Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Clinical Laboratory Data in Japan: A Comparative Study of Patients with Psychiatric Disorders and the General Population
Authors Iwata M, Hatano M ![]() , Ito K, Matsuzaki H, Yamada S
, Ito K, Matsuzaki H, Yamada S
Received 12 June 2023
Accepted for publication 16 September 2023
Published 2 October 2023 Volume 2023:19 Pages 2061—2068
DOI https://doi.org/10.2147/NDT.S425541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Miko Iwata,* Masakazu Hatano,* Kana Ito, Haruna Matsuzaki, Shigeki Yamada
Department of Pharmacotherapeutics and Informatics, Fujita Health University School of Medicine, Toyoake, Aichi, Japan
*These authors contributed equally to this work
Correspondence: Masakazu Hatano, Department of Pharmacotherapeutics and Informatics, Fujita Health University School of Medicine, 1-98 Dengakugakubo, Kutsukake, Toyoake, Aichi, 470-1192, Japan, Tel +81 562932157, Fax +81 562934537, Email [email protected]
Purpose: Several nationwide population-based studies have reported that patients with psychiatric disorders are at higher risk of developing chronic kidney disease, chronic liver disease, and metabolic syndrome than the general population; however, there are insufficient studies in the Japanese population. Thus, we aimed to clarify the influence of psychiatric disorders on clinical laboratory data in the Japanese population.
Patients and Methods: This cross-sectional study was based on medical records from the Department of Psychiatry at Fujita Health University Hospital and the 6th National Database of Health Insurance Claims and Specific Health Checkups of Japan Open Data Japan (specific health checkups in 2018) in the Ministry of Health, Labor and Welfare. The primary endpoint was the incidence of clinical laboratory abnormalities in patients with psychiatric disorders and the general Japanese population.
Results: Compared to the general Japanese population, patients with psychiatric disorders had significantly higher rates of the following clinical laboratory abnormalities: estimated glomerular filtration rate, alanine transaminase, aspartate aminotransferase (AST), body mass index (BMI), high-density lipoprotein cholesterol (HDL-C), triglycerides, and hemoglobin A1c (HbA1c). In the age-specific analysis, AST, BMI, HDL-C, and HbA1c levels were more frequently abnormal in patients with psychiatric disorders only in the 40– 49 and 50– 59 age groups.
Conclusion: Our results showed that patients with psychiatric disorders have higher rates of various clinical laboratory abnormalities than the general Japanese population, with stronger influences in the middle-aged group. These data suggest the importance of monitoring and preventing chronic diseases in patients with psychiatric disorders in Japan.
Keywords: big data, chronic kidney disease, diabetes mellitus, liver diseases, metabolic syndrome, mental disorders
Introduction
The life expectancy of patients with psychiatric disorders, such as schizophrenia and bipolar disorder, is approximately 10–20 years shorter than that of the general population.1–3 A recent meta-analysis provided strong evidence that patients with schizophrenia have significantly higher mortality due to a variety of conditions, including respiratory, endocrine, and cardiovascular diseases.4 The estimated prevalence and relative risk (RR) of obesity, dyslipidemia, and diabetes in patients with schizophrenia is 45–55% (RR:1.5–2), 25–69% (RR:2–3), and 10–15% (RR:2), respectively. In patients with bipolar disorder, the estimated prevalence and RR of obesity, dyslipidemia, and diabetes is 21–49% (RR:1–2), 23–38% (RR: ≤ 3), and 8–17% (RR:1.5–2), respectively.5 Therefore, patients with psychiatric disorders are at a higher risk of developing metabolic syndrome (MetS) than the general population. Furthermore, these comorbidities are considered risk factors for chronic kidney (CKD) and chronic liver disease (CLD), and population-based studies have shown that patients with schizophrenia are significantly associated with CKD and CLD.6–8
These factors have been attributed not only to unhealthy lifestyle habits but also to the risk of metabolic abnormalities caused by second-generation antipsychotics.9 Moreover, lithium use has been reported as a risk factor for CKD.10,11 Since most psychotropic drugs are metabolized in the liver, the impact of long-term use on CLD is also concerning. In Japan, the rate of polypharmacy and high-dose prescription of psychotropic drugs is particularly high compared to that in other countries.12 With this background, patients with schizophrenia in Japan might be at high risk for hepatic dysfunction.
The risk of developing MetS, CKD, and CLD is influenced by ethnicity and culture (eg, lifestyle); thus, study results may differ between countries. To our knowledge, there are no studies comparing renal and hepatic function in Japanese patients with psychiatric disorders to the general population, and therefore, a nationwide population-based study in Japan is needed to evaluate this issue. This study aimed to clarify the influence of psychiatric disorders on clinical laboratory data in the Japanese population by referring to the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB) Open Data Japan and comparing it with the general Japanese population.
Materials and Methods
Study Design
This cross-sectional study was based on medical records and NDB Open Data Japan. The NDB Open Data Japan is a national healthcare database that records health insurance claims and specific health checkups and guidance data. Specific health checkups are medical checkups conducted for insured individuals aged 40–74 years to prevent metabolic syndrome. The clinical laboratory data of patients with psychiatric disorders were obtained from the medical records of the Department of Psychiatry at Fujita Health University Hospital. Data on the Japanese general population was obtained from the 6th NDB Open Data Japan (specific health checkups in 2018) from the Ministry of Health, Labor and Welfare website (https://www.mhlw.go.jp/index.html). The study period was from April 2018 to March 2019, corresponding to specific health checkups conducted in 2018. The clinical laboratory data included estimated glomerular filtration rate (eGFR), aspartate aminotransferase (ALT), alanine aminotransferase (AST), body mass index (BMI), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglyceride (TG), and hemoglobin A1c (HbA1c). If more than one clinical laboratory data point was registered during the study period, the oldest point was used.
Clinical laboratory data in the NDB Open Data Japan are categorized according to each value (eg, AST:30 IU/L or less, 31–50 IU/L, and 51 IU/L or more) and are further aggregated by age (in 5-year increments), sex, and prefecture. We created a contingency table based on whether these data exceeded the reference intervals (eGFR ≧ 60 mL/min/1.73 m2, ALT ≦ 30 IU/L, AST ≦ 30 IU/L, BMI < 25 kg/m2, HDL-C ≧ 40 mg/dL, LDL-C < 140 mg/dL, TG < 150 mg/dL, and HbA1c < 5.6%). Because the NDB Open Data Japan omitted aggregate results of < 10, we treated these as missing values. Similarly, we created a contingency table in the same format as the clinical laboratory data of the Department of Psychiatry at Fujita Health University Hospital.
The study procedures were performed in accordance with the principles of the Declaration of Helsinki, and the study was approved by the Institutional Review Board of Fujita Health University (HM22-034). No informed consent was required because this was an observational study conducted using medical records; however, the patients had the right to revoke their consent and opt out of the study since we made information about the study publicly available.
Assessment
The primary endpoint was the incidence of clinical laboratory abnormalities (defined as the number of patients whose clinical laboratory data exceeded the institutional reference interval for each laboratory test) in patients with psychiatric disorders compared with that in the general Japanese population. The secondary endpoints were age- and sex-specific incidences of clinical laboratory abnormalities.
Statistical Analysis
Since the data from NDB Open Data Japan were registered as aggregated data, patient backgrounds were available only for patients with psychiatric disorders, and each clinical laboratory data was presented as mean and standard deviation. Based on a contingency table created from the medical records of the Department of Psychiatry, Fujita Medical University Hospital, and NDB Open Data Japan, we evaluated the incidence of clinical laboratory abnormalities in patients with psychiatric disorders and the general Japanese population. The odds ratio [OR] and 95% confidence interval [CI] were calculated using Fisher’s exact test. Missing values in each dataset were excluded. P-values were two-sided, and statistical significance was set at P < 0.05. The sample size was determined based on the number of participants enrolled during the study period. All statistical analyses were performed using R 4.1.2 (The R Foundation for Statistical Computing).
Results
Patient Characteristics
A total of 615 patients (mean age ± standard deviation [SD], 54.3 ± 10.0; male, 256) with psychiatric disorders for whom clinical laboratory data were obtained from medical records were included. The characteristics of the patients with psychiatric disorders at Fujita Health University Hospital are summarized in Table 1. Approximately 29.4 million people are registered for specific health checkup data in the NDB Open Data Japan.
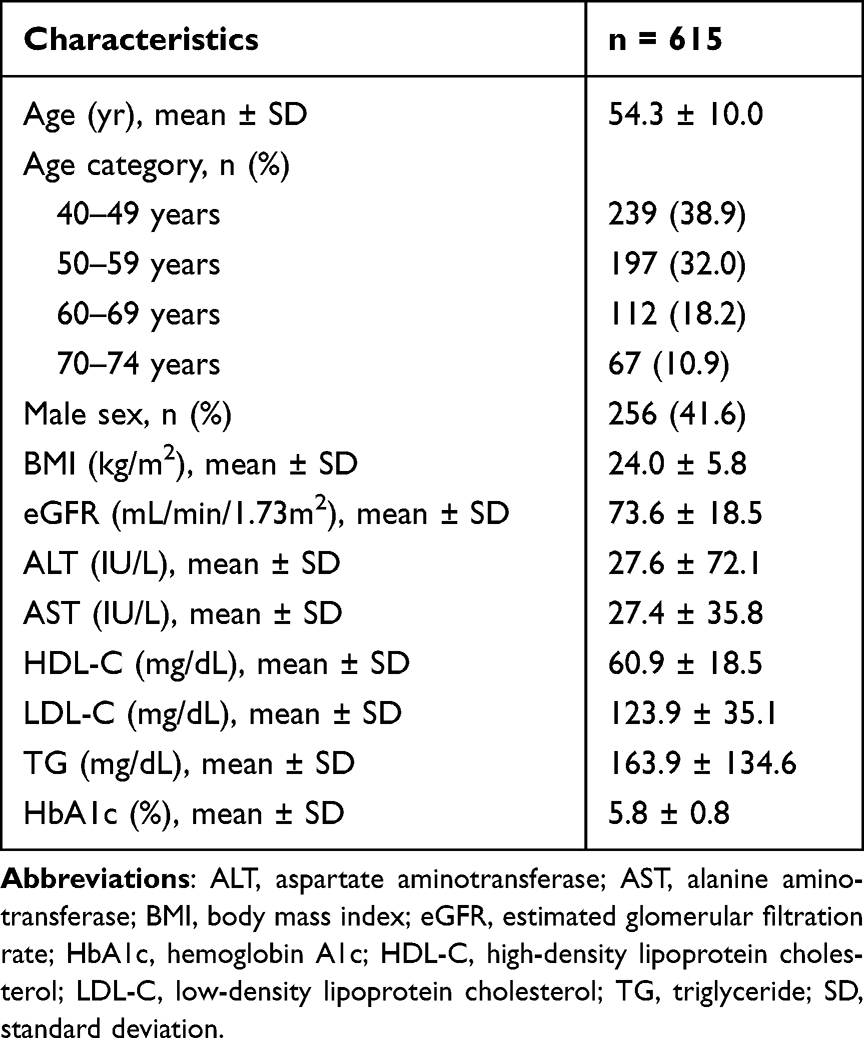 |
Table 1 Background of Patients with Psychiatric Disorders |
Incidences of Clinical Laboratory Abnormalities
The incidences of clinical laboratory abnormalities in patients with psychiatric disorders and in the general Japanese population are summarized in Table 2. Compared to the general Japanese population, patients with psychiatric disorders had significantly higher rates of the following clinical laboratory abnormalities: eGFR (OR, 1.96; 95% CI, 1.58–2.42), ALT (OR, 1.34; 95% CI, 1.09–1.62), AST (OR, 1.51; 95% CI, 1.24–1.84), BMI (OR, 1.62; 95% CI, 1.17–2.24), HDL-C (OR, 2.53; 95% CI, 1.75–3.57), TG (OR, 2.78; 95% CI, 2.28–3.37), and HbA1c (OR, 1.27; 95% CI, 1.04–1.56).
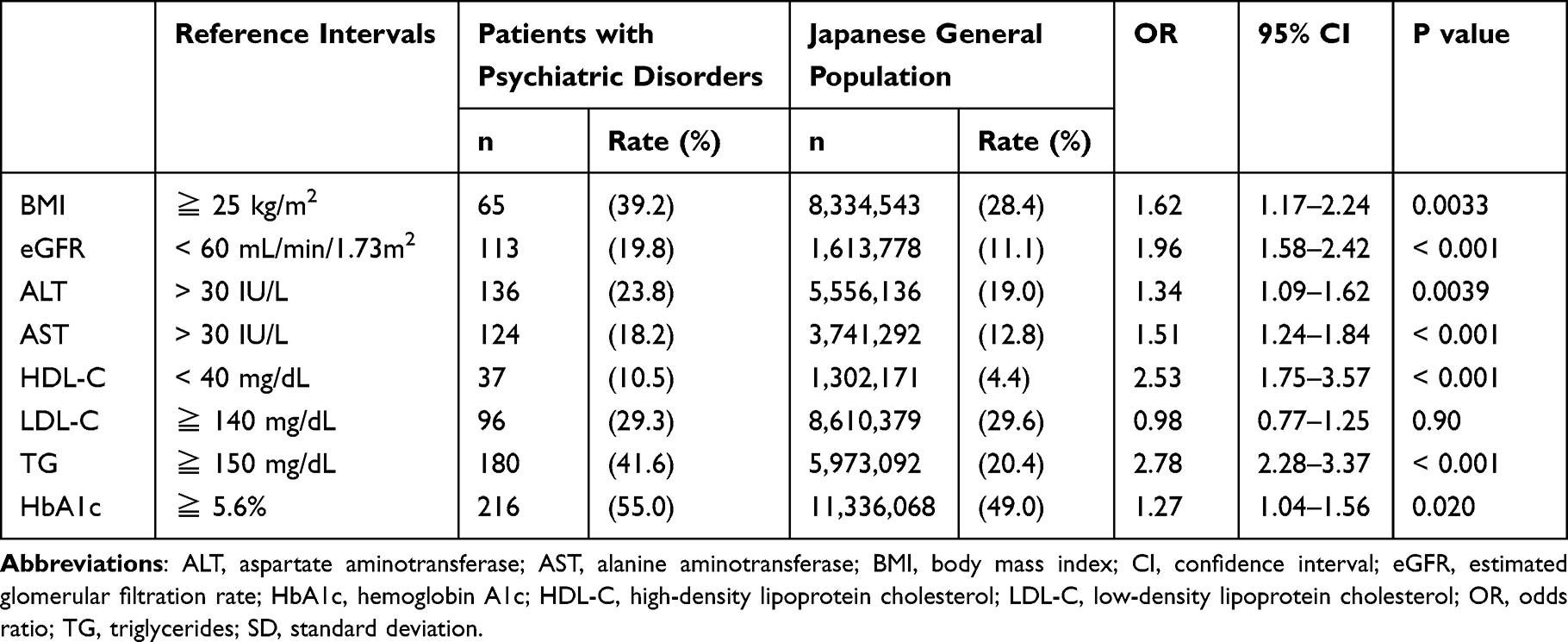 |
Table 2 Incidences of Clinical Laboratory Abnormalities |
Age- and Sex-Specific Incidences of Clinical Laboratory Abnormalities
The age-specific incidences of clinical laboratory abnormalities in patients with psychiatric disorders and in the general Japanese population are summarized in Table 3. In the 40–49 age group, compared to the Japanese general population, patients with psychiatric disorders had significantly higher rates of the following clinical laboratory abnormalities: eGFR (OR, 3.28; 95% CI, 2.07–4.99), AST (OR, 1.50; 95% CI, 1.02–2.15), BMI (OR, 1.99; 95% CI, 1.18–3.33), HDL-C (OR, 3.19; 95% CI, 1.82–5.28), TG (OR, 2.74; 95% CI, 2.02–3.70), and HbA1c (OR, 1.74; 95% CI, 1.25–2.43). In contrast, in the 70–74 age group, only eGFR (OR, 2.83; 95% CI, 1.67–4.82) and TG (OR, 2.44; 95% CI, 1.12–5.10) exhibited significantly higher rates of abnormalities in patients with psychiatric disorders compared to the general population. Additionally, only TG levels showed significant differences among all age groups.
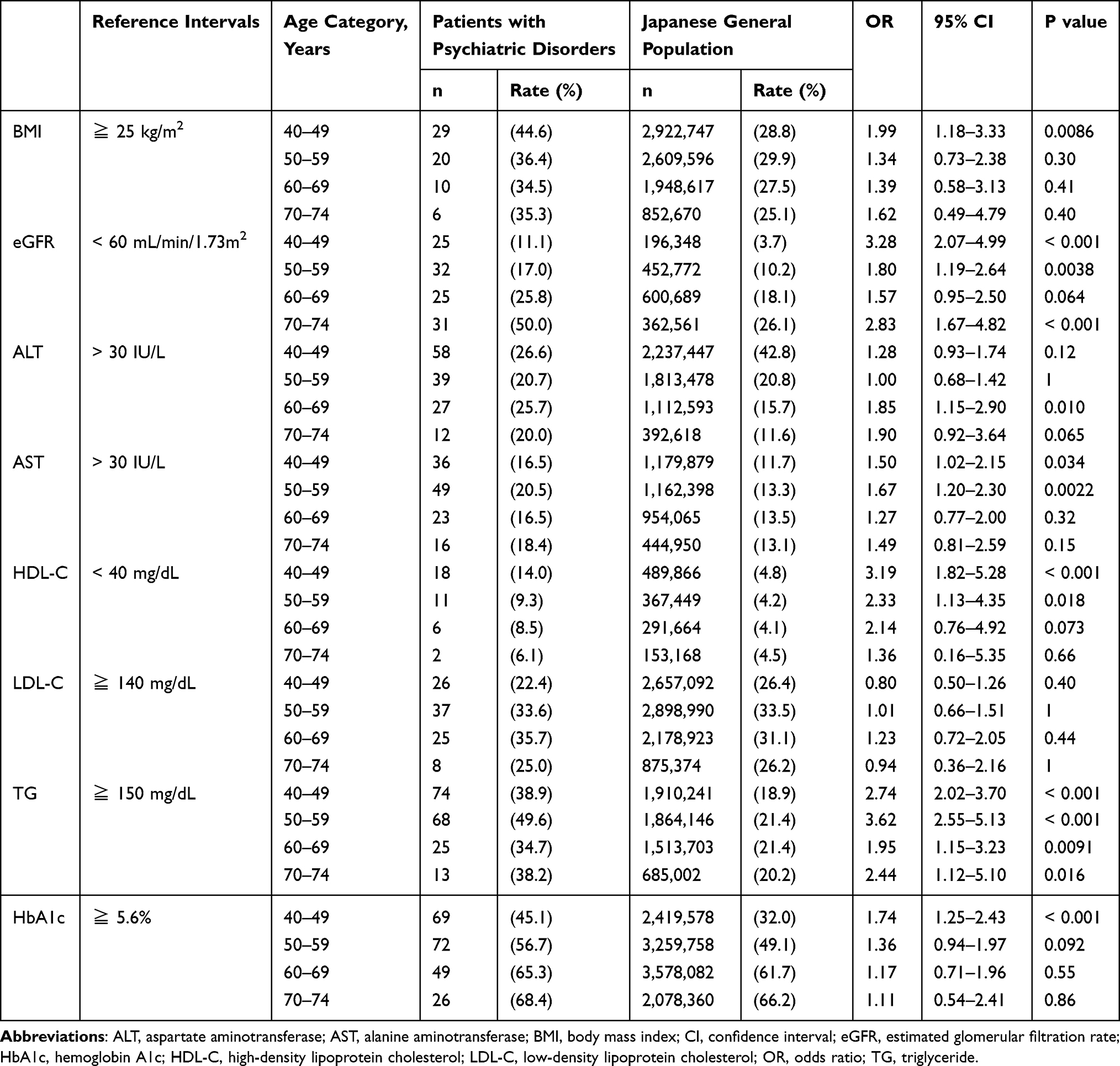 |
Table 3 Age-Specific Incidences of Clinical Laboratory Abnormalities |
The sex-specific incidences of clinical laboratory abnormalities in patients with psychiatric disorders compared to those in the general Japanese population are summarized in Table 4. HbA1c was associated with a significantly higher rate of laboratory abnormalities in males with psychiatric disorders (OR, 1.38; 95% CI, 1.00–1.91), and BMI was associated with a significantly higher rate of laboratory abnormalities in females with psychiatric disorders (OR, 2.24; 95% CI, 1.41–3.50).
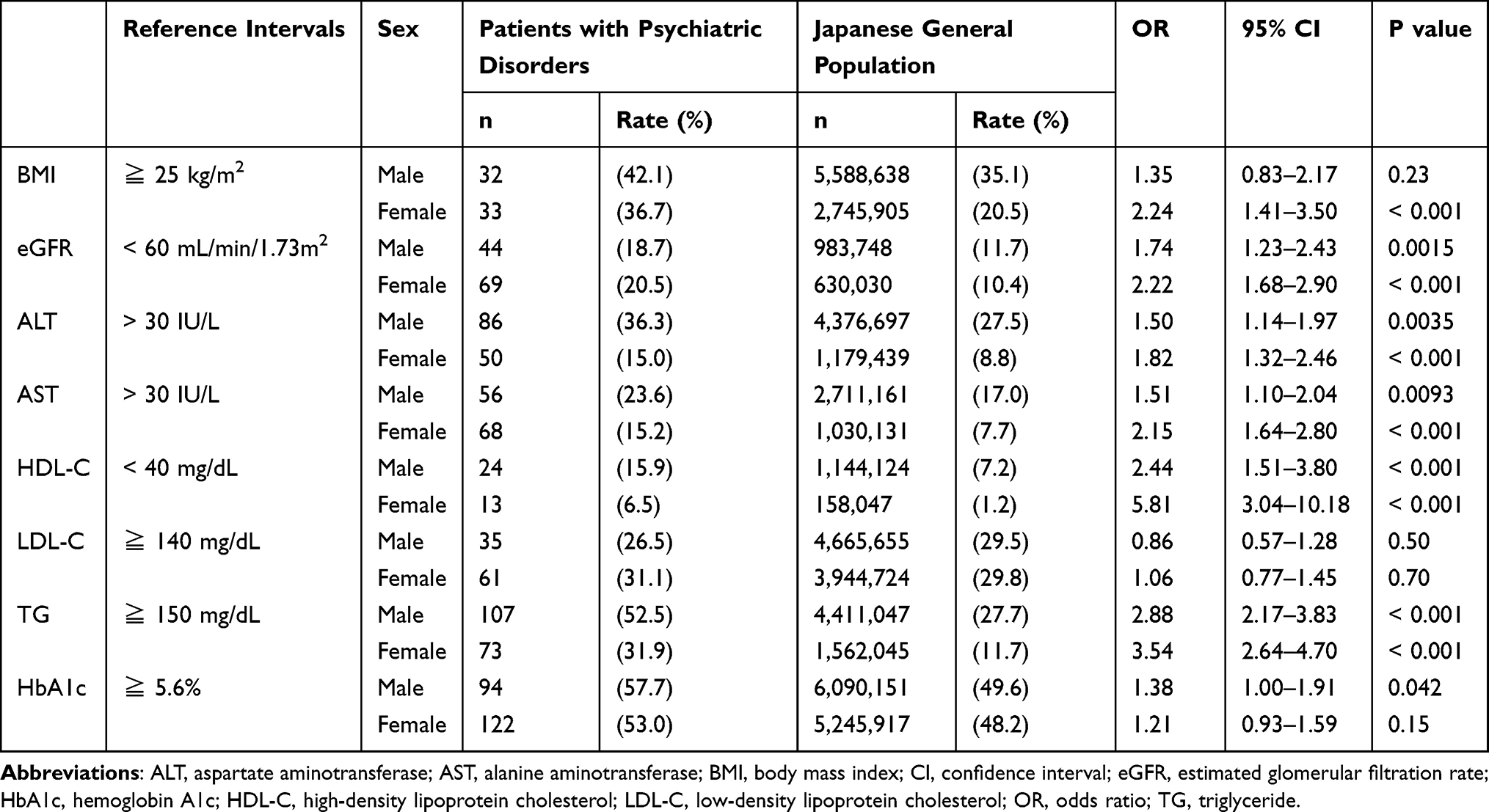 |
Table 4 Sex-Specific Incidences of Clinical Laboratory Abnormalities |
Discussion
This study evaluated renal function, hepatic function, and MetS-related clinical laboratory abnormalities in patients with psychiatric disorders. This is the first study to reference the NDB Open Data Japan for the general Japanese population and to compare it with the clinical laboratory data of patients with psychiatric disorders. Our results revealed that patients with psychiatric disorders exhibited significantly increased rates of clinical laboratory abnormalities in all parameters except LDL-C compared to the general Japanese population. A cross-sectional study based on medical records in Japanese psychiatric hospitals reported a higher prevalence of MetS in patients with schizophrenia than in the general population.13 Another cohort study showed that patients with depression had significantly higher rates of one of the following in addition to abdominal obesity: high blood pressure, hyperglycemia, and dyslipidemia.14 To our knowledge there are no studies comparing the renal and hepatic function of Japanese patients with psychiatric disorders to those in the general population. Nonetheless, nonalcoholic fatty liver disease is significantly associated with the total dose of antipsychotics in patients with schizophrenia in Japan.15 The results of this study directly or indirectly support previous studies in Japanese patients, and replicated studies from other countries showing an association between CKD and psychiatric disorders. Thus, our findings suggest that the physical risk is similarly high in Japanese patients with psychiatric disorders.
In the age-specific analysis, AST, BMI, HDL-C, and HbA1c levels were more frequently abnormal in patients with psychiatric disorders only in the 40–49 and 50–59 age groups. The abovementioned study on the prevalence of MetS in Japanese patients with schizophrenia showed a similar trend, with significant differences from the general population only in the middle-aged group.13 Population-based studies in Taiwan have also reported that the risk of metabolic diseases, such as diabetes and dyslipidemia, is higher in younger than in older people.16 In this regard, Liao et al noted that older patients may have already gone through the age of developing metabolic diseases. With regard to AST, nonalcoholic fatty liver disease affects people of any age,17 but this disease is strongly correlated with components of MetS, such as obesity, diabetes, and dyslipidemia, and may have been influenced by these factors.18 However, ALT was not significantly different between patients with psychiatric disorders and the general population in the middle-aged group in this study. Nonetheless, this needs to be further examined.
Our results showed that BMI was significantly higher in psychiatric patients only among women and HbA1c was significantly higher only in men. In the general Japanese population, women have lower rates of obesity than men.19 However, women with schizophrenia or bipolar disorder have higher MetS and abdominal obesity.20–22 This could be because weight gain due to antipsychotics is greater in women than in men.23 In contrast, the risk of weight gain and hyperglycemia varies among antipsychotics, and the failure to account for these effects may be the reason for the inconsistent results in this study.24,25
This study had several limitations. First, data for the general Japanese population was referred from a large national database, whereas that for patients with psychiatric disorders was limited to the medical records of a single institution. Therefore, this study may not reflect the general population of patients with psychiatric disorders which limits any extrapolations. In addition, the patients may have been at a higher-than-usual mental and physical risk because they were admitted to a university hospital. Future evaluations should increase the sample size of patients with psychiatric disorders, ideally using a national database of similar sizes. Second, this study did not account for the background factors of patients with psychiatric disorders and the general Japanese population. These include the influence of medication on existing physical illnesses and psychiatric disorders. Third, our study included all psychiatric disorders but did not consider their detailed breakdown (eg, schizophrenia, bipolar disorders, etc.) or severity. Fourth, explaining the risk of each physical disease solely in terms of clinical laboratory abnormalities is difficult. Particularly, liver function should be comprehensively evaluated not only by assessing ALT and AST but also by albumin, bilirubin, platelets, and prothrombin time. However, these clinical laboratory data could not be compared because they were not registered in the NDB Open Data Japan. Finally, because this was a cross-sectional observational study, the influence of psychiatric disorders over time remains unknown. Thus, it is difficult to demonstrate a strictly causal relationship between a history of psychiatric disorders and clinical laboratory abnormalities.
Conclusion
In conclusion, our results showed that patients with psychiatric disorders had a higher rate of various clinical laboratory abnormalities than the general Japanese population. The results also reveal that a history of psychiatric disorders has a greater influence on laboratory parameters of middle-aged individuals than in older adults. These data suggest the importance of monitoring and preventing chronic diseases in patients with psychiatric disorders in Japan. Further studies with larger sample sizes that account for confounding factors are required to confirm this causal relationship.
Acknowledgments
We would like to thank Editage for the English language editing.
Funding
This study was funded by TAIHO PHARMACEUTICAL through scholarship donations. These funders were not involved in the study design; collection, analysis, interpretation of data; writing of this article; or the decision to submit it for publication.
Disclosure
MH received honoraria from Ishiyaku Publishers, Inc., Meiji Seika Pharma Co., Ltd., Medical Friend. Co., Ltd., Nanzando Co., Ltd., Sumitomo Pharma Co., Ltd., and WELCIA Holdings Co., Ltd. SY received honoraria from AstraZeneca K.K., Daiichi Sankyo Co., Ltd., EA Pharma Co., Ltd., Eisai Co., Ltd., Meiji Seika Pharma Co., Ltd., Nippon Shinyaku Co., Ltd., Nipro Corporation, Otsuka Pharmaceutical Factory, Pfizer Japan Inc., Taisho Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., Toa Eiyo Ltd., and Towa Pharmaceutical Co., Ltd. And funding from EA Pharma Co., Ltd., Kissei Pharmaceutical Co., Ltd., Mochida Pharmaceutical Co., Ltd., SUGI Holdings Co., Ltd., and Otsuka Pharmaceutical Factory. The authors report no other conflicts of interest in this work.
References
1. Chan JKN, Tong CHY, Wong CSM, Chen EYH, Chang WC. Life expectancy and years of potential life lost in bipolar disorder: systematic review and meta-analysis. Br J Psychiatry. 2022;221(3):567–576. doi:10.1192/bjp.2022.19
2. Chang CK, Hayes RD, Perera G, et al. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS One. 2011;6(5):e19590. doi:10.1371/journal.pone.0019590
3. Crump C, Winkleby MA, Sundquist K, Sundquist J. Comorbidities and mortality in persons with schizophrenia: a Swedish national cohort study. Am J Psychiatry. 2013;170(3):324–333. doi:10.1176/appi.ajp.2012.12050599
4. Correll CU, Solmi M, Croatto G, et al. Mortality in people with schizophrenia: a systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry. 2022;21(2):248–271. doi:10.1002/wps.20994
5. De Hert M, Schreurs V, Vancampfort D, Van Winkel R. Metabolic syndrome in people with schizophrenia: a review. World Psychiatry. 2009;8(1):15–22. doi:10.1002/j.2051-5545.2009.tb00199.x
6. Grant RK, Brindle WM, Donnelly MC, et al. Gastrointestinal and liver disease in patients with schizophrenia: a narrative review. World J Gastroenterol. 2022;28(38):5515–5529. doi:10.3748/wjg.v28.i38.5515
7. Tzeng NS, Hsu YH, Ho SY, et al. Is schizophrenia associated with an increased risk of chronic kidney disease? A nationwide matched-cohort study. BMJ Open. 2015;5(1):e006777. doi:10.1136/bmjopen-2014-006777
8. Tzur Bitan D, Krieger I, Berkovitch A, Comaneshter D, Cohen A. Chronic kidney disease in adults with schizophrenia: a nationwide population-based study. Gen Hosp Psychiatry. 2019;58:1–6. doi:10.1016/j.genhosppsych.2019.01.007
9. Pillinger T, McCutcheon RA, Vano L, et al. Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry. 2020;7(1):64–77. doi:10.1016/S2215-0366(19)30416-X
10. Iwagami M, Mansfield KE, Hayes JF, et al. Severe mental illness and chronic kidney disease: a cross-sectional study in the United Kingdom. Clin Epidemiol. 2018;10:421–429. doi:10.2147/CLEP.S154841
11. Kessing LV, Gerds TA, Feldt-Rasmussen B, Andersen PK, Licht RW. Use of lithium and anticonvulsants and the rate of chronic kidney disease: a nationwide population-based study. JAMA Psychiatry. 2015;72(12):1182–1191. doi:10.1001/jamapsychiatry.2015.1834
12. Dong M, Zeng LN, Zhang Q, et al. Prescription of antipsychotic and concomitant medications for adult Asian schizophrenia patients: findings of the 2016 Research on Asian Psychotropic Prescription Patterns (REAP) survey. Asian J Psychiatry. 2019;45:74–80. doi:10.1016/j.ajp.2019.08.010
13. Sugawara N, Yasui-Furukori N, Sato Y, et al. Prevalence of metabolic syndrome among patients with schizophrenia in Japan. Schizophr Res. 2010;123(2–3):244–250. doi:10.1016/j.schres.2010.08.030
14. Ohmori Y, Ito H, Morita A, Deura K, Miyachi M; Saku Cohort Study Group. Associations between depression and unhealthy behaviours related to metabolic syndrome: a cross sectional study. Asia Pac J Clin Nutr. 2017;26(1):130–140. doi:10.6133/apjcn.112015.01
15. Koreki A, Mori H, Nozaki S, Koizumi T, Suzuki H, Onaya M. Risk of nonalcoholic fatty liver disease in patients with schizophrenia treated with antipsychotic drugs: a cross-sectional study. J Clin Psychopharmacol. 2021;41(4):474–477. doi:10.1097/JCP.0000000000001421
16. Liao CH, Chang CS, Wei WC, et al. Schizophrenia patients at higher risk of diabetes, hypertension and hyperlipidemia: a population-based study. Schizophr Res. 2011;126(1–3):110–116. doi:10.1016/j.schres.2010.12.007
17. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346(16):1221–1231. doi:10.1056/NEJMra011775
18. Marchesini G, Bugianesi E, Forlani G, et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology. 2003;37(4):917–923. doi:10.1053/jhep.2003.50161
19. Yamakita M, Uchida H, Kawamura K, Homma T, Odagiri Y. 日本人成人の肥満者割合および脂肪エネルギー比率の年次推移に対する年齢–時代–コホートの影響[Effects of age, period, and cohort on the trends in obesity rate and energy intake ratio from fat in Japanese adults]. Nihon Koshu Eisei Zasshi. 2014;61(8):371–384. Japanese.
20. Baskaran A, Cha DS, Powell AM, Jalil D, McIntyre RS. Sex differences in rates of obesity in bipolar disorder: postulated mechanisms. Bipolar Disord. 2014;16(1):83–92. doi:10.1111/bdi.12141
21. Shojaeimotlagh V, Hashiehbaf A, Karami M, Monjazebi F, Gheshlagh RG. Prevalence of metabolic syndrome in Iranian patients with schizophrenia: a systematic review and meta-analysis. Diabetes Metab Syndr. 2019;13(1):143–147. doi:10.1016/j.dsx.2018.08.014
22. Nayerifard R, Bureng MA, Zahiroddin A, Namjoo M, Rajezi S. Comparison of metabolic syndrome prevalence in patients with schizophrenia and bipolar I disorder. Diabetes Metab Syndr. 2017;11(suppl 1):S411–S416. doi:10.1016/j.dsx.2017.03.027
23. Seeman MV. Secondary effects of antipsychotics: women at greater risk than men. Schizophr Bull. 2009;35(5):937–948. doi:10.1093/schbul/sbn023
24. Huhn M, Nikolakopoulou A, Schneider-Thoma J, et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis. Lancet. 2019;394(10202):939–951. doi:10.1016/S0140-6736(19)31135-3
25. Sawagashira R, Yamamura R, Okubo R, et al. Subthreshold change in glycated hemoglobin and body mass index after the initiation of second-generation antipsychotics among patients with schizophrenia or bipolar disorder: a nationwide prospective cohort study in Japan. J Clin Psychiatry. 2022;83(3). doi:10.4088/JCP.21m14099
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Metabolic Syndrome and Socioeconomic Status in Association with Chronic Kidney Disease: A Cross-Sectional Study in Ningbo, China
Huang S, Yao X, Chen X, Chen X, Li Y, Kanwar Y, Chan FKS, Ye P, Zhan M
Diabetes, Metabolic Syndrome and Obesity 2024, 17:3891-3901
Published Date: 21 October 2024