")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Manifestations and Risk Factors of Tigecycline-Associated Thrombocytopenia
Received 16 June 2023
Accepted for publication 31 August 2023
Published 15 September 2023 Volume 2023:16 Pages 6225—6235
DOI https://doi.org/10.2147/IDR.S426259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yuanchao Zhu, Fei Zhao, Pengfei Jin
Department of Pharmacy, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing Key Laboratory of Assessment of Clinical Drugs Risk and Individual Application (Beijing Hospital), Beijing, 100730, People’s Republic of China
Correspondence: Pengfei Jin, Tel +86-01085133620, Email [email protected]
Background: Thrombocytopenia, characterized by a diminished platelet count, emerged as the most frequently reported coagulation dysfunction event according to the FDA Adverse Event Reporting System (FAERS) database. In recent years, numerous clinical studies have investigated the potential link between tigecycline usage and the occurrence of hypofibrinogenemia. However, a research gap remains in comprehensively examining the association between tigecycline and thrombocytopenia in real-world settings.
Methods: This study was conducted to explore the incidence and clinical manifestations of tigecycline-associated thrombocytopenia. A retrospective case-control study of patients treated with tigecycline was conducted between January 2018 and June 2022.
Results: In total, 373 patients were included in this study. Among these patients, 12.3% experienced thrombocytopenia. The onset of thrombocytopenia occurred within a range of 2 to 22 days after the initiation of tigecycline, with a median period (25– 75th percentile) of 9 (6– 11) days. Among the patients manifesting thrombocytopenia, 60.9% exhibited mild-to-moderate cases (grades 1– 2) while 39.1% endured severe cases (grades 3– 4). Multivariate analysis delineated several factors as independent risk factors for thrombocytopenia. Notably, advanced age (≥ 74 years) (p=0.028), risk of malnutrition (p< 0.001), tigecycline therapy for ≥ 7 days (p=0.003), DBIL> 8.1μmol/L (p< 0.001)), BUN> 8.1mmol/L (p=0.002) emerged as independent risk factors associated with thrombocytopenia. When comparing the control group to the thrombocytopenia group, 70.7% of patients in the control group exhibited 0– 2 risk factors, while all patients in the thrombocytopenia group demonstrated risk factors. Specifically, 95.7% of patients in the thrombocytopenia group presented with three to five risk factors, with only 4.4% having 0– 2 risk factors.
Conclusion: Tigecycline administration is associated with thrombocytopenia. Healthcare professionals should exercise vigilance, particularly in cases of severe tigecycline-associated thrombocytopenia, and undertake routine monitoring of patients’ platelet counts, especially for those who possess three or more risk factors.
Keywords: tigecycline, thrombocytopenia, risk factor, pharmacovigilance, coagulation disorder
Introduction
Tigecycline, a novel glycylcycline antibacterial agent, has shown remarkable efficacy against a wide spectrum of bacterial pathogens.1 Its potent activity extends across Gram-positive, Gram-negative and anaerobic bacteria, including methicillin-resistant Staphylococcus aureus, methicillin-resistant Staphylococcus epidermidis, vancomycin-resistant enterococci, KPC-producing Klebsiella pneumonia, extended-spectrum β-lactamase (ESBL)-producing Enterobacteriaceae, and other multidrug-resistant (MDR) Gram-negative bacteria.2,3
The escalating prevalence of drug-resistant bacterial infections as a serious concern aggravated by the scarcity of efficacious antibacterial agents. Since its approval by the US FDA in 2005, tigecycline has gained recognition as an exceptionally potent antimicrobials agent. In China, tigecycline has received approval for the treatment of community-acquired pneumonia (CAP), complicated intra-abdominal infections (cIAIs) and complicated skin and skin structure infections (cSSSIs). Additionally, tigecycline exhibits the advantage of obviating the necessity for dose adjustment in patients with renal impairment and has minimal proclivity for drug interactions, thereby underscoring its viability as a reasonable option for managing severe bacterial infections.3
Clinical trials have provided evidence acknowledging the general tolerability of tigecycline. Within these trials, which enrolled 1415 patients, the prevailing adverse events included nausea (29.5%), vomiting (19.7%), diarrhea (12.7%), infection (8.3%), thrombocytopenia (6.1%), ALT increase (5.6%), AST increase (4.3%), rash (2.4%) and bilirubinemia (2.3%).4 While occurrences of tigecycline-induced thrombocytopenia have been sporadically documented, they have frequently been overlooked by physicians. The first documented case of tigecycline-induced thrombocytopenia was in 2017.5 However, recent pharmacovigilance data have raised apprehension regarding this adverse event.6 According to data from the FDA Adverse Event Reporting System, thrombocytopenia, hypofibrinogenemia, increased international normalized ratio (INR), prolonged activated partial thromboplastin time (APTT), and prolonged prothrombin time emerged as the most common coagulation disorder associated with tigecycline. Although several clinical studies have focused on tigecycline-associated hypofibrinogenemia and coagulopathy, this present study represents the inaugural endeavor to specifically investigate tigecycline-associated thrombocytopenia in real-world patients undergoing tigecycline therapy, and to identify any clinical factors that may increase the susceptibility to this particular adverse event.
Materials and Methods
Study Population
This retrospective, single-center, observational study was conducted at Beijing Hospital between January 2018 and June 2022. The study included patients of 18 years or above who had undergone tigecycline treatment for a minimum duration of 72 hours. Patient data were retrieved from the Pharmacy Department Database. Patients with incomplete laboratory test results or medical records, a confirmed diagnosis of hematological diseases, pre-treatment PLT count below 100×109/L, absence of baseline information or follow-up PLT count data, or concomitant administration of linezolid were excluded from the study. This study was approved by the Beijing Hospital Ethics Committee.
For a comprehensive schematic of the patient screening process, refer to Figure 1.
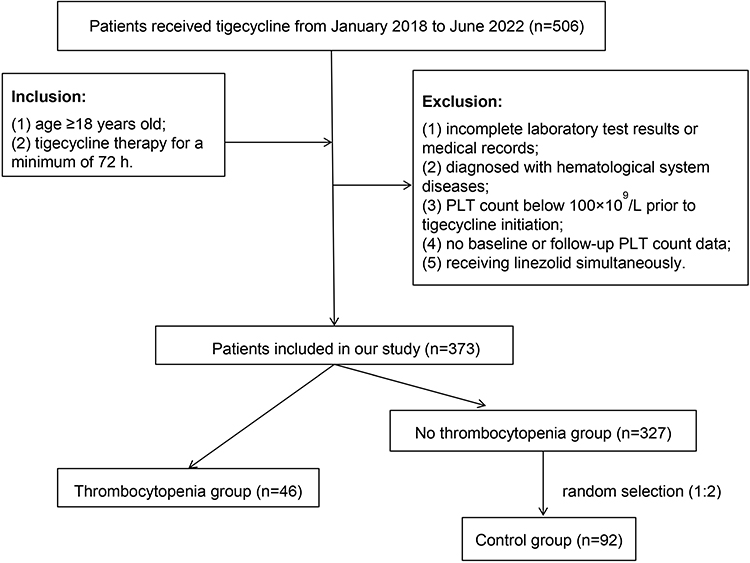 |
Figure 1 The schematic of the patient selection process. |
Data Collection
Patient’s information was extracted from their medical records, encompassing the following data: (1) demographic information (eg, age, gender, weight, diet, and comorbidities), (2) primary underlying disease, (3) the dose, frequency and duration of tigecycline treatment, (4) the occurrence time, symptoms, signs and grading of adverse reaction related to thrombocytopenia, and (5) clinical laboratory test results, including liver function indicators [aspartate transaminase (AST), alanine transaminase (AST), direct bilirubin (DBIL), total bilirubin (TBIL)], renal function indicators [serum creatinine (SCR), blood urea nitrogen (BUN)], coagulation function indicators [fibrinogen concentration, international normalized ratio (INR)], platelet (PLT) count, blood albumin (ALB), white blood cell (WBC) count, C reactive protein (CRP), and procalcitonin (PCT).
Adverse Events Definitions and Severity Grading
Thrombocytopenia was precisely delineated in accordance with the criteria laid out in the Common Adverse Event Evaluation Criteria (CTCAE) version 5.0.7 Thrombocytopenia was characterized by a PLT count <100×109/L. The severity of thrombocytopenia was stratified into four grades: Grade 1 (PLT count of 75–10×109/L), Grade 2 (PLT count of 50–75×109/L), Grade 3 (PLT count of 25–50×109/L), and Grade 4 (PLT count below 25×109/L).
The primary outcome of the study was to determine the incidence and severity of thrombocytopenia after tigecycline treatment. As a secondary outcome, the study also aimed to evaluate the incidence of coagulation disorders, specifically hypofibrinogenemia and INR elevation. Additionally, the study examined the concomitant medications that might potentially correlate with the incidence of thrombocytopenia.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics 17.0. Continuous variables were presented as mean ± standard deviation (SD) in cases of normal distribution, or as median and interquartile range for variables exhibiting non-normal distribution. Categorical variables were reported in terms of percentages. The comparison of laboratory indicators before and after tigecycline treatment was carried our using a paired t-test. To access disparities between the control and non-thrombocytopenia groups, either the t-test or Chi-square test was employed as appropriate. To identify risks factors associated with thrombocytopenia, binary logistic regression analysis was performed. For variables that exhibited significance in univariate analyses, stepwise multiple logistic analysis was conducted to identify independent risk factors. Statistical significance was established at P < 0.05.
Ethics
This study, which was in compliance with the Declaration of Helsinki, received ethical approval from the Ethics Committee of Beijing Hospital (Permit Number: 2022BJYYEC-312-02). As neither individual data were published nor any intervention was performed on patients, patient consent was waived by the Ethics Committee of Beijing Hospital.
Results
Clinical Features of Patients with Thrombocytopenia
Figure 1 illustrates the schematic representation of the patient selection process. A cohort of 506 patients who received tigecycline underwent preliminary screening for potential inclusion in the study. Following this screening, 373 patients fulfilled the inclusion criteria for participation and were included in the study. The average age of the enrolled patients was (75.4 ± 14.7) years. Among these patients, 46 individuals experienced thrombocytopenia and were subsequently categorized into the thrombocytopenia group. The remaining 321 patients were classified into the no-thrombocytopenia group. Within the no-thrombocytopenia group, a subset of 96 patients were randomly selected and designated as the control group. There were no significant differences in demographic characteristics between the two groups. The above findings are elaborated upon in Table 1.
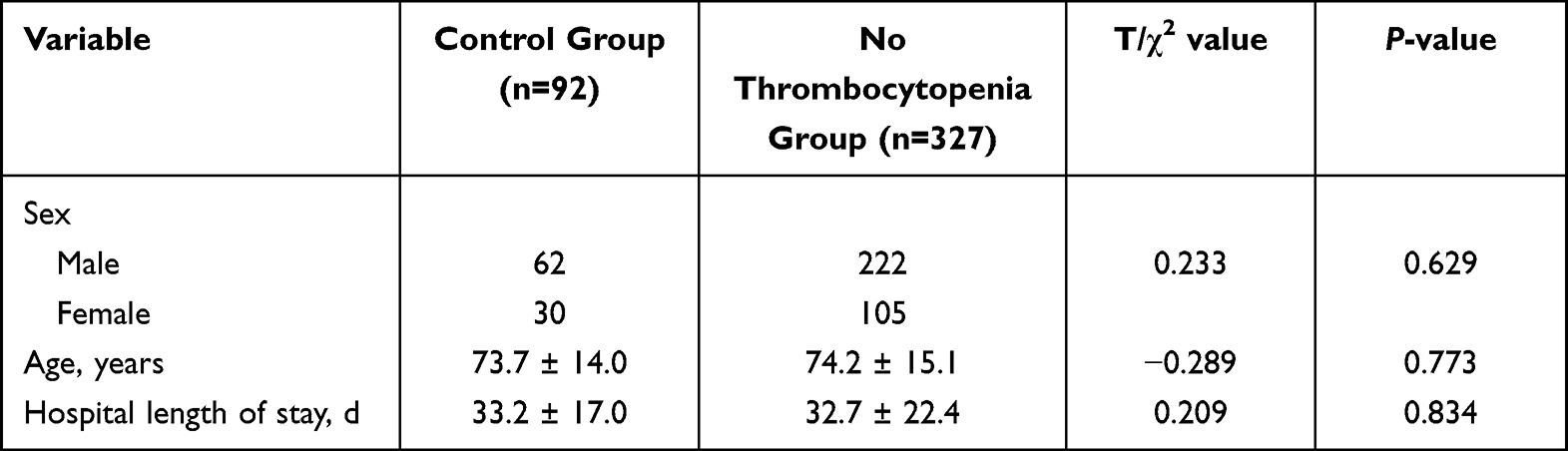 |
Table 1 Demographic of Control Group and No Thrombocytopenia Group |
Thrombocytopenia manifested within the thrombocytopenia group over a span of 2 to 22 days after the initiation of tigecycline treatment, with a median onset occurring at 9 days (25–75th percentile) (Figure 2). A total of 9 patients discontinued tigecycline treatment due to thrombocytopenia. Furthermore, within the patient cohort, 25 patients exhibited a return of platelet count levels to normal prior to their discharge from the hospital (Figure 3). The classification of thrombocytopenia severity is shown in Table 2. The incidence of tigecycline-associated thrombocytopenia was 12.3% (46/373). The severity of thrombocytopenia varied among the patients, with 60.9% (28/46) experiencing mild-to-moderate thrombocytopenia, while 39.1% (18/46) experienced severe thrombocytopenia. Eight patients died within 30 days after receiving tigecycline treatment.
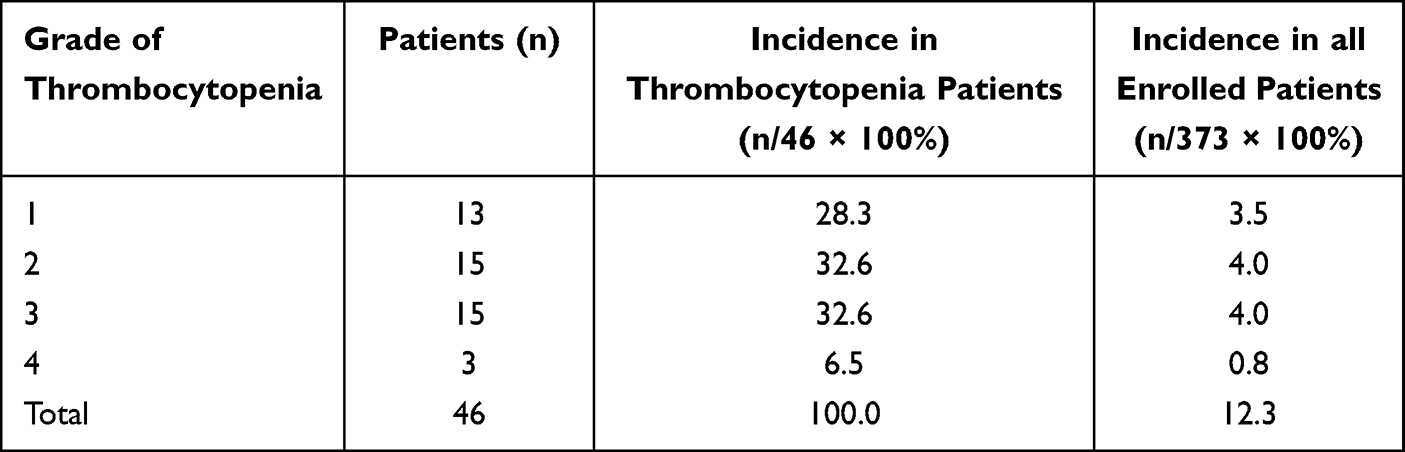 |
Table 2 Grade and Incidence of Tigecycline-Associated Thrombocytopenia |
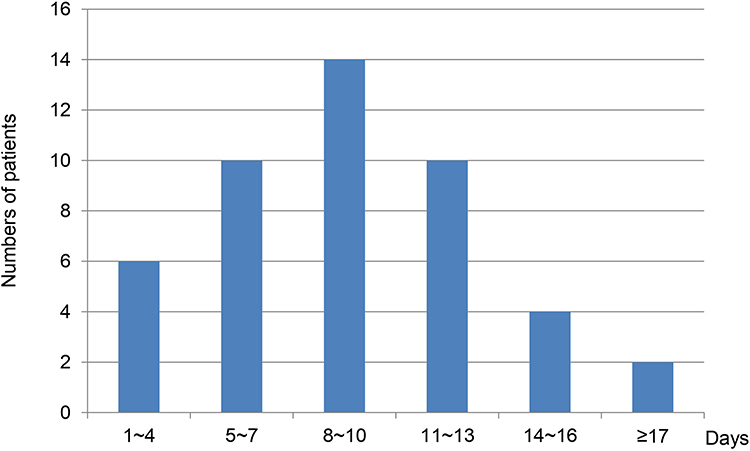 |
Figure 2 Days from tigecycline initiation to thrombocytopenia. |
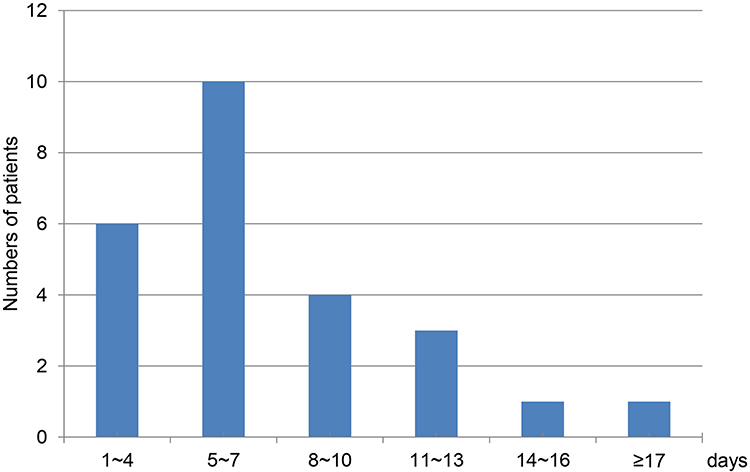 |
Figure 3 Days until the platelet count levels return to normal after the discontinuation of tigecycline. |
The analysis extended to coagulation indicators within both the thrombocytopenia and control groups (Table 3). When compared to the control group, patients in the thrombocytopenia group displayed an increased likelihood of elevated INR (82.6% (38/46) vs 37.0% (34/92), χ2=24.444, p<0.001) and hypofibrinogenemia (69.6% (32/46) vs 33.7% (31/92), χ2=15.903, p<0.001).
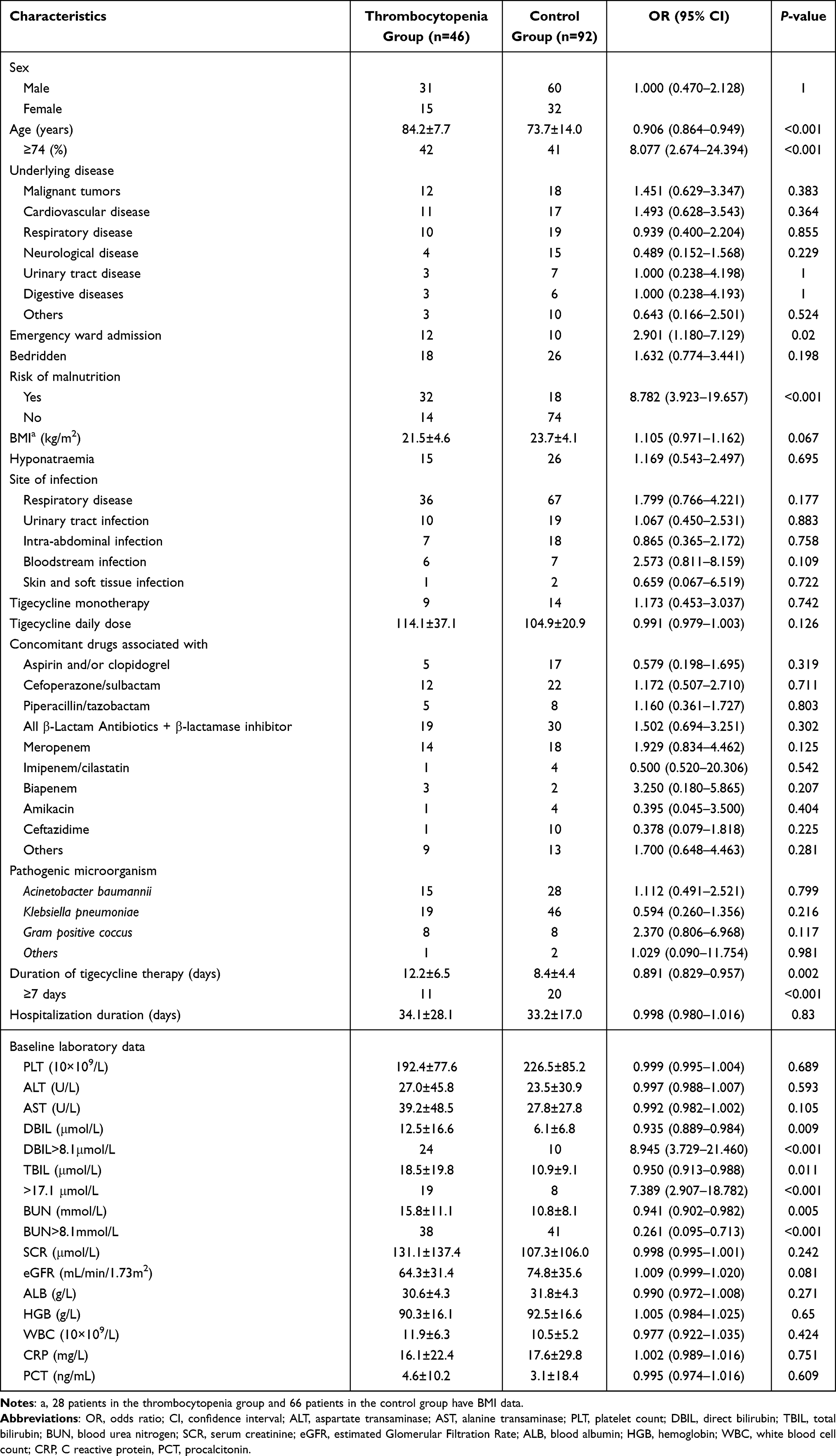 |
Table 3 Univariate Analysis of Risk Factors for Tigecycline-Associated Thrombocytopenia |
Risk Factors for Thrombocytopenia Group
The baseline characteristics and clinical features of both the thrombocytopenia and control groups are displayed in Table 3.
In the univariate analysis, several factors exhibited statistically significant associations with thrombocytopenia, including advanced age (≥74 years), emergency ward admission, risk of malnutrition, tigecycline therapy for ≥7 days, DBIL >8.1μmol/L, TBIL >17.1μmol/L and BUN >8.1mmol/L (P<0.05).
Conversely, no significant differences were detected between the thrombocytopenia group and the control group in terms of other indicators, such as AST, AST, SCR, PLT count, ALB, WBC count, CRP and PCT.
No substantial association was identified between tigecycline-induced thrombocytopenia and concomitant medications acknowledged for their potential association with the risk of thrombocytopenia, including aspirin, clopidogrel, cefoperazone/sulbactam, piperacillin/tazobactam, imipenem/cilastatin, meropenem, amikacin, or ceftazidime.
Considering the intrinsic relationship between DBIL and TBIL, DBIL was chosen as an independent variable in the multivariate logistic regression analysis with other risk factors. According to multivariate analysis, advanced age (≥74 years), risk of malnutrition, tigecycline therapy for ≥7 days, DBIL>8.1μmol/L, BUN>8.1mmol/L emerged as independent risk factors associated with thrombocytopenia (Table 4).
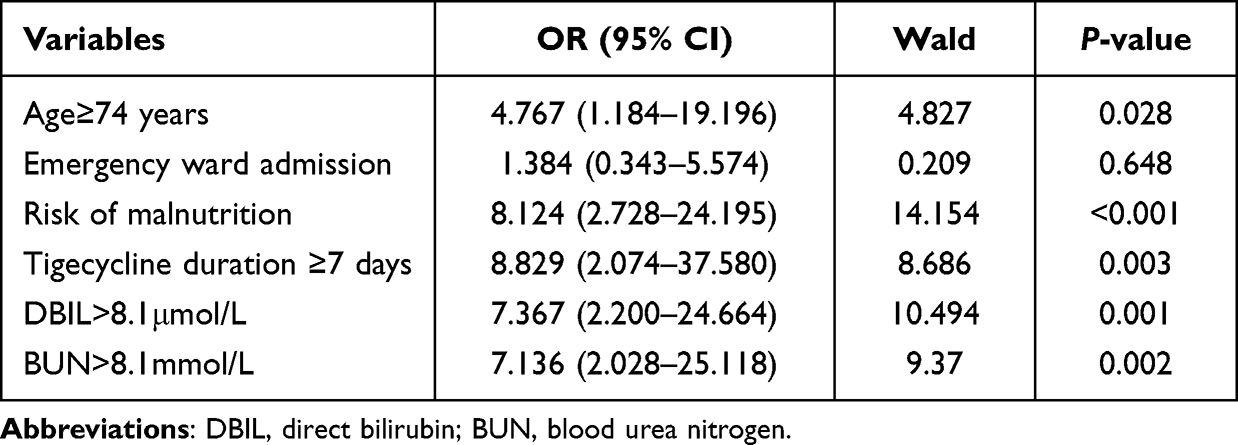 |
Table 4 Multivariate Analysis of Risk Factors for Tigecycline-Associated Thrombocytopenia |
Furthermore, an assessment of the quantity of coexisting risk factors among patients was conducted (Table 5). In the control group, 70.7% (65/92) of the patients exhibited a range of 0 to 2 risk factors. In contrast, all patients in the thrombocytopenia group presented with accompanying risk factors, with a notable 95.7% (44/46) of them manifesting three to five risk factors.
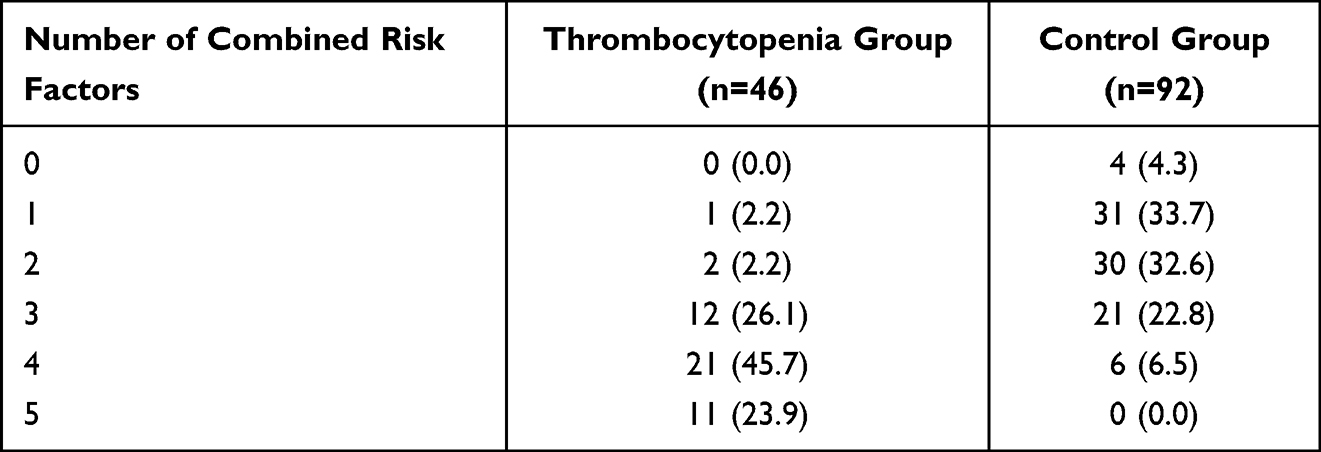 |
Table 5 Number of Combined Risk Factors in 2 Groups (n, %) |
Tigecycline Effects on Laboratory Test
Based on our analysis, we found significant elevations in DBIL, TBIL and BUN level in both thrombocytopenia group and control group (p<0.05) (Table 6). Conversely, we observed no significant changes in AST, ALT, SCR or eGFR levels associated with the treatment (p> 0.05). Additionally, the levels of ALB and HGB decreased in the thrombocytopenia group (p<0.05), but not in the control group (p>0.05).
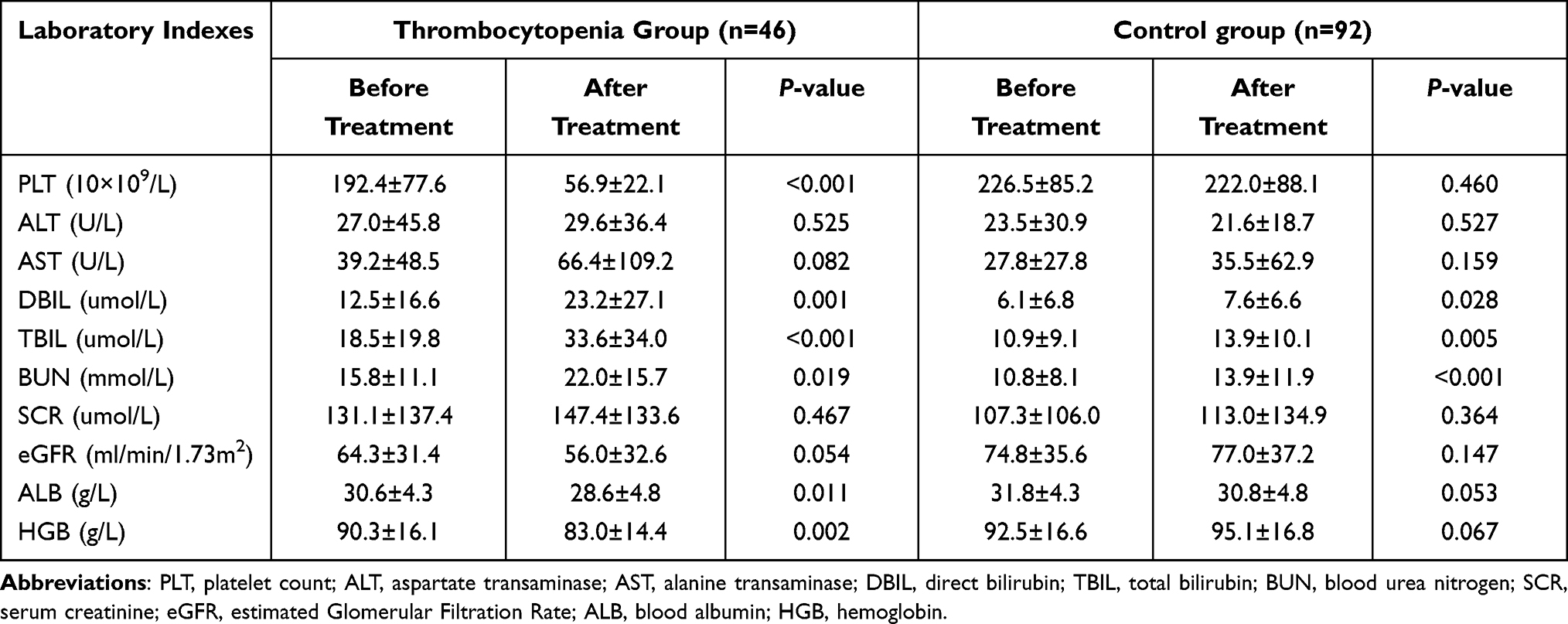 |
Table 6 Effect of Tigecycline on Laboratory Tests |
Discussion
Drug induced thrombocytopenia (DIT) necessitates special attention due to its relatively high incidence, particularly among critically ill patients. The prevalence of DIT is estimated at around 25% in critically ill patients.8 Various antimicrobial agents can trigger DIT through diverse mechanisms, including both immune-mediated and non-immune-mediated pathways.9 DIT primarily falls into two main categories: decreased platelet (PLT) production due to bone marrow suppression, and increased PLT destruction, often mediated by the immune pathway.10
The precise mechanism of tigecycline-induced DIT remains ambiguous. Our research revealed that thrombocytopenia developed within a timeframe spanning 2 to 22 days following the initiation of tigecycline treatment, with a median onset occurring at 9 days. Most patients demonstrated recovery of PLT counts upon discontinuation of tigecycline. Based on mechanism insights, non-immune-mediated thrombocytopenia tends to evolve gradually over a few weeks, linked to suppressed megakaryocytes leading to reduced PLT production. Conversely, immune-mediated thrombocytopenia typically emerges more rapidly, often after 7 to 14 days of treatment. In patients with prior exposure, its onset can occur within 1 to 3 days. Recovery of PLT levels after discontinuation of the medication may occur within days for immune-mediated DIT, whereas non-immune DIT may require an extended recovery duration.11 Considering the potential mechanism of tigecycline-induced thrombocytopenia, it is possible that this drug elicits thrombocytopenia through the immune-mediated pathway. A few studies have demonstrated that the relative occurrence of immune-mediated DIT, including hapten-dependent antibodies, quinine-type antibodies and autoantibodies.9,11 Therefore, conducting laboratory tests to identify platelet-reactive antibodies in suspected patients might prove valuable in investigating tigecycline-induced DIT. It is our anticipation that future research will shed more light on the association between tigecycline and thrombocytopenia.
Furthermore, in a two-week animal study, researchers observed that tigecycline induced bone marrow hypo-cellularity in rats and dogs at doses 8 and 10 times higher than the equivalent human daily dose, respectively. These effects demonstrated reversibility after a two-week administration period, implying that tigecycline may suppress bone marrow function.12 In a murine model, antibiotic therapy was found to suppress various types of hematopoietic progenitors, including HSCs and common lymphoid progenitors, indicating that the antibiotic-mediated myelopoiesis suppression relies on microbiome depletion. Therefore, preserving the microbiome could potentially mitigate the occurrence of tigecycline-associated bone marrow suppression.13
In our research, a comparison of concomitant medication between the thrombocytopenia group and the control group was conducted. The outcomes of univariate analysis revealed no discernible disparity in medication utilization pattern between the two groups, suggesting that the occurrence of thrombocytopenia was not associated with concomitant medications.
However, it is important to acknowledge that numerous non-pharmaceutical factors may also contribute to thrombocytopenia. In severely infected populations, conditions such as DIC and HIT should be considered in the differential diagnosis. The risk factors we identified in our study also demonstrated associations with aggravated sepsis and poor prognosis. Notably, eight patients in the thrombocytopenia group died, potentially hinting at a correlation with the occurrence of thrombocytopenia. Recent research has additionally proposed a potential role of Covid-19 in the development of thrombocytopenia.14
In our study, the incidence of tigecycline-associated thrombocytopenia was 12.3%, which is higher than that reported in previous studies. Specifically, a thrombocytopenia rate of 6.0% (49/817) was reported in a Phase III studies.15 This difference may be attributed to the advanced age and underlying health conditions characterizing our study’s patient cohort. The average age of the enrolled patients in our study was (75.4 ± 14.7) years, in contrast to the average age of (47.1 ± 18.6) years reported in the aforementioned phase III trial. Moreover, patients with significant hepatic or renal disease were excluded from the phase III study but deliberately included in our research. Our results demonstrated that advanced age (≥74 years), risk of malnutrition, tigecycline therapy for ≥7 days, DBIL>8.1μmol/L, BUN>8.1mmol/L were independent risk factor for tigecycline-associated thrombocytopenia. These findings are consistent with earlier studies that also identified older age and prolonged tigecycline exposure as risk factors for hypofibrinogenemia associated with tigecycline.16 Furthermore, a retrospective study investigating linezolid-induced thrombocytopenia found that renal insufficiency (crCL <60 mL/min), hemodialysis, and the extended linezolid therapy duration represented significant risk factors for thrombocytopenia associated with linezolid.17
The primary route of tigecycline elimination is biliary excretion (59%), wherein the compound is excreted unaltered. Renal excretion serves as a secondary route.18 An impairment in biliary excretion can prolong the tigecycline excretion time, leading to drug accumulation and potential overdosage. In addition, we observed that tigecycline therapy could elicit elevated bilirubin levels, particularly noticeable in patients with thrombocytopenia (DBIL: (12.5 ± 16.6) vs (23.2 ± 27.1), p=0.001; TBIL: (18.5 ± 19.8) vs (33.6 ± 34.0), p<0.001). Our study did not establish a relationship between eGFR and thrombocytopenia, a finding divergent from linezolid-induced thrombocytopenia.16 This suggests that renal function may not play a significant role in the development of thrombocytopenia during tigecycline therapy.19
In terms of risk factors for thrombocytopenia, our analysis highlighted that elevated BUN, distinct from SCR, emerged as an independent risk factor. BUN, modulated by both renal and non-renal factors, has exhibited predictive value for long-term mortality among critically ill patients, even when creatinine levels are within the normal range.20 Hyper-catabolism and nutrition support have demonstrated correlation with increased BUN levels and can potentially lead to compromised immune function.21,22 Additionally, malnourished patients receiving nutritional support after admission are prone to experience hyper-catabolism, thereby contributing to elevated BUN levels.
In contrast to the control group, patients in the thrombocytopenia group exhibit a heightened susceptibility towards underlying coagulation disorder, such as elevated INR or hypofibrinogenemia. This observation could potentially elucidate the rationale behind the reduction of ALB and HGB in the thrombocytopenia group. The serious consequences of erythropenia, neutropenia and thrombocytopenia underline the necessity for vigilant monitoring of bleeding manifestations and coagulation disorders during tigecycline therapy.23
Currently, scarce evidence supports the efficacy of specific treatment for DIT apart from discontinuation of the causative drug. Previous research addressing vancomycin-induced thrombocytopenia have indicated that interventions such as platelet transfusions, corticosteroids, plasma exchange, intravenous immunoglobulin, and anti-Rh immune globulin did not consistently elevate platelet levels in most patients until vancomycin was stopped.24 In our research, 95.7% of thrombocytopenic patients exhibited 3 to 5 risk factors. Thus, in cases where patients exhibit multiple risk factors for DIT, prudent consideration of alternative antimicrobials agent becomes paramount. However, if tigecycline remains imperative, we recommend routine blood examinations every three days to monitor platelet levels.
Several limitations warrant consideration. Firstly, this investigation adopted a retrospective case-control design, making it susceptible to selection bias. Secondly, despite the study’s execution within a substantial hospital setting, the findings may lack generalizability to all patient populations. Lastly, it is important to acknowledge that other factors, beyond tigecycline, can contribute to thrombocytopenia.
Conclusion
Thrombocytopenia constitutes a prevalent and potentially life-threatening adverse event linked to tigecycline, yet often remained underestimated. Through our analysis, advanced age (≥74 years), risk of malnutrition, tigecycline therapy for ≥ 7 days, DBIL>8.1μmol/L and BUN>8.1mmol/L emerged as independent risk factors for tigecycline-induced thrombocytopenia. Therefore, healthcare professionals should be vigilant to discern potential bleeding and regularly monitor platelet counts every three days throughout tigecycline therapy, particularly in patients with multiple risk factors. In scenarios where a decline in platelet levels becomes evident, deliberation over alternative antimicrobials should be considered.
Data Sharing Statement
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study, which was in compliance with the Declaration of Helsinki, received ethical approval from the Ethics Committee of Beijing Hospital (Permit Number: 2022BJYYEC-312-02).
The manuscript strictly omits any identifying information of human participants. As neither individual data were published nor any intervention was performed on patients, patient consent was waived by the Ethics Committee of Beijing Hospital.
Our research received ethical exemption from patient informed consent, granted by the Ethics Committee of Beijing Hospital (Permit Number: 2022BJYYEC-312-02).
Consent for Publication
All authors approved the final manuscript and the submission to this journal.
Acknowledgments
The author is indebted to Dr. Hu for his constructive suggestions, to Mr. Li for assisting in shaping the outline of this paper.
Funding
This manuscript was supported by funding from National High Level Hospital Clinical Research Funding (BJ-2022-173).
Disclosure
The authors declare the absence of known competing financial interests or personal relationships that could potentially influence the work reported in this paper.
References
1. Mckeage K, Keating GM. Tigecycline. Drugs. 2008;68(18):2633–2644. doi:10.2165/0003495-200868180-00008
2. Giamarellou H, Poulakou G. Pharmacokinetic and pharmacodynamics evaluation of tigecycline. Expert Opin Drug Metab Toxicol. 2011;7(11):1459–1470. doi:10.1517/17425255.2011.623126
3. Kasbekar N. Tigecycline: a critical safety review. Expert Opin Drug Saf. 2015;14(2):335–342. doi:10.2146/ajhp050487
4. Peterson LR. A review of tigecycline--the first glycylcycline. Int J Antimicrob Agents. 2008;32(Suppl 4):S215–22. doi:10.1016/S0924-8579(09)70005-6
5. Giryes S, Azzam ZS, Reem IB, Norberto K, Gidon B. Severe Coagulation Disorder and Thrombocytopenia Associated with Tigecycline - Case Report and Review of Literature. Curr Drug Saf. 2017;12(1):7–9. doi:10.2174/1574886311666160920090714
6. Guo M, Liang J, Li D. Coagulation dysfunction events associated with tigecycline: a real-world study from FDA adverse event reporting system (FAERS) database. Thromb J. 2022;20(1):12.
7. NIH. Common Terminology Criteria for Adverse Events.CTCAE. v6.0; 2020. Available from: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
8. Kam T, Alexander M. Drug-induced immune thrombocytopenia. Drug Saf. 2004;27(15):1243–1252. doi:10.2165/00002018-200427150-00007
9. Mitta A, Curtis BR, Reese JA, George JN. Drug-induced thrombocytopenia: 2019 Update of clinical and laboratory data. Am J Hematol. 2019;94(3):E76–E78. doi:10.1002/ajh.25379
10. Aster RH, Bougie DW. Drug-induced immune thrombocytopenia. N Engl J Med. 2007;357:580–587. doi:10.1177/0897190014546099
11. Loo AS, Gerzenshtein L, Ison MG. Antimicrobial drug-induced thrombocytopenia: a review of the literature. Semin Thromb Hemost. 2012;38(8):818–829. doi:10.1055/s-0032-1328882
12. FDA Label. TYGACIL; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/021821s049lbl.pdf.
13. Josefsdottir KS, Baldridge MT, Kadmon CS, King KY. Antibiotics impair murine hematopoiesis by depleting the intestinal microbiota. Blood. 2017;129(6):729–739. doi:10.1182/blood-2016-03-708594
14. Lassandro G, Palladino V, Palmieri VV, Amoruso A, Del Vecchio GC, Giordano P. Covid-19 and Children with Immune Thrombocytopenia: emerging Issues. Mediterr J Hematol Infect Dis. 2020;12(1):e2020028. doi:10.4084/MJHID.2020.028
15. Babinchak T, Ellis-Grosse E, Dartois N, Gilbert MR, Evan L; Tigecycline 301 Study Group, Tigecycline 306 Study Group. The efficacy and safety of tigecycline for the treatment of complicated intra-abdominal infections: analysis of pooled clinical trial data. Clin Infect Dis. 2005;41(Suppl 5):S354–67. doi:10.1086/431676
16. Hanai Y, Matsuo K, Ogawa M, et al. A retrospective study of the risk factors for linezolid-induced thrombocytopenia and anemia. J Infect Chemother. 2016;22(8):536–542. doi:10.1016/j.jiac.2016.05.003
17. Hu J, Xiao YH, Zheng Y, Lai YX, Fang XL, Fang Q. Clinical characteristics and risk factors of tigecycline-associated hypofibrinogenaemia in critically ill patients. Eur J Clin Pharmacol. 2020;76(7):913–922. doi:10.1007/s00228-020-02860-w
18. Hoffmann M, DeMaio W, Jordan RA, et al. Metabolism, excretion, and pharmacokinetics of [14C] tigecycline, a firstin-class glycylcycline antibiotic after intravenous infusion to healthy male subjects. Drug Metab Dispos. 2007;35:1543–1553. doi:10.1124/dmd.107.015735
19. Yaghoubi S, Zekiy AO, Krutova M, et al. Tigecycline antibacterial activity, clinical effectiveness, and mechanisms and epidemiology of resistance: narrative review. Eur J Clin Microbiol Infect Dis. 2022;41(7):1003–1022. doi:10.1007/s10096-020-04121-1
20. Beier K, Eppanapally S, Bazick HS, et al. Elevation of blood urea nitrogen is predictive of long-term mortality in critically ill patients independent of normal creatinine. Crit Care Med. 2011;39:305–313. doi:10.1097/CCM.0b013e3181ffe22a
21. Ballmer PE, McNurlan MA, Hulter HN, Anderson SE, Garlick PJ, Krapf R. Chronic metabolic acidosis decreases albumin synthesis and induces negative nitrogen balance in humans. J Clin Investigation. 1995;95:39–45. doi:10.1172/JCI117668
22. Chen WJ, Oashi E, Kasai M. Amino acid metabolism in parenteral nutrition: with special reference to the calorie: nitrogen ratio and the blood urea nitrogen level. Metabolism. 1974;23(12):1117–1123. doi:10.1016/0026-0495(74)90028-6
23. Farruggia P, Fioredda F, Puccio G, et al. Idiopathic neutropenia of infancy: data from the Italian Neutropenia Registry. Am J Hematol. 2019;94(2):216–222. doi:10.1002/ajh.25353
24. Von Drygalski A, Curtis BR, Bougie DW, et al. Vancomycin-induced immune thrombocytopenia. N Engl J Med. 2007;356:904–910. doi:10.1056/NEJMoa065066
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.