Back to Journals » International Journal of Women's Health » Volume 15
Clinical Performance of a Dedicated Urine-Based Assay for the Detection of Human Papillomavirus and Cervical Intraepithelial Neoplasia
Authors Zhao Y, Zhao L, Wang Z, Cui S, Ren C, Yang L, Bai Y, Zhu Y, Xie J, Li Y, Wu X, Feng J ![]() , Man S, Huang L, Li X, Yu X, Wang J
, Man S, Huang L, Li X, Yu X, Wang J
Received 29 June 2023
Accepted for publication 8 November 2023
Published 4 December 2023 Volume 2023:15 Pages 1909—1916
DOI https://doi.org/10.2147/IJWH.S424621
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Yun Zhao,1,* Lijun Zhao,1,* Zhaohuang Wang,1 Shuhui Cui,1 Chenchen Ren,2 Li Yang,2 Yang Bai,2 Yuanhang Zhu,2 Jingyan Xie,3 Yujuan Li,3 Xiaoqing Wu,3 Jing Feng,3 Shanqing Man,4 Longmei Huang,4 Xiaoqi Li,4 Xiaotian Yu,4 Jianliu Wang1
1Department of Obstetrics and Gynecology, Peking University People’s Hospital, Beijing, People’s Republic of China; 2Department of Obstetrics and Gynecology, The Third Affiliated Hospital of Zhengzhou University, National Clinical Research Center for Obstetrics and Gynecology, Zhengzhou Key Laboratory of Cervical Disease, Zhengzhou Key Laboratory of Endometrial Disease Prevention and Treatment, Zhengzhou, Henan, People’s Republic of China; 3Department of Obstetrics and Gynecology, Nanjing First Hospital, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 4Hangzhou New Horizon Health Technology Co. Ltd, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianliu Wang, Department of Obstetrics and Gynecology, Peking University People’s Hospital, 11 Xizhimen South Street, Xicheng District, Beijing, 100044, People’s Republic of China, Tel +8618901086568, Email [email protected]
Objective: The objective of this study is to assess the clinical performance of a urine-based high-risk human papillomavirus (hrHPV) test for the detection of cervical intraepithelial neoplasia grade 2 or higher (CIN2+).
Methods: Between September and December 2021, women aged 20 to 65 years referred to colposcopy clinic were prospectively recruited at three clinical centers in China. Paired urine and cervical specimens from all enrolled women were obtained for hrHPV DNA fluorescence quantitative PCR test. The results of liquid-based cytology (LBC), colposcopy and diagnostic biopsies were collected. We evaluated the sensitivity and specificity for CIN and assessed the agreement/kappa value.
Results: A total of 732 women (median age, 40 years) with valid results were included in the study, and 130 (17.8%) women were histologically confirmed as CIN2+. The sensitivity of urine and cervical test for CIN2+ and CIN3+ were 87.69% and 85.45%, respectively. The specificity of urine test performed better than cervical test in women with
Keywords: HPV testing, cervical intraepithelial neoplasia, diagnostic test accuracy, human papillomavirus, urine
Introduction
Cervical cancer ranks the fourth for females worldwide according to Global Cancer Statistics 2020,1 and about 20% of the new cancer incidence were reported in China. Persistent infection with high-risk human papillomavirus (hrHPV) is the major causative agent of cervical cancer,2 and it has been well accepted that the early detection of HPV infection is essential to the prevention of cervical cancer. HrHPV test combined with cytology is recommended for primary cervical screening by the World Health Organization (WHO).3–5 However, the coverage and compliance of routine screening are relatively poor in some countries due to the regional and ethnic disparities as well as low-resource settings for preventive medical care.6–8 According to the latest reported data, only 25.7% of Chinese women aged 20–64 had previously attended cervical cancer screening in 20159 and more than 50% of the new incidence occurred in women who were not adequately screened.10 Furthermore, the COVID-19 pandemic has contributed to the impediment in access to healthcare facilities.11
Compared with invasive cervical HPV sampling, urine-based HPV test appears to be more acceptable and thus increase the attendance of routine screening.12–15 And the latest meta-analysis indicated that urine HPV test demonstrated similar clinical accuracy to cervical test for the detection of cervical intraepithelial neoplasia (CIN).16 However, the clinical outcomes for urine HPV varied substantially between recent studies17,18 and currently there is no specific urine HPV assay available on the market.19 In addition, the previous studies were conducted primarily overseas, and few data was reported in the Chinese population.
In this study, we aim to evaluate the clinical performance of a newly developed urine-specific hrHPV test—CerviClear® for detecting CIN and compare the results with a commercially available cervical-based HPV assay in China.
Materials and Methods
Study Design and Population
The study was a prospective, registry-based multicenter clinical study (NCT05210348) carried out in Peking University People’s Hospital, the Third Affiliated Hospital of Zhengzhou University and Nanjing First Hospital of Nanjing Medical University in China between September and December 2021. The study included eligible participants who fulfilled the following criteria: individuals aged 20–65 years, women with history of sexual life, and indications for colposcopy due to abnormal cervical cytology or infection with HPV16 and 18. Participants who were pregnant, treated for cervical disease previously (including conization, physiotherapy, hysterectomy, neoadjuvant therapy), suffered from acute gynecological inflammation, other malignant tumors or serious systemic diseases were excluded. This study was approved by the Medical Ethics Committee in Peking University People’s Hospital (number 2021PHB056_001), the Third Affiliated Hospital of Zhengzhou University (number 2021-067-01) and Nanjing First Hospital of Nanjing Medical University (number KY20210604-05). Participants were identified and informed about the details by clinicians through face-to-face communication in the outpatient room. Written informed consent was obtained before enrollment.
Sample Collection
All participants were required to provide at least 20mL of the initial stream urine prior to gynecological examination using the specific urine collection kit (CerviClear®, a disposal collection kit containing 5mL preservative solution (New Horizon Co., Ltd)). Next, cervical samples were collected by a clinical collector using a cervical brush (Tellgen Corporation Co., Ltd) in a clockwise fashion with two 360° turns during the pelvic examination. All the samples were transported to the central laboratory of New Horizon Co., Ltd for subsequent hrHPV test. Colposcopy was conducted by a professional gynecologist who was blinded to the urine test results. After staining with 5% acetic acid, suspicious lesions and endocervical curettage (ECC) were performed for pathological biopsy. If there was no suspicious lesion, samples were taken from the four quadrants near the squamo-columnar junction area.
Sample Processing and Laboratory Analyses
The hrHPV tests for urine and cervical samples were performed in the central laboratory according to the manufacturer’s instructions, and the clinical diagnostic information was blinded to the laboratory staff. Briefly, samples were shipped to the laboratory and stored below −20°C before DNA extraction. During sample processing, 10mL of urine sample was transferred to a 50mL centrifuge tube containing 20μL magnetic bead-binding solution and vortex-mixed for 10s afterward at room temperature. With the supernatant removed, the pellet was resuspended in 300μL lysis buffer after 500μL washing solution added and transferred to a molecular tube containing 70μL diluent buffer. A negative control sample was involved in the whole DNA extraction process. Fifty microliters of negative control was added into a 1.5 mL centrifuge tube, and then Tris-EDTA buffer was added until the volume reaches 500μL. HPV DNA in cervical was purified using the kit from Tellgen Corporation Co., Ltd. The amplification of hrHPV DNA from urine sample was undertaken using CerviClear®, which was based on the ABI7500 real-time PCR system (Thermo Fisher Scientific Inc., USA). It identifies 14 types of hrHPV (HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) with HPV 16 and 18 detected with their own dedicated fluorescent dye and the other 12 types detected using the same fluorescent dye. HrHPV DNA from cervical sample was undertaken using High-risk HPV 2+12 assay kit (Tellgen Corporation Co., Ltd) which was based on the ABI7500 real-time PCR system and could also identify HPV 16, 18 and other 12 high-risk types (31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68). Finally, cycle number values for three HPV signals (HPV16, HPV18, and other hrHPV) were reported. The final result of urine and cervical test was defined as “valid result” with available positive and negative control results. After two retests, if the control results were still unavailable, the final result was defined as “invalid result”. Histological diagnosis served as “gold standard” for the clinical assessment in this study. Cervical biopsy samples were identified by a professional pathologist and reviewed by another practicing pathologist who was aware of the patient’s clinical information and cervical HPV test results but blinded to the urine results. Histologically confirmed disease endpoints were defined as CIN2+, including CIN2, CIN3, microinvasive cancer and squamous cell carcinoma (SCC), according to the published WHO classification of cervical cancer in 2020.20
Sample Size Considerations and Statistical Analyses
The sample size calculation was based on the hypothesis that the sensitivity of the urine hrHPV test for detecting CIN2+ is no less than 85%. At a two-sided type I error rate of 0.05 and a power of 80%, the minimum number required for CIN2+ patients is 65.
Descriptive statistics were used to assess the sociodemographic characteristics of included cases. We calculated the sensitivity and specificity with 95% confidence intervals (CIs) of hrHPV detection in urine and cervical samples against histologically confirmed results (<CIN2 versus CIN2+). And McNamar’s test was used to assess the difference between groups or tests. P < 0.05 were considered statistically different. Cohen’s kappa was used to measure concordance between urine and cervical for detecting hrHPV. Kappa values of ≤0 were defined as no agreement, 0.01–0.20 “poor” agreement, 0.21–0.40 “fair” agreement, 0.41–0.60 “moderate” agreement, 0.61–0.80 “substantial” agreement and 0.81–1.00 “perfect” agreement. Analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, N.Y., USA).
Results
Study Population
A total of 811 participants were recruited during the study period and 766 were eligible. Of these, 34 were excluded after enrolment due to the following reasons: invalid urine or cervical test (5), incomplete medical diagnosis records (12), and failure to undergo colposcopy when indicated (17). A total of 732 valid paired urine and cervical samples were analyzed. The mean age of these women was 41.2 ± 11.1 years with a medium of 40 years. The flow diagram for the study is shown in Figure 1.
 |
Figure 1 Flow diagram for the inclusion of study cases and the reasons excluded from the analysis. |
Clinical Performance for Cervical Intraepithelial Neoplasia Detection
Among the 732 included women, 130 (17.76%) had histologically confirmed CIN2+, including 75 with CIN2, 40 with CIN3 and 15 with microinvasive cancer or greater. For CIN2+ detection, the sensitivity of hrHPV test in urine and cervical samples was 87.69% and 94.62%, respectively, which showed marginal differences (P = 0.049) (Table 1). The specificity of hrHPV test showed significant differences between urine and cervical assays in the test of hrHPV (P<0.001), urine-based test performed better in the specificity than cervical samples (33.55% vs 26.91%). And for the CIN3+ detection, the sensitivity was 85.45% and 94.55% in urine and cervical samples, indicating no difference statistically (P=0.180). There was significantly different between the two assays in the specificity (31.02% vs 24.52%).
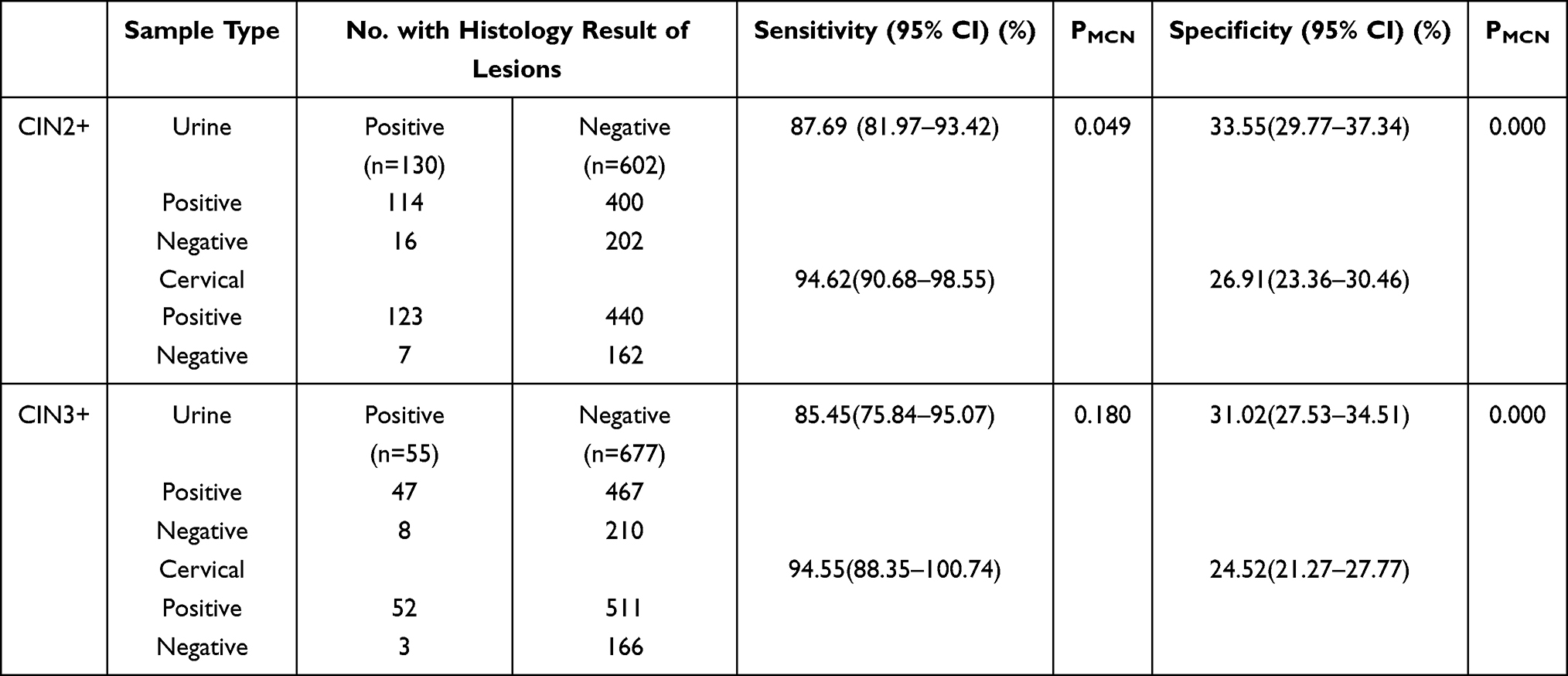 |
Table 1 Clinical Sensitivity and Specificity for CIN2+ of the hrHPV Test in Urine and Cervical Assay |
Performance of HPV Genotype for Detection of CIN2+
Subgroup analysis was conducted to analyze the performance of HPV16/18 and other high-risk types for the detection of CIN2+(Table 2). The results showed that the specificity of urine HPV16/18 was 82.23% and 94.52%, respectively, and the specificity of HPV16 in urine samples was better than that in the cervical samples (82.23% vs 78.84%, p = 0.05). And the sensitivity of HPV genotype was not statistically different between the two samples.
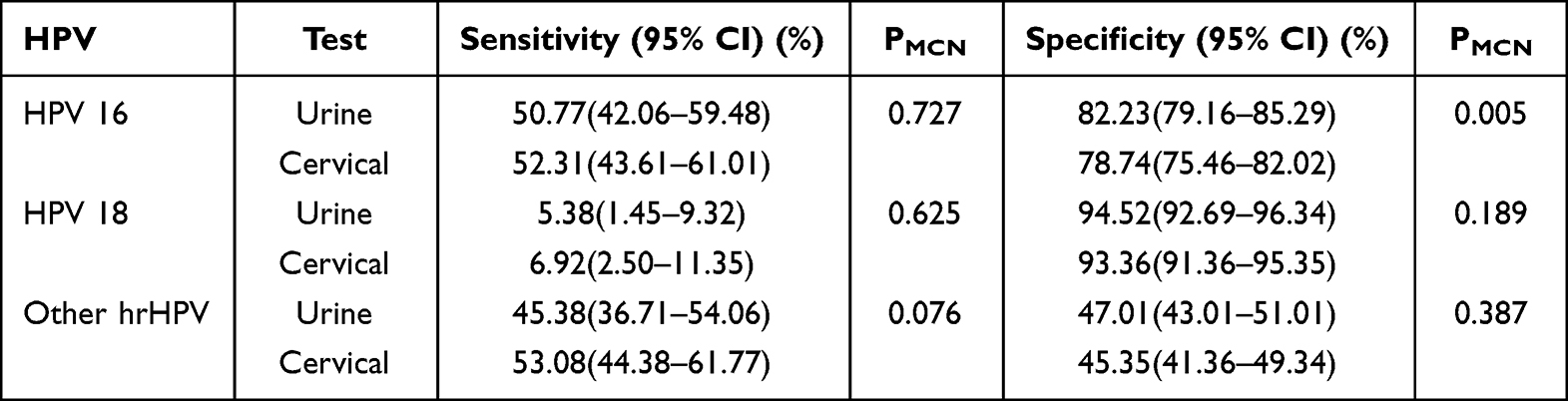 |
Table 2 HPV Genotype for Detection of CIN2+ |
Agreement in Different Samples
The overall agreement between hrHPV detection in urine and cervical assays was 80.74% with positive agreement of 83.13% and negative agreement of 72.78%. Urine-based hrHPV detection was in moderate agreement with cervical samples (kappa = 0.508). And the overall agreement of HPV16, 18 and other types was 91.67%, 96.58% and 81.69%, correspondingly, which suggested substantial agreement between urine and cervical assays (Table 3).
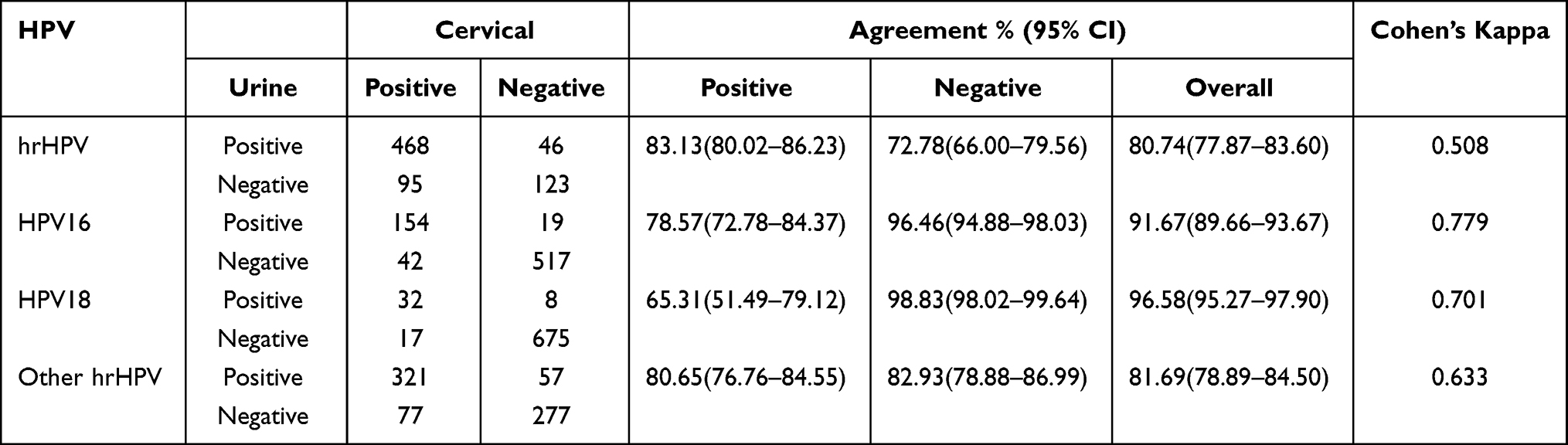 |
Table 3 Agreement Between Urine and Cervical Assay for Detecting hrHPV |
Discussion
Nowadays, cervical cancer screening methods mainly include liquid-based cytology (LBC) and HPV testing, which are both clinician-dependent and invasive for collection. Non-invasive and easy-to-use screening method may improve the coverage of cervical cancer screening. Therefore, the development of a more acceptable detection method with clinically validated accuracy has aroused attention in preventive care of the cervical cancer. It has been speculated that urine sample could be a feasible complement to the cervical cancer screening program, and a series of comprehensive studies have been conducted to compare the performance of hrHPV test results between urine and cervical samples. However, most of the studies used homemade or cervical hrHPV test, and the reported performance varied significantly. Cuzick et al17 showed that the sensitivity from urine was slightly lower than cervical test (CIN2+ 88.3% (95% CI, 81.9–93.0), P = 0.06; CIN3+ 91.4% (95% CI, 83.0–96.5), P = 0.30). However, Dorthe and colleagues demonstrated that urine was comparable to the cervical samples, with the sensitivity of 93% and 96% in urine and for detection of CIN2+.21 The significant heterogeneity may prevent the generation of high-quality evidence for deciding the role of urine HPV test in cervical cancer screening.
In this study, we evaluate and confirm the clinical performance of the newly developed standardized DNA-based hrHPV assay specially designed for urine test. Our study showed that the sensitivity of hrHPV for CIN2+ detection in women referred for colposcopy was at almost the same level in urine samples compared to cervical samples (87.69% vs 94.62%, p = 0.049). Further analysis also indicated that there was no statistical difference in sensitivity between HPV16/18 and other types for the detection of CIN2+. Meanwhile, urine samples performed better in specificity (33.55% vs 26.91%, p < 0.001). And for the detection of CIN3+, the sensitivity and specificity of the two samples performed similarly, which clearly demonstrated that CerviClear® assay has substantially potential to be applied in the detection of CIN.
The study indicated comparable or better results than previous studies. Faruk and colleagues observed a significantly lower sensitivity (77.6%, 95% CI: 66.8–88.4%) in urine samples using Colli-Pee.22 In 2022, a meta-analysis of 21 studies has shown that the urine HPV test had a pooled sensitivity of 79% (95% CI = 0.72–0.86) and specificity of 48% (95% CI = 0.42–0.54) compared with clinician-collected samples.16 However, it was also slightly lower than several studies. Senkomago et al examined 37 female colposcopy clinic attendees, and the results demonstrated that the sensitivity of HPV tests in urine for CIN2+ detection was 89.9% (95% CI, 62.7–99.6).23 It is obviously concluded from the studies that the results of various studies are not the same, which may be related to the large sample size of our study and heterogeneity across the studies, including the collection kit and sampling method. In addition, other important factors comparably influence the results of urine test, including storage conditions, DNA extraction, DNA amplification and transshipment, which will all generate substantial variation in clinical performance. Furthermore, the agreement for all hrHPV detections indicated moderate consistency between the two samples, which probably provided further evidence for certain homology in HPV detection. Higher agreements were obtained for the detection of HPV 16/18 with substantial consistency. In theory, the HPV-infected cervical epithelial cells slough off and enter the vagina with cervical secretions that accumulate near the vaginal and labia minora, which would be washed away with the first catch of urine passing through the vaginal orifice.24 As reported in the literature, the concentration of HPV DNA in urine is lower than cervical samples, so it is necessary to obtain HPV DNA in abundance and develop a sensitive detection method. The CerviClear® assay applied in our study has focused on optimization of the extraction process, which has contributed to better clinical performance than previous studies.25–29 Further studies are still needed to evaluate and improve the test accuracy. The COVID-19 pandemic has changed the model of global healthcare, and the European Federation for Colposcopy (EFC) and European Society of Gynaecological Oncology (ESGO)8 have made recommendations that the screening programs should be delayed in countries involved in COVID-19 epidemic. In China, the isolation measures are strictly conducted in high-risk areas which may produce blockage on the early screening of cervical cancer. Under such circumstances, urine-based HPV detection could serve as a promising countermeasure for primary screening of cervical cancer to avoid the impact of the epidemic. To our best knowledge, this is the first study to evaluate and confirm the value of the newly developed commercial available DNA-based assay specially designed for urine test, which expands the evidence for the effectiveness of self-sampling methods on the detection of cervical intraepithelial neoplasia. In conclusion, urine samples have sensitivity comparable to physician-collected cervical samples, which revealed that it could be a viable measure to attract nonresponders and increase screening rate especially in low-infrastructure settings.
Synopsis
- Confirm the performance of the standardized hrHPV assay designed for urine test.
- Expand the evidence for the effectiveness of self-sampling on the detection of CIN.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author Jianliu Wang (Email address: [email protected]), upon reasonable request.
Ethical Approval
This study was approved by the Medical Ethics Committee in Peking University People’s Hospital (number 2021PHB056_001), the Third Affiliated Hospital of Zhengzhou University (number 2021-067-01) and Nanjing First Hospital of Nanjing Medical University (number KY20210604-05). The study was conducted in accordance with the Helsinki Declaration.
Acknowledgments
Yun Zhao and Lijun Zhao are co-first authors for this study. We are grateful to all included women for their participation in the study. We thank HuiL Li, MingZ Li, Chao Zhao, JingR Li, YuanY Wang, Ting Zhang, JunJ Zhou, ShuJ Zhao, YaJ Zhang, Li Zhang, ShanH Xue, YanX Yu, Juan Chen, SuL Zhao, LiL Shi, WeiH Qi, Ai Chen, AiW Zhang, Ning Luo, YanB Liu, ChunY Xie, LinY Dong for the day-to-day coordination of this study, including the recruitment of participants and data collection, and the staff members of Peking University People’s Hospital, the Third Affiliated Hospital of Zhengzhou University and Nanjing First Hospital colposcopy clinics who supported this study. We also thank New Horizon Co., Ltd for donating the urine hrHPV test kits (CerviClear®) and Tellgen Corporation Co., Ltd for the cervical hrHPV test kits
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Xiaotian Yu is the Medical Director of New Horizon Ltd. The authors have no other competing interests to declare for this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Walboomers JM, Jacobs MV, Manos MM, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189(1):12–19. doi:10.1002/(SICI)1096-9896(199909)189:1<12::AID-PATH431>3.0.CO;2-F
3. WHO Guidelines Approved by the Guidelines Review Committee, in WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention.
4. Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American cancer society. CA Cancer J Clin. 2020;70(5):321–346. doi:10.3322/caac.21628
5. Curry SJ,Krist AH, Owens DK, et al. Screening for cervical cancer: us preventive services task force recommendation statement. JAMA. 2018;320(7):674–686. doi:10.1001/jama.2018.10897
6. Sargent A, Fletcher S, Bray K, et al. Cross-sectional study of HPV testing in self-sampled urine and comparison with matched vaginal and cervical samples in women attending colposcopy for the management of abnormal cervical screening. BMJ Open. 2019;9(4):e025388. doi:10.1136/bmjopen-2018-025388
7. Pruitt SL, Werner CL, Borton EK, et al. Cervical cancer burden and opportunities for prevention in a safety-net healthcare system. Cancer Epidemiol Biomarkers Prev. 2018;27(12):1398–1406. doi:10.1158/1055-9965.EPI-17-0912
8. Ciavattini A, Delli Carpini G, Giannella L, et al. European federation for colposcopy (EFC) and European society of gynaecological oncology (ESGO) joint considerations about human papillomavirus (HPV) vaccination, screening programs, colposcopy, and surgery during and after the COVID-19 pandemic. Int J Gynecol Cancer. 2020;30(8):1097–1100. doi:10.1136/ijgc-2020-001617
9. Zhang M, Zhong Y, Zhao Z, et al. cervical cancer screening rates among Chinese women - china, 2015. China CDC Wkly. 2020;2(26):481–486. doi:10.46234/ccdcw2020.128
10. Lam JUH, Elfström KM, Ejegod DM, et al. High-grade cervical intraepithelial neoplasia in human papillomavirus self-sampling of screening non-attenders. Br J Cancer. 2018;118(1):138–144. doi:10.1038/bjc.2017.371
11. Miller MJ, Xu L, Qin J, et al. Impact of COVID-19 on cervical cancer screening rates among women aged 21–65 years in a large integrated health care system - Southern California, January 1-September 30, 2019, and January 1-September 30, 2020. MMWR. 2021;70(4):109–113. doi:10.15585/mmwr.mm7004a1
12. Chamot E, Mulambia C, Kapambwe S, et al. Preference for human papillomavirus-based cervical cancer screening: results of a choice-based conjoint study in Zambia. J Low Genit Tract Dis. 2015;19(2):119–123. doi:10.1097/LGT.0000000000000081
13. Shin HY, Lee B, Hwang S-H, et al. Evaluation of satisfaction with three different cervical cancer screening modalities: clinician-collected pap test vs. HPV test by self-sampling vs. HPV test by urine sampling. J Gynecol Oncol. 2019;30(5):e76. doi:10.3802/jgo.2019.30.e76
14. Chatzistamatiou K, Vrekoussis T, Tsertanidou A, et al. Acceptability of self-sampling for human papillomavirus-based cervical cancer screening. J Womens Health. 2020;29(11):1447–1456. doi:10.1089/jwh.2019.8258
15. Pattyn J,Van Keer S, Téblick L, et al. Non-invasive assessment of vaccine-induced hpv antibodies via first-void urine. Front Immunol. 2020;11:1657. doi:10.3389/fimmu.2020.01657
16. Cho HW,Shim SR, Lee JK, et al. Accuracy of human papillomavirus tests on self-collected urine versus clinician-collected samples for the detection of cervical precancer: a systematic review and meta-analysis. J Gynecol Oncol. 2022;33(1):e4. doi:10.3802/jgo.2022.33.e4
17. Cuzick J, Cadman L, Ahmad AS, et al. Performance and diagnostic accuracy of a urine-based human papillomavirus assay in a referral population. Cancer Epidemiol Biomarkers Prev. 2017;26(7):1053–1059. doi:10.1158/1055-9965.EPI-16-0960
18. Rohner E, Rahangdale L, Sanusi B, et al. Test accuracy of human papillomavirus in urine for detection of cervical intraepithelial neoplasia. J Clin Microbiol. 2020;58(3):doi:10.1128/JCM.01443-19
19. Daponte A, Michail G, Daponte A-I, et al. Urine HPV in the context of genital and cervical cancer screening-an update of current literature. Cancers. 2021;13(7):1640. doi:10.3390/cancers13071640
20. Höhn AK, Brambs CE, Hiller GGR, et al. 2020 WHO classification of female genital tumors. Geburtshilfe Frauenheilkd. 2021;81(10):1145–1153. doi:10.1055/a-1545-4279
21. Ørnskov D, Jochumsen K, Steiner PH, et al. Clinical performance and acceptability of self-collected vaginal and urine samples compared with clinician-taken cervical samples for HPV testing among women referred for colposcopy. A cross-sectional study. BMJ Open. 2021;11(3):e041512. doi:10.1136/bmjopen-2020-041512
22. Ertik FC, Kampers J, Hülse F, et al. CoCoss-trial: concurrent comparison of self-sampling devices for HPV-detection. Int J Environ Res Public Health. 2021;18(19):10388. doi:10.3390/ijerph181910388
23. Senkomago V,Des Marais AC, Rahangdale L, et al. Comparison of urine specimen collection times and testing fractions for the detection of high-risk human papillomavirus and high-grade cervical precancer. J Clin Virol. 2016;74:26–31. doi:10.1016/j.jcv.2015.11.005
24. Pattyn J, Van Keer S, Téblick L, et al. HPV DNA detection in urine samples of women: ‘an efficacious and accurate alternative to cervical samples?’. Expert Rev Anti Infect Ther. 2019;17(10):755–757. doi:10.1080/14787210.2019.1668776
25. Hwang S-H, Shin HY, Lee DO, et al. A prospective pilot evaluation of vaginal and urine self-sampling for the roche cobas 4800 HPV test for cervical cancer screening. Sci Rep. 2018;8(1):9015. doi:10.1038/s41598-018-27390-5
26. Khunamornpong S, Settakorn J, Sukpan K, et al. Comparison of human papillomavirus detection in urine and cervical samples using high-risk HPV DNA testing in northern Thailand. Obstet Gynecol Int. 2016;2016:6801491. doi:10.1155/2016/6801491
27. Stanczuk GA, Currie H, Baxter G, et al. Cobas 4800 HPV detection in the cervical, vaginal and urine samples of women with high-grade CIN before and after treatment. J Clin Pathol. 2015;68(7):567–570. doi:10.1136/jclinpath-2014-202851
28. Arias M, Jang D, Dockter J, et al. Treatment of first-void urine with aptima transfer solution increases detection of high-risk HPV E6/E7 mRNA. J Virol Methods. 2019;267:48–52. doi:10.1016/j.jviromet.2019.02.007
29. Asciutto KC, Ernstson A, Forslund O, et al. Self-sampling with HPV mRNA analyses from vagina and urine compared with cervical samples. J Clin Virol. 2018;101:69–73. doi:10.1016/j.jcv.2018.02.002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Human Papillomavirus Infection Characteristics for Patients with Cervical Intraepithelial Neoplasia in Yunnan, China: A Sampling Survey Analysis
Zhi HF, Yang LF, Ge J, Yang XT
Infection and Drug Resistance 2022, 15:2843-2851
Published Date: 1 June 2022