Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Clinical Outcomes Of Using Nebulized Budesonide As The Initial Treatment For Acute Exacerbations Of Chronic Obstructive Pulmonary Disease: A Post-Hoc Analysis
Authors Zheng JP, Zhang J, Ma LJ, Chen P, Huang M, Ou XM, Zhao ZW, Jiang SJ, Cao J, Yao W
Received 30 November 2018
Accepted for publication 12 September 2019
Published 29 November 2019 Volume 2019:14 Pages 2725—2731
DOI https://doi.org/10.2147/COPD.S196615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chunxue Bai
Jin-Ping Zheng,1,* Jing Zhang,2,* Li-Jun Ma,3 Ping Chen,4 Mao Huang,5 Xue-Mei Ou,6 Zi-Wen Zhao,7 Shu-Juan Jiang,8 Jie Cao,9 Wanzhen Yao2
1State Key Laboratory of Respiratory Disease, National Clinical Research Center, Guangzhou Institute of Respiratory Health, First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China; 2Department of Respiratory Medicine, Peking University Third Hospital, Beijing, People’s Republic of China; 3Department of Respiratory Medicine, Henan Provincial People’s Hospital, Henan, People’s Republic of China; 4Department of Internal Medicine, The Second Xiangya Hospital, Hunan, People’s Republic of China; 5Jiangsu Province Hospital, Jiangsu, People’s Republic of China; 6Department of Respiratory Medicine, West China Hospital, Chengdu, People’s Republic of China; 7Department of Respiratory Medicine, Guangzhou First People’s Hospital, Guangzhou, People’s Republic of China; 8Department of Respiratory Medicine, Shandong Provincial Hospital, Shandong, People’s Republic of China; 9Department of Respiratory Medicine, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wanzhen Yao
Department of Respiratory Medicine, Peking University Third Hospital, 49 North Garden Road, Beijing 100191, People’s Republic of China
Tel +86 156 1190 8216
Email [email protected]
Purpose: The current guidelines recommend the use of systemic corticosteroids (SCS) as the optimal treatment for acute exacerbations of chronic obstructive pulmonary disease (AECOPD). The aim of this real-world study was to evaluate whether nebulized budesonide (NBS) could also be used as an initial treatment for AECOPD.
Patients and methods: AECOPD patients initially treated with NBS or SCS (oral/intravenous) were enrolled. A large-scale, long-term multicenter cohort study of AECOPD patients was performed to analyze outcomes for each treatment (NCT02051166).
Results: Initial NBS and SCS treatment resulted in similar outcomes in terms of improvements in FEV1, PaO2, SaO2, and PaCO2. Disease severity affected outcome similarly in both groups. When the groups were stratified according to whether the initial treatment was subsequently intensified or reduced, more intubation was seen in the groups in which initial treatment was intensified. NBS escalation and SCS reduction groups spent more days in the hospital. The NBS escalation group was associated with the highest medical expenditure and a relatively higher rate of new-onset pneumonia. The NBS maintenance/reduction group showed the lowest mortality rate between groups. Stratification according to initial PaCO2 level showed more intubation in the groups with high initial PaCO2 concentrations.
Conclusion: These results indicate that NBS may be used as an initial treatment in certain AECOPD patients, and further studies are needed to better define those most likely to benefit.
Keywords: nebulized budesonide, systemic corticosteroids, chronic obstructive pulmonary disease, AECOPD
Introduction
Chronic obstructive pulmonary disease (COPD) affects 65 million people worldwide and is responsible for 3 million deaths per year.1 Most patients with COPD have at least one acute exacerbation of this disease (AECOPD) per year.2,3 Such exacerbations cause a decline in lung function, reduced quality of life, increased mortality, and an increased risk of further AECOPD.4 Treatment for AECOPD often requires hospitalization and is responsible for 60% of the global costs for COPD treatment.5
Systemic corticosteroids have been considered as the cornerstone of treatment for AECOPD2,6–8 and inhaled corticosteroids as useful for maintenance treatment thereafter to reduce the risk of further exacerbations.3,6 However, continued use of systemic corticosteroids will cause steroid resistance and systemic side effects. Also, higher doses or longer periods of treatment for AECOPD do not improve outcomes, and the optimal dosage of systemic corticosteroids for AECOPD is unclear.1,7,9
The use of nebulized instead of systemic corticosteroids to treat AECOPD would theoretically confine the anti-inflammatory action to the lung and avoid the undesirable systemic effects associated with oral or intravenous corticosteroid administration. In clinical practice, both nebulized budesonide (NBS) and systemic corticosteroids (SCS) are used for the initial treatment of AECOPD. A number of comparisons of NBS and SCS treatment of AECOPD have reported similar outcomes.2,10–13 To date, no study has been conducted on the results of initial NBS and SCS usage in general clinical practice. In the current report, we hypothesized that initial NBS and SCS, as used for AECOPD in current clinical practice, would give similar results. Our aim was to evaluate the real-world status of initial NBS and SCS usage in AECOPD in China and to determine what pre-treatment patient characteristics would potentially suggest the suitability of using NBS rather than SCS as initial AECOPD treatment.
Methods
Study Design And Patient Selection
The current study was a post-hoc analysis of a subset of data collected from a large, retrospective non-interventional study in China of corticosteroid treatment of patients hospitalized for AECOPD (NCT02051166).14 Patients were selected according to the initial therapy they received: NBS alone or SCS (oral/intravenous) alone. In our study, those who had received either NBS or SCS (oral/intravenous) for initial treatment of AECOPD were divided into two NBS groups (escalation group, defined as initial NBS followed by dose escalation or switch to SCS; maintenance group, defined as initial NBS followed by dose maintenance or reduction) and two SCS groups (maintenance group, defined as initial SCS followed by dose maintenance or escalation; reduction group, defined as initial SCS followed by dose reduction or switch to NBS). The demographics, clinical characteristics, and outcomes of the four groups were then compared to evaluate the real-world status of initial use of nebulized or systemic corticosteroids for the treatment of AECOPD and to determine which patients might benefit from initial NBS treatment. Since guidelines in China recommend antibiotic treatment for patients with COPD, most patients included in this study (97%) received such treatment. Thus, antibiotic use may not affect the results of this study. In addition, these included patients who did not receive other therapy, such as diuretics, non-invasive ventilation, and high flow nasal canula.
The study was conducted in accordance with the guidelines of the Helsinki Declaration and was approved by independent ethics committees at all study sites prior to the start of the study, including the Peking University Third Hospital Medical Science Research Ethics Committee [2013-98-ssh-hxx (2013-100)]; Institutional Review Board of Beijing ChaoYang Hospital (IRB20140109); Institutional Review Board of Beijing Chaoyang Hospital, Capital Medical University [2014-02-21 (1)]; Ethics Committee of Beijing Tongren Hospital, Capital Medical University (TREC2014-03); Ethical Committee of Ruijin Hospital Affiliated to Shanghai JiaoTong University School of Medicine (2014-16); Huashan Hospital Institutional Review Board (2014-5-26); Ethical Committee of Shanghai Pulmonary Hospital (3-075HX); Ethical Committee of the Fifth People’s Hospital of Shanghai (2014-016); Ethics committee of the Institutional Review Board of Shanghai Songjiang Central Hospital [201415-(2013-98-SSH-HXK)]; Ethics Committee of the Shanghai Minhang District Central Hospital of Ruijin Group [IRB20140325]; Peking University Third Hospital Medical Science Research Ethics Committee [2013-98-ssh-hxx (100)]; Ethics Committee of the First Affiliated Hospital, Nanjing Medical University, Jiangsu Province Hospital (IRB20140225); ERB of Guangzhou First People hospital (SOP-CX-011-03); Ethical Committee of Jiangsu Province (2014-SR-020); Committee of Nanjing General Hospital of Nanjing Military Command (2014NLY-003); Shandong Provincial Qianfoshan Hospital medical ethics committee (IRB20140211); Ethical Committee of The General Hospital Tianjin Medical University (IRB2013-088-01); Ethical Committee of The General Hospital of Shenyang Military Region (2014-#12); Ethics Committee of The First Hospital of Jilin University (140313-028); The Institutional Review Board of Second Hospital of Jilin University (2014-003); The Institutional Review Board of the Affiliated Hospital of Inner Mongolia University (2013MER-0002); The Institutional Review Board of the Affiliated Hospital of Inner Mongolia Medical University (2014-002); The Institutional Review Board of Hebei Provincial People’s Hospital (Y-2014-01); Ethical Committee of The Second Hospital of Hebei Medical University (IRB20140314); The Institutional Review Board of China National Petroleum Corporation Central Hospital (IRB20140109); Ethics Committee of Shanxi Provincial People’s Hospital (IRB20140301); Shanxi Dayi Hospital Ethical Committee (IRB20140402); Ethics Committee of First Hospital of Shanxi Medical University (2014-13); The Institutional Review Board of Yuncheng Central Hospital of Shanxi Province (IRB20140116); Institutional Review Board of Henan Provincial People’s Hospital (IRB20140308); Institutional Review Board of the People’s Hospital of Zhengzhou University (IRB20140228); Ethics Committee of Anhui Medical University (PJ2014-02-04); Ethics Committee of Fujian Provincial Hospital (IRB20140516); Institutional Review Board and the Ethics Committee at Jiangxi Province People’s Hospital (2014-004); Ethics Committee of Hubei Province Hospital of Traditional Chinese Medicine (2014-013); Ethics Committee Xiangya Hospital of Central-South University (IRB201403021); Ethical Committee of The Third Xiangya. Hospital of Central South University (2014-IRB-022); IRB of West China Hospital (2014-1); Ethical Committee of the First Affiliated Hospital of Third Military Medical University, PLA (2014-10); Ethics Committee of Xinqiao Hospital, Third Military Medical University (2014026); Medical Ethics Committee of Shaanxi Provincial People’s Hospital (2014-R003); IEC of Institution for National Drug Clinical Trails, Tangdu Hospital, Fourth Military Medical University (IRB2014013); Medical Ethics Committee of General Hospital of Ningxia Medical University (IRB20140306). Written informed consents were obtained from all patients prior to the start of the study.
Inclusion And Exclusion Criteria
The inclusion criteria in this study were as follows: (1) being older than 40 years; (2) being hospitalized due to AECOPD; and (3) having COPD for at least 3 months before the acute exacerbation. Exclusion criteria were (1) participation in any interventional study within 3 months of recruitment; (2) ongoing AECOPD during the recruitment period; (3) being discharged against medical advice; and (4) having a primary diagnosis for hospitalization other than AECOPD.
Variables
Demographic characteristics (age weight, height, BMI), smoking status, environment and drug exposure history, and intubation rate were taken from the study data, as well as the endpoint parameters listed below.
Primary endpoints were length of hospital stay (days) and change in FEV1, arterial blood gases (PaO2, SaO2, PaCO2), and pH after treatment. Secondary endpoints were rate of new-onset pneumonia during hospitalization and hospitalization expenses related to AECOPD.
Statistical Analysis
Continuous variables were presented as mean and standard deviation (SD), and categorical variables were presented as counts and percentages. One-way analysis of variance and Chi-square test were used to compare the difference between the four treatment groups with regard to intubation rate, mortality, rate of pneumonia, and rate of new-onset pneumonia. All statistical analyses were performed using SAS® version 9.4 (SAS Institute, Inc., Cary, NC, USA). Two-tailed P < 0.05 indicated statistical significance.
Results
Demographic Characteristics
Of the 3121 patients included in the current study, 756 (the NBS escalation group) were initially treated with NBS and then with dose escalation or a switch to SCS, while 1443 patients (the NBS maintenance/reduction group) were initially treated with NBS and then with dose maintenance or reduction. Some 404 patients (the SCS maintenance/escalation group) were initially treated with SCS and then with dose maintenance or escalation; the remaining 518 patients (the SCS reduction group) were initially treated with SCS and then with dose reduction or a switch to NBS.
Patients in the NBS groups were slightly younger and had lower baseline PaO2 than patients in the SCS groups. Baseline PaCO2 was lowest in the NBS maintenance/reduction group and highest in the SCS reduction group (Table 1).
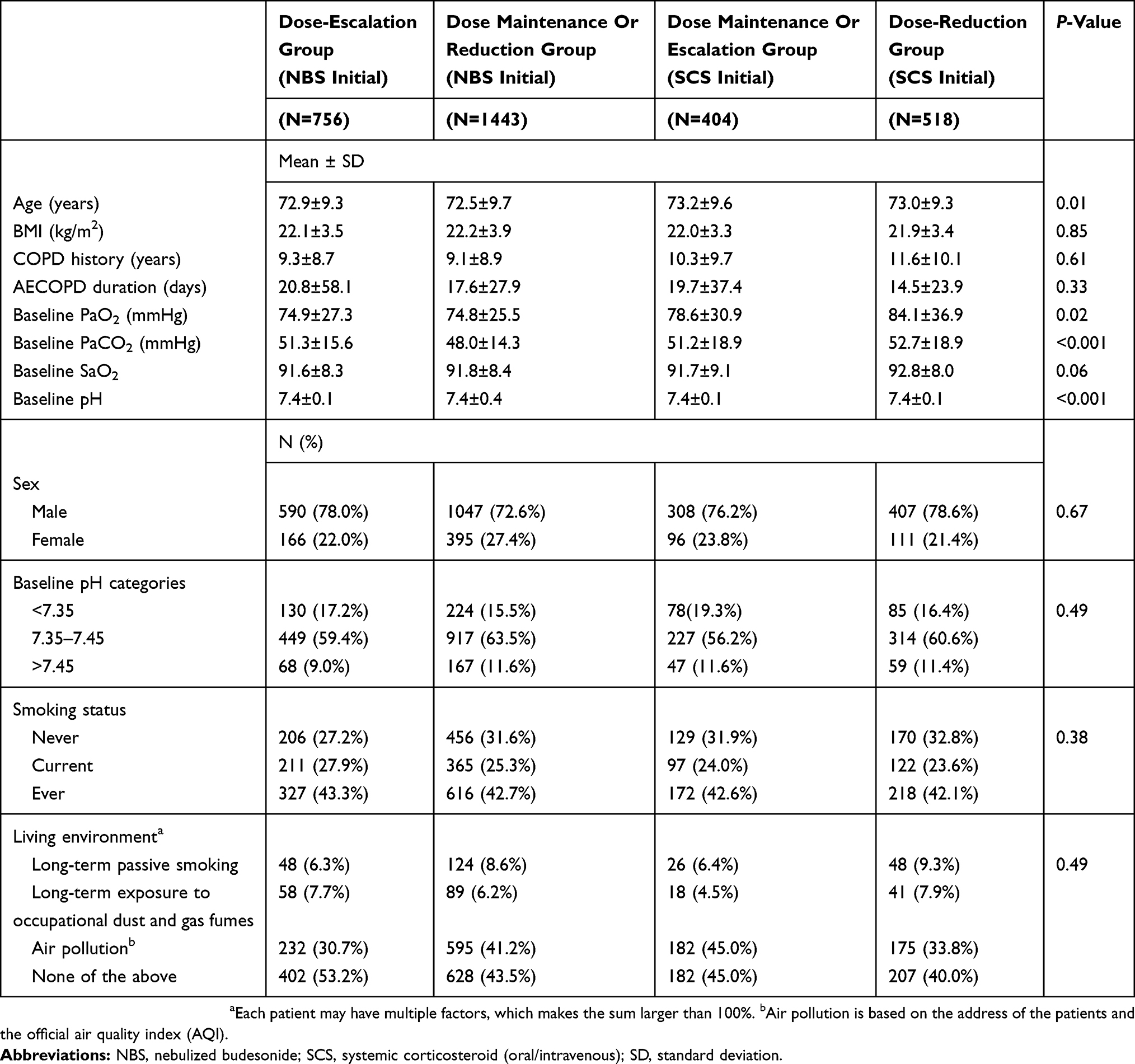 |
Table 1 Demographic Characteristics For NBS Or SCS By Intravenous Injection As Initial Treatment (Grouped By Further Treatment) |
Clinical Outcomes
Significant between-group differences were seen in length and expense of hospital stay, mortality, intubation, and improvement in FEV1 (Table 2). Mortality and intubation rates were higher in the two groups needing treatment escalation. Patients in the NBS maintenance/reduction group and those in the SCS maintenance/escalation group spent fewer days in the hospital. FEV1 improvement was worst (negative) in the NBS escalation group and best in the NBS maintenance/reduction group. Likewise, the NBS escalation group was associated with the highest hospitalization expenses of all groups, whereas expenses were lowest for the NBS maintenance/reduction group. No between-group differences were seen in improvement in arterial O2, CO2, or pH, or in the incidence of new-onset pneumonia.
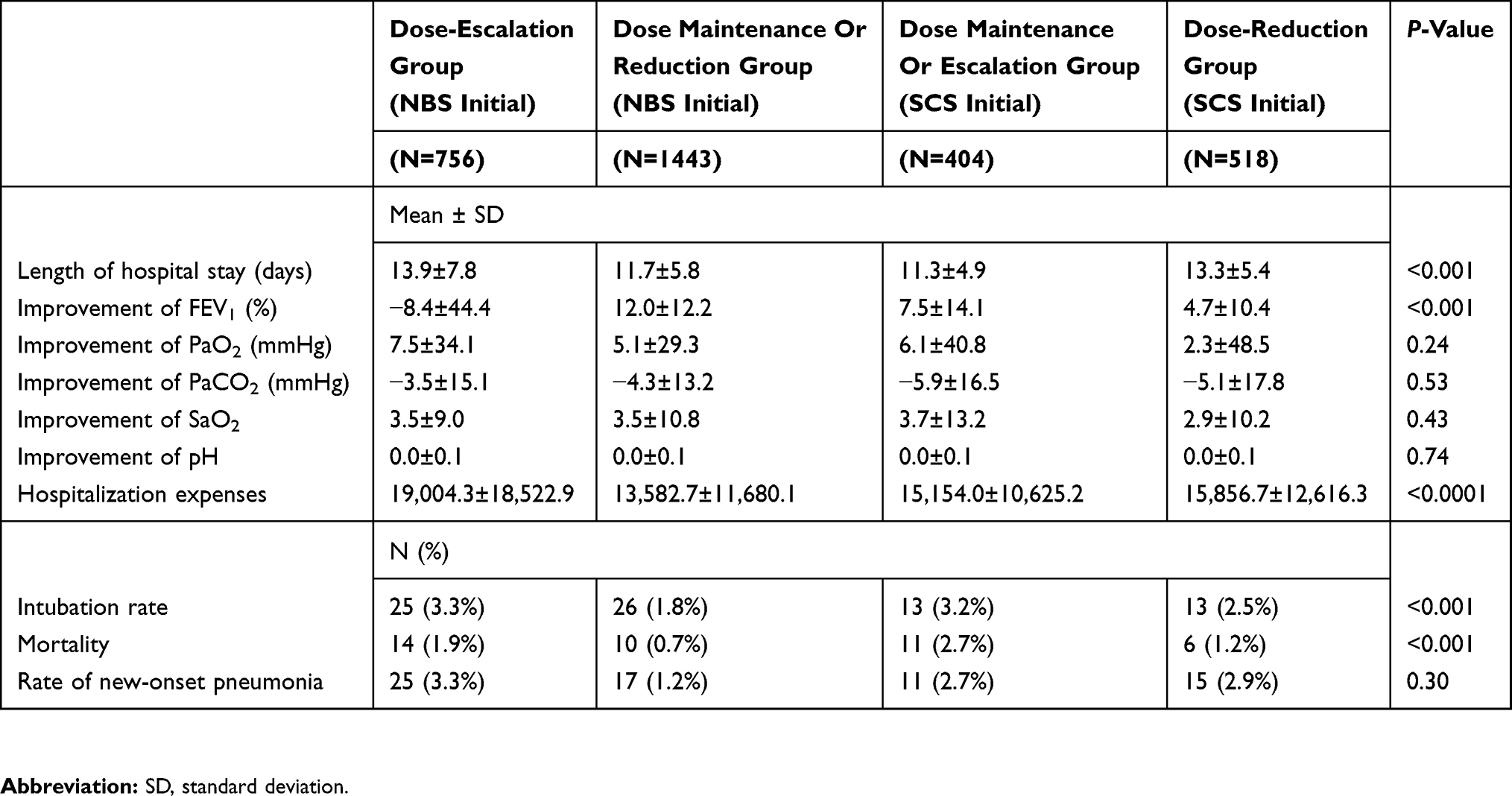 |
Table 2 Clinical Outcomes Of NBS Or SCS By Intravenous Injection As Initial Treatment (Grouped By Further Treatment) |
Stratified Analysis By Baseline PaCO2
When the four groups were stratified by baseline PaCO2 (PaCO2 ≤ 50 mmHg and PaCO2 > 50 mmHg), between-group differences were seen in mortality in both high and low PaCO2 groups and in intubation rates in the high PaCO2 group (Table 3). The SCS escalation group had a higher mortality rate in those with both low and high baseline PaCO2. In those with high baseline PaCO2, the SCS escalation group had the highest rate of intubation and the NBS maintenance/reduction group the lowest (Table 3).
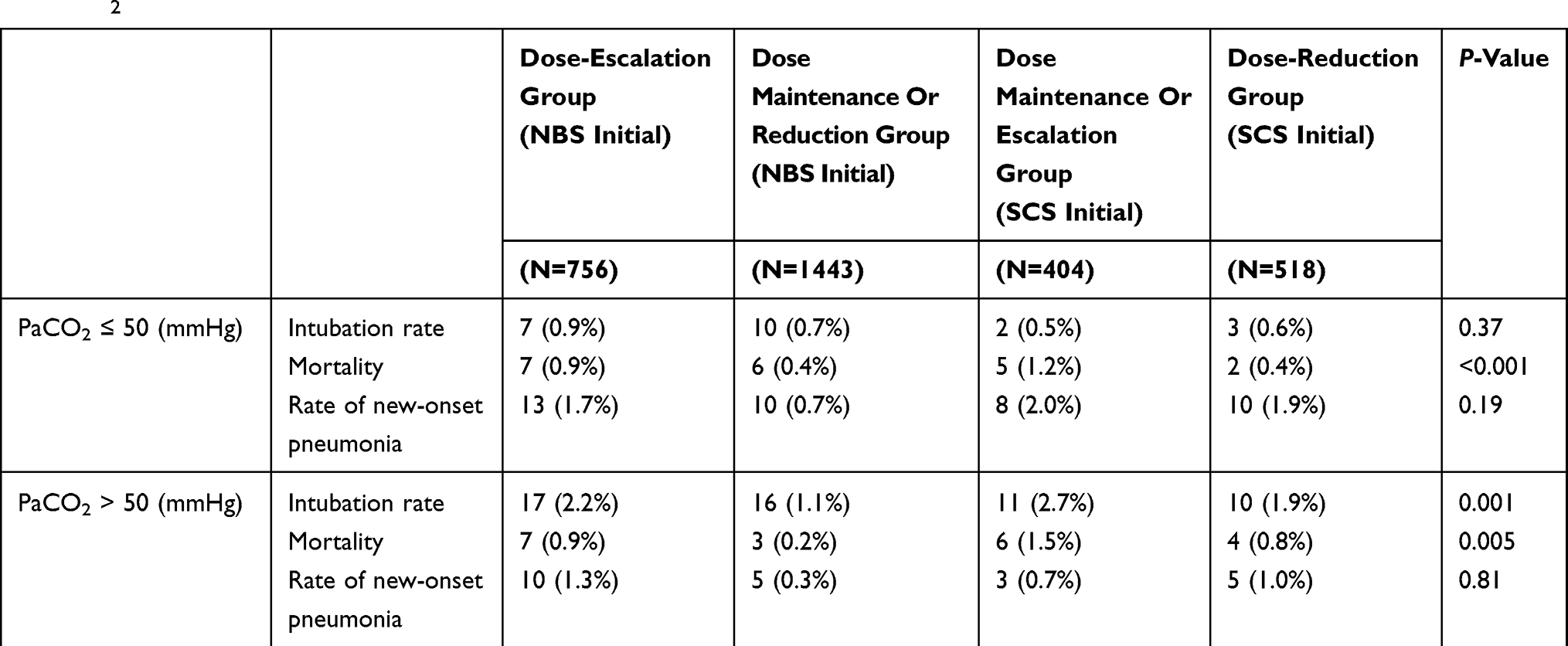 |
Table 3 Clinical Outcomes Of NBS Or SCS By Intravenous Injection As Initial Treatment (Grouped By Further Treatment), Stratified By PaCO2 |
Discussion
In the current post-hoc analysis of a subpopulation from a large, multicenter, non-interventional study of corticosteroid use to treat AECOPD in China,14 initial use of NBS or SCS for AECOPD generally resulted in similar outcomes and improvements in FEV1, PaO2, SaO2, and PaCO2.
In previous comparisons of the effectiveness of NBS and SCS in the treatment of AECOPD, the two corticosteroid delivery methods have been reported to be more effective than placebo (that is, standard but non-corticosteroid treatment),10–12 and to cause similar improvements in FEV12,10–13 and pH.2 In a meta-analysis of five studies, NBS was reported to be non-inferior to SCS.15 Two studies reported that the increase in PaO2 was significantly greater with SCS treatment2,12 and two reported hyperglycemia with SCS, but not NBS, treatment.19,12 One study reported decreased serum concentrations of inflammatory markers with both NBS and SCS treatment,13 but this study included only AECOPD patients who were also suffering from a bacterial infection, and so the decrease in inflammatory mediators was very likely due to antibiotic treatment rather than corticosteroid action. These previous studies were mostly small, with narrowly controlled subject eligibility. Our study results of initial NBS and SCS treatment as used in clinical practice extend these previous results. We also evaluated the effects of later dose escalation or reduction and of initial PaCO2 and found these parameters to influence NBS and SCS outcomes. In particular, lower initial PaCO2 might allow for selection of appropriate patients for initial NBS treatment, but additional controlled studies are needed to better define those most likely to benefit from such treatment.
Our results also showed that, for both NBS and SCS initial treatment, the intubation and mortality rates of the escalation groups were high and similar, with the highest initial hospital cost in the NBS dose-escalation group. Although the use of NBS cannot completely replace the use of SCS for AECOPD patients, the results suggest that certain patients can be considered for NBS therapy during AECOPD. In addition, some patients can be considered for SCS treatment at the outset, and then assessed as to whether a further combination therapy is needed.
Although initial SCS treatment was associated with a shorter duration of AECOPD than initial NBS treatment in the dose-reduction group (14.5 vs. 17.6 days), the difference was not significant (p=0.33). In contrast, those in the dose-reduction group receiving initial NBS treatment indeed had shorter length of hospital stays than those receiving initial SCS treatment (11.7 vs. 13.3 days, p<0.001). However, the dose-escalation group showed different and interesting results. Although the difference was not significant (p=0.33, Table 1), initial SCS treatment was associated with a shorter duration of AECOPD than initial NBS treatment in the dose-escalation group. Similarly, results in Table 2 showed shorter length of hospital stays in the initial SCS group than in the initial NBS group (11.3 vs. 13.9 days, p<0.001). Accordingly, SCS may be slightly preferable to NBS in sicker patients (the dose-escalation group). However, when the dose was reduced (dose-reduction group), NBS treatment performed better and can be considered a better option in the future. The matter warrants further investigation.
In China, it is a routine practice for hospitalized AECOPD patients to be treated with antibiotics to reduce the incidence of pneumonia (97% of the patients in the current study). This practice may be the main reason why the incidence of pneumonia was not significantly different between groups. However, there was a trend for a lower incidence of pneumonia in the NBS-initial/dose-reduction group.
Limitations of the study are its retrospective and post-hoc nature. For example, data availability was limited by the objective of the primary study, and information on comorbidities and the use of other drugs were not included in this analysis. Use of antibiotics was not a limiting factor, because 97% of the patients received such therapy, in accordance with China guidelines for the treatment of patients with COPD. Other initial drug selection was related to exacerbation severity at the time the patients were hospitalized, but the only such information available were test results such as PaO2 and PaCO2, and these, by themselves, are not sufficient for a complete description of the initial severity of the exacerbation. An example of the insufficiency of the available data is that, although overall improvement in FEV1 was similar in the NBS and SCS groups, FEV1 worsened in the NBS escalation group and improved in the NBS maintenance/reduction group. This anomaly probably reflects the initial seriousness of the AECOPD. Another probable effect of the underlying initial clinical condition was that the SCS escalation group had a higher mortality rate than the other three groups and that both dose-escalation groups had a higher intubation incidence than the dose-reduction groups when initial PaCO2 was high. Inclusion of relevant clinical symptoms might have clarified these results.
Conclusion
In summary, these results suggest that, in current clinical practice in China, NBS can be used for initial treatment of AECOPD in certain patients. A lower initial PaCO2 may allow for the selection of appropriate patients for such treatment, but further studies are needed to better define those most likely to benefit from NBS therapy.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank all patients and investigators involved in the study (see Appendix for a full list of investigators). In addition, the authors would like to thank Convergence CT for providing writing assistance and editorial support during development of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kiser TH, Vandivier RW. Severe acute exacerbations of chronic obstructive pulmonary disease: does the dosage of corticosteroids and type of antibiotic matter? Curr Opin Pulm Med. 2015;21:142–148. doi:10.1097/MCP.0000000000000142
2. Ding Z, Li X, Lu Y, et al. A randomized, controlled multicentric study of inhaled budesonide and intravenous methylprednisolone in the treatment on acute exacerbation of chronic obstructive pulmonary disease. Respir Med. 2016;121:39–47. doi:10.1016/j.rmed.2016.10.013
3. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of COPD; 2016. Available from: http://goldccopd.org/global-strategy-disgnosis-management-preventioin-copd-2016/.
4. Bishwakarma R, Zhang W, Kuo YF, et al. Long-acting bronchodilators with or without inhaled corticosteroids and 30-day readmission in patients hospitalized for COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:477–486. doi:10.2147/COPD.S122354
5. Bourbeau J, Sedeno MF, Metz K, et al. Early COPD exacerbation treatment with combination of ICS and LABA for patients presenting with mild-to-moderate worsening of dyspnea. COPD. 2016;13:439–447. doi:10.3109/15412555.2015.1101435
6. Chow L, Parulekar AD, Hanania NA. Hospital management of acute exacerbations of chronic obstructive pulmonary disease. J Hosp Med. 2015;10:328–339. doi:10.1002/jhm.2334
7. Kiser TH, Allen RR, Valuck RJ, et al. Outcomes associated with corticosteroid dosage in critically ill patients with acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014;189:1052–1064. doi:10.1164/rccm.201401-0058OC
8. Walters JA, Tan DJ, White CJ, et al. Systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;9:CD001288. doi:10.1002/14651858cd001288.pub4
9. Kiser TH, Sevransky JE, Krishnan JA, et al. A survey of corticosteroid dosing for exacerbations of chronic obstructive pulmonary disease requiring assisted ventilation. Chronic Obstr Pulm Dis. 2017;4:186–193. doi:10.15326/jcopdf.4.3.2016.0168
10. Maltais F, Ostinelli J, Bourbeau J, et al. Comparison of nebulized budesonide and oral prednisolone with placebo in the treatment of acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;165:698–703. doi:10.1164/ajrccm.165.5.2109093
11. Mirici A, Meral M, Akgun M. Comparison of the efficacy of nebulized budesonide with parenteral corticosteroids in the treatment of acute exacerbations of chronic obstructive pulmonary disease. Clin Drug Invest. 2003;23:55–62. doi:10.2165/00044011-200323010-00007
12. Gunen H, Hacievliyagil SS, Yetkin O, et al. The role of nebulized budesonide in the treatment of exacerbations of COPD. Eur Respir J. 2007;29:660. doi:10.1183/09031936.00073506
13. Sun X, He Z, Zhang J, et al. Compare the efficacy of inhaled budesonide and systemic methylprednisolone on systemic inflammation of AECOPD. Pulm Pharmacol Ther. 2015;31:111–116. doi:10.1016/j.pupt.2014.09.004
14. Zhang J, Zheng J, Huang K, et al. Use of glucocorticoids in patients with COPD exacerbations in China: a retrospective observational study. Ther Adv Respir Dis. 2018;12:1–7. doi:10.1177/1753466618769514
15. Zhai Y, Zhang H, Sun T, et al. Comparative efficacies of inhaled corticosteroids and systemic corticosteroids in treatment of chronic obstructive pulmonary disease exacerbations: a systematic review and meta-analysis. J Aerosol Med Pulm Drug Deliv. 2017;30(5):289–298. doi:10.1089/jamp.2016.1353
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.