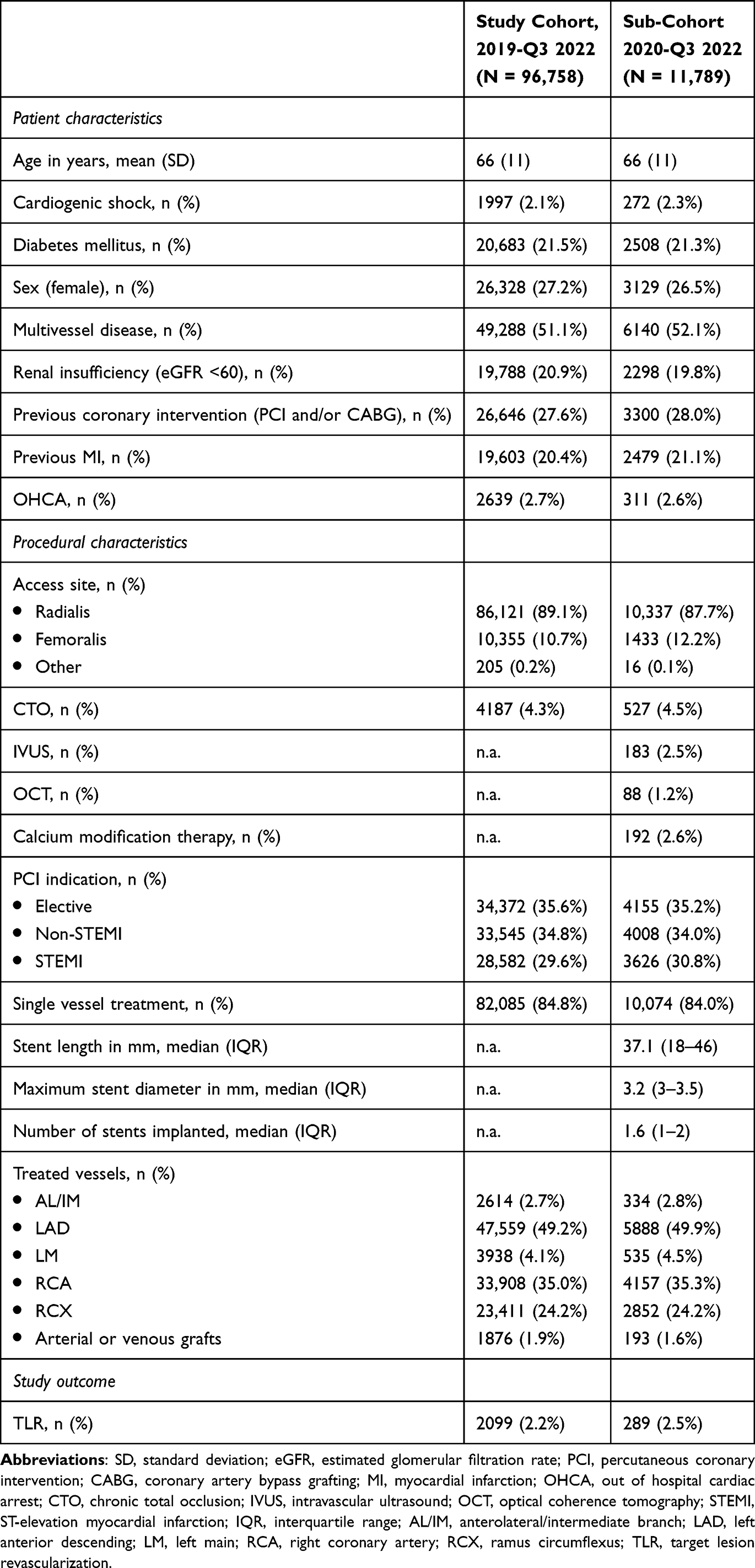 |
Table 1 Patient Characteristics, Procedural Characteristics and Outcomes Study Cohort (N = 96,758) and Sub-Cohort (N = 11,789) of Patients Undergoing Percutaneous Coronary Intervention with Drug-Eluting Stent Implantation |
In total, 17 potential predictors were selected based upon availability within the NHR database for the study cohort, and 20 potential predictors were available for the sub-cohort (Supplement Material 1 and Table S1). Univariable logistic regression analysis revealed the following characteristics to be associated (P-value < 0.1) with TLR within one year after PCI: age, interaction between age and sex, renal insufficiency (eGFR < 60), diabetes mellitus, multivessel disease, cardiogenic shock, OHCA, previous MI, previous coronary intervention, access site, PCI in left main vessel, PCI in arterial or venous grafts, number of treated vessels, and stent length (total and total length per treated vessel). Odds ratios and corresponding 95% confidence intervals (CIs) are presented in Table 2.
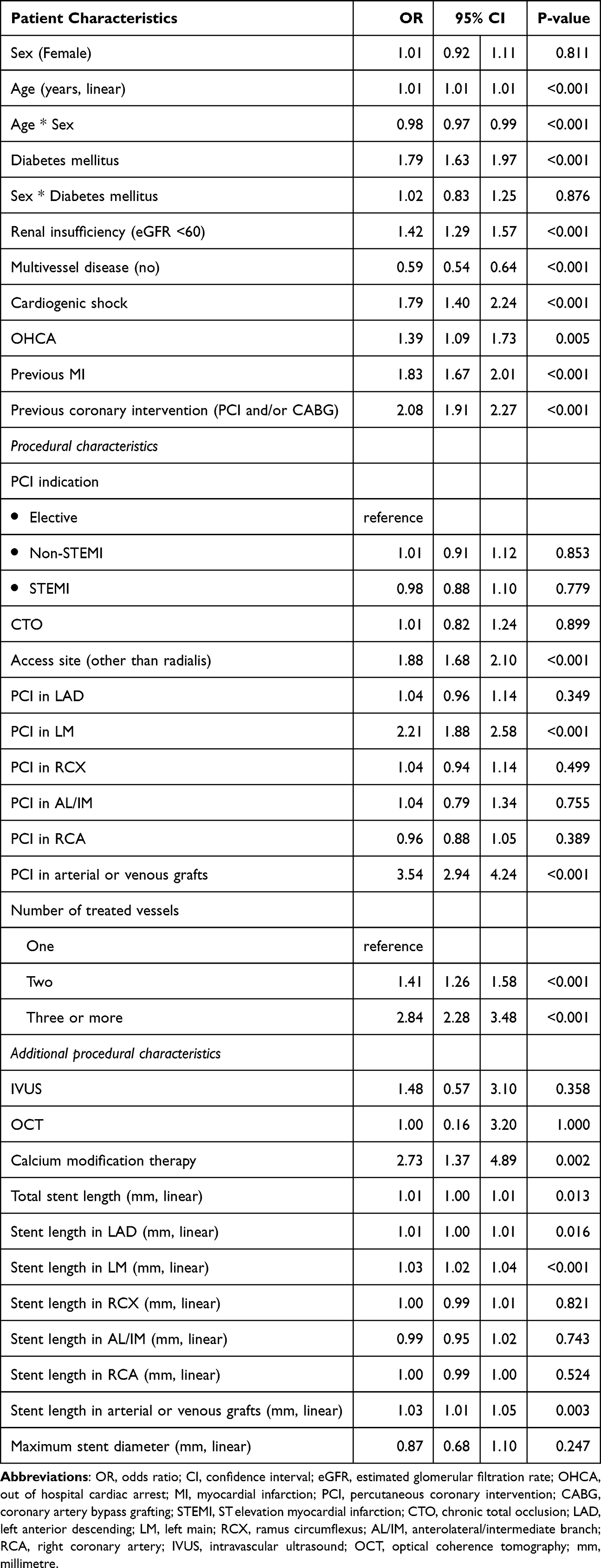 |
Table 2 Univariable Analysis of the Relation Between Target Lesion Revascularization (TLR) Within One Year After Percutaneous Coronary Intervention (PCI) and Patient or Procedural Characteristics |
Model Study Cohort
The final prediction model for TLR based on the study cohort included: sex, age, interaction between age and sex, renal insufficiency (eGFR < 60), multivessel disease, previous MI, number of treated vessels (two/three or more), OHCA, PCI in left main vessel, access site (other than radialis), diabetes mellitus, previous coronary intervention, cardiogenic shock and PCI in arterial or venous grafts. Model coefficients and odds ratios are presented in Table 3. The densities of the predicted probability are plotted in Figure 2A.
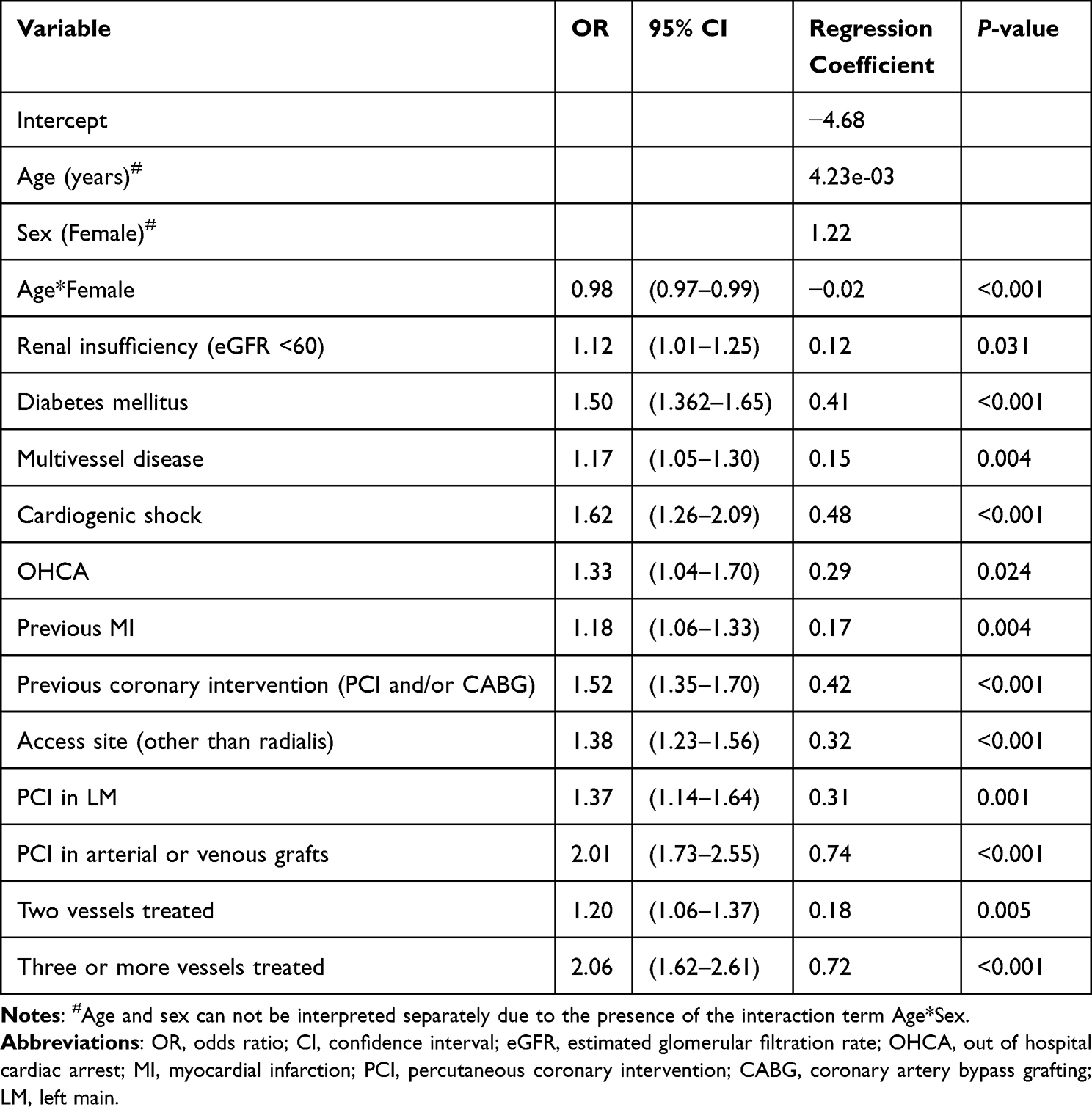 |
Table 3 Results of Multivariable Logistic Regression Analysis for Target Lesion Revascularization (TLR) Within One Year After Percutaneous Coronary Intervention (PCI), Study Cohort |
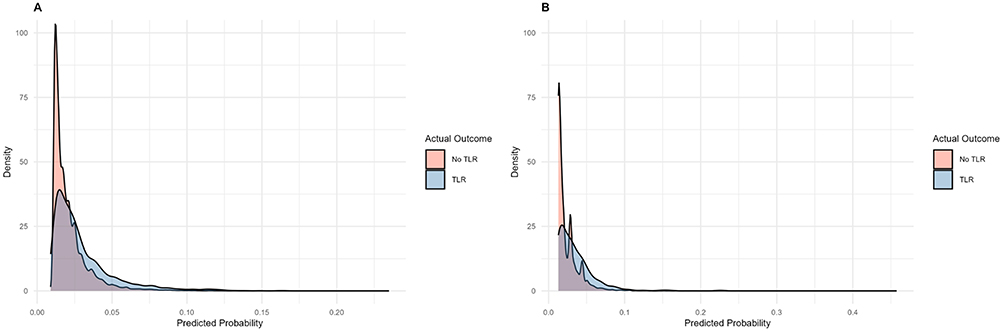 |
Figure 2 Density plot for predicted probability obtained from the logistic regression analysis for target lesion revascularization (TLR) within one year after percutaneous coronary intervention (PCI). Notes: (A) Results study cohort, (B) Results sub-cohort. |
Mean Brier score was 0.021 across imputations indicating strong accuracy of the model. The average AUC across imputations was 0.644 (95% CI: 0.644–0.644) indicating limited discriminatory power. The optimism corrected AUC based on the bootstrap estimate was 0.645 (95% CI: 0.633–0.657). The Hosmer-Lemeshow P-values ranged from 0.291 to 0.675 across imputations, with a mean of 0.525, suggesting good model calibration.
Sensitivity Analysis
Separate models were built for acute (STEMI and non-STEMI) and elective patients. The final model for acute patients included the same predictors as discovered in the study cohort (Supplement Material 2 and Table S2). For elective patients the following predictors were removed in the final model: renal insufficiency (eGFR < 60), OHCA, cardiogenic shock, previous MI, and PCI in left main vessel (Supplement Material 2 and Table S3).
Model Sub-Cohort
The final prediction model for TLR based on the sub-cohort included: renal insufficiency (eGFR < 60), previous coronary intervention, OHCA, total stent length in LAD, total stent length in arterial or venous grafts, and total stent length in the left main. Model coefficients and odds ratios are presented in Table 4. The densities of the predicted probability are plotted in Figure 2B.
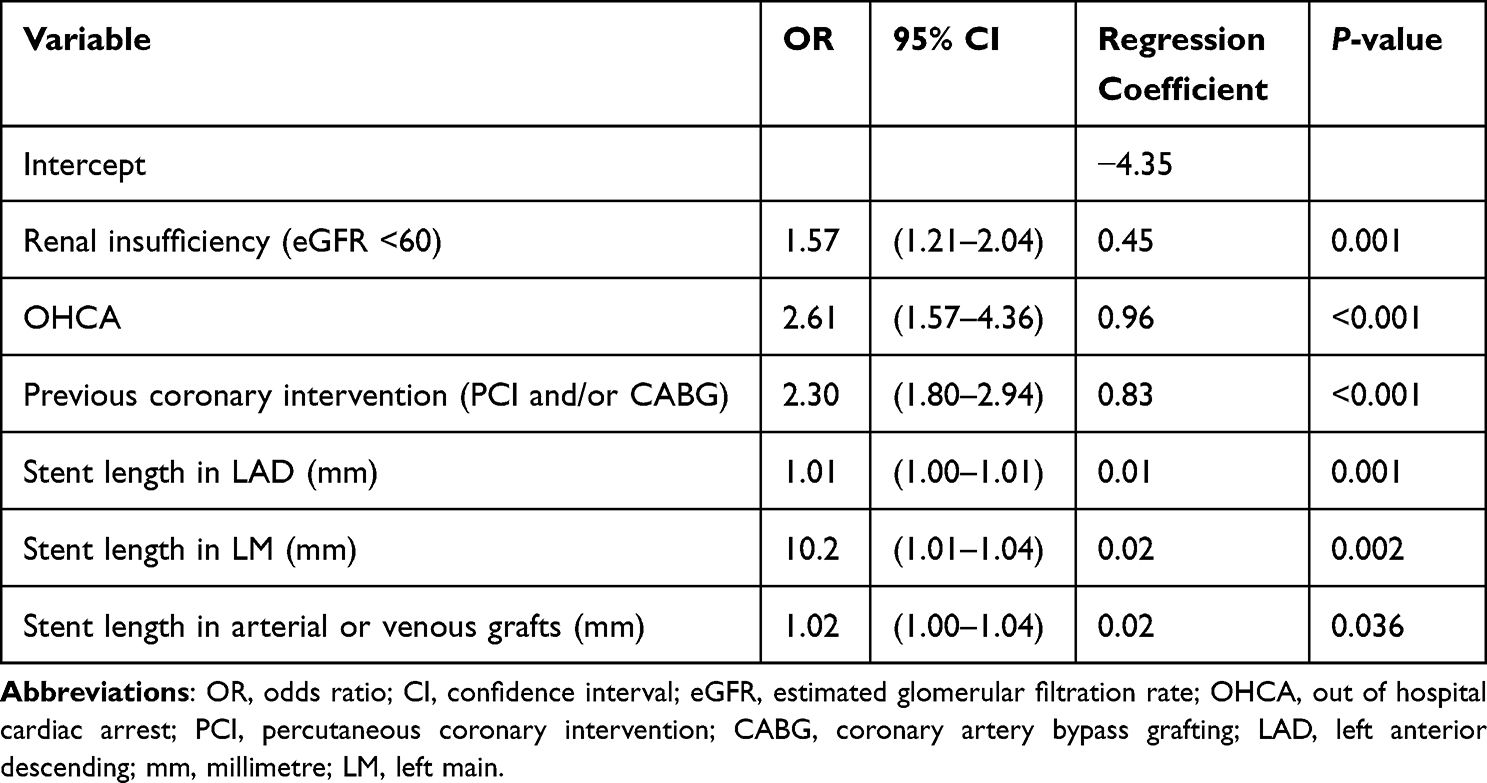 |
Table 4 Results of Multivariable Logistic Regression Analysis for Target Lesion Revascularization (TLR) Within One Year After Percutaneous Coronary Intervention (PCI), Sub-Cohort |
Mean Brier score was 0.024 across imputations indicating strong accuracy of the model. The average AUC across imputations was 0.662 (95% CI: 0.661–0.663) indicating limited discriminatory power. The optimism corrected AUC based on the bootstrap estimate was 0.662 (95% CI: 0.631–0.693). The Hosmer-Lemeshow P-values ranged from 0.025 to 0.615 across imputations, with a mean of 0.268, suggesting good model calibration.
Discussion
In this large-scale, registry-based, nationwide analysis of >95,000 patients undergoing a PCI with DES, we identified several key predictors of TLR one-year post-PCI and developed multiple models. These models provide a basis for predicting one-year TLR using routinely collected clinical and procedural data. Our models demonstrated good calibration with acceptable accuracy but limited discriminative power.
Our findings reaffirm several previously reported patient-related predictors of TLR, including age, sex, diabetes mellitus, multivessel disease, cardiogenic shock, renal insufficiency, and previous coronary intervention or MI.7,13–15 Notably, stent length in the treated vessels appears to be more influential than certain patient characteristics in our study, underscoring the importance of anatomic burden as a key determinant.16,17 This observation is consistent with other studies focusing on developing TLR prediction models. For instance, the model proposed by Stolker et al18 includes age and previous PCI as the only patient-related variables, while procedural factors such as left main PCI, arterial or venous grafts, and total stent length contribute significantly. Their model demonstrated comparable performance (c-statistic: 0.633). External validation using our dataset was not feasible due to the absence of minimum stent diameter data, only maximum stent diameter was available.
Another study performed by Dake et al19 developed a multivariate Cox regression model to predict TLR up to five years post-PCI. Their findings highlighted lesion-specific factors such as lesion length, Rutherford classification, and reference vessel diameter as having the greatest impact. Among patient characteristics, only age, sex, and prior intervention remained significant. Notably, they included total occlusion (TO) as a relevant factor, which encompasses both acute and chronic occlusions. In contrast, our study specifically focused on CTO, defined as occlusions persisting for more than three months, which were present in only 4.3% of our cohort and did not show a statistically significant association in univariate logistic regression analysis. This difference in definition and prevalence may partly explain the discrepancy in predictiveness. The J-CTO score,20 which reflects the complexity of CTOs, was unfortunately unavailable in both cohorts, precluding direct comparison. At the one-year mark, the model of Dake et al showed slightly better performance compared to ours (AUC: 0.668).
Our model complements existing risk scores such as GRACE Risk (2.0),21 TIMI Risk score,22,23 and CRUSADE,24 which are primarily designed to assess mortality and bleeding risk in acute coronary syndrome (ACS). These tools assist cardiologists in clinical decision-making regarding treatment strategy, for example, selecting the optimal antiplatelet regimen based on the CRUSADE score or prioritizing early revascularization for patients with a high GRACE score. In a similar vein, the models described in the current study can assist cardiologists in identifying patients at risk of TLR and tailoring their post-PCI management accordingly. The strength of our model is that it also accounts for procedural and anatomical factors, in contrast to the currently available risk scores, which lack this level of granularity.25
Nonetheless, the modest discriminatory performance of both our model and those previously published raises important questions about their clinical utility. As shown in the density plot of our study, there is a lot of overlap in the predicted probabilities, suggesting limited ability to differentiate between high- and low-risk patients. This indicates that the currently available variables may still not fully capture the biological and structural complexities underlying stent failure. Since identifying high-risk patients can help clinicians optimize treatment strategies and potentially improve patient prognosis, enhancing prediction models remains a critical goal. To achieve this, the integration of angiographic factors may be key to improving the accuracy of TLR risk assessment.26,27
Risk prediction may potentially be further enhanced by incorporating intracoronary imaging variables, which can provide more accurate estimations of true vessel and stent dimensions during PCI. However, most PCI procedures are currently still guided by angiography alone.28 Similarly, in our study the use of the two imaging modalities, intravascular ultrasound (IVUS) and optical coherence tomography (OCT) were used in only a minority of the PCIs (2.5% and 1.2%, respectively). Although several recent studies have reported associations between the use of intracoronary imaging during PCI and lower TLR rates in complex lesions, it remains uncertain whether such data would meaningfully improve model discrimination.14,29,30 As its application is expected to increase in the coming years, future availability of more intracoronary imaging data may allow for further model refinement.28
Target lesion calcification is associated with increased TLR risk, as calcified lesions are more prone to stent malapposition and underexpansion.31–33 Calcium modification techniques can be used to optimize lesion preparation and improve the likelihood of achieving full stent expansion after implantation.34 In our sub-cohort, the use of calcium modification was limited to 2.6%. Coronary calcification can be scored based on angiography and on intracoronary imaging, however, such detailed information was not available in the current study. Incorporating information on coronary calcification could potentially contribute to TLR risk estimation, but its incremental predictive value remains to be established.
Future studies should evaluate whether integrating lesion complexity, intracoronary imaging, and calcium modification techniques into predictive models offers meaningful improvements in the discriminatory ability towards stent failure and TLR. More advanced modelling approaches, such as random forest algorithms, may facilitate model development. However, it remains crucial to translate complex models into easily applicable risk scores for routine clinical use.
Study Limitations
Our study findings should be interpreted in light of several limitations. Firstly, due to the retrospective observational design of the study, not all potential predictive factors for TLR were available. Consequently, important variables may be missing from our model. Nevertheless, all included factors are accessible in clinical practice and thus readily applicable. Secondly, it was not possible to distinguish TLR due to in-stent restenosis. Other contributing factors may be relevant to this outcome. Since 1 July 2023, the PCI registry of the NHR has been updated to separately record in-stent restenosis, enabling future studies to differentiate between these outcomes. Thirdly, the one-year follow-up period limits our ability to predict later TLR events, occurring beyond this timeframe.
Conclusion
The developed models provide a basis for predicting one-year TLR following PCI with DES, using only routinely collected clinical and procedural data. Despite strong calibration, the modest discriminatory performance highlights the need for more detailed variables and advanced modelling approaches to improve performance. Future research should aim to evaluate if incorporate lesion complexity and imaging modalities, amongst others, enhance predictive accuracy, while ensuring models remain feasible for clinical implementation post-PCI.
Data Sharing Statement
The data underlying this article were provided by the NHR with the permission of the participating centers. Data are available upon reasonable request to the corresponding author and with permission of the NHR.
Acknowledgments
This study was carried out on behalf of the PCI Registration Committee of the Netherlands Heart Registration.
Collaborators
Members of the PCI Registration Committee of the Netherlands Heart Registration (NHR): Dr. J.M. Cheng (Albert Schweitzer ziekenhuis), Dr. M. Meuwissen (Amphia Ziekenhuis), Dr. M. Grundeken (Amsterdam UMC), Dr. R. Al Hashimi (Canisius Wilhelmina Ziekenhuis), Dr. K. Teeuwen (Catharina Ziekenhuis), Dr. S. Hubbers (Elisabeth-TweeStedenZiekenhuis), Dr. R. Diletti (Erasmus Medisch Centrum), Dhr. B.J. Sorgdrager (Haaglanden Medisch Centrum), Dhr. C.E. Schotborgh (HagaZiekenhuis), Dr. T. Meijers (Isala), Dr. J. Polad (Jeroen Bosch Ziekenhuis), Dr. R. Scherptong (Leids Universitair Medisch Centrum), Dr. E. Bakker (Maasstad Ziekenhuis), Prof. dr. A.J.W. van ‘t Hof (Maastricht UMC+, Zuyderland Medisch Centrum), Dhr. F. Spano (Meander Medisch Centrum), Dhr. J. Brouwer (Medisch Centrum Leeuwarden), Dhr. K.G. van Houwelingen (Medisch Spectrum Twente), Dr. M. Ewing (Noordwest Ziekenhuisgroep), Dr. G. Amoroso (Onze Lieve Vrouwe Gasthuis), Dhr. C. Camaro (Radboudumc), Dr. P.W. Danse (Rijnstate), Dr. K. Sjauw (St. Antonius Ziekenhuis), Dr. E.K. Arkenbout (Tergooi), Dhr. W.T. Ruifrok (Treant Zorggroep), Dr. A.O. Kraaijeveld (UMC Utrecht), Dr. E. Lipsic (Universitair Medisch Centrum Groningen), Dhr. L. Hoebers (Viecuri Medisch Centrum), Dhr. R. Erdem (ZorgSaam Ziekenhuis), Dr. L. Ruiters (Zuyderland Medisch Centrum).
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Murray CJL. Findings from the global burden of disease study 2021. Lancet. 2024;403(10440):2259–12. doi:10.1016/S0140-6736(24)00769-4
2. Byrne RA, Rossello X, Coughlan JJ, et al. ESC Guidelines for the management of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J. 2023;44(38):3720–3826. doi:10.1093/eurheartj/ehad191
3. Stolker JM, Cohen DJ, Kennedy KF, et al. Repeat revascularization after contemporary percutaneous coronary intervention: an evaluation of staged, target lesion, and other unplanned revascularization procedures during the first year. Circ Cardiovasc Interv. 2012;5(6):772–782. doi:10.1161/CIRCINTERVENTIONS.111.967802
4. Shlofmitz E, Iantorno M, Waksman R. Restenosis of drug-eluting stents. Circulation. 2019;12(8):e007023. doi:10.1161/CIRCINTERVENTIONS.118.007023
5. Madhavan MV, Kirtane AJ, Redfors B, et al. Stent-related adverse events >1 year after percutaneous coronary intervention. J Am Coll Cardiol. 2020;75(6):590–604. doi:10.1016/j.jacc.2019.11.058
6. Lui JNM, Williams C, Keng MJ, et al. Impact of new cardiovascular events on quality of life and hospital costs in people with cardiovascular disease in the United Kingdom and United States. J Am Heart Assoc. 2023;12(19):e030766. doi:10.1161/JAHA.123.030766
7. Choi IJ, Park HJ, Seo SM, et al. Predictors of early and late target lesion revascularization after drug-eluting stent implantation. J Interv Cardiol. 2013;26(2):137–144. doi:10.1111/joic.12001
8. Konigstein M, Madhavan MV, Ben-Yehuda O, et al. Incidence and predictors of target lesion failure in patients undergoing contemporary DES implantation-Individual patient data pooled analysis from 6 randomized controlled trials. Am Heart J. 2019;213:105–111. doi:10.1016/j.ahj.2019.03.011
9. Zheng C, Kang J, Park KW, et al. The predictors of target lesion revascularization and rate of in-stent restenosis in the second-generation drug-eluting stent era. J Interv Cardiol. 2019;2019:3270132. doi:10.1155/2019/3270132
10. Langhoff R, Arjumand J, Waliszewski M, et al. The real-world CONSEQUENT ALL COMERS study: predictors for target lesion revascularization and mortality in an unselected patient population. Angiology. 2021;72(8):724–732. doi:10.1177/0003319721997314
11. Timmermans MJC, Houterman S, Daeter ED, et al. Using real-world data to monitor and improve quality of care in coronary artery disease: results from the Netherlands Heart Registration. Neth Heart J. 2022;30(12):546–556. doi:10.1007/s12471-022-01672-0
12. Derks L, Medendorp NM, Houterman S, Umans V, Maessen JG, van Veghel D. Building a patient-centred nationwide integrated cardiac care registry: intermediate results from the Netherlands. Neth Heart J. 2024;32(6):228–237. doi:10.1007/s12471-024-01877-5
13. Kosmidou I, Leon MB, Zhang Y, et al. Long-term outcomes in women and men following percutaneous coronary intervention. J Am Coll Cardiol. 2020;75(14):1631–1640. doi:10.1016/j.jacc.2020.01.056
14. de Filippo O, Bruno F, Pinxterhuis TH, et al. Predictors of target lesion failure after treatment of left main, bifurcation, or chronic total occlusion lesions with ultrathin-strut drug-eluting coronary stents in the ULTRA registry. Catheter Cardiovasc Interv. 2023;102(2):221–232. doi:10.1002/ccd.30696
15. Xiang Q, Xiong XY, Liu S, et al. Risk prediction model for in-stent restenosis following PCI: a systematic review. Front Cardiovasc Med. 2024;11:1445076. doi:10.3389/fcvm.2024.1445076
16. Jiang Z, Tian L, Liu W, et al. Random forest vs. logistic regression: predicting angiographic in-stent restenosis after second-generation drug-eluting stent implantation. PLoS One. 2022;17(5):e0268757. doi:10.1371/journal.pone.0268757
17. Bujak K, Vidal-Cales P, Gabani R, et al. Relationship between stent length and very long-term target lesion failure following percutaneous coronary intervention for ST-elevation myocardial infarction in the drug-eluting stents era: insights from the EXAMINATION-EXTEND study. Am Heart J. 2023;264:72–82. doi:10.1016/j.ahj.2023.05.021
18. Stolker JM, Kennedy KF, Lindsey JB, et al. Predicting restenosis of drug-eluting stents placed in real-world clinical practice: derivation and validation of a risk model from the EVENT registry. Circ Cardiovasc Interv. 2010;3(4):327–334. doi:10.1161/CIRCINTERVENTIONS.110.946939
19. Dake MD, Fanelli F, Lottes AE, et al. Prediction model for freedom from TLR from a multi-study analysis of long-term results with the Zilver PTX drug-eluting peripheral stent. Cardiovasc Intervent Radiol. 2021;44(2):196–206. doi:10.1007/s00270-020-02648-6
20. Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC. 2011;4(2):213–221. doi:10.1016/j.jcin.2010.09.024
21. Fox KA, Dabbous OH, Goldberg RJ, et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). BMJ. 2006;333(7578):1091. doi:10.1136/bmj.38985.646481.55
22. Morrow DA, Antman EM, Charlesworth A, et al. TIMI risk score for ST-elevation myocardial infarction: a convenient, bedside, clinical score for risk assessment at presentation: an intravenous nPA for treatment of infarcting myocardium early II trial substudy. Circulation. 2000;102(17):2031–2037. doi:10.1161/01.CIR.102.17.2031
23. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284(7):835–842. doi:10.1001/jama.284.7.835
24. Subherwal S, Bach RG, Chen AY, et al. Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines) Bleeding Score. Circulation. 2009;119(14):1873–1882. doi:10.1161/CIRCULATIONAHA.108.828541
25. Kovacic JC, Limaye AM, Sartori S, et al. Comparison of six risk scores in patients with triple vessel coronary artery disease undergoing PCI: competing factors influence mortality, myocardial infarction, and target lesion revascularization. Catheter Cardiovasc Interv. 2013;82(6):855–868. doi:10.1002/ccd.25008
26. Yeh RW, Normand SL, Wolf RE, et al. Predicting the restenosis benefit of drug-eluting versus bare metal stents in percutaneous coronary intervention. Circulation. 2011;124(14):1557–1564. doi:10.1161/CIRCULATIONAHA.111.045229
27. Stolker JM, Cohen DJ, Kennedy KF, et al. Combining clinical and angiographic variables for estimating risk of target lesion revascularization after drug eluting stent placement. Cardiovasc Revasc Med. 2017;18(3):169–176. doi:10.1016/j.carrev.2016.12.014
28. Madder RD, Seth M, Sukul D, et al. Rates of Intracoronary Imaging Optimization in Contemporary Percutaneous Coronary Intervention: a Report From the BMC2 Registry. Circ Cardiovasc Interv. 2022;15(10):e012182. doi:10.1161/CIRCINTERVENTIONS.122.012182
29. Ali ZA, Landmesser U, Maehara A, et al. OCT-guided vs angiography-guided coronary stent implantation in complex lesions: an ILUMIEN IV substudy. J Am Coll Cardiol. 2024;84(4):368–378. doi:10.1016/j.jacc.2024.04.037
30. Stone GW, Christiansen EH, Ali ZA, et al. Intravascular imaging-guided coronary drug-eluting stent implantation: an updated network meta-analysis. Lancet. 2024;403(10429):824–837. doi:10.1016/S0140-6736(23)02454-6
31. Kawaguchi R, Tsurugaya H, Hoshizaki H, Toyama T, Oshima S, Taniguchi K. Impact of lesion calcification on clinical and angiographic outcome after sirolimus-eluting stent implantation in real-world patients. Cardiovasc Revasc Med. 2008;9(1):2–8. doi:10.1016/j.carrev.2007.07.004
32. Huang BT, Huang FY, Zuo ZL, et al. Target lesion calcification and risk of adverse outcomes in patients with drug-eluting stents. A meta-analysis. Herz. 2015;40(8):1097–1106. doi:10.1007/s00059-015-4324-1
33. Yabumoto N, Fujino M, Sugane H, et al. Clinical implications of calcification severity adjacent to calcified nodule: its association with first and recurrent risks of target lesion revascularization after percutaneous coronary intervention. Atherosclerosis. 2025;402:119116. doi:10.1016/j.atherosclerosis.2025.119116
34. Hamana T, Kawamori H, Toba T, et al. Predictors of target lesion revascularisation after drug-eluting stent implantation for calcified nodules: an optical coherence tomography study. Euro Intervention. 2023;19(2):e123–e133. doi:10.4244/EIJ-D-22-00836
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.