Back to Journals » Infection and Drug Resistance » Volume 17
Clinical Features and Prognostic Predictors in Patients with Renal Transplant Complicated by SARS-CoV-2 Infection, a Retrospective Single-Center Study
Received 25 February 2024
Accepted for publication 16 May 2024
Published 20 May 2024 Volume 2024:17 Pages 1999—2007
DOI https://doi.org/10.2147/IDR.S465805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yinfeng Wang, Xiaogen Tao, Peng Jin
Department of Intensive Care Unit, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China
Correspondence: Xiaogen Tao; Peng Jin, Department of Intensive Care Unit, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, 230001, Anhui, People’s Republic of China, Email [email protected]; [email protected]
Background: This study examines the clinical outcomes and prognostic factors of COVID-19 in renal transplant recipients. Given their immunosuppressed status, these patients are at higher risk of severe complications from COVID-19. The study aims to provide healthcare professionals with critical insights for diagnosing and managing this vulnerable population.
Patients and methods: This retrospective cohort study included adult renal transplant recipients diagnosed with COVID-19. Data on demographics, medical history, laboratory results, and patient outcomes were analyzed to identify clinical characteristics and prognostic factors.
Results: This study included 115 renal transplant recipients with COVID-19, predominantly male, with a mortality rate of 10.4% (12 deaths). The overall vaccination rate was 20%. Univariate analysis showed significant differences between survivors and non-survivors in initial serum creatinine levels, and percentages of neutrophils, monocytes, and lymphocytes, along with CRP levels on day 3. Additionally, CRP levels, hemoglobin, and platelet counts on day 7 also differed significantly. Multivariate analysis identified CRP levels on days 3 and 7, day 7 hemoglobin and platelet counts, and concurrent bacterial infections as independent risk factors for mortality.
Conclusion: Elevated CRP levels, renal impairment, and bacterial co-infections play a significant role in the outcomes of COVID-19 in kidney transplant recipients. This study highlights the importance of monitoring these factors for early identification and management of high-risk patients.
Keywords: COVID-19, renal transplant recipients, clinical outcomes, prognostic factors, immunosuppression
Introduction
Since its emergence in late 2019, Coronavirus disease 2019 (COVID-19) has rapidly evolved into a global pandemic, affecting millions worldwide. As of February 2023, over 671.6 million cases and 6.8 million fatalities have been officially reported, underscoring the virus’s devastating impact.1 COVID-19 primarily manifests as a respiratory tract infection, with clinical presentations varying from mild, flu-like symptoms to severe acute respiratory distress syndrome (ARDS).2 Extensive research identifies key risk factors for severe COVID-19 outcomes, including advanced age, obesity, diabetes mellitus, chronic pulmonary conditions, cardiovascular diseases, malignancies, and compromised immune systems.3,4 Notably, immunosuppressed states, particularly those in solid organ transplant recipients, are associated with the highest risk of severe complications.5,6 Intriguingly, some studies suggest that diminished inflammatory responses, attributed to weakened immune systems, may confer a degree of protection against severe manifestations of COVID-19.7,8 Consequently, the clinical characteristics and prognoses of COVID-19 in immunocompromised individuals, especially those who have undergone solid organ transplants, warrant thorough investigation.
Renal transplantation stands as the preferred treatment for individuals with end-stage renal disease, reflecting a global increase in such procedures. In 2021, the Global Observatory on Donation and Transplantation reported a significant milestone with over 92,500 renal transplants performed, a testament to the advancements in transplantation medicine and the advent of novel immunosuppressive medications.9 Although these therapies are pivotal in mitigating organ rejection, they simultaneously heighten the susceptibility to viral, bacterial, and fungal infections among transplant recipients.10 Moreover, the administration of immunosuppressive therapy has been independently associated with an adverse prognosis in a spectrum of infections.11,12 Recent studies have underscored the importance of various prognostic markers in predicting COVID-19 outcomes among immunocompromised populations. Elevated levels of inflammatory markers such as C-reactive protein (CRP) and interleukin-6 (IL-6), along with diminished lymphocyte counts, have been consistently associated with worse outcomes in these patients.13,14
Consequently, we conducted a retrospective analysis of clinical manifestations, imaging data, laboratory results, and patient outcomes among individuals who contracted COVID-19 post-renal transplantation at our institution during the pandemic. Our objective was to delineate the clinical characteristics and prognostic factors pertinent to diagnosing and managing SARS-CoV-2 pneumonia in the post-transplantation setting. By doing so, we aim to furnish healthcare professionals with critical insights that could guide the diagnostic and therapeutic strategies for this vulnerable population.
Methods
Study Design and Participants
This retrospective cohort study was conducted at the First Affiliated Hospital of the University of Science and Technology of China in Hefei, Anhui Province, China. We included adult patients (aged ≥18 years) who had undergone renal transplantation and were subsequently diagnosed with COVID-19 between November 2022 and February 2023. COVID-19 was confirmed by RT-PCR testing of nasal or pharyngeal swab specimens.
Ethical Considerations
This study was approved by the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (2023-RE-149). Due to its retrospective nature, the requirement for informed consent was waived. However, all patient information was anonymized and de-identified prior to analysis to protect patient privacy and comply with ethical standards. All kidneys were donated voluntarily with written informed consent, and this process was conducted in accordance with the Declaration of Istanbul.
Inclusion and Exclusion Criteria
Inclusion criteria: Adults who had received kidney transplants and had a confirmed diagnosis of COVID-19 post-transplantation.
Exclusion criteria: Patients without complete medical records, those who had severe organ failure prior to COVID-19 infection not related to the transplantation, and individuals participating in other clinical trials that could influence the outcome of this study.
Data Collection
Data were collected on demographics (age, gender, BMI), medical history (comorbid conditions), timing of renal transplantation, types of oral immunosuppressive medications, and laboratory findings at various time points post-admission. These included complete blood count, neutrophil-to-lymphocyte ratio, absolute lymphocyte count, absolute monocyte count, eosinophil count, hemoglobin, platelet count, infection markers (C-reactive protein, procalcitonin), nutritional status indicators (albumin, prealbumin, globulin), renal function markers (creatinine, cystatin C), and coagulation-related indicators (D-dimer, fibrinogen, prothrombin time). Information on concurrent bacterial infections, ICU admissions, invasive mechanical ventilation.
Treatment Measures
Treatment for COVID-19 included antiviral therapy as per health authorities and hospital guidelines at the time, supportive care (fluid replacement, electrolyte balancing, nutritional support), and symptomatic treatment based on clinical presentation. Severe cases received intensive care, including invasive or non-invasive mechanical ventilation as necessary.
Adjustments to immunosuppressive therapy post-COVID-19 infection were made based on the patient’s clinical status and immune response, including dose reduction or temporary cessation of certain medications. The adjustment strategy was personalized, considering the patient’s renal function, the severity of infection, and the characteristics of the immunosuppressive drugs.
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics, clinical features, and outcomes. Continuous variables were presented as means ± standard deviations or medians with interquartile ranges, and categorical variables as frequencies and percentages. Comparative analyses were performed using Chi-square or Fisher’s exact tests for categorical variables and Student’s t-test or Mann–Whitney U-test for continuous variables. Multivariable logistic regression analysis was employed to identify independent predictors of mortality, reporting odds ratios with 95% confidence intervals. A p-value <0.05 was considered statistically significant. Statistical analyses were conducted using (SPSS Version 26).
Results
Our single-center retrospective study meticulously dissected the clinical trajectories of kidney transplant recipients affected by COVID-19, aiming to illuminate the clinical characteristics and determinants of mortality within this vulnerable cohort. The study encompassed a total of 115 patients, with a demarcation into survivors (103) and non-survivors (12), enabling a granular analysis of demographic data, clinical presentations, and laboratory markers.
Baseline Characteristics of Patients Infected with Covid-19 After Kidney Transplantation
The cohort was predominantly male, with 92 out of 115 participants (80%) being male. This included 81 males (78.6%) in the survival group and 11 males (91.7%) in the non-survival group. The age range of the participants was between 23 and 63 years, with a mean age of 41 years. There was no statistically significant difference in age between the survival and non-survival groups (P=0.989). Regarding gender distribution, as mentioned, males constituted the majority of the study population, comprising 80% of the cases. The survival group had a slightly lower percentage of males (78.6%) compared to the non-survival group (91.7%), though this difference was not statistically significant. The Body Mass Index (BMI) of participants also showed no significant difference between the two groups, with values of 22.68±3.12 in the survival group versus 22.55±3.25 in the non-survival group (P=0.886). This indicates that BMI was not a discriminating factor for survival outcomes in this cohort. The average time from renal transplantation to COVID-19 infection was 49 months, with no significant difference observed between the survival (49.78±45.82 months) and non-survival groups (44.64±42.14 months, P=0.612). This suggests that the duration since transplantation did not significantly impact the likelihood of survival post-COVID-19 infection. Comorbidities were common among participants. In the survival group, hypertension was present in 53 patients (52.5%), and diabetes in 17 patients (16.5%). The non-survival group had a higher proportion of patients with hypertension (58.3%) and diabetes (41.7%), indicating a trend towards more severe comorbid conditions in those who did not survive, although the small sample size warrants caution in interpretation. Vaccination status showed that out of the total participants, 23 patients (20%) had received at least one dose of a COVID-19 vaccine. Within this subset, the survival group included 19 vaccinated individuals (18.4%), whereas the non-survival group had 4 (33.3%). This data suggests a potential impact of vaccination on survival, though the differences were not statistically analyzed for significance. Out of the 115 patients, 9 received kidneys from deceased donors. Specifically, 8 patients in the survival group and 1 patient in the non-survival group had kidneys from deceased donors. Upon statistical review, we did not uncover any significant differences in outcomes between these two groups. Table 1 shows the demographic characteristics the patients.
 |
Table 1 Patients’ Demographic Characteristics |
Laboratory Results During Hospitalization
The laboratory results of the study participants upon admission, and at 3 and 7 days post-admission, reveal several key findings: Initially, there was no significant difference in leucocyte counts between survivors and non-survivors. However, neutrophil percentages were significantly higher in survivors by day 3 (p<0.001), indicating a potentially stronger innate immune response. The lymphocyte percentage, inversely related to outcomes, was lower in non-survivors by day 7 (p<0.001), suggesting that lymphopenia could be associated with worse outcomes. Serum C-reactive protein (CRP) levels were significantly higher in non-survivors by day 3 and continued to rise, highlighting inflammation’s role in severity. Similarly, procalcitonin (PCT) levels were elevated in non-survivors, pointing to bacterial co-infections or a severe systemic response. Serum creatinine levels were significantly higher in non-survivors (p=0.003), indicating renal impairment or failure as a critical factor in mortality. Hemoglobin levels and platelet counts, though initially not significantly different, showed disparities by day 7, with non-survivors experiencing worsening anemia and thrombocytopenia. A significant increase in combined bacterial infections was observed in non-survivors during hospitalization (21 cases, 18.3% overall, p<0.001), suggesting a correlation between secondary infections and increased mortality risk. Out of the total cohort, there was one case of bloodstream infection in the non-survivor group, which was a concurrent bacterial infection that contributed to the patient’s demise due to septic shock. Table 2 shows the laboratory results during hospitalization.
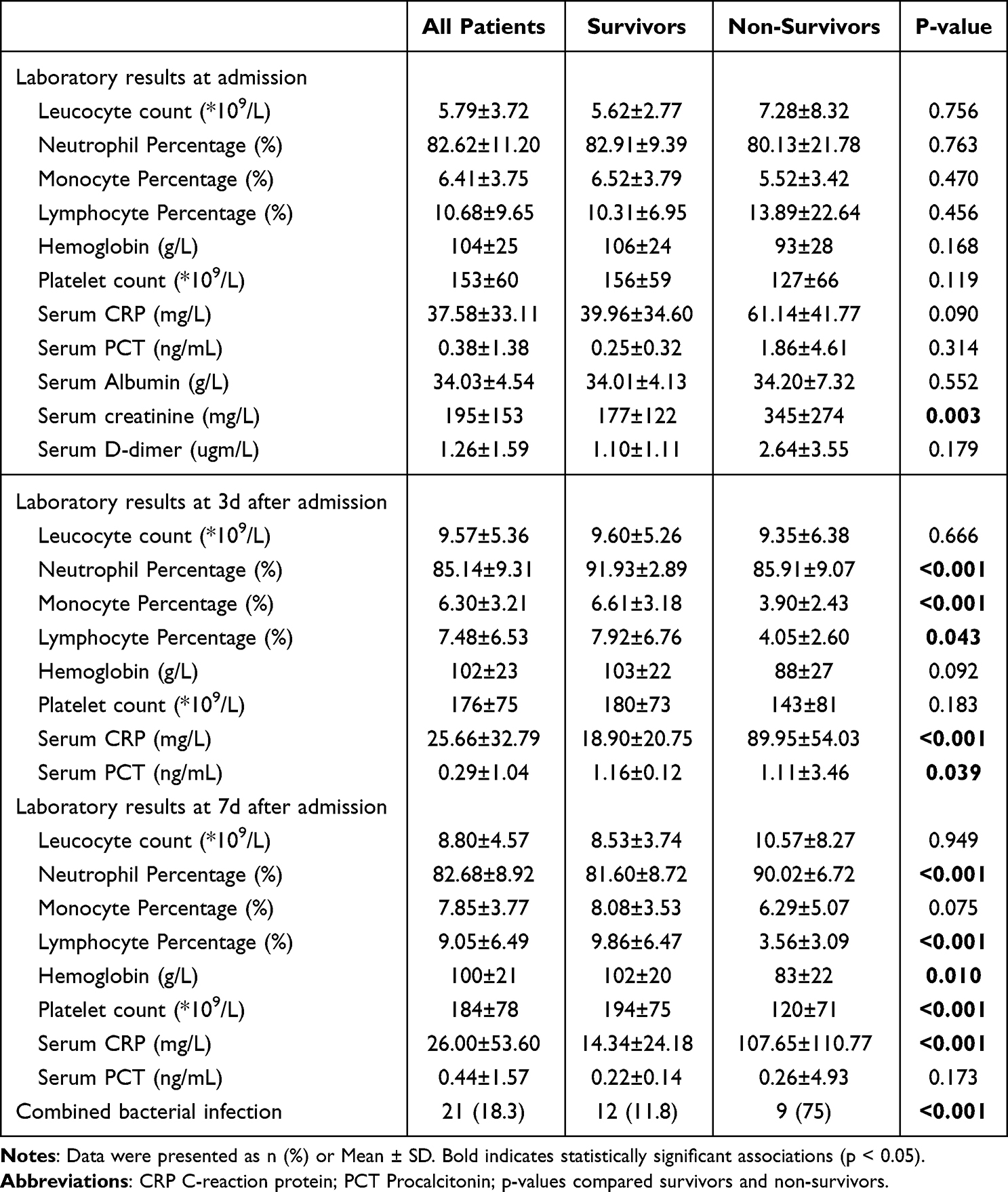 |
Table 2 Patients’ Laboratory Results |
Multivariate Logistic Regression Analysis
Our multivariate analysis identified several significant predictors of mortality among kidney transplant recipients who contracted COVID-19. Elevated serum C-reactive protein (CRP) levels at both 3 days (OR = 2.48, 95% CI: 2.18–2.79, p<0.001) and 7 days (OR = 3.06, 95% CI: 2.81–3.31, p<0.001) post-admission were associated with an increased risk of death. This suggests that higher inflammation levels, as indicated by CRP, significantly exacerbate mortality risk. The odds ratio (OR) of 2.48 for CRP at 3 days indicates that patients with elevated CRP levels are approximately 2.5 times more likely to die compared to those with lower levels, underlining the impact of systemic inflammation on patient outcomes. Furthermore, the presence of a combined bacterial infection was another significant predictor (OR = 1.94, 95% CI: 1.70–2.18, p<0.001), indicating nearly double the risk of mortality for affected individuals. Hemoglobin levels at 7 days post-admission also emerged as a critical factor (OR = 0.66, 95% CI: 0.42–0.90, p<0.001), suggesting that lower hemoglobin levels are associated with a higher risk of death. Table 3 shows the results of multivariate logistic regression analysis.
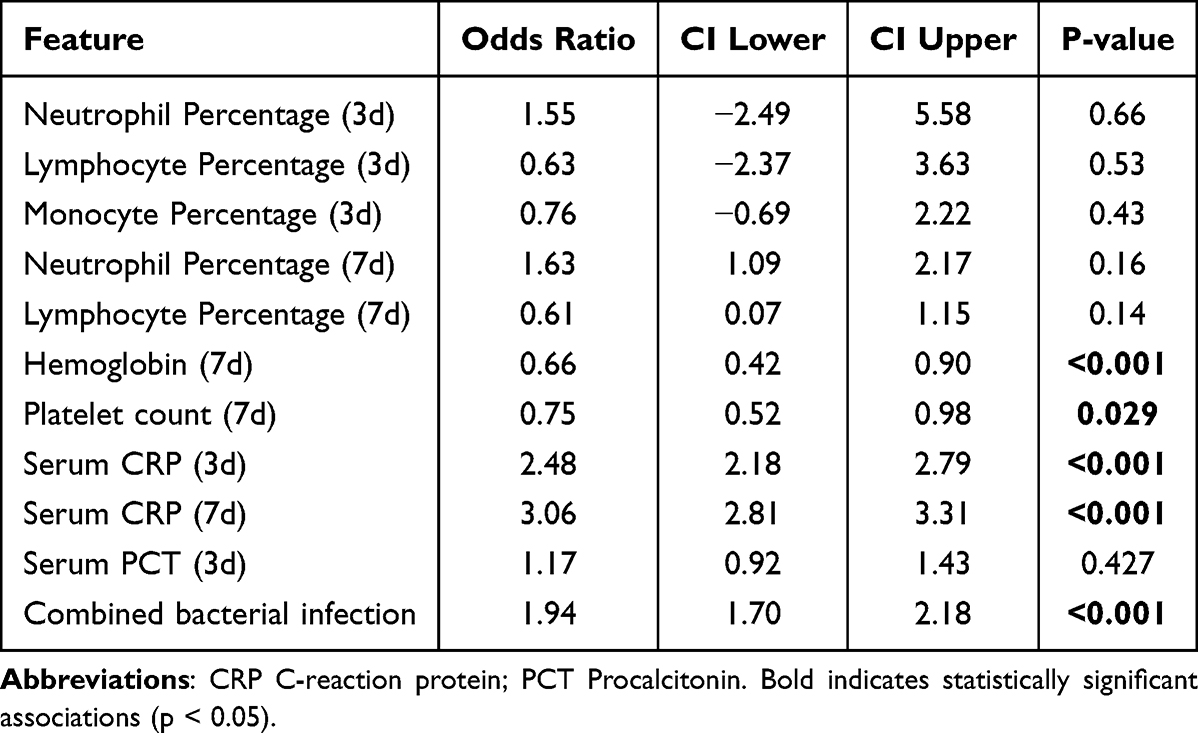 |
Table 3 Multivariate Analysis of Mortality Risk Factors for Retal Transplant Recipients |
Discussion
This study retrospectively explores the clinical outcomes of COVID-19 in kidney transplant recipients, with a particular focus on the clinical characteristics and risk factors associated with mortality. Through descriptive analysis, univariate analysis, and multivariate logistic regression, we have identified key factors that influence outcomes in this vulnerable population. Our findings on elevated CRP levels, serum creatinine, and the impact of bacterial coinfections not only provide insights into the pathophysiology of COVID-19 in transplant recipients but also offer a comparison point with existing studies, highlighting unique challenges and considerations for this group.
In our single-center study, we observed a 10.4% mortality rate among kidney transplant recipients who infected by COVID-19. This finding is significantly higher than the reported mortality rate of 0.5–1.0% in the general population infected with COVID-19.2,15,16 Demir et al reported a similar mortality rate of 9.9% among kidney transplant recipients during the COVID-19 pandemic.17 The increased mortality rate in kidney transplant recipients can be attributed to several factors. First, kidney transplant recipients are immunosuppressed to prevent organ rejection.18 This immunosuppression renders them more susceptible to infections, including COVID-19.19 Second, kidney transplant recipients often have underlying medical conditions, such as diabetes, hypertension, and cardiovascular disease, which can increase the risk of severe COVID-19.20,21 Third, kidney transplant recipients may experience delayed diagnosis and treatment of COVID-19 due to their immunosuppressed status. This can lead to more severe disease progression and higher mortality rates.22 A study by Wu et al found that the median time from symptom onset to diagnosis was longer in kidney transplant recipients with COVID-19 than in non-transplant patients with COVID-19.23
The vaccination rate among renal transplant recipients in our study was observed to be 21%, markedly lower than the reported national coverage in China, which stood at 89.54% for full vaccination and 91.89% for at least one dose as of February 2023. This contrast emphasizes the vaccination hesitancy or barriers faced by immunocompromised patients, despite the proven benefits of vaccination in reducing COVID-19 severity and mortality.24,25 In comparison, a study conducted in the United States found that only 41% of immunocompromised individuals received four doses of mRNA COVID-19 vaccine, with uptake of a fifth dose at just 0.9%.26 This indicates a global challenge in achieving optimal vaccination rates among immunocompromised populations, including those with cancer, organ transplant recipients, and patients with immune-mediated inflammatory disorders.
Notably, our findings reveal no significant differences in initial laboratory parameters including levels of C-reactive protein (CRP) and procalcitonin (PCT) between the two groups of patients upon admission. However, significant differences were observed on the 3rd and 7th day post-admission, particularly with CRP levels, which emerged as an independent risk factor for mortality in multivariate analysis. The absence of early differences in inflammatory markers between the groups suggests a similar initial immune response to COVID-19 infection among kidney transplant recipients. This finding aligns with early observations in the general population, indicating that the initial immune response may not significantly differ in immunocompromised individuals.27–29 However, the subsequent divergence in CRP levels on the 3rd and 7th day highlights a critical period where the inflammatory response, and possibly the viral replication dynamics, could differ significantly in patients leading to varied outcomes.30 Our results underscore the prognostic value of CRP as an indicator of disease severity and mortality risk in this patient population. Elevated CRP levels have been widely recognized as markers of inflammation and have been linked to poor outcomes in various infectious diseases, including COVID-19.31,32 In the context of kidney transplant recipients, the heightened inflammatory response indicated by rising CRP levels may reflect a combination of viral pathogenicity and the unique immunological landscape of these patients, which could exacerbate disease severity.33,34 Moreover, the identification of CRP levels on the 3rd and 7th day as independent risk factors for mortality provides valuable insights for clinical management. It suggests that close monitoring of CRP levels during this critical period could aid in early identification of patients at higher risk of adverse outcomes, thereby facilitating timely interventions.
Although there was no statistically significant relationship between Lymphocyte Percentage, Neutrophil Percentage, and Monocyte Percentage and mortality in the multifactorial analysis, we observed that these indices were significantly lower in the patients in the mortality group than in the patients in the non-mortality group. This finding beckons an in-depth exploration into the potential underlying biological mechanisms. The observed reduction in immune cell ratios, particularly lymphocytes, neutrophils, and monocytes, suggests a compromised immune system, which plays a pivotal role in defending the body against infections and malignancies.35 Specifically, the decreased lymphocyte count could signal an impaired capacity to combat infectious agents and tumor cells.36 Simultaneously, a reduction in neutrophil and monocyte ratios may indicate a weakened inflammatory response, crucial for the initial defense against pathogens and for orchestrating an effective immune response.37,38 Furthermore, the diminished Neutrophil Percentage, by reflecting an inadequate inflammatory response, might impair the clearance of pathogens and necrotic tissues, potentially exacerbating patient mortality and facilitating disease progression.39 This scenario underscores the importance of further research into how variations in these immune parameters can influence patient outcomes, providing insights into the complex interplay between immune response efficiency and clinical prognosis in life-threatening conditions.
The observed significant reduction in hemoglobin and platelet levels by the 7th day of hospitalization in the non-survivor group among kidney transplant recipients with COVID-19, and their identification as independent risk factors for mortality. The association between lower hemoglobin levels and increased mortality risk in COVID-19 patients, including those with kidney transplants, can be multifactorial.40,41 Hemoglobin, the oxygen-carrying component of red blood cells, is crucial for tissue oxygenation. Its reduction could indicate several underlying conditions, such as anemia of chronic disease, hemolysis, or bleeding, which may be exacerbated by the systemic inflammation and immune dysregulation caused by SARS-CoV-2 infection.42 Furthermore, reduced hemoglobin levels may impair oxygen delivery to tissues, exacerbating hypoxia, a critical determinant of COVID-19 severity.43 In the context of kidney transplantation, medications, underlying chronic kidney disease, or the infection itself could contribute to anemia, highlighting the need for careful management of these patients. Similarly, low platelet levels, observed in the non-survivor group, is a significant finding. Platelets play a vital role in hemostasis and are also involved in the immune response to infections.44 Thrombocytopenia in COVID-19 patients has been associated with increased disease severity and mortality, potentially reflecting a heightened state of systemic inflammation, endothelial dysfunction, and coagulopathy commonly observed in severe infections.45,46 This condition can lead to disseminated intravascular coagulation (DIC), contributing to organ failure and adverse outcomes. The interaction between the virus, immune system, and endothelium, especially in immunosuppressed individuals such as kidney transplant recipients, might further amplify these effects, underscoring the importance of monitoring and managing these parameters closely.47,48 Given these observations, it is imperative to closely monitor hemoglobin and platelet levels in kidney transplant recipients with COVID-19, as changes in these parameters may serve as early indicators of disease progression towards severe outcomes.
The study, while providing valuable insights into the outcomes of renal transplant recipients infected with COVID-19, is subject to several limitations that merit consideration. First, the research is confined to a single large teaching hospital, which may impact the generalizability of the findings to different healthcare settings or populations. This constraint could limit the applicability of the results to broader, more diverse cohorts. Second, the retrospective nature of the study introduces inherent limitations related to the accuracy and completeness of medical records. The potential for biases in data recording and the challenge of controlling for all confounding variables might affect the robustness of the conclusions. Lastly, the sample size of 115 participants, though substantial, may not fully capture the variability and nuances of clinical outcomes in this patient population. A larger, more diverse cohort could enhance the validity of the findings and allow for a more detailed analysis of factors influencing mortality and morbidity in renal transplant recipients following COVID-19 infection.
Conclusion
In conclusion, this study underscores the complex interplay of systemic inflammation, renal impairment, and bacterial coinfections in determining the outcomes of COVID-19 in kidney transplant recipients. By comparing our findings with existing literature, we highlight both the challenges and the opportunities for optimizing the care of this vulnerable population. As the global medical community continues to navigate the COVID-19 pandemic, the insights from this study will be crucial in guiding clinical management and shaping future research directions.
Ethics Approval and Consent to Participate
The ethical approval for this investigation was obtained from the Medical Research Ethics Committee of the First Affiliated Hospital of USTC, under the approval identifier 2023-RE-149. Due to the retrospective and traceable characteristics of the study, the committee granted a waiver for informed consent. The institution maintains a steadfast dedication to safeguarding patient confidentiality and ensuring compliance with the ethical guidelines delineated in the Helsinki Declaration. Official approval documents can be made accessible upon request for verification purposes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from Anhui Provincial Natural Science Foundation (2208085MH234 to Peng Jin).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Qin C, Du M, Wang Y, et al. Assessing acceptability of the fourth dose against COVID-19 among Chinese adults: a population-based survey. Hum Vaccin Immunother. 2023;19:2186108. doi:10.1080/21645515.2023.2186108
2. Guan WJ, Ni ZY, Hu Y, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382:1708–1720. doi:10.1056/NEJMoa2002032
3. Williamson EJ, Walker AJ, Bhaskaran K, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584:430–436. doi:10.1038/s41586-020-2521-4
4. Postolache PA, Nechifor A, Buculei I, Soare I, Mocanu H, Petrariu FD. Clinical features and paraclinical findings in patients with SARS CoV-2 pneumonia and the impact of pulmonary rehabilitation on the instrumental activities of daily living in POST-COVID-19 patients. J Pers Med. 2023;14:13. doi:10.3390/jpm14010013
5. Roberts MB, Izzy S, Tahir Z, Al Jarrah A, Fishman JA, El Khoury J. COVID-19 in solid organ transplant recipients: dynamics of disease progression and inflammatory markers in ICU and non-ICU admitted patients. Transpl Infect Dis. 2020;22:e13407.
6. Pereira MR, Mohan S, Cohen DJ, et al. COVID-19 in solid organ transplant recipients: initial report from the US epicenter. Am J Transplant. 2020;20:1800–1808. doi:10.1111/ajt.15941
7. Niemann CU, da Cunha-Bang C, Helleberg M, Ostrowski SR, Brieghel C: patients with CLL have a lower risk of death from COVID-19 in the Omicron era. Blood. 2022;140:445–450. doi:10.1182/blood.2022016147
8. Treon SP, Castillo JJ, Skarbnik AP, et al. The BTK inhibitor ibrutinib may protect against pulmonary injury in COVID-19-infected patients. Blood. 2020;135:1912–1915. doi:10.1182/blood.2020006288
9. Sigera LSM, Denning DW, Etayo J, Beltrán-Sanz N. Invasive aspergillosis after renal transplantation. J Fungi. 2023;10:9. doi:10.3390/jof10010009
10. Vinod PB, Sharma RK. Opportunistic infections (non-cytomegalovirus) in live related renal transplant recipients. Indian J Urol. 2009;25:161–168. doi:10.4103/0970-1591.39547
11. Mangalgi S, Madan K, Das CJ, et al. Pulmonary infections after renal transplantation: a prospective study from a tropical country. Transpl Int. 2021;34:525–534. doi:10.1111/tri.13817
12. Velioglu A, Guneri G, Arikan H, et al. Incidence and risk factors for urinary tract infections in the first year after renal transplantation. PLoS One. 2021;16:e0251036.
13. Rangel EB, de Lucena DD, Aguiar-Brito I, et al. COVID-19 in kidney transplant recipients with diabetes mellitus: a propensity score matching analysis. Transpl Int. 2022;35:10375. doi:10.3389/ti.2022.10375
14. AbdulRahim N, McAdams M, Xu P, et al. Association of inflammatory biomarkers with immunosuppression management and outcomes in kidney transplant recipients with COVID-19. Transplant Proc. 2021;53:2451–2467. doi:10.1016/j.transproceed.2021.08.002
15. Luo D, Mei B, Wang P, et al. Prevalence and risk factors for persistent symptoms after COVID-19: a systematic review and meta-analysis. Clin Microbiol Infect. 2024;30:328–335. doi:10.1016/j.cmi.2023.10.016
16. Faramarzi A, Norouzi S, Dehdarirad H, Aghlmand S, Yusefzadeh H, Javan-Noughabi J. The global economic burden of COVID-19 disease: a comprehensive systematic review and meta-analysis. Syst Rev. 2024;13:68. doi:10.1186/s13643-024-02476-6
17. Demir E, Ucar ZA, Dheir H, et al. COVID-19 in kidney transplant recipients: a multicenter experience from the first two waves of pandemic. BMC Nephrol. 2022;23:183. doi:10.1186/s12882-022-02784-w
18. Szumilas K, Wilk A, Wisniewski P, et al. Current status regarding immunosuppressive treatment in patients after renal transplantation. Int J Mol Sci. 2023;25:24. doi:10.3390/ijms25010024
19. Zong K, Peng D, Yang H, et al. Risk factors for weak antibody response of SARS-CoV-2 vaccine in adult solid organ transplant recipients: a systemic review and meta-analysis. Front Immunol. 2022;13:888385. doi:10.3389/fimmu.2022.888385
20. Fava A, Cucchiari D, Montero N, et al. Clinical characteristics and risk factors for severe COVID-19 in hospitalized kidney transplant recipients: a multicentric cohort study. Am J Transplant. 2020;20:3030–3041. doi:10.1111/ajt.16246
21. Ajaimy M, Liriano-Ward L, Graham JA, Akalin E. Risks and benefits of kidney transplantation during the COVID-19 pandemic: transplant or not transplant? Kidney360. 2021;2:1179–1187. doi:10.34067/KID.0002532021
22. Karas M, Bernal I, Diaz O, et al. A scoping review of the impact of COVID-19 on kidney transplant patients in the United States. Cureus. 2023; 15:e35725.
23. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in china: summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA. 2020;323:1239–1242. doi:10.1001/jama.2020.2648
24. Costantino A, Morlacchi L, Donato MF, et al. Hesitancy toward the full COVID-19 vaccination among kidney, liver and lung transplant recipients in Italy. Vaccines. 2022;11:10. doi:10.3390/vaccines11010010
25. Pan Y, Gong S, Zhu X, et al. Investigation on the hesitancy of COVID-19 vaccination among liver transplant recipients: a cross-sectional study in China. Front Public Health. 2022;10:1014942. doi:10.3389/fpubh.2022.1014942
26. Tartof SY, Slezak JM, Puzniak L, et al. Analysis of mRNA COVID-19 vaccine uptake among immunocompromised individuals in a large US health system. JAMA Network Open. 2023;6:e2251833.
27. Cantarelli C, Angeletti A, Perin L, et al. Immune responses to SARS-CoV-2 in dialysis and kidney transplantation. Clin Kidney J. 2022;15:1816–1828.
28. Gleeson S, Martin P, Thomson T, et al. Lack of seroresponse to SARS-CoV-2 booster vaccines given early post-transplant in patients primed pre-transplantation. Front Immunol. 2022;13:1083167. doi:10.3389/fimmu.2022.1083167
29. Antinori A, Bausch-Jurken M. The burden of COVID-19 in the immunocompromised patient: implications for vaccination and needs for the future. J Infect Dis. 2023;228:S4–S12.
30. Garcia LF. Immune response, inflammation, and the clinical spectrum of COVID-19. Front Immunol. 2020;11:1441. doi:10.3389/fimmu.2020.01441
31. Lentner J, Adams T, Knutson V, et al. C-reactive protein levels associated with COVID-19 outcomes in the United States. J Osteopath Med. 2021;121:869–873. doi:10.1515/jom-2021-0103
32. Abdullah AJ, Arif AT, Rahman HA, et al. Assessing serum C-reactive protein as a predictor of COVID-19 outcomes: a retrospective cross-sectional study. Ann Med Surg Lond. 2023;85:3359–3363. doi:10.1097/MS9.0000000000000761
33. Heldal TF, Asberg A, Ueland T, et al. Inflammation in the early phase after kidney transplantation is associated with increased long-term all-cause mortality. Am J Transplant. 2022;22:2016–2027. doi:10.1111/ajt.17047
34. Luan YY, Yin CH, Yao YM. Update advances on C-Reactive protein in COVID-19 and other viral infections. Front Immunol. 2021;12:720363. doi:10.3389/fimmu.2021.720363
35. Casanova JL, Abel L. Mechanisms of viral inflammation and disease in humans. Science. 2021;374:1080–1086. doi:10.1126/science.abj7965
36. Huang Y, Guo Y, Huang L, et al. Kisspeptin-54 attenuates oxidative stress and neuronal apoptosis in early brain injury after subarachnoid hemorrhage in rats via GPR54/ARRB2/AKT/GSK3beta signaling pathway. Free Radic Biol Med. 2021;171:99–111.
37. Baba DF, Suciu H, Avram C, et al. Elevated levels of neutrophil-to monocyte ratio are associated with the initiation of paroxysmal documented atrial fibrillation in the first two months after heart transplantation: a uni-institutional retrospective study. J Cardiovasc Dev Dis. 2023;2023:10.
38. Peng B, Yang M, Zhuang Q, et al. Standardization of neutrophil CD64 and monocyte HLA-DR measurement and its application in immune monitoring in kidney transplantation. Front Immunol. 2022;13:1063957. doi:10.3389/fimmu.2022.1063957
39. Buonacera A, Stancanelli B, Colaci M, Malatino L. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23:3636. doi:10.3390/ijms23073636
40. Kuno T, So M, Takahashi M, Egorova NN. U shape association of hemoglobin level with in-hospital mortality for COVID-19 patients. J Thromb Thrombolysis. 2022;53:113–117. doi:10.1007/s11239-021-02516-1
41. Veronese N, Segala FV, Carruba L, et al. Anemia as a risk factor for disease progression in patients admitted for COVID-19: data from a large, multicenter cohort study. Sci Rep. 2023;13:9035. doi:10.1038/s41598-023-36208-y
42. Mancilha EMB, Oliveira JSR. SARS-CoV-2 association with hemoglobin and iron metabolism. Rev Assoc Med Bras. 2021;67:1349–1352. doi:10.1590/1806-9282.20210555
43. Rogers SC, Brummet M, Safari Z, et al. COVID-19 impairs oxygen delivery by altering red blood cell hematological, hemorheological, and oxygen transport properties. Front Physiol. 2023;14:1320697. doi:10.3389/fphys.2023.1320697
44. Sonmez O, Sonmez M. Role of platelets in immune system and inflammation. Porto Biomed J. 2017;2:311–314. doi:10.1016/j.pbj.2017.05.005
45. Asrie F, Tekle E, Gelaw Y, et al. Baseline thrombocytopenia and disease severity among COVID-19 patients, tibebe ghion specialized hospital COVID-19 treatment center, Northwest Ethiopia. J Blood Med. 2022;13:315–325. doi:10.2147/JBM.S366478
46. Yang Q, Gao J, Zeng X, Chen J, Wen D. Relationship between platelet count and in-hospital mortality in adult patients with COVID-19: a retrospective cohort study. Front Med Lausanne. 2022;9:802412. doi:10.3389/fmed.2022.802412
47. Vanichanan J, Udomkarnjananun S, Avihingsanon Y, Jutivorakool K. Common viral infections in kidney transplant recipients. Kidney Res Clin Pract. 2018;37:323–337. doi:10.23876/j.krcp.18.0063
48. Piotti G, Palmisano A, Maggiore U, Buzio C. Vascular endothelium as a target of immune response in renal transplant rejection. Front Immunol. 2014;5:505. doi:10.3389/fimmu.2014.00505
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.