")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Clinical Guideline (CANMAT 2016) Discordance of Medications for Patients with Major Depressive Disorder in China
Authors Zhu Y , Wu Z , Zhao D, Wu X, He R, Wang Z , Peng D , Fang Y
Received 13 December 2022
Accepted for publication 23 March 2023
Published 12 April 2023 Volume 2023:19 Pages 829—839
DOI https://doi.org/10.2147/NDT.S401359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Richard J Porter
Yuncheng Zhu,1– 3,* Zhiguo Wu,4,* Dongmei Zhao,5 Xiaohui Wu,2 Ruoqiao He,6 Zuowei Wang,1,3 Daihui Peng,2 Yiru Fang2,7– 9
1Division of Mood Disorders, Shanghai Hongkou Mental Health Center, Shanghai, People’s Republic of China; 2Clinical Research Center & Division of Mood Disorders, Shanghai Mental Health Center, Shanghai JiaoTong University School of Medicine, Shanghai, People’s Republic of China; 3Clinical Research Center for Mental Health, School of Medicine, Shanghai University, Shanghai, People’s Republic of China; 4Clinical Research Center in Mental Health, Shanghai Yangpu District Mental Health Center, Shanghai University of Medicine & Health Sciences, Shanghai, People’s Republic of China; 5Division of Psychiatry, Shanghai Changning Mental Health Center, Shanghai, People’s Republic of China; 6New York University, New York, NY, USA; 7Department of Psychiatry & Affective Disorders Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 8CAS Center for Excellence in Brain Science and Intelligence Technology, Shanghai, People’s Republic of China; 9Shanghai Key Laboratory of Psychotic Disorders, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yiru Fang, Email [email protected]
Objective: This survey aims to explore the current medical treatment of major depressive disorder (MDD) in China and match its degree with Canadian Network for Mood and Anxiety Treatments (CANMAT).
Methods: A total of 3275 patients were recruited from 16 mental health centers and 16 general hospitals in China. Descriptive statistics presented the total number and percentage of drugs, as well as all kinds of treatments.
Results: Selective serotonin reuptake inhibitors (SSRIs) accounted for the largest proportion (57.2%), followed by serotonin-noradrenaline reuptake inhibitors (SNRIs) (22.8%) and mirtazapine (7.0%) in the first therapy, while that of SNRIs (53.9%) followed by SSRIs (39.2%) and mirtazapine (9.8%) in the follow-up therapy. An average of 1.85 medications was administered to each MDD patient.
Conclusion: SSRIs were the first choice in the first therapy, while the proportion of those drugs decreased during the follow-up therapy and were replaced by SNRIs. Plenty of combined pharmacotherapies were directly selected as the first trial of patients, which was inconsistent with guideline recommendations.
Keywords: major depressive disorder, Chinese, guideline, antidepressants
A successful treatment for major depressive disorder (MDD) depends on early diagnosis, proper treatment in time, and relieving symptoms. Antidepressants are acknowledged as the main treatment method for moderate to major depression during outpatient treatment. It is advocated that the second-generation antidepressants (SSRIs, SNRIs, NaSSA, and so on) are the first-line recommendations with high safety and promising efficacy.1 With a high failure rate of initial therapy, switching to another antidepressant is one of the alternative treatment strategies.2
With growing attention to evidence-based medicine in psychiatry, a number of clinical guidelines have been published. These guidelines were well-designed to help clinicians make the right clinical decisions. It is worth noticing that the CANMAT attracts compelling attention in China.3–5 Compared to the 2015 Guidelines for Prevention and Treatment of Depressive Disorder in China (PTDDC), second edition,6 the CANMAT guideline has been more widespread and updated. Furthermore, patients’ adherences to the CANMAT guideline recommendations are related to a greater remission in symptoms and improvement in outcomes of MDD.7 Moreover, PTDDC and CANMAT are highly consistent in the description of medications except for quetiapine or traditional Chinese medicine (TCM). Therefore, we compared both guidelines to the present medications of MDD for the convenience of domestic and foreign readers.
From a more macroscopic perspective, we need to know that the purpose of the guidelines initially informed mental healthcare provision in China.8 It should be more applicable to basic medical institutions such as community mental health services. Evidence-based graded recommendations for quality assurance in mental health were developed, which should next be implemented and evaluated for feasibility and validity in China. It would lead to the necessary investigation of the current status of medications in China since the feedback system has not been established yet.
The CANMAT guideline has three levels of recommendations. A first-line treatment recommendation indicates good-quality evidence (Meta-analysis with randomized controlled trials) as well as clinical utility. However, treatments with good-quality evidence may be downgraded to second- or third-line recommendations because of safety or side effect profiles.9
The National Survey on Symptomatology of Depression (NSSD) involved the commonly used antidepressants: selective serotonin reuptake inhibitors (SSRIs), serotonin-noradrenaline reuptake inhibitors (SNRIs), mirtazapine and bupropion, which were recommended as the first-line treatment strategy, as well as tricyclic antidepressants (TCAs), trazodone and quetiapine as the second-line recommendations, and monoamine oxidase inhibitors (MAOIs) as the third. Furthermore, antipsychotic and antidepressant cotreatment for MDD with psychotic features (Level 1) and benzodiazepines for clinical specifiers and dimensions of MDD with catatonic features (Level 3) are also recommended.9 Nowadays, the third-line treatment is rarely used in China because of some potential side effects and drug–drug interactions.10
There is evidence that greater provider adherence to guideline recommendations was associated with greater treatment effectiveness11 toward improving the outcome of the disease. However, China is a developing country with an expansive land, a large population, and an extremely uneven distribution of mental health resources or services.12 In particular, the development of psychiatry is relatively lagging behind. Therefore, this survey aims to explore the current status of MDD treatment in China to inform the decision-making and resource allocation policy in the future. Antidepressant treatment is supposed to be consistent with the guidelines. We already have two editions of the guidelines13 that are significantly influenced by the CANMAT. In this study, we tried to focus on the CANMAT concordance for the treatment of MDD in China.
Methods
Study Design
The NSSD was blueprinted to investigate the magnitude of symptoms across a widespread symptomatology14 within and outside the DSM framework and medical treatment of MDD with guidelines concordance. The data were constructed based on the following materials for decades (Chinese version).
(1) The diagnostic criteria derived from three diagnostic systems [DSM-IV /DSM-5, ICD-10, and the Chinese Classification of Mental Disorders, 3rd version (CCMD-3)].15 The DSM system has been widely accepted in clinical research fields in China for decades, while to some extent a formal psychiatric diagnosis cannot be made based on the ICD system. The ICD-10 is currently accepted in routine clinics in China according to insurance policies and medical regulations. The CCMD system had been abolished nearly a decade ago, and there was no major discrepancy in the diagnostic requirements of depression from the ICD system.16,17
(2) A variety of literatures examining the classic description of depression from Chinese textbooks and the clinical presentation of MDD represent Chinese psychiatric experts’ opinions about the important signs and symptoms of depression, as well as diagnosis and treatment guidelines with Chinese characteristics. We list commonly used medications recommended by the clinical guidelines. See Table 1.
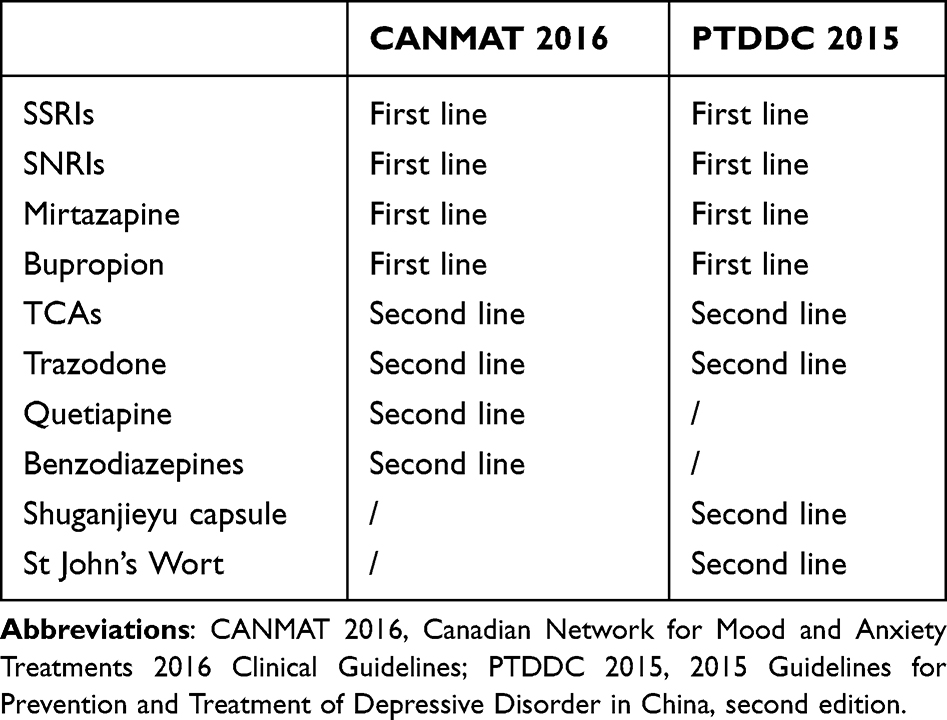 |
Table 1 Comparison of Recommendation Level Between CANMAT 2016 and PTDDC 2015 |
The study protocol was designed by team experts and a discussion group composed of 10 senior psychiatrists who have sophisticated expertise in psychiatric clinics and research on depression in China. Then the consensus was reached.
Settings and Participants
Participants’ data were consecutively collected from 16 mental health centers and psychiatric departments of 16 general hospitals within 22 cities of 15 provinces, across all 7 administrative regions (ie, East, Southwest, South, Northwest, North and Northeast China) of mainland China from 07/2014 to 02/2015. They are Beijing Anding Hospital, Peking University Sixth Hospital, Beijing Huilongguan Hospital, Beijing Chaoyang Hospital, Shanghai Mental Health Center, Shanghai Jinshan Health Center, Shanghai Ruijin Hospital, Shanghai Tenth People’s Hospital, Zhejiang Provincial Tongde Hospital, Changshu Third People’s Hospital, No. 102 Hospital of People’s Liberation Army, the Seventh People’s Hospital of Dalian, Guangzhou Brain Hospital, the Third People’s Hospital of Huzhou, Nanjing Brain Hospital, Mental Health Center of Shantou University, Shenzhen Kangning Hospital, Suzhou Guangji Hospital, the Third People’s Hospital of Taicang, Jiangsu Provincial People’s Hospital, West China Hospital of Sichuan University, Guangdong Provincial People’s Hospital, Tianjin Medical University General Hospital, the First Affiliated Hospital of Harbin Medical University, Hubei Provincial People’s Hospital, the First Affiliated Hospital of Kunming Medical University, the First Hospital of Shanxi Medical University, First Affiliated Hospital of China Medical University, the Second Affiliated Hospital Zhejiang University, the Second Xiangya Hospital of Central South University, Xijing Hospital and Nanjing Drum Tower Hospital. The institutional review boards at each site approved the study. This study was approved by the Institutional Ethical Committee for Clinical Research of Shanghai Mental Health Center (2012BAI01B04), Shanghai, China. The research evaluators at each multicenter had undergone consistency training for this clinical investigation. Besides, all participants provided written informed consent prior to research entry according to the Declaration of Helsinki after the treatment had been chosen.
Inclusion and Exclusion Criteria
Participants aged ≥18 years old, currently under a major depressive episode, who were seeking care in inpatient or outpatient psychiatric departments, received screening interviews by trained research evaluators. Those who met DSM-IV TR criteria for the current episode of MDD would be eligible for inclusion as decided by a research psychiatrist. Overall exclusion criteria included (1) an imminent risk for suicide or homicide; (2) a lifetime diagnosis of bipolar disorder; (3) female patients during pregnancy or postpartum period; or (4) reception of modified electroconvulsive therapy within a month prior to study entry.
Variables
We divided the participants’ data into the first visit patient group and the follow-up visit patient group. First-visit patients were recorded only once, whereas follow-up patients provided medication data and information for their first therapy and current therapy. The demographic information of recruited patients was collected with a self-designed case report form including age, gender, education level, number of episodes, treatment-resistant depression, marital status, vocational status, patient setting, and ethnicity.
Statistical Analyses
Statistical analyses were performed with SPSS version 17.0. Descriptive statistics include total and percentage of medicine use, as well as drug types. Skewed distribution data were represented by median (IQR).
Results
Sociodemographic Factors and Clinical Characteristics of the MDD Patients
A total of 3516 patients who suffered from significant depressive symptoms or a depressive episode were prescreened. After the clinical screening, 241 patients did not meet the criteria for a current major depressive episode or did not finish the assessment. Finally, 3275 patients finished the study and were collected in the present analysis except for six missing records in the statistics. See Table 2.
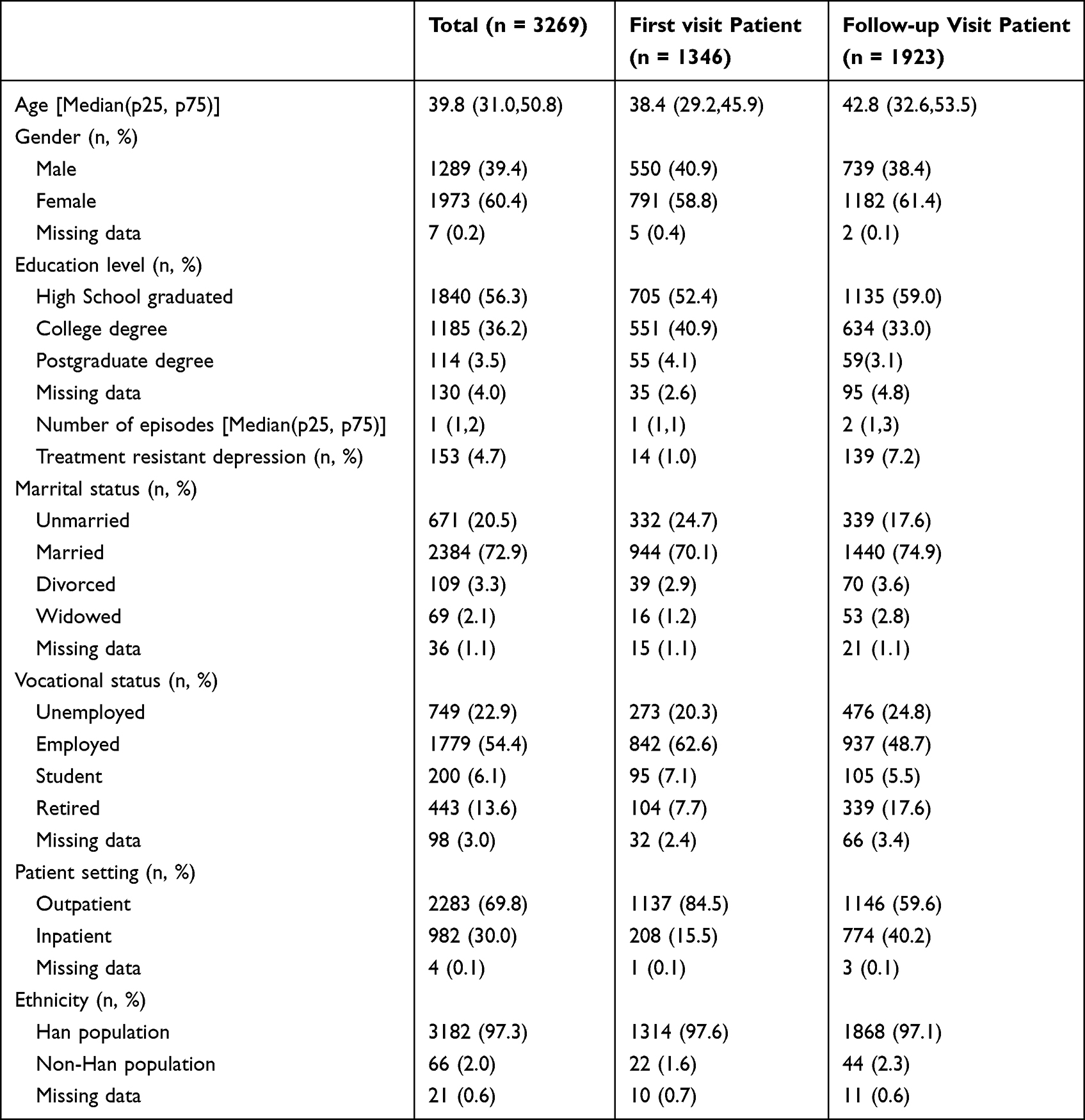 |
Table 2 Demographic and Clinical Information of the MDD Patients (n = 3269) |
Comparison of the Current Status of Antidepressant Treatment Between First Therapy and Follow-Up Therapy Groups in 32 Centers
For the patients with switching treatment, the total course was 3.42 (±4.56) months. In the first-line recommendations, SSRIs accounted for the largest proportion (57.2%), followed by SNRIs (22.8%) and mirtazapine (7.0%) in the first therapy, while in the follow-up therapy the proportion were SNRIs (53.9%) followed by SSRIs (39.2%) and mirtazapine (9.8%). In the second-line recommendations, TCAs accounted for the largest proportion (3.6%), followed by trazodone (1.6%) in the first therapy, while those of trazodone (1.7%) followed by TCAs (0.5%) in the follow-up therapy. The rate of benzodiazepines was lower in the first therapy group than in the follow-up therapy group (19.0% vs 52.0%).
Within the TCM recommended by the Chinese Guidelines, the total use of Shuganjieyu capsules (0.3% vs 0.2%) or St John’s Wort was few (0.1% vs 0.1%).
On the “without recommendations” list, compared to the first therapy, the total use of flupentixol and melitracen tablets (2.5% vs 1.1%) decreased in the follow-up therapy, while the use of antipsychotics (0.6% vs 17.2%) and mood stabilizers (0.1% vs 6.9%) increased.
The results also showed that SSRIs accounted for 57.2% (1099/1923) of first prescriptions for follow-up patients, while SSRIs accounted for 36.3% (489/1346) of first therapy among follow-up patients. Benzodiazepines accounted for 1.6% of first therapy among follow-up patients (n = 1923), but 46.1% (620/1346) among first-visit patients (n = 1346). See Table 3.
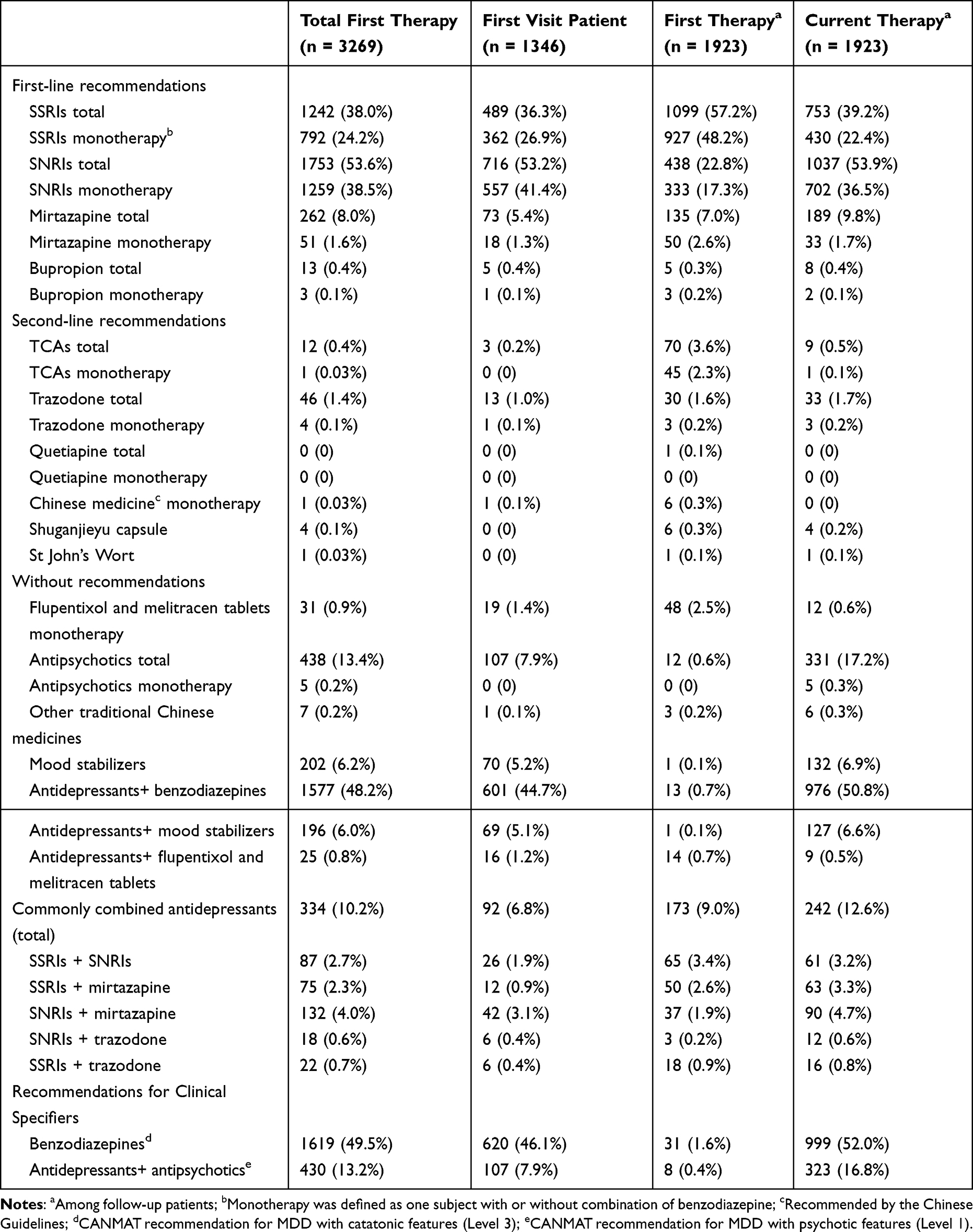 |
Table 3 Current Status of Antidepressant Treatment and Common Combined Antidepressants in 32 Centers |
When the 1346 first visitors were not accounted in the first therapy group (Table 2), 1923 patients with their first visit and follow-up visit of treatment remained. A paired-sample design was conducted. In the first-line recommendations, SSRIs still accounted for the largest proportion (1099/1923, 57.2%), followed by SNRIs (438/1923, 22.8%) and mirtazapine (135/1923, 7.0%) compared to themselves of the proportion of SSRIs (753/1923, 39.2%), SNRIs (1037/1923, 53.9%) and mirtazapine (189/1923, 9.8%) in the follow-up therapy. In the second-line recommendations, TCAs accounted for the largest proportion (70/1923, 3.6%) followed by trazodone (30/1923, 1.6%) compared to themselves of TCAs (9/1923, 0.5%) and trazodone (33/1923, 1.7%). See Figure 1.
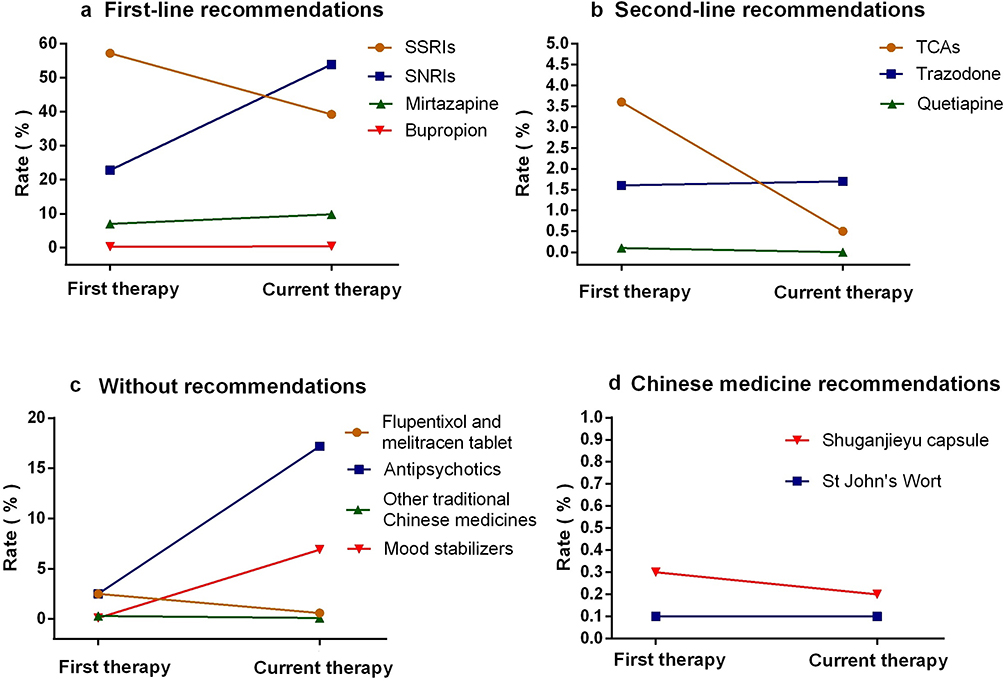 |
Figure 1 Line chart of switching antidepressants in their first visit and follow-up visit of treatment (n = 1923). The sub-figures respectively show the first-line recommendations (a), the second-line recommendations (b) and the “without recommendations” list (c) by CANMAT 2016 and the Chinese medicine recommendations (d) by PTDDC 2015. |
Comparison of Commonly Combined Antidepressants Between First Therapy and Follow-Up Therapy Groups in 32 Centers
The rate of common antidepressant combinations in the first therapy was lower than that in the follow-up therapy (9% vs 12.6%), higher than that in the first-visit patient group (6.8%). See Table 3.
Moreover, we calculated the kind(s) of antidepressants (SSRIs, SNRIs, mirtazapine, bupropion, TCAs, and trazodone) used in MDD treatment. An average of 1.85 medications was administered to each MDD patient, 7% accepted psychotherapy, while the use of more than one drug reached up to 62.9% (49.5% for two medications, and 13.5% for more than two medications). See Figure 2.
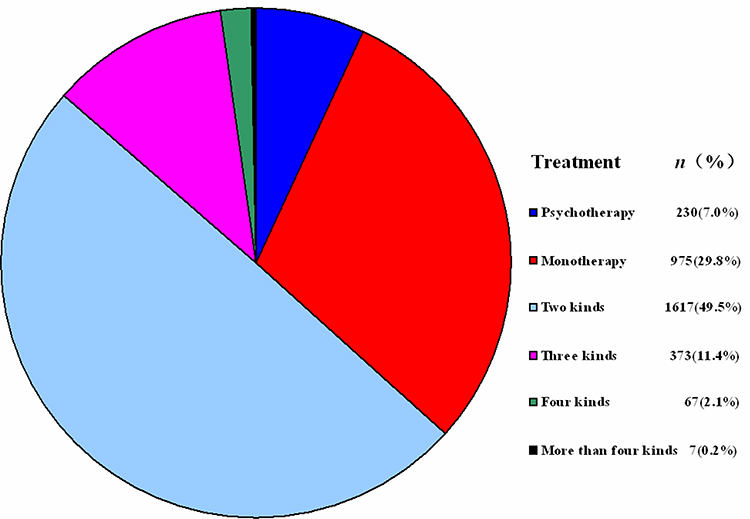 |
Figure 2 Statistics of psychotherapy or kind(s) of pharmacotherapy (n = 3269). |
Discussions
Through this survey, the proportion of SSRIs (57.2%) were the first choice in the first therapy, while the proportion of those drugs decreased during the follow-up therapy, which was replaced by SNRIs (53.9%), suggesting that SNRIs were the most considered alternative drugs. Antidepressant switching is also one of the alternative treatment strategies adopted in MDD patients who have no remission despite the adequate trial of antidepressant(s).2 We endorse this kind of opinion that follows the evidence-based support by the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial, because the results indicate that a switch to sertraline is a cost-effectiveness treatment option, comparing with a switch to venlafaxine in MDD patients after unsuccessful treatment with citalopram for economic evaluation.2 Nevertheless, the switch options of bupropion, sertraline, and venlafaxine were not significantly different from each other in terms of cost-effectiveness.18 The actual difference of using conditions could be variations of drug prices in different countries due to the self-regulation of pharmaceutical industry.19 From the perspective of pharmacology, the switch to a different mechanism of antidepressants would contribute to affecting different signs and symptoms.20,21 This variation strategy may provide more chances of cure22 when comparing the effects of sertraline with duloxetine,23 rather than those of venlafaxine with escitalopram.22 In the first-line recommendations, the prescription of bupropion was surprisingly low, even lower than the second-line recommendations except for quetiapine. Efforts remain to be made to promote the coverage of bupropion in China from the aspects of efficiency and security.24 On the opposite, obsolete knowledge is another phenomenon. We found in the statistics that many hospitals still adhere to compound preparations such as flupentixol and melitracen tablets (1.7%, total) in that the efficacy was exhibited in MDD patients accompanied with chronic somatic diseases.25 The flupentixol/melitracen combination was used to be the most frequently prescribed compounds in China.26 However, in the current developed process of atypical antipsychotics and second-generation antidepressants, we can see the trend that this type of drug has been phased out for decades due to the irrational fixed-dose combination,27 which has been prohibited for sale or use in many countries. There are many regions in China where knowledge dissemination mainly depends on the succession of teachings from a master to his disciples. Although many treatment strategies are out-of-date, it is common for people to adhere to the Confucian principle of “honoring the teacher and respecting his teachings” rather than evidence-based medicine.
The gap between 57.2% of first SSRI prescriptions for follow-up patients and 36.3% of first-visit patients may come from many first-visit patients who record their medical history from the beginning of taking medicine. It takes a while of adaptation for patients to establish treatment compliance at outpatient clinic.28 Moreover, MDD patients who tend to seek medical help from general hospitals29 were more likely to suffer from urinary system complaints, headache, sensory system complaints, trunk pain, and nervous system complaints.14 These symptoms were likely to be prescribed benzodiazepines or medications for treating physical illnesses, instead of antidepressant by physicians. After a follow-up referral to a psychiatric specialist, the phenomena of seeking rapid relief were adjusted within a reasonable range. The onset of MDD will be probably defined when they come to a psychiatric hospital. That may explain why so many first benzodiazepine prescriptions were not accounted for follow-up patients. CANMAT recommends for MDD with catatonic features, but benzodiazepine use is very common (49.5%) in China, obviously not for catatonic features.
Compared with the CANMAT guideline, drug uses without recommendations were observed in our survey. The commonly combined pharmacotherapy was directly selected for the first treatment (9%), while antipsychotics (17.2%) and mood stabilizers (6.9%) adjunctive therapy to antidepressant therapy was increased in the follow-up treatment. In the cross-sectional study, the use of two or more drugs reached up to 62.9%, so the prescription of multiple antidepressants is still a common problem, especially in East Asia.30 This trend may result from consideration for a synergistic effect of antipsychotics in the treatment of MDD,31 but the combined pharmacotherapy also increases the risk of side effects caused by psychotropic medications.32 Drug–drug interactions and clinical considerations should be adequately integrated to construct a co-administration of medical therapy.33,34 For the reason above, the antipsychotics (except for quetiapine) and mood stabilizers are inconsistent with the CANMAT guideline.9,35 Meanwhile, we have also noticed that lithium, as a classic mood stabilizer, would likely to be inappropriate for patients with a partial response to the first antidepressant trial. However, if the patient has failed several treatment strategies, lithium would be recommended for adjunctive medication for nonresponse or partial response to an antidepressant in the CANMAT guideline.9
Polypharmacy is a worldwide issue in psychiatry.36 Our study calculated the clinical prescriptions of psychiatry in 32 centers. In the cross-sectional study, an average of 1.85 medications were administered to each MDD patient, while those taking two or more medications reached up to 62.9%. Polypharmacy leads to many disadvantages for patients with MDD. Polypharmacy treatment not only increases the incidence and severity of side effects, but also increases the burden of treatment costs.37 According to Healthy People 2020, prescription of multiple medications is the No. 1 drug safety priority to Americans’ aging population, in which the proportion of Asian Americans was 48%.38 The main reason may be an inadequate understanding of pharmacodynamics and pharmacokinetics of commonly used psychiatric medications. We found these problems in their records, including an irrational fixed-dose combination (flupentixol and melitracen tablets), antipsychotics (eg, a low dose of olanzapine, perphenazine, clozapine or chlorpromazine), and a mood stabilizer (eg, lithium or valproate) compared with the CANMAT guideline. Furthermore, some irrationally combined uses of drugs were prescribed in the follow-up therapy, such as SSRIs with SNRIs or SNRIs with mirtazapine.39 SSRIs or SNRIs are first-line pharmacotherapies for MDD, which inhibit many common cytochrome enzymes,40 so they may have drug interactions. Because more than half of the patients with MDD starting treatment did not remit after an adequate trial with the first agent, they will need a second-line therapy.41 Therapeutic alliance always prefers drug combinations rather than switch the existing ineffective medication(s), which made the rate of drug combination increase from 7% to 12.6% in MDD patients who returned to those psychiatric departments. This phenomenon needs more than a theoretical discussion of the psychopharmacological effects of the drug combination. Instead, there needs to be high-quality clinical research in China to investigate this phenomenon, which is supposed to be converted into guidelines.
In addition, we found that unrealistic treatment expectations might exist in this survey, leading a therapeutic alliance to prefer “good drugs” (such as newly imported antidepressants), “strong drugs” (such as antipsychotics as a synergistic agent), “fast drugs” (such as benzodiazepines) or “TCM” [Following the principles of “Monarch”, “Minister”, “Assistant”, and “Guide” (君臣佐使)].37 A 10-years cohort study showed that patients with MDD starting treatment might be expected to spend three-quarters of the next decade in euthymia, and the remaining period in subthreshold or threshold depression.42 Nowadays in China, patients and their guardians are unwilling to wait for the gradual improvements afforded by most antidepressants,37 so doctor-patient alliance should make efforts to reach a rational agreement on their following treatment compliance, especially when the doctor has not prepared them for the slow onset of treatment effects.38
Additionally, the dominant position of a psychiatrist may increase the dosage and type of medication. Indeed, patients’ lack of relevant knowledge leaves their psychiatrists dominate the negotiations about treatment. The use of psychotropic medications can be an unintended (or intended) method of increasing patient compliance.37 Urgent need for improving mental health care should be a more collaborative model instead of the current psychiatrists’ dominant position. This issue is acute in psychiatry because of its relatively subjective judgment and slow development in comparison with that of other medical specialties.
TCM has a distinctly Chinese characteristic with its theoretical rationality. Shuganjieyu capsule and St. John’s Worts (called Hypericum monogynum in China) were recommended to be used in mild-to-moderate depression by evidence-based supports43,44 according to the Chinese guideline, while the CANMAT guideline for complementary and alternative medicine treatments indicated St. John’s wort as a second-line recommendation for moderate to severe MDD,45 so we put them into the consideration of our study. However, it was also found in the study that some TCM with the formula of “君臣佐使” failed to be collected due to a large number of drug materials. Therefore, to some extent, TCM has also increased the use of medications, and it still has a long way to attend further from a transnational perspective to the innovations of this period, as well as to be approved and recommended by international guidelines in the future.46
Limitations
The real-world antidepressant combinations may be less than what we calculated within our research data, for as many of these may have been “combined” during a cross-titration (eg, switching an SSRI to SNRI) with no intention of dual SSRI-SNRI therapy. Furthermore, many patients may have previously been treated with antidepressants. As a real-world practice, first therapy cannot be equal to the real “first”, which depends on their accurate medical history provided.
Acknowledgment
The authors would like to acknowledge and thank all the participants in this study and all the members of the NSSD team. The authors also thank Lu Yang for proofreading the final edition.
Funding
The National Key Research and Development Program of China (2016YFC1307100), the National Natural Science Foundation of China (91232719, 81771465, 81930033), Shanghai Key Medicine Specialties Program (ZK2019A06), Shanghai Clinical Research Center for Mental Health (SCRC-MH, 19MC1911100), the Scientific Research Project of Hongkou District Health Commission (2101-03) and Excellent Talent Training Program of Shanghai Hongkou Mental Health Center (2023XKDTR01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kato T, Furukawa TA, Mantani A, et al. Optimising first- and second-line treatment strategies for untreated major depressive disorder - The SUND study: a pragmatic, multi-centre, assessor-blinded randomised controlled trial. BMC Med. 2018;16(1):103.
2. Leelahanaj T. Switching to sertraline or venlafaxine after failure of SSRIs treatment in major depressive disorder: an economic evaluation of the STAR*D trial. J Med Assoc Thai. 2012;95(5):S29–37.
3. Wang Z, Gao K, Hong W, et al. Pharmacotherapy for acute mania and disconcordance with treatment guidelines: bipolar mania pathway survey (BIPAS) in mainland China. BMC Psychiatry. 2014;14(167):167.
4. Wang Z, Gao K, Hong W, et al. Guidelines disconcordance in acute bipolar depression: data from the national Bipolar Mania Pathway Survey (BIPAS) in mainland China. PLoS One. 2014;9(4):e96096.
5. Wang Z, Chen J, Zhang C, et al. Guidelines concordance of maintenance treatment in euthymic patients with bipolar disorder: data from the national bipolar mania pathway survey (BIPAS) in mainland China. J Affect Disord. 2015;182:101–105.
6. Niu YJ. Interpretation of drug therapy of Chinese Guidelines for Prevention and Treatment of Depression. Clin Med J. 2018;16(5):6–8.
7. Kennedy SH, Lam RW, Cohen NL, Ravindran AV. Clinical guidelines for the treatment of depressive disorders. IV. Medications and other biological treatments. Can J Psychiatry. 2001;46(1):38S–58S.
8. Docherty M, Shaw K, Goulding L, et al. Evidence-based guideline implementation in low and middle income countries: lessons for mental health care. Int J Ment Health Syst. 2017;11:8.
9. Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: section 3. Pharmacological Treatments. Can J Psychiatry. 2016;61(9):540–560.
10. Tripathi AC, Upadhyay S, Paliwal S, Saraf SK. Privileged scaffolds as MAO inhibitors: retrospect and prospects. Eur J Med Chem. 2018;145:445–497.
11. Rosenblat JD, Simon GE, Sachs GS, et al. Treatment effectiveness and tolerability outcomes that are most important to individuals with bipolar and unipolar depression. J Affect Disord. 2018;243:116–120.
12. Patel V, Xiao S, Chen H, et al. The magnitude of and health system responses to the mental health treatment gap in adults in India and China. Lancet. 2016;388(10063):3074–3084.
13. Zhang M. Major depressive disorder treatment guidelines in China. J Clin Psychiatry. 2010;71(Suppl E1):e06.
14. Zhao D, Wu Z, Zhang H, et al. Somatic symptoms vary in major depressive disorder in China. Compr Psychiatry. 2018;87:32–37.
15. Chen YF. Chinese classification of mental disorders (CCMD-3): towards integration in international classification. Psychopathology. 2002;35(2–3):171–175.
16. Lee DT, Kleinman J, Kleinman A. Rethinking depression: an ethnographic study of the experiences of depression among Chinese. Harv Rev Psychiatry. 2007;15(1):1–8.
17. Parker G, Gladstone G, Chee KT. Depression in the planet’s largest ethnic group: the Chinese. Am J Psychiatry. 2001;158(6):857–864.
18. Singh A, Brooks MM, Voorhees RE, et al. Cost-Effective Drug Switch Options After Unsuccessful Treatment With an SSRI for Depression. Psychiatr Serv. 2017;68(1):81–87.
19. Zetterqvist AV, Mulinari S. Misleading advertising for antidepressants in Sweden: a failure of pharmaceutical industry self-regulation. PLoS One. 2013;8(5):e62609.
20. Zhu Y, Ji H, Niu Z, et al. Biochemical and Endocrine Parameters for the Discrimination and Calibration of Bipolar Disorder or Major Depressive Disorder. Front Psychiatry. 2022;13:875141.
21. Zhu Y, Wu X, Liu H, et al. Employing biochemical biomarkers for building decision tree models to predict bipolar disorder from major depressive disorder. J Affect Disord. 2022;308:190–198.
22. Jaracz J, Gattner K, Jaracz K, Gorna K, Moczko J, Hauser J. Is Venlafaxine More Effective than Escitalopram and Nortriptyline in the Management of Painful Symptoms in Patients with Major Depression? Pharmacopsychiatry. 2018;51(4):148–152.
23. Mowla A, Dastgheib SA, RazeghianJahromi L. Comparing the Effects of Sertraline with Duloxetine for Depression Severity and Symptoms: a Double-Blind, Randomized Controlled Trial. Clin Drug Investig. 2016;36(7):539–543.
24. Zhang F, Li Y, Hu J, Zhong J, Population Pharmacokinetics LH. Safety and Tolerability of Extended-Release Bupropion and Its Three Metabolites in Chinese Healthy Volunteers. Eur J Drug MetabPharmacokinet. 2019;44(3):339–352.
25. Wang L, Zhong Z, Hu J, et al. Sertraline plus deanxit to treat patients with depression and anxiety in chronic somatic diseases: a randomized controlled trial. BMC Psychiatry. 2015;15:84.
26. Zhang Y, Becker T, Kosters M. Preliminary study of patterns of medication use for depression treatment in China. Asia Pac Psychiatry. 2013;5(4):231–236.
27. Solanki MS, Banwari G. Irrational fixed dose combinations of psychotropic drugs in India: cause of concern. Indian J Pharmacol. 2016;48(4):468–469.
28. Zhu Y, Wu Z, Sie O, et al. Causes of drug discontinuation in patients with major depressive disorder in China. Prog Neuropsychopharmacol Biol Psychiatry. 2020;96:109755.
29. Cui L, Wang C, Wu Z, et al. Symptomatology differences of major depression in psychiatric versus general hospitals: a machine learning approach. J Affect Disord. 2020;260:349–360.
30. Huang CY, Yang SY, Mojtabai R, et al. Trends of Polypharmacy and Prescription Patterns of Antidepressants in Asia. J Clin Psychopharmacol. 2018;38(6):598–603.
31. Han C, Wang SM, Kato M, et al. Second-generation antipsychotics in the treatment of major depressive disorder: current evidence. Expert Rev Neurother. 2013;13(7):851–870.
32. O’Brien H, Kiely F, Barry A, Meaney S. Cross-sectional examination of extrapyramidal side effects in a specialist palliative care inpatient unit. BMJ Support Palliat Care. 2018;9(3):271–273.
33. Corponi F, Fabbri C, Serretti A. Pharmacogenetics in Psychiatry. Adv Pharmacol. 2018;83:297–331.
34. Zhu Y, Wu X, Zhou R, et al. Hypothalamic-Pituitary-End-Organ Axes: hormone Function in Female Patients with Major Depressive Disorder. Neurosci Bull. 2021;37(8):1176–1187.
35. Komossa K, Depping AM, Gaudchau A, Kissling W, Leucht S. Second-generation antipsychotics for major depressive disorder and dysthymia. Cochrane Database Syst Rev. 2010;8(12):CD008121.
36. Qiu H, He Y, Zhang Y, et al. Antipsychotic polypharmacy in the treatment of schizophrenia in China and Japan. Aust N Z J Psychiatry. 2018;52(12):1202–1212.
37. Xu Y. ‘Less is more’ in the Chinese context. Shanghai Arch Psychiatry. 2015;27(6):371–373.
38. Karter AJ, Laiteerapong N, Chin MH, et al. Ethnic Differences in Geriatric Conditions and Diabetes Complications Among Older, Insured Adults With Diabetes: the Diabetes and Aging Study. J Aging Health. 2015;27(5):894–918.
39. Yang L, Su Y, Dong S, et al. Concordance of the treatment patterns for major depressive disorders between the Canadian Network for Mood and Anxiety Treatments (CANMAT) algorithm and real-world practice in China. Front Pharmacol. 2022;13:954973.
40. Cazet L, Bulteau S, Evin A, et al. Interaction between CYP2D6 inhibitor antidepressants and codeine: is this relevant? Expert Opin Drug MetabToxicol. 2018;14(8):879–886.
41. Yonemoto N, Tanaka S, Furukawa TA, et al. Strategic use of new generation antidepressants for depression: SUN(^_^) D protocol update and statistical analysis plan. Trials. 2015;16:459.
42. Furukawa TA, Yoshimura R, Harai H, et al. How many well vs. unwell days can you expect over 10 years, once you become depressed? Acta Psychiatr Scand. 2009;119(4):290–297.
43. Feng DD, Tang T, Lin XP, et al. Nine traditional Chinese herbal formulas for the treatment of depression: an ethnopharmacology, phytochemistry, and pharmacology review. Neuropsychiatr Dis Treat. 2016;12:2387–2402.
44. Ng QX, Venkatanarayanan N, Ho CY. Clinical use of Hypericum perforatum (St John’s wort) in depression: a meta-analysis. J Affect Disord. 2017;210:211–221.
45. Ravindran AV, Balneaves LG, Faulkner G, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: section 5. Complementary and Alternative Medicine Treatments. Can J Psychiatry. 2016;61(9):576–587.
46. Scheid V. Transmitting Chinese Medicine: changing Perceptions of Body, Pathology, and Treatment in Late Imperial China. Asian Med. 2013;8(2):299–360.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.