")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Outcomes of Anticoagulant Therapy in COVID-19 Patients with Pre-Existing Cardiovascular Diseases: A Systematic Review
Authors Alhawiti NM, Alhawiti JM, Alshalan SD, Alotaibi BA, Khobrani AY
Received 20 March 2023
Accepted for publication 25 May 2023
Published 14 June 2023 Volume 2023:16 Pages 3767—3775
DOI https://doi.org/10.2147/IDR.S410374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Naif M Alhawiti,1,2 Jamal M Alhawiti,3 Saif D Alshalan,3 Badi A Alotaibi,1,2 Ahmad Y Khobrani4
1Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), Riyadh, Kingdom of Saudi Arabia; 2King Abdullah International Medical Research Center (KAIMRC), Riyadh, Kingdom of Saudi Arabia; 3College of Medicine, Al Jouf University, Riyadh, Kingdom of Saudi Arabia; 4Emergency Department, King Abdullah Bin Abdulaziz University Hospital, Princess Norah University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Naif M Alhawiti, Associate Professor and Consultant of Hematology, Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Kingdom of Saudi Arabia, Tel +11-4299999 Ext. 95139, Email [email protected]; [email protected]
Abstract: The COVID-19 infection caused by SARS-CoV-2 is a healthcare crisis that has led to unparalleled disruption and has impacted healthcare services, leading to significant morbidity and mortality in the worldwide population. Insufficient data on the management of COVID-19 complications such as hypercoagulability and the controversy about the benefits of anticoagulant therapy are major challenges encountered by clinicians, especially for patients with pre-existing cardiovascular diseases (CVD), and are still debatable. Therefore, we endeavored to conduct a systematic review to assess the clinical outcomes of prior anticoagulant therapy in patients with COVID-19 having pre-existing CVD. Electronic searches of the PubMed database and EBSCO Information Services were carried out, and all relevant articles were employed. Seven articles with data from 21,989 subjects were included. Despite the promised clinical outcomes of anticoagulant therapy, the results of the current systematic review indicated insignificant improvements in the reduction of mortality rate or ICU admission among patients with COVID-19 having pre-existing CVD. Furthermore, direct oral anticoagulant (DOAC) were favored over vitamin K antagonists (VKAs) due to better action and less side effects. In conclusion, the findings are controversial as we did not statistically analyze the results. The data showed inconsistent information with no clear effect of anticoagulant use before patient hospitalization or decreasing COVID-19 severity, particularly in those with CVD. Further studies including randomized controlled trials are required to describe the best course as well as optimal dose of anticoagulant use in the treatment of patients with COVID-19, particularly those with comorbidities such as CVD.
Keywords: COVID-19, anticoagulant, comorbidities, thrombosis
Introduction
The emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causing the coronavirus disease (COVID-19) pandemic has significantly impacted 188 nations around the world with a terrifying increase of morbidity and mortality, causing a terrible burden for healthcare systems.1,2 Globally, COVID-19 has claimed the lives of more than 6 million patients, particularly those with pre-existing cardiovascular diseases (CVD).3 Recent studies have suggested that alterations in hemostatic systems are linked with further serious complications of the COVID-19 infection. COVID-19 infection can be further complicated by hypercoagulability, resulting in an elevated risk of thrombosis of up to 30% in patients with concomitant CVD. At worst, the disease can manifest as progression of venous thromboembolism (VTE) in those patients, reflecting the complexity of the COVID-19 infection.4–6 In line with this theory, VTE has been reported in 30–60% of severe COVID-19 cases, sometimes even in the presence of therapeutic anticoagulation.7,8 There may be a two-way link between COVID-19 and CVD. The endothelium and, probably, coagulation are directly altered by SARS-CoV-2 infection, both of which have been linked to CVD.9,10 Although the mechanisms are unclear, a few isolated case reports have linked COVID-19 to exposure of thrombogenic molecules or proinflammatory cytokines.11,12 Individuals with a history of vascular diseases may be at a meaningfully increased risk of thrombo-vascular complications after contracting COVID-19.13 Furthermore, untreated patients with COVID-19 may result in a cytokine storm in which the immune system overproduces pro-inflammatory substances such as tumor necrosis factor-α and interleukins, and there is an activation of coagulation patterns.4,5
In 2020, initial data from China revealed that individuals with COVID-19 diagnostically had pre-existing comorbidities such as hypertension, hyperlipidemia, and hyperglycemia were at high risk for cardiovascular disease.14 In a previous study from Wuhan encompassing 41 patients hospitalized due to the SARS-CoV-2 infection, the incidence of comorbidities was 32%, and the most prevalent underlying comorbidities were hyperglycemia (20%), hypertension (15%), and other known cardiovascular problems (15%). Two patients who died and those who were seriously unwell showed a greater prevalence of these pre-existing diseases. Published cohort data from a single-center study analyzed the information of 138 patients infected by coronavirus and hospitalized to Wuhan hospitals demonstrated that 31% had hypertension; 15%, other CVDs; and, 10%, diabetes. Of these patients, 46% had comorbidities, accounting for 72% of patients in the ICU.15,16 Reliable data showed that patients with COVID-19 may experience substantial, unwarranted activation of the coagulation system. For instance, circulating natural antithrombotic substances such as antithrombin III were suggestively lower in 94 patients with COVID-19 than those in 40 healthy individuals, although plasma D-dimer and fibrinogen levels were significantly high.17
Additionally, within the first 30 days, 449 patients with COVID-19 had a death rate that was twice that of 104 patients with non-COVID-19 pneumonia (29.8% versus 15.4%, respectively), and the earlier phase had a considerably higher platelet count than the latter, indicating that the earlier phase had more severe inflammatory response. Overall, COVID-19 may cause severe cardiovascular dysfunction, both linked to concomitant vascular disorders worsening through coronavirus infection and as medical indicators of illness manifestation. Furthermore, COVID-19 may be involved in the initiation and activation of the endothelial cell and coagulation cascade, particularly in the presence of predisposing factors, which mostly manifests as thromboembolic events damaging body organs such as lungs.18,19 Thus, according to some scientific data, healthcare clinicians had taken the responsibility to utilize therapeutic antithrombotic agents including aspirin, low-molecular-weight heparin (LMWH), or heparin for reducing the severity of COVID-19 by minimizing thrombotic formation.20,21 Patients with COVID-19 may have a better prognosis while taking LMWH for preventing thrombus formation.22,23 Furthermore, patients infected by SARS-CoV-2, particularly older people or those with comorbidities, should be given an anticoagulant at therapeutic dose to prevent microthrombus formation, according to the American Society of Hematology.22
Study Rationale
Many cases have reported that arterial or venous thrombosis were frequently concurrent with COVID-19. Thus, anticoagulants, antiplatelet, or antithrombotic agents have been primarily ordered for patient treatment. However, information on the prognosis of patients with concomitant CVD regularly using anticoagulants before being presented to the clinics complaining of COVID-19 symptoms is still debatable, and more evidence are primarily required to investigate the valuable outcomes of the use of anticoagulants in these patients.
However, the available data on the impact of prior usage of antithrombotic agents such as aspirin or LMWH in patients with COVID-19 having pre-existing vascular diseases can be used to recognize and maintain the scientific data for evidence to express consistent clinical and practical research knowledge that was generated on preceding information. This systematic review was proposed to summarize existing knowledge to deliver additional insights regarding the prior usage of anticoagulants in patients with COVID-19 with pre-existing CVD and describe where potential clinical research may add to what is identified.
Methods
Study Participants
The systematic review included all studies that reported on anticoagulant use and COVID-19 comprising all patients including children, adults, families, and health workers that we came across in the studies on prior utilization of anticoagulants among patients diagnosed with COVID-19 with a history of CVD. This study was approved by Institutional Review Board in the King Abdullah International Medical Research Centre under the reference (#NRC22R/483/10).
Search Strategy
A systematic search was implemented using a sequence of Medical Study Headings and maintained vocabulary to classify peer-reviewed papers on prior usage of anticoagulants in patients with COVID-19 with concomitant medication use. Clinical study articles published between October 2019 and August 2022 were searched in the following databases: PubMed/MEDLINE, Scopus/Embase (Elsevier), EbscoHost, and Google Scholar.
Study Eligibility Criteria
This systematic review comprised peer-reviewed studies. Collected data from qualitative and quantitative methods were assessed for inclusion or exclusion criteria, if the qualitative elements were relevant. We included all studies that were published between October 2019 and August 2022 and met the inclusion criteria. Articles that were relevant to the objectives of the study were chosen. The reviewers excluded any studies that were not written in English, or were textbooks, grey literature, and editorial letters. However, English language articles without geographical restriction that reported the incidence and clinical management or adverse events of patients with COVID-19 with concomitant CVD with prior usage of anticoagulants were included. We excluded published papers that did not have the keywords separately or in combination with anticoagulant, coagulation, COVID-19, SARS-CoV-2, coronavirus, cardiovascular disease, and thrombosis.
Selection of Study
The enhancing transparency in reporting the synthesis of qualitative reviews (ENTREQ) guideline was used to determine the choice procedures and findings. All retrieved studies were initially imported into Endnote library to remove duplicates. After deleting the duplicates, the Endnote library was shared between the two reviewers for independent screening. The articles that both reviewers agreed on were subjected to full-text review. A third reviewer adjudicated any discrepancies between the two reviewers. The two reviewers independently reviewed the full texts of all eligible studies. When there were discrepancies between the two reviewers, consensus was sought through discussion on the difference with the third reviewer. Finally, the full texts of all relevant studies that met the inclusion criteria were retained for the final framework synthesis.
Data Extraction
Data was independently extracted by two reviewers from eligible studies onto a customized data extraction form and populated with variables pertaining to the study population and phenomena of interest. The third reviewer double checked and verified the extracted articles. Study characteristics included name of the first author and year of publication; data collection period and region in which the study was conducted; and, specific study details including study design, study population, sample size, sampling procedures, and clinical outcomes. Prevalence and risk factors of prior usage of anticoagulants in the population of patients with COVID-19 with pre-existing CVD were systematically identified.
Data Synthesis and Analysis
No software was used to analyze the data (Table 1). The reviewers sorted the data by theme and described the themes in the form of an analysis table (chart). The columns and rows of the table reflect the studies and related themes and enabled us to compare findings of the studies across different themes and subthemes.
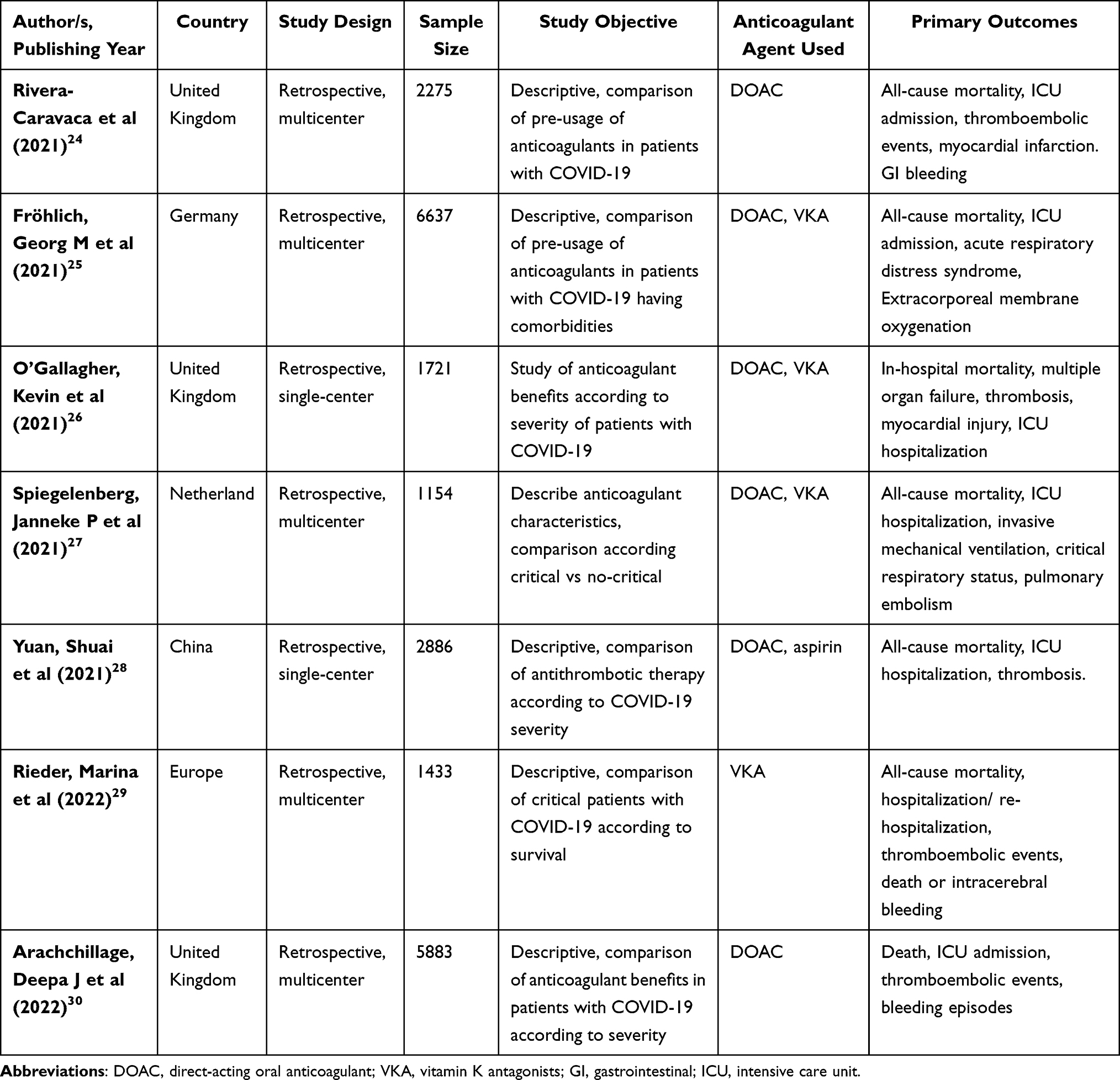 |
Table 1 Characteristics and Clinical Outcomes of Included Studies |
Mapping and Interpretation
The reviewers used charts to define the identified concepts, map the range and nature of the phenomena. We explored the associations between the themes to clarify the findings. The current review mapped and interpreted the results in line with the study objectives and emerging themes.
Results
We retrieved a total of 105 potentially eligible studies through electronic search databases. The manual search did not show any further relevant studies. Based on the exclusion criteria, duplicate studies were excluded, and the full texts of the remaining 63 publications were thoroughly reviewed. Then, the full-text published papers of the remaining 31 studies were systematically assessed for eligibility, and 24 articles were removed from the final review as they were considered irrelevant to the research question, or were review articles, clinical guides or case reports. Of the remaining articles, seven clinical studies were included in this systematic review. Study selection has been summarized in Figure 1.
 |
Figure 1 Literature search flowchart. |
Rivera-Caravaca et al stated that using DOAC and VKA gave similar results regarding several parameters, especially regarding patient prognosis. The main difference was the possibility of having arterial or venous thrombosis, which was much higher in cases using VKA.24 Similar data was reported by Fröhlich et al who carried out clinical studies in Germany hospitals, examining the impact of anticoagulants in the admitted patients with COVID-19 complications having a history of vascular diseases, where the usage of therapeutic anticoagulants displayed insignificant outcomes in the reduction of death rate and prognosis of the condition, whereas antiplatelet therapy had no efficacy.25
Moreover, O’Gallagher et al reported that, patients hospitalized with COVID-19, patients under the age of 70 having concomitant vascular complications seemed to have a greater potential contribution to in-hospital mortality than those without co-existing vascular diseases. This reinforced the risk of occurrence of vascular complications in individuals with co-existing CVD lately infected by SARS-CoV-2. However, an indication of therapeutic anticoagulation for reducing the risk of thromboembolism events showed promising outcomes.26
In contrast, Spiegelenberg et al reported that, while previously administered therapeutic anticoagulation obviously contributed to the decrease of vascular thrombosis or pulmonary embolism development, favorable clinical outcomes were not obtained in hospitalized patients with COVID‐19 with respect to all‐cause mortality or intensive care unit (ICU) hospitalization. In addition, cited data did not show clear significant clinical findings in patients with COVID-19 treated with VKA or DOAC.27
Furthermore, Yuan et al concluded that the usage of low-dose aspirin as an anticoagulant for patients with COVID-19 did not show any significant improvement; further analysis revealed that old age, inflammatory diseases, and organ dysfunction were the main risk factors. Aspirin use was not correlated with a reduction in mortality risk in patients with COVID-19 having vascular complications.28
Similarly, Rieder et al reported that a pre-existing anticoagulant regimen is protective in COVID-19 and has a key role in significant reduction in all-cause and COVID-19-linked mortality, thrombotic incidences, and an improved retrieval level in individuals with co-existing anticoagulation regimes compared to patients without pre-existing therapeutic anticoagulation.29 In contrast, Arachchillage et al found that the development of thrombosis is associated with the augmented rate of mortality in hospitalized patients with SARS-CoV-2 infection regardless of therapeutic anticoagulant regimen prior to hospitalization. However, the regulation of optimal therapeutic-dose anticoagulation is a key challenge to have full benefit from therapeutic anticoagulants to prevent thrombotic progression or reduce the incidence of hemorrhagic events.30
Discussion
Older people and those with concomitant CVD have much more fatal COVID-19 disease than the general population.30 Only 136 of the 3335 Italian patients who died in the hospitals and whose clinic records could be examined had no pre-existing diseases, whereas 493 stated having one, two, or at least three chronic diseases. Vascular diseases included diabetes mellitus, and hypertension were the most frequently reported comorbidities, followed by ischemic heart disease and organ dysfunction.31
Thromboembolic events may be occurred because of hypercoagulability associated with COVID-19 infection. Patients with COVID-19 frequently experience higher D-dimer plasma levels, mildly reduced platelet production, and slightly extended prothrombin times. In 2020, published data reported that 46% of all patients with COVID-19 from China had D-dimer levels >0.5 mg/l. Similarly, research in patients with COVID-19 in Wuhan showed that 42% of all patients who died had raised D-dimer levels (>1 mg/l), which was linked to an 18-fold higher probability of death.29–31 Additionally, these patients had high fibrinogen and factor VIII levels, which determined a hypercoagulable condition. These results demonstrated that a significant proportion of patients with COVID-19 have coagulation problems that may facilitate the emergence of the thromboembolic events.32
According to an autopsy-based research, pulmonary embolism was found in 4 of 12 patients with COVID-19, whereas venous thrombosis was found in 7 of 12 patients.33 These anomalies in the coagulation system, particularly the state of hypercoagulability in the context of COVID-19, are accompanied by unknown molecular processes. One theory is that patients may be predisposed to a hypercoagulable state because of the severe inflammatory process and endothelial dysfunction caused by COVID-19 when combined with underlying co-existing comorbidities. Antiviral drugs and experimental treatments provided to these individuals may increase the risk of thrombosis or hemorrhagic events through pharmacological associations with therapeutic anticoagulants.6,34
The prognosis of COVID-19 may be improved by therapeutic anticoagulant administration before infection by impeding coagulation activation. In fact, compared to thromboprophylaxis alone, the administration of therapeutic anticoagulation at hospital admission resulted in the decreased incidence of VTE.35 A reduced extrahepatic vitamin K status was found in patients with COVID-19, and Dofferhof et al revealed that this condition was associated with a bad prognosis due to the low vitamin K status.36
Moreover, the association of systemic anticoagulation with extended survival of hospitalized patients with COVID-19 demonstrated no statistical significance according to a previous study conducted in New York, where 786 of the 2773 patients were administered therapeutic anticoagulants. In addition, while the overall proportion of mortality between the two cohorts was comparable (22.5% against 22.8%), the median duration of survival of patients who received anticoagulation was better than those of individuals with concomitant CVD who did not receive prior anticoagulant therapy.37 Another study conducted in China found that LMWH treatment decreased the death rate in individuals with COVID-19-associated coagulopathy. However, the direct-acting anticoagulation agents such as VKA and unfractionated heparin have not clearly showed a protective effect on thrombotic events or diminishing severity of COVID-19.38
Moreover, long-term oral anticoagulation treatment using VKA or DOACs was independently linked to better outcomes. The procoagulatory state brought on by COVID-19 raises the likelihood of thromboembolic events and may be crucial in the development of serious complications, particularly among people with pre-existing CVD. Atrial fibrillation was the primary reason for long-term therapeutic anticoagulations in the German sample. Nevertheless, independent of VKA or DOAC therapy, patients with atrial fibrillation have a higher chance of unfavorable outcomes.22
Recent studies among patients with chronic illnesses related to vascular disorders have shown that the use of DOAC significantly lowers the risk of stroke without increasing bleeding. Patients with COVID-19 having vascular disorders using DOACs are linked to a reduced risk of thrombosis than those using other anticoagulants such as VKA.39 Patients priorly on VKA had a higher risk of problems within 30 days of getting a COVID-19 diagnosis; hence, whenever practical, switching to a DOAC should be considered.40,41 The optimal course/dose of DOAC therefore must be precisely determined according to the risk of thromboembolism to effectively contribute towards prevention and treatment in those patients.
Furthermore, due to its antiplatelet qualities, low-dose aspirin is frequently used to prevent myocardial infarction and stroke in high-risk individuals. As a result, it may lessen the frequency of coagulopathy caused by COVID-19 and prevent serious worsening of cardiovascular problems. Published study showed that the aspirin and non-aspirin groups did not differ in terms of myocardial infarction.28 Another observational trial involving 412 patients with COVID-19 found that aspirin had minimal association with improved clinical outcomes in hospitalized patients with COVID-19 with respect to the frequency of overt thrombosis.42 The findings were explained as extended prothrombin time, and an increased D-Dimer level are the primary signs of coagulation failure in patients with COVID-19. All the articles included in this study were retrospective studies. Published results on period, type of the optimal dose of anticoagulant, and other clinical findings were still incomplete in most combined clinical studies; thus, we were incapable of further analysis.
Conclusion
As COVID-19 is a current worldwide concern with greater mortality particularly in those with cardiovascular diseases, and our paper addresses the outcomes of prior anticoagulant therapy in patients with COVID-19 with pre-existing cardiovascular diseases. We believe that patients with COVID-19 are susceptible to comorbidities, mainly hypercoagulability, and a pro-inflammatory state. Management of these patients requires a complete understanding of the pathogenesis of these comorbidities. Data showed that the usage of anticoagulants may be linked to an improvement in the case of patients with COVID-19. However, if anticoagulants are to be used, DOACs are favored due to their better action and lesser side effects compared with other anticoagulant agents such as VKAs. Despite the promised clinical outcomes of anticoagulant therapy, we could state that the results of the current systematic review indicated insignificant improvements in the reduction of mortality rate or ICU admission. Furthermore, there was no clear effect of anticoagulant use before patient hospitalization or decreasing COVID-19 severity. Further research is required to describe the best course and optimal dose of anticoagulant use in the treatment of patients with COVID-19 with comorbidities such as CVD.
Acknowledgments
The authors would like to acknowledge Hussain S. Aldera, professor of Clinical Physiology, College of Medicine, KSAU-HS for his support and advice in completing this work.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Klok FA, Kruip MJ, Van der Meer NJ, et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: an updated analysis. Thromb Res. 2020;191:148–150. doi:10.1016/j.thromres.2020.04.041
2. Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565–574.
3. Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. cell. 2020;181(2):271–280.
4. Nopp S, Moik F, Jilma B, Pabinger I, Ay C. Risk of venous thromboembolism in patients with COVID‐19: a systematic review and meta‐analysis. Res Practice Thrombosis Haemostasis. 2020;14(7):12439–12452.
5. Tay MZ, Poh CM, Rénia L, MacAry PA, Ng LF. The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol. 2020;20(6):363–374.
6. Bikdeli B, Madhavan MV, Jimenez D, et al. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(23):2950–2973.
7. Wichmann D, Sperhake JP, Lütgehetmann M, et al. Autopsy findings and venous thromboembolism in patients with COVID-19: a prospective cohort study. Ann Intern Med. 2020;173(4):268–277.
8. Llitjos JF, Leclerc M, Chochois C, et al. High incidence of venous thromboembolic events in anticoagulated severe COVID‐19 patients. J Thrombosis Haemostasis. 2020;18(7):1743–1746.
9. Schulman S. Coronavirus disease 2019, prothrombotic factors, and venous thromboembolism. Semin Thromb Hemost. 2020;46(7):772–776.
10. Ghosh R, Roy D, Mandal A, et al. Cerebral venous thrombosis in COVID-19. Diabetes Metab Syndr. 2022;15(3):1039–1045.
11. Hu H. Coronavirus fulminant myocarditis saved with glucocorticoid and human immunoglobulin. Eur Heart J. 2021;42(1):206–213.
12. Hua A, O’Gallagher K, Sado D, Byrne J. Life-threatening cardiac tamponade complicating myo-pericarditis in COVID-19. Eur Heart J. 2020;41(22):2130–2137.
13. Sánchez-Recalde Á, Solano-López J, Miguelena-Hycka J, Martín-Pinacho JJ, Sanmartín M, Zamorano JL. COVID-19 and cardiogenic shock. Different cardiovascular presentations with high mortality. Rev Esp Cardiol. 2020;73(8):669–672.
14. Guo T, Fan Y, Chen M, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(7):811–818.
15. Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential effects of coronaviruses on the cardiovascular system: a review. JAMA Cardiol. 2020;5(7):831–840.
16. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. lancet. 2020;395(10223):497–506.
17. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069.
18. Han H, Yang L, Liu R, et al. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin Chem Lab Med. 2020;58(7):1116–1120.
19. Fried JA, Ramasubbu K, Bhatt R, et al. The variety of cardiovascular presentations of COVID-19. Circulation. 2020;141(23):1930–1936.
20. Young E. The anti-inflammatory effects of heparin and related compounds. Thromb Res. 2008;122(6):743–752.
21. Lin L, Lu L, Cao W, Li T. Hypothesis for potential pathogenesis of SARS-CoV-2 infection–a review of immune changes in patients with viral pneumonia. Em Microbes Infections. 2020;9(1):727–732.
22. Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thrombosis Haemostasis. 2020;18(5):1094–1099.
23. Cuker A, Tseng EK, Nieuwlaat R, et al. American Society of Hematology living guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19. Blood Adv. 2021;5(20):3951–3959.
24. Rivera-Caravaca JM, Harrison SL, Buckley BJ, et al. Efficacy and safety of direct-acting oral anticoagulants compared to vitamin K antagonists in COVID-19 outpatients with cardiometabolic diseases. Cardiovasc Diabetol. 2021;20(1):1.
25. Fröhlich GM, Jeschke E, Eichler U, et al. Impact of oral anticoagulation on clinical outcomes of COVID-19: a nationwide cohort study of hospitalized patients in Germany. Clin Res Cardiol. 2021;110(2):1041–1050.
26. O’Gallagher K, Shek A, Bean DM, et al. Pre-existing cardiovascular disease rather than cardiovascular risk factors drives mortality in COVID-19. BMC Cardiovasc Disord. 2021;21(1):1–3.
27. Spiegelenberg JP, van Gelder MM, Maas ML, et al. Prior use of therapeutic anticoagulation does not protect against COVID‐19 related clinical outcomes in hospitalized patients: a propensity score‐matched cohort study. Br J Clin Pharmacol. 2021;87(12):4839–4847.
28. Yuan S, Chen P, Li H, Chen C, Wang F, Wang DW. Mortality and pre‐hospitalization use of low‐dose aspirin in COVID‐19 patients with coronary artery disease. J Cell Mol Med. 2021;25(2):1263–1273.
29. Rieder M, Gauchel N, Kaier K, et al. Pre-medication with oral anticoagulants is associated with better outcomes in a large multinational COVID-19 cohort with cardiovascular comorbidities. Clin Res Cardiol. 2022;111(3):322–332.
30. Arachchillage DJ, Rajakaruna I, Odho Z, et al. Clinical outcomes and the impact of prior oral anticoagulant use in patients with coronavirus disease 2019 admitted to hospitals in the UK—a multicentre observational study. Br J Haematol. 2022;196(1):79–94.
31. Palmieri L, Vanacore N, Donfrancesco C, et al. Clinical characteristics of hospitalized individuals dying with COVID-19 by age group in Italy. J Gerontol. 2020;75(9):1796–1800.
32. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Eng j Med. 2020;382(18):1708–1720.
33. De Rosa S, Spaccarotella C, Basso C, et al. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era. Eur Heart J. 2020;41(22):2083–2088.
34. Razi M, Gu J, He X, Kong J, Ahmed MJ. Venous thromboembolism in patients with COVID-19. A prevalent and a preventable complication of the pandemic. J Interventional Med. 2021;4(2):62–65.
35. Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;323(18):1824–1836.
36. Dofferhoff AS, Piscaer I, Schurgers LJ, et al. Reduced vitamin K status as a potentially modifiable risk factor of severe coronavirus disease 2019. Clin Infectious Dis. 2021;73(11):4039–4046.
37. Paranjpe I, Fuster V, Lala A, et al. Association of treatment dose anticoagulation with in-hospital survival among hospitalized patients with COVID-19. J Am Coll Cardiol. 2020;76(1):122–124.
38. Levi M, Thachil J, Iba T, Levy JH. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020;7(6):e438–40.
39. Ueyama H, Kuno T, Ando T, et al. Meta-analysis comparing direct oral anticoagulants versus vitamin K antagonists after transcatheter aortic valve implantation. Am J Cardiol. 2020;125(7):1102–1107.
40. Michael F, Natt N, Shurrab M. Direct oral anticoagulants vs vitamin K antagonists in left ventricular thrombi: a systematic review and meta-analysis. CJC Open. 2021;3(9):1169–1181.
41. Testa S, Prandoni P, Paoletti O, et al. Direct oral anticoagulant plasma levels’ striking increase in severe COVID‐19 respiratory syndrome patients treated with antiviral agents: the Cremona experience. J Thrombosis Haemostasis. 2020;18(6):1320–1323.
42. Chow JH, Khanna AK, Kethireddy S, et al. Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019. Anesth Analg. 2021;132(4):930–941.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.