Back to Journals » Psychology Research and Behavior Management » Volume 19
Clinical Phenotype Identification in Chinese Children with ADHD Using Latent Profile Analysis and Implications for Precision Nursing Pathways
Authors Ma Y, Cui YH, Gao JJ, Wen F, Yan JJ, Sun MM, Duan HM, Song N
Received 26 March 2026
Accepted for publication 19 May 2026
Published 10 June 2026 Volume 2026:19 611629
DOI https://doi.org/10.2147/PRBM.S611629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Yue Ma,1,2 Yong-Hua Cui,3 Jia-Jia Gao,2 Fang Wen,3 Jun-Juan Yan,3 Ming-mei Sun,2 Hong-Mei Duan,1 Nan Song4
1School of Nursing, Beijing University of Chinese Medicine, Beijing, 100029, People’s Republic of China; 2Department of Nursing, Shunyi Maternal and Children’s Hospital of Beijing Children’s Hospital, Beijing, 101300, People’s Republic of China; 3Department of Psychiatry, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, 100101, People’s Republic of China; 4Department of Nursing, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, 100101, People’s Republic of China
Correspondence: Nan Song, Department of Nursing, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, 56 Nanlishi Road, Beijing, 100101, People’s Republic of China, Email [email protected]
Background: Attention-deficit/hyperactivity disorder (ADHD) is characterized by substantial clinical heterogeneity, underscoring the need for a shift toward precision nursing approaches. The present study aimed to identify relatively homogeneous subgroups (phenotypes) among children with ADHD based on multidimensional clinical characteristics and to validate their distinct cognitive profiles using objective cognitive assessments, thereby providing an empirical basis for the development of a precision nursing practice pathway.
Methods: A cohort of 403 treatment-naïve children with newly diagnosed ADHD were included. Behavioral, emotional, and social functioning were evaluated using the Swanson, Nolan, and Pelham Version IV Scale, the Strengths and Difficulties Questionnaire, and the Weiss Functional Impairment Rating Scale–Parent Report. Cognitive validation was conducted using the Continuous Performance Test (CPT). The primary analytical methods included latent profile analysis (LPA) and between-group comparisons.
Results: The optimal LPA model identified three distinct classes: the “functionally balanced type” (25.8%), the “impulsivity-predominant type” (55.6%), and the “emotional-cognitive dysregulation subtype” (18.6%). Cognitive validation using the CPT indicated that the impulsivity-predominant type demonstrated a significantly higher commission error rate, whereas the emotional-cognitive dysregulation subtype exhibited significantly greater reaction time variability.
Conclusion: The “behavioral subtyping–cognitive validation” framework proposed in this study links subjective behavioral clustering with objective cognitive indicators relevant to nursing care. This approach provides an important empirical foundation for shifting ADHD management from a uniform model toward mechanism-informed precision intervention.
Keywords: attention-deficit/hyperactivity disorder, children, cognition, nursing, phenotype
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental disorder of childhood characterized by three core features: inattention, hyperactivity, and impulsivity. In most affected individuals, symptoms persist into adulthood and are associated with substantial impairment in academic achievement, social adaptation, and occupational functioning.1,2 Globally, the prevalence of ADHD among school-age children and adolescents is estimated to be approximately 7.2%, while the prevalence among school-enrolled children aged 6 to 16 years in China has been reported to be 6.26%.3,4 In addition to core cognitive dysfunction, children with ADHD frequently present with comorbid emotional dysregulation and a range of behavioral problems. According to data from the latest Global Burden of Disease (GBD) study, the disease burden experienced by families of children with ADHD in China has increased steadily between 1990 and 2021.5
To address the marked heterogeneity of ADHD, previous research has attempted to classify the disorder into subtypes from multiple perspectives. Traditional diagnostic classifications including the predominantly inattentive presentation, predominantly hyperactive–impulsive presentation, and combined presentation provide an initial clinical framework; however, these categories do not adequately capture patterns of comorbidity or functional impairment that extend beyond core symptoms.6 In recent years, studies utilizing behavioral rating scales, neuroimaging, or genetic markers have increasingly aimed to identify more homogeneous subgroups of individuals with ADHD.7 Notably, recent advances in neuroimaging have highlighted the potential to differentiate ADHD subtypes based on imaging features, supporting the use of such techniques to refine subgroup identification.8 Nevertheless, most existing studies have primarily focused on the etiology or neurobiological mechanisms of ADHD, with limited attention directed toward translating subtyping findings into practical nursing intervention pathways capable of guiding clinical management.9 Nursing as a discipline holds a distinct advantage in translating foundational scientific findings into clinically applicable decision-support frameworks; however, nursing-led research addressing the transition from “subtyping” to “precision intervention” remains limited.10
To address this gap, the present study aims to bridge the translational divide between research findings and clinical nursing practice by proposing an integrative analytical framework that combines latent profile analysis (LPA) with objective cognitive validation. LPA is a person-centered, data-driven method that identifies internally homogeneous patient subgroups, or “clinical phenotypes”, based on multidimensional clinical characteristics such as core behavioral symptoms, emotional problems, and social functioning. This approach enables the characterization of heterogeneity beyond traditional diagnostic classifications.11,12 Factor analytic studies have confirmed that CPT shares the same underlying cognitive construct as standard attention paradigms, supporting its use as a valid measure of attentional function.13 This “behavioral subtyping–cognitive validation” paradigm is intended to link subjective behavioral clustering with underlying cognitive and neurological mechanisms relevant to clinical care, including response inhibition and attentional stability.
Based on this framework, a cross-sectional study design was adopted, and treatment-naïve children with newly diagnosed ADHD were recruited. Standardized behavioral rating scales including the Swanson, Nolan, and Pelham Version IV Scale (SNAP-IV) and the Strengths and Difficulties Questionnaire (SDQ) were used to assess clinical symptoms. Multidimensional clinical data were subsequently analyzed using LPA to identify latent clinical phenotypes. Cognitive functioning was then evaluated using the CPT, and between-group differences in CPT indices were examined across the identified phenotypes to determine whether each phenotype demonstrated a distinct cognitive profile. A cross-sectional design was chosen for two main reasons: (1) the primary aim was to identify latent phenotypes at a single time point, which is best achieved with a cross-sectional snapshot; and (2) recruiting treatment-naïve children at diagnosis provides a “pure” baseline unaffected by medication, making it ideal for initial phenotype discovery and cognitive validation.We hypothesized that: (1) LPA would identify three distinct clinical phenotypes (functionally balanced, impulsivity-predominant, and emotional-cognitive dysregulation) based on multidimensional behavioral and functional characteristics; (2) the impulsivity-predominant type would show a significantly higher commission error rate on the CPT, reflecting response inhibition deficits; and (3) the emotional-cognitive dysregulation subtype would show greater reaction time variability, reflecting attentional instability.
Participants and Methods
Study Population
A cross-sectional study design was employed. Children with ADHD who attended the outpatient clinic of the Department of Psychiatry at the study institution between January and November 2024 were recruited using convenience sampling.
The inclusion criteria were as follows: (1) age 6–16 years; (2) fulfillment of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnostic criteria for ADHD; (3) no prior pharmacological treatment for neurodevelopmental disorders, including ADHD, tic disorder, or autism spectrum disorder, before enrollment; and (4) provision of written informed consent by the legal guardian.
The exclusion criteria were as follows: (1) presence of severe physical illness, epilepsy, intellectual disability (IQ < 70), or other severe psychiatric disorders (eg., schizophrenia or bipolar disorder); (2) visual or auditory impairment, or insufficient cognitive capacity to complete the required assessments; and (3) incomplete questionnaire responses, regular-pattern responding, or other indicators of invalid data. Such cases were treated as missing data and excluded from the final analysis.
Recent methodological studies have provided systematic guidance for power analysis and sample size estimation in SEM, supporting the use of this rule of thumb as a practical approach.14 In the present study, 5 demographic variables and 11 scale-derived observed variables were included, resulting in a total of 16 observed variables and an estimated required sample size of 160–320 participants. After accounting for an anticipated invalid response rate of approximately 20%, the target sample size was adjusted to 192–384 participants. A total of 403 valid participants were ultimately included in the analysis.
The study protocol was approved by the institutional Ethics Committee (Approval No. 2023–021-01). All study procedures were conducted after written informed consent had been obtained from the legal guardians of participating children.
Research Instruments
General Information Questionnaire
A general information questionnaire was developed by the research team based on relevant literature and expert consultation with two pediatric nursing specialists and one child psychiatry specialist. The questionnaire was completed by the child’s legal guardian and collected demographic information, including the child’s sex, age, only-child status, maternal parity, and the caregiver’s monthly household income.
Chinese Version of the SNAP-IV-Parent Form
The Chinese version of the SNAP-IV has demonstrated satisfactory reliability and validity.15,16 This instrument is used to assess behavioral symptoms and symptom severity in children aged 6 to 18 years with ADHD. The scale comprises 26 items across three dimensions: inattention, hyperactivity–impulsivity, and oppositional defiant disorder. Parents rate the child’s behavior over the preceding six months, and completion typically requires less than 10 minutes. Items are rated using a 4-point Likert scale (0 = never, 1 = sometimes, 2 = often, 3 = always). Scores for each dimension are calculated as the mean of the corresponding item scores and interpreted as follows: 0–1.0 = normal, 1.1–1.5 = mild, 1.6–2.0 = moderate, and 2.1–3.0 = severe. Higher scores indicate greater symptom severity in the respective domain. The Cronbach’s α coefficients for the subscales were 0.90 for inattention, 0.89 for hyperactivity–impulsivity, and 0.88 for oppositional defiant behavior.
SDQ-Parent Version
The SDQ was originally developed by Goodman, and the Chinese version was revised by Kou et al17,18 The instrument is applicable to children aged 4–16 years and is commonly used to screen for comorbid emotional and behavioral problems in children with ADHD. The questionnaire contains 25 items distributed across five dimensions: emotional symptoms, conduct problems, hyperactivity/inattention, peer relationship problems, and prosocial behavior. Parents complete the questionnaire based on the child’s behavior during the preceding six months using a 3-point Likert scale (0 = not true, 1 = somewhat true, 2 = certainly true). In the present study, only the emotional symptoms and conduct problems subscales were used to screen for comorbid emotional and behavioral difficulties in children with ADHD, comprising a total of 10 items.
The Cronbach’s α coefficient for the combined emotional symptoms and conduct problems subscales was 0.82. Higher scores indicate greater severity of emotional or behavioral difficulties. For the parent-rated version, the cutoff values are as follows: 0–3 = normal, 4 = borderline, and 5–10 = abnormal. This instrument functions as a screening tool, and its results are not sufficient for the clinical diagnosis of mood disorders.
Weiss Functional Impairment Rating Scale-Parent Report
The Weiss Functional Impairment Rating Scale–Parent Report (WFIRS-P) is a disorder-specific instrument designed to evaluate functional impairment associated with ADHD.19 The scale assesses the extent to which symptoms, behaviors, or emotional difficulties affect functioning across multiple domains of daily life. The WFIRS-P consists of 50 items distributed across six functional domains: family, learning/school, daily living skills, self-concept, social activities, and risk-taking activities. The total score ranges from 0 to 150, with maximum scores of 30, 30, 30, 9, 21, and 30 for the respective domains. Higher scores indicate greater functional impairment in the corresponding domain.
The scale is completed by a parent or guardian and typically requires approximately 15 minutes. Items are rated using a 4-point Likert scale (0–3). In clinical evaluation, the mean score of each dimension is commonly used to assess the degree of functional impairment. Clinically meaningful impairment is indicated when the overall mean scale score exceeds 1.5, when at least two items within a domain are scored 2, or when at least one item is scored 3. Scores exceeding these thresholds are considered indicative of clinically significant functional impairment. The WFIRS-P demonstrates satisfactory reliability, and subscale Cronbach’s α coefficients ranging from 0.70 to 0.89.
CPT
The CPT is an objective, quantitative instrument used to assess core cognitive deficits associated with ADHD and is widely applied in the study of ADHD-related cognitive endophenotypes.20 In the present study, the Sustained Attention Test Software System (Version 3.0), developed by Luo at the Mental Health Institute of Central South University, Hunan, was used.21 This system is designed for cognitive assessment in children aged 6–16 years. The software provides three testing modes differentiated by sensory modality: visual attention (VCPT), auditory attention (ACPT), and combined visual and auditory attention (VCPT + ACPT).
All participants in this study completed the visual attention test. During the assessment, digits from 0 to 9 were randomly presented at the center of a computer screen. Participants were instructed to press the spacebar when the target digit “3” appeared. The interstimulus interval was 1,500 ms, and the target stimulus occurred with a frequency of 10%. All participants first received standardized instructions followed by a 1-minute practice session. Formal testing commenced only after confirmation that the task instructions had been understood. The total duration of the formal test was 12 minutes. Upon completion, the software automatically generated five outcome indices: accuracy rate, number of errors, number of omissions, correct response time, and reaction time variability.
The omission error rate reflects sustained attention and represents the proportion of target stimuli to which no response was made; higher omission rates indicate reduced vigilance or attentional lapses. The commission error rate reflects impulse control and represents the proportion of incorrect responses to non-target stimuli; higher commission rates indicate impaired behavioral inhibition and increased impulsivity. Correct response time refers to the mean response latency for correct responses to target stimuli and reflects information processing speed. Reaction time variability represents the standard deviation of correct response times and reflects attentional stability, with higher variability indicating greater attentional fluctuation and reduced attentional persistence.
Statistical Methods
All statistical analyses were conducted using R version 4.2.2. Continuous variables with a normal distribution are presented as mean ± standard deviation, whereas non-normally distributed continuous variables are reported as median (interquartile range). Categorical variables are summarized as frequencies and percentages.
LPA
To identify heterogeneous clinical phenotypes among children with ADHD, LPA was performed using standardized scores from 11 dimensions reflecting ADHD-related behavioral symptoms, emotional difficulties, and social functioning. Z-score standardized mean item scores derived from the subscales of the SNAP-IV, SDQ, and WFIRS-P were used as indicator variables. Model estimation began with a one-class model, and the number of latent classes was sequentially increased to evaluate models specifying one to four classes. Model selection was based on a comprehensive evaluation of the following fit indices, including the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), adjusted Bayesian Information Criterion (aBIC), entropy, and the Bootstrap Likelihood Ratio Test (BLRT). Lower values of AIC, BIC, and aBIC indicate better model fit. Entropy values range from 0 to 1, with higher values indicating greater classification accuracy. A statistically significant BLRT result (p < 0.05) indicates that the k-class model provides a significantly better fit than the (k − 1)-class model. Based on these criteria, the three-class model was identified as the optimal solution.
Subtype Characterization Comparisons and CPT Validation Analysis
For continuous variables, including CPT indices, normality and homogeneity of variance were evaluated using the Kolmogorov–Smirnov test and Levene’s test, respectively. Due to the large sample size (n = 403) and the robustness of parametric methods against moderate violations of normality, one-way analysis of variance (ANOVA) was applied for overall between-group comparisons,22 followed by Tukey’s honestly significant difference (HSD) post hoc test when the overall F-test was significant. Effect sizes were quantified using eta-squared (η2), with interpretation based on the following thresholds: 0.01 ≤η2< 0.06 indicating a small effect, 0.06 ≤η2< 0.15 indicating a medium effect, andη2≥ 0.15 indicating a large effect.All statistical tests were two-sided, and the significance level was set at α = 0.05.
Results
General Characteristics
A total of 403 children with ADHD who met the DSM-5 diagnostic criteria were included in this study. The sociodemographic characteristics of the participants are presented in Table 1. The sample was predominantly male (n = 292, 72.46%), and most participants were aged 6–9 years (n = 236, 58.56%). The majority of the children were only children (n = 363, 90.07%). Maternal parity was predominantly primiparity (n = 296, 73.45%). Caregiver monthly household income was most commonly within the range of 3,001–5,000 CNY (n = 299, 74.19%). Descriptive statistics for all clinical scale scores are presented in Table 2. On the SNAP-IV, which assesses core ADHD symptoms, the inattention subscale demonstrated the highest mean item score (1.64 ± 0.79). On the SDQ, the mean score for emotional symptoms (0.90 ± 0.68) was substantially higher than that for conduct problems (0.50 ± 0.28). Regarding functional impairment assessed by the WFIRS-P, scores across all six domains indicated a moderate level of impairment. The family domain demonstrated the highest mean score (1.29 ± 1.09), while scores for the remaining domains ranged from 1.18 to 1.26, indicating widespread functional difficulties across multiple areas of daily life.
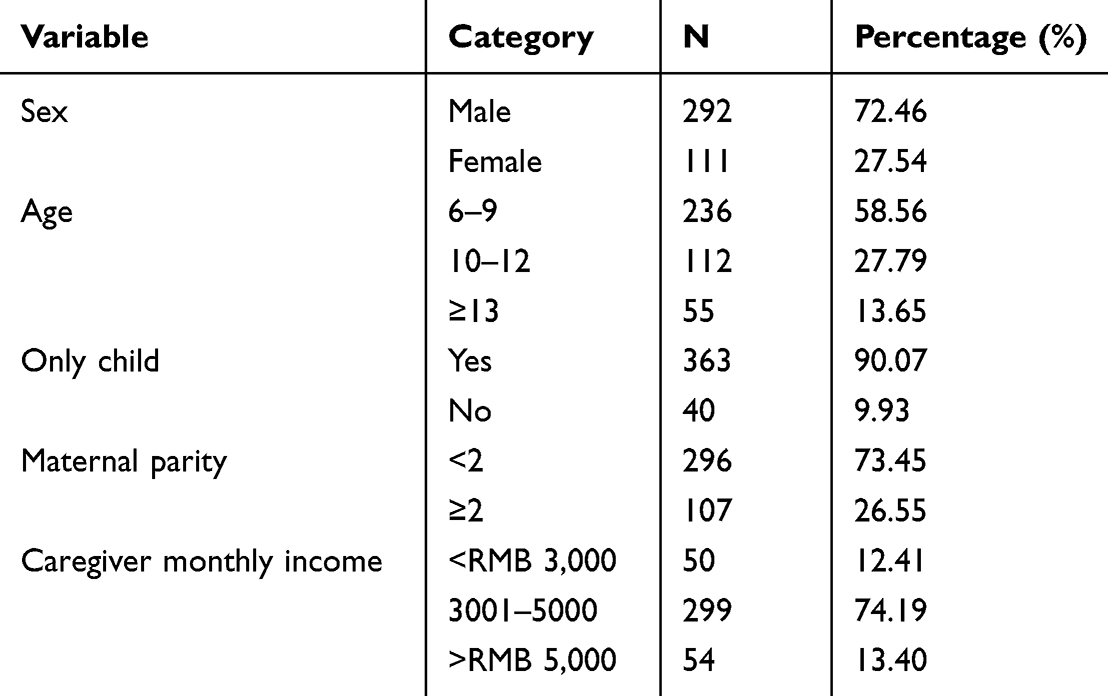 |
Table 1 Sociodemographic and Clinical Characteristics of Children with ADHD (n = 403) |
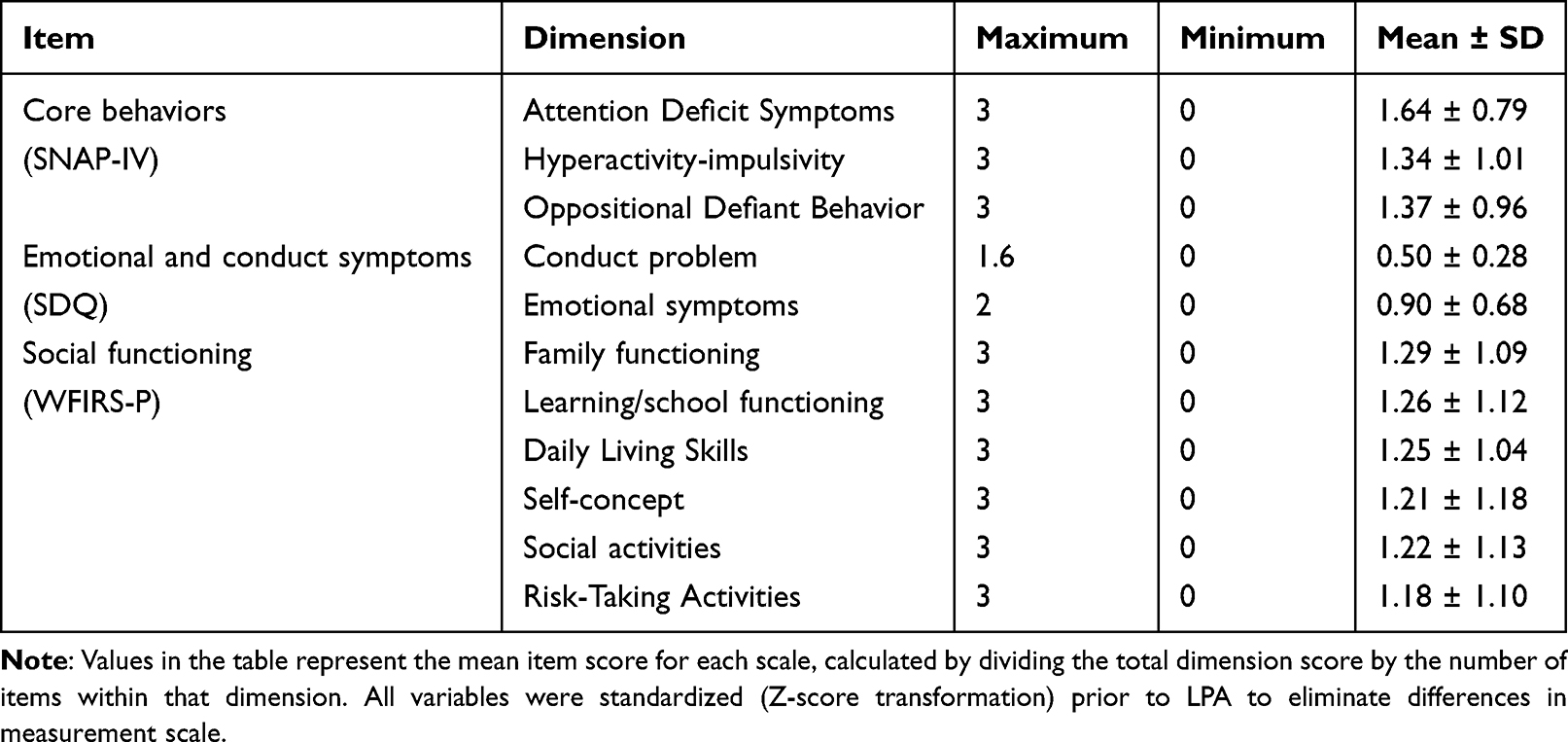 |
Table 2 Social Functioning Scores in Children with ADHD (Mean Item Scores, n = 403) |
LPA Model Fit and Class Determination
To characterize heterogeneity in multidimensional clinical features among children with ADHD, including core behavioral symptoms, emotional problems, conduct problems, and social functioning, LPA was conducted using 11 standardized clinical indicators derived from the SNAP-IV, SDQ, and WFIRS-P. Model fit indices are presented in Table 3. As the number of latent classes increased from one to four, the information criteria (AIC, BIC, and aBIC) demonstrated a monotonic decrease. Considering model parsimony, classification accuracy (Entropy = 0.99), and the clinical interpretability of the latent profiles, the three-class model was selected as the optimal solution. The BLRT was statistically significant (p < 0.01), indicating that the three-class model provided a significantly better fit than the two-class model. The three latent classes accounted for 25.8% (n = 104), 55.6% (n = 224), and 18.6% (n = 75) of the sample, respectively, indicating a relatively balanced distribution of participants across the identified subgroups.
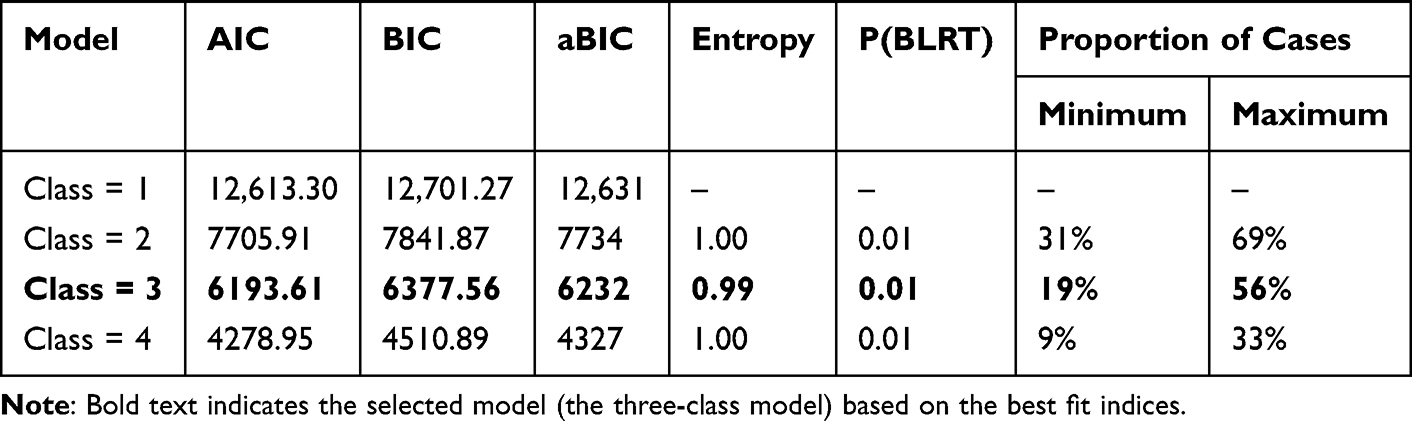 |
Table 3 LPA Model Fit Indices (n = 403) |
Based on the patterns of standardized scores (z-scores) across the 11 clinical dimensions (Figure 1), the latent classes were defined as follows.
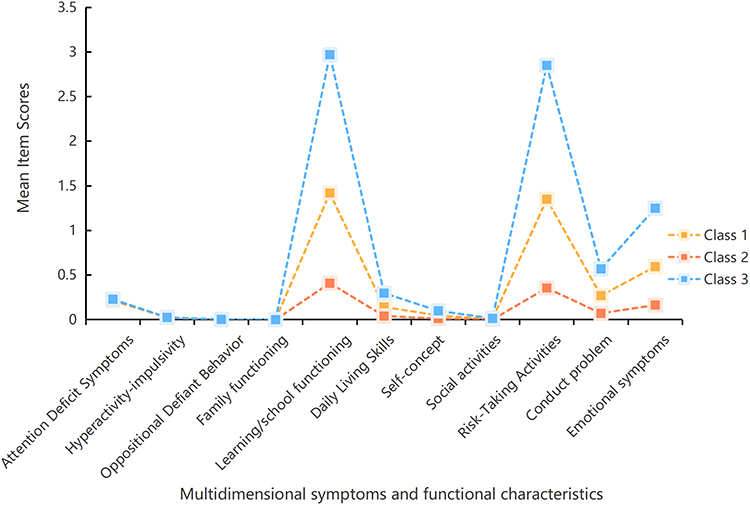 |
Figure 1 Latent profile model of multidimensional symptoms and functional characteristics in children with ADHD. |
Functionally Balanced Type
This class demonstrated scores across all clinical domains, including ADHD core symptoms, emotional symptoms, conduct problems, and social functioning, closest to the overall sample mean. The profile reflects relatively mild and balanced levels of symptoms and functional impairment and represents the subgroup with the lowest overall clinical burden. The near-mean distribution across dimensions indicates the absence of prominent dysfunction in any specific behavioral, emotional, or functional domain.
Impulsivity-Predominant Type
This class was characterized by markedly elevated externalizing symptoms, particularly in the hyperactivity–impulsivity and oppositional defiant disorder–related domains. In contrast, emotional symptoms and impairment in certain executive function–related domains (eg., self-concept and daily living skills) were comparatively less pronounced. This pattern indicates that the underlying functional deficits in this subgroup may be primarily related to impaired behavioral inhibition. These characteristics provided the rationale for further evaluation using the CPT to objectively assess impulse control and related cognitive processes.
Emotional-Cognitive Dysregulation Subtype
This class was characterized by markedly elevated emotional symptoms (internalizing problems, Z = 1.54), accompanied by substantial impairment in executive function–related domains (such as self-concept and daily living skills), whereas typical ADHD behavioral symptoms were relatively less pronounced. This pattern highlights the clinical relevance of emotional and cognitive regulatory difficulties within the ADHD presentation and indicates that this subgroup may require intervention strategies beyond those targeting behavioral symptoms alone.
Comparison of Neurocognitive Performance Across Latent Subgroups: CPT Results
One-way ANOVA was applied for between-group comparisons. Due to the large sample size (n = 403), parametric tests are robust to moderate violations of normality. Normality was assessed using the Kolmogorov–Smirnov test. The ANOVA revealed a statistically significant between-group difference only in the commission error rate (F(2,400) = 3.391, p = 0.034, η2 = 0.017). No statistically significant differences were observed among the three groups for the remaining indices, including omission error rate, correct response time, and reaction time variability (p > 0.05; Figure 2).
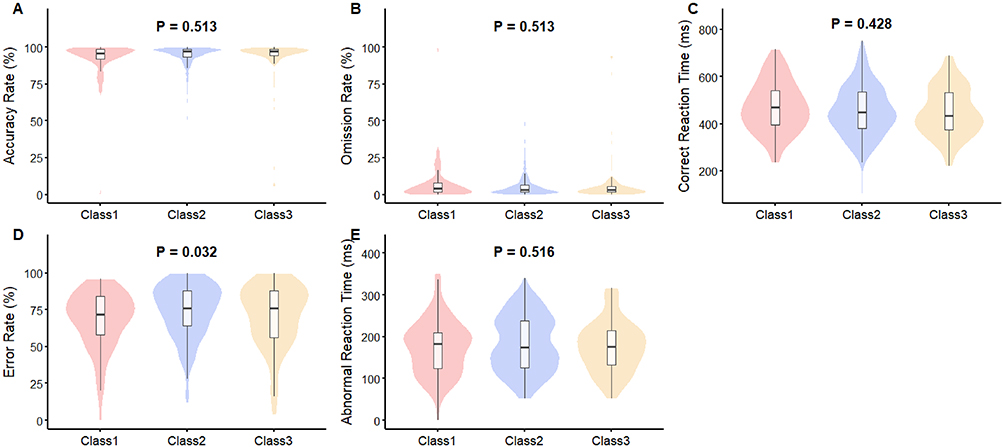 |
Figure 2 Comparison of core CPT cognitive indices across three ADHD clinical phenotypes identified by latent profile analysis. (A) Accuracy rate (%). (B) Omission rate (%). (C) Correct reaction time (ms). (D) Commission error rate (%). (E) Reaction time variability (ms). One-way ANOVA revealed a significant difference among the three groups only in commission error rate (D) (F(2,400) = 3.391, p = 0.034). No significant differences were found in the other indices (all p > 0.05). |
Descriptive statistics for commission error rates across the three groups are presented in Table 4. Post hoc comparisons using Tukey’s HSD test showed that the impulsivity-predominant type (G2) had a significantly higher commission error rate than the functionally balanced type (G1) (adjusted p = 0.033). No statistically significant differences were observed between G2 and G3 or between G1 and G3 (adjusted p > 0.05). Although the between-group difference reached statistical significance, the effect size was small (η2 = 0.017), indicating that the magnitude of the observed difference in commission error rate was limited and that substantial within-subgroup variability was present (standard deviation range: 18.5% to 21.8%).
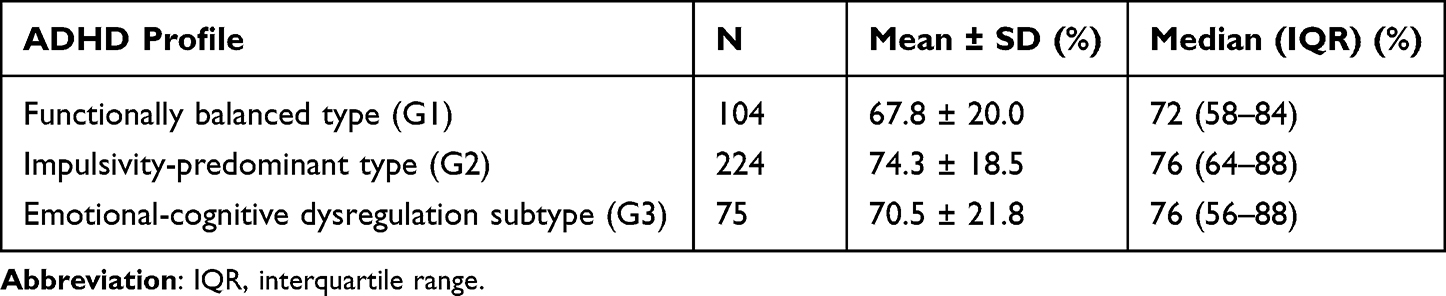 |
Table 4 Descriptive Statistics for CPT Commission Error Rate Across Three ADHD Clinical Subtypes |
Comparison of Demographic Characteristics Across Latent Profiles
To examine whether the identified clinical subtypes were associated with sociodemographic factors, the distribution of key demographic variables across the three latent profiles was compared (Table 5). Chi-square tests indicated no statistically significant differences among the three profiles with respect to sex (χ2 = 5.765, p = 0.056), age group (χ2 = 8.051, p = 0.090), only-child status (χ2 = 1.557, p = 0.459), maternal parity (χ2 = 5.055, p = 0.282), or caregiver monthly household income (χ2 = 3.882, p = 0.422). These findings indicate that the clinical heterogeneity identified in this study is more likely attributable to intrinsic patterns of symptom expression and functional impairment associated with ADHD rather than to the examined sociodemographic characteristics. Furthermore, these results reduce the likelihood that socioeconomic status or related demographic variables substantially confounded the subtype classification.
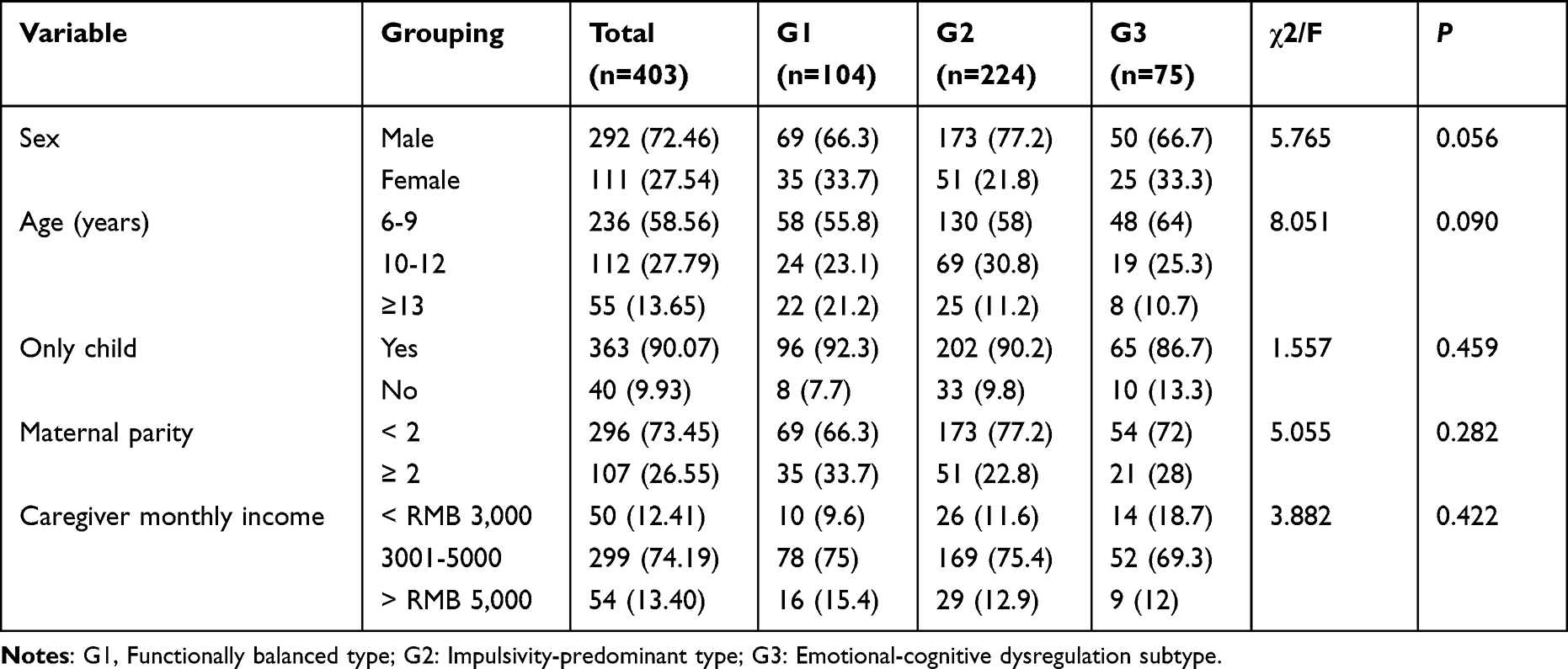 |
Table 5 Comparison of Sociodemographic Characteristics Across Latent Classes of Children with ADHD |
Discussion
Clinical Heterogeneity and the Need for Precision Nursing
ADHD presents substantial challenges for clinical management due to pronounced heterogeneity in core symptoms, patterns of comorbidity, and levels of functional impairment.23 Traditional diagnostic subtypes and standardized intervention protocols are often insufficient to address the individualized needs of children with ADHD. The present study addresses this limitation by applying a data-driven analytical approach to identify internally homogeneous clinical phenotypes and linking these phenotypes with specific cognitive–neurological characteristics.24 By integrating behavioral assessment with objective cognitive validation, this approach provides empirical support for transitioning ADHD nursing management from a uniform care model to a mechanism-guided precision nursing framework.
Identification and Validation of Three Behavioral Phenotypes
Using LPA, three stable and clinically interpretable ADHD phenotypes were identified: the functionally balanced type, the impulsivity-predominant type, and the emotional–cognitive dysregulation subtype. These findings indicate that the clinical heterogeneity observed in ADHD may reflect systematic differences in underlying neuropsychological characteristics.25 Cognitive validation using the CPT further supported mechanistic interpretations of these behavioral profiles, thereby extending the classification beyond descriptive symptom patterns toward cognitive–behavioral phenotypes with identifiable intervention targets.26
Consistent with this finding, adults with ADHD also exhibit elevated commission errors on the CPT, further supporting the role of response inhibition deficits in the impulsive phenotype across developmental stages.27 Elevated reaction time variability has also been observed in clinical populations with emotion–cognition dysregulation, further linking this cognitive feature to difficulties in emotional and attentional control.28 These findings are consistent with the prominent emotional regulation difficulties observed in this phenotype. In comparison, the functionally balanced type demonstrated relatively preserved cognitive performance, indicating that nursing strategies for this subgroup may benefit from emphasizing environmental optimization and developmental support rather than intensive deficit-focused interventions.
This interpretation is consistent with recent comprehensive reviews, which have emphasized that the heterogeneity of ADHD is fundamentally rooted in the diverse presentation of symptoms and neurocognitive impairment, as well as structural and functional brain differences, rather than being primarily driven by socioeconomic or other external demographic variables.29 This interpretation is consistent with emerging evidence from genetic and neurobiological research—including findings that genetic variations are directly associated with alterations in brain structure and functional connectivity in ADHD—indicating that symptom expression and functional outcomes are influenced more strongly by individual differences in genetic susceptibility and brain functional connectivity than by socioeconomic background alone.30 Consequently, nursing assessment may benefit from prioritizing a comprehensive evaluation of individual neuropsychological characteristics in order to support the development of individualized care strategies.
Constructing a Mechanism-Guided Precision Nursing Framework
Beyond the identification of clinical phenotypes, the present study aimed to provide a preliminary framework for mechanism-guided precision nursing in ADHD care. Based on the identified phenotypes and their associated cognitive characteristics, a structured nursing pathway spanning assessment, validation, and intervention can be proposed. Such an approach represents a transition from traditional empirically driven nursing practice toward a precision-oriented decision-making model informed by individualized clinical data.31
The proposed pathway begins with stratified assessment, in which standardized behavioral rating scales are used to conduct rapid screening and preliminary phenotype classification. The second stage involves targeted validation, during which objective cognitive assessment tools such as the CPT may be used to quantify specific cognitive deficits, particularly response inhibition and attentional stability, in children classified within higher-risk phenotypes. This step allows nursing goals to be formulated with greater specificity and alignment with the individual’s cognitive profile. Interventions may then be implemented according to phenotype-specific needs. For the impulsivity-predominant type, nursing care may focus on enhancing behavioral control through response inhibition training strategies, such as structured “stop–think–act” behavioral exercises, along with the establishment of a low-stimulation and highly structured environment.
For the emotional–cognitive dysregulation subtype, a dual-support approach integrating emotional regulation training (eg., mindfulness-based techniques) with executive function support strategies may be appropriate.
For the functionally balanced type, nursing interventions may emphasize risk prevention and functional promotion through parent education and environmental optimization.
This framework also highlights the potential role of nursing within translational clinical research by transforming findings from cognitive neuroscience into practical assessment and intervention strategies that can directly inform nursing decision-making in clinical settings.
Study Limitations and Future Directions
Several limitations should be considered when interpreting the findings of this study. First, the cross-sectional design does not allow for causal inference and does not permit evaluation of the long-term stability of the identified phenotypes. Second, the study sample was recruited from a single clinical center and consisted exclusively of treatment-naïve children, which may limit the generalizability of the findings. Future research should include longitudinal studies to examine the stability of the identified phenotypes over time and to evaluate the effectiveness of phenotype-guided precision nursing interventions. In particular, intervention studies are needed to determine whether strategies tailored to specific cognitive mechanisms such as response inhibition training for the impulsivity-predominant type result in improved outcomes compared with those achieved with standard care.
Replication of the phenotype structure in larger and more diverse populations will also be necessary to confirm the reliability of the classification model. In addition, the integration of multimodal data sources, including neuroimaging and neurophysiological measures, may facilitate a more comprehensive understanding of the biological mechanisms underlying the identified phenotypes. The incorporation of cognitive indicators such as attentional stability into digital health platforms may also enable continuous home-based monitoring and intervention, potentially extending precision nursing strategies beyond the clinical setting into everyday life.
Conclusion
Consistent with our hypotheses, this study integrated behavioral subtyping with objective cognitive validation and identified three distinct clinical phenotypes of childhood ADHD using LPA. As hypothesized, the impulsivity-predominant type demonstrated a significantly higher commission error rate, and the emotional-cognitive dysregulation subtype showed greater reaction time variability, confirming the distinct cognitive profiles of these phenotypes. Each phenotype was further linked to specific cognitive characteristics, particularly deficits in response inhibition and variability in attentional stability. These findings provide empirical support for the development of a mechanism-guided precision nursing pathway for children with ADHD.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki.This study was conducted with approval from the Ethics Committee of Shunyi Maternal and Children’s Hospital of Beijing Children’s Hospital (2023-021-01).A written informed consent was obtained from legal guardians of all participants.
Consent for Publication
Consent for publication was obtained from legal guardians of every individual whose data are included in this manuscript.
Funding
Health Development Research Special Project of Shunyi District, Beijing (Project No. Wsjkfzkyzx-2023-q-06). Principal Investigator: Yue Ma.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (Handbook).
2. Palladino VS, Mcneill R, Reif A, et al. Genetic risk factors and gene-environment interactions in adult and childhood attention-deficit / hyperactivity disorder. Psychiatr Genet. 2019;29(3):63. doi:10.1097/YPG.0000000000000220
3. Rajaprakash M, Leppert ML. Attention-deficit/hyperactivity disorder. Pediatr Rev. 2022;43(3):135–12. doi:10.1542/pir.2020-000612
4. Li F, Cui Y, Li Y, et al. Prevalence of mental disorders in school children and adolescents in China: diagnostic data from detailed clinical assessments of 17,524 individuals. J Child Psychol Psychiatry. 2022;63(1):34. doi:10.1111/jcpp.13445
5. Lai MQ, Li KX, Zeng SH, et al. Burden of attention deficit hyperactivity disorder in children and adolescents in China and globally from 1990 to 2021. Med J Peking Union Med College Hospital. 2025:1–17. https://link.cnki.net/urlid/11.5882.R.20250805.0851.002.
6. Antshel KM, Barkley R. Attention deficit hyperactivity disorder. Handb Clin Neurol. 2020;174:37–45. doi:10.1016/B978-0-444-64148-9.00003-X
7. Pereira-Sanchez V, Castellanos FX. Neuroimaging in attention-deficit/hyperactivity disorder. Curr Opin Psychiatry. 2021;34(2):105–111. doi:10.1097/YCO.0000000000000669
8. Firouzabadi FD, Ramezanpour S, Firouzabadi MD, et al. Neuroimaging in attention-deficit/hyperactivity disorder: recent advances. AJR Am J Roentgenol. 2022;218(2):321–332. doi:10.2214/AJR.21.26316
9. Olagunju AE, Ghoddusi F. Attention-deficit/hyperactivity disorder in adults. Am Fam Physician. 2024;110(2):157–166.
10. Lee BO. Precision health and nursing care in the digital age. Hu Li Za Zhi. 2022;69(2):4–6. doi:10.6224/JN.202204_69(2).01
11. Chen C, Tang S. Profiles of grief, post-traumatic stress, and post-traumatic growth among people bereaved due to COVID-19. Eur J Psychotraumatol. 2021;12(1):1947563. doi:10.1080/20008198.2021.1947563
12. Shin Y, Nam JK, Lee A, et al. Latent profile analysis of post-traumatic stress and post-traumatic growth among firefighters. Eur J Psychotraumatol. 2023;14(1):2159048. doi:10.1080/20008066.2022.2159048
13. Jobst LJ, Bader M, Moshagen M. A tutorial on assessing statistical power and determining sample size for structural equation models. Psychol Methods. 2023;28(1):207–221. doi:10.1037/met0000423
14. Moshagen M, Bader M. semPower: general power analysis for structural equation models. Behav Res Methods. 2024;56(4):2901–2922. doi:10.3758/s13428-023-02254-7
15. Hall CL, Guo B, Valentine AZ, et al. The validity of the SNAP-IV in children displaying ADHD symptoms. Assessment. 2020;27(6):1258–1271. doi:10.1177/1073191119842255
16. Zhou JB, Guo LT, Chen Y. Reliability and validity of the Chinese version of Swanson,Nolan,and Pelham Version IV rating scale-parent form for attention-deficit/hyperactivity disorder. Chinese Mental Health J. 2013;27(6):424–428.
17. Goodman R. Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry. 2001;40(11):1337–1345. doi:10.1097/00004583-200111000-00015
18. Kou JH, Du YS, Xia LM. Reliability and validity of “children strengths and difficulties questionnaire” in Shanghai norm. Shanghai Arch Psychiatry. 2005;17(1):25–28.
19. Hadianfard H, Kiani B, Weiss MD. Psychometric properties of the Persian version of the Weiss functional impairment rating scale-self-report form in Iranian adolescents. J Atten Disord. 2017;23(13):1600–1609. doi:10.1177/1087054717738084
20. Lee T, Park KJ, Lee HJ, et al. Clinical and neuropsychological characteristics of ADHD according to DSM-5 age-of-onset criterion in Korean children and adolescents. J Atten Disord. 2020;24(1):20–28. doi:10.1177/1087054716684378
21. Varela JL, Magnante AT. Miskey HM,et al.A systematic review of the utility of continuous performance tests among adults with ADHD. Clin Neuropsychol. 2024;38(7):1524–1585. doi:10.1080/13854046.2024.2315740
22. Blanca MJ, Arnau J, García-Castro FJ, Alarcón R, Bono R. Non-normal data in repeated measures ANOVA: impact on type I error and power. Psicothema. 2023;35(1):21–29. doi:10.7334/psicothema2022.292
23. Buitelaar J, Bölte S, Brandeis D, et al. Toward precision medicine in ADHD. Front Behav Neurosci. 2022;16:900981. doi:10.3389/fnbeh.2022.900981
24. Wolfers T, Beckmann CF, Hoogman M, et al. Individual differences v. the average patient: mapping the heterogeneity in ADHD using normative models. Psychol Med. 2020;50(2):314–323. doi:10.1017/S0033291719000084
25. Dunn VJ, Abbott RA, Croudace TJ, et al. Profiles of family-focused adverse experiences through childhood and early adolescence: the ROOTS project a community investigation of adolescent mental health. BMC Psychiatry. 2011;11:109. doi:10.1186/1471-244X-11-109
26. Li X, Zhu YT, Jiao DD, et al. Subtyping of internalizing and externalizing behaviors in Japanese community-based children: a latent class analysis and association with family activities. Children. 2022;9(2).
27. Alaghband-Rad J, Dashti B, Tehranidoost M, et al. A preliminary investigation of deficits in executive functions of adults with attention deficit hyperactivity disorder. J Nerv Ment Dis. 2021;209(1):35–39. doi:10.1097/NMD.0000000000001247
28. Krause-Utz A, Walther JC, Kyrgiou AI, et al. Severity of childhood maltreatment predicts reaction times and heart rate variability during an emotional working memory task in borderline personality disorder. Eur J Psychotraumatol. 2022;13(1):2093037. doi:10.1080/20008198.2022.2093037
29. Faraone SV, Bellgrove MA, Brikell I, et al. Attention-deficit/hyperactivity disorder. Nat Rev Dis Primers. 2024;10(1):11. doi:10.1038/s41572-024-00495-0
30. Yadav SK, Bhat AA, Hashem S, et al. Genetic variations influence brain changes in patients with attention-deficit hyperactivity disorder. Transl Psychiatry. 2021;11(1):349. doi:10.1038/s41398-021-01473-w
31. Zhang J, Zhao X, Li S, et al. Frailty profiles and symptomatic radiation pneumonitis in patients with lung cancer undergoing radiotherapy: a latent class analysis. Asia Pac J Oncol Nurs. 2025;13:100840. doi:10.1016/j.apjon.2025.100840
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Adherence and Related Factors Among Children with Attention-Deficit/Hyperactivity Disorder in Saudi Arabia
Alsubaie MA, Alshehri ZY, Alawadh IA, Abulreesh RY, Altaweel HM, Alateeq DA
Patient Preference and Adherence 2024, 18:337-348
Published Date: 3 February 2024
Correlation Analysis Between Real-Time Cerebral State Parameters and Emergence Agitation in Children Undergoing Decayed Tooth Surgery Under General Anaesthesia: Exploring Dental-Related Influencing Factors
Li L, Meng Q, Tian A, Hao Z, Zhang W
International Journal of General Medicine 2025, 18:7049-7057
Published Date: 19 November 2025