Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Clinical Practice Recommendations for Switching from Once-Monthly to Longer-Interval Paliperidone Palmitate Injectable in Schizophrenia Patients: A Modified Delphi Study in China
Authors Ma H, Cai J ![]() , Jia F, Zhou J, Zhou B, Zhang W, Ye C
, Jia F, Zhou J, Zhou B, Zhang W, Ye C ![]() , Jia M, Si T
, Jia M, Si T
Received 7 November 2025
Accepted for publication 10 February 2026
Published 28 February 2026 Volume 2026:22 579943
DOI https://doi.org/10.2147/NDT.S579943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Hong Ma,1 Jun Cai,2 Fujun Jia,3 Jiansong Zhou,4 Bo Zhou,5 Wanyi Zhang,6 Chong Ye,6 Miaomiao Jia,6 Tianmei Si1
1Department of Psychiatry, Peking University Institute of Mental Health (Sixth Hospital), NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Beijing, People’s Republic of China; 2Department of Psychiatry, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Mental Health Branch, China Hospital Development Institute, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 3Department of Psychiatry, Guangdong Mental Health Center, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 4Department of Psychiatry, National Clinical Research Center for Mental Disorders, The Second Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China; 5Department of Psychiatry, Sichuan Provincial Center for Mental Health, Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Key Laboratory of Psychosomatic Medicine, Chinese Academy of Medical Sciences, Chengdu, Sichuan, People’s Republic of China; 6Medical Affairs, Johnson & Johnson, Beijing, People’s Republic of China
Correspondence: Tianmei Si, Department of Psychiatry, Peking University Institute of Mental Health (Sixth Hospital), NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Huayuanbeilu 51#, Haidian District, Beijing, 100191, People’s Republic of China, Tel +86 13910987793, Email [email protected]
Purpose: Schizophrenia is a chronic mental disorder with substantial socioeconomic burden. Long-acting injectable antipsychotics (LAIs) demonstrate superior efficacy over oral antipsychotics in reducing relapse and improving adherence. Switching from short-interval LAIs (such as paliperidone palmitate one-month formulation, PP1M) to longer-intervals LAIs (like paliperidone palmitate three-month and six-month formulations) offers additional benefits to disease outcome. This modified Delphi study aimed to explore clinical consensus on switching strategies to longer-interval LAIs.
Patients and Methods: A steering committee of six psychiatrists experienced LAIs treatment in schizophrenia guided questionnaire design and consensus alignment. Thirteen panelists participated in two Delphi rounds. A targeted literature review (TLR) was conducted to generate key topics, preliminary statements and open-ended questions for steering committee interviews. A total of 37 statements were finalized for Delphi. Two Delphi rounds were conducted via one-on-one interviews (Nov–Dec 2024). Each statement was rated following a nine-point Likert scale. Measures of central tendency and variation were calculated. Consensus levels were categorized as “Strong/Moderate/Nearing/No Consensus”. Qualitative analyses were performed to refine statements. A final virtual meeting with steering committee confirmed consensus.
Results: In the two Delphi rounds, 35 statements reached strong consensus, one moderate consensus, and one nearing consensus. After reviewed by the six steering committee experts, four semantically statements were removed, yielding a final set of 33 consensus statements. Intraclass correlation coefficient improved from 0.674 to 0.751.
Conclusion: Final consensus was reached on 33 statements across five domains: clinical necessity, target patient populations, switching strategy, long-term disease management, factors influencing treatment willingness. It presents the first expert consensus in China on longer-interval LAIs usage in schizophrenia, offering evidence-informed guidance for patient selection, switching strategies and long-term disease management to promote standardized clinical use.
Keywords: long-acting injectable, schizophrenia, clinical consensus, switching strategy, Delphi process, paliperidone palmitate
Introduction
Schizophrenia, a chronic and severe psychiatric disorder exerts a profound impact on both individuals and society, often resulting in marked impairments in social functioning.1,2 The lifetime prevalence of schizophrenia in China is 0.6% and has imposed considerable direct medical costs related to hospitalizations, outpatient visits, medications, and rehabilitation services, alongside substantial indirect costs including lost productivity, caregiver burden, and social management expenses.3–5 The most important contributor to the substantial burden is the recurrent relapses of the disorder. 33.4% of the patients report relapse during the first year following discharge, and 82% of patients experiencing relapse within five years of initial diagnosis.6–8 Each relapse causes irreversible brain damage,9 making the illness more resistance to treatment, hindering patients’ ability to regain their previous level of functioning, and concurrently increase the risk of mortality.10–13
Medication non-adherence in schizophrenia contributes significantly to the recurrent relapses and disease burden.14 To address these challenges and enable more reliable monitoring of adherence, long-acting injectable (LAI) antipsychotics were developed, with an extended-release mechanism, significantly reduces the risk of relapse and improves long-term outcomes.15–17 Multiple real-world studies have demonstrated that patients who switched from monthly formulation LAI (such as paliperidone palmitate one-month formulation, PP1M) to longer-interval LAI (acting duration greater than one month, such as paliperidone palmitate three-month formulation PP3M and six-month formulation PP6M) demonstrate lower risk of relapse, reduced psychiatric hospitalizations, and increased treatment persistence.18–21 While maintaining symptom stability, treatment with longer-interval formulations is associated with a significant improvement in social functioning, better quality of life (QoL) and decreased perceived stigma,22 help patients recovery to their pre-illness life.23
Despite the substantial benefits of LAIs, their current overall utilization in China remains relatively low. In China, the long-acting injectables (LAIs) approved for schizophrenia include paliperidone palmitate (PP1M, PP3M and PP6M), aripiprazole once-monthly LAI, risperidone microspheres (every 2 weeks), and first-generation decanoate options such as haloperidol decanoate and fluphenazine/flupentixol decanoate.24 A 2020 multi-national study examining LAI prescribing patterns across 15 countries/regions in Asia reported that the use of LAIs in China was only 0.66%, far below the regional average of 17.9%.25 The number of patients who could benefit from longer-interval LAIs is consequently reduced, as they must first achieve stabilization with monthly LAIs prior to transitioning. Paliperidone palmitate is currently the only LAI in China available in a longer-interval formulation, other LAIs are approved only for shorter dosing intervals. The indication for PP3M is for patients who have been adequately treated with PP1M for at least 4 months, while PP6M is restricted for patients who have been adequately treated with PP3M for at least 3 months.
At present, there is an absence of standardized guidelines or expert consensus in China specifically addressing the use of longer-interval LAIs, including criteria for patient selection, switching strategies, how to monitor and manage post-switch variability, and how to communicate to enhance acceptance. To address this, the present study employed a structured, three-step modified Delphi panel method to systematically establish expert consensus on key clinical aspects of switching from monthly formulation LAIs to longer-interval LAIs in the treatment of schizophrenia. By addressing key decision challenges when switching to longer interval LAIs–such as the clinical necessity of extended intervals, patient suitability, practical switching approaches, long-term post-switch management, and determinants of treatment willingness and acceptance, this study aims to offer a reference for future practice and the potential adoption of other extended-interval formulations in China.
Methods
Study Design
The modified Delphi study approach was a structured process systematically gathering expert opinions with anonymity, diversity, and efficiency to reach a focused and well-considered consensus. The process comprised two panel rounds with expert panelists, followed by an in-depth consensus meeting with the steering committee to finalize agreement (Figure 1). A three-step modified Delphi panel study method was used to collect and aggregate expert opinions on clinical practice of switching patients with schizophrenia to longer-interval LAIs, comprising two panel rounds with expert panelists, followed by an in-depth consensus meeting with the steering committee to finalize agreement (Figure 1).
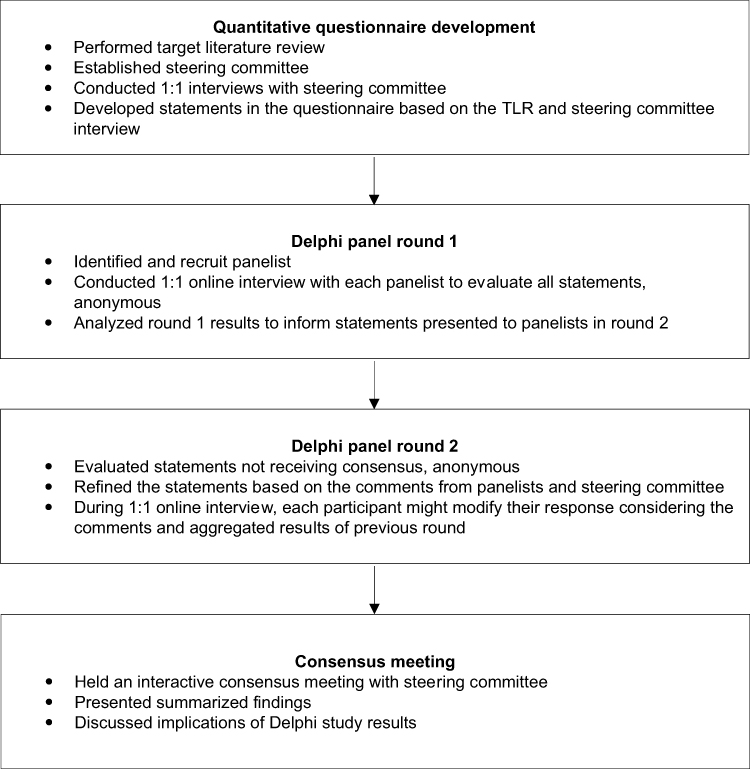 |
Figure 1 Modified Delphi framework. |
The opinions of experts on our topic were collected using a Delphi questionnaire, with statements categorized into five key domains, including clinical benefits, target patient population, switching strategies, long-term disease management, and factors influencing treatment willingness. These domains were selected aiming to address the existing knowledge gaps and ensure safe and effective implementation. Initially, the statements were generated through targeted literature review and discussion with a steering committee, which is formed by six psychiatrists with expertise in schizophrenia and LAIs that provided input on questionnaire design, recommended potential panelists, and assisted in survey development. Further details regarding the identification and selection criteria for steering committee members are provided in Supplementary Material 1. These statements were subsequently rated anonymously across two iterative rounds to assess the level of consensus and were finalized during the consensus meeting.
Panelist Selection
To reach the target sample of 12, as per the recommended sample size of 5–20 individuals,26 potential panelists were identified through a review of recent guidelines, publications and conferences related to schizophrenia treatment, or through recommendations by the steering committee.
Panelists were screened according to the following inclusion criteria:
- Psychiatrists with more than 5 years’ experience of schizophrenia diagnosis, treatment, and management.
- Extensive experience with PP3M usage (having managed more than 15 patients using PP3M in the last 3 years).
- Meeting at least one of the following inclusion criteria (over the past 5 years):
- Author/co-author of a publication on schizophrenia in major journals.
- Presented papers or spoken at a regional, national, or international conference on schizophrenia.
- Actively provided training relevant to schizophrenia at academic institutions.
- Involved in the development of current and/or historical clinical guidelines for schizophrenia diagnosis and/or treatment management.
- Actively involved in a psychiatry society or association focused on schizophrenia, such as Chinese schizophrenia Coordination Group (CSCG) or relevant clinical body.
- Currently practicing in China.
Target Literature Review (TLR) for Delphi Questionnaire Development and Consensus Definition
The research group conducted a targeted literature review to generate an initial list of key topics related to longer-interval LAIs and generated preliminary statements and open-ended research questions for the SC interview and discussion. This TLR captured current literature related to LAIs such as PP1M, PP3M, and PP6M for schizophrenia patients, including randomized clinical trials (RCTs), systematic reviews, meta-analysis, guidelines, as well as any further research literature from January 2004 to the start date. Searches were conducted across English databases, including PubMed, Cochrane, and Embase, as well as Chinese local databases, including WanFang and CNKI. In the article selection process for the target literature review, a total of 1692 articles were retrieved through the initial search. After removing 546 duplicates and excluding 252 articles based on title and abstract screening, 136 articles were assessed in full text, and 97 studies were ultimately included for data extraction. The search strategy was structured around the PICOST (Patient, Intervention, Comparator, Outcome, Study type, and Time period) framework, and the details were provided in Supplementary Material 2.
The findings of the TLR served as the foundation for these discussions and were used to elicit in-depth feedback through one-on-one interviews. A total number of 37 statements for the Round 1 survey were then created by reviewing literature and incorporating feedback from the steering committee regarding clinical accuracy, clarity, and practicality for the virtual survey. The statements were categorized into five sections: clinical necessity and potential benefits of longer-interval LAIs, target patients, switching strategies, long-term disease management after switching, and factors influencing treatment willingness. Each statement was to be scored by panelists according to a nine-point Likert scale quantifying the level of panelists’ agreement with the statement. The level of consensus was categorized as “Strong Consensus (≥80% of panelists rating as 7–9 & Median ≥8),” “Moderate Consensus (≥70% but <80% of panelists rating as 7–9 & Median ≥7 but <8),” “Nearing Consensus (≥60% but <70% of panelists rating as 7–9 & Median ≥6 but <7),” or “No Consensus (<60% of panelists rating as 7–9 & Not applicable)”.
Delphi Panels
In this study, a modified Delphi panel study was carried out in two rounds. The Delphi panel was conducted via one-on-one virtual interview to ensure the quality of collected data and facilitate discussion of statements. After providing consent to participate in the study, each panelist will be provided with a personalized Email link to join in the virtual one-on-one meeting for the survey. Considering potential dropout during the panel circulation, fifteen panelists were planned to be recruited in the first round, with a minimum target of twelve panelists completing the survey to proceed to the second-round panel.
In the first round, statements that have achieved consensus were included in the final list of consensus statements. For statements reaching “Moderate Consensus” or “Nearing Consensus”, modifications were made based on feedback from the panelists with validation by the steering committee. Statements classified as “No Consensus” were considered to have failed to reach agreement and were therefore excluded.
In the second round, statements where consensus was not completely achieved in the first round (including “Moderate Consensus” or “Nearing Consensus”) or those impacted by supplementary evidence and explanation were revised based on the feedback provided by panel experts in the previous round. Each revised statement from the first round was presented along with the aggregate ratings and comments from each expert panel member in the first round of the modified Delphi panel consultation.
Once both rounds of the survey were completed, a moderated virtual meeting took place to encourage interactive discussions among the steering committee. This meeting aimed to validate the findings and pinpoint areas of agreement as well as other clinically relevant issues. The consolidated responses and analyses from both rounds were presented to enable the steering committee to cast votes on statements still lacked consensus in the second round. Upon the final discussion and voting session, a comprehensive report summarizing the objectives, methods, final consensus statements, and conclusions was created and shared with the steering committee and the expert panel.
Data Analysis
Quantitative responses from each Delphi round were analyzed using descriptive statistics, including measures of central tendency (median) and dispersion (range). Categorical data were summarized using counts and proportions. The coefficient of variation (CV) was calculated to assess response consistency across rounds. The intraclass correlation coefficient (ICC) was used to assess the rating consistency among the experts within each round. SPSS and Microsoft Excel® were used for quantitative data analysis in this study.
In parallel, the comments provided by the expert panelists in the two rounds of the modified Delphi panel study were analyzed qualitatively, including panelists’ recognition, revision suggestions and whether they were consistent with clinical practice on each statement. Various categories of comments were established after reviewing the comments provided in the first Delphi panels. Two research group members independently reviewed all the comments provided in each Delphi panel round and grouped them according to the established categories. The research group further discussed the grouped comments with the SC and updated the statements in the Delphi questionnaire accordingly.
Results
Basic Information on the SC Experts and Panelists
The steering committee was composed of six professors from major psychiatric institutions located in North, East, South, Central, and Southwest China. All SC experts are nationally recognized experts in schizophrenia and the clinical application of long-acting injectable antipsychotics. The Delphi panelists consisted of 13 physicians from 10 institutions across six major cities in China, including Beijing, Shanghai, Guangzhou, Hangzhou, Tianjin, Changsha, and Nanchang. All panelists had substantial clinical experience with PP3M over the past three years. Their roles ranged from Associate Chief Physician to Chief Physician, and the number of PP3M cases managed per expert varied from 15 to over 100. All 13 experts participated in both rounds of the Delphi study. The study deliberately engaged experienced clinicians from these hospitals to ensure the depth and reliability of clinical insights.
Quantitative Analysis Results for Delphi Panels
In the first round, the coefficient of variation for all statements ranged from 0.042 to 0.226, with an average of 0.102, all indicating acceptable levels of variability. In the second round, the CV ranged from 0 to 0.179, with a lower average of 0.072 demonstrating improved consistency compared to the first round.
The intraclass correlation coefficient (ICC) was 0.674 (p < 0.001) in the first round. In the second round, the experts’ ratings for each research question or statement were relatively consistent, and no additions or deletions were proposed for the existing statements. The ICC for the second round was 0.751 (p < 0.001), which indicates that the experts reached a higher consistency.
Detailed scoring for each statement in the two rounds was provided in Supplementary Material 3.
Consensus Reached After Qualitative Analysis
A total of 37 statements were presented to the panelists across two Delphi rounds. With 35 statements reached the minimum level of agreement (≥80% of panelists rating as 7–9) to be considered a consensus, one statement achieved moderate consensus (≥70% but <80% of panelists rating as 7–9), and one statement achieved nearing consensus (≥60% but <70% of panelists rating as 7–9). During the online Expert Consensus Meeting, steering committee experts conducted an in-depth discussion on the statements that were widely debated or discussed during the two rounds of the Delphi consultation. After discussion and agreement with the six steering committee experts, four statements were removed due to semantic overlap, and consensus was ultimately reached in 33 statements. The finalized statements are detailed in Tables 1–5.
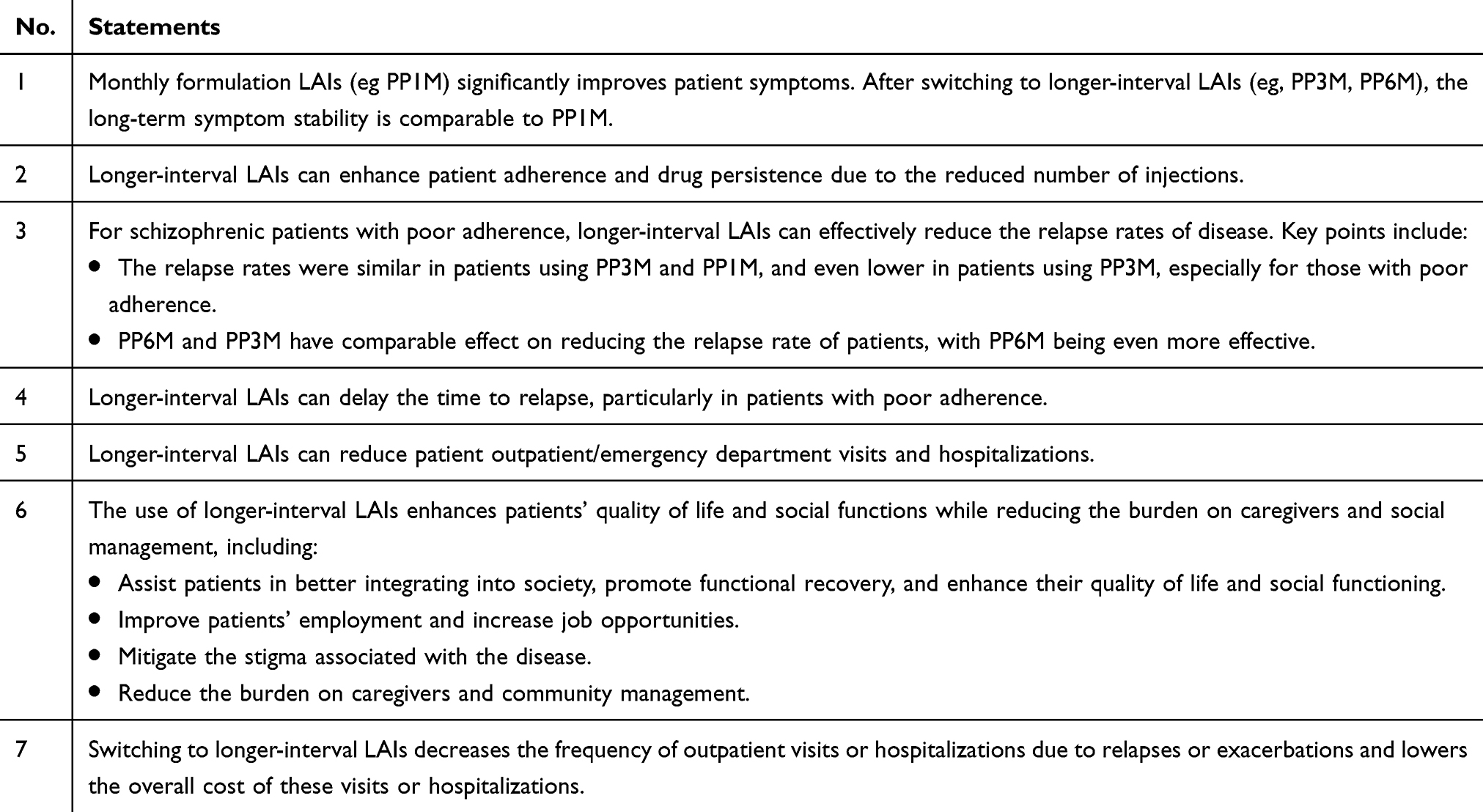 |
Table 1 Consensus on the Clinical Necessity of Longer-Interval LAIs |
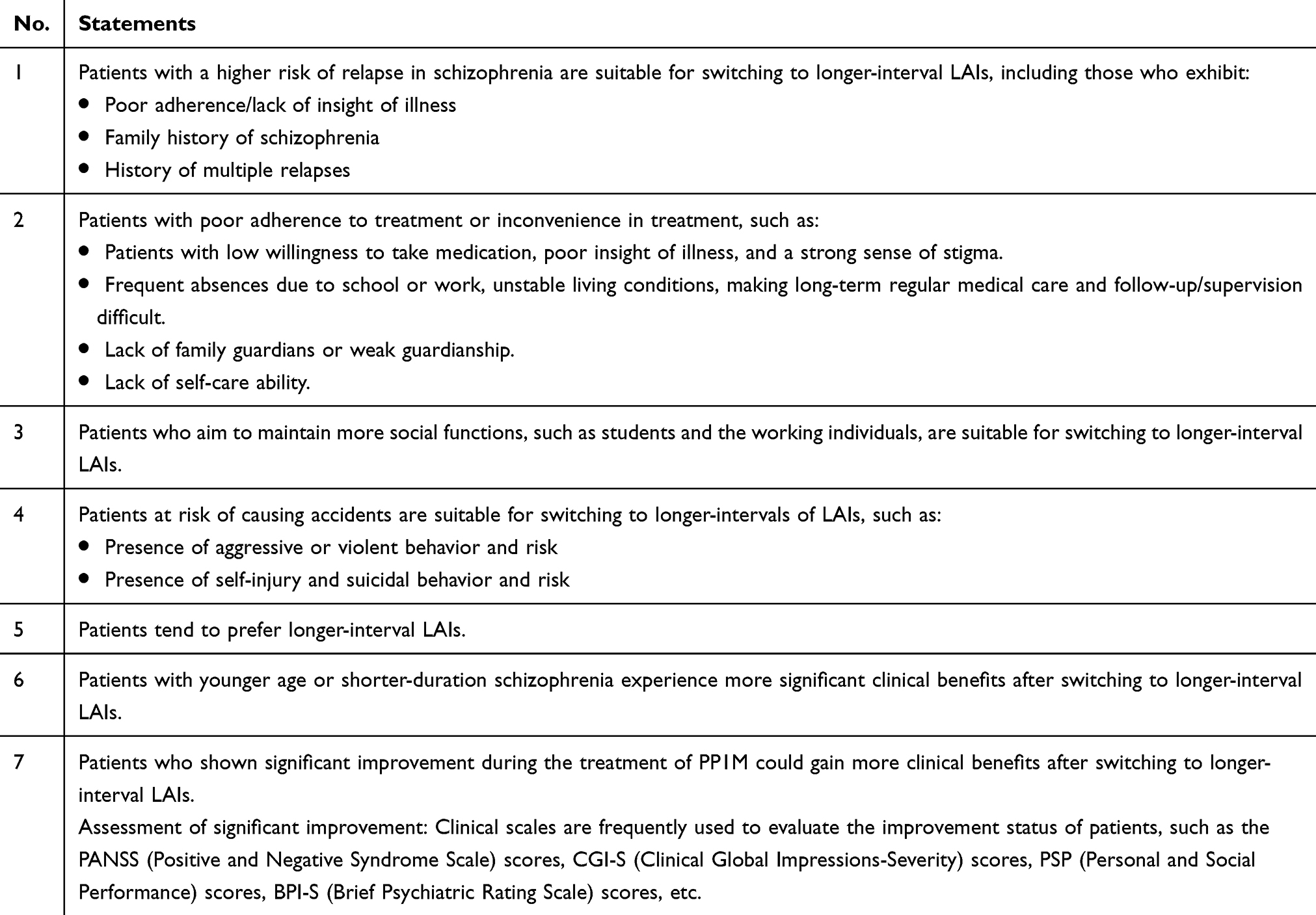 |
Table 2 Consensus on the Target Population for Longer-Interval LAIs |
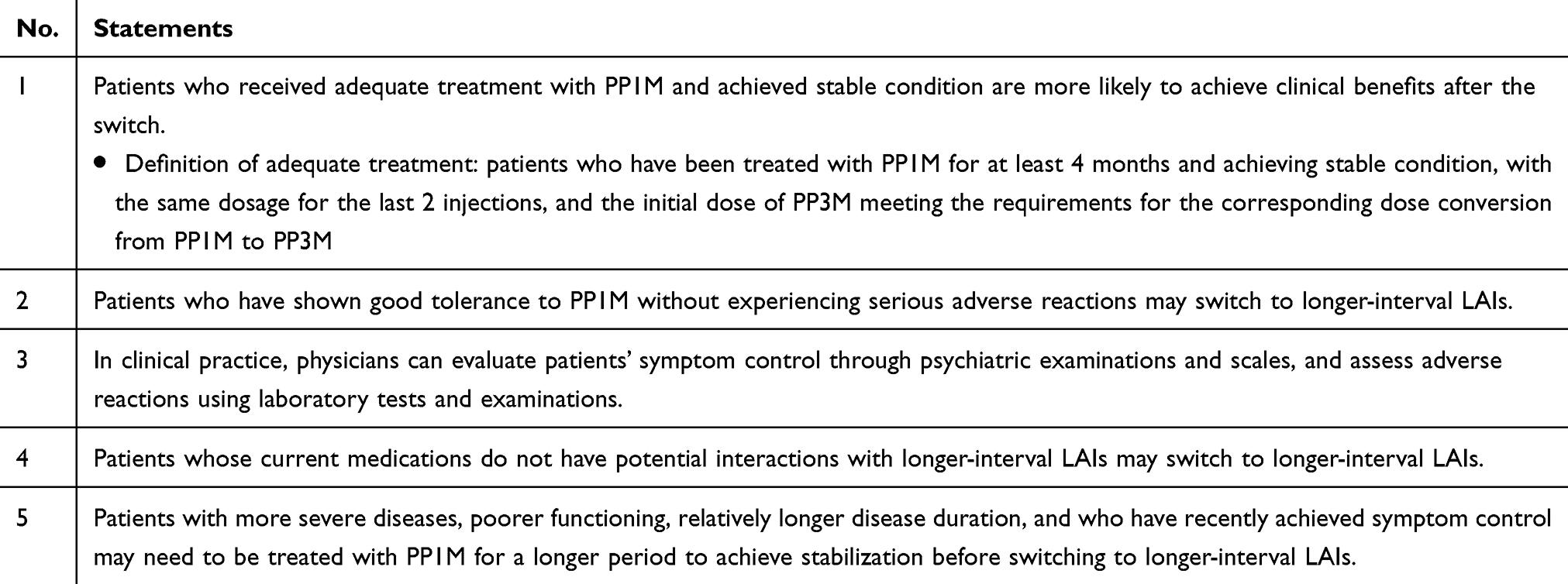 |
Table 3 Consensus on the Switching Strategies for Longer-Interval LAIs |
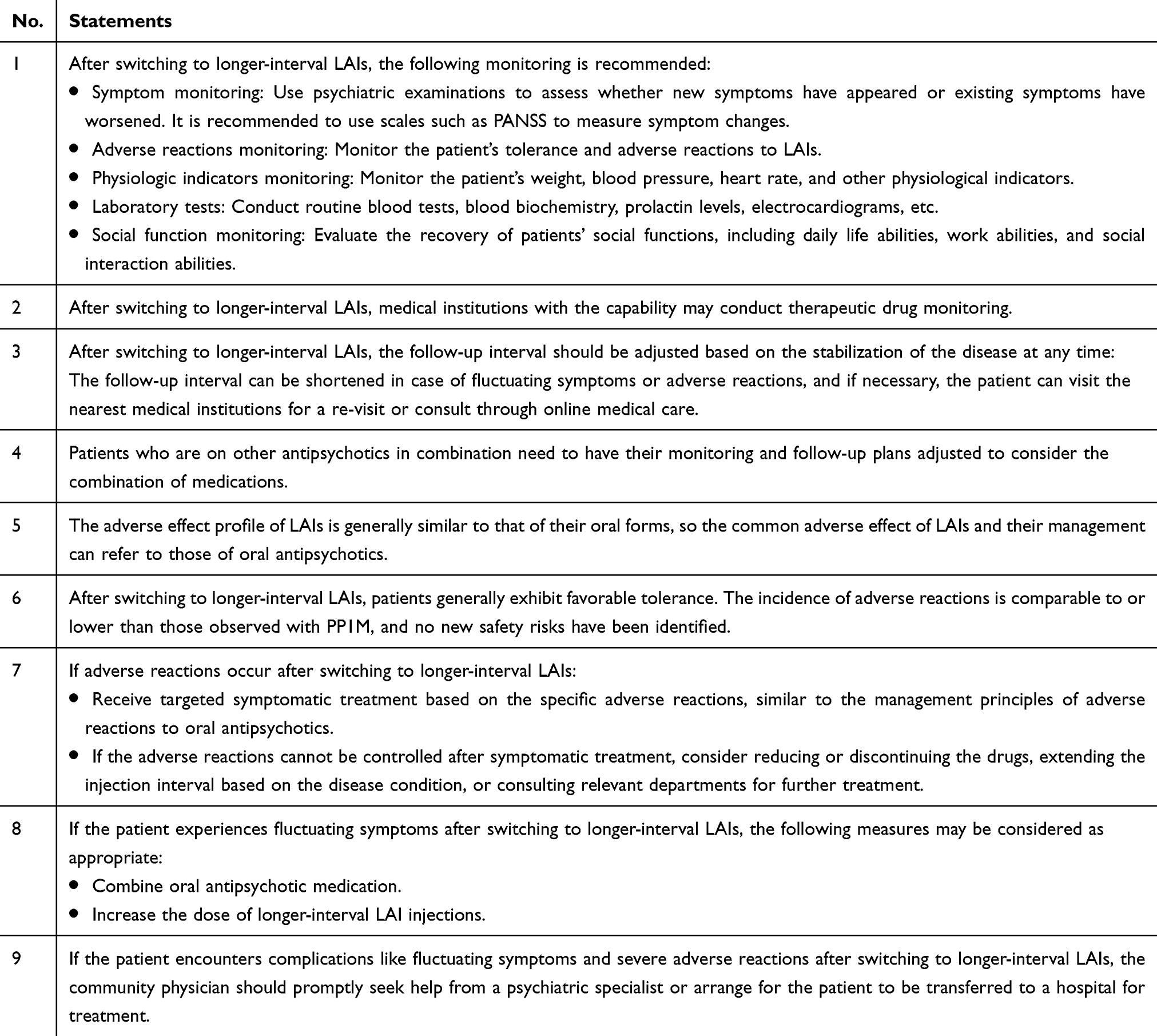 |
Table 4 Consensus on the Long-Term Disease Management After Switching to Longer-Interval LAIs |
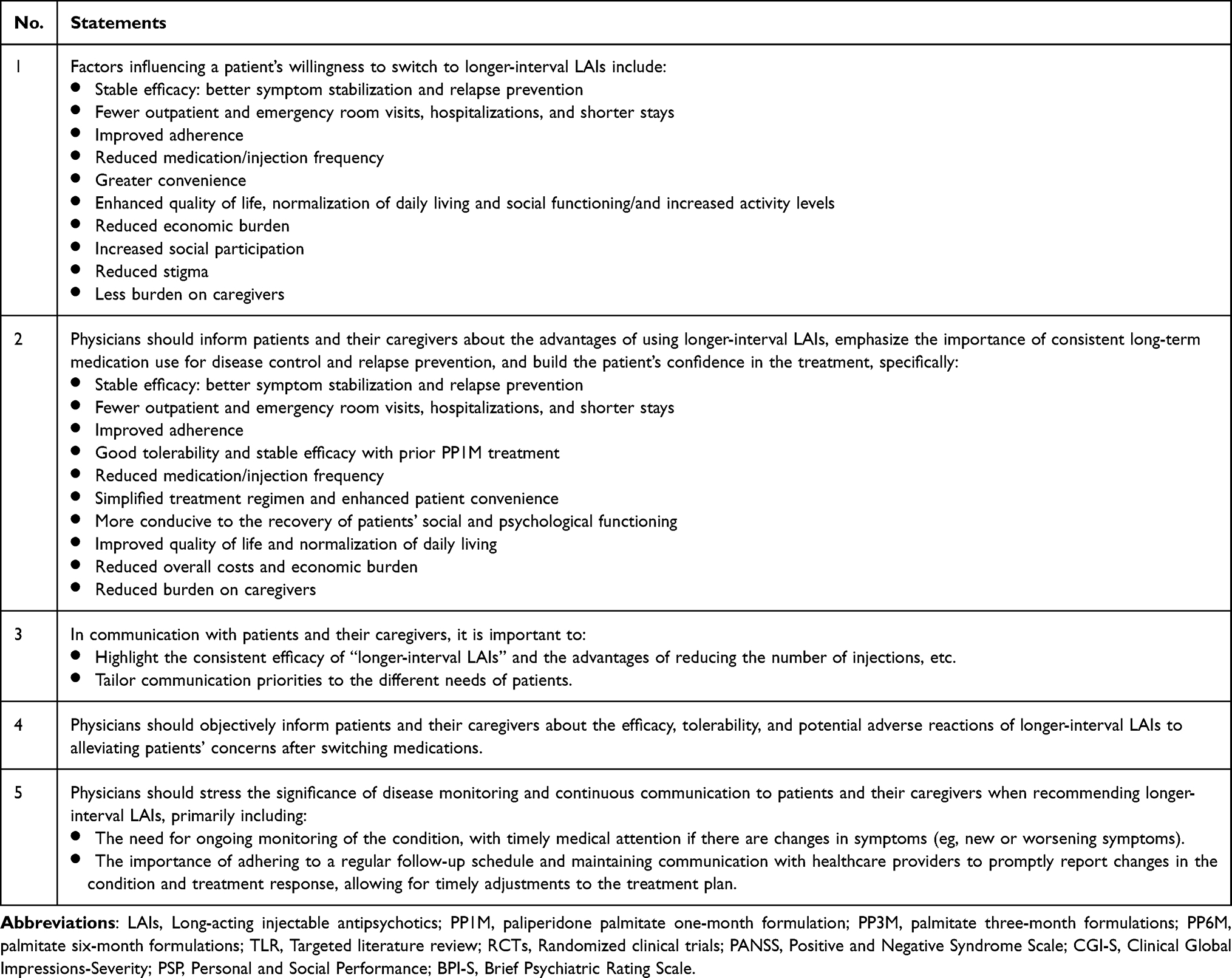 |
Table 5 Consensus on the Factors Influencing the Willingness to Use Longer-Interval LAIs |
Section 1 Clinical Necessity of Longer-Interval LAIs
In the first section, eight statements concerning clinical necessities were presented to the expert panel. This section outlines the clinical rationale and overarching advantages of switching from monthly to longer-interval LAIs in schizophrenia treatment. All statements achieved unanimous consensus across two rounds of evaluation. To eliminate redundancy, one statement demonstrates longer-interval LAIs’ clinical benefits was subsequently removed, resulting in a final set of seven statements (Table 1). This part of the statement summarized the clinical necessity of longer-interval LAIs. Longer-interval LAIs such as PP3M and PP6M offer significant benefits, including maintaining symptom stability comparable to PP1M, improving patient adherence, and reducing relapse rates for schizophrenic patients (statement 1–5). Longer-interval LAIs also lower outpatient visits and hospitalizations, thus reducing healthcare costs (statement 6). Overall, longer-interval LAIs offer a cost-effective advantage by improving patient outcomes and reducing disease burden.
Section 2 Suitable Population for Longer-Interval LAIs
In the second section, seven statements pertaining to the target population were presented to the panel. This section identifies patient subgroups who may benefit most from longer-interval LAIs, based on expert consensus and clinical experience. Six statements reached a consensus in two rounds, while the statement suggests that younger individuals or those with a shorter duration of illness may present a suitable population – reached nearing consensus in both round 1 and round 2 (Supplementary Material 3, statement 2.6). After all, the suitable population for switching to longer-interval LAIs are considered as: patients with high risk of relapse (statement 1), poor adherence to treatment (statement 2), high demands of social functions (statement 3) and at high risk of causing accidents or harm (statement 4). Patients generally prefer longer-interval LAIs are suitable to consider switching (statement 5). Patients who are in the early stages of their condition or have shown significant improvement during PP1M treatment may achieve better outcomes with the management of longer-interval LAIs and should be prioritized for conversion (statements 6–7) (Table 2).
Section 3 Switching Strategy for Longer-Interval LAIs
In the third section, eight statements regarding switching strategies were submitted for expert panel review. This section provides practical guidance for safely and effectively switching from monthly LAIs to longer-interval formulations. Seven statements reached consensus, while one statement regarding the assessment of patients’ symptoms and adverse reactions through the use of scales has achieved moderate consensus across both rounds of evaluation (Supplementary Material 3, statement 3.5). Three statements were removed due to content redundancy, resulting in a final total of five statements in this section (Table 3). Before the decision of conversion to longer-interval LAIs, patients should be stable and tolerant with PP1M (statement 1–3), and the interaction with current medications should also be considered (statement 4). Patients with severe disease, poor functioning, longer disease duration, or recent symptom control may need PP1M treatment for longer time before switching (statement 5).
Section 4 Long-Term Disease Management After Switching to Longer-Interval LAIs
In the fourth section, nine statements about long-term disease management after switching to longer-interval LAIs were brought forward for expert panel deliberation, all of which achieved consensus across two rounds of review (Table 4). These nine statements involved recommendations on monitoring items during follow-up (statements 1–2), consideration regarding follow-up interval (statements 3–4), reaction to the adverse reactions (statements 5–7) and symptom changes (statements 8–9).
Section 5 Factors Influencing Treatment Willingness of Longer-Interval LAIs
The fifth section highlights key communication strategies for clinicians to engage patients and caregivers, based on the advantages outlined in Section 1, to facilitate acceptance and adherence to longer-interval LAI treatment. In this section, the factors influencing the willingness to use longer-interval LAIs from patient’s aspect (statement 1), and the benefit of longer-interval LAIs that could be introduced by the clinicians (statement 2) are separately demonstrated. And the importance of tailored communication regarding specific needs from different patients is also strengthened (statement 3). Besides the benefit, the consideration of patient tolerability to the treatment (statement 4), the education about regular follow-up (statement 5) were also summarized. All the five statements reached consensus in two rounds (Table 5).
Discussion
This study employed a structured, three-step modified Delphi panel methodology to establish expert consensus on the switching from monthly formulation LAIs to longer-interval LAIs in the treatment of schizophrenia. To our understanding, this is the first clinical consensus specifically focused on the practical application of longer-interval LAIs in China. Through a rigorous process comprising a targeted literature review, two rounds of Delphi panel consultation, and a final consensus meeting, a total of 33 statements were finalized, reflecting the collective judgment of leading clinical experts that generally endorsing the clinical value and practical relevance of longer-interval LAIs across a range of treatment scenarios. Statements obtained high scores of ICC during two rounds of Delphi panel, which also indicated a higher consistency among the panelists. Throughout the study, panelists provided a wealth of constructive insights regarding the current use of longer-interval LAIs, offering valuable recommendations to support switching strategies and long-term disease management.
While only statements meeting the predefined threshold for strong consensus (≥80% of panelists rating 7–9 and median ≥8) were formally classified as such, certain statements with moderate or nearing consensus—such as Statement 2.6—were also discussed. These statements represent areas of high clinical interest and were included to explore expert concerns and refine recommendations. This process aligns with the study’s objective and methodology, which emphasize not only consensus formation but also the adjustment of statements to better reflect clinical realities. This approach distinguishes the present study from traditional Delphi designs and enhances its applicability to real-world practice.
Ultimately, the expert panel underscored the necessity of formulating such a consensus to provide clear, practice-oriented guidance that can inform and enhance clinical decision-making in real-world settings. The usage of longer-interval LAIs is generally recognized among clinical experts. When treatment efficacy is well-established, adverse effects are considered tolerable, and economic advantages are apparent, physicians are more likely to adopt longer-interval LAIs in clinical practice and to recommend them to patients when appropriate. Regarding the clinical necessity of longer-interval LAIs, their advantages had been recognized in enhancing adherence, reducing relapse rates, minimizing outpatient and hospitalization needs, offering cost-effectiveness, and improving quality of life and social functioning. The longer-interval LAIs offer a viable treatment option for patients with limited accessibility to care or treatment-related inconveniences. There has been evidence support that longer-interval LAIs (eg, PP3M) treatment can significantly delay the time to relapse, even after occasional cessation of treatment.27,28
Despite the overall agreement among experts on the clinical value of longer-interval LAIs, several statements prompted considerable discussion during the Delphi process. Prior stabilization through adequate treatment of monthly formulation LAIs is critical in the usage of longer-interval LAIs. Determining the optimal timing for transitioning a patient to a longer-interval LAI is considered a clinical challenge. It is important to define stability not just by symptom remission, but through a comprehensive evaluation that considers both symptoms and adverse reactions to facilitate a more accurate assessment of a patient’s condition. Additionally, it is important to review a longer historical context to determine the durability of stability. Understanding how long patients have maintained stable conditions can provide valuable insights into treatment effectiveness and support better clinical decision-making. A post-hoc analysis of the Chinese sub-group in the Phase III trial of PP3M revealed factors associated with successful transition from PP1M to PP3M.29 Patients with lower baseline CGI-S scores and greater reductions in PANSS and CGI-S scores by week 13 were more likely to achieve disease stabilization, potentially facilitating a successful transition. These findings may provide insights into clinical practice, suggesting that prioritizing transitions for patients demonstrating significant improvement and lower severity could lead to a more stable conversion process.
Effective long-term disease management after transitioning to longer-interval LAIs requires careful attention to monitoring content and follow-up frequency. Based on the findings of our study, the recommendations on monitoring items not only contain the symptoms, adverse reactions and the physiological indicators of patients’ general health status, but also highlight the importance of assessing social function to reflect their overall recovery. Besides, the follow-up intervals should be customized according to the patient’s disease condition rather than solely on the injection schedule of the LAIs. Follow-ups during the transition period may need to be more frequent, but stable management under longer-interval LAIs could facilitate more extended follow-up opportunities in the long run.
Communication regarding the transition to longer-interval LAIs is critical but also challenging. To achieve tailored communication, clinicians must fully understand the advantages of longer-interval LAIs, allowing them to develop strategies that match the individual motivations of different patients. Training and education should be strengthened to support clinicians in applying these therapies with confidence and consistency. The benefits of longer-interval LAIs for caregivers should not be underestimated, as their involvement can significantly impact patient decision-making processes. Besides, while the convenience of longer-acting injectable therapies presents an attractive option, it is crucial to emphasize during discussions that regular follow-ups and treatment adherence are essential components of patient recovery.
While this study aims to develop clinical consensus on strategies for switching from LAIs to longer‑interval formulations, the persistently low uptake of LAIs in China remains a critical contextual constraint, shaping the environment in which these strategies must be implemented. Evidence points to three major contributing factors. First, shifting clinician attitudes continues to be challenging. Psychiatrists could overestimate patients’ adherence to oral antipsychotics, thereby reducing the perceived need for LAIs.30,31 Moreover, historically limited range of LAI formulations means that switching requires a change in molecule or dose re‑titration, further increasing resistance to conversion.32,33 Second, discontinuity across the treatment pathway may hinder initiation. Most patients are managed in community settings,34 where surveys from Beijing indicate that community psychiatrists express strong willingness to use LAIs to reduce relapse risk and improve public safety.35 Yet relapses are often treated in tertiary hospitals, where LAIs initiation practices differ substantially across institutions,36 and handoffs back to community care remain inconsistent, creating missed chances for timely continuation after discharge. Third, substantial regional heterogeneity in reimbursement and access persists. In provinces with supportive policies37—such as Guangdong38 and Sichuan39—LAIs may be provided at low or no cost. In contrast, financial barriers remain significant in other regions, limiting both initiation and sustained use.
Evidence has demonstrated that higher proportion of patients in early stages of schizophrenia could achieve symptomatic or functional remission after switching to longer-interval LAIs.40 Experts in this study also acknowledge this finding and emphasize the importance of receiving stable treatment to reduce the functional loss. It is expected that the recommendations in this study could enable more schizophrenia patients to transition to longer-interval LAIs early in their treatment, and ultimately mitigate the risk of disease relapse and facilitate functional recovery.
Limitations
Utilizing a modified Delphi approach, the study offers several methodological strengths. Notably, the use of one-on-one interviews, rather than traditional written surveys, enabled a deeper exploration of the rationale behind experts’ ratings, facilitating a more nuanced understanding of clinical perspectives. In addition, the process was supported by a well-structured design, including a comprehensive targeted literature review, which provided robust scientific context and evidence to inform the development of consensus statements. The active involvement and oversight of the steering committee, along with stringent selection criteria for expert panelists, further contributed to the credibility, comprehensiveness, and clinical relevance of the final consensus. By synthesizing real-world insights from experienced psychiatrists, the study provides practical, context-specific recommendations to guide clinical decision-making and promote the standardized use of longer-interval LAIs in China.
Despite these strengths, certain limitations should be acknowledged. Given the currently limited use of longer‑interval LAIs in China, our panel did not foreground detailed guidance on treatment in patients with renal impairment or on missed‑dose management; as clinical experience accumulates, future updates may refine these domains. The use of interviews, while valuable for eliciting in-depth insights, may have introduced the potential for conformity bias, as participants might have felt implicit pressure to align with perceived expectations. However, this approach did not compromise the anonymity traditionally associated with the Delphi method. All panelist experts were blinded to each other’s identities and responses, which helped mitigate the influence of academic seniority or peer pressure. Furthermore, all the experts were asked to explain the rationale behind their ratings, reducing the likelihood of conformity and ensuring that responses reflected individual clinical judgment. Interviewers followed a standardized protocol and did not guide or influence participants’ answers. These measures helped control potential bias and preserved the methodological rigor of the Delphi process. Given all panelists practiced in urban referral hospitals, translation to community management should be locally adapted to available resources, workforce, and workflows.
Conclusion
This study represents the first expert consensus in China focused on the clinical application of longer-interval LAIs in the treatment of schizophrenia. Through a structured, three-step modified Delphi process, a total of 33 consensus statements were finalized. These statements provide practical guidance across key areas, including clinical benefits, target populations, switching strategies, long-term disease management, and factors influencing treatment acceptance. The findings reflect a high level of expert agreement on endorsing the value of longer-interval LAIs and offer valuable insights to inform clinical decision-making, bridge current gaps in treatment guidelines, and promote standardized and evidence-informed use in real-world practice.
Ethics Approval and Informed Consent
Patient-related ethical approval was not applicable to this Delphi study. The exemption was based on the following considerations: no individual patient data were collected; physician participation was entirely voluntary; all participating panelists provided written informed consent prior to the study, including consent for audio and video recording of interviews and meetings; and all survey responses were anonymized to ensure confidentiality.
Acknowledgments
The authors would like to extend their sincere gratitude to all expert panelists who participated in this study. Their valuable knowledge, clinical experience, and thoughtful contributions were instrumental in shaping the consensus and enriching the study findings. The authors also wish to thank the Health Economics & Value Access study team from IQVIA Solutions Enterprise Management Consulting (Shanghai) Co., Ltd. for their support in executing the Delphi process and for their contributions to the manuscript development.
Funding
Johnson & Johnson funded the study procedure and medical writing support, which was provided by IQVIA Solutions Enterprise Management Consulting (Shanghai) Co., Ltd. The sponsor was involved in the study design, data analysis, and publication plan.
Disclosure
Tianmei Si reports consultancy for Johnson & Johnson and Lundbeck, and speaker honoraria from Johnson & Johnson, Lundbeck, Otsuka, Teva. W. Zhang, Chong. Ye, and M. Jia, are employees of Johnson & Johnson and may hold stock in Johnson & Johnson. Dr Bo Zhou reports grants from Health Science Research Project of Sichuan Province, ZH2024-203, outside the submitted work. The authors report no other conflicts of interest in this work.
The abstract of this paper was presented at the 36th CINP World Congress Neuropsychopharmacology –CINP-AsCNP 2025 Joint Congress as a conference talk and poster with interim findings. The poster’s abstract was published in “Congress Abstracts” in International Journal of Neuropsychopharmacology: https://academic.oup.com/ijnp/article/28/Supplement_2/ii3/8236817.41
References
1. Owen M, Sawa A, Mortensen P. Schizophrenia. Lancet. 2016;388(10039):86–14. doi:10.1016/S0140-6736(15)01121-6
2. Liu T, Zhang L, Pang L, Li N, Chen G, Zheng X. Schizophrenia-related disability in China: prevalence, gender, and geographic location. Psychiatr Serv. 2015;66(3):249–257. doi:10.1176/appi.ps.201400032
3. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
4. Zhai J, Guo X, Chen M, Zhao J, Su Z. An investigation of economic costs of schizophrenia in two areas of China. Int J Mental Health Sys. 2013;7(1):26. doi:10.1186/1752-4458-7-26
5. Zhong Q, Tan Y, Chen W, et al. Disease burden of schizophrenia patients visiting a Chinese regional mental health centre. J Comparat Effect Res. 2020;9(7):469–481. doi:10.2217/cer-2019-0129
6. Jääskeläinen E, Juola P, Hirvonen N, et al. A systematic review and meta-analysis of recovery in schizophrenia. Schizophrenia Bulletin. 2013;39(6):1296–1306. doi:10.1093/schbul/sbs130
7. Kane J, Correll C. Optimizing treatment choices to improve adherence and outcomes in schizophrenia. J Clin Psychiatry. 2019;80(5). doi:10.4088/JCP.IN18031AH1C
8. Xiao J, Mi W, Li L, Shi Y, Zhang H. High relapse rate and poor medication adherence in the Chinese population with schizophrenia: results from an observational survey in the People’s Republic of China. Neuropsychiatr Dis Treat. 2015;11:1161–1167. doi:10.2147/NDT.S72367
9. Andreasen NC, Liu D, Ziebell S, Vora A, Ho BC. Relapse duration, treatment intensity, and brain tissue loss in schizophrenia: a prospective longitudinal MRI study. Am J Psychiatry. 2013;170(6):609–615. doi:10.1176/appi.ajp.2013.12050674
10. Lieberman JA, Perkins D, Belger A, et al. The early stages of schizophrenia: speculations on pathogenesis, pathophysiology, and therapeutic approaches. Biol. Psychiatry. 2001;50(11):884–897. doi:10.1016/s0006-3223(01)01303-8
11. Gardner KN, Nasrallah HA. Managing first-episode psychosis: an early stage of schizophrenia with distinct treatment needs: minimize duration of untreated psychosis; aim for remission. Curr Psychiatry. 2015;14(5):
12. Correll CU, Bookhart BK, Benson C, Liu Z, Zhao Z, Tang W. Association of relapse with all-cause mortality in adult patients with stable schizophrenia. Int J Neuropsychopharmacol. 2025:pyaf018;285:doi:10.1093/ijnp/pyaf018
13. De Sousa A, Lodha P. Suicide and Schizophrenia: factors Affecting Recovery. In: Shrivastava A, De Sousa A editors. Schizophrenia Treatment Outcomes: An Evidence-Based Approach to Recovery. Springer International Publishing; 2020:125–131. doi:10.1007/978-3-030-19847-3_11
14. Guo Y, Yang X, Wang D, et al. Prevalence of violence to others among individuals with schizophrenia in China: a systematic review and meta-analysis. Front Psychiatry. 2022;13:939329. doi:10.3389/fpsyt.2022.939329
15. Kim H, Seo G, Lee B. Real-world effectiveness of long-acting injections for reducing recurrent hospitalizations in patients with schizophrenia. Ann Gen Psychiatry. 2020;19(1):1. doi:10.1186/s12991-019-0254-2
16. Kirk Morton N, Zubek D. Adherence challenges and long-acting injectable antipsychotic treatment in patients with schizophrenia. J Psychosoc Nurs Ment Health Serv. 2013;51(3):13–18. doi:10.3928/02793695-20130215-01
17. Kishimoto T, Hagi K, Kurokawa S, Kane JM, Correll CU. Long-acting injectable versus oral antipsychotics for the maintenance treatment of schizophrenia: a systematic review and comparative meta-analysis of randomised, cohort, and pre-post studies. Lancet Psychiatry. 2021;8(5):387–404. doi:10.1016/S2215-0366(21)00039-0
18. Gutierrez-Rojas L, Sanchez-Alonso S, Garcia Dorado M, Lopez Rengel P. Impact of 3-Monthly long-acting injectable paliperidone palmitate in schizophrenia: a retrospective, real-world analysis of population-based health records in Spain. CNS Drugs. 2022;36:917. doi:10.1007/s40263-022-00917-1
19. Lin D, Pilon D, Zhdanava M, et al. Medication adherence, healthcare resource utilization, and costs among Medicaid beneficiaries with schizophrenia treated with once-monthly paliperidone palmitate or once-every-three-months paliperidone palmitate. Curr Med Res Opin. 2021;37(4):675–683. doi:10.1080/03007995.2021.1882412
20. Takács P, Kunovszki P, Timtschenko V, et al. Comparative effectiveness of second generation long-acting injectable antipsychotics based on nationwide database research in Hungary: an update. Schizophrenia Bulletin Open. 2022;3(1). doi:10.1093/schizbullopen/sgac013
21. Turkoz I, Daskiran M, Siddiqui U, Knight R, Johnston K, Correll C. Relapse rates with paliperidone palmitate in adult patients with schizophrenia: results for the 6-month formulation from an open-label extension study compared to real-world data for the 1-month and 3-month formulations. Int J Neuropsychopharmacol. 2024;27(2):pyad067. doi:10.1093/ijnp/pyad067
22. Garcia-Portilla M, Benito Ruiz A, Gomez Robina F, Garcia Dorado M, Lopez Rengel P. Impact on functionality of the paliperidone palmitate three-month formulation in patients with a recent diagnosis of schizophrenia: a real-world observational prospective study. Expert Opin Pharmacother. 2022;23(5):629–638. doi:10.1080/14656566.2021.2023496
23. Barnett J, Pappa S. Switching from monthly to three-monthly long-acting injectable paliperidone: a survey on subjective satisfaction and safety. Patient Prefer Adherence. 2023;17:1603–1610. doi:10.2147/PPA.S410028
24. Si T, Wu R. Chinese Guidelines for the Prevention and Treatment of Schizophrenia (2025 Edition). (Psychiatry CS of, ed.). People’s Medical Publishing House; 2025.
25. Tang CT, Chua EC, Chew QH, et al. Patterns of long acting injectable antipsychotic use and associated clinical factors in schizophrenia among 15 Asian countries and region. Asia-Pac Psychiatry. 2020;12(4):e12393. doi:10.1111/appy.12393
26. Rowe G, Wright G. Expert Opinions in Forecasting: The Role of the Delphi Technique. Kluwer Academic; 2001.
27. Berwaerts J, Liu Y, Gopal S, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2015;72(8):830–839. doi:10.1001/jamapsychiatry.2015.0241
28. Mathews M, Gopal S, Singh A, et al. Comparison of relapse prevention with 3 different paliperidone formulations in patients with schizophrenia continuing versus discontinuing active antipsychotic treatment: a post-hoc analysis of 3 similarly designed randomized studies. Neuropsychiatr Dis Treat. 2020;16:221242. doi:10.2147/ndt.S221242
29. Li X, Ye C, Wang G, Jia M, Wang G. Factors associated with symptom stabilization that allow for successful transition from once-monthly paliperidone palmitate to three-monthly paliperidone palmitate: a post hoc analysis examined clinical characteristics in Chinese patients with schizophrenia. CNS Drugs. 2024;38(1):55–65. doi:10.1007/s40263-023-01056-x
30. Olivares JM, Alptekin K, Azorin JM, et al. Psychiatrists’ awareness of adherence to antipsychotic medication in patients with schizophrenia: results from a survey conducted across Europe, the Middle East, and Africa. Patient Preference Adherence. 2013;7:121–132. doi:10.2147/PPA.S37534
31. Keenan A, Lin D, Shepherd J, Bailey H, Benson C, Meakin S. Patient-psychiatrist discordance and drivers of prescribing long-acting injectable antipsychotics for schizophrenia management in the real-world: a point-in-time survey. BMC Psychiatry. 2022;22(1):187. doi:10.1186/s12888-022-03846-x
32. Højlund M, Correll CU. Switching to long-acting injectable antipsychotics: pharmacological considerations and practical approaches. Expert Opinion Pharmacother. 2023;24(13):1463–1489. doi:10.1080/14656566.2023.2228686
33. Chinese Schizophrenia Coordination Group. Chinese Society of Psychiatry, Chinese Society of General Practice. Expert consensus on long-acting injectable antipsychotic in the treatment of schizophrenia in community. Chin General Pract. 2022;25(29):3587–3602. doi:10.12114/j.issn.1007-9572.2022.0537
34. Zhao M, Ma N, Wang X, et al. Community-based management and treatment services for psychosis — China, 2019. China CDC Weekly. 2020;2(41):791–796. doi:10.46234/ccdcw2020.217
35. Jin L, Chen Y, Zhu J, et al. The willingness of community psychiatric management physicians to preferentially recommend long-acting injections in Beijing. Front Public Health. 2021;9:779563. doi:10.3389/fpubh.2021.779563
36. Zhang L, Wu T, Li J, et al. Effect of long-acting injectable antipsychotics on treatment adherence and healthcare utilization in Chinese patients with schizophrenia: a mirror-image study. Therape Advanc Psychopharmacol. 2025;15:20451253251360400. doi:10.1177/20451253251360400
37. National Health and Family Planning Commission. National guideline of basic public health services (third edition). 2017. Available from: http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/04/20170417104506514.pdf.
38. Wang SB, Tan W, Fu XY. The use and evaluation of long-acting injectable antipsychotic medications in community-dwelling patients with schizophrenia in Guangdong Province, China. Alpha Psychiatry. 2024;25(4):561–563. doi:10.5152/alphapsychiatry.2024.241591
39. Sichuan Provincial Health Commission. Sichuan Province carried out the pilot work of outpatient treatment with second-generation long-acting injections for patients with severe mental disorders. 2022. Available from: https://wsjkw.sc.gov.cn/scwsjkw/gzdt/2022/3/17/80180902b2484835bb9705dcff194118.shtml.
40. Pungor K, Bozikas V, Emsley R, et al. Stable patients with schizophrenia switched to paliperidone palmitate 3-monthly formulation in a naturalistic setting: impact of patient age and disease duration on outcomes. Ther Adv Psychopharmacol. 2020;10:204512532098150. doi:10.1177/2045125320981500
41. Ma H, Cai J, Jia F, et al. Clinical practice recommendations for switching to longer-interval injectable antipsychotics in schizophrenia patients: a modified delphi study in China. Int J Neuropsychopharmacol. 2025;28(Suppl 2):ii3–ii4. doi:10.1093/ijnp/pyaf052.006
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.